ExpErimEntal - University of...
9
www.PRSJournal.com 1004 D amage to sensory nerves may result in a painful neuroma. This results from aber- rant proliferation of nerve endings in the stump, 1 and may result in neuropathic pain because of persistent abnormal excitability of sen- sory nerve endings. 2 A number of techniques have been described to reduce the incidence of neuro- mas in sharply transected nerves. These include burying in muscle, 3,4 capping with vein, 5 and even oblique transection of the nerve. 6 In the management of peripheral nerves, where neuromas are typically encountered and studied, these are sharply transected where indicated in such situations as amputation surgery or trauma. In the senior author’s (B.G.) practice, however, a significant number of patients present for migraine surgery, with one of the trigger sites requiring ablation of the zygomaticotemporal branch of the facial nerve. 7 The small caliber of the nerve and the surgical approach allow avulsion or transection and possibly transection and folding of the nerve. Another situation where avulsion of nerves may occur is in surgical approaches to the upper craniofacial skeleton and midface, where the supraorbital, supratrochlear, or infraorbital nerves may be damaged close to the orbital rim where the available muscles (corrugator and The Role of Different Methods of Nerve Ablation in Prevention of Neuroma Harvey Chim, M.D. Erin Miller, M.D. Christy Gliniak, B.S. Mark L. Cohen, M.D. Bahman Guyuron, M.D. Cleveland, Ohio Background: The aim of this study was to compare the incidence of neuroma formation and neuropathic pain following different techniques of nerve abla- tion in a rat sural nerve model. Methods: Rat sural nerve was subjected to four different techniques of abla- tion with standardized creation of a 1-cm gap (n = 15 in each group). These included nerve avulsion, transection and burying in muscle, transection and folding of nerve, and transection alone. Animals were killed after 3 months. Explanted nerves were sectioned and stained with Masson trichrome and S-100 stain against neural tissue. The maximal neural cross-sectional area and neural- to-connective tissue ratio was quantified. Quantitative reverse-transcriptase poly- merase chain reaction (n = 5) was used to analyze relative mRNA expression of ciliary neurotrophic factor and calcitonin gene-related peptide. Results: Neural cross-sectional area was statistically increased (p < 0.05) com- pared with controls in folded, muscle buried, and transected specimens but decreased in avulsed specimens. The neural-to-connective tissue ratio was sta- tistically decreased in the avulsed group. Relative mRNA expression of cili- ary neurotrophic factor was lowest in muscle buried (4 percent of control) (p < 0.05) and avulsed specimens (15 percent of control) (p < 0.05) and higher in folded (52 percent of control) and transected specimens (75 percent of con- trol). Relative mRNA expression of calcitonin gene-related peptide was highest in folded specimens (302 percent of control) (p < 0.05). Conclusions: Folding and transection lead to increased histologic evidence of neuroma formation, whereas folding leads to neuropathic pain, assayed by calci- tonin gene-related peptide expression. Avulsion and muscle burying are prefer- able techniques for nerve ablation and inhibit nerve regeneration, evidenced by decreased ciliary neurotrophic factor expression. Avulsion offers an alternative to muscle burying when there is no muscle in the vicinity to bury the transected nerve. (Plast. Reconstr. Surg. 131: 1004, 2013.) Disclosure: The authors have no financial interest to declare in relation to the content of this article. From the Department of Plastic Surgery and the Department of Pathology, Case Western Reserve University. Received for publication July 17, 2012; accepted November 30, 2012. Copyright © 2013 by the American Society of Plastic Surgeons DOI: 10.1097/PRS.0b013e3182879ec2 EXPERIMENTAL
Transcript of ExpErimEntal - University of...

www.PRSJournal.com1004
Damage to sensory nerves may result in a painful neuroma. This results from aber-rant proliferation of nerve endings in
the stump,1 and may result in neuropathic pain because of persistent abnormal excitability of sen-sory nerve endings.2 A number of techniques have been described to reduce the incidence of neuro-mas in sharply transected nerves. These include burying in muscle,3,4 capping with vein,5 and even oblique transection of the nerve.6
In the management of peripheral nerves, where neuromas are typically encountered and
studied, these are sharply transected where indicated in such situations as amputation surgery or trauma. In the senior author’s (B.G.) practice, however, a significant number of patients present for migraine surgery, with one of the trigger sites requiring ablation of the zygomaticotemporal branch of the facial nerve.7 The small caliber of the nerve and the surgical approach allow avulsion or transection and possibly transection and folding of the nerve. Another situation where avulsion of nerves may occur is in surgical approaches to the upper craniofacial skeleton and midface, where the supraorbital, supratrochlear, or infraorbital nerves may be damaged close to the orbital rim where the available muscles (corrugator and
The Role of Different Methods of Nerve Ablation in Prevention of Neuroma
Harvey Chim, M.D.Erin Miller, M.D.
Christy Gliniak, B.S.Mark L. Cohen, M.D.
Bahman Guyuron, M.D.
Cleveland, Ohio
Background: The aim of this study was to compare the incidence of neuroma formation and neuropathic pain following different techniques of nerve abla-tion in a rat sural nerve model.Methods: Rat sural nerve was subjected to four different techniques of abla-tion with standardized creation of a 1-cm gap (n = 15 in each group). These included nerve avulsion, transection and burying in muscle, transection and folding of nerve, and transection alone. Animals were killed after 3 months. Explanted nerves were sectioned and stained with Masson trichrome and S-100 stain against neural tissue. The maximal neural cross-sectional area and neural-to-connective tissue ratio was quantified. Quantitative reverse-transcriptase poly-merase chain reaction (n = 5) was used to analyze relative mRNA expression of ciliary neurotrophic factor and calcitonin gene-related peptide. Results: Neural cross-sectional area was statistically increased (p < 0.05) com-pared with controls in folded, muscle buried, and transected specimens but decreased in avulsed specimens. The neural-to-connective tissue ratio was sta-tistically decreased in the avulsed group. Relative mRNA expression of cili-ary neurotrophic factor was lowest in muscle buried (4 percent of control) (p < 0.05) and avulsed specimens (15 percent of control) (p < 0.05) and higher in folded (52 percent of control) and transected specimens (75 percent of con-trol). Relative mRNA expression of calcitonin gene-related peptide was highest in folded specimens (302 percent of control) (p < 0.05).Conclusions: Folding and transection lead to increased histologic evidence of neuroma formation, whereas folding leads to neuropathic pain, assayed by calci-tonin gene-related peptide expression. Avulsion and muscle burying are prefer-able techniques for nerve ablation and inhibit nerve regeneration, evidenced by decreased ciliary neurotrophic factor expression. Avulsion offers an alternative to muscle burying when there is no muscle in the vicinity to bury the transected nerve. (Plast. Reconstr. Surg. 131: 1004, 2013.)
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
From the Department of Plastic Surgery and the Department of Pathology, Case Western Reserve University.Received for publication July 17, 2012; accepted November 30, 2012.Copyright © 2013 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e3182879ec2
Plastic and Reconstructive Surgery
XXX
xxx
XXX
XXX
XXX
2013
ExpErimEntal

Volume 131, Number 5 • Nerve Ablation for Prevention of Neuroma
1005
depressor supercilii and procerus muscles) are removed for therapeutic or aesthetic reasons. An unanswered question, therefore, is the effect of nerve avulsion or folding on formation of neuromas.
In this study, we investigated the effect of four different techniques of nerve ablation on the inci-dence and degree of neuroma formation. These four methods included nerve avulsion, nerve transection, folding a nerve, and sharply transect-ing a nerve and burying in muscle, which served effectively as the negative control for neuroma formation.
MATERIALS AND METHODSSurgical Procedures
Thirty adult Sprague-Dawley rats were used in this study, with both legs of each animal subjected to different interventions using a sural nerve model. The 60 nerves studied were assigned ran-domly to a different intervention, with experimen-tal groups as follows: group 1, avulsion; group 2, transection; group 3, folding; and group, muscle burying. Control nerves (n = 15) were obtained from both legs of other animals of the same rat species and age, not subjected to any intervention, that were used for microsurgical practice by plas-tic surgery residents, for the purposes of all analy-ses. The study was approved by the Institutional Animal Care and Use Committee of Case Western Reserve University. Animals were anesthetized through induction with intraperitoneal injections of ketamine hydrochloride (100 mg/kg) and xyla-zine (5 mg/kg), and subsequently maintained under inhalational anesthesia for the duration of
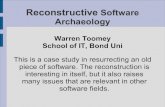
the operation. An incision was made on the dor-sal surface of the leg from the mid thigh to the mid leg. The biceps femoris was divided and the sural nerve exposed (Fig. 1, left). The identity of the nerve was confirmed through proximal dis-section to the trifurcation of the tibial, common peroneal, and sural nerves (Fig. 1, right).
For group 1 (avulsion), a 1-cm segment of nerve was removed through proximal and dis-tal avulsion using a nontraumatic forceps, with care taken not to crush the nerve. The nerve was gripped 2 mm distal to the trifurcation point with a smooth forceps. A second forceps was then used to grip the nerve distal to the point held by the first forceps, and steady moderate traction in a caudal direction was used to avulse the nerve proximally. In a similar fashion, the nerve was avulsed distally using steady moderate traction in a cephalic direc-tion to create a 1-cm nerve gap. For group 2 (tran-section), a 1-cm segment of nerve was removed through sharp transection of proximal and distal nerves. For group 3 (folding), a 1-cm segment of nerve was removed through sharp transection. The proximal nerve stump was then folded onto itself for a length of 5 mm and secured with a single 6-0 Ethilon suture (Ethicon, Norderstedt, Germany). For group 4 (muscle burying), a 1-cm segment of nerve was removed through sharp transection. The proximal nerve stump was then buried in a pocket created in the gastrocnemius muscle and secured with a single 6-0 Ethilon suture. All surgi-cal procedures were performed under an operat-ing microscope by the first author (H.C.), with a uniform 1-cm nerve gap created for all experimen-tal groups. Skin incisions were closed with inter-rupted 5-0 Vicryl (Ethicon) sutures. Animals were
Fig. 1. a rat sural nerve model was used for this study. (Left) Exposure was achieved through a dorsal incision on the leg with splitting of the biceps femoris. (Right) the sural nerve was identified through proximal dissection to the trifurcation of the tibial, common peroneal, and sural nerves.

1006
Plastic and Reconstructive Surgery • May 2013
housed in the animal facility at the Case School of Medicine and had access to unlimited food and water. Postoperative analgesia was achieved with twice-daily injections of buprenorphine (0.01 to 0.05 mg/100 g) for 3 days.
Animals were killed after 3 months, and the entire proximal nerve segment was explanted for analysis. Table 1 summarizes the experimental design.
Experimental MethodsNerves were embedded in paraffin and cut
into 5-μm sections for histologic evaluation (n = 10 from each group), or processed for real-time polymerase chain reaction for amplification of mRNA (n = 5 from each group). Histology stains used included hematoxylin and eosin and Mas-son trichrome. Immunostaining was performed against S-100 to identify phenotypically differenti-ated Schwann cells. Histomorphometric analysis (n = 5 from each group) was performed using a Leica MZ16F stereomicroscope (Leica Microsys-tems, Bannockburn, Ill.) and Leica LAS Image analysis software (Leica Microsystems), with the second author (E.M.) performing the analysis blinded to different experimental groups. Nerve cross-sectional area was analyzed on transverse histologic section, and the ratio of neural to con-nective tissue was calculated within the confines of the epineurium. Sections stained against Masson trichrome were used for analysis. The total area stained blue and red was used to determine nerve cross-sectional area. The ratio of areas stained red (against axons) compared to blue (against collag-enous connective tissue) was used to determine the ratio of neural to connective tissue. Three separate transverse section slides of the widest part of each nerve specimen were analyzed sepa-rately and the mean designated as the value for
each specimen. Histopathologic examination was performed with the aid of a board-certified neu-ropathologist (M.L.C.) in a single-blind fashion to ensure accuracy of analyses. Because the aim of the study was to compare formation of neuromas following different nerve ablation techniques, only basic measures of nerve survival were used in histomorphometric analysis for this experiment.
Real-time polymerase chain reaction was per-formed to assess for expression of ciliary neuro-trophic factor and calcitonin gene-related peptide. Ciliary neurotrophic factor is a neurotrophic fac-tor and supports and maintains normal function of axons, and is expected to be elevated with nerve regeneration.8,9 Calcitonin gene-related peptide is responsible for maintenance of neuropathic pain, and is an assay of mechanical allodynia.10,11 Thus, it is expected to be increased in neuromas. Quantification of mRNA was performed using Roche Sybr Green I Supermix (Roche, Indianap-olis, Ind.) on a Roche Lightcycler480 real-time polymerase chain reaction instrument. Real-time polymerase chain reaction was conducted using 2.5 μl of diluted cDNA per 10-μl assay under the following conditions: denaturation for 10 min-utes at 95°C, amplification for 45 cycles at 95°C for 10 seconds and 62°C for 1 minute, with fluo-rescence measured during the final 95 percent of each 60°C step. Melt curve analysis was performed from 55° to 95°C at 0.5°C every 10 seconds with continuous fluorescence measurement. Expres-sion of ciliary neurotrophic factor and calcitonin gene-related peptide mRNA was normalized to the mRNA levels of glyceraldehyde-3-phosphate dehydrogenase. The relative ratio of mRNA in treatment groups versus controls was determined using methods described by Pfaffl.12 Controls were obtained from sham-operated rats, with no inter-vention performed to the sural nerve.
Table 1. Schematic Diagram of Experimental Design
Sprague-Dawley rats (30 animals)(n = 60 legs)
Group 1 (n = 15)Avulsion
Group 2 (n = 15)Transection
Group 3 (n = 15)Folding
Group 4 (n = 15)Muscle burying
Animals sacrificed after 3 moHistology (n = 10)
RT-PCR (n = 5)Histology (n = 10)
RT-PCR (n = 5)Histology (n = 10)
RT-PCR (n = 5)Histology (n = 10)
RT-PCR (n = 5)RT-PCR, real-time polymerase chain reaction.

Volume 131, Number 5 • Nerve Ablation for Prevention of Neuroma
1007
Statistical AnalysisMultiple linear regression methods using
JMP8 statistical software (SAS Institute, Inc., Cary, N.C.) were used to compare nerve cross-sectional area and neural-to-connective tissue ratio between different experimental groups and controls. Covariates used for nerve cross-sectional area were nerve size and presence of abnormal and invasive connective tissue. Covariates used for neural-to-connective tissue ratio were nerve size, status of degeneration, and shape. Because of the multivari-ate nature of the factor variables for each response, multiple linear regression methods were used to develop models for predicting each response. Only factor variables that were statistically significant (p < 0.05) were included in the models. Factors not included in the models all had values of p > 0.10. The goodness-of-fit for each model was based on a comparison of the square root of the mean square error from the regression analysis, with the pure error estimate from the repeated measurements of the same nerve using an F test (p < 0.05) rather than relying on a test based on the R2 value.
One-way analysis of variance with the Tukey-Kramer multiple comparisons test was performed using the GraphPad InStat version 3.05 for Win-dows 95/NT computer program (GraphPad Soft-ware, Inc., San Diego, Calif.) to compare relative expression of mRNA for ciliary neurotrophic fac-tor and calcitonin gene-related peptide between experimental groups and controls.
RESULTSAll animals survived after surgery and did not
exhibit movement patterns or distress postopera-tively suggestive of neuropathic pain. There were no perioperative or late postoperative complica-tions of surgery. No trophic changes or gait distur-bance was observed following surgery.
Nerve cross-sectional area (Fig. 2, above) was highest in folded (mean, 8.8 ± 2.4 mm2) followed by muscle buried (4.7 ± 0.7 mm2) and transected (4.0 ± 0.4 mm2) specimens. Nerve cross-sectional area in folded, muscle buried, and transected sam-ples was statistically increased (p < 0.05) compared with control (3.1 ± 0.4 mm2) and avulsed (2.2 ± 0.4 mm2) specimens. Increased cross-sectional area of the proximal nerve stump is often indicative of a disordered bundle of overgrown terminal nerve fibers and suggestive of neuroma formation. The neural-to-connective tissue ratio did not show a sta-tistical difference between transected, muscle bur-ied, and folded groups compared with controls. This value was highest for transected (1.2 ± 0.1),
muscle buried (1.2 ± 0.2), and folded nerves (1.2 ± 0.1), followed by control specimens (1.1 ± 0.1). Avulsed specimens (1.0 ± 0.1) had a statistically decreased neural-to-connective tissue compared with control specimens, correlating with decreased abnormal nerve tissue from neuroma formation.
Histologic analysis of specimens in groups 2 and 3 (transection and folding) showed evidence of disordered myelinated fibers with overgrowth of axons and loss of normal neural architecture. In contrast, specimens in groups 1 and 4 (avul-sion and muscle burying) showed preservation of normal fascicular architecture with parallel arrangement of nerve fibers. Representative sec-tions stained with Masson trichrome (Fig. 3) and S-100 are shown in Figure 4.
Relative mRNA expression of ciliary neuro-trophic factor (Fig. 5, above) was lowest in muscle
Fig. 2. Quantitative histomorphometry was used to analyze transverse sections of nerves. nerve cross-sectional area (above) was highest for folded, followed by muscle buried, transected, control, and then avulsed groups. Asterisk indicates that com-parison with the control group showed a statistically significant difference. the neural-to-connective tissue ratio (below) was sta-tistically decreased for avulsed nerves compared with controls, with no significant difference from controls for muscle buried, folded, and transected specimens. T-bars indicate SD.

1008
Plastic and Reconstructive Surgery • May 2013
buried (4 percent of control) (p < 0.05) and avulsed specimens (15 percent of control) (p < 0.05) and higher in folded (52 percent control) and transected specimens (75 percent of control). The relative expression of ciliary neurotrophic factor for muscle buried and avulsed specimens was statistically lower compared with control spec-imens (p < 0.05). No statistical difference was seen between folded and transected specimens and controls. These findings suggested that regen-eration of the proximal nerve stump was strongly inhibited in muscle buried and avulsed groups.
Relative mRNA expression of calcitonin gene-related peptide (Fig. 5, below). was highest in folded specimens (302 percent of control) (p < 0.05), followed by transected (137 percent of control), avulsed (116 percent of control), and muscle bur-ied specimens (24 percent of control). Relative
expression of calcitonin gene-related peptide for folded specimens was statistically higher compared with controls. This suggests that animals in this group experienced a significant degree of neu-ropathic pain. No statistical difference was seen between transected, avulsed, and muscle buried specimens and controls. A summary of results for different groups is presented in Table 2.
DISCUSSIONPrevention of neuroma formation is essen-
tial for achieving an optimal clinical outcome after nerve ablative surgery. Surgical procedures involving nerve ablation have evolved from tran-section of peripheral nerves during extirpative or trauma surgery of the extremities to, more recently, therapeutic interventions for chronic
Fig. 3. representative histologic sections of explanted nerves stained with masson trichrome (original magnification, ×100). (Above, left) Group 1 (avulsion): normal nerve architecture with parallel myelinated fibers is shown. (Above, right) Group 2 (transection): evidence of disordered architecture with chaotic arrangement and overgrowth of axons, demonstrative of neuroma formation. (Below, left) Group 3 (folding): evidence of disordered architecture with chaotic arrangement and over-growth of axons, demonstrative of neuroma formation. (Below, right) Group 4 (muscle burying): normal nerve architecture with maintenance of fascicular structure and parallel arrangement of myelinated fibers is shown.

Volume 131, Number 5 • Nerve Ablation for Prevention of Neuroma
1009
pain13,14 and surgery for treatment of migraine headaches.7,15,16
A favored technique for decreasing the inci-dence of neuroma formation is implantation of the proximal nerve stump into adjacent muscle.17,18 This was described in 198517 and is used widely in clinical practice. Other described techniques19 include cap-ping with a vein graft, transection with lasers, epi-neural sleeves, and end-to-side or end-to-end nerve anastomoses where possible. All of these varied tech-niques have the aim of blocking neurotropic signals from the distal nerve stump or preventing aberrant proximal nerve stump regeneration. Experimental studies have also linked a shorter nerve gap with increased incidence of neuroma formation.20
In our clinical experience with ablation of smaller nerves in the head and neck for migraine surgery, techniques such as muscle burying or vein capping are technically difficult because of the surgical approach. Ablation of the zygomati-cotemporal branch of the trigeminal nerve for
treatment of migraine headaches21 in the practice of the senior author (B.G.) is achieved through an endoscopic brow-lift approach, with all dissection performed under endoscopic visualization. The small caliber of this sensory nerve allows nerve ablation to be most easily performed through either nerve avulsion or transection. An unan-swered question in the literature involves which of these techniques, avulsion or transection, is more efficacious in prevention of neuromas.
The results of this study show that nerve folding, muscle burying, and transection lead to increased nerve cross-sectional area. Histology demonstrates that folding and transection result in increased neu-roma formation. Transection and folding also lead to a very high mRNA expression of ciliary neurotrophic factor, correlated with nerve regeneration. Con-versely, avulsed nerves had a very low cross-sectional area and low ciliary neurotrophic factor mRNA expression. Expression of ciliary neurotrophic factor in Schwann cells of injured nerves is linked to the
Fig. 4. representative histologic sections of explanted nerves stained with S-100 (original magnification, ×100) (neural tissue stains brown). (Above, left) Group 1 (avulsion): normal nerve architecture is preserved. (Above, right) Group 2 (tran-section): evidence of neuroma formation. (Below, left) Group 3 (folding): evidence of neuroma formation. (Below, right) Group 4 (muscle burying): normal nerve architecture with maintenance of fascicular structure is shown.

1010
Plastic and Reconstructive Surgery • May 2013
nerve’s functional state,22 and studies have shown that ciliary neurotrophic factor is down-regulated when the nerve is demyelinated and undergoes Wallerian degeneration.23 Similarly, ciliary neurotrophic factor is up-regulated when nerve fibers regenerate.24 Cili-ary neurotrophic factor is therefore a neurotrophic
factor and supports and maintains normal func-tion of axons, and is expected to be elevated with nerve regeneration. Thus, nerve avulsion appears to abrogate nerve regeneration effectively and reduce neuroma formation. A possible explanation for this could be that avulsion results in interruption of axons at multiple different levels, therefore inhibiting effec-tive nerve regeneration and neuroma formation in a single level. In addition, nerve avulsion results in a more severe injury than transection,25 possibly pre-venting effective nerve regeneration and subsequent neuroma formation.
As the aim of migraine surgery and other inter-ventions aimed at treating neuromas and other sources of chronic pain is to permanently elimi-nate the pain, another important issue is the inci-dence of neuropathic pain with different nerve ablative techniques. Calcitonin gene-related pep-tide has been implicated as one of the neuropep-tides involved in peripheral nerve injury–induced neuropathic pain.26 Injecting calcitonin gene-related peptide into the spinal subarachnoid space was found to reduce pain threshold, whereas injec-tion of calcitonin gene-related peptide antiserum could increase the pain threshold.27,28 Therefore, determining the effect of different techniques of nerve ablation on expression of ciliary neuro-trophic factor and calcitonin gene-related peptide is also important for determining the degree of nerve regeneration and neuropathic pain.
Interestingly, calcitonin gene-related peptide mRNA expression was highest in the folded nerve group. This is consistent with findings from an experimental study where chronic constriction injury was found to result in increased autonomic fiber sprouting from skin, resulting in increased sensitivity of nociceptive fibers to sympathetic and parasympathetic stimulation.29 A similar constric-tive mechanism would explain the increased level of neuropathic pain in rats with folded nerves. Conversely, the level of calcitonin gene-related peptide mRNA expression was lowest in the mus-cle buried group. It is possible that burying the proximal nerve stump in muscle abrogates the inflammatory response to pain, which has been
Fig. 5. (Above) relative mrna expression of ciliary neuro-trophic factor (CNTF) as assessed using quantitative real-time polymerase chain reaction. Asterisks indicate a statistically sig-nificant difference when compared with control specimens. GAPDH, glyceraldehyde-3-phosphate dehydrogenase. (Below) relative mrna expression of calcitonin gene-related peptide (CGRP) as assessed using quantitative real-time polymerase chain reaction. Asterisks indicate a statistically significant differ-ence when compared with control specimens. GAPDH, glyceral-dehyde-3-phosphate dehydrogenase.
Table 2. Summary of Results for Different Nerve Ablation Techniques
Nerve CSA (mm2) N:CTR CNTF mRNA (% of control) CGRP mRNA (% of control)
Avulsion 2.2 ± 0.4 1.0 ± 0.1* 15* 116Transection 4.0 ± 0.4* 1.2 ± 0.1 75 137Folding 8.8 ± 2.4* 1.2 ± 0.1 52 302*Muscle burying 4.7 ± 0.7* 1.2 ± 0.2 4* 24Control 3.1 ± 0.4* 1.1 ± 0.1CSA, cross-sectional area; N:CTR, nerve-to-connective tissue ratio; CNTF, ciliary neurotrophic factor; CGRP, calcitonin gene-related peptide.*Statistically significant difference (p < 0.05) compared with control specimens.

Volume 131, Number 5 • Nerve Ablation for Prevention of Neuroma
1011
implicated in the pathogenesis of neuropathic pain through up-regulation of interleukin-6 and increased calcitonin gene-related peptide release mediated in part by invading macrophages.30 Whether increased calcitonin gene-related pep-tide expression would necessarily correlate with a painful neuroma in humans has not been shown. However, what is clear is that calcitonin gene-related peptide expressing sensory neurons responds to painful stimuli.31
This study is limited by a small sample size and short duration of follow-up. Future studies would aim at a longer duration of follow-up with more detailed neuropathologic histologic analy-ses, analyses of the distal nerve and cell body, and localization of RNA expression.
CONCLUSIONSThis study suggests that avulsion and mus-
cle burying are both efficacious for ablation of peripheral nerves, and we would advocate the use of both techniques clinically. This study also sug-gests that nerve folding leads to neuropathic pain, assayed by calcitonin gene-related peptide expres-sion. Avulsion offers an alternative to muscle bury-ing when there is no muscle in the vicinity to bury the transected nerve.
ACKNOWLEDGMENTSThis research project was supported by a Prentiss
Fund grant. The authors thank Amad Awadallah for help with histologic sections and staining, and also Har-old S. Haller, Ph.D., from the Department of Statistics, Case Western Reserve University, for aid with statistical analyses.
REFERENCES 1. Janes S, Renaut PH, Gordon MK. Traumatic (or amputation)
neuroma. ANZ J Surg. 2004;74:701–702. 2. Zimmerman M. Pathobiology of neuropathic pain. Eur J
Pharmacol. 2001;429:23–37. 3. Dellon AL, Mackinnon SE. Treatment of the painful neu-
roma by neuroma resection and muscle implantation. Plast Reconstr Surg. 1986;77:427–438.
4. Otfinowski J, Pawelec A, Kałuza J. Implantation of peripheral neural stump into muscle and its effect on the development of posttraumatic neuroma. Pol J Pathol. 1994;45:195–202.
5. Herbert TJ, Filan SL. Vein implantation for treatment of painful cutaneous neuromas: A preliminary report. J Hand Surg Br. 1998;23:220–224.
6. Marcol W, Kotulska K, Larysz-Brysz M, et al. Prevention of painful neuromas by oblique transection of peripheral nerves. J Neurosurg. 2006;104:285–289.
7. Guyuron B, Reed D, Kriegler JS, Davis J, Pashmini N, Amini S. A placebo-controlled surgical trial of the treatment of migraine headaches. Plast Reconstr Surg. 2009;124:461–468.
8. Dubový P, Raška O, Klusáková I, Stejskal L, Celakovský P, Haninec P. Ciliary neurotrophic factor promotes motor reinnervation of the musculocutaneous nerve in an experi-mental model of end-to-side neurorrhaphy. BMC Neurosci. 2011;12:58.
9. Leibinger M, Müller A, Andreadaki A, Hauk TG, Kirsch M, Fischer D. Neuroprotective and axon growth-promoting effects following inflammatory stimulation on mature retinal ganglion cells in mice depend on ciliary neurotrophic factor and leukemia inhibitory factor. J Neurosci. 2009;29:14334–14341.
10. Jaggi AS, Singh N. Therapeutic targets for the management of peripheral nerve injury-induced neuropathic pain. CNS Neurol Disord Drug Targets 2011;10:589–609.
11. Michot B, Bourgoin S, Viguier F, Hamon M, Kayser V. Dif-ferential effects of calcitonin gene-related peptide receptor blockade by olcegepant on mechanical allodynia induced by ligation of the infraorbital nerve vs the sciatic nerve in the rat. Pain 2012;153:1939–1948.
12. Pfaffl MW. A new mathematical model for relative quantifi-cation in real-time RT-PCR. Nucleic Acids Res. 2001;29:e45.
13. Ducic I, Mafi AA, Attinger CE, Couch K, Al-Attar A. The role of peripheral nerve surgery in the management of painful chronic wounds: Indications and outcomes. Plast Reconstr Surg. 2008;122:193–197.
14. Ducic I, Larson EE. Posttraumatic headache: Surgical management of supraorbital neuralgia. Plast Reconstr Surg. 2008;121:1943–1948.
15. Guyuron B, Kriegler JS, Davis J, Amini SB. Comprehensive surgical treatment of migraine headaches. Plast Reconstr Surg. 2005;115:1–9.
16. Guyuron B, Kriegler JS, Davis J, Amini SB. Five-year outcome of surgical treatment of migraine headaches. Plast Reconstr Surg. 2011;127:603–608.
17. Mackinnon SE, Dellon AL, Hudson AR, Hunter DA. Altera-tion of neuroma formation by manipulation of its microenvi-ronment. Plast Reconstr Surg. 1985;76:345–353.
18. Dellon AL, Mackinnon SE. Treatment of the painful neu-roma by neuroma resection and muscle implantation. Plast Reconstr Surg. 1986;77:427–438.
19. Yildirim AM, Okur MI, Ozveren F, Ozercan R. Reduction of the incidence of neuroma formation by proximal epineu-ral stripping: An experimental study in rats. J Hand Surg Br. 2006;31:450–452.
20. Sinis N, Haerle M, Becker ST, et al. Neuroma formation in a rat median nerve model: Influence of distal stump and mus-cular coating. Plast Reconstr Surg. 2007;119:960–966.
21. Janis JE, Hatef DA, Thakar H, et al. The zygomaticotemporal branch of the trigeminal nerve: Part II. Anatomical varia-tions. Plast Reconstr Surg. 2010;126:435–442.
22. Ip NY, Yancopoulos GD. The neurotrophins and CNTF: Two families of collaborative neurotrophic factors. Annu Rev Neu-rosci. 1996;19:491–515.
23. Rabinovsky ED, Smith GM, Browder DP, et al. Peripheral nerve injury down-regulates CNTF expression in adult rat sciatic nerves. J Neurosci Res. 1992;31:188–192.
Bahman Guyuron, M.D.Department of Plastic Surgery
Case Western Reserve University29017 Cedar Road
Cleveland, Ohio [email protected]

1012
Plastic and Reconstructive Surgery • May 2013
24. Smith GM, Rabinovsky ED, McManaman JL, et al. Tem-poral and spatial expression of ciliary neurotrophic fac-tor after peripheral nerve injury. Exp Neurol. 1993;121: 239–247.
25. Zachary LS, Dellon AL, Seiler WA IV. Relationship of intra-neural damage in the rat sciatic nerve to the mechanism of injury. J Reconstr Microsurg. 1989;5:137–140.
26. Zhang YQ, Guo N, Peng G, et al. Role of SIP30 in the development and maintenance of peripheral nerve injury-induced neuropathic pain. Pain 2009;146:130–140.
27. Cridland RA, Henry JL. Intrathecal administration of CGRP in the rat attenuates a facilitation of the tail flick reflex induced by either substance P or noxious cutaneous stimula-tion. Neurosci Lett. 1989;102:241–246.
28. Bennett AD, Chastain KM, Hulsebosch CE. Alleviation of mechanical and thermal allodynia by CGRP(8-37) in a rodent model of chronic central pain. Pain 2000;86:163–175.
29. Grelik C, Bennett GJ, Ribeiro-da-Silva A. Autonomic fibre sprouting and changes in nociceptive sensory innervation in the rat lower lip skin following chronic constriction injury. Eur J Neurosci. 2005;21:2475–2487.
30. Ma W, Quirion R. Increased calcitonin gene-related peptide in neuroma and invading macrophages is involved in the up-regulation of interleukin-6 and thermal hyperalgesia in a rat model of mononeuropathy. J Neurochem. 2006;98:180–192.
31. McCoy ES, Taylor-Blake B, Zylka MJ. CGRPα-expressing sen-sory neurons respond to stimuli that evoke sensations of pain and itch. PLoS One 2012;7:e36355.
New Submission Guideline: Level of EvidenceBeginning with submissions made July 1, 2011, and going forward, all manuscripts amenable to Level ofEvidence grading need to indicate the clinical question addressed by the article and the Level of Evidence.The clinical question will be one of three categories: Diagnostic, Therapeutic, or Risk. Please use the ASPSLevels of Evidence and Grading Recommendations: Evidence Rating Scales to grade the level of evidencein your manuscript.
In general, the following types of articles are not gradable for level of evidence:
• Animal studies
• Cadaver studies
• Basic science studies
• Review articles
• Instructional course lectures
• CME courses
• Editorials
• Correspondence
As far as what is or is not ratable, the standard is to exclude basic science, bench work, animal, and cadavericstudies because the information gained from these studies is not something that can be applied directly topatient treatment decisions.
See the article “The Level of Evidence Pyramid: Indicating Levels of Evidence in Plastic and ReconstructiveSurgery Articles,” in the July 2011 issue (Plast Reconstr Surg. 2011;128:311–314), for more information ondetermining the Level of Evidence of your manuscript.
NOTE: While we require authors to provide an initial Level of Evidence grade for their submissions, the finalLOE grade for accepted papers will be determined and assigned by an independent panel of LOE experts,whose determination is final.