
Expression of ALK protein, mRNA and fusion transcripts in anaplastic large cell lymphoma
6
Expression of ALK protein, mRNA and fusion transcripts in anaplastic large cell lymphoma Wentao Huang a , Xiaoqiu Li a , Xiaohong Yao b , Yongming Lu a , Baizhou Li a , Weiqi Sheng a , Hongfen Lu a , Aiping Jin a , Xiaoyan Zhou a, ⁎ a Department of Pathology, Cancer Hospital, Department of Oncology, Shanghai Medical Collage, Fudan University 270 Dongan Road, Shanghai 200032, P.R. China b Department of Pathology, Xinhua Hospital, Shanghai Jiao Tong University, Shanghai 200092, P.R. China abstract article info Article history: Received 7 August 2008 Available online 14 December 2008 Keywords: Anaplastic large cell lymphoma ALK Anaplastic lymphoma kinase Fusion transcript Immunohistochemistry Reverse transcription polymerase chain reaction Systemic anaplastic large cell lymphoma (ALCL) can be divided into two subgroups, anaplastic lymphoma kinase (ALK)-positive and ALK-negative, based on the expression of ALK protein. Expression of this protein is due to genetic alterations of ALK at 2p23. Overall, observations on ALK protein, ALK mRNA, ALK-associated genetic alterations and their relationships, to one another are not often reported in the literature. In this study, we investigated the expression of ALK protein, mRNA and fusion transcripts involving ALK and their relationships in ALCL and analyzed formalin-fixed, paraffin-embedded tissues. Forty-five human cases were analyzed with immunohistochemistry for the ALK protein and RT-PCR for ALK mRNA and seven kinds of ALK involved fusion transcripts. Our results showed that the expression of ALK protein, ALK mRNA and ALK fusion transcripts were significantly related to one another (P b 0.01). Consistent with the expression of ALK protein, patients presenting with ALK mRNA or ALK involved fusion transcripts were significantly younger than those lacking ALK gene alteration (P b 0.01). This study demonstrates expression of both ALK protein and ALK mRNA are positively correlated with expression of ALK-associated fusion transcripts. Combined detection of ALK protein, ALK mRNA and ALK fusion transcripts can complement each other to aid in the diagnosis of ALCL. © 2008 Elsevier Inc. All rights reserved. Introduction Anaplastic large-cell lymphoma (ALCL) was first described in 1985 by Stein and his co-workers, who reported that a subset of non- Hodgkin lymphoma expressed the CD30/Ki-1 antigen with frequent cohesive proliferation and lymph node infiltration (Stein et al., 1985). It is now agreed that ALCL is a T/null cell neoplasm frequently characterized by the aberrant anaplastic lymphoma kinase (ALK) protein expression, which results from chromosome translocation involving the ALK gene. About 80% of genetic alterations involve t(2;5) (p23;q35) translocation between the ALK gene on chromosome 2p23 and the nucleophosmin (NPM) gene on chromosome 5q35 (Delsol et al., 2001). Moreover, several studies have shown that the remaining 20% of ALK positive ALCLs are associated with other translocations in the ALK gene at 2p23, Some of these translocations include t(1;2)(q21;p23) creating the TPM3-ALK protein, t(2;19)(p23; q13.1) creating the TPM4-ALK Protein, t(2;3)(p23;q21) creating the TFG-ALK protein, t(2;17)(p23;q23) creating the CLTC-ALK protein, inv2(p23;q35) creating the ATIC-ALK protein, and t(2;17)(p23;q25) creating the ALO17-ALK protein (Pulford et al., 2004). All transloca- tions involve ALK possesses significant oncogenic potential resulting from the constitutive activation of the tyrosine kinase ALK. This kinase activation can induce growth factor-independent proliferation, cel- lular transformation, protection from apoptosis, and resistance to therapeutic drugs (Li and Morris, 2008). According to the current World Health Organization (WHO) classification of lymphomas, ALCL can be subdivided into two biologic subtypes based on the presence or absence of aberrant expression of ALK (Delsol et al., 2001). Moreover, studies have demonstrated that ALK-positive ALCL exhibits different molecular, pathological and clinical features, and suggest that it is a distinct entity (Salaverria et al., 2008). The examinations of ALK always present a challenge for the clinical pathologist in ALCL diagnosis. In previous studies, extensive immunophenotypic and molecular studies had used to detect ALK protein and related fusion transcripts (Dunphy et al., 2000; Rust et al., 2005; Schumacher et al., 2004; Suzuki et al., 2000). However, the simultaneous observation of ALK protein, ALK mRNA and ALK-associated fusion transcripts have been less frequently investigated, especially in formalin-fixed and paraffin-embedded tumors, and especially for their relationships to one another and their significances in pathological diagnosis. In this study, we explored in ALCL tissues (a) the expression of ALK protein by immunohistochemistry and mRNA, and (b) seven kinds of ALK-related fusion transcripts by RT-PCR following gene sequencing. These procedures were done in an effort to clarify their potential Experimental and Molecular Pathology 86 (2009) 121–126 ⁎ Corresponding author. Fax: +08621 64174774. E-mail address: [email protected] (X. Zhou). 0014-4800/$ – see front matter © 2008 Elsevier Inc. All rights reserved. doi:10.1016/j.yexmp.2008.11.012 Contents lists available at ScienceDirect Experimental and Molecular Pathology journal homepage: www.elsevier.com/locate/yexmp
-
Upload
wentao-huang -
Category
Documents
-
view
212 -
download
0
Transcript of Expression of ALK protein, mRNA and fusion transcripts in anaplastic large cell lymphoma

Experimental and Molecular Pathology 86 (2009) 121–126
Contents lists available at ScienceDirect
Experimental and Molecular Pathology
j ourna l homepage: www.e lsev ie r.com/ locate /yexmp
Expression of ALK protein, mRNA and fusion transcripts in anaplastic largecell lymphoma
Wentao Huang a, Xiaoqiu Li a, Xiaohong Yao b, Yongming Lu a, Baizhou Li a, Weiqi Sheng a, Hongfen Lu a,Aiping Jin a, Xiaoyan Zhou a,⁎a Department of Pathology, Cancer Hospital, Department of Oncology, Shanghai Medical Collage, Fudan University 270 Dongan Road, Shanghai 200032, P.R. Chinab Department of Pathology, Xinhua Hospital, Shanghai Jiao Tong University, Shanghai 200092, P.R. China
⁎ Corresponding author. Fax: +08621 64174774.E-mail address: [email protected] (X. Zhou).
0014-4800/$ – see front matter © 2008 Elsevier Inc. Adoi:10.1016/j.yexmp.2008.11.012
a b s t r a c t
a r t i c l e i n f oArticle history:
Systemic anaplastic large c Received 7 August 2008Available online 14 December 2008Keywords:Anaplastic large cell lymphomaALKAnaplastic lymphoma kinaseFusion transcriptImmunohistochemistryReverse transcription polymerasechain reaction
ell lymphoma (ALCL) can be divided into two subgroups, anaplastic lymphomakinase (ALK)-positive and ALK-negative, based on the expression of ALK protein. Expression of this protein isdue to genetic alterations of ALK at 2p23. Overall, observations on ALK protein, ALK mRNA, ALK-associatedgenetic alterations and their relationships, to one another are not often reported in the literature. In thisstudy, we investigated the expression of ALK protein, mRNA and fusion transcripts involving ALK and theirrelationships in ALCL and analyzed formalin-fixed, paraffin-embedded tissues. Forty-five human cases wereanalyzed with immunohistochemistry for the ALK protein and RT-PCR for ALK mRNA and seven kinds of ALKinvolved fusion transcripts. Our results showed that the expression of ALK protein, ALK mRNA and ALKfusion transcripts were significantly related to one another (Pb0.01). Consistent with the expression of ALKprotein, patients presenting with ALK mRNA or ALK involved fusion transcripts were significantly youngerthan those lacking ALK gene alteration (Pb0.01). This study demonstrates expression of both ALK proteinand ALK mRNA are positively correlated with expression of ALK-associated fusion transcripts. Combineddetection of ALK protein, ALK mRNA and ALK fusion transcripts can complement each other to aid in thediagnosis of ALCL.
© 2008 Elsevier Inc. All rights reserved.
Introduction
Anaplastic large-cell lymphoma (ALCL) was first described in 1985by Stein and his co-workers, who reported that a subset of non-Hodgkin lymphoma expressed the CD30/Ki-1 antigen with frequentcohesive proliferation and lymph node infiltration (Stein et al., 1985).It is now agreed that ALCL is a T/null cell neoplasm frequentlycharacterized by the aberrant anaplastic lymphoma kinase (ALK)protein expression, which results from chromosome translocationinvolving the ALK gene. About 80% of genetic alterations involve t(2;5)(p23;q35) translocation between the ALK gene on chromosome 2p23and the nucleophosmin (NPM) gene on chromosome 5q35 (Delsolet al., 2001). Moreover, several studies have shown that theremaining 20% of ALK positive ALCLs are associated with othertranslocations in the ALK gene at 2p23, Some of these translocationsinclude t(1;2)(q21;p23) creating the TPM3-ALK protein, t(2;19)(p23;q13.1) creating the TPM4-ALK Protein, t(2;3)(p23;q21) creating theTFG-ALK protein, t(2;17)(p23;q23) creating the CLTC-ALK protein,inv2(p23;q35) creating the ATIC-ALK protein, and t(2;17)(p23;q25)creating the ALO17-ALK protein (Pulford et al., 2004). All transloca-tions involve ALK possesses significant oncogenic potential resulting
ll rights reserved.
from the constitutive activation of the tyrosine kinase ALK. This kinaseactivation can induce growth factor-independent proliferation, cel-lular transformation, protection from apoptosis, and resistance totherapeutic drugs (Li and Morris, 2008).
According to the current World Health Organization (WHO)classification of lymphomas, ALCL can be subdivided into two biologicsubtypes based on the presence or absence of aberrant expression ofALK (Delsol et al., 2001). Moreover, studies have demonstrated thatALK-positive ALCL exhibits different molecular, pathological andclinical features, and suggest that it is a distinct entity (Salaverriaet al., 2008). The examinations of ALK always present a challenge forthe clinical pathologist in ALCL diagnosis. In previous studies,extensive immunophenotypic and molecular studies had used todetect ALK protein and related fusion transcripts (Dunphy et al., 2000;Rust et al., 2005; Schumacher et al., 2004; Suzuki et al., 2000).However, the simultaneous observation of ALK protein, ALK mRNAand ALK-associated fusion transcripts have been less frequentlyinvestigated, especially in formalin-fixed and paraffin-embeddedtumors, and especially for their relationships to one another andtheir significances in pathological diagnosis.
In this study, we explored in ALCL tissues (a) the expression of ALKprotein by immunohistochemistry and mRNA, and (b) seven kinds ofALK-related fusion transcripts by RT-PCR following gene sequencing.These procedures were done in an effort to clarify their potential

Table 1Primers used to detect PGK, ALK, and ALK fusion transcripts
Prime Sequence 5′-3′ PCR productsize
Anneallingtemperature
(bp) (°C)
PGK F-GGGCTGCATCACCATCATAGG 148 57R-GAGAGCATCCACCCCAGGAAG
ALK F-GATGGACCCACCCAAGAACTG 154 60R-CGGCAAAGCGGTGTTGATTAC
NPM-ALK F-TCCCTTGGGGGCTTTGAAATAACAC 177 60R-CGGCAAAGCGGTGTTGATTAC
ALO17 F-TGAAGATGTGTGGGAACGTG 115 60TPM3 F-AGAGACCCGTGCTGAGTTTGCTGA 147 60TPM4 F-TGAGACCCGTGCTGAATTTGCAGA 147 60TFG F-CAGCAGCCACCATATACAGGA 128 60ATIC F-TGGAATGAACCCACATCAGAC 144 60CLTC F-GAAGGAGTACTTGACAAAGGTGGAT 174 60ALK† R-CGGAGCTTGCTCAGCTTGTA
F: Forward primer; R: reverse primer.† A common reverse primer was used in RT-PCR for detection of various ALK fusion
genes.
122 W. Huang et al. / Experimental and Molecular Pathology 86 (2009) 121–126
relevance and the contribution of ALK protein, ALK mRNA, and ALK-associated fusion transcripts in the clinicopathologic diagnosis ofALCL.
Materials and methods
Patient population and tissue samples
Samples for a total of 45 cases of primary systemic ALCL (formalin-fixed and paraffin-embedded tissues) were retrieved from the
Fig. 1. Morphology of primary systemic ALCL: (a) a common histologic variant showing asinusoidal involvement (H&E, ×400); (c) a lymphohistiocytic variant (H&E, ×400); (d) a s
institutional and consultation files from two departments of pathol-ogy, Cancer Hospital, Fudan University and the department ofpathology, Xinhua Hospital, Shanghai Jiao Tong University, Shanghai,P.R. China. All patientswere diagnosed between January 1999 and June2006. Each casewas independently reviewed by twopathologists, whomade a diagnosis based on morphological and immunophenotypiccriteria, as described in the WHO classification (Delsol et al., 2001).Twenty-seven patients were male and 18 were female (M: F=1.6:1),with amean age of 31 years (range3 to 71 years). Of them, 42 cases hadat least one lymph node involved, and 3 cases had only extranodaldisease observed (one skull, one right elbow, one peritoneal cavity).
Immunohistochemistry
Immunohistochemical staining was performed using an immuno-peroxidase technique, as described elsewhere (Rassidakis et al., 2001).In brief, paraffin sections were dewaxed with xylene and rehydratedin a graded ethanol series. After heat-induced antigen retrieval in0.01 mol/L citrate buffer (pH6.0), the sections were incubated withALK monoclonal antibody (ALK1, 1:30 dilution; Dako), CD30 mono-clonal antibody (Ber-H2, 1:30 dilution; Dako), CD20 monoclonalantibody (L26, 1:100 dilution; Dako) and CD3 polyclonal antibody(1:50 dilution; Dako) in a humidified chamber at room temperaturefor 60 min and then at 4 °C overnight. Slides known to express ALK,CD30, CD20 and CD3 were used as the positive controls and slidesprocessed with tris buffered saline (TBS) instead of primaryantibodies were used as the negative controls. On the second day,the sections were washed with phosphate buffered saline (PBS) threetimes, incubated with the EnVision reagent (Dako) at room
diffuse and cohesive pattern (H&E, ×400); (b) a common histologic variant, showingmall cell variant (H&E, ×400).

123W. Huang et al. / Experimental and Molecular Pathology 86 (2009) 121–126
temperature for 30 minutes, visualized with 3,3′-diaminobenzidinetetrahydochloride (DAB)/H2O2 for 10 minutes and finally counter-stained with hematoxylin. Positive reactivity with ALK was defined asnuclear and/or cytoplasmic staining in tumor cells with no back-ground. We used previously published criteria for identifying a panelof antibodies (Asano et al., 2007). In addition, lymphomas wereconsidered to be of T-cell lineage when tumor cells expressed CD3,and considered Null type when CD3 and CD20 were both negative.
RNA extraction and RT-PCR sequencing
Total RNA was extracted from tumor tissues using Trizol reagent(Invitrogen Life Technologies) as described previously (Lamant etal., 1996; Trinei et al., 2000; Wellmann et al., 1995). RNAs extractedfrom the t(2;5)-positive SU-DHL-1 and Karpas299 cell line wereused as positive controls, while DEPC water and RNA from propernegative tissue (normal lymph node) were used as negativecontrols. Reverse transcription of RNA into cDNA was performedby incubating one μg RNA (purified by DNase digestion using TURBODNase from Ambion), one μL of random primer (Promega, USA),and 200 U of reverse transcriptase (Promega, USA) in a 25 μLreaction volume at 37 °C for one hour. One μL cDNA was thensubmitted to PCR amplification. To assess the quality of cDNA ineach sample, the transcripts of a housekeeping gene PGK weresimultaneously detected as an internal control. To detect theexpression of ALK mRNA and seven kinds of ALK-associated fusiontranscripts, all PCR reactions were performed using specific primers,which revealed the expected ALK or ALK chimeric mRNA fragment.
Fig. 2. Immunohistochemical detection in ALCL tumors: (a) showing CD30+ lymphoma cellscells (membranous and cytoplasmic, EnVision×400); (c) showing ALK1+ lymphoma celymphoma cells (cytoplasmic staining pattern, EnVision×400).
Informations regarding the primers, their sequences and annealingtemperatures were as previously described (Colleoni et al., 2000; Li etal., 2004) and are shown in Table 1. The optimized thermal cyclingcondition for ALKmRNA and ALK-associated fusion gene amplificationconsisted of an initial denaturation step at 95 °C for 10 minutes andthen 42 cycles of 94 °C for 30 seconds, 57 °C/60 °C for 30 seconds, and72 °C for 1minute, followedbya final extension at 72 °C for 10minutes.The presence of PCR products were tested using 2% agarose gels,compared with a 100 bp DNA marker. After observing clear andaccurately sized bands, the products were purified and sequencedusing the ABI Prism 3730 Sequence Detector System.
Statistical analysis
The χ2 and Fisher's exact tests for statistical significance wereperformed using the Statistical Package for the Social Sciencessoftware for Windows (SPSS version 11.0). P values of less than 0.05were considered statistically significant.
Results
Clinical, morphological and immunohistochemical features
According to the morphological features described in the WHOclassification of lymphomas, of the 45 ALCL cases we evaluated, 43were classified as common type ALCL, one as a small cell variant andone as a lymphohistiocytic variant (Figs. 1a, b, c, d). All 45 cases werepositive for CD30 and the staining patternwas, as previouslydescribed,
(membranous and Golgi zone pattern, EnVision×400); (b) showing CD3+ lymphomalls (nuclear and cytoplasmic staining pattern, EnVision×400); (d) showing ALK1+
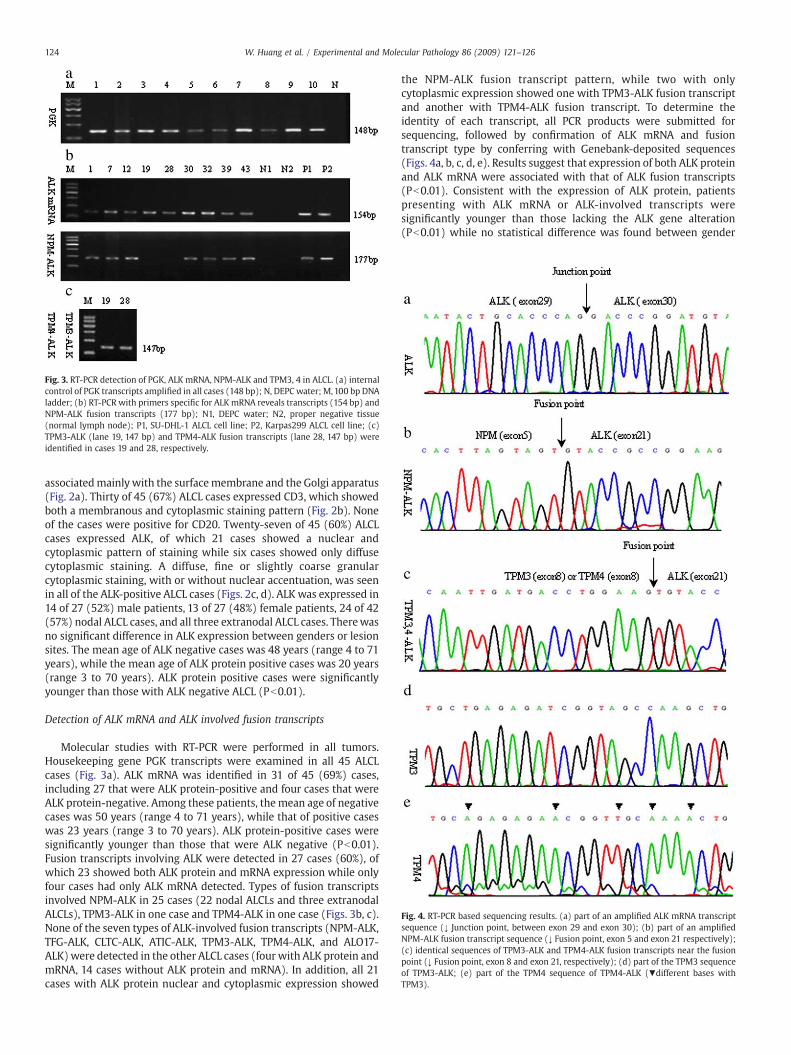
Fig. 3. RT-PCR detection of PGK, ALK mRNA, NPM-ALK and TPM3, 4 in ALCL. (a) internalcontrol of PGK transcripts amplified in all cases (148 bp); N, DEPC water; M,100 bp DNAladder; (b) RT-PCR with primers specific for ALKmRNA reveals transcripts (154 bp) andNPM-ALK fusion transcripts (177 bp); N1, DEPC water; N2, proper negative tissue(normal lymph node); P1, SU-DHL-1 ALCL cell line; P2, Karpas299 ALCL cell line; (c)TPM3-ALK (lane 19, 147 bp) and TPM4-ALK fusion transcripts (lane 28, 147 bp) wereidentified in cases 19 and 28, respectively.
Fig. 4. RT-PCR based sequencing results. (a) part of an amplified ALK mRNA transcriptsequence (↓ Junction point, between exon 29 and exon 30); (b) part of an amplifiedNPM-ALK fusion transcript sequence (↓ Fusion point, exon 5 and exon 21 respectively);(c) identical sequences of TPM3-ALK and TPM4-ALK fusion transcripts near the fusionpoint (↓ Fusion point, exon 8 and exon 21, respectively); (d) part of the TPM3 sequenceof TPM3-ALK; (e) part of the TPM4 sequence of TPM4-ALK (▾different bases withTPM3).
124 W. Huang et al. / Experimental and Molecular Pathology 86 (2009) 121–126
associatedmainlywith the surfacemembrane and the Golgi apparatus(Fig. 2a). Thirty of 45 (67%) ALCL cases expressed CD3, which showedboth a membranous and cytoplasmic staining pattern (Fig. 2b). Noneof the cases were positive for CD20. Twenty-seven of 45 (60%) ALCLcases expressed ALK, of which 21 cases showed a nuclear andcytoplasmic pattern of staining while six cases showed only diffusecytoplasmic staining. A diffuse, fine or slightly coarse granularcytoplasmic staining, with or without nuclear accentuation, was seenin all of the ALK-positive ALCL cases (Figs. 2c, d). ALK was expressed in14 of 27 (52%) male patients, 13 of 27 (48%) female patients, 24 of 42(57%) nodal ALCL cases, and all three extranodal ALCL cases. Therewasno significant difference in ALK expression between genders or lesionsites. The mean age of ALK negative cases was 48 years (range 4 to 71years), while the mean age of ALK protein positive cases was 20 years(range 3 to 70 years). ALK protein positive cases were significantlyyounger than those with ALK negative ALCL (Pb0.01).
Detection of ALK mRNA and ALK involved fusion transcripts
Molecular studies with RT-PCR were performed in all tumors.Housekeeping gene PGK transcripts were examined in all 45 ALCLcases (Fig. 3a). ALK mRNA was identified in 31 of 45 (69%) cases,including 27 that were ALK protein-positive and four cases that wereALK protein-negative. Among these patients, themean age of negativecases was 50 years (range 4 to 71 years), while that of positive caseswas 23 years (range 3 to 70 years). ALK protein-positive cases weresignificantly younger than those that were ALK negative (Pb0.01).Fusion transcripts involving ALK were detected in 27 cases (60%), ofwhich 23 showed both ALK protein and mRNA expression while onlyfour cases had only ALK mRNA detected. Types of fusion transcriptsinvolved NPM-ALK in 25 cases (22 nodal ALCLs and three extranodalALCLs), TPM3-ALK in one case and TPM4-ALK in one case (Figs. 3b, c).None of the seven types of ALK-involved fusion transcripts (NPM-ALK,TFG-ALK, CLTC-ALK, ATIC-ALK, TPM3-ALK, TPM4-ALK, and ALO17-ALK)were detected in the other ALCL cases (four with ALK protein andmRNA, 14 cases without ALK protein and mRNA). In addition, all 21cases with ALK protein nuclear and cytoplasmic expression showed
the NPM-ALK fusion transcript pattern, while two with onlycytoplasmic expression showed one with TPM3-ALK fusion transcriptand another with TPM4-ALK fusion transcript. To determine theidentity of each transcript, all PCR products were submitted forsequencing, followed by confirmation of ALK mRNA and fusiontranscript type by conferring with Genebank-deposited sequences(Figs. 4a, b, c, d, e). Results suggest that expression of both ALK proteinand ALK mRNA were associated with that of ALK fusion transcripts(Pb0.01). Consistent with the expression of ALK protein, patientspresenting with ALK mRNA or ALK-involved transcripts weresignificantly younger than those lacking the ALK gene alteration(Pb0.01) while no statistical difference was found between gender

Table 2Characteristics and relationships between ALK protein, ALK mRNA, and ALK fusiontranscripts in ALCL
ALK Protein P ALK mRNA P
Positive Negative Positive NegativeN=27 N=18 N=31 N=14
AgeMedian(years) 20 48 0.001 23 50 0.000Range(years) 3∼70 4∼71 3∼70 4∼71Gender 0.079 0.128Male 14 14 17 11Female 13 4 14 3Site 0.264† 0.541†
Nodal 24 18 28 14Extranodal 3 0 3 0Fusion transcript 23 4 0.000‡ 27 0 0.000‡
NPM-ALK fusion transcript 21 4 25 0TPM3-ALK fusiontranscript
1 0 1 0
TPM4-ALK fusiontranscript
1 0 1 0
Lacking fusion transcript 4 14 4 14
† Calculated using Fisher's exact test.‡ Measure of agreement Kappa.
Table 3Ten ALCL cases without concordant results of ALK protein, ALK mRNA and ALK-NPM
Case no. Age(years)/Sex ALK Protein ALK mRNA ALK involvedfusion transcript
17 34/M - + NPM-ALK35 35/M - + NPM-ALK43 69/F - + NPM-ALK45 29/M - + NPM-ALK21 15/M + + NF31 8/M + + NF37 42/M + + NF47 22/F + + NF
M: Male; F: Female; NF: Not Found.
125W. Huang et al. / Experimental and Molecular Pathology 86 (2009) 121–126
and lesion sites. The clinical characteristics and relationships betweenALK protein, ALKmRNA and ALK fusion transcripts are listed in Table 2,and the cases without concordant results are summarized in Table 3.
Discussion
It is now agreed upon that ALCL is a heterogeneous group amongaggressive lymphomas (Falini, 2001). Due to ALK gene translocations,about 60% of ALCLs express the ALK chimeric protein, thus represent-ing a distinct clinicopathologic entity known as ALK-positive (ALK+)ALCL (Delsol et al., 2001; Falini et al., 1999). There is generalagreement that immunohistochemical analysis is well suited for ALK+ ALCL tissue specimens (Amin and Lai, 2007), especially in formalin-fixed, paraffin-embedded sections. Further, RT-PCR methods have agreater role in the assessment of minimal residual disease (Medeirosand Elenitoba-Johnson, 2007). In order to determine if the expressionof ALKmRNA and fusion transcripts are correlated with ALK protein inALCL samples and are suitable for clinical diagnosis, we combinedimmunohistochemical staining and RT-PCR following gene sequen-cing. The results showed that expression of ALK protein, mRNA, andfusion transcripts were found in 60% (27/45), 69% (31/45) and 60%(27/45), respectively, which are similar to one another. Cataldo et al.(1999), who used the same approach for 27 ALCL samples, showedthat the expression of ALK protein and NPM-ALK mRNAwas 51% (14/27) and 19% (5/27), respectively. The higher ALKmRNA in the presentstudy may be due to the greater quantity of reserved samples andricher tumor cells. Our data also suggest that the detection of ALKmRNA by RT-PCR may be more sensitive than that of ALK protein byimmunohistochemistry, although RNA was extracted from paraffinembedded tissues. In a recent study, Li et al. (2007) used RT-PCRanalysis in 26 cases of ALK+ ALCL, and showed that NPM-ALK, TPM3-ALK and TFG-ALK fusion transcripts were 81% (21/26),11% (3/26) and4% (1/26) respectively. One remaining case (4%) was ATIC-ALK fusiontranscript confirmed by 5′RACE. Our study data showed similarpercentages of ALK fusion types: NPM-ALK, TPM3-ALK and TPM4-ALKfusion transcripts were 92% (25/27), 4% (1/27) and 4% (1/27)respectively. RT-PCR may be used to analyze for 5′RACE in the fourcases without any ALK fusion partners. In addition, our study putsgreater emphasis on the relationships between ALK protein, ALKmRNA and fusion transcripts in ALCL. The data show striking andsignificant associations among ALK protein, mRNA, and fusiontranscripts, and therefore these markers may supplement each otherin the clinicopathologic diagnosis of ALCL.
Some evidence demonstrates that the NPM-ALK fusion protein isdirected from the cytoplasm to the nuclei of the tumor cells(Rosenwald et al., 1999). In our study, RT-PCR results were inagreement with these staining patterns and demonstrated theexpression of TPM3-ALK and TPM4-ALK transcripts with cytoplasmicALK staining. Therefore, the type of ALK-associated fusion transcriptcan directly reflect the type of ALK translocations, and we canindirectly infer the types of ALK translocations by ALK expressioncharacteristics. Malignant cells carrying the t(2;5) translocation showboth cytoplasmic and nuclear staining for NPM-ALK, and it appears tobe due to NPM-ALK form heterodimers with wild-type NPM throughthe NPM oligomerization domain, which imports NPM-ALK into thenucleus via shuttling (Benharroch et al., 1998; Naoe et al., 2006). Theproducts of other genes translocated with ALKmay originally locate incytoplasm, fusion protein results from confined to cytoplasm(Benharroch et al., 1998). In addition, mesin is a part of the plasmamembrane, and therefore the MSN-ALK chimeric protein exhibits acell membrane-associated immunostaining pattern (Pulford et al.,2004; Tort et al., 2004).
ALK is a receptor tyrosine kinase truncated and fused to a variety ofN-terminal, activating partner proteins, the most common chimericform being NPM-ALK in ALCL (Pulford et al., 2004) ALK protein isfound in 60%-85% of ALCLs, and is regarded as a specific marker forALCL (Borisch et al., 2003; Pulford et al., 2004). In addition, full-lengthALK proteins are detected in rare scattered neural cells, pericytes andendothelial cells of the normal human brain (Pulford et al., 1997).Other pathologic lesions also overexpress ALK including some solidtumors, a subset of inflammatory myofibroblastic tumors (IMTs), anda rare subtype of diffuse large B-cell lymphoma (DLBCL). This subtypeof lymphoma was originally thought to express full-length ALK but itis now confirmed that they present the ALK fusion protein CLTC-ALK(De Paepe et al., 2003; Gascoyne et al., 2003). Therefore, immuno-histochemical association with RT-PCR and gene sequencing may behelpful for the clinical differential diagnosis of ALCL. In addition toNPM-ALK, our study identified two cases of other fusion partners,TPM3-ALK and TPM4-ALK, which are generated by the t(1;2) and the t(2;19) translocations, respectively. TPM3 encodes a non-muscletropomyosin, of which the N-terminal residues are fused to ALK,while TPM4 is a homologue of TPM3 (Bohling et al., 2008; Pulford et al.,2004). Moreover, the fusion breakpoints were found in the corre-sponding location for both genes. RT-PCR showed 147-bp transcriptsproducts in two cases, and following sequencing analysis showed onecase with TPM3-ALK and another case with TPM4-ALK. There wereonly a few bases differences between the TPM3-ALK and TPM4-ALKfusion transcripts. Our study demonstrates the convenience of theidentification of fusion transcript type by the sequencing of RT-PCRproducts.
Although the current WHO classification of lymphomas considersthe ALK+ ALCL and ALK- ALCL to share the same morphological andimmunohistochemical phenotypic features, it is now suggested thatthese two types of lymphomas have different gene expression profiles,supporting the idea that they are indeed different biological entities(Lamant et al., 2007; Salaverria et al., 2008). ALCL has a peak incidence

126 W. Huang et al. / Experimental and Molecular Pathology 86 (2009) 121–126
in childhood and accounts for approximately 40% of non-Hodgkin'slymphoma cases diagnosed in pediatric populations, particularly inALK+ patients, which shows a favorable prognosis (Jacobsen, 2006).In addition, the clinical outcome of patients with ALK+ ALCL is usuallyyounger than that of ALK- ALCL patients (Chiarle et al., 2008; Delsol etal., 2001). In our study, we found that patients in ALK groups (positivefor ALK protein, ALK mRNA or ALK-involved fusion transcripts) aresignificantly younger than ALK negative groups, which is consistentwith previous studies (Li et al., 2007). In addition, NPM-relatedtranslocations are regarded as a marker indicating a favorableprognosis (Falini et al., 2007). Whether other mutated genes, suchas TPM3 or TPM4, also apply to the same prognostic category of ALCLpatients remains to be shown. The significance of ALK- ALCL iscurrently still controversial. Some researchers regard it as a variant ofperipheral T-cell lymphoma, unspecified (PTCL-u), or the end stage ofhistological transformation for other types of T-cell lymphomas(Medeiros and Elenitoba-Johnson, 2007). The biological mechanismand prognostic markers for ALK- ALCL need to be further investigated.
In summary, ALK+ ALCL is a specific type of lymphomacharacterized by clinical presentation, morphology, and geneticaberrations. Our study demonstrates that both ALK protein and ALKmRNA expression are positively correlated with ALK-related fusiontranscripts. Further, the combination of immunohistochemical detec-tion of ALK protein, RT-PCR detection of mRNA and fusion transcriptsinvolving ALK may be beneficial in the clinicopathologic diagnosis ofALK-positive ALCL.
Acknowledgments
This studywas supported by a grant from the Science & TechnologyCommission of Shanghai Municipality (STCSM) (Code No:054119638).
References
Amin, H.M., Lai, R., 2007. Pathobiology of ALK+ anaplastic large-cell lymphoma. Blood110, 2259–2267.
Asano, N., et al., 2007. Cytotoxic molecule expression is predictive of prognosis inHodgkin's-like anaplastic large cell lymphoma. Histopathology 50, 705–715.
Benharroch, D., et al., 1998. ALK-positive lymphoma: a single disease with a broadspectrum of morphology. Blood 91, 2076–2084.
Bohling, S.D., et al., 2008. Analysis of gene expression profile of TPM3-ALK positiveanaplastic large cell lymphoma reveals overlapping and unique patterns with thatof NPM-ALK positive anaplastic large cell lymphoma. Leuk. Res. 32, 383–393.
Borisch, B., et al., 2003. ALK-positive anaplastic large-cell lymphoma: strong T and Banti-tumour responses may cause hypocellular aspects of lymph nodes mimickinginflammatory lesions. Eur. J. Haematol. 71, 243–249.
Cataldo, K.A., et al., 1999. Detection of t(2;5) in anaplastic large cell lymphoma:comparison of immunohistochemical studies, FISH, and RT-PCR in paraffin-embedded tissue. Am. J. Surg. Pathol. 23, 1386–1392.
Chiarle, R., et al., 2008. The anaplastic lymphoma kinase in the pathogenesis of cancer.Nat. Rev., Cancer 8, 11–23.
Colleoni, G.W., et al., 2000. ATIC-ALK: A novel variant ALK gene fusion in anaplastic largecell lymphoma resulting from the recurrent cryptic chromosomal inversion, inv(2)(p23q35). Am. J. Pathol. 156, 781–789.
De Paepe, P., et al., 2003. ALK activation by the CLTC-ALK fusion is a recurrent event inlarge B-cell lymphoma. Blood 102, 2638–2641.
Delsol, G.R.E., Stein, H., et al., 2001. Anaplastic large cell lymphoma. In: Jaffe, ES, Harris,NL, Stein, H, et al. (Eds.), World Health Organization Classification of Tumours:Pathology and Genetics of Tumours of Aematopoietic and Lymphoid Tissues. IARCPress, lyon, France, pp. 230–235.
Dunphy, C.H., et al., 2000. CD30+ anaplastic large-cell lymphoma with aberrantexpression of CD13: case report and review of the literature. J. Clin. Lab. Anal. 14,299–304.
Falini, B., 2001. Anaplastic large cell lymphoma: pathological, molecular and clinicalfeatures. Br. J. Haematol. 114, 741–760.
Falini, B., et al., 1999. ALK+ lymphoma: clinico-pathological findings and outcome.Blood 93, 2697–2706.
Falini, B., et al., 2007. Translocations and mutations involving the nucleophosmin(NPM1) gene in lymphomas and leukemias. Haematologica 92, 519–532.
Gascoyne, R.D., et al., 2003. ALK-positive diffuse large B-cell lymphoma is associatedwith Clathrin-ALK rearrangements: report of 6 cases. Blood 102, 2568–2573.
Jacobsen, E., 2006. Anaplastic large-cell lymphoma, T-/null-cell type. Oncologist 11,831–840.
Lamant, L., et al., 1996. High incidence of the t(2;5)(p23;q35) translocation in anaplasticlarge cell lymphoma and its lack of detection in Hodgkin's disease. Comparison ofcytogenetic analysis, reverse transcriptase-polymerase chain reaction, and P-80immunostaining. Blood 87, 284–291.
Lamant, L., et al., 2007. Gene-expression profiling of systemic anaplastic large-celllymphoma reveals differences based on ALK status and two distinct morphologicALK+ subtypes. Blood 109, 2156–2164.
Li, R., Morris, S.W., 2008. Development of anaplastic lymphoma kinase (ALK) small-molecule inhibitors for cancer therapy. Med. Res. Rev. 28, 372–412.
Li, X.Q., et al., 2004. Expression of anaplastic lymphoma kinase in soft tissue tumors: animmunohistochemical and molecular study of 249 cases. Hum. Pathol. 35, 711–721.
Li, C., et al., 2007. Prognostic significance of NPM-ALK fusion transcript overexpressionin ALK-positive anaplastic large-cell lymphoma. Mod. Pathol. 20, 648–655.
Medeiros, L.J., Elenitoba-Johnson, K.S., 2007. Anaplastic large cell lymphoma. Am. J. Clin.Pathol. 127, 707–722.
Naoe, T., et al., 2006. Nucleophosmin: a versatile molecule associated with hematolo-gical malignancies. Cancer Sci. 97, 963–969.
Pulford, K., et al., 1997. Detection of anaplastic lymphoma kinase (ALK) and nucleolarprotein nucleophosmin (NPM)-ALK proteins in normal and neoplastic cells withthe monoclonal antibody ALK1. Blood 89, 1394–1404.
Pulford, K., et al., 2004. Anaplastic lymphoma kinase proteins in growth control andcancer. J. Cell. Physiol. 199, 330–358.
Rassidakis, G.Z., et al., 2001. Differential expression of BCL-2 family proteins in ALK-positive and ALK-negative anaplastic large cell lymphoma of T/null-cell lineage.Am. J. Pathol. 159, 527–535.
Rosenwald, A., et al., 1999. t(1;2)(q21;p23) and t(2;3)(p23;q21): two novel varianttranslocations of the t(2;5)(p23;q35) in anaplastic large cell lymphoma. Blood 94,362–364.
Rust, R., et al., 2005. High expression of Mcl-1 in ALK positive and negative anaplasticlarge cell lymphoma. J. Clin. Pathol. 58, 520–524.
Salaverria, I., et al., 2008. Genomic profiling reveals different genetic aberrations insystemic ALK-positive and ALK-negative anaplastic large cell lymphomas. Br. J.Haematol. 140, 516–526.
Schumacher, J.A., et al., 2004. Utility of linearly amplified RNA for RT-PCR detection ofchromosomal translocations: validation using the t(2;5)(p23;q35) NPM-ALKchromosomal translocation. J. Mol. Diagn. 6, 16–21.
Stein, H., et al., 1985. The expression of the Hodgkin's disease associated antigen Ki-1 inreactive and neoplastic lymphoid tissue: evidence that Reed-Sternberg cells andhistiocyticmalignancies are derived fromactivated lymphoid cells. Blood 66, 848–858.
Suzuki, R., et al., 2000. Prognostic significance of CD56 expression for ALK-positive andALK-negative anaplastic large-cell lymphoma of T/null cell phenotype. Blood 96,2993–3000.
Tort, F., et al., 2004. Heterogeneity of genomic breakpoints inMSN-ALK translocations inanaplastic large cell lymphoma. Hum. Pathol. 35, 1038–1041.
Trinei, M., et al., 2000. A new variant anaplastic lymphoma kinase (ALK)-fusion protein(ATIC-ALK) in a case of ALK-positive anaplastic large cell lymphoma. Cancer Res. 60,793–798.
Wellmann, A., et al., 1995. Analysis of the t(2;5)(p23;q35) translocation by reversetranscription-polymerase chain reaction in CD30+ anaplastic large-cell lympho-mas, in other non-Hodgkin's lymphomas of T-cell phenotype, and in Hodgkin'sdisease. Blood 86, 2321–2328.


















