External auditory canal anatomy pathologies & management
101
Dr. vikas
-
Upload
vikas-jorwal -
Category
Health & Medicine
-
view
611 -
download
2
Transcript of External auditory canal anatomy pathologies & management

Dr. vikas

External Auditory Canal
The supporting framework of the canal wall is cartilage in the lateral one-third and bone in the medial two-thirds.
Length of the canal is approximately 2.4 cm
The lateral cartilaginous portion is about 8 mm long and is continuous with the auricular cartilage.
The two or three variably present perforations in the anterior aspect of the cartilaginous canal are the fissures of Santorini.
The isthmus is the narrowest portion of the EAC, lies just medial to the junction of the bony and cartilaginous canals.

Cartilaginous part is directed upwards, backwards & medially while bony part is directed downwards, forwards & medially.
The canal is straightened by gently moving the auricle upwards and backwards to counteract the direction of the cartilaginous portion.
In the neonate, there is no bony external meatus as the tympanic bone is not yet developed.
The tympanic membrane is more horizontally placed so that the auricle must be gently drawn downwards and

The medial border of the meatal cartilage is attached to
the rim of the bony canal by fibrous bands.
The bony canal wall, about 1.6 mm long, is narrower than
the cartilaginous portion and itself becomes smaller
closer to the tympanic membrane.
The medial end of the bony canal is marked by a groove,
the tympanic sulcus, which is absent superiorly. Although
the tympanic bone makes up the greater part of the
canal, and also carries the sulcus, the squamous bone
forms the roof.
The tympanomastoid suture is a complex suture line
between the anterior wall of the mastoid process and the
tympanic bone.

The external canal is lined with skin.
Body skin normally grows directly from the basal layers towards the surface where it is shed into the surroundings.
If this pattern of growth were to occur in the external ear canal then the canal would soon become filled with desquamated skin.
Instead of maturation taking place directly towards the surface, there is outward, oblique growth of the epidermis of the canal skin and pars flaccida so that the surface layers effectively migrate towards the external opening of the canal.

Atresia Atresia is the absence of or closure of a passage of the body.
This includes both congenital and acquired lesions.
TOS defines acquired atresia of the external ear as 'intraluminal
sequelae of either intraluminal or extraluminal processes of varying
aetiology, resulting in a blind sac in the external acoustic meatus'.
Epidemiology
1 in 10,000 to 15,000 births
Up to 50% of the time associated with some craniofacial syndrome
Unilateral : Bilateral, about 3:1
30% are bilateral
Atresia : Microtia, 7:1
Slightly more common on the right
Male : Female, 2:1

AtresiaAural atresia associated with craniofacial
syndromes
Treacher Collins (Mandibulofacial Dysostosis)
Nager Syndrome (Acrofacial Dysostosis)
Cruzoun’s Craniofacial Dysostosis
Goldenhar’s Syndrome
Hemifacial Microsomia

Atresia
Embryology – 7th Month
Canalization complete
Mastoid separation from mandible
Normal posterior-
inferior growthNo mastoid
growth
Normal Atresia

Atresia
Embryology
Mastoid growth affects the facial nerve position
Normal 120o
CurveAcute Curve in
Atresia

Atresia

12/11/201411

Classification of Deformities
After Colman-3 types
Minor Aplasia-incomplete recanalization
Moderate Aplasia- the tympanic bone has
developed but has failed to recanalize
Severe Aplasia-complete absence of the external
canal

Atresia
Severe Aplasia- Complete Atresia, no tympanic
bone

AtresiaModerate Aplasia
The most common, solid mass of compact bone
that has failed to recanalize

Atresia
Minor Aplasia-partial recanalization
Middle space constricted, often with severe ossicular
abnormalities

Radiological Evaluation
High resolution CT in coronal and axial planes
Axial to delineate malleus, incus and I-S joint and
round window
Coronal to delineate stapes, oval window and
vestibule
3-D CT of little help

Atresia Surgery
First attempt to surgically correct aural atresia
was by Thomson in 1843
Shambaugh, 1967, recommended unilateral
surgery only if the cochlear reserve allowed
hearing to improve by 25dB
Jahrsdoerfer, 1978, first large series using the
anterior approach

Surgical Considerations
Most consider repair in bilateral atresia
Many are reluctant to operate on unilateral cases
Not simply the hearing loss
Expectations of hearing recovery
Lifetime care of mastoid cavity
Potential risks to facial nerve and labyrinth
55-65% achieve 25 dB speech-hearing level

Surgical Considerations
Most surgeons choose the anterior approach to
avoid the mastoid cavity
40% of patients with unilateral atresia are not
surgical candidates such as those with severe
aplasia as in Treacher Collins syndrome
Bilateral atresia- best ear by CT done as child
approaches school age

Surgical ConsiderationsTiming of surgery
Usually performed after age 6 or 7 years
This allows for microtia repair to be done first
Canal cholesteatoma in the stenotic ear usually develops in canals less than 2mm in diameter. If ear unfavorable, canalplasty alone is offered

Surgical Technique
Minor aplasia- canal widening and middle ear
ossicular work with tympanoplasty
Moderate Aplasia
Mastoid or posterior approach
Anterior approach

Surgical Technique
Anterior Approach
Middle ear approached through the atretic bone
with a limited mastoid opening

Surgical Technique
The posterior wall of the
glenoid fossa becomes the
anterior wall of the new ear
canal
The epitympanum is the first
part of the middle ear
encountered
Fused ossicles identified

Surgical Technique
Atretic bone removed at times with a curette
Globular mass separated from the stapes to
avoid cochlear trauma
Course of facial nerve determined
Ossiculoplasty performed
Tympanic membrane grafted
Meatoplasty
Split thickness skin graft (.006-.008 inches) lines
the canal

Surgical Technique
The Meatoplasty must be aligned with the newly
created bony canal

Surgical Technique
3cm X 5cm split thickness skin graft
The graft is positioned in the canal and sewn to the meatal margin
Graft stabilized with Merocelwicks and hydrated with ear drops

MASTOID APPROACH This employs a more posterior route to the middle ear
cleft using the dura of the middle cranial fossa, the
sigmoid sinus and sino dural angles as landmarks to
the antrum with subsequent identification of the lateral
semicircular canal (LSCC), atretic plate and the facial
nerve.
The atretic plate is removed in a similar fashion, trying
to centre the cavity on the stapes.
The aim is to create a stable, small, cavity lined with
squamous epithelium.

Hearing Results
Post-op hearing level of 30 dB or better In 50-
75% of patients with moderate or severe aplasia
20 dB or better in 15-20%
Bellucci 20 dB in 50% @ 2 years
Schuknect similar results at 1.3 years
De La Cruz 56 patients 53% @ 20 dB at 6 mo.
Lambert early 60% @25 dB, 46% >1 yr.

Alternatives to Surgery
Bone anchored hearing aid (BAHA)

Surgical Complications Persistent or recurrent conductive hearing loss
Lateralization of graft Scar tissue
SNHL
VIIth Nerve injury
30 % revision rate Re-stenosis Graft migration Inadequate hearing
Chronic cavity infection

Acquired atresia of the
external ear

Atresias may be solid or membranous.
Solid atresia consists of a continuous block of either fibrous or fibrous & bony material which is continuous with the structure of the tympanic membrane and is of variable extent.
Solid atresia, obliterating the medial aspect
of
the bony external ear canal.
Extensive funnel-shaped solid atresia.

Membranous atresia is typified by fibrous tissue that has a covering of ear canal skin on both sides, thus separating the ear canal into a medial and lateral segment.
The medial part inevitably collects keratin from desquamation of the skin; this may become an erosive process and thus be defined as an external auditory canal cholesteatoma.
Membranous atresia in lateral external
auditory meatus.

Diagnosis
The clinical diagnosis of acquired atresia is
supported by the use of computed tomography
(CT) scanning
It particularly helps in the differentiation of solid
and membranous atresia.
Solid atresia is a safe form of ear disease.
Membranous atresia will inevitably produce
associated cholesteatoma and therefore erosion
of local structure.
Surgical outcome is superior to solid atresia.

AETIOLOGYInflammation
- otitis externa;
- psoriasis, eczema and other dermatological conditions;
- active chronic otitis media;
- Trauma
- burns, (thermal, chemical, electrical or post-irradiation)
Surgery – any operation involving a meatal approach
(tympanoplasty, etc,)
Meatal surgery (removal of an osteoma)

Pathogenesis
SOLID ATRESIA
In cases associated with otitis externa or media the key development is of granular medial otitis externa with granulations of the tympanic membrane that persist for many months in spite of treatment.
The granulations become fibrotic and the eardrum thickens as the medial meatal mass is re-epitheliazed.
principle complaint is of conductive hearing loss.
MEMBRANOUS ATRESIA
This originates in the lateral meatus as a web formation, which is precipitated by a circular irritation from inflammation, trauma or burns and ulceration of the skin around the entire circumference of the external ear canal.
The web-like stenosis forms after fibrosis and re-epitheliazation as with solid atresias.
Associated with medial cholesteatoma, which can potentially produce local erosion and complications.

MANAGEMENT OPTIONS
Medical
During the wet phase, the medial granulations can
be removed by aspiration and cauterization with
silver nitrate or trichloroacetic acid, and the ear
packed with ribbon gauze or a wick.
This local treatment may result in a change to the
dry phase and prevent further progression of the
atresia.
The conductive hearing impairment (if bilateral) may
be managed by hearing aid.

SurgeryFIBROUS ATRESIA
The principle of surgery in fibrous atresia
is to remove the fibrous tissue by
elevating it from the ear canal bone, the
fibrous annulus and lamina propria of the
tympanic membrane.
A circumferential incision is made lateral
to the blunt face of the atretic plate and a
plane of dissection developed between
the bone of the ear canal and the canal
skin, followed by the atretic plate and,
finally, lateral to the fibrous annulus and
lamina propria of the tympanic membrane.
The epithelial defect is repaired by a fine
split skin graft which can be laid in single
or multiple pieces.
A silastic disc or tube may be inserted to
stabilize the epithelial surface. Finally, the
ear canal is packed with ribbon gauze
soaked in antiseptic.

MEMBRANOUS ATRESIA
Similar to fibrous atresia, membranous atresia can
be approached transcanal using an ear speculum.
If the fibrous lesion is very thick a retroauricular
approach may be superior, allowing preservation of
the lateral and medial epithelial coverings to aid
repair of the ear canal skin.
The whole lesion is excised with sacrifice of the
minimum of surrounding epithelium.
Silastic sheets are overlaid, holding the lateral and
medial skin edges against the bone of the ear canal.

Pathological conditions

Furunculosis Localized form of otitis externa resulting from infection
of a single hair follicle.
Hair follicles are only present in the lateral (cartilaginous) segment of the external auditory canal.
Furunculosis is, therefore, confined to the lateral canal.
Bacterial invasion of a single hair follicle results initially in a well-circumscribed deep skin infection.
As the infection progresses a pustule forms and this progresses to local abscess formation, often with considerable associated cellulitis and oedema.

FurunculosisFuruncle of the external auditory canal.
Localized rather than generalized oedema of otitisexterna.
The affected ear is extremely painful, feels blocked and exudes a scanty serosanguinousdischarge.
The pinna and tragus are tender on palpation.
Otoscopic examination usually establishes the diagnosis

Characteristically, the oedema and inflammation
is restricted to the lateral segment of the canal,
with relative sparing of the medial canal and an
unaffected tympanic membrane.
If the infection is advanced, the abscess may be
seen to be pointing into the canal or have
discharged already.
If the oedema and secondary cellulitis spreads to
the post -auricular crease, the condition may be
mistaken for acute mastoiditis.

AETIOLOGY AND EPIDEMIOLOGY
Staphylococcus aureus is the most common organism causing furunculosis.
Leukocidal toxins of S. aureus trigger lysis of phagocytic cells and may have an important role in cutaneous infection.
Local risk factors include heat, humidity, trauma, maceration.
Recurrent furunculosis presents as repeated episodes of infection at multiple sites.
Conditions associated with recurrent furunculosisinclude hypogammaglobulinaemia, diabetes mellitus and dysphagocytosis.

OUTCOMES If untreated, the infection usually progresses to a
localized abscess which then discharges into the
external ear canal.
With adequate drainage the infection will resolve
spontaneously.
The infection can also spread towards the deeper
tissues, where it may cause a diffuse soft tissue
infection spreading to the pinna, post-auricular skin
and parotid gland.
Repeated infection can cause permanent scarring
and fibrosis of the external canal with subsequent
meatal stenosis.

MANAGEMENT
Furunculosis of the external canal is exquisitely
painful and appropriate analgesics should be
offered to all patients.
Treatment choices include:
oral or systemic antistaphylococcal antibiotics
(penicillinase-resistant penicillin, macrolide,
cephalosporin, clindamycin or quinolone);
topical treatment (antibiotics, astringents,
hygroscopic dehydrating agents);
incision and drainage.

MANAGEMENT OPTIONS Oral antibiotic treatment is recommended in the early
stages of the disease.
Severe spreading soft tissue infection should be treated
with intravenous antibiotic therapy.
Abscess formation is an indication for drainage.
After the abscess has discharged, surgically or
spontaneously, topical treatment is preferable.
Topical antibiotics are prescribed.
Insertion of a wick into the ear canal facilitates treatment
in the presence of severe canal oedema and narrowing.

Glycerol and ichthammol solution has a specific antistaphylococcal action and is hygroscopic, thus causing dehydration of the canal tissue. Aluminiumacetate solution is an astringent as well as a hygroscopic agent.
Options include:
eradication therapy with nasal mupirocin;
eradication therapy with oral flucloxacillin for 14 days;
bacterial interference therapy:
Deliberately implanting a nonpathogenic strain of S. aureus(strain S02A is the most popular) to recolonizethe nares and skin.

BuIlous myringitis
Bullous myringitis (myringitis bullosa
haemorrhagica) is the finding of vesicles in the
superficial layer of the tympanic membrane.
PATHOLOLOGY
The vesicles occur between the outer epithelium
and the lamina propria of the tympanic
membrane.

AETIOLOGY Cultures from aspirates of the vesicles and middle ear
fluid are similar to that in acute otitis media.
An infection by influenza virus or by Mycoplasma
pneumoniae has been suggested as the aetiological
agent but no evidence for this, other than circumstantial,
has been presented.
Bullous myringitis occurs in all age groups but children,
adolescents and young adults are more frequently
affected

SYMPTOMS
Sudden onset of severe, usually unilateral, often
throbbing pain in the ear is the most common
presentation?
The symptoms usually set in during or following
an upper respiratory tract infection.
A blood stained discharge can be present for a
couple of hours.
Hearing impairment (conductive and/or
sensorineural) is common in the affected ear.

SIGNS
Otoscopy reveals blood-filled, serous or serosanginous blisters involving the tympanic membrane and sometimes the medial aspect of the ear canal.
A serosanginous secretion can be seen if the blisters rupture.
The tympanic membrane is intact.
In young children with bullous myringitis, middle ear fluid was present in the majority (97 percent) but is an uncommon finding in other age groups.
The site of the sensorineural hearing loss is the cochlea; however, the‘ pathogenic base is not understood.

DIAGNOSIS
The clinical entity, bullous
myringitis is based on
physical examination.
Vesicles in the superficial
layer of the tympanic
membrane are present.
The main differential
diagnoses are acute otitis
media or herpes zoster
oticus.
Bullae on the tympanic membrane

Investigations Inspection of the ear using a microscope is essential for
diagnosis. Pneumatic otoscopy and tympanometry help
determine whether the middle ear contains fluid.
Pure-tone audiogram including bone conduction
thresholds is essential for detection of sensorineural
hearing impairment.
A serologic sample for herpes zoster is of value in cases
with sensorineural hearing loss and may be of help in the
differential diagnosis.

MANAGEMENT OPTIONS
In cases without middle ear affection and without sensorineural hearing loss, only analgesics are recommended.
When the middle ear is affected, antibiotics can be used as in the treatment of acute otitis media.
In children less than two years of age, acute bullous myringitisshould be treated as acute otitis media.
Antibiotics have also been recommended in cases with sensorineural hearing impairment.
Effect of management
Spontaneous resolution of the blisters and middle ear effusion.
Complete recovery of the sensorineural impairment within three months occurred in between 60 and 100 percent of affected patients treated with amoxicillin.

Granular myringitis
DEFINITION
Characterized by granulation tissue on the lateral
aspect of the tympanic membrane with possible
involvement of the external ear canal
Some authors have suggested there are two
distinct entities:
Myringitis externa granulosa- has granulations on
the lateral surface of the drum and the medial part
of the ear canal skin.
Granular myringitis- only involves the eardrum.

PATHOLOGY
Microscopic examination shows oedematous
granulation tissue with capillaries and diffuse
infiltration of chronic inflammatory cells.
Large areas of the granulation tissue have no
covering epithelium.
It has been suggested that a non-specific injury
involving the lamina propria of the tympanic
membrane suppresses epithelialization which leads to
the development of granulation tissue.

AETIOLOGY The incidence of granular myringitis is not related to sex,
age, systemic disease or season,
High-ambient temperature, swimming, lack of hygiene, local irritants and foreign bodies have all been suggested as causative factors.
bacterial and sometimes fungal infection is present in the affected ear.
Granular myringitis is also occasionally seen as a postoperative complication of tympanic membrane grafting.
An incidence of up to 5 percent has been reported and the use of tympanic homo grafts seems to result in a higher incidence (8 percent).

SYMPTOMS
The dominant symptom is a foul-smelling
discharge from the affected ear.
There is usually little or no pain.
Some individuals have a sensation of fullness or
irritation in the ear.
The hearing is either not at all or only slightly
impaired.
Associated tinnitus is uncommon.
Some patients can be asymptomatic

SIGNS Purulent secretion is seen in the affected ear.
The tympanic membrane is covered with secretions that sometimes crust.
After aural toilet the granulation tissue is revealed.
There seems to be a localized and a diffuse form of granular myringitis.
The localized form is most common, in that small areas of the drum are affected or one or more polyps are present.
Most commonly, the granulations are situated posterosuperior on the eardrum and may affect the adjacent canal wall.
A slightly raised carpet of granulations, which covers the tympanic membrane, is seen in the diffuse form.
Perforation of the tympanic membrane is not present

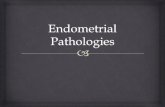
Right granular myringitis. (a)
There is pus in the canal but the
pars tensa appears intact.
However, there is granulation
tissue arising from it posteriorly
extending on to the adjacent
canal wall. The intactness of the
pars tensa can be confirmed by
pneumatic otoscopy or
tympanometry.
(b) The ear is active, there being
pus in the canal and granulation

DIAGNOSIS
In granular myringitis a discharge from the ear is present.
Inflammation and granulation tissue are seen on the lateral aspect of the tympanic membrane with possible involvement of the external ear canal.
Differential diagnoses are-
chronic (suppurative) otitis media
diffuse external otitis.
Most cases can readily be differentiated by the normal movement of the tympanic membrane on pneumatic otoscopy and no signs of an inflammatory reaction in the lateral ear canal.
The lack of a conductive hearing impairment and a normal computed tomography (CT) scan excludes chronic otitis media.

Investigations
Inspection of the ear using a microscope is essential for diagnosis and treatment.
Pneumatic otoscopy and tympanometry -to confirm that the middle ear is normal and no perforation is present.
Pure-tone audiometry - to exclude a conductive hearing impairment due to chronic otitis media.
Culture for bacteria as well as for fungi is important in detecting the pathogens if conservative treatment with ear drops fails.
Gram-negative bacteria (Pseudomonas aeruginosa, Proteus species and Staphylococcus aureus) and Candida albicans are most commonly Cultured.
The bacterial culture does not differ from specimens found in external otitis and chronic otitis media.
HRCT scan can help exclude chronic otitis media.
biopsy for histological examination should be carried out to exclude carcinoma. If the granulations do not resolve with treatment,

OUTCOMES, NATURAL HISTORY AND
COMPLICATIONS
Granular myringitis has a chronic course and
granulations may continue to grow slowly for years;
however, healing may happen spontaneously.
The inflammation in the epithelial layer and lamina
propria of the tympanic membrane sometimes leads
to replacement with proliferating granulation tissue,
fibrosis and an atresia forming from the medial part
of the ear canal.
When the fibrosis and atresia has extended laterally,
the atresia ceases to grow.

MANAGEMENT OPTIONS

Benign necrotizing otitis
externa
Idiopathic necrosis of a localized area of bone of the tympanic ring, with secondary inflammation of the overlying soft tissue and skin. There are a number of synonyms for the condition: benign necrotizing otitis externa; benign necrotizing osteitis of the external auditorymeatus
canal; benign osteonecrosis of the external auditory meatus; aseptic necrosis of the external auditory meatus; idiopathic tympanic bone necrosis; necrosis and sequestration of the tympanic bone; necrosis and sequestration of the tympanic part of the
temporal bone; focal or circumscribed osteonecrosis of the external auditory

PATHOLOGY
The pathology is nonspecific.
The characteristic necrotic sequestrum of bone appears to
involve the superficial cortical layer primarily or
exclusively.
Histology of the bone reveals dead lamellar bone with
inflammatory cells filling the marrow spaces.
Usually there are very limited and mild inflammatory
changes of the adjacent skin and soft tissue
(subcutaneous tissue) of the external auditory meatus.
Apart from the normal skin flora a wide range of bacteria
may be cultured, with Staphylococcus aureus being the
most frequent isolate.

AETIOLOGY
The cause of this condition is unknown.
Suggested etiologies include-
vascular insufficiency because of its relatively poor
blood supply
The micro angiopathy of diabetes
Small arterial emboli have been suggested.
Repeated local trauma is a popular theory, for
example ear bud abuse, picking of the ear or the
use of hearing aids.
Aassociation with respiratory tract inflammatory
conditions

DIAGNOSISHistory
The symptoms are characteristic of mild local inflammation with perhaps pruritis, otorrhea or otalgia.
Exclude underlying conditions such as previous radiotherapy, diabetes mellitus or systemic disease with depression of the immune system.
There should also not be persistent deep boring otalgia, suggestive of malignant otitisexterna.
Examination
The condition is diagnosed clinically by the characteristic positive findings of a small area of deficient skin and soft tissue in the external auditory meatus revealing a segment of necrotic superficial bone.
The condition is usually unilateral.

Clinical examination should exclude the
characteristic granuloma and evidence of deep
osteitis of the temporal bone, such as cranial nerve
palsies, found in malignant otitis externa.
There should be no evidence of an exophytic
tumour and no obstructive collection of keratin
debris expanding the canal as found in keratosis
obturans.
The bony necrosis is usually limited

Diffrential diagnosis (a) Normal external auditory
canal. (b) Benign necrotizing otitis
externa. There is deficient area of skin, and bony sequestrum.
(c) Canal cholesteatoma. A sac of canal skin invades bone.
(d) Keratosis obturans. The bony canal is 'ballooned' out.
Of these, the condition most similar to benign necrotizing otitis externa is canal cholesteatoma, the only real difference being the absence of a lining of

Investigations
These are seldom indicated.
If gross infection is present a pus swab may be taken. Should Pseudomonas be cultured, the diagnosis should be queried in favour of malignant otitis externa,
Computed tomography may be indicated in order to identify the extent of bone necrosis.
If prominent inflammatory or granulation tissue coexists, chronic 'granulomatous' conditions including syphilis and tuberculosis should be excluded.
Exophytic lesions in the ear canal may require brush cytology and biopsy to exclude neoplastic conditions.
Audiometry should be normal unless debris in the external canal causes a mild conductive hearing impairment.

OUTCOMES. INCLUDING NATURAL
HISTORY
AND COMPLICATIONS
Separation of the sequestrum, followed by epithial
growth to cover the bony defect, as encouraged by
conservative management, is the most likely
outcome.
Canal cholesteatoma might be a consequence of
benign necrotizing otitis externa.
Once there is an area of necrotic bone, squamous
epithelium might grow from the ulcer margins, under
the sequestrum, in an attempt to demarcate the
sequestrum.

MANAGEMENT OPTIONS
Traditional conservative management consists of removing the bony sequestrum once it separates spontaneously with local toilet and local treatment to control any infection.
An oral antibiotic may be used.
A more aggressive surgical approach has been advocated, with early surgical removal of them sequestrum down to healthy bone.
Adjunctive hyperbaric oxygen may be considered when there is progression despite intensive local and systemic treatment and when there is necrosis beyond the tympanic plate.

Malignant otitis externaDEFINITION
Malignant otitis externa is an aggressive and potentially life-threatening infection of the soft tissues of the external ear and surrounding structures, quickly spreading to involve the periostium and bone of the skull base.
NOMENCLATURE
Also called 'skull base osteomyelitis' and 'necrotizing external otitis'
It has been suggested that necrotizing external otitis should be used for aggressive soft
tissue infection in the absence of bony involvement
skull base osteomyelitis be used for the condition once bone infection is confirmed.
Malignant otitis externa is a misnomer as it is not a neoplasticprocess

STAGING
Stage
1 Clinical evidence of malignant otitis externa with infection of soft tissues
beyond the external auditory canal, but negative Tc-99 bone scan
2 Soft tissue infection beyond external auditory canal with positive Tc-99
bone scan
3 As above, but with cranial nerve paralysis
3a Single
3b Multiple
4 Meningitis, empyema, sinus thrombosis or brain abscess

PATHOLOGY
Malignant otitis externa is the end -stage of a severe
infection thatoriginates from the external auditory canal
and progresses through cellulitis, chondritis, periostitis,
osteitis and finally osteomyelitis.
Infection is thought to spread out of the cartilaginous
external auditory canal through the fissures of Santorini,
congenital defects in the floor of the external auditory
canal.
Malignant otitis externa mainly affects the Haversian
system of compact bone and involvement of the
pneumatized portion of the temporal bone is a late
finding.
The otic capsule is usually spared
Pseudomonas aeruginosa is the most common pathogen

Predisposing factors
Elderly diabetic (both type I and type II) patients
impaired host response to Pseudomonas
microangiopathy in diabetic tissues, exacerbated by the vasculitic
properties of Pseudomonas.
The cerumen in diabetic patients is also of a higher pH than that of
normal controls, which may reduce the bactericidal properties of their
cerumen.
Non-diabetics accounted for almost a third of one large series.
Children more commonly have a facial nerve palsy and involvement
of the middle ear.
Other causes of immunocompromise, especially conditions that affect
cell-mediated immunity (e.g. AIDS), can also predispose to malignant
otitis externa

DIAGNOSIS Malignant otitis externa is a clinical
diagnosis made on the basis of pain, exudate, granulations and oedema of the external auditory canal , often supported by a positive bone scan and/or the presence of microabscesses at surgery.
The combination of pain, granulations, otorrhea and resistance to local therapy for at least eight to ten days are highly sensitive for making a diagnosis of malignant otitis externa.
Diabetes or other immunocompromisedstate, Pseudomonas aeruginosa onculture, a positive bone scan and cranial nerve palsy are confirmatory factors that enhance the specificity of the diagnosis.
The erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels are nonspecific measures of inflammation that are significantly raised in untreated cases.
The ESR is often over 100 mm/hour.
Malignant otitis externa with granulations
of the floor of the right external auditory
canal

RADIOLOGY
Technetium (Tc-99m) radio nuclide bone scans will detect bony involvement
even before high-resolution computed tomography (CT) scans can
demonstrate bone destruction.
As the isotope is absorbed by osteoclasts and osteoblasts that continue
remodelling after the infection has resolved, the scan may remain positive for
up to nine months.
As such, Tc-99m is only useful for detecting initial bony involvement.
Gallium (Ga-67) is absorbed by leukocytes and is a more sensitive monitor of
infection.
The scan quickly returns to normal after the infection has resolved and as
such, is a good measure to ascertain when to terminate treatment.
In recent years, magnetic resonance imaging (MRI) has added much to the
management of this infection.
Increased signal in the soft tissues beneath the skull base as a result of
inflammation does much to establish the extent of the disease. In addition, it

MANAGEMENT OPTIONS
Aural toilet
Local toilet to the external auditory canal is essential to control the granulations and improve local pain control.
The use of topical antibiotics is controversial.
They are likely to alter the microbiological flora of the external auditory canal and prevent adequate culture and sensitivities at a future date
Systemic antibiotics
The treatment of choice for the management of malignant otitis externais systemic anti-Pseudomonas antibiotics.
The drug often needs to be given for at least six weeks and in advanced cases, several months.
These are often given initially, with transition to oral antibiotics once the CRP and ESR start to fall.
Hyperbaric oxygen

MANAGEMENT OPTIONS
Surgery
There is now widespread agreement that surgical
intervention for malignant otitis externa should be
reserved for a few selected cases and no longer has
the goal of removing all the infected tissue.
Surgery for the removal of sequestra, collections of
pus and debridement of necrotized and granulating
tissues can be beneficial,but should only be used if
the patient is deteriorating clinically and if definable
surgical goals can be easily achieved.

Keratosis obturans and primary auditory
canal
cholesteatoma
Keratotis obturans is the
accumulation of a large
plug of desquaminated
keratin in the external
auditory meatus, while
primary auditory canal
cholseteatoma is the
invasion of squamous
tissue from the ear into a
localized area of bony
erosion.
The keratoma has been removed from the
right ear with keratosis obturans and
shows expansion of the bony canal just
lateral to the tympanic membrane

Comparison of keratosis obturans and primary auditory canal cholesteatoma.
keratosis obturans primary auditory canal
cholesteatoma
Aetiology Abnormal epithelial migration. Abnormal bone leading to migration of epithelium into this bone
Clinical symptoms andfindings
Severe otalgiaConductive hearing lossYounger agesOccasionally bilateralAssociation with lung and sinus diseaseCan present with a plugged feeling
OtorrhoeaNormal hearingItchiness or painOlder populationsUsually unilateral
Pathology Keratin plug occluding canalTympanic membrane thickenedEar canal balloonedHyperaemia of canal skin sometimes with granulations
Keratin in random patternTympanic membrane normalLocalized osteitis/erosion of ear canal usuallyPosterioinferior Sequestration of bone
Treatment Removal of plugLocal treatments of granulationsBiopsyMay need continued cleanings
Surgically remove cholesteatoma and abnormal boneGraft with fasciaBiopsy
Differential diagnosis
Wax impaction with infectionNeoplastic disease
Necrotizing otitis externaBenign sequestrumNeoplastic disease

Otitis externa Otitis externa is a generalized condition of the skin of the external
auditory canal that is characterized by general oedema and erythema associated with itchy discomfort and usually an ear discharge.
Predisposing factors for otitis externaType Factor
Anatomical Narrow external auditory meatus
Obstruction of normal meatus
DermatologicaI Eczema, sebhorrhoeic dermatitis
Allergic Atopy, nonatopic allergy, exposure to
topical medications
Physiological Humid environment,
immunocompromisation
Traumatic Skin maceration (bathing), ear probing,
laceration, radiotherapy
Microbiological Active chronic otitis media, exposure to
P. Aeruginosa (50-65%) or fungi

PATHOLOGY
pre-inflammatory stage-protective lipid/acid
balance (normal pH 4-5) of the ear is lost
acute inflammatory stage-progressively thickening
exudate, further oedema, obliteration of the lumen
and increasing pain.
chronic inflammatory-thickening of the external
canal skin and fibrous canal stenosis

DIAGNOSIS
clinical diagnosis based on
the following symptoms
and signs: pain, itch,
oedema and erythema of
the external auditory
canal with purulent
otorrhoea and debris in
the meatus
Debris and inflammation in the left external
auditory meatus.
After removal of debris, the swollen
oedematous canal skin of otitis externa can be seen

MANAGEMENT OPTIONS
Aural toilet-most effective single treatment for otitis
externa
Topical medication-
Steroid-antibiotic medication in the form of drops or
sprays
Glycerol and ichthammol (90:10 percent) aural wick (dehydrating and antiinflammatory properties and antibacterial activity)
Systemic antibiotics
Prevention of recurrence-
avoidance of water penetration into the ear (Cotton wool with
petroleum jelly)

Otomycosis
Otomycosis accounts for approximately 10
percent of all cases.
More common in hot, humid climates
Often secondary to prolonged treatment with
topical antibiotics.
Diabetes and immunocompromised states also
predispose to the condition.

Otomycosis with Aspergillus niger.
•Aspergillus accounts for 80-90
percent of cases
•Candida being responsible for the
remaining 10-20 percent.
CLINICAL FINDINGS
•The most common finding is black,
grey, green, yellow or white discharge
with debris that is often said to
resemble wet newspaper.
•Sometimes debris is seen with visible
fungal hyphae

MANAGEMENT
Treatment is aural toilet and removal of the debris
and topical antifungal drops,
In cases of resistant otomycosis, it is essential to
exclude fungal infection elsewhere, including
athelete's foot.
The 'foot and ear’ dermatophytid reaction can occur
from a fungal infection in a remote location.
Immunotherapy with dermatophyte Trichophyton ,
Oidiomycetes and Epidermophyton (TOE) extracts
and dust mite, is the treatment of choice.

Exostoses and Osteoma
External auditory exostoses and osteomas are
benign clinical entities characterized by
hyperplastic growth of bone in the osseous EAC.
Both types of lesions are most commonly noted
incidentally in asymptomatic patients.
However,as EAC obstruction worsens, symptoms
of chronic debris trapping, recurrent otitis externa,
and hearing loss develop.

Exostoses Osteomas
Bilateral & multiple
Non-neoplastic bony outgrowth
Broadly based protrusions originating from the anterior and posterior canal walls
Lacks fibrovascularchannels
EAC obstruction seen.
Associated with cold water exposure
More often unilateral,
Benign slow growing tumor
Pedunculated growth located at suture lines
Fibrovascular channels are present
lesser degrees of EAC obstruction.
Etiology is unknown

Multiple exostosis osteoma

DIAGNOSIS
characteristic otoscopic appearances of multiple and usually bilateral sessile, hemispherical, bony swellings arising deep in the external auditory canal, adjacent to the tympanic membrane.
In the presence of a tight stenosis of the deep ear canal, a high resolution computed tomography (CT) scan will help differentiate large exostoses from other causes of stenosis, such as chronic otitis externa.
A scan will also demonstrate complications, such as a canal cholesteatoma, developing medial to the exostoses.

MANAGEMENT
Treatment is usually unnecessary in small
exostoses,
but advice to avoid further cold water exposure
may be appropriate
Management of exostoses and osteomas
consists of periodic cerumen disimpaction and
débridement and treatment of infection as
necessary.
In cases refractory to medical treatment, a
meatoplasty operation may be necessary.

Foreign bodies in the ear
Type of foreign body Method of removal
Living insects First kill with oil
Irregular/graspable objects Remove with crocodile forceps
organic/vegetabIe Do not syringe
Button batteries Do not syringe
Round, hard, smooth,
non-graspable
Syringe/remove with wax hook/removal
under anaesthetic
•Consider the nature of the foreign body when choosing
management options

Inexpert or ill-advised
attempts at removal may
cause serious
complications such as canal
lacerations, tympanic
membrane perforations and
ossicular fractures or
dislocations.
Firmly impacted foreign
bodies medial to the
isthmus may warrant
removal in theatre and may
require surgical removal via

Herpes zoster oticusDEFINITION
Herpes zoster oticus is defined as a herpetic vesicular rash on the concha, external auditory canal or pinnawith a lower motor neurone palsy of the ipsilateralfacial nerve
PATHOLOGY
The disease is a reactivated varicella zoster infection from dormant viral particles resident in the geniculate ganglion of the facial nerve and the spiral and vestibular ganglia of the VIIIth nerve.
Diagnosis is clinical
hearing loss, tinnitus and/or vertigo

MANAGEMENT
Improved outcomes obtained if commenced on
acyclovir and prednisolone within three days of the
onset of symptoms.
Haemorrhagic vesicle in the right external
auditory canal in herpes zoster oticus

THANK YOU