Extent of resection in the treatment of gliomas Fred G. Barker II, M.D. Neurosurgical Grand Rounds...
83
Extent of resection Extent of resection in the treatment of gliomas in the treatment of gliomas Fred G. Barker II, M.D. Fred G. Barker II, M.D. Neurosurgical Grand Rounds Neurosurgical Grand Rounds Massachusetts General Hospital Massachusetts General Hospital February 28, 2008 February 28, 2008
-
Upload
vernon-porter -
Category
Documents
-
view
215 -
download
1
Transcript of Extent of resection in the treatment of gliomas Fred G. Barker II, M.D. Neurosurgical Grand Rounds...

Extent of resection Extent of resection in the treatment of gliomasin the treatment of gliomas
Fred G. Barker II, M.D. Fred G. Barker II, M.D. Neurosurgical Grand Rounds Neurosurgical Grand Rounds
Massachusetts General HospitalMassachusetts General Hospital
February 28, 2008February 28, 2008

EOR questionsEOR questions
GTR vs biopsy?GTR vs biopsy?
Debulking vs biopsy?Debulking vs biopsy?
GTR vs. near-GTR?GTR vs. near-GTR?
GTR vs. GTR plus margin of GTR vs. GTR plus margin of “normal” tissue (lobectomy)?“normal” tissue (lobectomy)?

Resection of malignant gliomaResection of malignant glioma
Cochrane Review, Metcalfe & Grant, 2001Cochrane Review, Metcalfe & Grant, 2001
““The electronic database search yielded The electronic database search yielded 2100 citations. Of these, 2 articles 2100 citations. Of these, 2 articles were identified for possible inclusion, were identified for possible inclusion, however both were excluded. The however both were excluded. The hand search and personal hand search and personal communication were similarly communication were similarly unproductive. unproductive. No studies were No studies were included in the review and no data included in the review and no data were synthesized.were synthesized.””

Goals of surgery for malignant gliomasGoals of surgery for malignant gliomas
1. Providing diagnosis1. Providing diagnosis
2. Relieving symptomatic mass 2. Relieving symptomatic mass effecteffect
3. “Setting up” postoperative 3. “Setting up” postoperative externally delivered therapiesexternally delivered therapies
4. Prolonging survival through 4. Prolonging survival through cytoreductioncytoreduction
5. Applying locally-delivered therapies5. Applying locally-delivered therapies

1. Providing a diagnosis1. Providing a diagnosis
Main differentials: stroke – DWI, vascular distribution; “infection” (i.e. encephalitis) – susceptibility, location; demyelinating disease – incomplete ring sign
T1 with gad FLAIR T1 with gad post 6 wk

Providing a diagnosisProviding a diagnosis
Nonenhancing tumors are not always Nonenhancing tumors are not always low-gradelow-grade
Chance of anaplasia increases in older patients (50% by mid-40’s)
Barker et al. (UCSF), Cancer 1997

Providing a diagnosisProviding a diagnosis
Gliomas are notoriously Gliomas are notoriously heterogeneousheterogeneous
More extensive resections more More extensive resections more frequently provide higher grade frequently provide higher grade diagnosisdiagnosis
Glantz et al., Neurology, 1991Glantz et al., Neurology, 1991
higher grade diagnosis more likely higher grade diagnosis more likely as extent of resection increasedas extent of resection increased

Stereotactic bx: grade 2; resection grade 3Stereotactic bx: grade 2; resection grade 3
Providing a diagnosisProviding a diagnosis

Providing a diagnosisProviding a diagnosis
Perry et al., Cancer 1999Perry et al., Cancer 1999identification of oligo component in identification of oligo component in
grade 3 tumors was more likely as grade 3 tumors was more likely as extent of resection increased extent of resection increased (p = 0.01)(p = 0.01)
% containing oligo components:% containing oligo components:
BxBx 3%3%
STRSTR 29%29%
GTRGTR 43%43%

Providing a diagnosisProviding a diagnosis
Aghi et al., unpublished MGH data (grade 2)Aghi et al., unpublished MGH data (grade 2)
% containing oligo components:% containing oligo components:
BxBx 46% 46% ((more specimens -> more oligo)more specimens -> more oligo)
GTRGTR 89% 89% p < 0.001p < 0.001
Carter et al., unpublished SEER data (grade 2)Carter et al., unpublished SEER data (grade 2)
% containing oligo components:% containing oligo components:
BxBx 32%32%
ResectionResection 62%62% p < 0.001p < 0.001

Year of diagnosis
Pro
babi
lity
1985 1990 1995 2000
0.0
0.2
0.4
0.6
0.8
1.0100%100%
AstroAstro
Year of diagnosisYear of diagnosis
19951995 20002000
Pro
bab
ilit
yP
rob
abil
ity
0%0%
20%20%
40%40%
60%60%
1990199019851985
OligoOligo
80%80%
OligoastroOligoastro
p < 0.001p < 0.001
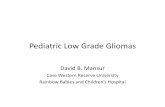
SEER data;Carter BS et al unpublished
Probability of oligo-containing histology Probability of oligo-containing histology has increased significantly with timehas increased significantly with time

Year of diagnosis
Pro
babi
lity
1985 1990 1995 2000
0.0
0.1
0.2
0.3
0.4
0.0
0.2
0.4
Probability of oligo-containing histologyProbability of oligo-containing histology
vs. literature on chemo for oligosvs. literature on chemo for oligos 40%40%
PubMed # articles PubMed # articles on chemo for oligoson chemo for oligos
Year of diagnosisYear of diagnosis
19951995 20002000
Pro
bab
ilit
y o
f o
lig
o d
iag
no
sis
Pro
bab
ilit
y o
f o
lig
o d
iag
no
sis
0%0%
10%10%
20%20%
30%30%
1990199019851985
SEER % oligosSEER % oligos
2020
1010
0 0
Nu
mb
er of articles o
n ch
emo
for o
ligo
sN
um
ber o
f articles on
chem
o fo
r olig
os
SEER, PubMed data;Carter BS et al unpublished

Providing a diagnosisProviding a diagnosis
Jackson et al., Neuro-Oncol 2001Jackson et al., Neuro-Oncol 2001
81 pts referred to MD Anderson after 81 pts referred to MD Anderson after stereo bx elsewhere who were accepted stereo bx elsewhere who were accepted for resectionfor resection
>95% resection in 57% of patients>95% resection in 57% of patients
38% had different pathology even after 38% had different pathology even after central review of outside slides; 26% central review of outside slides; 26% would affect treatmentwould affect treatment
Mortality/major morbidity in 17%Mortality/major morbidity in 17%

Providing a diagnosisProviding a diagnosis
MR spectroscopy can MR spectroscopy can assist in choosing a assist in choosing a biopsy targetbiopsy target

2. Relieve mass effect2. Relieve mass effect
Obvious and frequent success in Obvious and frequent success in most neurosurgeons’ experience most neurosurgeons’ experience in relieving neurological in relieving neurological symptoms from mass effectsymptoms from mass effect
Possible effect in increasing KPS in Possible effect in increasing KPS in malignant gliomamalignant glioma
Low grade glioma: relieving Low grade glioma: relieving medically intractable seizuresmedically intractable seizures

Relieve mass effectRelieve mass effect
Ciric et al., Neurosurgery 1987Ciric et al., Neurosurgery 1987neurologic condition at dischargeneurologic condition at discharge
EOREOR ImproveImprove SameSame WorseWorse
PartialPartial 0%0% 60%60% 40%40%
Near GTNear GT 30%30% 70%70%0%0%
GTGT 41%41% 55%55%4%4%

Relieve mass effectRelieve mass effect
Sawaya et al., Neurosurgery 1998Sawaya et al., Neurosurgery 199830% of all patients had improved KPS 30% of all patients had improved KPS
after resectionafter resection
8% had decreased KPS8% had decreased KPS
% “major neurologic complications”:% “major neurologic complications”:
PartialPartial 12%12%
SubtotalSubtotal 15%15%
TotalTotal 7%7%

Relieve mass effectRelieve mass effect
Fadul et al., Neurology 1988Fadul et al., Neurology 1988Neurologic deterioration Neurologic deterioration
(1 week postop)(1 week postop)
BxBx 29%29%
PartialPartial 39%39%
SubtotalSubtotal 30%30%
TotalTotal 20%20%
most hemorrhages and herniations most hemorrhages and herniations occurred after bx or partial resectionoccurred after bx or partial resection

3. “Setting up” postoperative therapies3. “Setting up” postoperative therapies
Is response to postoperative Is response to postoperative adjuvant radiation in newly-adjuvant radiation in newly-diagnosed glioblastoma improved diagnosed glioblastoma improved by prior resection?by prior resection?
Neurosurgery 49:1288, 2001

Response to radiation after surgeryResponse to radiation after surgery
301 GM pts treated using two 301 GM pts treated using two prospective UCSF clinical prospective UCSF clinical protocolsprotocols
age, KPS, extent of resection, age, KPS, extent of resection, radiation response recorded radiation response recorded prospectivelyprospectively
radiation response assessed by radiation response assessed by imaging criteria (postop image imaging criteria (postop image compared with post-XRT image)compared with post-XRT image)

ResultsResults
More extensive surgical resection predicted better More extensive surgical resection predicted better imaging-assessed response to postoperative imaging-assessed response to postoperative adjuvant radiation in both univariate and adjuvant radiation in both univariate and multivariate analyses (adjusted for age, KPS)multivariate analyses (adjusted for age, KPS)

““Setting up” postoperative therapiesSetting up” postoperative therapies
Resection and TMZ – EORTC 26981 (Stupp)Resection and TMZ – EORTC 26981 (Stupp)
2-year survival2-year survival median survivalmedian survival
+TMZ -TMZ+TMZ -TMZ +TMZ -TMZ +TMZ -TMZ
GTRGTR 37%37% 14% 14% 18m18m 14m 14m
STRSTR 23%23% 9% 9% 14m14m 12m 12m
BxBx 10%10% 5% 5% 9m 9m 8m 8m
van den Bent et al., Eur J Cancer 2005 [abstr]

Subset Analysis – Subset Analysis – Overall SurvivalOverall Survival

““Setting up” postoperative therapiesSetting up” postoperative therapies
Keles et al. J Neurosurg 2004 Keles et al. J Neurosurg 2004
119 pts with recurrent GM119 pts with recurrent GM
Reoperation -> TMZReoperation -> TMZ
Volume of disease at start of Volume of disease at start of chemotherapy was a significant chemotherapy was a significant predictor of time to progressionpredictor of time to progression and and survival (progression risk doubled survival (progression risk doubled for 10-15cc residual mass c/w GTR, for 10-15cc residual mass c/w GTR, quadrupled for >15 cc)quadrupled for >15 cc)

4. Prolong survival4. Prolong survival
Cushing believed that resection Cushing believed that resection extended survival in malignant extended survival in malignant gliomas but recognized shorter gliomas but recognized shorter and shorter intervals between and shorter intervals between operation as the disease operation as the disease progressed – “ideally all should be progressed – “ideally all should be operative mortalities”operative mortalities”
McKenzie first to replace bone flap McKenzie first to replace bone flap after resection to after resection to limitlimit prognosis, prognosis, but generally benefit of resection but generally benefit of resection was not questionedwas not questioned

Review ArticleReview Article

4. Prolong survival4. Prolong survival
Nazzaro and Neuwelt, 1990Nazzaro and Neuwelt, 1990
Reviewed neurosurgical literature 1940 Reviewed neurosurgical literature 1940 - 1990 (184 refs)- 1990 (184 refs)
““This analysis shows that there is little This analysis shows that there is little justification for dogmatic statements justification for dogmatic statements concerning the relationship between concerning the relationship between increasing patient survival times and increasing patient survival times and aggressive surgical management …”aggressive surgical management …”

Nazzaro and Neuwelt, 1990Nazzaro and Neuwelt, 1990
Failure to adjust for other prognostic Failure to adjust for other prognostic factors such as agefactors such as age
Failure to adjust for difference in postop Failure to adjust for difference in postop treatments* treatments*
Failure to use “any form of statistical Failure to use “any form of statistical analysis”analysis”
All studies had retrospective designAll studies had retrospective design
Failure to adjust for resectabilityFailure to adjust for resectability
*logical fallacy – resection does influence chance *logical fallacy – resection does influence chance of tolerating XRT as well as chance of of tolerating XRT as well as chance of reoperationreoperation

Prolong survivalProlong survival
Considering the more than 30 years Considering the more than 30 years of experience and apparent failure, of experience and apparent failure, does it not seem that the does it not seem that the ostensible myth of the benefit of ostensible myth of the benefit of cytoreduction for the “isolated cytoreduction for the “isolated sake of cytoreduction” needs to sake of cytoreduction” needs to placed on the intellectual scrap placed on the intellectual scrap heap? heap?
-- Michael L.J. -- Michael L.J. ApuzzoApuzzo

Prolong survivalProlong survival
Many multivariate analyses of Many multivariate analyses of survival after resection of GM survival after resection of GM (nonrandomized) now provide (nonrandomized) now provide evidence that extent of resection evidence that extent of resection is an independent prognostic is an independent prognostic factor for survival (independent of factor for survival (independent of age and KPS)age and KPS)

Prolong survivalProlong survival
Laws et al., JNS 2003 (GO project)Laws et al., JNS 2003 (GO project)
788 patients (1997-2001)788 patients (1997-2001)
Resection was favorable prognostic Resection was favorable prognostic factor (compared to biopsy) after factor (compared to biopsy) after correction for age, correction for age, KPSKPS, and after , and after omission of patients with omission of patients with multifocal diseasemultifocal disease

GTR
STR
Bx
Years after diagnosis
Pro
po
rtio
n s
urv
ivin
g
0.0 0.5 1.0 1.5 2.0
0.0
0.2
0.4
0.6
0.8
1.0
p < 0.001
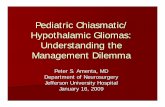
Barker et al. (UCSF), JNS 1996
Survival in GMSurvival in GMstratified bystratified byextent of resectionextent of resection(nonrandomized)(nonrandomized)

Extent of MST 1-yr 2-yr 5-yrresection (months)
Gross total 17 72% 31% 12% Subtotal 11 47% 15% 2% Biopsy 7 23% 2% 0%
Barker et al. (UCSF), JNS 1996
Survival in GM stratified by extent of resection(nonrandomized)

Survival after biopsy or resection of Survival after biopsy or resection of supratentorial lobar glioblastoma: supratentorial lobar glioblastoma:
a population-based studya population-based study
Manish K. Aghi, M.D., Ph.D., William T. Curry Jr., M.D., Manish K. Aghi, M.D., Ph.D., William T. Curry Jr., M.D., Bob S. Carter, M.D., Ph.D. and Fred G. Barker II, M.D. Bob S. Carter, M.D., Ph.D. and Fred G. Barker II, M.D.
Neurosurgical ServiceNeurosurgical ServiceMassachusetts General HospitalMassachusetts General Hospital
Harvard Medical SchoolHarvard Medical School

ResultsResults
11,134 glioblastoma patients diagnosed 1988 to 200111,134 glioblastoma patients diagnosed 1988 to 2001
11,108 intracranial tumors11,108 intracranial tumors
7,423 supratentorial lobar tumors7,423 supratentorial lobar tumors
60216021 tumors did not cross the midline or tentorial notch, tumors did not cross the midline or tentorial notch, had not spread outside brain, through CSF or to spine, had nohad not spread outside brain, through CSF or to spine, had no
contraindications to surgery, and had a surgical procedure specifiedcontraindications to surgery, and had a surgical procedure specified
(size known for 3520 tumors)(size known for 3520 tumors)

ResultsResults
Factors predicting biopsy over resection:Factors predicting biopsy over resection:
• Older ageOlder age (odds ratio 1.38 per decade) (odds ratio 1.38 per decade)
• Smaller tumor sizeSmaller tumor size (odds ratio 0.84 per cm) (odds ratio 0.84 per cm)
• Tumor locationTumor location (parietal – highest chance of (parietal – highest chance of biopsy, temporal lowest)biopsy, temporal lowest)
• HistologyHistology (glioblastoma – highest chance of (glioblastoma – highest chance of biopsy, giant cell glioblastoma lowest)biopsy, giant cell glioblastoma lowest)
• Unmarried statusUnmarried status
• SEER registrySEER registry

20
40
60
80
Age20
40
60
80
Tumor size (mm)
00.
10.
20.
30.
40.
5P
rob(
bx)
Pro
b (
bio
psy
)P
rob
(b
iop
sy)
Tumor size (mm)
Tumor size (mm) AgeAge
Probability of biopsy rather than resection:Probability of biopsy rather than resection:Relation to age and tumor sizeRelation to age and tumor size

Results: survivalResults: survival
0.0 0.5 1.0 1.5 2.0 2.5 3.0
Years after diagnosis
0.0
0.2
0.4
0.6
0.8
1.0
Su
rviv
alRESECTION
BIOPSY
Median survival – 12 months for resectionMedian survival – 12 months for resection7 months for biopsy7 months for biopsy
All pts had postop XRT

ResultsResults
Biopsy rates vary by SEER registry:Biopsy rates vary by SEER registry:
27%27%
4%4%
23%23%
13%13%
15%15%
13%13%
12%12%
15%15%
15%15%
22%22%
22%22%

Tumor size (mm)
Pro
babi
lity
of ra
diat
ion
0 20 40 60 80
0.60
0.65
0.70
0.75
0.80
0.85
0.90
ResectionResection
Tumor size (mm)Tumor size (mm)
4040 6060 8080
Pro
bab
ilit
y o
f p
ost
op
XR
TP
rob
abil
ity
of
po
sto
p X
RT
60%60%
65%65%
70%70%
90%90%
80%80%
75%75%
202000
BiopsyBiopsy
85%85%
Probability of XRT vs. tumor sizeProbability of XRT vs. tumor sizefor biopsied & resected patientsfor biopsied & resected patients

Cancer 2006;106:1358
Survival Rates and PatternsSurvival Rates and Patterns

Prolong survival - subgroupsProlong survival - subgroups
Do all glioblastoma patients benefit Do all glioblastoma patients benefit equally from extensive resection?equally from extensive resection?
Potentially important subgroups:Potentially important subgroups:
patients with mass effect patients with mass effect
younger patientsyounger patients

Mass effect and GM resectionMass effect and GM resection
Kreth et al., Cancer 1999Kreth et al., Cancer 1999
Stereo bx+XRT c/w resection+XRTStereo bx+XRT c/w resection+XRT
225 patients, supratentorial GM225 patients, supratentorial GM
Tumor resection effective only in Tumor resection effective only in group with midline shift (P < 0.01)group with midline shift (P < 0.01)

GraphGraph

GTR
STR
Bx
Years after diagnosis
Pro
po
rtio
n s
urv
ivin
g
Survival in GMSurvival in GMstratified bystratified by
extent of resectionextent of resection
0.5 1.0 1.5 2.00.0
0.0
0.2
0.4
0.6
0.8
1.0
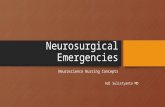
Age 16 to 39N = 47
p = 0.01
Age and GM resectionAge and GM resection

GTR
STR
Bx
Years after diagnosis
Pro
po
rtio
n s
urv
ivin
g
0.5 1.0 1.5 2.00.0
0.0
0.2
0.4
0.6
0.8
1.0
Age 40 to 49N = 58
p = 0.01
Survival in GMSurvival in GMstratified bystratified byextent of resectionextent of resection

GTR
STRBx
Years after diagnosis
Pro
po
rtio
n s
urv
ivin
g
0.5 1.0 1.5 2.0
0.0
0.0
0.2
0.4
0.6
0.8
1.0
Age 50 to 64N = 114p = 0.12
Survival in GMSurvival in GMstratified bystratified byextent of resectionextent of resection

GTRSTR
Bx
Years after diagnosis
Pro
po
rtio
n s
urv
ivin
g
0.5 1.0 1.5 2.00.0
0.0
0.2
0.4
0.6
0.8
1.0
Age 65 to 79N = 80
p = 0.04
Survival in GMSurvival in GMstratified bystratified byextent of resectionextent of resection

Survival after GM resection: Survival after GM resection: subgroupssubgroups
SubgroupSubgroup Hazard ratio Hazard ratio biopsy vs. resectionbiopsy vs. resection
Age Age ≤ 40≤ 40 1.971.97
Age > 40Age > 40 1.661.66
Size < 3 cmSize < 3 cm 1.541.54
Size 3-5 cmSize 3-5 cm 1.721.72
Size > 5 cmSize > 5 cm 1.731.73
Source: Aghi et al, unpub (SEER)

Grade II astro / oligo / oligoastroGrade II astro / oligo / oligoastroSurgerySurgery
Total N = 599

Nonrandomized trialsNonrandomized trials
Most trials in neurosurgery are not Most trials in neurosurgery are not randomizedrandomized
Some topics can only be studied using Some topics can only be studied using nonrandomized methods (such as nonrandomized methods (such as volume-outcome relationship)volume-outcome relationship)
Recent studies have shown that when Recent studies have shown that when nonrandomized trials use concurrent nonrandomized trials use concurrent controls eligible for the experimental controls eligible for the experimental treatment, results are often treatment, results are often reasonably similar to randomized trial reasonably similar to randomized trial results results

Solid: nonrandomized
GraphGraph

RCT of resection for gliomaRCT of resection for glioma
Design of RCT for resection in gliomaDesign of RCT for resection in glioma
Enrollment and randomization based Enrollment and randomization based on imaging diagnosis (sometimes bx on imaging diagnosis (sometimes bx is required in non-resected group)is required in non-resected group)
All tumors must be considered All tumors must be considered resectableresectable
Postop deaths and severe morbidities Postop deaths and severe morbidities should not be excluded (i.e. no loss should not be excluded (i.e. no loss to followup based on results of to followup based on results of surgery)surgery)

Loss to followup Loss to followup
Of 28 malignant glioma trials Of 28 malignant glioma trials included in NS review paper, 24 included in NS review paper, 24 were either cooperative group were either cooperative group trials (with explicit performance trials (with explicit performance status criteria) or single-center status criteria) or single-center trials (often with frank exclusion of trials (often with frank exclusion of poor results)poor results)
15/24 showed benefit of EOR – 15/24 showed benefit of EOR – compared with 1 of 4 population compared with 1 of 4 population based studiesbased studies

Better Study Design #1 - RCTBetter Study Design #1 - RCT
Only RCT of resection for malignant Only RCT of resection for malignant glioma: glioma: Vuorinen et al, Acta Nchir 2003Vuorinen et al, Acta Nchir 2003
Age > 65, KPS > 60 Age > 65, KPS > 60
30 pts randomized; 10/14 had resection 30 pts randomized; 10/14 had resection (refusal, hematoma, lymphoma, infarct), (refusal, hematoma, lymphoma, infarct), 13/16 had biopsy (met x 2, hematoma)13/16 had biopsy (met x 2, hematoma)
9/10 resected pts, 10/13 biopsied pts 9/10 resected pts, 10/13 biopsied pts started XRT (remainder: poor clinical started XRT (remainder: poor clinical condition)condition)

Malignant glioma resection - survivalMalignant glioma resection - survival
Vuorinen, Acta Neurochir 2003
P = 0.035Hazard ratio 2.7Favors resection

Malignant glioma resection – time to failureMalignant glioma resection – time to failure
Vuorinen, Acta Neurochir 2003
P = 0.057Favors resection

RCTRCT
RCT of bx vs resection for elderly RCT of bx vs resection for elderly with presumed malignant glioma with presumed malignant glioma was supposed to open in France was supposed to open in France in 2007in 2007

Adjustment for resectabilityAdjustment for resectability
While many nonrandomized studies While many nonrandomized studies of EOR in glioma have included of EOR in glioma have included “adjustment for location”, none “adjustment for location”, none have included adjustment for have included adjustment for resectabilityresectability
Barker et al., JNS 96

ResectabilityResectability
In fact, resectability is a complex concept In fact, resectability is a complex concept that is a frequent subject of disagreement that is a frequent subject of disagreement between surgeonsbetween surgeons
Factors influencing rates of resection include Factors influencing rates of resection include pt-related (age, KPS, marital status); tumor-pt-related (age, KPS, marital status); tumor-related (size, location, fuzziness of borders) related (size, location, fuzziness of borders) and provider-related (specialist status, and provider-related (specialist status, volume of practice, training and experience, volume of practice, training and experience, economic and professional incentives)economic and professional incentives)
Resectable and nonresectable tumors may Resectable and nonresectable tumors may well have different molecular pathologywell have different molecular pathology

PublicationPublication

Resectability in gliomaResectability in glioma
Two published attempts at defining a Two published attempts at defining a scale of resectability in gliomasscale of resectability in gliomas
Vorster and Barnett (Nsurg Focus 98)Vorster and Barnett (Nsurg Focus 98)
Eloquent / noneloquentEloquent / noneloquent
Eloquent areas: sensorimotor, Eloquent areas: sensorimotor, visual, language cortices, internal visual, language cortices, internal capsule, basal gangliacapsule, basal ganglia

Resectability in gliomaResectability in glioma
Sawaya Nsurg 98Sawaya Nsurg 98

Resectability in gliomaResectability in glioma

Better study design – # 2Better study design – # 2
Nonrandomized study in which all Nonrandomized study in which all tumors were eligible for resection, tumors were eligible for resection, but heterogeneity of surgeons’ but heterogeneity of surgeons’ practices pseudorandomizes practices pseudorandomizes patients to bx/resection (or patients to bx/resection (or STR/GTR)STR/GTR)
Propensity score for balancing (as Propensity score for balancing (as in Barker Nsurg 98)in Barker Nsurg 98)

An example – Shaw et al.An example – Shaw et al.
RTOG 9802 – surgeon-determined RTOG 9802 – surgeon-determined GTR of LGG, then observed GTR of LGG, then observed (single-arm phase II trial)(single-arm phase II trial)
111 pts entered 1998-2002111 pts entered 1998-2002

RTOG 9802RTOG 9802
PFSPFS
< 1 cm residual (59%)< 1 cm residual (59%) 74%74%
1 – 2 cm residual (32%)1 – 2 cm residual (32%) 32%32%
> 2 cm residual (9%)> 2 cm residual (9%) 11%11%
82% relapsed <2cm from resection 82% relapsed <2cm from resection cavity; 2% distantcavity; 2% distant
Shaw et al., JNS in revision 2008

Better Study Design #3Better Study Design #3
While it may be difficult to randomize pts While it may be difficult to randomize pts between biopsy and resection, at least between biopsy and resection, at least two RCTs of surgical adjuncts to improve two RCTs of surgical adjuncts to improve EOR have been completed and reportedEOR have been completed and reported
For an effective adjunct (with no For an effective adjunct (with no indempendent treatment effect) this indempendent treatment effect) this would in effect randomize between would in effect randomize between different EORsdifferent EORs
Neuronavigation trial was negative (Willems Neuronavigation trial was negative (Willems JNS 104:360, 2006)JNS 104:360, 2006)

Prolonging survival Prolonging survival
Stummer et al. RCT of fluorescence-guided Stummer et al. RCT of fluorescence-guided GM resectionGM resection
Pts for resection of presumed GM Pts for resection of presumed GM randomized to optimal white-light randomized to optimal white-light resection or fluorescence-guided (5-ALA)resection or fluorescence-guided (5-ALA)
5-ALA group had 65% GTR c/w 36% for WL 5-ALA group had 65% GTR c/w 36% for WL groupgroup
6-mo PFS doubled in 5-ALA group (41% vs. 6-mo PFS doubled in 5-ALA group (41% vs. 21%)21%)
Stummer et al., Lancet Oncol 2006

Malignant glioma resection - PFSMalignant glioma resection - PFS
Stummer et al., Lancet Oncol 2006
65% GTR 5-ALAvs 36% GTR WL

Prolonging survival Prolonging survival
Could an unexpected photodynamic Could an unexpected photodynamic treatment effect of 5-ALA at low light treatment effect of 5-ALA at low light intensity account for results?intensity account for results?
Unpublished subgroup analyses – no Unpublished subgroup analyses – no difference in survival between difference in survival between groups after GTR; minimal groups after GTR; minimal improvement in PFS in STR group improvement in PFS in STR group with 5-ALAwith 5-ALA
Suggests benefits are a direct result of Suggests benefits are a direct result of improved resectionimproved resection
Stummer et al., Lancet Oncol 2006

Balance against riskBalance against risk
Apples-oranges problemApples-oranges problem
Common coin – KPS as prognostic Common coin – KPS as prognostic factor for survivalfactor for survival
GTR/STR or STR/bx difference GTR/STR or STR/bx difference roughly worth ~10 to 30 KPS roughly worth ~10 to 30 KPS points points

TableTable

Age
Pro
babi
lity
30 40 50 60 70 80
0.0
0.1
0.2
0.3
0.4
0.5
Death + LTF + STFDeath + LTFDeath
UnivariateUnivariatePP < 0.001 < 0.001
AgeAge
3030 4040 5050 6060 7070 8080
Pro
bab
ilit
yP
rob
abil
ity
0.00.0
0.10.1
0.20.2
0.50.5
0.40.4
0.30.3
Barker et al., NeuroOnc 2005
Outcome vs. ageOutcome vs. ages/p resection of primary brain tumors/p resection of primary brain tumor

ConclusionsConclusions
Surgical resection is an independent prognostic Surgical resection is an independent prognostic factor for survival in GM and LGG in factor for survival in GM and LGG in nonrandomized trialsnonrandomized trials
Whether this would persist after adjustment for Whether this would persist after adjustment for resectability has been controversial; single resectability has been controversial; single RCT now available with confirmatory resultsRCT now available with confirmatory results
Burden of proof increasingly rests on nihilists; Burden of proof increasingly rests on nihilists; no likelihood of new LGG randomized trial no likelihood of new LGG randomized trial anytime soon, new trial in MG is possibly in anytime soon, new trial in MG is possibly in planning stagesplanning stages

LogoLogo

ReoperationReoperation
Who benefits from reoperation in Who benefits from reoperation in glioblastoma?glioblastoma?

Reoperation for GM: selection factorsReoperation for GM: selection factors
223 patients with documented failure before 223 patients with documented failure before death; multivariate logistic regression to death; multivariate logistic regression to predict patients who will undergo reoperationpredict patients who will undergo reoperation
ageage < 40 < 40 34%34%
p = 0.02p = 0.02 40-6040-60 23%23%
60+60+ 11% 11%
extent of initial surgeryextent of initial surgery GTR GTR 32%32%
p = 0.02p = 0.02 STRSTR 22%22%
BxBx 4%4%

Reoperation for GM: Reoperation for GM: relieving symptomsrelieving symptoms
KPS after second resection:KPS after second resection:
28% improved28% improved
49% stable49% stable
23% declined (by 10-30 points)23% declined (by 10-30 points)
more likely benefit when more likely benefit when recurrence was symptomaticrecurrence was symptomatic

Reoperation for GM: Reoperation for GM: comparison to unoperated patientscomparison to unoperated patients
Median survival after first failure (KPS known)Median survival after first failure (KPS known)
reoperated (36 pts)reoperated (36 pts) 41 wk41 wk
not reoperated (136 pts)not reoperated (136 pts) 23 wk23 wk
univariateunivariate hazard ratio 0.71hazard ratio 0.71 p = 0.036p = 0.036
CoxCox mvmv hazard ratio 0.66hazard ratio 0.66 p = 0.08p = 0.08after adj for age, KPS at failureafter adj for age, KPS at failure
extent of initial resection & interval until failure: NSextent of initial resection & interval until failure: NS

Survival after first relapseSurvival after first relapse
ReoperationReoperationNo reoperationNo reoperation

Reoperation for GM: survival benefitReoperation for GM: survival benefit
Cox simulation for “typical” patientCox simulation for “typical” patient
55 years old55 years old
KPS at recurrence of 80KPS at recurrence of 80
initial resection STR or GTRinitial resection STR or GTR
recurrence at/near original tumor siterecurrence at/near original tumor site
predicted difference in median survival between predicted difference in median survival between reoperated and nonreoperated groups:reoperated and nonreoperated groups: 8 weeks8 weeks
Barker et al. (UCSF), NS 1998

4. Prolong survival4. Prolong survival
Kowalczuk et al., Neurosurg 1997Kowalczuk et al., Neurosurg 1997
75 patients with malignant gliomas75 patients with malignant gliomas
significant: age, KPS, tumor grade, significant: age, KPS, tumor grade, complications within 30 days after complications within 30 days after surgery, XRT dose administeredsurgery, XRT dose administered
not significant: 17 other factors, not significant: 17 other factors, including extent of resection including extent of resection (volumetric analysis)(volumetric analysis)