
Exame físico do membro superior para o médico do …acemt.com.br/estatuto/exame101115.pdf ·...
28
Exame sico do membro superior para o médico do trabalho Chrisne Muniz Ago/2015
Transcript of Exame físico do membro superior para o médico do …acemt.com.br/estatuto/exame101115.pdf ·...
Exame físico do membro superior para o médico do trabalho
Christine MunizAgo/2015

OmbroAnamneseInspeção estáticaInspeção dinâmicaPalpaçãoForça muscularTestes especiais

Contribution of clinical tests to the diagnosis of rotator cuff disease: a systematic literature review.Beaudreuil et al. Joint Bone Spine. Jan,2009
OBJECTIVE: To evaluate the diagnostic performance of clinical tests for degenerative rotator cuff disease, based on a systematic literature review.
METHODS: We searched Medline, Embase, and Pascal Biomed until the first half of 2006 inclusive for articles that reported at least the sensitivity and specificity of clinical tests for rotator cuff disease. Predictive values and accuracy were recorded where available. The results were discussed and validated.
RESULTS: Selected nine studies, 03 investigated tests for subacromial impingement syndrome and 07 tests for rotator cuff tendinopathy. The Neer and Hawkins tests had good sensitivity but low specificity for subacromial impingement syndrome. For diagnosing tears of the supraspinatus or infraspinatus, the Jobe sign and the full can test showed similar performance characteristics to the Patte test and resisted external rotation with the elbow at the side flexed at 90 degrees . For tendinopathies with/without tears, active unresisted external rotation for the infraspinatus and the lift off test for the subscapularis were specific but lacked sensitivity. In one study, limitation of the range of active unresisted internal rotation was sensitive and specific for subscapularis tendon disease. The palm up test performed poorly for diagnosing long head of biceps disease.
CONCLUSIONS: Data on the diagnostic performance of clinical tests for rotator cuff tendon disease are fragmentary. Objective data exist to support the usefulness of some of these tests. Further studies are needed

Physical examination tests of the shoulder: a systematic review with meta-analysis of individual tests.Hegedus EJ et al. Br J Sports Med. Feb, 2008.
OBJECTIVE: Compile and critique research on the diagnostic accuracy of individual orthopaedic physical examination tests in a manner that would allow clinicians to judge whether these tests are valuable to their practice.
METHODS: MEDLINE, CINAHL, and SPORTDiscus databases (1966 to October 2006) using keywords related to diagnostic accuracy of physical examination tests of the shoulder. The QUADAS tool was used to critique the quality of each paper. Meta-analysis through meta-regression of the diagnostic odds ratio (DOR) was performed on the Neer test for impingement, the Hawkins-Kennedy test for impingement, and the Speed test for superior labral pathology.
RESULTS: 45 studies were critiqued with only half demonstrating acceptable high quality and only two having adequate sample size. For impingement, the meta-analysis revealed that the pooled sensitivity and specificity for the Neer test was 79% and 53%, respectively, and for the Hawkins-Kennedy test was 79% and 59%, respectively. For superior labral (SLAP) tears, the summary sensitivity and specificity of the Speed test was 32% and 61%, respectively. Regarding orthopaedic special tests (OSTs) where meta-analysis was not possible either due to lack of sufficient studies or heterogeneity between studies, the list that demonstrates both high sensitivity and high specificity is short: hornblowers's sign and the external rotation lag sign for tears of the rotator cuff, biceps load II for superior labral anterior to posterior (SLAP) lesions, and apprehension, relocation and anterior release for anterior instability. Even these tests have been under-studied or are from lower quality studies or both. No tests for impingement or acromioclavicular (AC) joint pathology demonstrated significant diagnostic accuracy.
CONCLUSION: Diagnostic accuracy of the Neer test and the Hawkins-Kennedy test for impingement and the Speed test for labral pathology is limited. There is a great need for large, prospective, well-designed studies that examine the diagnostic accuracy of the numerous physical examination tests of the shoulder. Currently, almost without exception, there is a lack of clarity with regard to whether common OSTs used in clinical examination are useful in differentially diagnosing pathologies of the shoulder

O que são os tendões do manguito rotador?
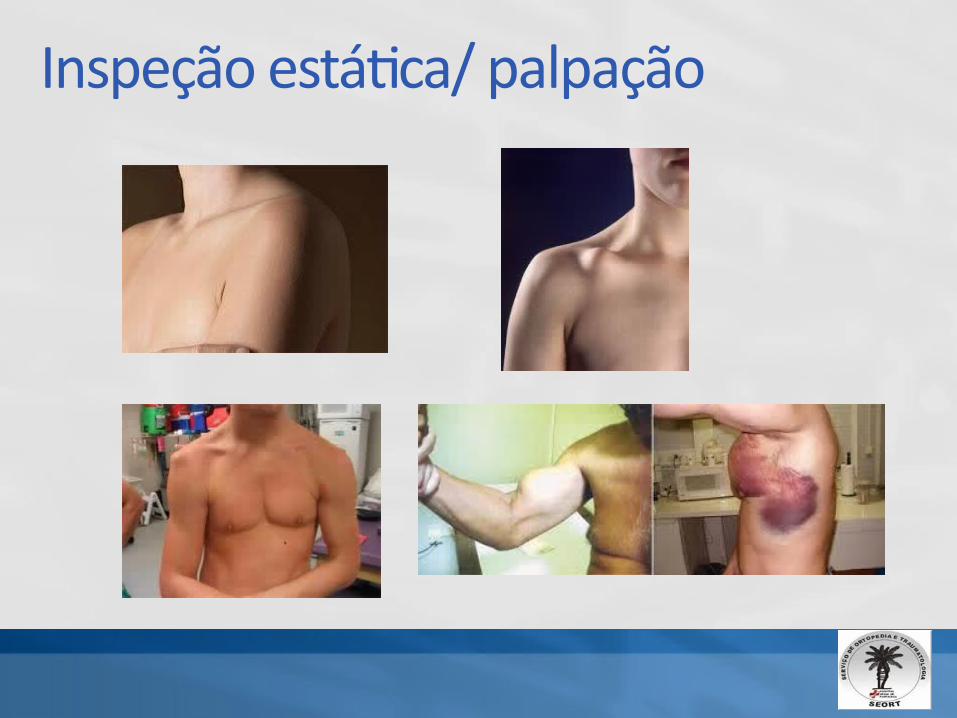
Inspeção estática/ palpação
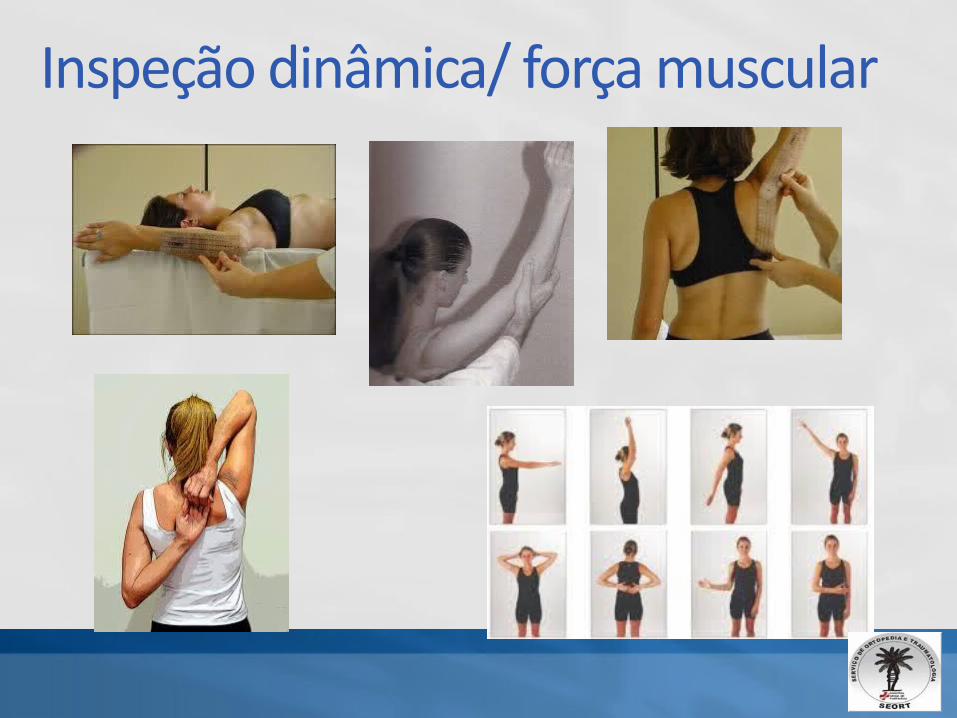
Inspeção dinâmica/ força muscular

Testes especiais
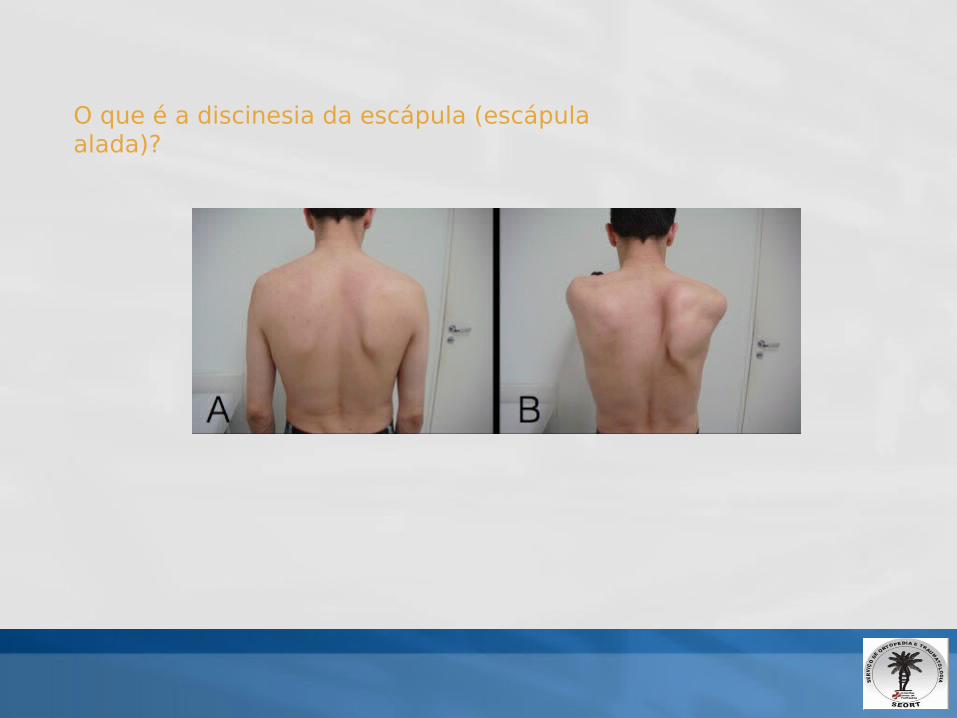
O que é a discinesia da escápula (escápula alada)?

Lesões neurológicas (escápula alada)
Secundárias
Lesão do nervo torácico longoLesão do nervo espinal acessório
Distrofia facioescapuloumeral

O que é e como ocorre a lesão dos tendões do manguito rotador?

Diagnostic accuracy of ultrasonography, MRI and MR arthrography in the characterisation of rotator cuff disorders: a meta-analysis.
Roy JS et al. Br J Sports Med. Feb, 2015
BACKGROUND: US, MRI, MR arthrography are commonly used for the characterisation of rotator cuff disorders. The first objective was to perform a meta-analysis on the diagnostic accuracy of medical imaging for characterisation of RC disorders. Since US is used at the point of care in environments such as sports medicine, a secondary analysis assessed accuracy by radiologists and non-radiologists.
METHODS: Systematic search in three databases. Two raters performed data extraction and evaluation of risk of bias independently, and agreement was achieved by consensus. Hierarchical summary receiver-operating characteristic package was used to calculate pooled estimates of included diagnostic studies.
RESULTS: Diagnostic accuracy of US, MRI and MRA in the characterisation of full-thickness RC tears was high with overall estimates of sensitivity and specificity over 0.90. As for partial RC tears and tendinopathy, overall estimates of specificity were also high (>0.90), while sensitivity was lower (0.67-0.83). Diagnostic accuracy of US was similar whether a trained radiologist, sonographer or orthopaedist performed it.
CONCLUSIONS: Since full thickness RC tear constitutes a key consideration for surgical repair, it is important kowns when selecting an imaging modality for RC disorder. When considering accuracy, cost, and safety, US is the best option.

Como é o tratamento cirúrgico da lesão dos tendões do manguito rotador?
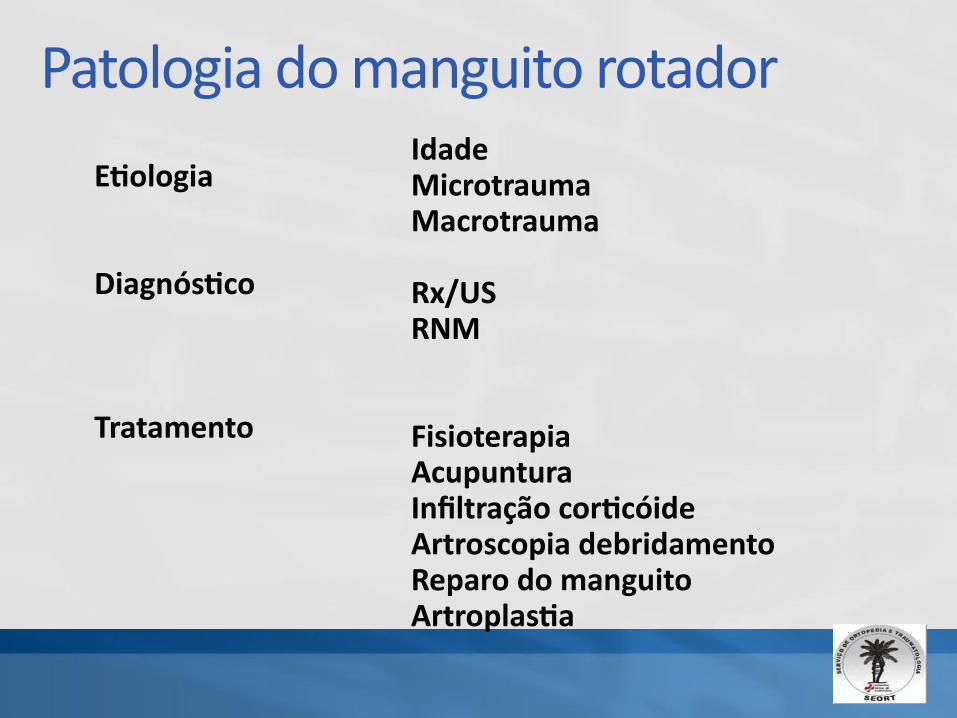
Patologia do manguito rotador
Etiologia
Diagnóstico
Tratamento
IdadeMicrotraumaMacrotrauma
Rx/USRNM
FisioterapiaAcupunturaInfiltração corticóideArtroscopia debridamentoReparo do manguitoArtroplastia
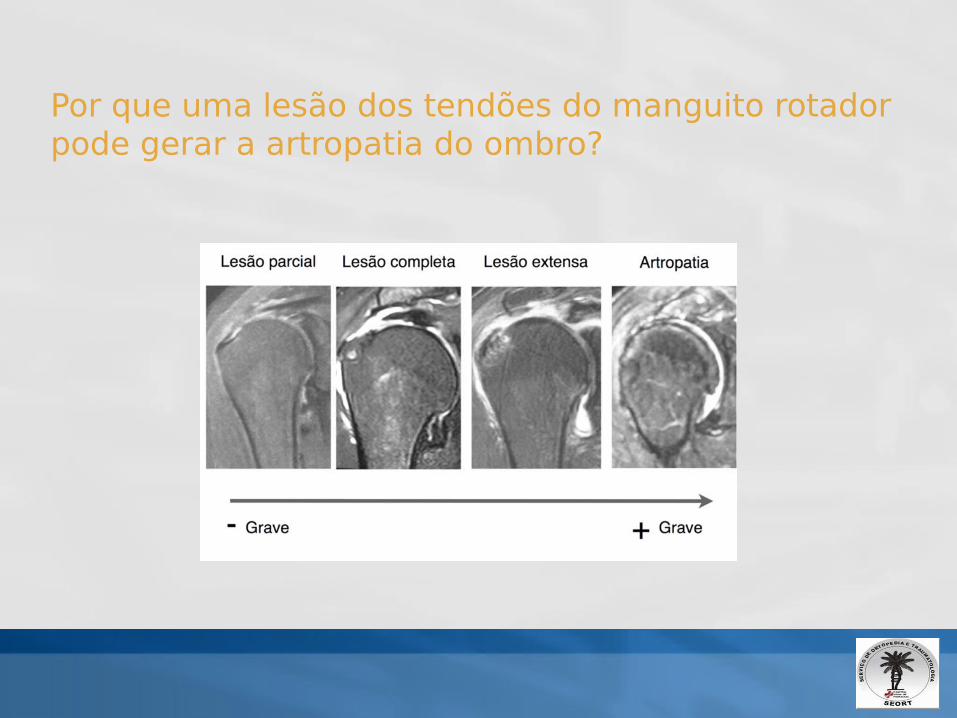
Por que uma lesão dos tendões do manguito rotador pode gerar a artropatia do ombro?

Cotovelo
AnamneseInspeção estáticaInspeção dinâmicaPalpação Força muscularTestes especiais
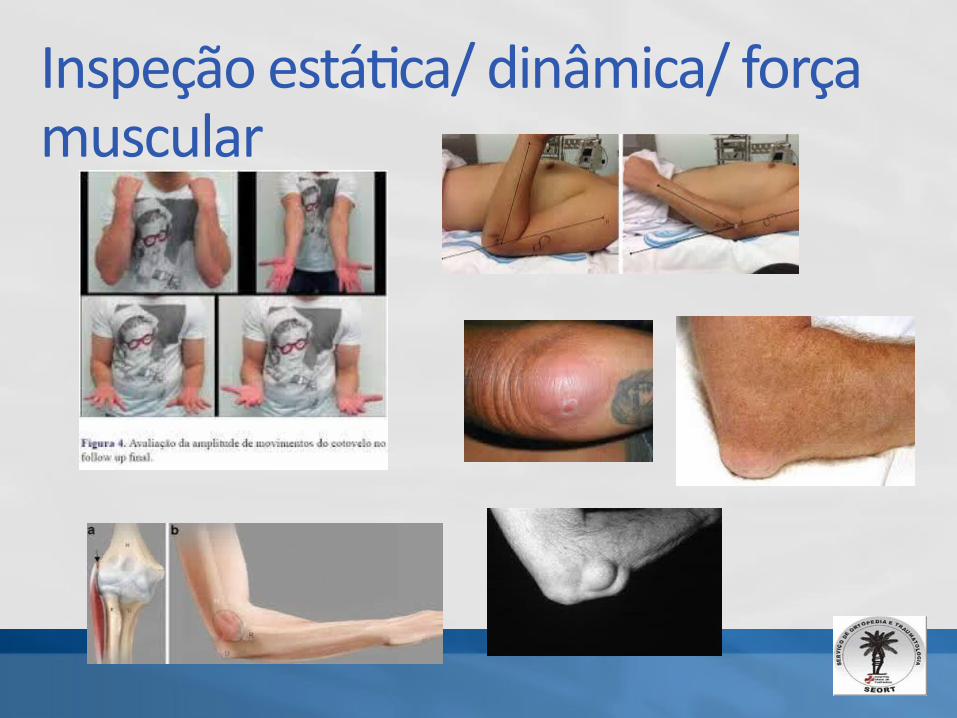
Inspeção estática/ dinâmica/ força muscular

Testes especiais

Punho
AnamneseInspeção estáticaInspeção dinâmicaPalpaçãoForça muscularTestes especiais
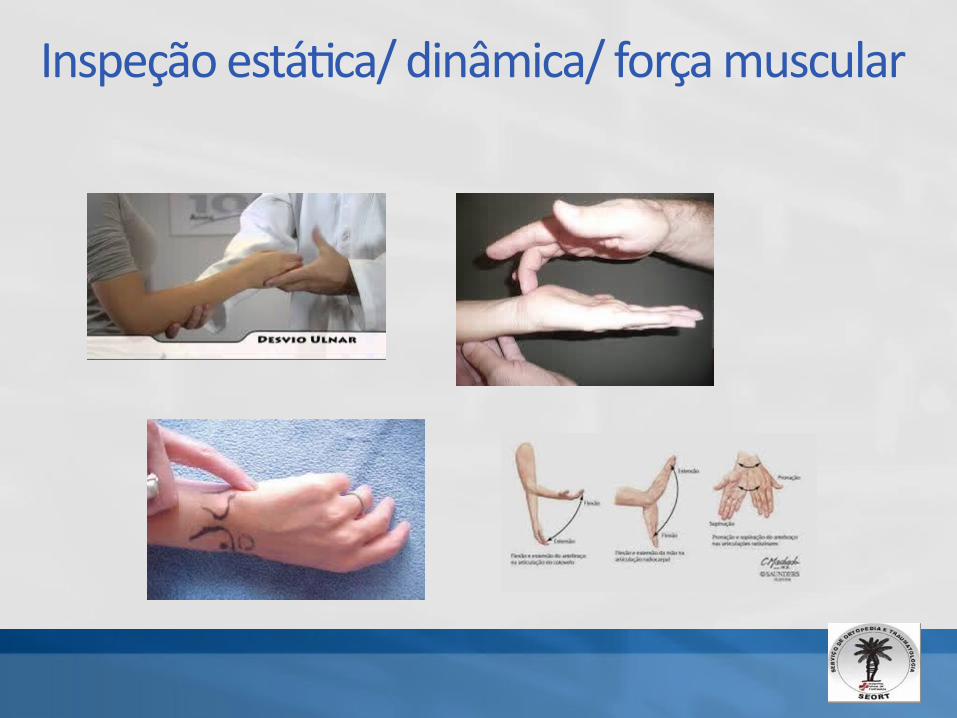
Inspeção estática/ dinâmica/ força muscular

Testes especiais

Mão
AnamneseInspeção estáticaInspeção dinâmicaPalpaçãoForça muscularTestes especiais

Inspeção estática/ dinâmica/ força muscular

Testes especiais
Obrigada

Isolated arthroscopic biceps tenotomy or tenodesis improves symptoms in patients with massive irreparable rotator cuff tears.Boileau P et al. J Bone Joint Surg Am. Apr 2007
BACKGROUND: Lesions of the long head of the biceps tendon are often associated with massive rotator cuff tears and may be responsible for shoulder pain and dysfunction. The purpose of this study was to evaluate the clinical and radiographic outcomes of isolated arthroscopic biceps tenotomy or tenodesis as treatment for persistent shoulder pain and dysfunction due to an irreparable rotator cuff tear associated with a biceps lesion.
METHODS: We conducted a retrospective study of sixty-eight consecutive patients (mean age [and standard deviation], 68 +/- 6 years) in whom a total of seventy-two irreparable rotator cuff tears had been treated arthroscopically with biceps tenotomy or tenodesis. A simple tenotomy was performed in thirty-nine cases, and a tenodesis was performed in thirty-three. No associated acromioplasty was performed. All patients were evaluated clinically and radiographically by an independent observer at a mean of thirty-five months postoperatively.
RESULTS: Fifty-three patients (78%) were satisfied with the result. The mean Constant score improved from 46.3 +/- 11.9 preoperatively to 66.5 +/- 16.3 postoperatively (p < 0.001). A healthy-appearing teres minor on preoperative imaging was associated with significantly increased postoperative external rotation (40.4 degrees +/- 19.8 degrees compared with 18.1 degrees +/- 18.4 degrees ) and a significantly higher Constant score (p < 0.05 for both) compared with the values for the patients with an absent or atrophic teres minor preoperatively. Three patients with pseudoparalysis of the shoulder did not benefit from the procedure and did not regain active elevation above the horizontal level. In contrast, the fifteen patients with painful loss of active elevation recovered active elevation. The acromiohumeral distance decreased 1.1 +/- 1.9 mm on the average, and glenohumeral osteoarthritis developed in only one patient. The results did not differ between the tenotomy and tenodesis groups (mean Constant score, 61.2 +/- 18 points and 72.8 +/- 12 points, respectively). The "Popeye" sign was clinically apparent in twenty-four (62%) of the shoulders that had been treated with a tenotomy; of the sixteen patients who noticed it, none were bothered by it.
CONCLUSIONS:1 Both arthroscopic biceps tenotomy and arthroscopic biceps tenodesis can effectively treat severe pain or dysfunction caused by an irreparable rotator cuff tear associated with a biceps lesion. 2. Shoulder function is significantly inferior if the teres minor is atrophic or absent. 3. Pseudoparalysis of the shoulder and severe rotator cuff arthropathy are contraindications to this procedure





![[@AJ] Manual do Membro Novo](https://static.fdocuments.in/doc/165x107/568c509e1a28ab4916af4607/aj-manual-do-membro-novo.jpg)












