EXECUTIVE COMMITTEE MEMBERS - nyp.org Committee Agenda 3... · Funds Flow Funds Flow Structure ......
47
NYP Queens DSRIP Executive Committee Meeting Thursday March 22, 2018 - 3:00p.m. 4:00p.m. 530 W. Conference Room 56-45 Main Street Flushing NY EXECUTIVE COMMITTEE MEMBERS: Maureen Buglino (Chair) - NewYork-Presbyterian Queens Robert Crupi, MD (Co-Chair) - NewYork-Presbyterian Queens Christopher Caulfield - NewYork-Presbyterian Queens Maria D’Urso - NewYork-Presbyterian Queens Mark Greaker - NewYork-Presbyterian Queens John Lavin - Mental Health Provider of Western Queens Daniel Muskin - The Grand Nursing Home Lorraine Orlando - NewYork-Presbyterian Queens Faivish Pewzner - Americare Ashook Ramsaran - PAC Member Michael Tretola - Silvercrest Center for Nursing and Rehabilitation Paul Vitale - Queens Coordinated Care Partners AGENDA: I. Welcome M. Buglino II. Review & Approve Minutes of Previous Meeting – Action Item M. Buglino III. Governance Structure - Action Item M. Buglino IV. Quality Committees • Committee Charters – Action Item M. Buglino V. Funds Flow • Funds Flow Structure – Action Item • Payment #6 – Action Item • EIP DY4 NYPQ PPS Selection – Action Item • AHPP Award – Informational A. Simmons VI. PMO Updates – Informational • New PMO Staff • DY3 Completion & DY4 Kick-Off • Clinical Project Sample Reporting • Performance Improvement Update M. Hay VII. Discussion & Questions M. Buglino VIII. Adjourn
Transcript of EXECUTIVE COMMITTEE MEMBERS - nyp.org Committee Agenda 3... · Funds Flow Funds Flow Structure ......

NYP Queens DSRIP Executive Committee Meeting Thursday March 22, 2018 - 3:00p.m. 4:00p.m.
530 W. Conference Room 56-45 Main Street Flushing NY
EXECUTIVE COMMITTEE MEMBERS:
Maureen Buglino (Chair) - NewYork-Presbyterian Queens Robert Crupi, MD (Co-Chair) - NewYork-Presbyterian Queens Christopher Caulfield - NewYork-Presbyterian Queens Maria D’Urso - NewYork-Presbyterian Queens Mark Greaker - NewYork-Presbyterian Queens John Lavin - Mental Health Provider of Western Queens Daniel Muskin - The Grand Nursing Home Lorraine Orlando - NewYork-Presbyterian Queens Faivish Pewzner - Americare Ashook Ramsaran - PAC Member Michael Tretola - Silvercrest Center for Nursing and Rehabilitation Paul Vitale - Queens Coordinated Care Partners
AGENDA:
I. Welcome M. Buglino
II. Review & Approve Minutes of Previous Meeting – Action Item M. Buglino
III. Governance Structure - Action Item M. Buglino
IV. Quality Committees • Committee Charters – Action Item
M. Buglino
V.
Funds Flow • Funds Flow Structure – Action Item • Payment #6 – Action Item • EIP DY4 NYPQ PPS Selection – Action Item • AHPP Award – Informational
A. Simmons
VI.
PMO Updates – Informational • New PMO Staff • DY3 Completion & DY4 Kick-Off • Clinical Project Sample Reporting • Performance Improvement Update
M. Hay
VII. Discussion & Questions M. Buglino
VIII. Adjourn



Executive CommitteePAC Audit
Compliance
NYP/Q Lead Hospital
Finance
NYP/QBoard of Trustees
Adult Ambulatory (Primary Care,
Chronic Disease & Behavioral Health)
Workforce / Cultural
Competency
Hospital Based (Hospital & Post
Acute)
HIV(Clinical Integration)
Clinical Integration &
Quality
PMO
Pediatric Ambulatory (Primary Care ,
Chronic Disease & Behavioral Health)
NYP/Q PPS: Process Improvement Governing StructureJanuary 2018
NYPQ PPS Executive Committee
NYP Queens PPS Executive Committee MeetingCommittee Charters

1 | P a g e
NewYork-Presbyterian Queens Performing Provider System (NYP/Q PPS) Pediatric Hospital Based Quality Committee Charter
Date: March 2018 - Version 1.0
Lead: Robert Crupi, MD, NYP/Q Co-Lead: Haddi Jabbar, MD, NYP/Q
Purpose Statement
The Committee will serve to prioritize the DSRIP quality metrics based on financial impact and historical performance of the PPS. The committee will work to create action plans and implement process improvement initiatives to meet the quality metric goals of the PPS. The committee will be accountable to the Clinical Integration & Quality (CIQ) committee and will report out progress to ensure strategic alignment. The committee will consist of internal and external providers and will be governed by PPS policies.
Goals and Aims Goal 1 Prioritize quality metrics based on performance data and DSRIP financial impact Goal 2 Utilize action plans to govern process improvement across partner network
Aim 1 Align quality measures with impacted network partner organizations Aim 2 Review clinical barriers, existing initiatives, action items, and timelines for all measures Aim 3 Receive performance reports from the RCE and request action as deemed necessary
Goal 3 Implement process improvement initiatives and act as a resource to partners as needed Deliverables Output 1 Prioritization of quality metrics Output 2 Create performance improvement plans with concrete action steps and accountability owners Output 3 Review financial impact of metrics and monitor progress Output 4 Ensure PPS meets quality metric targets annually Output 5 Work with RCE and PMO to implement process improvement initiatives
Prioritized Metrics Metric 1 Potentially Preventable Readmission (PPR) Metric 2 PDI 14 – Pediatric Asthma Metric 3 PDI 90 – Pediatric Composite
Communication Plan
Ensure provider network engagement for best practice & process implementation to impact change Provide updates to PM as action steps are completed Provide quarterly updates to the Clinical Integration & Quality Committee
Code of Conduct Opinions should be given with recognition of conflicts of interest and organization confidentiality Adequate time should be allocated to member schedules to ensure proper contribution Meeting proxies are discouraged All data shared with the committee is considered confidential and should not be distributed unless approved by the source Presentations from SME's (Subject Matter Experts) are encouraged All concepts presented should focus on the Medicaid and uninsured populations
Meeting Frequency - Monthly or as needed

1 | P a g e
NewYork-Presbyterian Queens Performing Provider System (NYP/Q PPS) Pediatric Ambulatory Quality Committee Charter
Date: March 2018 - Version 1.0
Lead: Robyn Rosenblum, MD, NYP/Q Co-Lead: Maria D’Urso, RN, NYP/Q
Purpose Statement
The Committee will serve to prioritize the DSRIP quality metrics based on financial impact and historical performance of the PPS. The committee will work to create action plans and implement process improvement initiatives to meet the quality metric goals of the PPS. The committee will be accountable to the Clinical Integration & Quality (CIQ) committee and will report out progress to ensure strategic alignment. The committee will consist of internal and external providers and will be governed by PPS policies.
Goals and Aims Goal 1 Prioritize quality metrics based on performance data and DSRIP financial impact Goal 2 Utilize action plans to govern process improvement across partner network
Aim 1 Align quality measures with impacted network partner organizations Aim 2 Review clinical barriers, existing initiatives, action items, and timelines for all measures Aim 3 Receive performance reports from the RCE and request action as deemed necessary
Goal 3 Implement process improvement initiatives and act as a resource to partners as needed Deliverables Output 1 Prioritization of quality metrics Output 2 Create performance improvement plans with concrete action steps and accountability owners Output 3 Review financial impact of metrics and monitor progress Output 4 Ensure PPS meets quality metric targets annually Output 5 Work with RCE and PMO to implement process improvement initiatives
Prioritized Metrics Metric 1 Child Access Primary Care (25 months – 6 years) Metric 2 Child ADHD Medication (Initiation) Metric 3 Child ADHD Medication (Continuation)
Communication Plan
Ensure provider network engagement to implement best practices and processes to impact change Provide updates to PM as action steps are completed Provide quarterly updates to the Clinical Integration & Quality Committee
Code of Conduct Opinions should be given with recognition of conflicts of interest and organization confidentiality Adequate time should be allocated to member schedules to ensure proper contribution Meeting proxies are discouraged All data shared with the committee is considered confidential and should not be distributed unless approved by the source Presentations from SME's (Subject Matter Experts) are encouraged All concepts presented should focus on the Medicaid and uninsured populations
Meeting Frequency - Monthly or as needed

1 | P a g e
NewYork-Presbyterian Queens Performing Provider System (NYP/Q PPS) DSRIP Hospital & Post-Acute Quality Committee Charter
Date: March 2018 - Version 1.0
Lead: Robert Crupi, MD, NYP/Q Co-Lead: Haddi Jabbar, MD, NYP/Q
Purpose Statement
The Committee will serve to prioritize the DSRIP quality metrics based on financial impact and historical performance of the PPS. The committee will work to create action plans and implement process improvement initiatives to meet the quality metric goals of the PPS. The committee will be accountable to the Clinical Integration & Quality (CIQ) committee and will report out progress to ensure strategic alignment. The committee will consist of internal and external providers and will be governed by PPS policies.
Goals and Aims Goal 1 Prioritize quality metrics based on performance data and DSRIP financial impact Goal 2 Utilize action plans to govern process improvement across partner network
Aim 1 Align quality measures with impacted network partner organizations Aim 2 Review clinical barriers, existing initiatives, action items, and timelines for all measures Aim 3 Receive performance reports from the RCE and request action as deemed necessary
Goal 3 Implement process improvement initiatives and act as a resource to partners as needed Deliverables Output 1 Prioritization of quality metrics Output 2 Create performance improvement plans with concrete action steps and accountability owners Output 3 Review financial impact of metrics and monitor progress Output 4 Ensure PPS meets quality metric targets annually Output 5 Work with RCE and PMO to implement process improvement initiatives
Prioritized Metrics Metric 1 Potentially Preventable Readmission (PPR) Metric 2 PDI 14 – Pediatric Asthma Metric 3 PDI 90 – Pediatric Composite
Communication Plan
Provide updates to PM as action steps are completed Provide quarterly updates to the Clinical Integration & Quality Committee
Code of Conduct Opinions should be given with recognition of conflicts of interest and organization confidentiality Adequate time should be allocated to member schedules to ensure proper contribution Meeting proxies are discouraged All data shared with the committee is considered confidential and should not be distributed unless approved by the source Presentations from SME's (Subject Matter Experts) are encouraged All concepts presented should focus on the Medicaid and uninsured populations
Meeting Frequency - Monthly or as needed

1 | P a g e
NewYork-Presbyterian Queens Performing Provider System (NYP/Q PPS) Adult Ambulatory Quality Committee Charter
Date: March 2018 - Version 1.0
Lead: Blanca Sckell, MD, NYPQ Co-Lead: Peggy Cartmell, RN, NYPQ
Purpose Statement
The Committee will serve to prioritize the DSRIP quality metrics based on financial impact and historical performance of the PPS. The committee will work to create action plans and implement process improvement initiatives to meet the quality metric goals of the PPS. The committee will be accountable to the Clinical Integration & Quality (CIQ) committee and will report out progress to ensure strategic alignment. The committee will consist of internal and external providers and will be governed by PPS policies.
Goals and Aims Goal 1 Prioritize quality metrics based on performance data and DSRIP financial impact Goal 2 Utilize action plans to govern process improvement across partner network
Aim 1 Align quality measures with impacted network partner organizations Aim 2 Review clinical barriers, existing initiatives, action items, and timelines for all measures Aim 3 Receive performance reports from the RCE and request action as deemed necessary
Goal 3 Implement process improvement initiatives and act as a resource to partners as needed Deliverables Output 1 Prioritization of quality metrics Output 2 Create performance improvement plans with concrete action steps and accountability owners Output 3 Review financial impact of metrics and monitor progress Output 4 Ensure PPS meets quality metric targets annually Output 5 Work with RCE and PMO to implement process improvement initiatives
Prioritized Metrics Metric 1 Adult Access Primary Care (20-44, 45-64, 65+) Metric 2 Diabetes Monitoring – Diabetes & Schizophrenia
Communication Plan
Ensure active engagement of network partners for implementation of best practices & processes Provide updates to Project Manager as action steps are completed Provide quarterly updates to the Clinical Integration & Quality Committee
Code of Conduct Opinions should be given with recognition of conflicts of interest and organization confidentiality Adequate time should be allocated to member schedules to ensure proper contribution Meeting proxies are discouraged All data shared with the committee is considered confidential and should not be distributed unless approved by the source Presentations from SME's (Subject Matter Experts) are encouraged All concepts presented should focus on the Medicaid and uninsured populations
Meeting Frequency - Monthly or as needed
PPS Funds Flow Methodology - UpdateNewYork-Presbyterian Queens DSRIP PPS
Quality Based Funds Flow

PPS Funds Flow Methodology – Move to Quality
DISTRIBUTION: Incentives – Pay for Performance
Quality Metric Performance Project Milestone Completion
DISTRIBUTION: Incentives – Pay for Reporting
CBO Revenue Loss Project Integration Contracts Engaged Patients Quality Metric
Reporting
EXPENSE: Fixed Cost
Admin Overhead Cost of Implementation Workforce
INCOME: PPS Performance Revenue
DSRIP EIP EPP HPP AHPP1
2
3
4
2

Changes from previous funds flow method:
Removal of Non-Covered Services funding
Removal of Contingency funding
Addition of Quality Pay-for-Reporting funding
Addition of Project Integration Contracts
Addition of Quality Pay-for-Performance funding
PPS Funds Flow Methodology – Move to Quality
3

PPS Funds Flow Methodology – Move to Quality
CBO –5%
Rev Loss – 5%
AOH –20%
COI –30%
Fixed Expenses –• Goals of Spend % (DSRIP
Initial Application)
• Actual Spend for COI & AOH
• Non-Safety Net Compliance – 5%
• Revenue Loss – Hospital Based with Partner Potential Upon Request & Approval
40% Income Remaining -Incentives
4

DY3 DY4 DY5
Project RequirementsAll projects except 4.c.ii which is
100% 50% 25% 10%
Patient Engagement All projects except 4.c.ii which is 0% 50% 15% 10%
Quality Pay-for-Reporting All projects except 4.c.ii which is 0% 0% 10% 10%
Quality Pay-for-Performance All projects except 4.c.ii which is 0% 0% 50% 70%
PPS Funds Flow Methodology – Move to QualityIncentive Allocation by DY
40% Income Remaining -Incentives
5

Contingency Fund Allocation Plan
6

Changes from previous funds flow method:
Requested Action: Approve changes to funds flow methodology to move to quality based incentive model as of Payment #7 (September 2018)
Requested Action: Approve of Contingency Fund Allocation Plan to stop allocation as of Payment #6 and redistribute as of Payment #7 (September 2018) balance totaling $488,729.30
PPS Funds Flow Methodology – Move to QualityACTION ITEMS
7

NYP Queens Executive CommitteePayment No. 6: Review and Submission for Approval

Approve Payment No. 6 Partner Distributions – ACTION ITEM
NewYork-Presbyterian Queens PPS is seeking approval for the allocation and release of the below outlined funds for our upcoming Payment #6
Total disbursement of Payment #6 will be: $1,979,843.75
- Slides 3 – 5 breakdown each partner’s total allotment by category
- Slides 6 – 11 detail the partners being funded in this cycle and the projects they are assigned to
- (2) Available RHIO allotments remain totaling $5,000.00 and are inclusive of the above total distribution. Contract documentation is pending; funds will be released once they are obtained.
NYPQ PPS Executive Committee 2

NYPQ PPS - Payment No. 6 (1 of 3) Overall Partner PayoutPYMT # 6
Partner Name Incentives Project Requirements Revenue Loss Grand TotalAdvanced Pediatrics, P.C. 56,916.42$ 56,916.42$ AIDS Center of Queens County, Inc. 21,392.44$ 21,392.44$ Alpine Home Health Care 2,500.00$ 2,500.00$ American Lung Association of the Northeast, Inc. 29,068.20$ 29,068.20$ Americare Certified Special Services, Inc. 34,062.62$ 34,062.62$ Archcare 2,500.00$ 2,500.00$ Brightpoint Health 56,189.87$ 56,189.87$ Caring Hands Pediatrics, P.C. 3,585.79$ 3,585.79$ Carlos A. Ortiz, MD, P.C. 3,504.28$ 3,504.28$ Chapin Home for the Aging 3,665.33$ 36,777.54$ 40,442.86$ Cliffside Rehabilitation and Residential Healthcare Center 4,571.01$ 36,777.54$ 41,348.55$ Community Healthcare Network 34,967.36$ 34,967.36$ Cypress Garden Center for Nursing & Rehabilitation 18,283.75$ 18,283.75$ Dry Harbor Nursing Home 6,701.37$ 36,777.54$ 43,478.91$ Elmcor Youth & Adult Activities, Inc. 29,068.20$ 29,068.20$ Elmhurst Care Center 2,321.14$ 36,777.54$ 39,098.68$ Fairview Nursing Care Center 1,953.91$ 36,777.54$ 38,731.45$ Forest Hills Care Center 18,283.75$ 18,283.75$ Forest View Center for Rehabilitation and Nursing 4,050.38$ 36,777.54$ 40,827.91$
NYPQ PPS Executive Committee 3

Partner Name Incentives Project Requirements Revenue Loss Grand TotalHighland Medical Care 5,462.58$ 5,462.58$ Highland Rehabilitation & Nursing Care Center 2,198.15$ 36,777.54$ 38,975.69$ Holliswood Center for Rehabilitation and Healthcare 1,657.96$ 36,777.54$ 38,435.50$ I.M. Pediatrics, P.C. 2,500.00$ 2,500.00$ Jose E. Quiwa, MD 736.15$ 736.15$ Long Island Care Center, Inc. 7,815.66$ 36,777.54$ 44,593.19$ Margaret Tietz Nursing and Rehabilitation Center 4,155.55$ 36,777.54$ 40,933.08$ Meadow Park Rehabilitation & Healthcare Center 4,118.17$ 36,777.54$ 40,895.71$ Metropolitan Jewish Home Care 8,793.57$ 8,793.57$ New Franklin Center for Rehabilitation and Nursing 19,177.13$ 36,777.54$ 55,954.67$ New York Center for Rehabilitation & Nursing 36,777.54$ 36,777.54$ NYPQ 137,543.75$ 134,305.06$ 271,848.81$ NYPQ - ACC 77,793.65$ 77,793.65$ NYPQ - Jackson Heights 42,780.38$ 42,780.38$ NYPQ - Pediatric Asthma Center 16,570.60$ 16,570.60$ NYPQ - Theresa Lang 15,899.88$ 15,899.88$
NYPQ PPS - Payment No. 6 (2 of 3) Overall Partner Payout
NYPQ PPS Executive Committee 4

Partner Name Incentives Project Requirements Revenue Loss Grand TotalOzanam Hall of Queens Nursing Home 2,215.97$ 36,777.54$ 38,993.51$ Parker Jewish Institute for Health Care and Rehabilitation 48,462.85$ 36,777.54$ 85,240.39$ Queens Boulevard Extended Care Facility 11,095.94$ 36,777.54$ 47,873.47$ Queens Coordinated Care Partners, LLC 29,068.20$ 29,068.20$ Rego Park Health Care 18,283.75$ 18,283.75$ Rego Park Medical Associates 31,601.13$ 31,601.13$ Rest Medical Care, P.C. 2,500.00$ 2,500.00$ Revival Home Health Care 10,194.37$ 10,194.37$ RiteCare Medical Office, P.C. 1,274.60$ 1,274.60$ Sapphire Center for Rehabilitation and Nursing of Central Queens 1,048.23$ 36,777.54$ 37,825.77$ St. Mary's Healthcare System for Children 10,789.31$ 10,789.31$ Sunharbor Manor 436.76$ 36,777.54$ 37,214.30$ The Grand Rehabilitation and Nursing at Queens 2,930.87$ 36,777.54$ 39,708.41$ The Pavilion at Queens 9,074.23$ 36,777.54$ 45,851.76$ The Silvercrest Center for Nursing and Rehabilitation 11,235.00$ 36,777.54$ 48,012.54$ Union Plaza Care Center 15,285.38$ 36,777.54$ 52,062.92$ Visiting Nurse Service of New York Home Care 63,740.91$ 63,740.91$ Waterview Nursing & Rehabilitation Center 2,722.27$ 36,777.54$ 39,499.81$ Woodcrest Rehabilitation & Residential Health Care 5,129.02$ 36,777.54$ 41,906.56$ Available RHIO Allotment 5,000.00$ 5,000.00$ Grand Total 908,026.55$ 937,512.14$ 134,305.06$ 1,979,843.75$
NYPQ PPS - Payment No. 6 (3 of 3) Overall Partner Payout
NYPQ PPS Executive Committee 5

NYPQ PPS - Payment No. 6 – Project 2.a.ii Summary
NYPQ PPS Executive Committee 6

NYPQ PPS Executive Committee
NYPQ PPS - Payment No. 6 – Project 2.b.v Summary
7
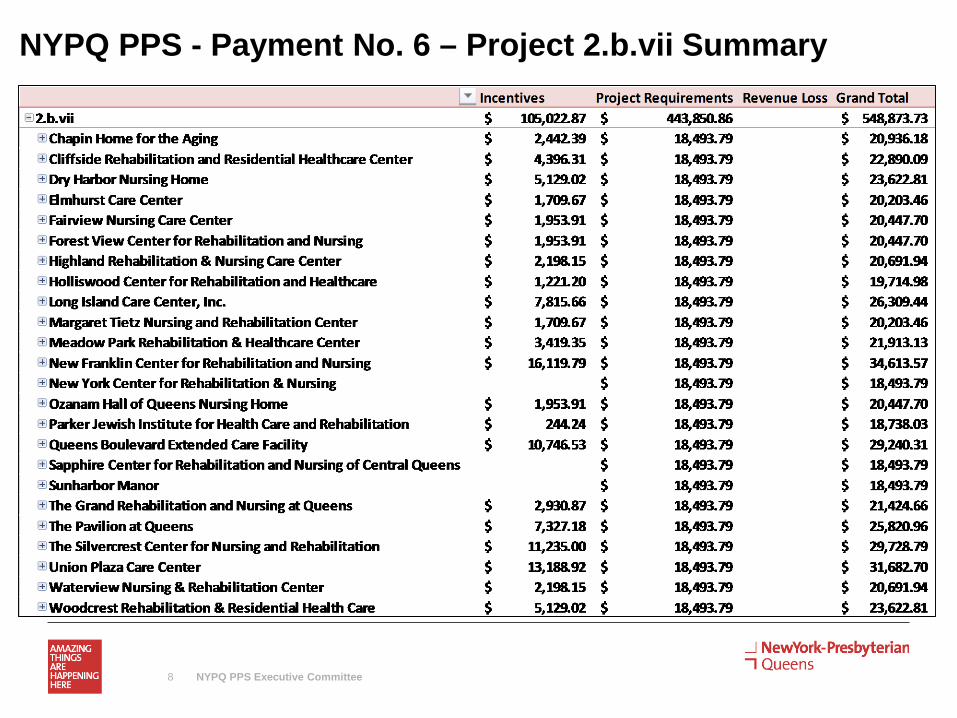
NYPQ PPS - Payment No. 6 – Project 2.b.vii Summary
NYPQ PPS Executive Committee 8

NYPQ PPS - Payment No. 6 – Project 2.b.viii, 3.a.i, 3.b.i, 3.d.ii Summary
NYPQ PPS Executive Committee 9

NYPQ PPS - Payment No. 6 – Project 3.g.ii Summary
NYPQ PPS Executive Committee 10

NYPQ PPS - Payment No. 6 – CBO, HIV, RHIO Summary
NYPQ PPS Executive Committee 11

NewYork-Presbyterian/Queens PPS
NYP/Q PPS
PPS #40
DY4 EIP activity selections Memo
Overview of the DY3 and DY4 activity changes
This memo explains the NYP/Q PPS EIP activities selection changes from DY3 to DY4. During DY3, the PPS selected the following activities:
1. Health Home – Contract with HH to coordinate enrollment activities utilizing the ED Navigator connection
2. RHIO Connection – Payment to partners for RHIO connectivity 3. MAX – Process improvement effort 4. HIV – Participation in statewide initiatives for HIV
For the DY4 EIP activities, the PPS has selected three of the previous four measures with the addition of one new measure. The specific activity that was removed is the RHIO initiative focused on assisting partners with funding for connectivity. The new activity that the PPS selected for DY4 is participation in a state recognized smoking cessation program. The following is a list of the DY4 activities:
1. MAX – Continue utilizing our Hospital Potentially Preventable Readmission (PPR) efforts & align with process improvement committees to
2. HIV – Continue participation in NYSDOH HIV meetings & planning 3. Health Home – Continue participation in a health home referral program with a focus on
reporting and improved patient outcomes. 4. State Recognized Tobacco Cessation Program - Participation in a state recognized
tobacco cessation program

PPS Name: NewYork Presbyterian/Queens
Selected EIP Activities for DY4 (4/1/18-3/31/19)
_____ IT TOM Initiatives
___X__ MAX Series Projects
___X__ Expanded Health Home (“HH”) enrollment
_____ Electronic Health Record (“EHR”) investment
____ Capital spending on primary/behavioral health integration
__X___ DOH-recognized tobacco cessation program *New to DY4
__X__ DOH and/or NYS efforts to end HIV/AIDS
____ Fraud deterrence and other surveillance activities
_____ Infrastructure spending related to SHIN-NY/RHIO Reporting and payment frequency will be semi-annual.
{Payer Name}
______________________________ By ______________________________ Print Name
______________________________ Title
NewYork Presbyterian/Queens
______________________________ By ______________________________ Print Name ______________________________ Title
______________________________ ______________________________ Date Date

Dear New York Presbyterian Hospital of Queens,
Additional High Performance Program Funds: Year 2
The Independent Assessor (IA) is providing The New York Presbyterian Hospital of Queens with a summary of funds earned based on performance in the Additional High Performance Program (AHPP) for Measurement Year 2. AHPP was created to further incentivize Performing Provider Systems (PPS) participating in the Delivery System Reform Incentive Payment (DSRIP) Program to maximize their achievement of selected key measures as part of the federally funded DSRIP High Performance Fund (HPF). For more detail please consult the guidance document found on the DSRIP website. AHPP award amounts were calculated based on the distribution of attributed lives for each of the PPS participating in DSRIP. Base award amounts will remain constant throughout the length of the program. Within a given year, unearned AHPP awards are redistributed and added to the base award amounts for PPS that met the AHPP performance requirements in a weighted manner based upon the distribution of DSRIP lives associated with the PPS. As a reminder, a PPS achieving less than 50% of the qualifying AHPP measures will not receive an AHPP award payment in a measurement year. If a PPS achieves at least 50% of their measures, the PPS will earn 100% of their allocated AHPP funding, as well as any additional funds that were made available from PPS that did not achieve 50% of the AHPP measures in that year. Measures with a denominator below thirty during this measurement year or the previous measurement year will be considered invalid. The following table provides a summary of The New York Presbyterian Hospital of Queens AHPP performance and funds earned in Demonstration Year 2:
Measure Achievement
Antidepressant Medication Management- Effective Acute Phase Treatment
Antidepressant Medication Management- Effective Continuation Phase Treatment
Cardiovascular Monitoring for People with Diabetes and Schizophrenia Low Denom. Diabetes Monitoring for People with Diabetes and Schizophrenia Follow-up after hospitalization for Mental Illness- within 30 days Follow-up after hospitalization for Mental Illness- within 7 days Potentially Avoidable Emergency Department Visits (PPV) (All Population) Potentially Avoidable Readmissions (PPR) (All Population) Potentially Preventable Emergency Department Visits (for persons with BH diagnosis) +/-
Percentage of Measures Achieved 50% Base Award Amount Earned $284,535 Additional AHPP Funds Earned $925,408
Total AHPP Funds Earned $1,209,943

For questions or comments regarding payment please contact your paired MCO. Questions or comments regarding the AHPP Award amounts can be addressed to the Supplemental Team at: [email protected]. For a breakdown of the measure results please refer to Report 11 on the Digital Library. Thank you, The DSRIP IA Team

NYP Queens PPS Executive Committee Meeting
NYPQ PPS Executive Committee Meeting
PMO Updates
PMO Updates 2018
DY3 Q4 Completion & DY4 Kick-off On March 31,2018 DSRIP Year 1 will end. Along with the ending of the DSRIP year, the pay for
performance phase of the program will also end.
In order to meet the remaining deliverables that are required to receive funding under the pay for reporting phase, our PMO will report on milestones for the following projects;
2.a.ii - PCMH b.viii - Hospital- Home Care 3. a.i - Primary Care and Behavioral 3. b.i - Cardio 3. d.ii - Asthma 3. g.ii - Palliative
DY4 Q1 begins on April 1,2018 and will kick-off the pay for performance phase of DSRIP
NYPQ PPS Executive Committee Meeting
PMO UpdatesStaffing
PPS PMO has recruited and filled the following positons;• New Team Members/Roles:
o 1 Nurse Practitioner - Palliative Care and Readmission initiatives
o 1 Care Coordinator – Palliative and Ambulatory
o 2 Patient Navigators - Hospital/Ambulatory and Post-Acute Care
PMO will adapt existing roles in order to support:• Improved quality measures
• Population Health Management
• Process Improvement and Rapid Cycle initiatives
NYPQ PPS Executive Committee Meeting

NYP Queens PPS Executive Committee Meeting
NYPQ PPS Executive Committee Meeting
Clinical Projects Reporting Sample

DY3 Q4 Reporting 2.a.ii (PCMH) - Sample
NYPQ PPS Executive Committee Meeting
PCMH- Deliverables Milestone #4 Ensure all PPS safety net providers are actively sharing EHR systems with
local health information exchange/RHIO/SHIN-NY and sharing health information among
clinical partners, including direct exchange (secure messaging), alerts and patient record look
up by the end of Demonstration Year(DY)3. (DY3 Q4)
Milestone #5 Ensure that EHR systems used by participating safety net providers meet
Meaningful Use and PCMH Level 3 standards and/or APCM by the end of Demonstration
Year 3. (DY3 Q4)

DY3 Q4 Reporting 2.b.vii - Sample
Hospital- Home Care – Deliverables
Milestone #1 Assemble Rapid Response Teams (hospital/home care) to facilitate patient discharge to home and assure needed home care services are in place, including, if appropriate, hospital. DY3 Q4)
Milestone #8 Integrate primary care, behavioral health, pharmacy, and other services into the model in order to enhance coordination of care and medication management DY3 Q4)
Milestone #10 Utilize interoperable EHR to enhance communication and avoid medication errors and/or duplicative services. DY3 Q4)
NYPQ PPS Executive Committee Meeting

DY3 Q4 – Reporting 3.a.i (PCBH)- Sample
NYPQ PPS Executive Committee Meeting
3. a.i - Primary Care and Behavioral Deliverables
Milestone #1 Co-locate behavioral health services at primary care practice sites.
Milestone #3 Conduct preventive care screenings, including behavioral health screenings (PHQ-2
or 9 for those screening positive, SBIRT) implemented for all patients to identify unmet needs.
Milestone #5 Co-locate primary care services at behavioral health sites.
Milestone #7 Conduct preventive care screenings, including behavioral health screenings (PHQ-2
or 9 for those screening positive, SBIRT) implemented for all patients to identify unmet needs.

1
DSRIP PPS Quality Committee Overview
DSRIP (Delivery System Reform Incentive Payment Program) is a NYS Medicaid initiative focused to reducing potentially preventable hospital utilization by 25% and improving the quality of care for patients utilizing networks of clinical and non-clinical community based organizations. The program began in April 2015 and concludes in March 2020 with aggressive goals to move the Medicaid system to value based payment methodologies. The program began with clinical integration of projects utilizing a committee structure developed to achieve project milestones for funding. As the program moves from pay for reporting to pay for performance the PPS is adapting the governing structure to align focus to quality performance improvement to maximize funding to the network. The network is accountable for improvements to over 70 quality metrics by the conclusion of DSRIP and for partnering with network providers to build financially sustainable models to adapt to VBP reform.
The refinement of the governing committee is crucial to the successful improvements of quality for hospital based and ambulatory activity. The quality structure will be inclusive of network partners and will align with lead hospital quality improvement efforts. Even though this process improvement strategy is lead through a Medicaid incentive program the committees will focus actions to ensure improvements for all payers and avoid payer specific clinical operations.
The PPS Project Management Office (PMO) and committee leads will work to prioritize quality metrics and design meetings to maximize return of efforts and ensure effective member engagement.
NYP/Q PPS: Process Improvement Governing StructureJanuary 2018
NYPQ PPS Executive Committee Meeting

2
Adult Ambulatory (Primary Care,
Chronic Disease & Behavioral
Health)
Hospital Based (Hospital & Post Acute)
HIV
Leads:• Dr. B. Sckell• Peggy Cartmell, RN
Leads:• Dr .G. Turett• Karen Francois, RN
Leads:• Dr. R. Crupi• Dr. H. Jabbar
NYP/Q PPS: Process Improvement Governing StructureJanuary 2018
Pediatric Ambulatory
Based (Primary Care, Chronic
Disease & Behavioral
Health
Leads:• Dr. R. Rosenblum• Maria D’Urso, RN
PMO Support: (per committee)
Project ManagerData Analyst Financial Analyst
DSRIP Sponsor:• Amanda Simmons
DSRIP Sponsor:• Sarah Schauman
DSRIP Sponsor:• Sarah Schauman
DSRIP Sponsor:• Amanda Simmons
Committee Goals:
• Prioritize quality metrics for targeted process improvement
• Discuss & develop action items for prioritized quality metrics based on evidence based medicine / Best Practices
• Monitor progress of Action Plans
• Utilize PMO staff to communicate change to the PPS network and to ensure strong communication of improvements
• Partner with other hospital or PPS improvement initiatives to ensure alignment & effectiveness of Action Plans
DSRIP Executive Lead: Maureen BuglinoDSRIP PMO Director: Marlon Hay
NYPQ PPS Executive Committee Meeting

3
DSRIP Executive Lead: Attend meetings as requested by Committee leads Align performance improvement strategies with other hospital initiatives Communicate progress to Executive Leadership
DSRIP PMO Director: Oversee Process Improvement Committee structure and ensure efficient and effective meetings Manages the PMO staff to ensure proper support to committee members Communicate progress to leadership
Committee Lead & Co-Lead: Serve as lead of committee to engage members in process improvement action planning Set the quality metric priority for the committee based on available data from analysts and insights from project managers Ensure process improvement is progressing to achieve metric goals Align metric priority with ongoing performance improvement initiatives when possible Provide updates to Executive leadership regarding DSRIP performance improvements Become a clinical or subject matter expertise to lead performance improvement efforts
Committee Members: Attend committee meetings Brainstorm with committee to identify best practice standards for performance improvement metrics Participate in performance improvement initiatives for committee Understand ongoing performance improvement processes at site that may align with committee and DSRIP agenda Implement process improvement at site based on decisions from the committee meetings Communicate process improvement efforts and/or action item expectations to PPS network partners
NYP/Q PPS: Process Improvement Governing StructureJanuary 2018
Roles & Responsibilities
NYPQ PPS Executive Committee Meeting

4
NYP/Q PPS: Process Improvement Governing StructureJanuary 2018
Roles & Responsibilities
DSRIP Sponsor: Provide DSRIP subject matter expertise Provide additional resources for best practice utilization or national trends for improvement efforts or reform Provide Executive leadership updates at additional meetings such as the Executive Committee meeting
Project Manager:• Manage scheduling, attendance, minutes, and administrative functions of meetings• Establish and maintain Project Management tools for progress tracking inclusive of timelines • Partner with meeting attendees to work on site specific process improvement• Meet with committee chair(s) before each meeting to prep the chair(s) and set the metric priority and agenda• Monitor risks to DSRIP projects or metric achievement with data analyst• Partner with the Data Analyst to create quality metric reports for meeting presentations or member communications• Ensure continued reporting and achievement of project deliverables and bring risks to chair(s) for committee discussion• Update PPS website with performance improvement efforts & progress
Data Analyst:• Create a standard reporting package based on available data• Run analytics to present at prep meeting to committee chair(s) and project manager to help guide decisions on metric priorities based on
data• Monitor impact of process improvement on measures• Monitor project speed & scale and bring risks to project manager & chair(s) for committee discussion
Financial Analyst:• Provide financial impact of measure achievement to assist chair(s) with setting priorities for committee (actual and/or forecast) • Partner with the Data Analyst to provide support for analytics and / or project management data tracking
NYPQ PPS Executive Committee Meeting

5
NYP/Q PPS: Process Improvement Governing StructureJanuary 2018
PPS Metrics by Committee (All Metrics)
Hospital Based
• PPV• PPR• PPV (BH)• PQI 90• PDI90• PQI 7• PQI 8• PQI 15• PCOS
Adult Ambulatory
• CAHPS • Access to Care• Care Coordination• Antidepressant Med
Management• Monitoring for
Diabetes & Schizophrenia
• Monitoring for Cardio & Schizophrenia
Pediatric Ambulatory
• Access to Care• Asthma Med
Management• ADHD Medication
Metrics included below are a representation of all metrics and do not reflect prioritization of process improvement efforts. The prioritization will occur quarterly and committee efforts will focus to single or similar metrics at a time
NYPQ PPS Executive Committee Meeting

6
Align resources and processes with prioritized quality metrics to ensure direct impact to the PPS provider network and patient base in order to maximize our
investment. This will be done in partnership with the NYP/Q QA team understanding the uniqueness of each quality data set which has very little overlap
but the ability to influence outcomes within the facility and system.
Quality Metrics
Provider Network & Data
Financial Impact
Quality Performance
Clinical & Operational Improvements
Incentives
NYP/Q PPS: Process Improvement Governing StructureJanuary 2018
Quality Process Improvement Technique
NYPQ PPS Executive Committee Meeting

7
Team Tools
Technique Time Zones
NYP/Q PPS: Process Improvement Governing StructureJanuary 2018
Quality Process Improvement Technique
1. Review Metric
2. Define Problem
3. Outline Gaps in Care /
Process / Tools
4. Identify PI by
Provider
5. Define Acton Plan
6. Follow-Up &
Account-ability Owner
NYPQ PPS Executive Committee Meeting

NYPQ PPS Executive Committee Meeting
Questions/Open Discussion
8