Excimer, Ho:YAG, and Q-switched Ho:YAG ablation of aorta: a comparison of temperatures and tissue...
9
Excimer, Ho:YAG, and Q-switched Ho:YAG ablation of aorta: a comparison of temperatures and tissue damage in vitro E. Duco Jansen, Tuong H. Le, and Ashley J. Welch The adjacent thermal and mechanical tissue damage after normal-mode Ho:YAG (pulse length = 250 us, X = 2.09 m), Q-switched Ho:YAG (pulse length = 200 ns, = 2.09 m), and excimer (pulse length = 120 ns, = 308 nm) pulsed laser irradiation of human thoracic aorta samples was studied in vitro. Surface temperatures were monitored during laser irradiation with an IR camera in air or a thermocouple in saline. Histological analysis of the irradiated sites was performed to assess thermal and mechanical damage to tissue surrounding the crater. The ablation of aortic tissue with any of the lasers resulted in a temperature buildup inside the tissue; this effect was most significant for the IR wavelength. Mechanical damage was observed in all cases but was most pronounced for the Q-switched Ho:YAG laser. Excimer ablation in air left behind a smooth surface; however, under saline the result was a much rougher surface. Key words: Pulsed laser, temperature, tissue, thermal damage, mechanical damage. Introduction Recently there has been a shift from cw lasers, such as argon and Nd:YAG, to pulsed lasers for precise tissue ablation. At present several types of pulsed laser are being used. In recent years research and prototype systems have focused on angioplasty'l and ophthalmology, 4 ' 5 but the use of pulsed lasers is also being explored for other disciplines such as dentistry, urology, and orthopedic surgery.- 8 The two main types of pulsed laser of interest are the excimer lasers in the UY region of the spectrum (190-400 nm) and the mid-IR lasers from 1.5 to 3.0 ,um. In particular, the holmium laser (X= 2.09 ,um) may be an alterna- tive to the XeCl excimer laser ( = 308 nm) for the ablation of superficial tissue layers with limited ther- mal injury to the adjacent tissue. 9 "1 0 Interestingly enough, although the chromophores for the two-wavelength regions are different, for every wavelength penetration depth in the V there is at least one IR wavelength that has the same penetration depth. The 1/e penetration depth of Ho:YAG-laser irradiation (300 [um) in aorta is 6 times larger than the penetration depth of the XeCl The authors are with the Biomedical Engineering Program, University of Texas at Austin, Austin, Texas 78712. Received 27 December 1991. 0003-6935/93/040526-09$05.00/0. e 1993 Optical Society of America. excimer laser in the same tissue (50 ,m)."1 Although the use of excimer lasers has been quite success- ful," 3 " 2 the fact that solid-state IR lasers are less expensive and easier to maintain has resulted in considerable pressure to accept IR lasers for the ablation task. In addition, for UV wavelengths (espe- cially those below 300 nm) there is concern that they may be mutagenic.1 3 "1 4 However, the IR wavelength causes larger dissections in the tissue.' 5 These fin- gerlike dissections are presumably caused by the vaporization of water just below the tissue surface, which causes a buildup of pressure and the subse- quent eruption of steam and tissue fragments. 5 - 7 Because the chromophores are different for UV than for IR laser irradiation, it is suggested that the mechanism of ablation may be different between the two cases. Thermal damage can be modeled as a reaction rate-of-formation process. 8 " 9 It has been shown that thermal damage in skin induced in vivo can be described by an Arrhenius reaction-rate function expressed as an integral of the form [C (0)] i In C(t) = Q(r, z, t) = JA exp[-E/RT(r, z, t)]dt' (1) where C(0) is the initial concentration of a molecule 526 APPLIED OPTICS / Vol. 32, No. 4 / 1 February 1993
Transcript of Excimer, Ho:YAG, and Q-switched Ho:YAG ablation of aorta: a comparison of temperatures and tissue...

Excimer, Ho:YAG, and Q-switched Ho:YAGablation of aorta: a comparison of temperaturesand tissue damage in vitro
E. Duco Jansen, Tuong H. Le, and Ashley J. Welch
The adjacent thermal and mechanical tissue damage after normal-mode Ho:YAG (pulse length = 250 us,X = 2.09 m), Q-switched Ho:YAG (pulse length = 200 ns, = 2.09 m), and excimer (pulse length = 120ns, = 308 nm) pulsed laser irradiation of human thoracic aorta samples was studied in vitro. Surfacetemperatures were monitored during laser irradiation with an IR camera in air or a thermocouple insaline. Histological analysis of the irradiated sites was performed to assess thermal and mechanicaldamage to tissue surrounding the crater. The ablation of aortic tissue with any of the lasers resulted in atemperature buildup inside the tissue; this effect was most significant for the IR wavelength.Mechanical damage was observed in all cases but was most pronounced for the Q-switched Ho:YAGlaser. Excimer ablation in air left behind a smooth surface; however, under saline the result was a muchrougher surface.
Key words: Pulsed laser, temperature, tissue, thermal damage, mechanical damage.
Introduction
Recently there has been a shift from cw lasers, suchas argon and Nd:YAG, to pulsed lasers for precisetissue ablation. At present several types of pulsedlaser are being used. In recent years research andprototype systems have focused on angioplasty'l andophthalmology,4' 5 but the use of pulsed lasers is alsobeing explored for other disciplines such as dentistry,urology, and orthopedic surgery.- 8 The two maintypes of pulsed laser of interest are the excimer lasersin the UY region of the spectrum (190-400 nm) andthe mid-IR lasers from 1.5 to 3.0 ,um. In particular,the holmium laser (X = 2.09 ,um) may be an alterna-tive to the XeCl excimer laser ( = 308 nm) for theablation of superficial tissue layers with limited ther-mal injury to the adjacent tissue.9"10
Interestingly enough, although the chromophoresfor the two-wavelength regions are different, forevery wavelength penetration depth in the V thereis at least one IR wavelength that has the samepenetration depth. The 1/e penetration depth ofHo:YAG-laser irradiation (300 [um) in aorta is 6times larger than the penetration depth of the XeCl
The authors are with the Biomedical Engineering Program,University of Texas at Austin, Austin, Texas 78712.
Received 27 December 1991.0003-6935/93/040526-09$05.00/0.e 1993 Optical Society of America.
excimer laser in the same tissue (50 ,m)."1 Althoughthe use of excimer lasers has been quite success-ful,"3" 2 the fact that solid-state IR lasers are lessexpensive and easier to maintain has resulted inconsiderable pressure to accept IR lasers for theablation task. In addition, for UV wavelengths (espe-cially those below 300 nm) there is concern that theymay be mutagenic.13"14 However, the IR wavelengthcauses larger dissections in the tissue.'5 These fin-gerlike dissections are presumably caused by thevaporization of water just below the tissue surface,which causes a buildup of pressure and the subse-quent eruption of steam and tissue fragments. 5- 7
Because the chromophores are different for UV thanfor IR laser irradiation, it is suggested that themechanism of ablation may be different between thetwo cases.
Thermal damage can be modeled as a reactionrate-of-formation process. 8" 9 It has been shownthat thermal damage in skin induced in vivo can bedescribed by an Arrhenius reaction-rate functionexpressed as an integral of the form
[C (0)] iIn C(t) = Q(r, z, t) = JA exp[-E/RT(r, z, t)]dt'
(1)
where C(0) is the initial concentration of a molecule
526 APPLIED OPTICS / Vol. 32, No. 4 / 1 February 1993

and C(t) is the concentration at time t, fl is thedimensionless total damage, A is the molecular colli-sion rate (s-1), E is the activation energy (J/mol), R isthe universal gas constant, 8.3144 (J/mol K), T(r, z, t')is the scalar temperature field (K), and t is the time(s). The total damage is dependent exponentially ontemperature and linearly on time.
The temperature response of human aorta to308-nm XeCl excimer irradiation and 2.09-VumHo:YAG irradiation are compared. The irradiatedsamples have been examined histologically so thattissue damage could be related to the temperaturehistory of the tissue (and thus laser irradiationparameters). Regular light microscopy has been usedfor assessing thermal damage to the tissue.
Materials and Methods
Lasers and Delivery
Infrared ExperimentsThe experiments in the IR region were performedwith a Ho:YAG laser (Schwartz Electro Optics, 1-2-3).The laser generated pulses of 250 s full width athalf-maximum (FWHM) at a wavelength of 2.09 p1m.The actual pulse consisted of an envelope of microsec-ond spikes as described elsewhere.17 Repetition ratesf of 3 and 5 Hz were employed in the experiments.The laser beam was coupled into a low OH opticalfiber with a core diameter of 600 ,um through the useof a CaFl lens with a focal length of 2.5 cm. The l/e 2
spot size in air at the tissue level was measured by astandard knife-edge method 2 0 to be 760 pLm after itwas determined that the knife-edge measurementswere in reasonable agreement with a Gaussian beamprofile. The distance between the fiber and thetissue was kept at 1 mm. The energy per pulse (E/p)at the fiber tip was varied from 100 to 200 mJ/p.This corresponds to irradiances at the tissue of0.22-0.44 J/mm 2 if a Gaussian distribution of energyover the spot is assumed. We also used the samelaser in the Q-switched mode (rotating mirror Q-switch); in which case the pulse length was 200 ns(FWHM) at repetition rates of 3 and 5.4 Hz (accordingto the manufacturer's specifications). The E/p wasthe same in the Q-switched case as in the normalmode.
Ultraviolet ExperimentsExperiments at the LW wavelength were performedwith a XeCl excimer laser (Technolas). This lasergenerated pulses of 120 ns (FWHM) at a wavelengthof 308 nm. Repetition rates f of 10 and 20 Hz wereused. The laser beam was coupled into a singlequartz fiber with a core diameter of 500 [im. Thedistance from the fiber to the tissue was 1 mm, andthe l/e 2 spot diameter was 615 ,um, which wasmeasured with a standard knife-edge technique afterwe established that the knife-edge measurementswere in reasonable agreement with a Gaussian profile.The E/p at the tip was varied from 6 to 20 mJ/p,corresponding to 20-67 mJ/mm2 .
The experiments (holmium and excimer) were de-signed so that the product
E = (E/p)ft (2)
was a constant (10.8 J for the holmium laser and 1 Jfor the excimer laser), where E/p is the energy perpulse (mJ/pulse), f is the repetition rate (pulses/s),and t is the exposure time (seconds). In other words,while the irradiance and the repetition rate werevaried, the exposure time was adjusted to keep thetotal amount of energy delivered to the tissue con-stant.
It should be noted that the irradiance for the LWlaser is an order of magnitude smaller than theirradiance used for the IR laser, which corresponds tothe clinically used laser parameters. Typical clinicalparameters are 1-3 J/mm 2 at 5 Hz for the normalmode holmium laser2l and 50 mJ/mm 2 at 20 Hz forthe 308-nm excimer laser', all delivered throughmultifibers.
SalineThe irradiation of tissue covered with 2 cm of salinewas achieved by placing the laser delivery fiber incontact with the tissue. In this case the spot diame-ters were equal to the fiber diameters (i.e., 500 and600 ,um for UV and IR experiments, respectively).The irradiances changed accordingly and varied from354 to 708 mJ/mm 2 for the Ho:YAG laser and from30.6 to 102 mJ/mm 2 for the XeCl excimer laser. Inthe contact mode the beam is assumed to have a flatprofile at the fiber tip. All the other parameterswere kept the same as in air.
Temperature Measurements
In Air-Thermal CameraThe fiber end was placed 1 mm away from theirradiated tissue surface in air. The tissue wasmounted on a two-dimensional translation stage sothat a fresh piece of tissue was irradiated for eachpulse sequence. The thermal response was mea-sured with an IR camera (Inframetrics, Model 600L).Camera optics included a 3 x telescope lens and aclose-up lens with a 9.5-in. (24.13-cm) focal length.This camera measures IR radiation in the 3-5-,umband. In the normal mode the time resolution be-tween two-dimensional images was 16.67 msec, andthe detector rise time (10-90% for a step change intemperature) was 5.15 ,uS.22 The thermal-cameraoutput was time coded by a video timer, which wastriggered by the first pulse from the laser (Fig. 1).The time-coded output was recorded on video andanalyzed later with Thermoteknix software version1.0. A region of 4 pixels was selected from which werecorded the average temperature as a function oftime. The temperatures that are reported here are1.0 mm away from the center of the beam. Allexperiments were performed at room temperature(22°C), and the results are given as temperature rise.
1 February 1993 / Vol. 32, No. 4 / APPLIED OPTICS 527

thermal
[I] ~~~~~~~~~~~Laser
tissue shutter
fiber
Fig. 1. Experimental setup for two-dimensional temperaturemeasurements in air with a thermal camera.
In Saline-ThermocoupleTo obtain temperature measurements in a situationthat is closer to clinical reality, we submerged tissueunder saline and measured the temperature with athermocouple. A type K (Chromel-Alumel) thermo-couple with a diameter of 0.3 mm was placed on thesurface of the aorta so that the center of the thermo-couple was located 0.65 mm from the center of theirradiation site. The thermocouple was located justbeyond the tip of a hypodermic needle so that thethermocouple wires, which were Teflon coated, werenot in contact with the metal of the needle. Thisavoided a heat-sink effect by the metal needle; yet thethermocouple had enough rigidity for precise position-ing next to the laser beam delivery fiber by a micropo-sitioner and an operating microscope. The last cen-timeter of supportive cladding was removed from theoptical fiber. Direct radiation of the thermocouplewas avoided, and the tissue temperature was mea-sured just lateral of the ablation crater. The thermo-couple signal was measured with respect to a thermo-couple placed in an ice bath and amplified by adifferential amplifier (Tektronix, DA 502) and re-corded with a fast strip-chart recorder (Clevite Mark220). The rise time (10-90%) of the thermocouplesystem was 7 ms.23 We brought the fiber in con-tact with the tissue without exerting any force byplacing the tray with tissue and saline on a balance.We brought the balance to equilibrium by addingweights to the other arm. Then the fiber and thethermocouple were lowered to the point where theytouched the tissue but did not disturb the equilib-rium.
Tissue
Fresh human aorta tissue (within 24 h after death)was used in these experiments. The tissue washarvested, and all blood was removed by cleaning thetissue in saline. The tissue was stored in salinemoist cloth at 4C until the moment of use. Beforeirradiation the tissue was brought to room tempera-ture while still wrapped in the moist cloth to avoiddehydration. Sites for irradiation were selected thatdid not show any kind of atherosclerosis on grossinspection by eye. The intimal side of the tissue wasirradiated perpendicular to the surface. Afterwardthe tissue was fixed in a 10% buffered formalinsolution and saved for histology. Samples were dehy-drated through a series of alcohols and xylenes and
embedded in paraffin. Multiple transverse sections5 ALm thick were cut from each lesion. The sectionswere stained with a standard hematoxilin and eosinstain. In the section containing the largest lesionthe extent of the thermal and mechanical damage wasmeasured microscopically with a calibrated eyepiece.
Results
Thermal Camera-Temperatures in Air
A typical result of the temperature history of a spotirradiated with the Ho:YAG laser is presented in Fig.2. Peak temperatures are undersampled because ofthe limitations of the thermal-camera time resolution;thus only portions of transient temperatures arerecorded. Nevertheless, the thermal camera doescorrectly record the effect of pulsed laser radiation onthe baseline temperature (i.e., the temperature justbefore the next pulse is delivered). The points justprior to the next laser pulse provide a picture of thesuperposition of temperatures for a sequence of pulses.Note that each temperature before a subsequentpulse is the minimum temperature for the proceedinglaser pulse at the point of measurement. Thesebaseline temperature-rise values at r = 1 mm areplotted against time for the different irradiationconditions in Fig. 3. Every baseline temperature-rise curve is an average of three experiments. Themaximum baseline temperature rise at the momentof laser shutoff for excimer, normal holmium, andQ-switched holmium laser radiation in air are pre-sented in Table 1 as the average standard deviation(sd) (n = 3). The first laser pulse started at t = 0,and the arrows indicate the moment the pulse se-quence was completed. The greatest temperaturerise (i.e., baseline temperature) for the holmium laser
800
o e
60-a,
E -
40
20- - l l l0 2 4 6 8 10
time [s]
Fig. 2. Typical temperature response of human aorta irradiatedwith the pulsed Ho:YAG in the normal mode recorded with thethermal camera. The repetition rate was 3 Hz, and the E/p was150 mJ/p. The temperature was measured 1.0 mm from the spotcenter. The thermal camera was not capable of capturing thepeak temperatures during the laser pulse but was an excellentdevice for recording the slower part of the temperature decay afterthe laser pulse. From this type of curve we measured the baselinetemperature rises as displayed in Fig. 3.
528 APPLIED OPTICS / Vol. 32, No. 4 / 1 February 1993

2 71 0 0 100 mJ/p
200 mJ/o 150 mJ/p
_ = I20 30
time [s]
(e)
time [s](f)
time [s](c)
100
80 AA100 mJ/p
60-
40 I
10 J/p20 I
200 mJ/p0~ _
0 10 20
Fig. 3. Baseline temperature rise (just before the next pulse) ofthe tissue at 1.0 mm from the spot center. The arrows indicatethe moment that the laser was shut off. Note the change in thetemperature scale between the plots for the holmium and excimerlasers. (a) Temperature caused by excimer irradiation in air at 10Hz with 6, 10, 15, and 20 mJ/p. (b) Temperature caused byexcimer irradiation in air at 20Hz with 6, 10, 15, and 20 mJ/p. (c)Temperature caused by normal-mode (250-ps) Ho:YAG irradiationin air at 3 Hz with 100, 150, and 200 mJ/p. (d) Temperaturecaused by normal-mode (250-ps) Ho:YAG irradiation in air at 5 Hzwith 100, 150, and 200 mJ/p. (e) Temperature caused by Q-switched (200-ns) Ho:YAG irradiation in air at 3 Hz with 100, 150,and 200 mJ/p. (f) Temperature caused by Q-switched (200-ns)Ho:YAG irradiation in air at 5.4 Hz with 100, 150, and 200 mJ/p.
30
time [s](d)
1 February 1993 / Vol. 32, No. 4 / APPLIED OPTICS 529
100
80 -
mJ/p
mJ/p
mJ/p
mJ/p
T.
.:2
Ea)I
time [s]
(a)
60 -
40 -
20- 7A
2
0
30 b,
_ 91- __
20 //
a ~ ~ ~ ~ ~ ~ ~ ~ ~ - 1
o~~~~~~~~~~~~~~::1
0 10
100
0 2
806 MJ/p
1 oMJ/p
5 MJ/p
20 MJ/p
U
8)
E8)
time [s](b)
60
40
20100
80
60
40
20
I mJ/p
mJ/p
mJ/p
F * r -
e o o l \ x
3
11(
1
6 8

Table 1. Baseline Temperature Rise at the Moment of Laser Shutoff at1.0 mm Away From the Spot Center during Irradiation of Human Aorta inAir with Normal and Q-Switched Holmium Laser Radiation and Excimer
308-nm Radiation
Ho:YAG LaserTotal Energy, 10.8 J
Excimer LaserTotal Energy, 1 J Free (Hz) Q-Switched (Hz)
E/p(mJ) 10Hz 20Hz E/p(mJ) 3 5 3 5
6 12±213±2 100 33±366±3 32±3 48±410 13±322±3 150 46±268±4 52±4 49±215 18±225±3 200 53±488±3 62±2 48±320 20±228±1
occurred at the highest repetition rate (5 Hz) and atthe highest E/p (200 mJ) and was 850C. The maxi-mum baseline temperature rise at 1.0 mm for excimer(308-nm) irradiation was produced at the highest E/p(20 mJ) and the highest repetition rate (20 Hz) andwas - 280C.
Thermocouple-Temperature
Temperature measurements at the end of Ho:YAG(250- js) irradiation with thermocouples and tissue ina saline environment are summarized in Table 2.The center of the thermocouple was 0.65 mm fromthe center of the laser fiber. The temperature isgiven as the mean sd with n = 4. Our mainconcern, direct radiation of the thermocouple, waseasily avoided by the precise positioning of the thermo-couple. Accidental irradiation of the thermocoupleproduces an out-of-range temperature. Further-more, since values of the temperature just before thenext pulse were used, the effects of direct radiationhad disappeared.23 Note that the temperature riseof the samples irradiated under saline was signifi-cantly lower than the corresponding cases of thesamples irradiated in air (270C versus 850C for thenormal mode holmium laser at 5 Hz and 440mJ/mm2 ).
Histology
The fluence threshold for the ablation of human aortawith the long-pulse holmium laser at 2.09 jIm in air,which was determined histologically, was 0.3J/mm 2. The determination of the crater depth bymeans of histological analysis was difficult and sub-ject to substantial errors since it depended heavily on
Table 2. Baseline Temperature Rise at the Moment of Laser ShutoffMeasured with the Thermocouple Just Next to the Fiber (Spot Center toThermocouple Center = 650 m) on Top of the Tissue during Irradiation
with the Ho:YAG Laser in the Normal Mode (250 Ais) of Human Aortaunder Saline
Repetition Rate
E/p (mJ) 3 Hz 5 Hz
100 9±1 16±2150 12±2 21±2200 16±2 17±2
the position of the plane of cutting relative to thelesion centet. However, in the cases in which wewere certain that the plane of cutting was at thecenter of the crater we measured the extent ofdamage.
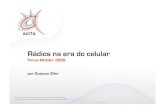
Typical craters produced with the three lasers bothin air and in saline are shown in Fig. 4. Damage totissue was divided into mechanical damage (fissuresand ruptures) and thermal damage (vacuolation, dark-ening, carbonization). Significant zones of vacuola-tion, estimated to be 250-450 jim around the craterwere observed for the normal-mode holmium laserboth in air and in saline. Q-switched holmium laserirradiation in air created a vacuolation zone of thesame order as the normal-mode holmium laser; but inaddition to that large dissections extending as far as0.5 mm beyond the crater edge were visible. Insaline, Q-switched holmium laser irradiation causedvery little thermal damage (<100 jim), but largedissections and ruptures of the tissue were noted asfar as 1.0 mm lateral of the crater wall. In generalwe observed that the ablation crater depth increasedslightly, and the thermal-damage zone decreasedwith increasing fluence. The histology of holmiumablation in an air environment had craters that weresometimes carbonized (the long pulse), especially atlong exposure times, and always had a large zone ofvacuolation around them (250-450 pIm) for the longpulse as well as the Q-switched pulse. Beyond thevacuolation zone a second zone could be observedwhere collagen was hyalinized and the cells appearedto be slightly darker.
The ablation fluence threshold for the 308-nmexcimer laser was determined histologically to be 18mJ/mm 2 . The excimer-laser irradiation of aortasamples in air produced lesions with very little ther-mal or mechanical damage (< 50 jim). However, inthe case of excimer irradiation in saline a larger zoneof mechanical damage of 100 jim was observed,which left behind a rough surface. No carbonizationwas seen around the lesions that were created withthe excimer laser.
Observations
An interesting observation was the difference innormal-mode versus Q-switched ablation under saline.The long pulses of the Ho:YAG laser started ablationwith a few loud pops, after which ablation continuedsilently, whereas the first few pulses of the Q-switched Ho:YAG were fairly silent and then becameextremely loud with violent explosions that evenmade droplets of saline splash out of the tray. Grossmicroscopically, the intimal surface was torn apart inthis case. In all irradiations of tissue under salinethe fiber moved into the tissue, although virtually noforce was exerted. The temperature sensor re-mained at the surface of the tissue. In fact, for bothair and saline experiments the surface temperatureswere those of nonablated tissue.
530 APPLIED OPTICS / Vol. 32, No. 4 / 1 February 1993

(a) (d)
(b) (e)
(c) (f )
Fig. 4. Photomicrographs of cross sections of the laser-induced lesions in human aorta tissue. The total energy delivered was 10.8 J forthe holmium laser and 1 J for the excimer laser. (a) Lesion made with the Q-switched Ho:YAG laser at 3 Hz and 100 mJ/p in air;magnification, 100x. (b) Lesion made with the long-pulse Ho:YAG laser at 3 Hz and 150 mJ/p in air; magnification, 100x. (c) Lesionmade with the excimer laser at 10 Hz and 10 mJ/p in air; magnification, 100x. (d) Lesion made with the Q-switched Ho:YAG laser at 3Hzand 100 mJ/p in saline; magnification, 40x. (e) Lesion made with the long-pulse Ho:YAG laser at 3 Hz and 200 mJ/p in saline;magnification, 40x. (f) Lesion made with the excimer laser at 10 Hz and 20 mJ/p in saline; magnification, 100x.
Discussion
Ablation in Air
There is a significant diffeience in thermal effects andthermal damage caused by Ho:YAG laser radiationand 308-nm excimer-laser radiation. However, con-sidering the fact that the fluences used with theholmium laser (220-440 mJ/mm2 ) are an order of
magnitude larger than those used with the excimerlaser (20-67 mJ mm2), this is not surprising. Theexcimer laser wavelength, which has a penetrationdepth in soft tissue of 60 pm, ablates much moreefficiently than the holmium wavelength that has apenetration depth in soft tissue of 300 pum. Alsothe ablation fluence thresholds are an order of magni-tude different, i.e., 300 mJ/mm 2 for the normal-mode
1 February 1993 / Vol. 32, No. 4 / APPLIED OPTICS 531

Ho:YAG laser versus 18 mJ/mm 2 for the excimerlaser. The excess energy of the holmium laser isconverted to heat and causes thermal damage to thetissue surrounding the crater.
The data that we obtained with the thermal cameraneed to be evaluated carefully. An excellent over-view of the limitations of this method is presented byTorres et al.2 2 The thermal camera provides anexcellent device for measuring the thermal responseof tissue surrounding the irradiation site. Althoughtemporal and spatial limitations of the camera pre-clude the measurement of temperature during theirradiation pulse, the camera captures the slow por-tion of the relaxation response to each laser pulse.The field of view of the flying spot scanner is notsynchronized with the laser. Thus in Fig. 2 the firsttemperature point measured after the onset of a laserpulse is unlikely to catch the peak of the transientresponse. Within milliseconds the temperature ofthe tissue 1.0 mm away from the beam center reachesa maximum. The transient decay lasts longer thanthe 333 ms between laser pulses; thus a superpositionof temperatures occurs. At the end of 30 laser pulses(10s) the baseline temperature at 1.0 mm is over450C. (The baseline temperature rise is over 20'C.)This elevated lower bound of the temperature sug-gests that thermal damage will extend beyond the1.0-mm measurement point.
The fact that the temperature 1 mm away from thespot center decays faster than the theory wouldpredict for this volume requires an explanation.The beam profile out of the fiber at a 1-mm distancewas assumed to be Gaussian and the /e2 beamradius 0o was 380 p.m. The thermal diffusion for avolume this large should be of the order of hundredsof milliseconds. Direct irradiation of the tissuecaused by the Gaussian beam cannot cause thetemperature rise as seen. At a radius of 1 mm theirradiance is only 0.00012 of the peak irradiance.A possible explanation could be that the heated-tissuewater vaporizes and a bubble of hot-water vapor,which can be as large as 3-4 mm in diameter andexpands and collapses within several hundred micro-seconds underneath the surface of the aorta, quicklyheats the tissue surface layer. The subsurface bub-ble formation has been photographed and describedby van Leeuwen et al. 15
It can be seen in Fig. 3 that, first, an increase in E/presulted in a faster temperature rise. This wasexpected since more energy per unit time was depos-ited and thus more heat was generated. Second, theincrease in the repetition rate resulted in a muchfaster baseline temperature rise since the time for thetissue to diffuse the deposited heat was shorter.
In comparing the baseline temperature rises causedby 250-Rus normal-mode holmium laser irradiationwith those caused by Q-switched holmium laserirradiation, at a repetition rate of 3 Hz, the base-linetemperature rises created by the 200-ns Q-switchedpulses were comparable with those created by thenormal-mode laser. However, at 5 Hz the lollal-
mode laser caused significantly greater baseline tem-perature rises than the Q-switched laser did. At thehigher repetition rate the baseline temperature risewas significantly larger than the baseline tempera-ture rise at 3 Hz. The higher temperature combinedwith the high peak power (2.2 x 104 W/cm2) of theQ-switched Ho:YAG laser created a more violentexplosion; thus part of the energy was converted tokinetic energy used to blow off particles, and part ofthe energy was carried away by the mass removal ofheated tissue. 6 24
Temperature and Tissue Damage
Since the temperature was measured at 1 mm awayfrom the center of the laser spot (which is also thecenter of the ablation crater), tissue damage at thispoint is discussed in relation to the temperatures atthis point. The vacuolation zone that is a dominantcharacteristic of thermal damage is associated withtemperatures of over 1000C.25 In none of the casesdid we observe vacuolation as far away as the 1-mmpoint.
The highest baseline temperature (105°G) wasachieved at 5 Hz and 440 mJ/mm 2 with the normal-mode Ho:YAG laser, in which case the vacuolationzone extended 0.9 mm from the center of the crater.Although the boundary of this zone was not clear, thecollagen hyalinization zone extended out to 1 mm inalmost all cases where the baseline temperatureexceeded 60C. (The baseline temperature rise was380C.) This corresponded to a temperature of 58°Cthat was reported for hyalinization of collagen byThomsen.25 With the excimer laser no thermal dam-age was observed histologically at 1 mm from thecenter of the crater, which was in agreement with thefact that the highest baseline temperature measuredwith the excimer laser at 1 mm was 50C.
The excimer laser caused much less heat to build upin the tissue in an air environment than the Ho:YAGlaser did. Since the ablation threshold was muchlower at this wavelength, less energy per pulse wasdeposited to achieve ablation. The baseline tempera-ture rise that was measured in air was below 30'C,although there are indications that the peak tempera-tures on a microscale are much higher, as reported byGijsbers et al.2 6
The temperature measurements with a thermalcamera required that experiments be conducted in anair environment since the 3-5-,um IR radiation isstrongly absorbed by water. Since the thermal con-ductivities of air and water at 300 K are 0.26 x 10-3and 6.13 x 10-'(W/mK), respectively,27 it obviouslymakes a significant difference in the temperatureresponse of tissue whether the tissue is in an air orwater environment during laser irradiation. Also,the effects of laser irradiation on the thermal proper-ties of tissue caused by dehydration are less signifi-cant in a saline environment.
Ablation Under Saline
There are several remarkable differences betweenHo:YAG ablation in i' arnd ablation unde a Iayer of
532 APPLIED OPTICS / Vol. 32, No. 4 / 1 February 1993

saline. Histologically a zone of vacuolation aroundthe crater produced by the free-running Ho:YAGablation was observed, that was slightly smaller thanthe comparable cases in air. Under saline, heat canbe diffused in a volume that is twice as large as in air,if we assume that tissue and saline have similarthermal properties. In addition to the vacuolationthere were also large dissections and tears thatextended laterally in the tissue as far as 1.0 mmbeyond the crater wall. The origin of these dissec-tions was described by van Leeuwen et al. 15 and wasassociated with the expanding water-vapor bubblethat tears apart layers of aortic tissue. The Q-switched holmium laser pulses left almost no vacuola-tion (i.e., no thermal damage), but the mechanicaldamage in the form of tears, ruptures, and flaps wasdevastating. This indicated that the vapor-bubbleexpansion was more violent in this case. A secondhypothesis is that mechanical damage was caused bypressure waves generated by the Q-switched puls-es. 2 8 ,2 9
The craters that were produced with the excimerlaser under saline were irregular. The edges of thecraters were rough, and more tearing was noted thanin the corresponding ablation in air. Bubble forma-tion induced by the excimer laser was most likely thecause of this effect. In fact, bubbles similar to thosethat were seen with the Ho:YAG laser were docu-mented for the excimer ablation process.'5 The zoneof damage extended 100 m laterally into thetissue. These values were smaller than the lateralthermal necrosis zone of 350 + 90 m reported byvan Leeuwen in vivo.15 However, in our experi-ments there was no blood present, which is a strongabsorber for the 308-nm wavelength. The presenceof blood was a key factor in the formation of bubblesthat were observed during 308-nm excimer ablation.
Conclusion
The temperature response of tissue to Ho:YAG, Q-switched Ho:YAG, and excimer pulsed laser radiationwas compared. The ablation of aortic tissue withany of the lasers resulted in a temperature buildupinside the tissue. This temperature superpositionwas more significant for the IR wavelength than forthe UV. Our in vitro experiments demonstratedthat the thermal-damage zone was larger for the IRwavelength. Mechanical damage was observed in allcases but was excessive in the case of the Q-switchedHo:YAG laser. Excimer ablation in air leaves behinda smooth surface; however, when ablated undersaline, the crater edges show significantly more me-chanical damage. To what extent the thermal andmechanical damage affect the clinical results with anyof the lasers remains to be studied.
We thank Ton van Leeuwen for his comments onthe manuscript and Roberto Bayardo for supplyingthe tissue samples. We also thank Trimedyne Inc.for the use of its facilities for part of the experimentalwork. This work was supported in part by the Officeof Naval Research under grant N00014-91-J-1564
and in part by the Albert and Clemmie Caster Foun-dation.
References1. F. Litvack, N. L. Eigler, J. R. Margolis, W. S. Grundfest, D.
Rothbaum, T. Linnemeier, L. B. Hestrin, D. Tsoi, S. L. Cook,and D. Krauthamer, "Percutaneous excimer laser coronaryangioplasty," Am. J. Cardiol. 66, 1027-1032 (1990).
2. K. R. Karsch, K. K. Haase, W. Voelker, A. Baumbach, M.Mauser, and L. Seipel, "Percutaneous coronary excimer laserangioplasty in patients with stable and unstable angina pectoris.Acute results and incidence of restenosis during 6-monthfollowup," Circulation 81, 1849-1859 (1990).
3. H. J. Geschwind, J. L. Dubois Rande, D. Murphy-Chutorian,T. Tomaru, R. Zelinsky, and D. Loisance, "Percutaneouscoronary angioplasty with mid-infrared laser and a new multi-fiber catheter," Lancet 336, 245-246 (1990).
4. A. M. Cotliar, H. D. Schubert, E. R. Mandel, and S. L. Trokel,"Excimer laser radial keratotomy," Opthalmology 92, 206-208 (1985).
5. J. S. Marshall, S. L. Trokel, S. Rothery, and H. D. Schubert,"An ultrastructural study of corneal incisions induced by anexcimer laser at 193 nm," Opthalmology 92, 749-758 (1985).
6. U. Keller and R. Hibst, "Experimental studies of the applica-tion of the Er:YAG laser on dental hard substances:II. Light microscopic and SEM investigations," Lasers Surg.Med. 9, 345-351 (1989).
7. R. Hofmann and R. Hartung, "Use of pulsed Nd:YAG laser inthe ureter," Urol. Clin. North Am. 15, 369-375 (1988).
8. M. Meller, J. Black, and H. Sherk, "Wavelength selection inlaser arthroscopy," Lasers Surg. Med. Suppl. 3, 50 (1991).
9. W. S. Grundfest, F. Litvack, J. S. Forrester, T. Goldenberg,H. J. Swan, L. Morgenstern, M. Fishbein, I. S. McDermid,D. M. Rider and T. J. Pacala, "Laser ablation of humanatherosclerotic plaque without adjacent tissue injury," J. Am.Coll. Cardiol. 5, 929-933 (1985).
10. C. J. White, S. R. Ramee, T. J. Collins, J. E. Mesa, D. B.Paulsen, and J. P. Murgo, "Recanalization of arterial occlu-sions with a lensed fiber and a holmium:YAG laser," LasersSurg. Med. 11, 250-256 (1991).
11. A. J. Welch, M. Motamedi, S. Rastegar, G. L. LeCarpentier,and D. Jansen, "Laser thermal ablation," Photochem. Photo-biol. 53, 815-823 (1991).
12. T. A. Sanborn, S. R. Torre, S. K. Sharma, R. A. Hershman, M.Cohen, W. Sherman, and J. A. Ambrose, "Percutaneouscoronary excimer laser-assisted balloon angioplasty: initialclinical and quantitative angiographic results in 50 patients,"J. Am. Coll. Cardiol. 17, 94-99 (1991).
13. M. S. Feld and J. R. Kramer, "Mutagenicity and the XeClexcimer laser: a relationship of consequence?" Am. Heart J.122, 1803-1805 (1991).
14. H. Lubatschowski, C. Otten, and K. Schmiedt, "Laser inducedsecondary radiation in 193 nm excimer laser photoablation ofcorneal, dental, and dermal tissues," Lasers Surg. Med. Suppl.3, 9 (1991).
15. T. G. van Leeuwen, L. van Erven, J. H. Meertens, M. Mota-medi, M. J. Post, and C. Borst, "Origin of arterial walldissections induced by pulsed excimer and mid-infrared laserablation in the pig," J. Am. Coll. Cardiol. 19, 1610-1618(1992).
16. J. A. Izatt, D. Albagli, M. Britton, J. M. Jubas, I. Itzkan, andM. S. Feld, "Wavelength dependence of pulsed laser ablation ofcalcified tissue," Lasers Surg. Med. 11, 238-249 (1991).
17. T. G. van Leeuwen, M. J. van der Veen, R. M. Verdaasdonk,and C. Borst, "Noncontact tissue ablation by holmium: YSGGlaser pulses in blood," Lasers Surg. Med. 11, 26-34 (1991).
18. A. R. Moritz and F. C. Henriques, "Studies in thermal injury
1 February 1993 / Vol. 32, No. 4 / APPLIED OPTICS 533

II. The relative importance of time and surface temperaturein the causation of cutaneous burns," Am. J. Pathol. 23,695-720 (1947).
19. F. C. Henriques and A. R. Moritz, "Studies in thermal injury I.The conduction of heat to and through skin and the tempera-ture attained therein. A theoretical and experimentalinvestigation," Am. J. Pathol. 23, 531-549 (1947).
20. J. M. Khosrofian and B. A. Garetz, "Measurement of aGaussian laser beam diameter through the direct inversion ofknife-edge data," Appl. Opt. 22, 3406-3410 (1983).
21. H. J. Geschwind, J. Kvasnicka, F. Nakamura, R. Zelinsky, andR. J. L. Dubois-Rande, "Infrared laser coronary angioplasty:initial results," MedTech 2, 9 (1991).
22. J. H. Torres, T. A. Springer, A. J. Welch, and J. A. Pearce,"Limitations of a thermal camera in measuring temperatureof laser-irradiated tissues," Lasers Surg. Med. 10, 510-523(1990).
23. R. M. Verdaasdonk, E. D. Jansen, F. C. Holstege, and C. Borst,"Temperature along the surface of modified fiber tips forNd:YAG laser angioplasty," Lasers Surg. Med. 11, 213-222(1991).
24. J. A. Izatt, D. Albalgli, I. Itzkan, and M. S. Feld, "Pulsed laserablation of calcified tissue: physical mechanisms and funda-
mental parameters," in Laser-Tissue Interaction, S. L. Jacques,ed., Proc. Soc. Photo-Opt. Instrum. Eng. 1202, 133-140(1990).
25. S. Thomsen, "Pathologic analysis of photothermal and photo-mechanical effects of laser-tissue interactions," Photochem.Photobiol. 53, 825-835 (1991).
26. G. H. Gijsbers, R. L. Sprangers, D. G. van den Broecke, N. vanWieringe, M. J. Brugmans, and M. J. C. van Gemert, "Temper-ature increase during in vitro 308 nm excimer laser ablation ofporcine aortic tissue," in Diagnostic and Therapeutic Cardio-vascular Interventions, G. S. Abela, ed., Proc. Soc. Photo-Opt.Instrum. Eng. 1425 (to be published).
27. F. P. Incropera and D. P. deWitt, Fundamentals of Heat andMass Transfer (Wiley, New York, 1990), App.
28. P. E. Dyer and R. K. Al-Dhahir, "Transient photoacousticstudies of laser tissue ablation," in Laser-Tissue Interaction,S. L. Jacques, ed., Proc. Soc. Photo-Opt. Instrum. Eng. 1202,46-60 (1990).
29. T. J. Flotte, Y. Yashima, S. Watanabe, D. J. McAuliffe, andS. L. Jacques, "Morphological studies of laser-induced photo-acoustic damage," in Laser-Tissue Interaction, S. L. Jacques,ed., Proc. Soc. Photo-Opt. Instrum. Eng. 1202, 71-77 (1990).
534 APPLIED OPTICS / Vol. 32, No. 4 / 1 February 1993