EWMA Journal Vol 11 No 2
76
Danish Wound Healing Society Working together to ensure better patient outcomes Volume 11 Number 2 May 2011 Published by European Wound Management Association
Transcript of EWMA Journal Vol 11 No 2

Danish WoundHealing Society
Working together to ensure
better patient
outcomes
Volume 11Number 2May 2011
Published byEuropeanWound ManagementAssociation

Jan ApelqvistPresident Elect
EWMA Council
The EWMA JournalISSN number: 1609-2759
Volume 11, No 2, May, 2011
Electronic Supplement May 2011www.ewma.org
The Journal of the EuropeanWound Management Association
Published three times a year
Editorial BoardCarol Dealey, Editor
Sue BaleFinn Gottrup
Martin KoschnickZena Moore
Marco RomanelliZbigniew Rybak
José Verdú SorianoRita Gaspar Videira
Peter Vowden
EWMA web sitewww.ewma.org
Editorial Officeplease contact:
EWMA SecretariatNordre fasanvej 113,
2000 Frederiksberg, Denmark.Tel: (+45) 7020 0305Fax: (+45) 7020 0315
Layout:Birgitte Clematide
Printed by:Kailow Graphic A/S, Denmark
Copies printed: 14,000
Prices:The EWMA Journal is distributed
in hard copies to members as part of their EWMA membership.
EWMA also shares the vision of an “open access” philosophy,
which means that the journal is freely available online.
Individual subscription per issue: 7.50€
Libraries and institutions per issue: 25€
The next issue will be published in October 2011. Prospective material for
publication must be with the editors as soon as possible and no later
than 15 July 2011.
The contents of articles and letters inEWMA Journal do not necessarily reflect
the opinions of the Editors or the European Wound Management Association.
Copyright of all published materialand illustrations is the property of
the European Wound ManagementAssociation. However, provided prior
written consent for their reproduction, including parallel publishing
(e.g. via repository), obtained from EWMA via the Editorial Board of the Journal,
and proper acknowledgement and printed, such permission will normally
be readily granted. Requests to reproduce material should state
where material is to be published, and, if it is abstracted, summarised,
or abbreviated, then the proposed new text should be sent to the
EWMA Journal Editor for final approval.
Dubravko Huljev
Robert StrohalRytis Rimdeika
Corrado M. DuranteTreasurer
Martin Koschnick
CO-OPERATING ORGANISATIONS’ BOARD
Christian Thyse, AFISCeP.be
Andrea Bellingeri, AISLeC
Elia Ricci, AIUC
Aníbal Justiniano, APTFeridas
Gerald Zöch, AWA
Luc Gryson, BFW
Vladislav Hristov, BWA
Els Jonckheere, CNC
Milada Francu, CSLR
Dubravko Huljev, CWA
Hans Martin Seipp, DGfW
Eskild Winther Henneberg, DSFS
Anna Hjerppe, FWCS
Pedro Pacheco, GAIF
J. Javier Soldevilla, GNEAUPP
Christian Münter, ICW
Aleksandra Kuspelo, LBAA
Mark Collier, LUF
Kestutis Maslauskas, LWMA
Corinne Ward, MASC
Hunyadi János, MSKT
Suzana Nikolovska, MWMA
Alison Johnstone, NATVNS
Kristin Bergersen, NIFS
Louk van Doorn, NOVW
Arkadiusz Jawien, PWMA
Rodica Crutescu, ROWMA
Severin Läuchli, SAfW (DE)
Hubert Vuagnat, SAfW (FR)
Goran D. Lazovic, SAWMA
Mária Hok, SEBINKO
Sylvie Meaume, SFFPC
Christina Lindholm, SSIS
Jozefa Košková, SSOOR
Guðbjörg Pálsdóttir, SUMS
Javorca Delic, SWHS
Magnus Löndahl, SWHS
Andrea Nelson, TVS
Jasmina Begic-Rahic, URuBiH
Barbara E. den Boogert-Ruimschotel, V&VN
Skender Zatriqi, WMAK
Georgina Gethin, WMAOI
Nada Kecelj Leskovec, WMAS
Bülent Erdogan, WMAT
Leonid Rubanov, WMS (Belarus)
For contact information, see www.ewma.org
Editorial Board MembersSue Bale, UK
Carol Dealey, UK (Editor)
Finn Gottrup, Denmark
Martin Koschnik, Portugal
Zena Moore, Ireland
Marco Romanelli, Italy
Zbigniew Rybak, Poland
José Verdú Soriano, Spain
Rita Gaspar Videira, Portugal Peter Vowden, UK
Paulo Jorge Pereira Alves, Portugal
Caroline Amery, UK
Michelle Briggs, UK
Mark Collier, UK
Bulent Erdogan, Turkey
Madeleine Flanagan, UK Milada Francu, Czech Republic
Peter Franks, UK
Francisco P. García-Fernández, Spain
Luc Gryson, Belgium
Alison Hopkins, UK
Gabriela Hösl, Austria
Klaus Kirketerp-Møller, Denmark
Zoltán Kökény, Hungary
Christian Münter, Germany
Andrea Nelson, UK
Pedro L. Pancorbo-Hidalgo, Spain Hugo Partsch, Austria
Patricia Price, UK
Rytis Rimdeika, Lithuania
Salla Seppänen, Finland
Carolyn Wyndham-White, Switzerland
Gerald Zöch, Austria
EWMA Journal Scientific Review Panel
Luc Gryson
Patricia PriceSecretary
Sue BaleRecorder
Carol DealeyEWMA Journal Editor
Barbara E. den Boogert-Ruimschotel
Paulo Alves
Zena MoorePresident
Marco RomanelliImmediate Past President
Gerrolt Jukema
Sylvie MeaumeMaarten J. Lubbers
Severin LäuchliEskild Winther Henneberg
2

Science, Practice and Education
Organisations
EWMA
ELECTRONIC SUPPLEMENT MAY 2011
WWW.EWMA.ORG
The May 2011 edition of the EWMAJournal Electronic Supplement consistof all the accepted abstracts for theEWMA 2011 Conference in Brussels.It is divided into 150 Oral presentationsand 358 Poster presentations and itis possible to download individualabstracts as well as the entire supplement(including all the abstracts) at
www.ewma.org/english/ewma-journal/electronic-supplement.html
Scientific Communication
5 EditorialCarol Dealey
7 The fight against biofilm infections: Do we have the knowledge and means?Klaus Kirketerp-Møller, Thomas Bjarnsholt, Trine Rolighed Thomsen
10 Biofilms in wounds: An unsolved problem?António Pedro Fonseca
25 Diabetic foot ulcer pain: The hidden burdenSarah E Bradbury, Patricia E Price
38 Topical negative pressure in the treatment of deep sternal infection following cardiac surgery: Five year results of first-line application protocolMartin Šimek
43 Wounds Research for Patient Benefit: A five year programme of research in wound careKaren Lamb, Nikki Stubbs, Jo Dumville, Nicky Cullum
48 EWMA Journal Previous Issues and Other Journals
50 Introducing the Belgian Federation of WoundcareBrigitte Crispin, Luc Gryson
52 EWMA Patient Outcome GroupPatricia Price
55 1st EWMA Health Economics Course organised by the EWMA Patient Outcome GroupFinn Gottrup
56 Advanced Wound Care Sector (AWCS) Status ReportHans Lundgren
60 EWMA Wound Surveys – Resource consumption for wound careFinn Gottrup
62 National collaboration for the Leg Ulcer & Compression Seminars 2011Hugo Partsch, Finn Gottrup
64 EWMA Corporate Sponsors Contact Data
66 Conference Calendar
69 Conference Report: EWMA Session, 20th Annual European Tissue Repair Society CongressGerrolt N. Jukema
70 FWCS: The 14th national wound healing congress in Helsinki, FinlandAnna Hjerppe
72 Wound Treatment Organisation established in UkraineRytis Rimdeika
74 EWMA Cooperating Organisations
75 International Partner Organisations
75 Associated Organisations
EWMA Journal 2011 vol 11 no 2 3

The Mölnlycke Health Care name and logo, Avance®, Mepiseal® and Safetac® are registered trademarks of Mölnlycke Health Care AB. © Copyright (2011) Mölnlycke Health Care. All rights reserved. Mölnlycke Health Care AB, Box 13080, SE-402 52 Göteborg, Sweden. Phone + 46 31 722 30 00. www.molnlycke.com
HQ
0245
7110
4
Welcome to Mölnlycke Health Care Satellite SymposiumInvestigating the Impact of Topical Antimicrobials in Wound CareMay 26, 2011 at 11.15-12.15Wound infection is the most concerning of all wound complications. Topical antimicrobials play an important role in preventing and managing local wound infections however there are some outstanding questions regarding the usage of these agents that need to be answered.
The aim of this Symposium is to support the appropriate use of topical antimicrobial agents and to promote clinical decision-making that ensures their prescription only when clinically indicated.
Chairmen: Assoc Prof Bill McGuiness & Lt Col Steven Jeffery
Speakers: Professor Kevin Chipman, Dr Paul Silverstein & Dr Jean-Charles Kerihuel
You said: “It’s time to change NPWT ” So we did.
We look forward to seeing you there!
Discover easy-to-use, less painful1 Avance®
Avance NPWT system can help prevent some of the unnecessary pain often experienced in NPWT. Thanks to two unique products with Safetac® technology: Avance film with Safetac and Mepiseal® sealant with Safetac, patients experience less blistering2, less damaging maceration to the periwound area3 and more comfortable dressing changes1. The properties of Safetac also means you can quickly and easily reposition the film during application with no pain to the patient and no loss of effectiveness. Avance NPWT is easy to learn for patients and professionals alike, and the same pump can be used in the hospital or at home. To see all the ways Avance is delivering NPWT the way you want it, visit our stand.
1. White R. A Multinational survey of the assessment of pain when removing dressings. Wounds UK 2008;Vol 4, No 1. 2. Submitted to International Journal of Orthopaedic and Trauma Nursing, 2011. 3. Meaume S et al. A study to compare a new self adherent soft silicone dressing with a self adherent polymer dressing in stage II pressure ulcers. Ostomy Wound Management
2003;49(9):44-51.
EWMA2011Brussels · Belgium
www.ewma2011.org

Dear Readers
Welcome to the Spring Issue of the EWMA Journal, sometimes known as the ‘Conference Issue’ as its publication
coincides with our annual conference. It is a great pleasure to know that conference delegates will all receive a copy of this issue, as I imagine that there may be a number who have not come across the EWMA Journal before. If this is you, please be aware that the Journal is freely available on-line via the EWMA website and also via Ebsco Host (free for NHS UK employees).
As ever we have a number of interesting papers for you as well as all the news of EWMA activities and updates from a number of our Co-operating Organ-isations. I would like to draw your attention to some in particular. We have two papers about biofilms, one an opinion piece from a Danish group led by Dr Klaus Kirketerp-Møller which highlights some of the problems surrounding biofilms; the other from Assistant Professor Pedro Fonseca which gives us really detailed information about biofilms and their effects. I would also recommend to you a quite different paper which looks at the impact of pain on the quality of life with patients with diabetic foot ulcers. This is the second of two papers by Bradbury and Price on this subject and they both make interesting reading.
In this issue we have what I hope is the start of a long series – the showcasing of large funded pro-grammes of research relating to wound healing and tissue viability. Professor Nicky Cullum provides us with details of an interesting programme of Re-search for Patient Benefit funded by the English National Institute for Health Research (NIHR). The NIHR provides funding for programme grants lasting 4-5 years and it is very encouraging that two such programmes are wound management/tissue viability related. The other programme grant called PURPOSE will be showcased in the next issue. We would be delighted to hear from other successful research teams about their projects and showcase them in the same way.
I am writing about something completely different in the final part of my editorial – and it could be called my farewell speech. At the An-
nual General Meeting this month I will be retiring from EWMA Council and I have decided it is also appropriate to step down as editor of the Journal. This will not be a shock to Council as we have been discussing this for some time and the Journal editorship is being passed over into the very capable hands of Sue Bale. Sue has been on the Editorial Board for a while, so she has a very good insight into the workings of the Journal. I would like to take this opportunity to thank all the members of the Editorial Board and of the Scientific Review Panel as well as the ‘Two Katja’s’ of EWMA Secretariat for their support over the last few years. The Editorial Board and the Scientific Review Panel have been very gracious about undertaking rapid reviews for me at short notice from time to time and I have depended on them all for their considered reviews of the papers we receive. As for the ‘Two Katja’s’ – they have had the thankless task of trying to keep me to deadlines and prompting me when I forget things! I wish them all well and I am sure the Journal will continue to go from strength to strength.
As for me, well it will seem strange as I have been involved with EWMA since before it was officially established and a member of Council all of that time as well. I have thoroughly enjoyed being part of EWMA and have friends in many countries in Europe through the meetings I have attended. On a very personal note I especially appreciated these friendships and the love and support I received when my husband died. So now, I am officially winding down towards my retirement in 2012 when I have many plans which include having more time to spend with friends and family, especially my little grandson who loves to help me with my digging in my vegetable garden.
Carol Dealey, Editor
EWMA Journal 2011 vol 11 no 2 5

What did we find living under some silver dressings?*
Not all silver dressings are created equal.AQUACEL® Ag and Versiva®XC®
Adhesive dressing
No bacterial growth*
ALLEVYN™ Ag Gentle Border dressing
Bacterial growth*
Mepilex® Ag dressing
Bacterial growth*
Further evidence to increase your confidence in AQUACEL® Ag dressing.*1
AQUACEL® Ag dressing. Micro-contouring, bacteria killing*2,3
Find out more about AQUACEL® Ag dressing. Call:1-800-422-8811 or visit:www.hydrofiber.com
*As demonstrated in vitro ConvaTec researchers used an in vitro bacteria-seeded agar overlay model simulating a colonized wound surface to investigate the antimicrobial activity of selected silver wound dressings. The dressings were separately applied to agar surfaces seeded with S. aureus and P. aeruginosa. After 48 hours, the dressings were removed from the agar surfaces. These photographs are representative of the visually observed results with S. aureus.
1. The Antimicrobial Activity of Silver-Containing Wound Dressings on a Simulated Colonised Wound Surface. Scientific Background Report. WHRI3415 MA162. 2011 Data on File, ConvaTec.2. Jones S, Bowler PG, Walker M. Antimicrobial activity of silver-containing dressings is influenced by dressing conformability with a wound surface. WOUNDS. 2005;17(9):263-270. 3. Jones SA, Bowler PG, Walker M, Parsons D. Controlling wound bioburden with a novel silver-containing Hydrofiber dressing. Wound Repair Regen. 2004;12(3):288-294.AQUACEL and Hydrofiber are registered trademarks of ConvaTec Inc. All other trademarks are the property of their respective owners.© 2011 ConvaTec Inc. AP-011145-MM [AM/EM]
NEW EVIDENCE
NEW in vitro Evidence
00000_AG_USLetterAd.indd 1 15/04/2011 10:16

Science, Practice and Education
1Klaus Kirketerp-Møller MD
2,3Thomas Bjarnsholt, Phd
4 Trine Rolighed Thomsen,Phd
1Orthopedic DepartmentHvidovre University HospitalDenmark
2University of CopenhagenFaculty Of Health SciencesDepartment of International Health, Immunology and MicrobiologyDenmark
3RigshospitaletDepartment for Clinical Microbiology, afsnit 9301,Denmark
4Department of BiotechnologyChemistry and Environmental EngineeringDenmark
Correspondence:Klaus Kirketerp-Mø[email protected]
Conflict of interest: None
When a ship arrives on the shores of an unknown territory with scarce or no information of what is beyond the ho-
rizon, it is only confidence in the capacity and the skills of the crew and hardware that will convince the commander that the land can be taken. Intel-ligence is of outmost importance. Do we have the intelligence in the battle against biofilm infections to win?
In the present paper we will list what we be-lieve is the key knowledge today and identify what science lacks, in order to suggest research strategies to resolve biofilm infections.
A Paradox: How wonderful that we have met with
a paradox. Now we have some hope of making progress. Niels Bohr (1885-1962)
It is more or less accepted that chronic wounds harbour bacterial biofilm. As illustrated later in this paper, bacterial biofilm has the ability to inter-fere with the human immune system in numerous ways and to prevent healing. Despite that, the majority of chronic wounds will heal if the cause or predisposing factors are treated; the venous leg ulcer will heal with compression therapy, the dia-betic ulcer will heal by off-loading and the cancer ulcer will heal after radiation. The residual group, the non-healing ulcers of mixed origin, could heal if unrecognized and untreated factors are treated well. One of these factors is bacterial biofilm. But what is the difference between the biofilm in the healing group and in the non-healing group?
To stay with the military metaphors, we have reports of some battles we have won, but does that give us knowledge of the bacteria’s full weaponry?
Communication and virulence factorsCommunication between bacteria is pointed out to be a target for intervention. Quorum Sens-ing (QS) in general and between Pseudomonas aeruginosa specifically is only a fragment of the communication between the bacteria. The N-acyl homoserine lactone QS signal molecule in P. aeruginosa will trigger the production of viru-lence factors such as rhamnolipids that, in vitro, can eliminate Neutrophils1. Blocking or modifi-cation of QS, in theory, will enable the immune system to eradicate the bacteria even in mature biofilms. However the QS molecules differ be-tween Gram-positive and Gram-negative bacteria and even within these. A single drug to regulate all the harmful effects of QS is hardly imaginable.
We have only a little overview of the com-munication in multi-species biofilm and of the communication between different mono-species biofilms. To interfere with the bacteria we need to decode their communication under different con-ditions. For instance: does antibiotic treatment alter the communication? Does surgical debride-ment? Insight into this will help us develop treat-ment strategies for different conditions.
ResistanceAntibiotic resistance and tolerance in bacterial biofilm is a major problem in the treatment of infections. The resistance is regulated in many different ways beside the resistance carried by the resistance genes, as in the mecA in Staphyloccocus aureus. Tolerance is partly QS controlled, partly influenced by different phenotypes within the biofilm e.g., different growth rates, efflux pumps etc, and by numerous other factors like the matrix components2;3. The response from the clinician has been newer drugs, higher dosages and poly-drug treatment. Understanding the mechanisms of resistance and tolerance in biofilms can help us develop new treatment strategies and hopefully stop the rising curve of antibiotic usage and of antibiotic resistance.
The fight against biofilm infections:
Do we have the knowledge and means?
Opinion Piece
EWMA Journal 2011 vol 11 no 2 7

Mono or multispecies biofilmChronic wounds are shown to be polymicrobial with no single bacterium exclusively colonizing the wounds4-7. The microbial community is highly variable, and it has been recently published that some primary populations exist in each wound, but there can also be hundreds of different species present, many of which are in trace amounts8. Using FISH, it has been illustrated that some individual microcolonies in chronic wounds only consist of a single species9. Mono and polyspecies biofilms probably exist in the same ulcer, but the importance or relevance of this is not yet established10.
The uneven distributionThe appearance of improved sampling techniques and molecular biology methods have illustrated that the tradi-tional culture-dependent methods often underestimate the micro-organisms present and that a non-random distribu-tion pattern of bacteria exists in the wounds. Differences in bacterial populations across the surface and also deep inside the wounds were found in several studies. S.aureus was primarily located close to the wound surface and P. aeruginosa was primarily located deeper in the wound5;11. This is highly relevant for the clinician. How and when is the sample taken? In an ideal world, the whole wound would be taken out to identify every single pathogen, but this is not possible nor does it provide us with the full answer. Which bacterial strain or even subgroup is im-portant? The newer culture-independent methods such as 16S rRNA gene-based pyrosequencing, 16S rDNA cycle, PCR, real time PCR and fingerprinting techniques like denaturant gradient gel electrophoresis are identifying bacteria never before associated with chronic wounds. The problem for the clinician to evaluate the result of a culture-independent method is paramount. Which bacte-ria is truly a pathogen and which is merely passing by in search of a friendlier environment? How about a cut-off limit that indicates that this bacterium is abundant enough to be a pathogen? Well, the pathogenecity between dif-ferent strains and phenotypes differs and probably differs over time within the same phenotype. Adding detection of known virulence genes to the molecular methods would be helpful in the process of interpretation.
The role of revision before sampling Neither the traditional culturing technique nor the cul-ture-independent methods can compensate for the three-dimensional uneven distribution of micro-organisms in chronic ulcers. When designing a protocol for sampling, we think the following should be considered: 1. Revise the ulcer before sampling. The surface is likely to host commensal flora, and it is more likely that an in-depth residing bacteria is pathogenic than a superficial one. 2: Swab a large area or take a big biopsy.
The introduction of a stringent protocol for sampling in diabetic foot ulcers reduced the frequency of MRSA by almost two-thirds in the ulcer and reduced the number of bacteria believed to be colonizers by three-fourths12.
Are the predominant bacteria the villain? Well they probably are, but some strains are highly viru-lent and co-exist very well with other species. The beta-haemolytic Streptococcus and the Staphylococcus aureus are an example. Yet we do not know whether the virulence of a certain strain is dependent upon another. The most abundant bacteria found by traditional methods could just be the one easiest to grow.
The paradigm shift in research: Instead of only finding the bacteria, look for what they are doing. The questions we, both researchers and clini-cian, should ask are: What role does every single bacterial and fungal species have in the ulcer? What role does the biofilm formation play and is it the same for all species? Which virulence factors are the most important, and does QS play a role etc. Only by having thorough knowledge of this, will we be able to develop sufficient treatment strategies for each individual ulcer.
Until then we have to rely on “Best-Practice Princi-ples”. m
References
1 van Gennip M, Christensen LD, Alhede M, Phipps R, Jensen PO, Christophersen L, et al. Inactivation of the rhlA gene in Pseudomonas aeruginosa prevents rhamnolipid production, disabling the protection against polymorphonuclear leukocytes. APMIS 2009 Jul;117(7):537-46.
2 Percival SL, Hill KE, Malic S, Thomas DW, Williams DW. Antimicrobial tolerance and the significance of persister cells in recalcitrant chronic wound biofilms. Wound Repair Regen 2011 Jan;19(1):1-9.
3 Lewis K. Persister cells, dormancy and infectious disease. Nat Rev Microbiol 2007 Jan;5(1):48-56.
4 Wolcott RD, Gontcharova V, Sun Y, Dowd SE. Evaluation of the bacterial diversity among and within individual venous leg ulcers using bacterial tag-encoded FLX and titanium amplicon pyrosequencing and metagenomic approaches. BMC Microbiol 2009;9:226.
5 Thomsen TR, Aasholm MS, Rudkjobing VB, Saunders AM, Bjarnsholt T, Givskov M, et al. The bacteriology of chronic venous leg ulcer examined by culture-independent molecular methods. Wound Repair Regen 2010 Jan;18(1):38-49.
6 Dowd SE, Sun Y, Secor PR, Rhoads DD, Wolcott BM, James GA, et al. Survey of bacterial diversity in chronic wounds using pyrosequencing, DGGE, and full ribosome shotgun sequencing. BMC Microbiol 2008;8:43.
7 Gjodsbol K, Christensen JJ, Karlsmark T, Jorgensen B, Klein BM, Krogfelt KA. Multiple bacterial species reside in chronic wounds: a longitudinal study. Int Wound J 2006 Sep;3(3):225-31.
8 Smith DM, Snow DE, Rees E, Zischkau AM, Hanson JD, Wolcott RD, et al. Evaluation of the bacterial diversity of pressure ulcers using bTEFAP pyrosequencing. BMC Med Genomics 2010;3:41.
9 Kirketerp-Moller K, Jensen PO, Fazli M, Madsen KG, Pedersen J, Moser C, et al. Distribution, organization, and ecology of bacteria in chronic wounds. J Clin Microbiol 2008 Aug;46(8):2717-22.
10 Burmolle M, Thomsen TR, Fazli M, Dige I, Christensen L, Homoe P, et al. Biofilms in chronic infections – a matter of opportunity – monospecies biofilms in multispecies infections. FEMS Immunol Med Microbiol 2010 Aug;59(3):324-36.
11 Fazli M, Bjarnsholt T, Kirketerp-Moller K, Jorgensen B, Andersen AS, Krogfelt KA, et al. Nonrandom distribution of Pseudomonas aeruginosa and Staphylococcus aureus in chronic wounds. J Clin Microbiol 2009 Dec;47(12):4084-9.
12 Sotto A, Richard JL, Combescure C, Jourdan N, Schuldiner S, Bouziges N, et al. Beneficial effects of implementing guidelines on microbiology and costs of infected diabetic foot ulcers. Diabetologia 2010 Oct;53(10):2249-55.
Science, Practice and Education
EWMA Journal 2011 vol 11 no 2 8

Lohmann & Rauscher
www.Lohmann-Rauscher.com
“Simplifying wound managementby means of new technology andnew definitions.”
A symposium - (60 min, Thursday 26.05.11, 11:15 - 12:15h)
“Wounds at risk – a new definition
(Chair: Thomas Eberlein, Sa Cabaneta/E, Andrew Kingsley, Devon/UK)”
■ Wound at risk and its new definition by the W.A.R. Score – Thomas Eberlein, Sa Cabaneta/E (15 min)
■ Sign Checker – symptoms, diagnosis, therapy – Andrew Kingsley, Devon/UK (15 min)
■ Reduction of SSI in a paediatric population: using a new postoperative polihexanide containing dressing regimen in a paediatric cardiology unit – Thomas Witter (RN Child) & Dr. Aaron Bell, London/UK (15 min)
■ Randomised controlled single center study comparing a polihexanide containing bio-cellulose dressing with silver sulfadiazine cream in partial thickness dermal burns – Andrzej Piatkowski de Grzymala, Aachen/DE (15 min)
9503
227
0411
e
specifi cally for wounds at risk of infection or infected wounds.
quick and effective pain reduction
wide antimicrobial spectrum
good tissue compatibility
independent moisture control by virtue of the unique HydroBalance system
Suprasorb® X + PHMB
B symposium - (60 min, Wednesday 25.05.11, 15:30 - 16:30h)“Gentle Debridement – rapid and effective(Chair: Trudie Young, Aneurin Bevan Health Board, Bangor/UK)”
■ Consensus guidance for the use of debridement techniques in the UK – Trudie Young (Aneurin Bevan Health Board), Bangor/UK (30 min)
■ The wound debrider – a new fibre technology for debridement: results on 60 patients – Michael Schmitz, Rengsdorf/DE (15 min)
■ Gentle debridement: first clinical experience in UK – Sylvie Hampton (Tissue Viability Consultancy Services), Eastbourne/UK (15 min)
Meet us at the EWMA 2011, stand 26!
EWMA Journal 2011 vol 11 no 2 9

António Pedro FonsecaPhD, Assistant Professor1,2
1Faculdade de Medicina, Universidade do Porto,
2 REQUIMTE, Faculdade de Farmácia,
Universidade do Porto, Porto, Portugal
Correspondance:António Pedro Fonseca, Alameda Prof. Hernâni
Conflict of interest: None
ABSTRACTChronically infected wounds are very costly to health care institutions and a significant cause of suffering. The major failure associated to chronic wounds is a delayed healing process due to the presence of single or polymicrobial communities that give protection to antimicrobials and host de-fenses. These biofilm communities can be healthy or pathogenic according to the predominant mi-croorganism so all the prophylactic and therapeu-tic measures should consider the wound healing process as a window of opportunity, ideally after a sharp and regular debridement. The aim of this review is to give an additional insight to health practitioners of the importance of the biofilm paradigm in explaining the delay in wound heal-ing and its relation to a diagnostic, prophylactic and therapeutic management.
1. BIOFILMSa. IntroductionThe ability of a microorganism to establish an infection is dependent on several factors, namely those of the host and the pathogen. There is a bal-ance between the pathogen and the host concern-ing the numbers of pathogens that are needed to start colonization and advance an infection. This balance is dependent on the host defense system and the presence and expression of pathogenic factors associated to the microorganism1,2.
b. Biofilm formationBiofilm is a community of single or multiple mi-croorganisms that are surface attached and encased within an extracellular matrix3. This community is found attached to abiotic surfaces like industrial waters systems and indwelling medical devices4 or biotic like mucosal surfaces5.Biofilm forma-tion in the host is a strategy of the microorganism to survive the host defenses and also to optimize the use of the nutrient rich environment and the cooperative work between the biofilm organisms6.
Biofilms can have either a positive effect such as the biodegradation7 in sewage treatment8 or a negative effect such as corrosion of pipes, infec-tion of indwelling medical devices and the per-sistent infections in cystic fibrosis and chronic wounds9,10.
Bacteria can grow in a free-living planktonic state or in a sessile form, a complex process that requires a sequence of coordinated activities11. This complex sequence starts with the adhesion of the microorganism. This adhesion can be re-versible at first and then becomes irreversible. Fol-lowing this there is the formation of microcolo-nies with the intervention of the quorum sensing (QS) molecules and afterwards the segregation of mucopolyssacharides (the matrix that encase the microcolonies in a biofilm)10.
Biofilms in wounds:
An unsolved problem?
References
1. Gardner SE, Frantz RA, Saltzman CL, Dodgson KJ. Staphylococcus aureus is associated with high microbial load in chronic wounds. Wounds 2004: 16(8):251-7.
2. Jensen PØ, Bjarnsholt T, Phipps R, Rasmussen TB, Calum H, Christoffer-sen L, Moser C, Williams P, Pressler T, Givskov M,, Høiby N. Rapid necrotic killing of polymorphonuclear leukocytes is caused by quorum-sensing-controlled production of rhamnolipid by Pseudomonas aerugi-nosa. Microbiology 2007: 153:1329-38.
3. Costerton JW, Stewart PS, Greenberg EP. Bacterial biofilms: a common cause of persistent infections. Science 1999: 284:1318-22.
4. Donlan RM, Costerton JW. Biofilms: Survival mechanisms of clinically relevant microorganisms. Clin Microbiol Rev 2002: 15(2):167-93.
5. Hall-Stoodley L, Costerton JW, Stoodley P. Bacterial biofilms: From the natural environment to infectious diseases. Nat Rev Microbiol 2004: 2:95-108.
6. Jefferson KK. What drives bacteria to produce a biofilm? FEMS Microbiol Lett 2004: 236(2):163-73.
7. Mor R, Sivan A. Biofilm formation and partial biodegradation of polystyrene by the actinomycete Rhodococcus rubber. Biodegradation 2008: 19(6):851-8.
8. Oliver R, May E, Williams J. Microcosm investigations of phthalate behaviour in sewage treatment biofilms. Sci Total Environ 2007: 372(2-3):605-14.
9. James GA, Swogger E, Wolcott R, Pulcini E, Secor P, Sestrich J, Costerton JW, Stewart PS. Biofilms in chronic wounds. Wound Repair Regener 2008: 16(1):37-44.
10. Fonseca AP, Sousa JC, Tenreiro R. Pseudomonas aeruginosa as a nosocomial pathogen: Epidemiology, virulence, biofilm formation and antimicrobial therapy. In: Pandalai SG, editor. Recent Research Developments in Microbiology. Kerala, India: Research Signpost; 2006. Volume 10. p. 97-132.
11. Davey ME, O’Toole GA. Microbial biofilms: from ecology to molecular genetics. Microbiol Mol Biol Rev 2000: 64(4):847-67.
12. Oliveira DR, Azeredo J, Teixeira P, Fonseca AP. The role of hydropho-bicity in bacterial adhesion. In: Gilbert P, Allison D, Brading M, Verran J, Walker J, editors. Biofilm Community Interactions: Chance or Necessity? Cardiff: Bioline; 2001. p. 11-22.
EWMA Journal 2011 vol 11 no 2 10

Science, Practice and Education
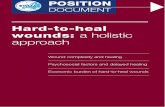
i. AdhesionPlanktonic motile and non motile bacteria can become sessile as they start the adhesion process to an abiotic or biotic surface. For this initial step the presence and functionality of several adhesins such as flagella and fimbrae are needed10,12. There are two possible stages, namely the reversible adhesion in which bacteria can revert to the planktonic state and the irreversible adhe-sion that is a really step to microcolony development and biofilm formation (Figure 1).
Figure 1. Biofilm development in Pseudomonas aeruginosa. This flowchart divides biofilm formation in different steps involving specific events and bacterial properties.Firstly, planktonic bacteria migrate to the surface and adhere (A, B). Once adhered, bacteria divide and twitch to form microcolonies (C). Then alginate production begins that helps to cement the biofilm matrix in a three dimensional structure (D). Some of singular or aggregate cells (also referred as “plank-tonic biofilms”) are released from the biofilm and adhere to the surface in a cyclic pathway (E).
LW-Lifshitz-Van der Waals forces; EL: electrostatic forces; AB: acid-base interactions; OMP: outer membrane protein; LPS: lipopolysaccharide (Adapted from Fonseca et al 2006) (10).
ii. Microcolonies and biofilm formationAfter the initial irreversible adhesion, the cells start to divide and form cell clusters called microcolonies. The dividing cells produce quorum sensing molecules that allow the aggregation of the microcolonies. These structures are thus able to produce a matrix of extra-cellular polymeric substances (EPS) that encases the aggregating cells in a biofilm. These cells can have a flagellum-drive movement within the biofilm thus they are not evenly distributed in the biofilm13 and in this particular case they demand the existence of intersti-tial water channels that also facilitate the exchange of nutrients and wastes10,14. Expression of genes was found to be different in several steps of biofilm formation; in fact the av-
13. Malic S, Hill KE, Hayes A, Percival SL, Thomas DW, Williams DW. Detection and identification of specific bacteria in wound biofilms using peptide nucleic acid fluorescent in situ hybridization (PNA FISH). Microbiology 2009: 155:2603-11.
14. Liu YC, Post JC. Biofilms in pediatric respiratory and related infections. Curr Allergy Asthma Rep 2009: 9(6):449-55.
15. Sauer K, Camper AK, Ehrlich GD, Costerton JW, Davies DG. Pseudomonas aeruginosa displays multiple phenotypes during development as a biofilm. J Bacteriol 2002: 184(4):1140-54.
16. Fux CA, Stoodley P, Hall-Stoodley L, Costerton JW. Bacterial biofilms: a diagnostic and therapeutic challenge. Expert Rev Anti-infect Ther 2003: 1(4):667-83.
17. Flemming HC, Wingender J. Relevance of microbial extracellular polymeric substances (EPSs)- Part I: Structural and ecological aspects. Water Sci Technol 2001: 43(6):1-8.
18. Barraud N, Hassett DJ, Hwang S, Rice RA, Kjelleberg S, Webb JS. Involvement of nitric oxide in biofilm dispersal of Pseudomonas aeruginosa. J Bacteriol 2006: 188(21):7344-53.
19. Davis SC, Ricotti C, Cazzaniga A, Welsh E, Eaglstein WH, Mertz PM. Microscopic and physiologic evidence for biofilm-associated wound colonization in vivo. Wound Repair Regen 2008: 16(1):23-9.
20. Wu J, Xi C. Evaluation of different methods for extracting extracellular DNA from the biofilm matrix. Appl Environ Microbiol 2009: 75(16):5390-5.
21. De Beer D, Stoodley P. Relation between the structure of an aerobic biofilm and transport phenomena. Water Sci Technol 1995: 32(8):11-18.
22. Barrett JF, Hoch JA. Two – component signal transduction as a target for microbial anti-infective therapy. Antimicrob Agents Chemother 1998: 42:1529–36.
23. Yao W, Yue D, Yong Z, YangBo H, BaoYu Y, ShiYun C. Effects of quorum sensing autoinducer degradation gene on virulence and biofilm formation of Pseudomonas aeruginosa. Sci China C Life Sci 2007: 50(3):385-91.
24. Kaplan JB. Biofilm dispersal: mechanisms, clinical implications, and potential therapeutic uses. J Dent Res 2010: 89(3):205-18.
25. Schaber JA,Triffo WJ, Suh SJ, Oliver JW, Hastert MC, Griswold JA, Auer M, Hamood AN, Rumbaugh KP. Pseudomonas aeruginosa forms biofilms in acute infection independent of cell-to-cell signaling. Infect Immun 2007: 75(8):3715-21.
26. Bjarnsholt T, Givskov M. Quorum-sensing blockade as a strategy for enhancing host defences against bacterial pathogens. Philos Trans R Soc 2007: 362(1483):1213-22.
27. Rasmussen TB, Bjarnsholt T, Skindersoe ME, et al (2005) Screening for quorum sensing inhibitors (QSI) by use of a novel genetic system, the QSI selector. J Bact 187(5): 1799–1814.
EWMA Journal 2011 vol 11 no 2 11

Science, Practice and Education
erage difference in protein regulation was 35%15. If planktonic cells are compared with biofilm cells, 800 proteins can be upregulated which demonstrates an expression level over 50% of the proteome15. The microcolonies and biofilm formation is a complex process that involves multiple factors and a variety of interactions, namely the adaptive responses of the sessile microorganisms. In fact the eventual pres-ence of optimal amount of nutrients can be an induc-ing factor for biofilm dispersal due to increased growth of the microorganisms16. Some of the biofilm cells can switch to a planktonic free-swimming phenothype or can detach as aggregates (“planktonic biofilms”)17 and this process aids the spread of the infection by the re-starting of the biofilm formation in other locations18.
iii. Biofilm physiologyThe knowledge of biofilm physiology is of utmost importance to understand the activities of the micro-organisms within the biofilm. This information is es-sential for any approach in order to control biofilm formation. There are several methods that can give some insights into biofilm morphophysiology such as the use of light, epifluorescence, electron and confocal laser microscopy19.
Biofilm architecture is an important factor that in-fluences the detachment process and is affected by the amount of extracellular polymeric substances (EPS) produced. EPS is often composed of polysaccharides, lipids, proteins, nucleic acids and enzymes, and is an aid to the bacterial adhesion process20. The bulk of the biofilm is 75-90% of EPS with only 10-25% be-ing made up of cells. Additionally it is known that biofilms from different species have their singular cel-lular and non cellular arrangements. An example of this are the water channels that are often dependent on the degree of hydration of the biofilm and are of utmost importance in the intake of the nutrients and excretion of the wastes, and are thus essential for bio-
film survival21. There are also several differences in a biofilm’s architecture due to the mono or poly specific character of the biofilm. The microbial ecology can also influence the production of virulence factors and have an effect in the biofilm phenotype as a collective virulence parameter and this may be caused by the communication between the cells. The ability to adapt and have adequate responses to the series of changes in the environment is dependent on cell-cell signal trans-duction systems22,23. Microorganisms can monitor and respond to the presence of others by the production of signaling molecules and this process is called quorum sensing. It is known that this process controls biofilm formation through the secretion of autoinducers, thus representing a key role in the regulation of biofilm architecture, the expression of virulence factors and in the dispersion of organisms24. Nevertheless, there are some strains of Pseudomonas aeruginosa that can form biofilm independently of quorum sensing25. The inhi-bition of cell communication has been shown lately as a new treatment strategy, in particular in the prevention of biofilm infections such as in the case of garlic that inhibits quorum sensing in P. aeruginosa26,27.
c. Factors that interfere in Biofilm formationThe formation of biofilm is influenced by various factors that range from the morphophysiology of the microorgan-isms to the complexity of the environment in terms of nutrients or the presence of chemical and physical agents.
The ability of the microorganisms to adhere to abiotic or biotic surfaces as well as the adherence rate is known to influence the formation of the biofilm28. Bacterial ad-hesins such as flagella or type IV fimbrae29 and the overall hydrophobicity of the bacterial surface can determine if the attachment to the surface is reversible or irreversible. The availability of nutrients is another important factor for the production of quorum sensing molecules, enzymes or amino acids that are essential for adhesion and biofilm formation16.
28. Lasaro MA, Salinger N, Zhang J, Wang Y, Zhong Z, Goulian M, Zhu J. F1C fimbriae play an important role in biofilm formation and intestinal colonization by the Escherichia coli commensal strain Nissle 1917. Appl Environ Microbiol 2009: 75(1):246-51.
29. O’Toole GA, Kolter R. Flagellar and twitching motility are necessary for Pseu-domonas aeruginosa biofilm development. Mol Microbiol 1998: 30:295-304.
30. Ammons MCB, Ward LS, Fisher ST, Wolcott RD, James GA. In vitro susceptibility of established biofilms composed of a clinical wound isolate of Pseudomonas aeruginosa treated with Lactoferrin and xylitol. Int J Antimicrob Agents 2009: 33(3):230-6.
31. Lee J, Jayaraman A, Wood TK. Indole is an inter-species biofilm signal mediated by SdiA. BMC Microbiol 2007: 18(7):42.
32. Giladi M, Porat Y, Blatt A, Shmueli E, Wasserman Y, Kirson ED, Palti Y. Microbial growth inhibition by alternating electric fields in mice with Pseudomonas aeruginosa lung infection. Antimicrob Agents Chemother 2010: 54(8):3212-18.
33. Percival SL, Thomas JG, Williams DW. Biofilms and bacterial imbalances in chronic wounds: anti-Koch. Int Wound J 2010: 7(3): 169-175.
34. Rusconi R, Lecuyer S, Guglielmini L, Stone HA. Laminar flow around corners triggers the formation of biofilm streamers. J R Soc Interface 2010: 7:1293-9.
35. Bryers JD. Medical Biofilms. Biotechnol Bioeng 2008: 100(1):1–18.
36. Kirketerp-Møller K, Jensen PØ, Fazli M, Madsen KG, Pedersen J, Moser C, Tolker-Nielsen T, Høiby N, Givskov M, Bjarnsholt T. Distribution, organization and ecology of bacteria in chronic wounds. J Clin Microbiol 2008: 46(8):2717-22.
37. Oh YJ, Lee NR, Jo W, Jung WK, Lim JS. Effects of substrates on biofilm formation observed by atomic force microscopy. Ultramicroscopy 2009: 109(8):874-80.
38. Leid JG, Shirtliff ME, Costerton JW, Stoodley AP. Human leukocytes adhere to, penetrate, and respond to Staphylococcus aureus biofilms. Infect Immun 2002: 70(11):6339-45.
39. Burmølle M, Webb JS, Rao D, Hansen LH, Sørensen SJ, Kjelleberg S. Enhanced biofilm formation and increased resistance to antimicrobial agents and bacterial invasion are caused by synergistic interactions in multispecies biofilms. Appl Environ Microbiol 2006: 72(6):3916-23.
40. Wenzel RP. Health care-associated infections: major issues in the early years of the 21st century. Clin Infect Dis 2007: 15(45 Suppl 1):S85-8.
41. Fonseca AP, Granja PL, Nogueira JA, Oliveira DR, Barbosa MA. Staphylococcus epidermidis RP62A adhesion to chemically modified cellulose derivatives. J Mat Sci: Mat Med 2001: 12:543-8.
EWMA Journal 2011 vol 11 no 2 12

helps healing.www.combisensation.com
Combination with innovation: HydroTac wound dressing and PütterFlex compression bandage.
When developing this CombiSensation we took our inspiration from you, as medical professionals: both products work hand in hand to treat venous leg ulcers, and are highly fl exible. The “intelligent” HydroTac wound dressing keeps dry wounds moisturised and excuding wounds dry. The PütterFlex compression bandage is so thin and fl exible that your patients can actually wear their normal shoes. These products work together to ensure the best possible medical care and maximum patient compliance – just like you.
CombiSensationProducts. Knowledge. Experience.Combine for maximum benefi t.
Working as a team for the optimum outcome. Just like our products.
Anzeige_EWMA_10_2010_v7_RZ.indd 1 25.08.2010 13:41:53 Uhr

i. Effect of chemical and physical agents on biofilmThe presence of specific substances during biofilm growth can affect it either stimulating or inhibiting formation. It is known that certain substances have a chelating effect for iron, which is important in low concentrations for sessile growth30. Another substance, indole, which is secreted by several gram negative mi-croorganisms, such as Escherichia coli, increases biofilm formation in Pseudomonas aeruginosa31. The applica-tion of electric currents, however, can inhibit biofilm development and have a synergetic activity with the an-timicrobials in the attack on biofilms32. This synergistic activity may provide a competitive advantage to the microorganisms and a real increase in the pathogenic effect of a biofilm in several diseases and infections, namely in chronic wounds, resulting in enhanced tis-sue degradation or impairment of the host immune response33. Another factor is the shear stress that affects the adhesion and biofilm formation process. In fact, the hydrodynamic conditions in which the biofilm oc-curs can influence the architecture and strength of the biofilm4. Additionally, biofilm formation can occur not only in laminar but also in turbulent flow, although it is known that for this case quorum sensing is less effective34.
d. Biofilm detection methodsThe early or even late detection of biofilms is of utmost im-portance. There are several methods to determine the pres-ence of the biofilm in vitro and in vivo in wounds isolated or in combination. Shape and size of the microorganisms in a singular or mixed culture and the eventual presence of polymorphonuclear neutrophils (PMN) in a tissue can be assessed by light microscopy35. If the microscope also has a fluorescent light it is possible to use fluorophores as stains, which absorb light emitted at a specific wavelength. If the fluorescence technique is used to stain specific components such as the DNA using peptide nucleic acids it is called Fluorescent in situ hybridization (FISH)36. It is possible, with the use of confocal laser scanning microscopy, which
allows a 3D visualization of the biological sample, and if coupled with a live/dead stain, to see the composition and distribution of living cells within the biofilm structure in vivo and in real time35. If necessary it is possible to have detailed information in the arrangement of the biofilm structures such as the type of adherence to the matrix or to a specific matrix through assessment using scanning electron microscopy (SEM), but, if available, it is also possible to have the levels of resolution of the SEM using “in vivo” conditions and studying real time effects of the antimicrobials, using atomic force microscopy (AFM)37. There is always the possibility to obtain the percentage of colony forming units, but, in the main, planktonic cells grow rather than biofilm cells. In this case special care must be taken if the biofilm is polymicrobial such in the case of wounds and if there is the possibility of the presence of anaerobic bacteria.
e. Medical importance of Biofilms Biofilms are resistance phenotypes for microorganisms that give protection to the antimicrobials35 and to the im-mune system38, namely through the effect of EPS and the slow growth rate of the microorganism within the biofilm. This biofilm ability often results in chronic infections. The close proximity of microorganisms within the biofilm cre-ates conditions for a better transference and acquisition of resistance and virulence genes35. These biofilm resistance strategies result in a huge resistance to antimicrobials as compared to their planktonic counterparts39 and under certain circumstances the detached biofilm can lead to an embolism when transported through the veins and this is definitely life threatening40.
Biofilms are often the cause of indwelling medical device associated infections. These devices, such as catheters, prosthesis, contact lenses4 etc serve as reservoirs for the microorganisms and are a source of nosocomial infections. Several species of bacteria can be biofilm forming microor-ganisms such as Staphylococcus species41, Enterococcus spe-
42. Extremina CI, Aguiar AI, Costa L, Peixe L, Fonseca AP. Optimization of processing conditions for the quantification of enterococci biofilms using microtitre-plates. J Microbiol Methods (in press).
43. Fonseca AP, Extremina C, Fonseca AF, Sousa JC. Effect of subinhibitory concentra-tion of piperacillin/tazobactam on Pseudomonas aeruginosa. J Med Microbiol 2004: 53:903-10.
44. Fonseca AP, Correia P, Sousa JC, Tenreiro R. Association patterns of Pseudomonas aeruginosa clinical isolates as revealed by virulence traits, antibiotic resistance, serotype and genotype. FEMS Immunol Med Microbiol 2007: 51:505-16.
45. Fonseca AP, Sousa JC. Effect of antibiotic-induced morphological changes on surface properties, motility and adhesion of nosocomial Pseudomonas aeruginosa strains under different physiological states. J Appl Microbiol 2007: 103:1828-37.
46. Fonseca AP, Sousa JC. Effect of shear stress on growth, adhesion and biofilm formation of Pseudomonas aeruginosa with antibiotic-induced morphological changes. Int J Antimicrob Agents 2007: 30:236-41.
47. Gaetti-Jardim Jr E, Nakano V, Wahasugui TC, Cabral FC, Gamba R, Avila-Campos MJ. Occurrence of yeasts, enterococci and other enteric bacteria in subgingival biofilm of HIV-positive patients with chronic gingivitis and necrotizing periodontitis. Braz J Microbiol 2008: 39(2):257-61.
48. Douglas LJ. Candida biofilms and their role in infection. Trends Microbiol 2003: 11(1):30-6.
49. Costerton JW, Lewandowski Z, Caldwell DE, Korber DR, Lappin-Scott HM. Microbial biofilms. Annu Rev Microbiol 1995: 49:711-45.
50. Thomas JG, Nakaishi LA. Managing the complexity of a dynamic biofilm. J Am Dent Assoc 2006: 137(3):10S-15S.
51. Dowd SE, Sun Y, Secor PR, Rhoads DD, Wolcott BM, James GA, Wolcott RD. Survey of bacterial diversity in chronic wounds using pyrosequencing, DGGE, and full ribosome shotgun sequencing. BMC Microbiol 2008: 8:43.
52. Anderson GG, O’Toole GA. Innate and induced resistance mechanisms of bacterial biofilms. Curr Top Microbiol Immunol 2008; 322:85-105.53. Borriello G, Werner E, Roe F, Kim AM, Ehrlich GD, Stewart PS. Oxygen limitation contributes to antibiotic tolerance of Pseudomonas aeruginosa in biofilms. Antimicrob Agents Chemother 2004: 48(4):2659-64.
54. Driffield K, Miller K, Bostock JM, O’Neill AJ, Chopra I. Increased mutability of Pseudomonas aeruginosa in biofilms. J Antimicrob Chemother 2008: 61(5):1053-6.
55. Phillips P, Sampson E, Yang Q, Antonelli P, Progulske-Fox A, Schultz G. Bacterial biofilms in wounds. Wound Healing Southern Africa 2008: 1(2):10-2.
56. Karatuna O, Yagci A. Analysis of the quorum sensing-dependent virulence factor production and its relationship with antimicrobial susceptibility in Pseudomonas aeruginosa respiratory isolates. Clin Microbiol Infect 2010 (Epub ahead of print).
Science, Practice and Education
EWMA Journal 2011 vol 11 no 2 14

With added portability,V.A.C.® Therapy is a snap.
Discover more: +44- (0) 800 980 8880 www.kci-medical.comNote: Specific indications, contraindications, warnings, precautions and safety information exist for KCI products and therapies. Please consult a physician and product instructions for use prior to application.
©2010 KCI Licensing, Inc. All Rights Reserved. The MEGA BLOK blocks are used with permission of MEGA Brands, Inc. All other trademarks are proprietary to KCI Licensing, Inc., its affiliates and/or licensors. For health care professionals only. CE mark pending. DSL#10-0179 (04/10)
It’s a first in simple sophistication: the ultra-portable, single-use V.A.C.Via™ Therapy System. Sleek, discreet and powered by our silent Vortis™ Pump Technology, the V.A.C.Via™ System streamlines both wound healing and patient compliance at the touch of a button. With simple features and sophisticated performance, the V.A.C.Via™ System makes wound healing easy on your patients and a snap for you.
20677_KCI_EMEA_1pg_Therapy_Via_EWMA2010.indd 1 01/09/2010 15:57:30

cies42, Pseudomonas aeruginosa10,41,43-46, Enteric bacteria47 and Candida albicans48, but most biofilms in wounds are often polymicrobial and several synergistic or antagonis-tic effects can occur between the virulence factors of the present microorganisms. For example, the Candida species produces a chemical substance that is inhibitory to quo-rum sensing in Pseudomonas aeruginosa. It is known that over 60% of chronic infections are biofilm related49. In fact biofilms are implicated in several microbial infections such as catheter infections16, ear and dental infections50, cystic fibrosis and human wounds13,51.
Biofilm composition and architecture represent key roles in resistance to antimicrobials52. Besides the singular resist-ance of each cell, the biofilm can be seen as a community that has a resistance phenotype and this starts in the begin-ning when adhesion occurs and increases with the biofilm development35. There are several mechanisms that allow the biofilm to work as a resistance phenotype: a) the oxy-gen tension, the pH and the chemical substances within can alter the activity of the antimicrobials53, b) the slow growth as a result of the low oxygen tension makes the mi-croorganisms less susceptible to the antimicrobials that are exponential growing cells, like the ß-lactams, c) the biotic or abiotic surface and the hydrodynamics (shear stress) of the biofilm formation process can select subpopulations resulting in different architectures and compositions of the biofilm, d) the close proximity of the microorganism within the biofilm creates the perfect conditions to the transfer/acquisition of genes. Additionally the microorgan-isms seem to increase their ability to mutate and this can affect the antimicrobial resistance54, e) quorum sensing molecules can regulate resistance genes but their absence does not necessarily mean a reduction in the susceptibil-ity to the antimicrobials55,56, and f) extracellular matrices (EPS) work as a physical barrier that restricts the diffusion of the antimicrobial agents into the biofilm.
2. BIOFILMS IN WOUNDS – WHY THEY ARE A PROBLEM? a. Wound formationIn the human body the frontier to the external environ-ment is the skin. This multi-layered structure is an ana-tomical barrier that also helps in the homeostatic preserva-tion, thermoregulation and protection against infection57. An additional condition of the skin is its dryness, and the ability to secrete antibodies and inhibitory substances. The skin is also the surface for the proliferation for mi-crobial normal flora that has the function of preventing the adhesion of pathogenic microorganisms58. A wound is a discontinuity of the skin that can be in more than a tissue or organ and have accidental or deliberate causes55.
b. Effect of Biofilm on wound healing – the biofilm paradigmThe pathogenicity of the microorganisms is dependent on their virulence ability within the wound. This capabil-ity of most microorganisms results from their production of toxins and enzymes, or from their biofilm production abilities. In the case of a slow reaction of the host to the biofilm, and in the particular case of an immunodefi-cient host, it increases the possibility of the development of chronic infections9,59. The PMN have little reaction against the “community resistance phenotype” called bio-film which in the case of wounds can be polymicrobial and thus quite recalcitrant. Virulent organisms, such as Pseudomonas aeruginosa and Staphylococcus aureus, when forming biofilms in vivo, show less susceptibility to anti-microbials compared to the planktonic culture60. There are two main wound microbial biofilm hypotheses that can explain why biofilms delay wound healing. The first suggests that there are specific bacterial species, despite the complexity of microbial populations within the biofilm, which are responsible for the delay in wound healing and in the overall infection process. The second argues that there is no specific bacterial species but that all the micro-bial community is responsible and the biofilm works as a
57. Church D, Elsayed S, Reid O, Winston B, Lindsay R. Burn Wound Infections. Clin Microbiol Rev 2006: 19(2):403-34.
58. Gariboldi S, Palazzo M, Zanobbio L, Selleri S, Sommariva M, Sfondrini L, Cavicchini S, Balsari A, Rimui C. Low molecular weight hyaluronic acid increases the self-defence of skin epithelium by induction of β-Defensin 2 via TLR2 and TLR4. J Immunol 2008: 181(3):2103-10.
59. Cooper R. Using honey to inhibit wound pathogens. Nurs Times 2008: 104(3): 46-9.
60. Davies CE, Hill KE, Newcombe RG, Stephens P, Wilson MJ, Harding KG, Thomas DW. A prospective study of the microbiology of chronic venous ulcers to reevaluate the clinical predictive value of tissue biopsies and swabs. Wound Repair Regen 2007: 15:17-22.
61. Bjarnsholt T, Kirketerp-Møller K, Jensen PØ, Madsen KG, Phipps R, Krogfelt K, Høiby N, Givskov M. Why chronic wounds fail to heal: a new hypothesis. Wound Repair Regen 2008: 16(1):2-10.
62. Burmølle M, Thomsen TR, Fazli M, Dige I, Christensen L, Homøe P, Tvede M, Nyvad B, Tolker-Nielsen T, Givskov M, Moser C, Kirketerp-Møller K, Johansen HK, Høiby N, Jensen PØ, Sørensen SJ, Bjarnsholt T. Biofilms in chronic infections – a matter of opportunity – monospecies biofilms in multispecies infections. FEMS Immunol Med Microbiol 2010: 59:324-36.
63. Thomsen TR, Aasholm MS, Rudkjøbing VB, Saunders AM, Bjarnsholt T, Givskov M, Kirketerp-Møller K, Nielsen PH. The bacteriology of chronic venous leg ulcer examined by culture-independent molecular methods. Wound Repair Regen 2010: 18(1):38-49.
64. Wolcott RD, Kennedy JP, Dowd SE. Regular debridement is the main tool for maintaining a healthy wound bed in most chronic. J Wound Care 2009: 18(2):54-6.
65. Leake JL, Dowd SE, Wolcott RD, Zischkau AM. Identification of yeast in chronic wounds using new pathogen-detection technologies. J Wound Care 2009: 18(3):103-4, 106, 108.
66. Fazli M, Bjarnsholt T, Kirketerp-Møller K, Jørgensen B, Andersen AS, Krogfelt KA, Givskov M, Tolker-Nielsen T. Non-random distribution of Pseudomonas aeruginosa and Staphylococcus aureus in chronic wounds. J Clin Microbiol 2009: 47(12):4084-9.
67. Prompers L, Schaper N, Apelqvist J, Edmonds M, Jude E, Mauricio D, Uccioli L, Urbancic V, Bakker K, Holstein P, Jirkovska A, Piaggesi A, Ragnarson-Tennvall G, Reike H, Spraul M, Van Acker K, Van Baal J, Van Merode F, Ferreira I, Huijberts M. Prediction of outcome in individuals with diabetic foot ulcers: focus on the differ-ences between individuals with and without peripheral arterial disease. The EURODIALE study. Diabetologia 2008: 51(5):747-55.
Science, Practice and Education
EWMA Journal 2011 vol 11 no 2 16

Finally closed.sorbion – the future in modern wound care.
We care for your wounds.Day by day.
www.sorbion.com
AG
-BS-
1372
-03/
11
NEW
Join our
EWMA Symposium
on Wednesday, May 25th
12:30 – 13:30 pm
For further information about our products, please visit us at stand 27 in the exhibition hall.
AZ_EWMA_Dachmarke_210x297+3.indd 1 29.04.11 08:46
EWMA2011Brussels · Belgiumwww.ewma2011.org

unit. Both theories are important to explain the wound healing process and need to be proven, so both may be taken into account by practitioners considering wound management strategies33.
The biofilm in the chronic wound is composed of a com-munity of microorganisms in which the overall effect in the community unit is greater than the sum of its singular or specific parts33, thus an important approach to promote wound healing could be to enable an “ecological shift” that increases growth of non-problematic bacteria. This could be a prevention approach with the development of tech-niques to continuously avoid the predominance of patho-genic bacteria within the biofilm. This could involve the use of probiotics and the idea of helpful biofilm in wound healing33. It is therefore of utmost importance to control the microbial progression during wound healing and to maintain “healthy” biofilms, thus avoiding the develop-ment of pathogenic biofilms. If the biofilm community pathogenic effect exceeds host immune response, there is a compromised wound healing process33,61.
3. HOW CAN BIOFILMS BE TREATED?a. Diagnosis of biofilms in wounds The diagnosis of wound infection is mainly done on the basis of clinical symptoms but it was demonstrated that the microbial load of wound samples can be higher than 1 x 105 microorganisms/g of tissue with no signs of clini-cal infection, thus showing an urgent need for revision of the established guidelines for wound infections diagnosis. There are cases of chronic wound infections that progress to septicemia or even death because they fail to show clini-cal symptoms55. Recently, it has been shown that using culture-dependent methods in the wound microorganisms enable the isolation and identification of only 5% of the bacterial species, thus biopsy samples are a better option to have accurate information on the microbial diversity in the biofilms13. Besides an improved sampling technique,
there is the emergence of molecular biology methods9,62, but the best option is perhaps the combination of cultiva-tion/molecular methods63.
There are several microorganisms that are predominant in the biofilms that cause chronic wounds and these include fastidious or anaerobic biofilm growing bacteria such as Staphylococcus, Pseudomonas, Serratia, Bacteroides, and Corynebacterium64.
The identification of the biofilm bacteria in wounds can be assessed using several molecular methods such as fingerprinting, using 16S rRNA, fluorescence in situ hy-bridization (FISH), pyrosequencing and quantitative PCR (Q-PCR)51,64. This last method enables a characteriza-tion within a few hours of the microorganisms present in wounds and has already been used to demonstrate that the numbers of certain bacteria such as P. aeruginosa and S. aureus varies between samples which are taken in dif-ferent locations in the same wound63. But if detection of the relative contribution of the bacteria or yeast is needed in a chronic wound sample, pyrosequencing methods are recommended, although they only give return results in 24 hours65. The use of rRNA gene based PCR techniques, that is using Q-PCR and pyrosequencing, gives informa-tion regarding presence of viable and nonviable bacteria, prevalence and type of bacterial species, but there is no information concerning the structural organization and spatial distribution of the bacteria in the biofilm nor even any information on the relative contribution of each bac-teria to the disease pathogenesis. This can be obtained by visualization of the bacterial communities that exist in the wound biofilms by using FISH with species-specific peptide nucleic acid-PNA DNA probe plus a PNA probe for all eubacterial species. Burmølle et al (2010)62 describe the use of a combination of PNA-FISH and confocal laser scanning microscopy (CLSM) to assess the spatial dis-tribution and structural organization of biofilm bacteria in chronic wounds62,66. The combined method demon-strated that the microbial communities in chronic wounds
68. Yasuhara H, Hattori T, Shigeta O. Significance of phlebosclerosis in non-healing ischaemic foot ulcers of end-stage renal disease. Eur J Vasc Endovasc Surg 2008: 36(3):346-52.
69. Hunt TK. Hyperbaric Oxygen and Wounds: A tale of two enzymes. EWMA J 2010: 10(2):7-9.
70. Rhoads DD, Wolcott RD, Percival SL. Biofilms in wounds: management strategies. J Wound Care 2008: 17(11):502-8.
71. Wolcott RD, Ehrlich GD. Biofilms and chronic infections. J Am Med Assoc 2008: 299(22):2682-4.
72. Schultz GS, Barillo DJ, Mozingo DW, Chin GA. Wound bed preparation and a brief history of TIME. Int Wound J 2004: 1(1):19-32.
73. Wolcott RD, Rumbaugh KP, James G, Schultz G, Phillips P, Yang Q, Watters C, Stewart PS, Dowd SE. Biofilm maturity studies indicate sharp debridement opens a time-dependent therapeutic window. J Wound Care 2010: 19(8):320-8.
74. Hofman D. The autolytic debridement of venous leg ulcers. Wound Essentials 2007: 2:68-73.
75. Armstrong DG, Salas P, Short B, Martin BR, Kimbriel HR, Nixon BP, Boulton AJM. Maggot therapy in “lower-extremity hospice” wound care; fewer amputations and more antibiotic-free days. J Am Podiatr Med Assoc 2005; 95(3):254-7.
76. Andersen AS, Jøergensen B, Bjarnsholt T, Johansen H, Karlsmark T, Givskov M, Krogfelt KA. Quorum-sensing-regulated virulence factors in Pseudomonas aerugi-nosa are toxic to Lucilia sericata maggots. Microbiology 2009; 156:400-7.
77. Marazzi M, Stefani A, Chiaratti A, Ordanini MN, Falcone L, Rapisarda V. Effect of enzymatic debridement with collagenase on acute and chronic hard-to-heal wounds. J Wound Care 2006: 15(5):222-7.
78. Cowan T. Biofilms and their management: implications for the future of wound care. J Wound Care 2010: 19(3):117-20.
79. Bratzler DW, Houck PM, Richards C, Steele L, Dellinger EP, Fry DE, Wright C, Ma A, Carr K, Red L. Use of antimicrobial prophylaxis for major surgery: baseline results from the national surgical infection prevention project. Arch Surg 2005: 140(2): 174-82.
80. Lipp C, Kirker K, Agostinho A, James G, Stewart P. Testing wound dressings using an in vitro wound model. J Wound Care 2010: 19(6):220-6.
81. Presterl E, Suchomel M, Eder M, Reichmann S, Lassnigg A, Graninger W, Rotter M. Effects of alcohols, povidone-iodine and hydrogen peroxide on biofilms of Staphylo-coccus epidermidis. J Antimicrob Chemother 2007: 60:417-20.
82. Demling RH, Burrell RE. The beneficial effects of nanocrystalline silver as a topical antimicrobial agent. Leadership Medica 2002: 16(7).
Science, Practice and Education
EWMA Journal 2011 vol 11 no 2 18

* At smith&nephew we seek imaginative solutions that improve wound outcomes for patients and at the same time conserve resources for healthcare systems.
How is it possible to achieve better patient outcomes and reduce costs? Join us for our symposia on the 25 and 26 May 2011 which will be held at EWMA 2011 in Brussels.
Symposium B
Reducing the human and economic cost of wounds - Part II
SpeakersProf John PosnettProf Patricia PriceDr Roland BeckerDr John LantisDate: Thursday, 26th MayTime: 16.00 - 17.00Venue: Silver Hall
Symposium A
Reducing the human and economic cost of wounds - Part I
Speakers: Prof John PosnettProf Christine Moffatt Prof Donald Hudson
Date: Wednesday, 25th MayTime: 12.30 - 13.30Venue: Gold Hall
Visit us at the Smith & Nephew booth and interactive educational area, at the exhibition hall booth stand number 6!
See you in Brussels! For patients. For budgets. For today.™
™Trademark of Smith & Nephew27892

Science, Practice and Education
are often polymicrobial but the bacterial aggregates are mainly composed of a single bacterial species62. Fazli et al (2009)66 showed by using PNA- FISH and CLSM there is a nonrandom distribution of the bacteria in wounds, for example P. aeruginosa is primarily at the deepest part and S. aureus is often near the surface. Dowd et al (2008)51 de-scribed some repeated patterns of coaggregation that have the ability to work in synergy to produce chronic infection as “functional equivalent pathogroups” (FEPs).The above referred techniques are complex and limited to research laboratories, thus there is a need to develop simpler means of detecting biofilms in a routine microbiology diagnostic.
b. Biofilm Treatments for chronic wounds Patient quality of life can be affected by a delayed wound healing process, thus the wound treatment aims to achieve its goal within a reasonable time frame. This is possible if appropriate care is taken and attention paid to the condi-tion of the wound and of the patient55.
Some predisposing factors such as underlying dis-eases67,68 and microbial infection with biofilm forming organisms51 can influence the healing process of infected and chronic wounds. There are several strategies targeted towards promoting wound healing in chronic wounds and they must take into account the factors that are responsible for the delay in the healing process. These factors should be identified as soon as possible to prevent complications. Nevertheless, if complications occur there are treatment strategies that range from using ultrasounds, debridement, negative pressure, hyperbaric oxygen69, and others70.
First of all, foreign bodies should be removed from the wound because their presence interferes with the healing process, thus a physical intervention is of utmost impor-tance for the management of biofilms71. This cleansing can be done by mechanical, chemical or biological methods. Additionally the presence of devitalized tissue serves as a nutritional matrix for microbial development and prolif-eration, thus removal of foreign bodies and devitalized tissue must be done and the process is called debride-ment. This technique cannot avoid the ability of the bio-
film to reconstitute itself, thus topical antimicrobial and antibiofilm strategies should be considered72, but during this recovery process the biofilm is more vulnerable to antimicrobials because it needs to reform its extracellular polymeric substances, increase cell division and colony activity64. Wolcott et al (2010)73 showed that debridement or post-debridement opens a time-dependent therapeutic window of increased antibiotic sensitivity which is 24-48 hours for P. aeruginosa.
In the wounds there is an autolytic debridement when the healing process is developing in the right timeframe and this process only functions when the wound is moist and the patient’s own enzymes can be used74. Debridement can also be done by larvae which feed on the dead tissues and excrete bactericidal products that help to reduce the wound’s bioburden75, although Andersen et al (2009)76 did describe the death of the larvae by P. aeruginosa quo-rum sensing molecules. There is also the possibility of a more selective debridement by using enzymes for the di-gestion of the slough of a wound and they can be obtained from microorganisms such as collagenase or fibrinolysin or from urea and papain or even plants77. In particular cases there is a need for removal of large amounts of necrotic tissue and this demands a more extreme course of action such as a surgical procedure78.
Treatment of biofilms in wounds often needs the use of antimicrobials in a systemic and/or topical therapy. An-timicrobials can also be used for prophylactics especially in immunocompromised patients79, but the correct pro-cedure is to identify the microorganisms involved and to determine antimicrobial susceptibility, although the information is always reduced because they are determined with planktonic, not sessile populations.
Antimicrobials can be administered topically as wound dressings80, orally, or injected intravenously or subcutane-ously and the main objective is to reduce or even com-pletely remove the microbial load of wounds78. Several
83. Russell AD, Hugo WB. Antimicrobial activity and action of silver. Prog Med Chem 1994: 31:351-70.
84. Knight GM, McIntyre JM, Craig GG, Mulyani, Zilm PS, Gully NJ. Inability to form a biofilm of Streptococcus mutans on silver fluoride- and potassium iodide-treated demineralised dentin. Quintessence Int 2009: 40(2):155-61.
85. Okhiria OA, Henriques AFM, Burton NF, Peters A, Cooper RA. Honey modulates biofilms of Pseudomonas aeruginosa in a time and dose dependent manner. J ApiProduct & ApiMedical Sci 2009: 1(1):6-10.
86. Molan PC. The evidence supporting the use of honey as a wound dressing. Int J Low Extrem Wounds 2006: 5(1):40-54.
87. Merckoll P, Jonassen TØ, Vad ME, Jeansson SL, Melby KK. Bacteria, biofilm and honey: A study of the effects of honey on ‘planktonic’ and biofilm-embedded chronic wound bacteria. Scand J Infect Dis 2009: 41:341-7
88. Extremina CI, Freitas da Fonseca A, Granja PL, Fonseca AP. Anti-adhesion and anti-proliferative cellulose triacetate membrane for prevention of biomaterial centered infections associated to Staphylococcus epidermidis. Int J Antimicrob Agents 2010: 35:164-8.
89. Thomas S, McCubbin P. A comparison of the antimicrobial effects of four silver-containing dressings on three organisms. J Wound Care 2003: 12(3):101-7.
90. Pietschmann S, Hoffmann K, Voget M, Pison U. Synergistic effects of Miconazole and Polymyxin B on microbial pathogens. Vet Res Commun 2009: 33:489-505.
91. Stewart PS, Costerton JW. Antibiotic resistance of bacteria in biofilms. Lancet 2001: 358(9276):135-8.
92. Katsuyama M, Kobayashi Y, Ichikawa H, Mizuno A, Miyachi Y, Matsunaga K, Kawashima M. A novel method to control the balance of skin microflora Part 2. A study to assess the effect of a cream containing farnesol and xylitol on atopic dry skin. J Dermatol Sci 2005: 38(3):207-13.
93. Kaneko Y, Thoendel M, Olakanmi O, Britigan BE, Singh PK. The transition metal gallium disrupts Pseudomonas aeruginosa iron metabolism and has antimicrobial and antibiofilm activity. J Clin Invest 2007: 117(4):877-88.
94. Martineau L, Dosch H-M. Biofilm reduction by a new burn gel that targets nocicep-tion. J Appl Microbiol 2007: 103:297-304.
95. Itoh Y, Wang X, Hinnebusch BJ, Preston JF 3rd, Romeo T. Depolymerization of beta-1,6-N-acetyl-D-glucosamine disrupts the integrity of diverse bacterial biofilms. J Bacteriol 2005: 187(1):382-7.
96. Gill AL, Bell CNA. Hyperbaric oxygen: its uses, mechanisms of action and outcomes. Q J Med 2004: 97:385-95.
EWMA Journal 2011 vol 11 no 2 20

COVIDIEN, COVIDIEN with logo, Covidien logo and positive results for life are U.S. and internationally registered trademarks of Covidien AG.
Other brands are trademarks of a Covidien company. ©2010 Covidien.
Covidien (UK) Commercial Ltd.154 Fareham RoadGosport, HampshirePO13 OAS, UK
+44(0)1329 224226/224411 (T)+44(0)1329 224334/224390 (F)[email protected].
www.covidien.com
To request a free product sample of the new Kendall™ AMD antimicrobial foam border dressing please visit:
www.KendallAMDFoam.com
NEW!
A great step forward in the treatment of acute and chronic wounds:
Kendall™ AMD antimicrobial foam border dressings
Designed to manage bacteria, moisture and friction.
New Kendall AMD antimicrobial foam border
dressings provide a balanced environment to help
promote wound healing.
• Low friction, high MVTR (Moisture Vapour
Transmission Rate) topsheet provides a waterproof
microbial barrier designed to allow movement without
transferring force to the periwound tissue
• Microstructured open-cell foam impregnated with
0.5% PHMB (Polyhexamethylene Biguanide) providing
maximum fluid absorbency while PHMB kills bacteria –
without resistance.
• Patented “landing zone” facilitates absorption,
minimizes periwound maceration, and prevents dead space
by swelling directionally into the wound.
AMD Foam Border_UK.indd 1 12/23/10 8:12 AM

antiseptics, such as Povidone iodine, can be used alone or in combination with the antibiotics in order to achieve increased antimicrobial activities81. In fact one of the pos-sible advantages of using antiseptics is the reduced prob-ability of developing bacterial resistance since they have several targets in the bacteria.
The use of silver as part of dressings has also proved to be successful, and this is due to the bactericidal proper-ties of silver82, as already reported for silver catheters83. Silver lethal activity works at much higher concentrations for sessile bacteria as compared to planktonic bacteria84. Another known antiseptic is honey, which is claimed to have antibacterial activity through the action of its phyto-chemicals and the ability to promote healing85-87.
Several works have demonstrated the importance of drug release in the prevention of biofilm formation88 and it is known that the rate of antimicrobial release from a dress-ing or catheter determines its efficacy89. Combinations of antimicrobials with synergistic activity can be used as in the case of bacitracin-polymyxin90 because there are major difficulties in having an effect on dormant cells within the biofilm91. Another issue is that systematic antibiotics have only 25-32% efficacy against biofilms70 because they only suppress rapidly growing cells at the outermost active edges of the biofilm91.
It is of utmost importance to combine strategies, i.e. combining the use of debridement and antibiotics, and especially those with antibiofilm abilities. There are a number of well-known antibiofilm agents, some of which have already been referred to during this review, like Lacto-ferrin and the use of phages and pulsed electric fields, but there are others such as Xylitol, Gallium, EDTA, Dispersin B, as well.92. Gallium can disrupt Fe-dependent proc-esses because many biological systems cannot distinguish Ga3+ from Fe3+ and this is particularly important for P. aeruginosa biofilm development93. Martineau and Dosch (2007)94 have recently described that EDTA in a wound gel can have some efficacy against P. aeruginosa biofilms. Dispersin B targets the EPS and degrades the community structure of the biofilm95.
As a conclusion, in order to suppress and eliminate bio-films, a triple strategy should be used incorporating topical antiseptics and systemic antibiotics for damaging of cell metabolism and integrity, using antibiofilm antimicrobi-als that act in the biofilm as a microbial community that works together in a “resistance phenotype”70 and using a strategy that augments the host’s defenses95. Alongside the triangle of antimicrobial – pathogenic agent – host, we must consider the environment in which all three work to-gether and this can be also used to enhance wound healing. An example of this is the use of topical oxygen therapy that involves the use of supersaturated oxygen delivered to the wound over a certain time period which increases protein production and cell homeostasis60. Another example is the use of hyperbaric oxygen therapy that supplies adequate tissue oxygenation96.
Prevention of biofilm should be the first and impor-tant aim of any strategy for infection control. Nevertheless with biofilm therapeutic measures, care should be taken in order to reduce the quantity of the microorganisms as well as the virulent factors they express allowing a better and facilitated work for the immune system97.
Several studies show that there are pathogens that can form biofilms within 10-16 h of culture45 and this ability has been reported in vivo in animal for 48-72 hours35. This ability of some pathogens to easily form biofilm in wounds should be stopped in the early step of the initial adhe-sion, and this is particularly important in immunocom-promised hosts. In this case the use of natural substances that stimulate cellular growth may promote enhancement of regenerative process as is the case in the use of bone marrow-derived cells98 or stem cells99. Another strategy to control biofilms is the use of phages to which particularly the young biofilms seem to be more susceptible100. Lactof-errin is a protein present in the gingival fluids and in saliva that has iron-binding properties. This ability is particularly important in the case of Pseudomonas aeruginosa wound biofilms, since they need iron for their stability. The use of Lactoferrin can interfere with normal biofilm formation
97. Percival SL, Cutting KF. Biofilms: possible strategies for suppression in chronic wounds. Nurs Stand 2009: 23(32):64-72.
98. Badiavas EV, Falanga V. Treatment of chronic wounds with bone marrow -derived cells. Arch Dermatol 2003; 139:510-6.
99. Branski LK, Gauglitz GG, Herndon DN, Jeschke MG. A review of gene and stem cell therapy in cutaneous wound healing. Burns 2009: 35(2):171-80.
100. Sillankorva S, Neubauer P, Azeredo J. Pseudomonas fluorescens biofilms subjected to phage phiIBB-PF7A. BMC Biotechnol 2008: 8:79.
101. Wakabayashi H, Yamauchi K, Kobayashi T, Yaeshima T, Iwatsuki K, Yoshie H. Inhibitory effects of Lactoferrin on growth and biofilm formation of Porphyromonas gingivalis and Prevotella intermedia. Antimicrob Agents Chemother 2009: 53(8):3308-16.
102. Bjarnsholt T, Jensen PØ, Rasmussen TB, Christophersen L, Calum H, Hentzer M, Hougen H, Rygaard J, Moser C, Eberl L, Høiby N, Givskov M. Garlic blocks quorum sensing and promotes rapid clearing of pulmonary Pseudomonas aeruginosa infections. Microbiology 2005: 151:3873-80.
103. Alipour M, Suntres ZE, Lafrenie RM, Omri A. Attenuation of Pseudomonas aeruginosa virulence factors and biofilms by co-encapsulation of bismuth–ethan-edithiol with tobramycin in liposomes. J Antimicrob Chemother 2010; 0:dkq036v1-dkq036.
104. Cooper RA, Okhiria O. Biofilms, wound infection and the issue of control. Wounds UK 2006: 2(3):52-61.
105. Uhlemann C, Heinig B, Wollina U. Therapeutic ultrasound in lower extremity wound management. Int J Low Extrem Wounds 2003: 2(3):152-7.
106. Petrofsky JS, Lawson D, Berk L, Suh H. Enhanced healing of diabetic foot ulcers using local heat and electrical stimulation for 30 min three times per week. J Diabetes 2010: 2:41-6.
107. Charles CA, Ricotti CA, Davis SC, Mertz PM, Kirsner RS. Use of tissue-engineered skin to study in vitro biofilms. Dermatol Surg 2009: 35(9):1334-41.
108. Kanno E, Toriyabe S, Zhang L, Imai Y, Tachi M. Biofilm formation on rat skin wounds by Pseudomonas aeruginosa carrying the green fluorescent protein gene. Exp Dermatol 2010: 19(2):154-6.
Science, Practice and Education
EWMA Journal 2011 vol 11 no 2 22

allowing improved efficacy in the antimicrobial action101. Another biofilm control measure is to use substances that can interfere in the cell to cell communication, namely by quorum sensing attenuation26. Garlic has been used for the rapid clearance of P. aeruginosa from the lungs of mice models102. Synergistic activity has been reported between tobramycin and bismuth against P. aeruginosa quorum sensing, virulence factors and biofilm formation ability103. Several studies have demonstrated in vitro that the use of honey can influence biofilm formation85 there-by having the possibility of topical application in wound management104. Another strategy is to disrupt the biofilm in wounds by using ultrasound105, electric stimulation or electromagnetic therapy106.
In order to evaluate potential biofilm interventions there is a need for the development of biofilm mod-els13,107,108, however before effective anti-biofilm inter-ventions are accepted there is a need for clinical evidence of biofilm associated infections.
CONCLUSION REMARKS AND FUTURE WORKThe increased number of chronic wounds in ageing popu-lations is a major problem. The knowledge of the relation between the concepts of wound chronicity and biofilm is of utmost importance. It is therefore crucial to develop means to diagnose biofilm infections, and there is a strong need for effective treatment strategies. However it should be stated that there are no routine biofilm detection meth-ods available yet and effective interventions depend on the quality of the diagnosis.
It is certainly possible to explain, under a biofilm para-digm, the delay in chronic wound healing, therefore the biofilm communities must be identified as soon as pos-sible as well as their distribution within the biofilm, but more information regarding their specific contribution to the pathogenesis is fundamental for the selection of adequate therapeutic methods. The debridement or post-debridement of chronic wounds can induce a restart in the biofilm formation and this can create a window of opportunity that should be exploited using a combination of methods, within an antibiofilm strategy. The relative predominance of pathogens in the biofilm community can also be avoided by promoting the shift to healthy biofilm that can be an easier target for host defenses. m
AcknowledgementsI gratefully acknowledge to Dr. Clara Extremina from REQUIMTE, Faculdade de Farmácia, Universidade do Porto and to Professor A. Freitas da Fonseca, for the critical review of the manuscript.
The compact lightweight the complete solution for wound drainage
With the next generation of the ATMOS S 041 Wound you get a solution for sensor-controlled wound drainage at a fair price!
Please ask for further information.
N E W Now with intermittent function
S i l e n t . G e n t l e . P o w e r f u l .
ATMOS MedizinTechnik GmbH & Co. KG Ludwig-Kegel-Str. 12, 14-16, 18 79853 Lenzkirch / GermanyTel: +49 7653 689-374 | Fax: +49 7653 [email protected] | www.atmosmed.com
EWMA Journal 2011 vol 11 no 2

SOON YOU WON’T BE ABLE TO IMAGINE A WORLD WITHOUT
IMAGINE A WORLD WITHOUT WHEELS...
www.systagenix.comSYS/GLO
/451/0311
Systagenix are pleased to announce the name of our soon to be launched test for elevated Protease activity, WOUNDCHEK™ Protease Status. Come and see us at EWMA, May 25-27 2011 in Brussels when we’ll have more to share with you on the arrival of WOUNDCHEK™ Protease Status.
In the meantime, find out why you need to get involved by going to www.proteasemarker.com or email us at [email protected] to request a FREE ‘Do you know your Proteases?’ information pack.
WATCH THIS SPACE!

Sarah E Bradbury, MSc
Research Nurse, Cardiff University
Patricia E Price, PhD
Professor and Dean of Healthcare Studies, Cardiff UniversityDepartment of Dermato logy and Wound Healing, Cardiff University
Correspondence: Sarah Bradbury Research NurseDept. of Dermatology and Wound HealingRoom 13 Upper Ground FloorSchool of MedicineHeath ParkCardiff
Conflict of interest: None
Science, Practice and Education
ABSTRACTBackground: Diabetic foot ulcers (DFU) are often considered painless due to sensory peripheral neu-ropathy, with pain only occurring with infection or other complications (Sibbald et al., 2006). Re-cent research suggests DFU pain is more prevalent than expected and severely impacts on quality of life (Ribu et al., 2006; Bengtsson et al., 2007).Aim: To explore the effect of specific DFU pain on life quality from the patient’s perspective.Methods: Purposive sampling identified three patients from a specialist DFU clinic. Data was collected using semi-structured interviews. Inter-views were recorded, transcribed and analysed using thematic content analysis. Results: Four themes emerged: Experience of Pain; Physical Effects of Pain; Coping, Support and Social Impact; and Psychological Impact. Re-sults indicated that DFU pain affected patients physically and psychologically, especially with re-gards to sleep, mobility and social roles. Feelings of depression, isolation and loss of independence were expressed. Pressure from footwear and dress-ing changes caused or worsened DFU pain. Conclusions: DFU pain is an under-recognised phenomenon which can be both severe and debili-tating, and also negatively impact on life quality across physical and psychosocial domains. Further qualitative work into the patients’ lived experi-ences of DFU pain is needed to help clinicians understand the relevance to holistic diabetic foot care and service provision.
INTRODUCTIONDiabetic Foot Ulcer (DFU) pain is a phenomenon which has been both under-estimated and under-researched. The exploratory study published in part one of this article on the presence and char-acteristics of DFU pain found that patients can experience specific DFU pain despite the pres-ence of neuropathy, and not always related to Decorrelated complications. This supported the findings of previous works1,2. A second phase was therefore conducted within the same study
to investigate the impact of specific DFU pain on quality of life (QoL).
Previous research has indicated that DFUs nega-tively impact on QoL3,4,5, as does pain from vari-ous causes6,7,8,9. DFU can significantly decrease QoL for a variety of reasons, including decreased mobility, diminished independence, loss of employment, increased risk of amputation and repetitive trips to clinicians for care10. Despite this, there is relatively little research in this area. Although pain is often raised as an issue in stud-ies on DFU and QoL, none have looked specifi-cally at DFU pain and QoL from the patient’s perspective.
Ribu et al.1 evaluated health-related quality of life (HRQoL) as part of their research into DFU pain using generic and disease-specific measurement tools. Results found that patients experiencing DFU pain had consistently low scores in both physical and psychological domains.
A qualitative study on the patient’s perspective of living with a DFU identified pain as one of six commonly experienced problems11. Almost all patients experienced pain at some time, with most reporting ulcer pain woke them at night and having to lie in certain positions to avoid pres-sure on the ulcer. Pain was reported when walk-ing even short distances. Three patients avoided taking analgesia due to fear of reliance. Pain was mainly discussed in relation to painful neuropa-thy, although direct relationship with the ulcer or other causes was not considered. The effect of the pain in causing sleep deprivation and fatigue affecting overall QoL was highlighted.
Pain was raised as a significant factor in a phenom-enological study12 to determine the QoL issues of 21 patients with DFUs. Just under half of the patients complained of ulcer pain impairing their ability to walk, discomfort on lying down and during dressing changes. The authors felt unable
Diabetic foot ulcer pain:
The hidden burden (Part two)
EWMA Journal 2011 vol 11 no 2 25

to confirm that pain was definitely originating from the ulcer rather than an underlying pathology, but it suggests that patients feel they are experiencing ulcer pain which is impairing their QoL. A comparable study by Watson-Miller13 yielded similar results.
Other studies also found patients with DFU experi-enced pain, but did not further explore the nature of that pain or its specific impact on QoL4,14,15.
Despite providing useful information on the effect of DFU on HRQoL, studies generally have small sample sizes and the subject would still benefit from further research. The difficulty with measuring HRQoL with specific regard to foot ulcers in diabetic patients is that they often do not experience only one complication of the disease in isolation. This can make it difficult to determine with certainty that it is the ulcer that is affecting QoL, espe-cially in studies which do not exclude patients with other diabetic complications. The lack of disease-specific tools for DFU until relatively recently may also have hindered progress within this field – as Vileikyte16 stated, the effects of DFU on HRQoL are distinct from those associated with the disease itself and need to be addressed separately.
Overall, it is clear from the qualitative work under-taken, which allows the patients to voice their individual difficulties and experiences, that pain is an important contributor to reduced QoL for patients with DFU. Un-fortunately, QoL studies related to DFU generally do not provide enough detail on the effect of pain as this is not their primary aim. Substantial conclusions cannot be drawn from their results with relation to pain, but they do provide a useful overview and some insight into the nature and degree of the problem, thereby justifying the need for more specific work.
The need for further research on the subject of pain from DFU and QoL was thus identified to determine the extent to which the problem needs consideration in clinical practice.
METHODSAn exploratory research design was continued in this phase using qualitative methods.
Participants were chosen using purposive sampling from the same local specialist diabetic foot clinic as in
phase one. Basic inclusion/exclusion criteria were used to assess if a participant was suitable (Table 1).
Face-to-face semi-structured interviews were consid-ered an appropriate method to collect qualitative data on the effect of DFU pain on everyday life. An interview schedule was developed to guide the conversation onto relevant topics based on the study aims and issues identi-fied within the literature, but with a particular focus on pain. The first interview acted as a pilot of the sched-ule to determine if the questions were valid and easy to understand, and to gain insight into how the questions were interpreted by patients to try to improve reliability. Following this the interview schedule was shortened and revised to include broader topic areas.
The interviews were recorded and manually tran-scribed. Reflective notes were also made shortly after com-pleting the interview recording any non-verbal communi-cation, the researcher’s thoughts on the topics covered and the response of the participant to ensure the best quality information was assembled for analysis.
The study protocol was approved by the Local Re-search Ethics Committee. Confidentiality and anonym-ity were maintained throughout the research process, and written informed consent was taken. Identification of suitable participants and completion of the interviews occurred over a six month period. All participants chose to be interviewed at home, and each interview lasted ap-proximately 30 minutes.
The taped conversations were transcribed by the re-searcher and then verified by a second researcher not in-volved with the interviews. A copy was sent to the appro-priate participant for verification and to make any required changes or additions. These processes were performed to improve reliability and minimise bias within the study findings. The transcribed and verified data was then ana-lysed using thematic content analysis, guided by elements of the method published by Burnand 17.
In an effort to demonstrate methodological rigour and reduce researcher bias, the identified data categories were checked by a second researcher to ensure the primary inter-pretation fairly represented the data. The themes were then examined to identify any associated relationships which were discussed and compared.
Table 1
Inclusion criteria Exclusion criteria
Over eighteen years of age Dementia or learning/communication difficulties
Experience of specific DFU pain
Willing to participate in an interview
Able to fully understand and give informed consent
Science, Practice and Education
EWMA Journal 2011 vol 11 no 2 26

If your patients have wounds that are slow to heal, Abound® may help.
Wound healing as easy as 1-2-3:
1 2Abound® is a one-of-a-kindtherapeutic nutrition productintended to benefit people who need nutrition therapy forhard-to-heal wounds.
Oral consumption ortube-feeding of Abound® isan important part of totalcare for wound healing; it is used along with a dietdesigned for wound healingand proper wound care.
Abound® is a unique blend of 3 key ingredients–arginine, glutamine, andHMB*–working together to help support wound healing.
*HMB, Beta-hydroxy-beta-methylbutyrate
3
After surgical debridement on a 7-month-old foot ulcer
Two weeks on Abound® Eight weeks on Abound®
People who may benefit from Abound®
include those with:• Pressure ulcers, venous leg ulcers, and diabetic foot ulcers
• Burn injuries
• Non-healing surgical incisions
Ask your Abbott sales representative for more information
about how you can use Abound® to turn science to caring.
Rebuild. Recover. Resume. Live life again.
Slows Protein
Breakdown
Enhances Tissue Growth
HMB
Glutamine
Arginine© 2008 Abbott Laboratories Use under medical supervision5001 0908 0017 A1
Abound EWMA Ad-FullPg 4/13/10 1:37 PM Page 1

RESULTSThree patients were recruited between September 2007 and January 2008. The intended sample was five patients but, mainly due to the time delay while waiting for eth-ics approval, a number of patients achieved ulcer healing and were discharged, or no longer had pain in their ulcer. Some patients refused to participate.
The study sample, again although small, presented views from a male and female perspective (Table 2). The type and duration of diabetes and ulcer aetiology and duration were similar across the group. All the patients had complex medical histories consisting of independent diseases and diabetes-related complications, which could impact on QoL. The interview data will be presented using the four themes generated during analysis.
Experience of PainThis theme was generated from the patient’s descriptions of their pain, when it occurred, the factors that caused it or made it worse and how they managed it.
Participants described their pain in various ways – sharp, unexpected, variable in occurrence but of severe intensity, intermittent, spontaneous, continuous and un-relenting. One described it “...as if my foot were in a bed of stinging nettles”, while another stated it was the worst he’d ever had.
None of the patients seemed surprised to be experienc-ing pain, despite having peripheral neuropathy. One felt that pain could even be a good sign, while another was more surprised at its severity.
The main issue consistently raised relating to factors that increased or worsened pain was application of pressure on the wound, especially during dressing changes and from footwear. All patients described pain occurring in bed due to pressure from bedclothes or moving to lie on the ulcer:
“…I can’t sleep in bed, I can’t stand blankets or anything on the foot”.
Two patients having dressings changed by family members stated it was not terribly painful, except during cleansing and if the dressing had ‘dried out’.
The patient having dressings changed by District Nurs-es remarked that cleansing could be painful, but felt the pain at was more dependent on the individual performing it, describing some as ‘rough-handed’. He also experienced pain during dressing application and for some time after-wards: “If anybody touches it, it’s hell”.
Difficulty finding footwear that did not exert pressure and cause pain was expressed by two patients. Both had bought their own shoes or found solutions, but not always ideal ones, such as wearing sandals throughout the winter. One was particularly frustrated with the service provided by the hospital:
“The shoes they make are too heavy and are no good to me, but I can’t make them understand that”; “…they bruised all my feet and aggravated the toe”.
Analgesia was used by all three participants for pain man-agement. Two took a codeine-based preparation which helped decrease their pain most of the time, although one felt the pain never went away entirely. This patient was reluctant to take increased or further analgesia due to poly-pharmacy. The third patient was taking multiple forms of analgesia, including Morphine tablets and liquid, an anti-epileptic for neuropathic pain and Paracetamol, but still experienced uncontrolled ulcer pain:
“…the medicine I’m taking is not touching me…”; “… If I could find a tablet or a medicine that could take it away just for a few hours, I’d be more than happy”.
He had previously overdosed on Oramorph in des-peration to get rid of the pain, leaving him feeling ill for several days. When discussing a previous possibility of having the leg amputated due to a back condition and reduced circulation, he felt that at times amputation would be preferable to continuing in such pain from his ulcer:
“I suppose that’s the worst I can look forward to, but if it can get rid of that [pointing at the ulcer]…I know it sounds stupid…”.
He described restlessness at not getting any relief from the pain, describing himself as like ‘an animal in a cage’, stating he’d try anything to decrease the pain.
Table 2: Sample Demographics
Study number P1 P2 P3
Gender M F M
Age 72 86 71
Type of Diabetes 2 2 2
Duration of Diabetes (Years) 30 21 10
DFU Aetiology NI NI NI
Duration of DFU (Months) 17 16 6
No. of Diabetes Related Complications 2 1 2
Science, Practice and Education
EWMA Journal 2011 vol 11 no 2 28

Less Pain – More Gain! Measure to determine
length of dressing needed, cut off excess.
1
3
Insert the finger into the rolled end of the dressing.
5
Roll the dressing on the finger.
6
The dressing should fit securely on finger or toe.
Remove the insert from the rolled end and discard.
2
the ideal choice for managing:
•Sprains•Strains•Contusions•Abrasions•Lacerations•Burns•Ulcers•Matricectomies
This is an overview. Please see package insert for complete instructions.
4
Push the finger into the dressing and begin rolling.
Unless otherwise indicated, all trademarks are owned by or licensed to Ferris. © 2010, Ferris Mfg. Corp., Burr Ridge, IL 60527 USA MKL-563-I, REV-0, 1210
Ferris Mfg. Corp. 16W300 83rd Street, Burr Ridge, IL 60527 USA | International: +1 630.887.9797 | www.PolyMem.eu
Contact us for more information at www.PolyMem.eu
PolyMem® dressings help reduce edema, bruising, pain and inflammation when applied to open or closed injuries.Significant efficiencies are assured due to ease of application and use.

Science, Practice and Education
Physical Effects of PainThis theme was identified from patient comments regard-ing the effects of DFU pain on physical aspects of their daily life.
Problems with mobility due to pain were discussed by all participants, leading to feelings of loss of independence. One felt his pain was improving as his ulcer was beginning to heal – he was using a walking stick rather than a Zimmer frame, and commented that feelings of loss of control in his life had diminished as his mobility improved.
Another felt decreased mobility had the biggest ef-fect on QoL. Already experiencing limited mobility, the ulcer pain now forced her to use a wheelchair. Footwear problems highlighted previously also had adverse effects.
Another participant identified walking as a dominant factor in increasing his ulcer pain, requiring an electric scooter outside the house and leaving him unable to drive.
Sleep was also altered due to DFU pain, particularly for one. He slept in a chair as he couldn’t tolerate the pres-sure of the duvet on his foot while in bed, but was awake for long periods during the night. Sleeping tablets were ineffective:
“I just move my foot like everybody else does in bed…and that’s it, bang, it wakes me up”; “…about half hour and I wake…”; “I’ve gone through the roof with smoking... every time I wake up I’ve got to have something to do…”.
He thought lack of sleep made him feel much worse, feeling he could cope much better generally if his sleep improved.
Another commented that pain affected her sleep, finding she needed daytime naps due to tiredness, but felt that analgesia taken at night helped. One participant felt ulcer pain did not specifically wake him during the night, but took sleeping tablets with his bedtime analgesia.
Pain had also led to the loss of a previously healthy appetite for one participant:
“Well, I’m not living, it’s as simple as that. I’ve got no appetite, I eat like a pigeon. I used to love my Sunday dinners, but the look of them makes me feel ill now”.
Coping, Support and Social ImpactThis theme was derived from the patients’ accounts of the impact ulcer pain had on their relationship with family, friends and healthcare professionals, including the support they received and coping strategies they adopted.
All participants remarked they were unable to perform all their activities of daily living independently. This was also due to other medical conditions which affected their general health, such as cardiovascular disease, haemolytic anaemia and previous back surgery, in addition to the pain.
Help and support from family members also enabled them to cope. One felt the support received from her daughter made a big difference to her daily life and with coping with the pain. She performed dressing changes, reminded her to take analgesia and performed housework. This, however, made the patient feel she was putting pressure on her daughter’s time.
Feeling a burden on their family was also identified by the other participants, with one commenting he and his wife had no retirement. Another also depended greatly on his wife, feeling that DFU pain and the limitations it placed on his mobility was impacting on his family relationships:
“I’ve got a daughter nearby… I hardly see her..”; “I’ve got to the stage where I don’t want anybody…I mean I love having the grandkids up here but they can be noisy, and it makes me irritable”; “…as kids are, they don’t realise. I’m frightened when one of them is behind me. All I need is a tap on that and I’m up in the air”; “…it has changed my life, without a doubt”.
He also felt unable to perform any household mainte-nance or previously enjoyed social activities, especially as there were steep steps outside his house:
“…I’m not in the mood, I just can’t be bothered. I’m sick of being in but I don’t want to do anything else”.
Another participant stated: “I’ve just been like a zombie. With no interest. Now I’m
beginning to get out a bit, I feel better. I want to go out more”.
All participants commented on the care received from various clinicians for their DFU and related pain. Two felt that healthcare professionals had provided them with good care and support, which helped them cope.
“…There was one nurse… she sat with me and gave me comfort. Now that is something that you cannot get with swallowing a pill”.
One felt psychological support wouldn’t have helped, as she felt she had adapted to living with pain.
Neither felt there was anything clinicians could have done better.
Conversely, one participant was unhappy with the sup-port he had received from his general practitioner and district nurses, in particular, feeling there was no encour-agement with progress of the wound and they were always in a rush to leave. He did feel more supported by the DFU clinic that had referred him to a Pain Specialist whose interventions had provided some relief for a short while. He was, however, frustrated with delays in treatment.
EWMA Journal 2011 vol 11 no 2 30

The Mölnlycke Health Care name and logo are registered trademarks of Mölnlycke Health Care AB.Mölnlycke Health Care AB, Box 13080, SE-402 52 Göteborg, Sweden. Phone + 46 31 722 30 00. www.molnlycke.com
HQ
0225
7110
4
Investigating the Impact of Topical Antimicrobials in Wound CareWelcome to the Mölnlycke Health Care Satellite Symposium,May 26, 2011 at 11.15-12.15 in Gold hall
Wound infection is the most concerning of all wound complications. Topical antimicrobials play an important role in preventing and managing local wound infections however there are some outstanding questions regarding the usage of these agents that need to be answered.
The aim of this Symposium is to support the appropriate use of topical antimicrobial agents and to promote clinical decision-making that ensures their prescription only when clinically indicated.
The Chairmen Assoc Prof Bill McGuiness, Acting Head of School, Nursing and Midwifery, La Trobe University and AWMA President Australia, and Lt Col Steven Jeffery, Consultant Plastic Surgeon, The Royal Centre for Defence Medicine UK, will open and close the seminar by discussing commonly raised questions regarding using topical antimicrobials.
Professor Kevin Chipman, Professor of Cell Toxicology, University of Birmingham, UK, will give an overview of published safety data on topical antimicrobials.
Dr Paul Silverstein, Clinical Professor Plastic Surgery, University of Oklahoma, USA will discuss the importance of considering the health economic aspect in clinical studies in burn care.
Dr Jean-Charles Kerihuel, Medical Director and Consultant Physician & Methodologist, France, will reveal results from a large observational study using topical antimicrobial dressings in different wound types.
We look forward to seeing you there!
EWMA2011Brussels · Belgium
www.ewma2011.org

Psychological ImpactThis theme concerns the patient’s emotions, including feelings of depression, isolation and loss of independence, which overlapped considerably with the other themes due to the wide impact of the pain overall.
Loss of motivation and feelings of depression due to ulcer pain were expressed by two participants:
“…the worst time I’ve got at the moment is getting out of bed in the morning. I need real willpower to go into the bathroom and dress”.
“I look out there now and think spring is coming, but what can I do? Nothing.”.
Feelings of isolation and loss of independence were also raised. One participant felt frustrated with the lack of relief from the pain and that the ulcer controlled his life.
Two participants did however express trying to cope with things by thinking more positively, especially one whose pain was slowly improving:
“There’s a light at the end of the tunnel now”.
DISCUSSIONA larger, more diverse sample would have provided a richer data set and increased expression of views, but time con-straints made it difficult to address this issue. It would have been interesting to learn the experience of patients with purely neuropathic ulceration to determine any differences in QoL issues. Data saturation was not achieved so the collected data may be lacking in diversity or consistency. However, the main aim was not to generate theory but to gain information and perspective of the lived experience of DFU pain.
Experience of PainThe reported descriptions of pain are varied and intense in nature, similar to the results of the Short-Form McGill Pain Questionnaire18 used in phase one. Despite the com-mon perception that neuropathy leads to painless ulcers, the patients were not surprised to be experiencing pain. Preconceptions often held by patients and clinicians re-garding the pain experience need addressing if DFU pain is to be understood and adequately managed.
The causes of pain were similar to that reported by qualita-tive studies relating to DFU as a whole11,12, with pressure from footwear or bedding being recurrent themes. Pain at dressing change has been noted by other QoL stud-ies into DFU12, and is a common finding with studies related to wound pain19,20,21. As with one patient here, leg ulcer studies have reported how individual clinicians’ technique and basic understanding can impact on the ex-perience, with patients feeling that they are not listened to or cared about22. VLU were once considered painless
or not as painful as arterial ulcers which potentially caused increased pain at dressing change due to a poor knowledge base – a similar situation could occur with DFU due to the preconception that the pain sensation is compromised. Although pain at dressing change is becoming a more prominent and researched area, more consideration needs to be given to treatment of DFU with the awareness that they can be painful.
Problems with footwear are commonly cited within the QoL research relating to both DFU and VLU, although not always necessarily related to pain. The dissatisfaction or difficulties expressed by two patients regarding find-ing appropriate footwear could be an important issue for future care. Appropriate footwear for patients with DFU is paramount due to the requirement for offloading to improve healing23,24,25. Use of appropriate orthoses can improve physical and mental functioning in diabetic pa-tients26, reinforcing the requirements for an efficient and effective orthotic service within diabetic foot clinics to not only improve healing but also QoL. The adverse ef-fect of footwear on DFU pain is a significant issue for any healthcare professional (HCP) involved in the manage-ment of DFU, which again requires raised awareness and consideration within service provision.
Participants reported varying efficacy of analgesia for con-trolling DFU pain. Whereas previous literature is mainly concerned with the under-use of analgesia or the fear of dependence by patients11,27, some findings here suggest DFU pain can be so severe and multi-factorial that oral analgesia alone may not be sufficient. The only temporary relief one patient experienced was following referral to a chronic pain specialist, yet until clinicians acknowledge that specific ulcer pain exists and is not necessarily of neu-ropathic origin, there may be minimal referrals to specialist services. Management of some DFU pain may require treatment such as nerve blocks, psychological support or complementary therapies. Further research into this area alone is necessary if DFU pain assessment and manage-ment is to become even adequate.
Physical Effects of PainThe majority of research into chronic wounds and QoL suggests they impact significantly on physical aspects of daily life4,11,12,22,28,29,30. Qualitative work consistently highlights issues with mobility and sleep, the consequences of which appear far-reaching in terms of fatigue, loss of independence and social isolation.
Similar reports were found here, particularly with re-gard to mobility. Standing and walking even short dis-tances was found to increase pain, which concurred with previous findings in both quantitative and qualitative
Science, Practice and Education
EWMA Journal 2011 vol 11 no 2 32

AG
-BS-
1374
-03/
11
sorbion sachet borderWound Bed Preparation
www.sorbion.com
Finally closed.sorbion sachet border – the space you need.
NEWAvailable from May 2011
Quick and easy application
Hypoallergenic
Flexible backsheet
Still excellent absorption and retention
AZ_EWMA_border_210x297+3.indd 1 11.04.11 15:00

studies1,2,11,12. Some patients with DFU report frustra-tion at the enforced decrease in mobility due to the need to offload the foot, and state they would rather adopt risk-taking behaviours and accept the possible consequences to their physical health for an increase in their QoL11,12,30. If pain, however, is the cause of reduced mobility, then this option may not be available, leaving patients feeling completely restricted and isolated and with few coping mechanisms on which to depend. Achieving ulcer healing may be the only way of returning to a more normal physi-cal functioning, as described by one participant.
Sleep was an important issue for patients both in this study and previous works, leading to extreme fatigue and changes in mood4,28. The patients seem to become trapped in a vicious circle whereby the consequence of one problem exacerbates another. Increased fatigue due to sleep depriva-tion leads to further decreased mobility, which increases fatigue further due to patients becoming lonely, isolated and lacking in energy and motivation.
The results reinforce the idea that the impact of physical restrictions from DFU pain has the same widespread ef-fect on psychosocial well-being as other types of chronic wound. This emphasises the need for a holistic approach in order to facilitate a better understanding of patients’ needs.
Coping, Support and Social ImpactThe accounts of DFU pain causing increased depend-ence on others for assistance with simple daily activities is in accordance with general QOL studies into patients with DFU and VLU11,13,30. This causes feelings of loss of control and loss of self, which can leave patients anxious, depressed and vulnerable. While supportive families are a common theme within this study and others, and recog-nised as invaluable by patients, it is common for patients to feel burdensome and guilty, placing unwanted restric-tions on their loved ones, especially if partners are elderly and may not be in perfect health. These issues can affect relationships whereby patients feel a loss of their previous life and a change in their social role, as reflected by the comments of one subject regarding not being able to play with his grandchildren or wanting to socialise with other family and friends. These comments are again a recurring theme in other QoL literature on patients with chronic wounds, where fear of others knocking their wound and causing pain led to the avoidance of social or public situ-ations12,19,29,30,31,32. Again, a perpetual cycle may devel-op where decreased mobility and increased dependence leads to social isolation, leaving patients depressed and not wanting contact with others. One patient alluded to such feelings, mentioning he could not perform tasks re-lated to the upkeep of his home, a restriction which may have left him with feelings of low self-worth due to his
change of role within the family. These issues highlight the extent to which DFU pain can restrict individuals and compromise lives, so clinicians need to be aware of these feelings if they are to address all the needs of the patient.
Varying positive and negative relationships with HCPs were reported by participants. The literature suggests many patients with chronic wounds become disillusioned with their HCPs, feeling their personal experience is not being recognised, thus inhibiting freedom of expression13, and that they are not provided with enough education or involvement in decision-making regarding their care31. Others get frustrated with the inconsistency of treatment and develop a lack of confidence in their HCP’s32. It has been suggested that clinicians become focused on treating illnesses rather than people, or on curing rather than help-ing patients to live and cope with chronic illness29,33 – this may be the case with the patient who felt ignored and that his clinicians never offered him encouragement or reas-surance, but seemed only concerned with completing the task in hand (redressing the ulcer) as quickly as possible. The ulcer and its healing can become the sole focus of all interventions, and the clinician loses sight of the per-sonal experience and caring perspective. This underlines the need for clinicians to develop effective interpersonal skills and consider psychosocial aspects to recognise indi-vidual needs. The aim should be to prevent or lessen the psychosocial implications of DFU pain in the same way as physical treatment. Support in the form of allowing patients to talk, providing comfort and information-giving were the factors which participants felt fostered good re-lationships with their HCPs and helped them to cope.
Psychological ImpactThe psychological impact of DFU pain is a common thread running through all the themes already discussed – the experience of pain, physical restrictions and changes in relationships all led to feelings which created a change in psychosocial well-being. Several comments dealt solely with feelings of depression, loss of motivation and resig-nation at their situation and the effect it was having on their lives.
Increased anxiety and depression in patients with diabetes and foot ulcers has been documented3,414,34. These feelings can be enhanced due to concern that ulcers will never heal and a fear for the future at the loss of hope over regaining any control over their lives. One patient commented that the ulcer and pain controlled him, leaving him without positive thoughts. Another expressed a loss of motivation to even get up and wash and dress, yet was concerned about being a burden on his carer and frustrated at his lack of independence. Fear of amputation and its link to
Science, Practice and Education
EWMA Journal 2011 vol 11 no 2 34

Treatment of Venous Leg Ulcersin a new light.
Cutimed®
Discover an innovative rangeof wound management, medi-cal skin care and compressionproducts which reliably coverall stages of wound healing.Especially developed for the
successful treatment of chronic,difficult-to-heal-wounds, suchas venous leg ulcers, ourrange offers a complete selec-tion of effective and patient-friendly products.
On request, we will provide youwith further information onindications and treatmentoptions. Contact us: www.cutimed.com
A D VA N C E D W O U N D C A R E
Cutimed® PROTECT Cutimed® Sorbact® Cutimed® Siltec JOBST® Comprifore JOBST® UlcerCARE
Int_EWMA_AZ_RZ_Cutimed_advert 15.04.11 09:46 Seite 1

depression is often mentioned within the literature11,13, yet the desperation and anxiety felt by one patient regarding the lack of relief from his DFU pain had led him to ques-tion if amputation would be the more preferable option. These issues underline the importance for clinicians to pay more than lip service to holistic and psychological care, especially with regard to patients experiencing DFU pain, if prevention and management of such severe emotions is to be achieved.
Some patients coped with the feelings surrounding their DFU pain and its impact on their lives by either resigning themselves to its existence and their need to adapt to it, or by trying to think positively rather than succumbing to negative feelings. Husband29 suggested after a period of adaptation and endurance of long-term ulceration pa-tients may learn to shift the focus of their life away from the ulcer in order to cope with it. Small improvements in one patient’s ulcer pain may have enabled him to see a future without pain and a return to his old feelings of self. Either way, clinicians need to consider helping the patient to cope and adapt to potentially chronic conditions while also trying to address physical needs and ulcer healing.
Limitations to the study are acknowledged, such as the potential for poor external validity. Smaller than expected sample sizes were obtained, and were chosen from a spe-cialist environment dealing with complex and chronically ill patients. Therefore, similar findings may not occur with a larger, less complex population, and it is possible ob-served effects were not independent of natural variation within the clinic. However, the study was purely explora-tory and filled a void by providing interesting and valuable information on an under-researched area. The results act
as a basis for future research and highlight the requirement for this work to be performed.
The presence of complications related to diabetes and other medical conditions within the sample could also raise the question as to the extent to which the views and experiences expressed were solely attributable to DFU pain. They could also incorporate the difficulties of liv-ing with foot ulcers or diabetes itself, or even just general ill-health. Attempts were made to overcome this through reading of a statement at the commencement of each inter-view reiterating the specific subject matter and study aims.
CONCLUSIONOverall, the results of the qualitative component of this study into DFU pain have confirmed that this under-recognised phenomenon can have detrimental physical and psychosocial effects. This has major implications for clinical practice in that it challenges current assessment practices and accentuates the need for clinicians to im-prove their understanding of DFU pain and its conse-quences in order to increase quality of care provision and ensure the holistic needs of patients are met.
Lloyd and Orchard35 considered that improvements in QoL have become a more accepted goal of medical care, in addition to the alleviation of physical symptoms, but it is still evident that advancements can be made with regard to psychosocial issues. External pressures such as limited time and resources within diabetic foot clinics may lead to QoL issues related to pain and other aspects of living with a foot ulcer being overlooked, as the physical challenge of the ulcer itself is prioritised. Clinicians need to consider
Science, Practice and Education
References
1. Ribu L, Rustoen T, Birkeland K, Hanestad BR, Paul SM, Miaskowski C (2006) The Prevalence and Occurrence of Diabetic Foot Ulcer Pain and its Impact on Health-Related Quality of Life The Journal of Pain 7 (4) 290-299
2. Bengtsson L, Jonsson M, Apelqvist J (2008) Wound-Related Pain is Underestimated in Patients with Diabetic foot Ulcers Journal of Wound Care 17 (10) 433
3. Carrington AL, Mawdsley SKV, Morley M, Kincey J, Boulton AJM (1996) Psychologi-cal Status of Diabetic People with or without Lower Limb Disability Diabetes Research and Clinical Practice 32: 19-25
4. Brod M (1998) Quality of Life Issues in Patients with Diabetes and Lower Extremity Ulcers: Patients and Care Givers Quality of Life Research 7: 365 – 372
5. Meijer JWG, Trip J, Jaegers SMHJ, Links TP, Smits AJ, Groothoff JW, Eisma WH (2001) Quality of Life in Patients with Diabetic Foot Ulcers Disability and Rehabilita-tion 23 (8) 336-340
6. Paul SM, Zelman DC, Smith M, Miaskowski C (2005) Categorizing the Severity of Cancer Pain: Further Exploration of the Establishments of Cutpoints Pain 113: 37-44
7. Zelman DC, Dukes E, Brandenburg N, Bostrom A, Gore M (2005) Identification of Cut-points for Mild, Moderate and Severe Pain due to Diabetic Peripheral Neuropa-thy Pain 115: 29-36
8. Benbow M (2006) Holistic Assessment of Pain and Chronic Wounds Journal of Community Nursing 20 (5) 24-28
9. Flanagan M (2006) Managing Chronic Wound Pain in Primary Care Practice Nurse 31 (2) 34-37
10. Goodridge D, Trepman E, Embil, JM (2005) Health-Related Quality of Life in Diabetic Patients with Foot Ulcers Journal of Wound, Ostomy and Continence Nursing 32 (6) 368-377
11. Ribu L, Wahl A (2004) Living with Diabetic Foot Ulcers: a Life of Fear, Restrictions, and Pain Ostomy/Wound Management 50 (2) 57-67
12. Ashford RL, McGee P, Kinmond K (2000) Perception of Quality Of Life by Patients with Diabetic Foot Ulcers the Diabetic Foot 3 (4) 150-155
13. Watson-Miller S (2006) Living with a Diabetic Foot Ulcer: A Phenomenological Study Journal of Clinical Nursing 15: 1336-1337
14. Tennvall GR, Apelqvist, J (2000) Health-Related Quality of Life in Patients with Diabetes Mellitus and Foot Ulcers Journal of Diabetes and Its Complications 14: 235-241
15. Ribu L, Hanestad BR, Moum T, Birkeland K, Rustoen T (2007) A Comparison of the Health-Related Quality of Life in Patients with Diabetic Foot Ulcers, with a Diabetes Group and a Nondiabetes Group from the General Population Quality of Life Research 16: 179-189
16. Vileikyte L (2001) Diabetic Foot Ulcers: A Quality of Life Issue Diabetes/Metabolism Research and Reviews 17: 246-249
17. Burnand P (1991) A Method of Analysing Interview Transcripts in Qualitative Research Nurse Education Today 11: 461-466
18. Melzack R (1987) The Short-Form McGill Pain Questionnaire Pain 30: 191-197
19. Mudge E, Holloway S, Simmonds W, Price P (2006) Living with Venous Leg Ulceration: Issues Concerning Adherence British Journal of Nursing 15 (21) 1166-1171
20. White R (2008) A Multinational Survey of the Assessment of Pain when Removing Dressings Wounds UK 4 (1) 14-24
21. Price P, Fagervik-Morton H, Mudge EJ, Beele H, Ruiz JC, Nystrom TH, Lindholm C, Maume S, Melby-Ostergaard B, Peter Y, Romanelli M, Seppanen S, Serena TE, Sibbald G, Soriano JV, White W, Wollina U, Woo KY, Wyndham-White C, Harding KG (2008) Dressing-Related Pain in Patients with Chronic Wounds: An International Perspective International Wound Journal 5 (2) 159-171
22. Charles H (1995) The Impact of Leg Ulcers on Patients’ Quality of Life Professional Nurse 10 (9) 571-574
EWMA Journal 2011 vol 11 no 2 36

This cutaway shows how Heelift literally suspends the heel in space.
Pressure is transferred to the calf so the heel never makes contact with the bed.
Heelift Suspension Boot— The Pressure-Free SolutionUse it for prevention. Use it for treatment. Use it for peace of mind.
• If required, Heelift can be customized by trimming the extra pad to meet the need of any patient
• Use the included extra pad to prevent foot-drop or control hip rotation• Available in Smooth or Convoluted Foam• Now also available in Bariatric and Petite
There is only one Heelift®.
DARCO (Europe) GmbHGewerbegebiet 18, 82399 RaistingTelefon +49 (0) 8807.9228-0
Fax +49 (0) [email protected]
www.darco-online.com
Heelift® Patent No. 5449339 & 7,458,948.
© 2011, DM Systems, Inc. All rights reserved. EWMA2011
WOULD YOU LIKE A SAMPLE?Please use the link below to request
a sample, demo DVD, or CD:www.heelift.com/j
EWMA 2011Stand #
57
increased QoL as a measure of success as well as objec-tive physical outcome measures, because while these are important, dealing with a chronic and progressive disease such as diabetes may mean that patients have to cope with such problems for long periods of time. More work into the effect of DFU pain on QoL may help to raise aware-ness and aid clinicians in the provision of holistic care that facilitates both physical and psychological well-being.
Implications for clinical practicen Clinicians need to be more aware of the importance
of providing psychosocial care in addition to focus-ing on ulcer healing.
n Collaborative working between diabetic foot spe-cialists, wound care specialists, pain specialists and primary care teams could promote better assessment and management of DFU pain and its impact on QoL.
n Patients should be involved in decision-making regarding their treatment.
Further researchn Further qualitative work into the patient’s perspec-
tive on DFU pain could help clinicians to under-stand the relevance to diabetic foot care and to their own practice, and aid in meeting patient needs more completely.
n Quantitative work using formal HRQoL tools could provide interesting information and comparative data with other patient populations.
n The development of a tool incorporating the physi-cal assessment of DFU pain in conjunction with a review of psychosocial issues might be a useful method of increasing awareness and improving dissemination of information. m
23. Krasner D (1998) Diabetic Ulcers of the Lower Extremity: A Review of Comprehen-sive Management Ostomy/Wound Management 44 (4) 56-75
24. Frykberg RG (2002) Diabetic Foot Ulcers: Pathogenesis and Management American Family Physician 66 (9) 1655-1662
25. Jeffcoate WJ, Harding KG (2003) Diabetic Foot Ulcers The Lancet 361: 1545-1551
26 Davies S, Gibby O, Phillips C, Price P, Tyrrell W (2000) The Health Status of Diabetic Patients Receiving Orthotic Therapy Quality of Life Research 9: 233-240
27. Persoon A, Heinen MM, van der Vleuten CJM, de Rooij MJ, van de Kerkhof PCM, van Achterberg T (2004) Leg Ulcers: A Review of their Impact on Daily Life Journal of Clinical Nursing 13: 341-354
28. Douglas V (2001) Living with a Chronic Leg Ulcer: An Insight into Patients’ Experiences and Feelings Journal of Wound Care 10 (9) 355-360
29. Husband LL (2001) Shaping the Trajectory of Patients with Venous Ulceration in Primary Care Health Expectations 4: 189-198
30. Kinmond K, McGee P, Gough S, Ashford R (2003) ‘Loss of Self’: A Psychosocial Study of the Quality of Life of Adults with Diabetic Foot Ulceration Journal of Tissue Viability 13 (1) 6-16
31. McPherson MV, Binning J (2002) Chronic Foot Ulcers Associated with Diabetes: Patient’s Views The Diabetic Foot 5: 198-204
32. Rich A, McLachlen L (2003) How Living with a Leg Ulcer Affects People’s Daily Life: A Nurse-Led Study Journal of Wound Care 12 (2) 51-54
33. Pott E (1992) Health Promotion and Chronic Illness: Discovering a New Quality of Health Geneva: World Health Organisation
34. Anderson RJ, Clouse RE, Freedland KE, Lustman PJ (2001) The Prevalence of Comorbid Depression in Adults with Diabetes: A Meta Analysis Diabetes Care 24 (6) 1069-1078
35. Lloyd CE, Orchard TJ (1999) Physical and Psychological Well-Being in Adults with Type 1 Diabetes Diabetes Research and Clinical Practice 44: 9-19
EWMA Journal 2011 vol 11 no 2

1 Martin Šimek, MD,PhD
1Martin Kaláb, MD, 2Martin Molitor, MD,PhD1Roman Hájek, MD,PhD
1Jana Grulichová 1Patrick Tobbia, MD
2Bohumil Zálešák, MD,PhD 1Vladimír Lonský, MD,PhD
Short paper1Department of Cardiac
Surgery2Department of Plastic and Aesthetic Surgery
University Hospital and Palacky University Faculty
of Medicine, Olomouc, Czech Republic
Correspondence: Martin Šimek
The authors have no financial relationship
with KCI Company San Antonio, TX, USA
ABSTRACTAim: We sought to evaluate a five year sin-gle centre experience for the application of topical negative pressure therapy (TNP) as the first-line therapy in the treatment of deep sternal wound infection (DSWI) following cardiac surgery.Methods: Prospective analysis of 50 consecu-tive patients (27 men, 23 women, mean age 67.8±9.2 years) who underwent first-line application of topical negative pressure for the treatment of deep sternal wound infec-tion within a five year period (from Septem-ber 2004 to September 2009). Clinical and wound care outcomes were evaluated, thera-peutic failure rates, in-hospital and as well as the one year mortality of unified application protocol.Results: During follow-up 4% of 30-day mortality, 8% of in-hospital mortality, and 14% of one year mortality (10% DSWI-re-lated complication adjusted) were observed. The mean length of overall therapy reached 12.6±8.0 days including the mean of 5.4±2.5 revision/dressing changes within 38.1±14.6 days of the mean in-hospital stay. The sternal bone was stabilized in 94% of cases; various flaps were employed in covering of the re-sidual soft tissue defect in 70% of patients. Treatment failed in 6% of all cases, 4% due to DSWI recurrence, and 2% due to necro-sis of the advanced muscle flap. The risk of wire-related fistula was 14% during whole follow-up period.Conclusion: TNP therapy is a reliable meth-od for the treatment of DSWI following cardiac surgery. The primary application of TNP demonstrated a low risk of failure and a significant decrease in short- and mid-term mortality was observed.
INTRODUCTIONDeep sternal wound infection (DSWI) is one of the most serious complications of cardiac surgery per-formed through median sternotomy with predicted mortality ranging between 5 to 30%1. Despite well-described risk-related factors, improved antibiotic prophylaxis and aseptic methods, the incidence re-mains unchanged, varying from 1% to 5%2. The treat-ment strategies of DSWI is still challenging; it differs from one country to another, from one institution to another and even from one surgeon to another at the same department2.
METHODSBetween March 2002 to September 2009, 6009 me-dian sternotomies were performed at our department as a primary access for heart surgery. DSWIs were diagnosed according to the guidelines of the Centre for Disease Control and Prevention (CDC, 3), DSWI occurred in 84 patients which represented an inci-dence rate of 1.39%. Fifty consecutive patients (59%) were primarily scheduled for the first-line application of topical negative pressure therapy (TNP) between September 2004 and September 2009. The detailed unified therapeutic protocol has been described pre-viously4,5,6. The median sternotomy was completely released and all suture material removed during pri-mary revision. After bacterial sampling, when two to three swabs were taken (subticular, and mediastinal tissue, sternal bone), the wound was repeatedly flushed out with tepid saline solution. Inherent surgical de-bridement included removing only clearly necrotic tissue and was performed with aid of a scalpel, sur-gical spoon, and low-voltage electrocautery. Hydro-surgical debridement using saline jet-powered device (Versajet™, Smith and Nephew, UK) has not been employed. Moreover, debridement on the mediasti-nal structures was done extremely gently to avoid the risk of severe bleeding from grafts or the right ventri-
Topical negative pressure in the treatment of deep sternal infection following cardiac surgery: Five year results of first-line application protocol
Presented at the 20th Conference of the
European Wound Management Association, 26-28 May,
Geneva, Switzerland.
EWMA Journal 2011 vol 11 no 2 38

Science, Practice and Education
cle. If the bone mass was affected with osteomyelitis, it was removed with adherent sternocostal joints and costal cartilages. Emphasis was put on meticulous haemostasis throughout each debridement. Bleeding from the bone marrow was controlled with temporally placed bone wax, which was removed within next dressing changes. Surgical debridement with repetitive application of TNP (Vacuum-assisted closure™, KCI San Antonio, Tx, USA) was car-ried out every 48 hours until the wound bed was found to be free of infection, then the wound was covered by well-vascularised granulation tissue. When C-reactive protein levels dropped below 30 mg/l, then the chest was reclosed (Figure 1). Peri-procedural, wound care characteristics and clinical outcomes were recorded in a prospective manner. All patients had a one year follow-up for the evaluation of long-term morbidity and mortality, Kaplan-Meier ac-tuarial analysis of survival was plotted. Approval of the local ethics committee was obtained for the protocol of the application of TNP to the open chest wound in 2004.
RESULTSThere were 27 males (54%) and 23 females (47%) with an average age 67.8±9.2, and BMI 29.9±5.3 kg/m2. Detailed peri-operative characteristics including co-morbidities, surgical procedures and post-operative complications re-lated to DSWI are summarized in Table 1. A total of 45 patients underwent coronary artery bypass grafting either as single procedure or in combination with valve surgery. In this subgroup of patients, 28 (63%) had diabetes and the internal thoracic artery (IMA) was taken down in 40 (89%). Unilateral IMA harvesting (80%) was done in pedicled fashion, whereas bilateral IMA harvesting (20%) was always performed without surrounding tissue as a skel-etonized graft with maximal effort to spare the chest bone blood supply. The presentation of DSWI was delayed in average 16.1±14.2 days after the primary surgery, and twenty-three (46%) patients were re-admitted to the hos-pital due to DSWI despite an uneventful wound healing progress at the time of discharge. Gram positive strains
were dominantly cultivated from swabs obtained from the infected wound site, particularly staphylococcal aureus and coagulase-negative staphylococcus (Graph 1). There was no significant difference in outcome based on etiological causative agent. Based on the protocol, mean length of primary therapy reached 10.8±7.9 days including mean of 5.0±2.1 number of dressing changes in average until the wound bed was free of infection. All dressing changes were performed in the operating theatre, every patient was given a general anaesthetic and relaxed to avoid right ventricle or graft injury caused by the sternal lamella margins. The cost of each surgical debridement and dressing changes were analysed. The expenditure was approximately 2000 CZK (77 €) for general anaesthesia, 900 CZK (35 €) for surgical debridement, and 2500 CZK (96 €) for dressing material and collecting canister. A calculated total cost per one dressing change reached 5400 CZK (208 €).Chang-es in laboratory inflammatory parameters characteristics
Table 1. Perioperative characteristics TNP (n=50)
Age (years) 67.8±9.2BMI (kg/m2 ) 29.9±5.3Male/female ration (%) 54.0/46.0DM (%) 58.0COPD (%) 34.0Immunosuppressive therapy (%) 18.0Renal impairment (kreatinin>120 mmol/l) (%) 28.0LVEF (%) 40.8±13.6EuroSCORE log 6.9±6.2
CABG/valve/combined procedure (%) 60/10/30Mean operation time (min) 230.5±44.8Mean XC time (min) 62.8±45.6Mean ECC time (min) 90.7±40.1Emergency surgery (%) 24.0Postoperative blood loss (ml) 910±540.3Mean artificial pulmonary ventilation (hours) 19.4±28.1Mean ICU stay (hours) 61.1±34.8
Revision for bleeding/tamponade (%) 18.0Revision for sternal instability (%) 40.0Prolonged mechanical ventilation/tracheostomy (%) 8.0
Figure 1. Therapeutic protocol
BMI – body mass indexDM – diabetes mellitus COPD – chronic obstructive pulmonary diseaseLVEF – left ventricle ejection fraction
CABG – coronary artery bypass graftingXC – cross clampECC – extracorporeal circulationICU – intensive care unit
Graph 1. Predominant wound microorganisms
EWMA Journal 2011 vol 11 no 2 39

(C-reactive protein, white blood count) throughout the therapy are displayed in Graph 2. The sternum was ap-proximated in 47 patients (94%), and residual soft tissue defect needed to be covered with local flaps in 45 patients (70%). Detail of employed flaps is showed in Graph 3. Primary treatment failed in three patients (6%); in two patients (4%) due to DSWI recurrence, and in one (2%) due to necrosis of bipedicle muscle flap owing to the tech-nical failure. All those patients underwent TNP therapy according to the therapeutic protocol similar to primary application (rescue therapy), and the necrotic flap was removed. Furthermore, superficial sternal wound infection (SSWI) or soft tissue dehiscence occurred in four patients (8%) which was treated with moist healing therapy and/or was surgically closed. Mean overall length of TNP therapy reached 12.6±8.0 days including 5.4±2.5 dressing changes on average, mean in-hospital time was 38.1±14.6 days. Focusing on the mortality, 4% of 30-day mortality (two patients), and 8% of in-hospital mortality (four patients) was recorded ranging between the 9th-94th post-operative day. Three patients (6%) died of multiple organ failure and one (2%) of intractable bleeding from a right ventricle rupture that occurred shortly after the primary revision. Detailed therapy characteristics and clinical outcomes are recorded in table 2. During the one year follow-up, a total of seven patients (14%) were lost, five of whom (10%) were an immediate consequence of DSWI (DSWI ad-justed mortality), another seven patients (14%) underwent treatment for wire-related fistula. The one year plotted survival analysis using Kaplan-Meier analysis is displayed in Figure 2.
DISCUSSIONThe treatment of DSWI poses an ongoing challenge for cardiac surgeons; thus far there is no consensus about the standard of care covering this issue2. TNP therapy has been used in cardiac surgery since 1997. Despite growing and encouraging experience, evidence that TNP is better than conventional therapy is still lacking4. Several studies comparing TNP versus conventional therapy showed su-periority of TNP in terms of reduction of primary therapy failure, short- and long-term mortality and morbidity, and
better quality of life, however, all had retrospective design and were conducted on a limited number of patients5,6,7,8. Recently initial data showed the cost-effectiveness of this therapy9. Even though the cost of TNP was comparable with other treatment strategies of DSWI, this treatment brought a significant reduction in mortality and in-hos-pital stay9. Thus, there is still essential need for further investigations including larger prospective multi-centre study, and randomized trials4. From a surgical point of view, TNP combines advantages of the open therapy which enables repetitive debridement and wound drain-age with the closed therapy, because even in the absence of sternal closure, applied negative pressure of 125 mm Hg effectively stabilizes the chest. It allows immediate postoperative extubation and mobilization of the patient. Moreover, sealing the sternal wound minimizes the risk of secondary contamination and facilitates handling with patients, particularly if they need to be hospitalized in the ICU10.
The exact mechanism of TNP action on wound heal-ing has not been fully explained as yet10. It has been shown to accelerate granulation tissue building, reduce wound surface area, decrease local and interstitial tissue oedema, and increase perfusion of the peri- and wound area10,11,12 even when the left internal mammary artery has been har-vested for bypass grafting13. Moreover, diminished bacte-rial load or modulation of bacterial species together with the reduction of the amount of metalloproteinase detected in the wound bed strongly suggest that the effect of TNP on wound healing processes is rather more fundamental than adjunct14,15.
A new negative pressure therapy (V.A.C – Instilla-tion™, KCI, San Antonio, TX, USA) has been recently introduced. It combines the positive effect of sub atmos-pheric pressure with intermittent instillation of antiseptic solution. This therapy demonstrated its effectiveness in the treatment of chronic-infected wounds such as pelvic and leg post-traumatic osteomyelitis. Applied negative pressures together with intermittent instillation of poly-hexanide solution significantly reduced total in-hospital stay (36 vs. 73 days, p<0.0001) and recurrence of infec-tion (3 vs.59%, p<0.0001) compared with conventional treatment16.
Graph 2. Laboratory inflammatory parameters characteristics Graph 3. Flap employment
EWMA Journal 2011 vol 11 no 2 40

Although the manufacturer’s recommended negative pressure setting is 125 mmHg for polyurethane foam, and 150 mmHg for polyvinyl alcohol foam, some of the studies that focused on cutaneous blood flow suggested that further increase in sub atmospheric pressure, even up to 300 mmHg, leads to a three times increase of cutane-ous blood flow for polyvinyl alcohol and five times for polyurethane foam17.
The aim of this prospective study was to evaluate the clinical outcome of first-line application of TNP for DSWI as a standard of care. The results suggested that TNP therapy is associated with low rates of therapy failure, and reduction in short- and mid-term mortality. Uniform treatment protocol allowed for equivalent outcomes to be achieved among all surgeons at one unit.
CONCLUSIONTNP therapy is a safe method for the treatment of DSWI following cardiac surgery. The first-line application pro-tocol of TNP demonstrated a low risk of failure and a significant decrease in short- and mid-term mortality was observed.
Implications for Clinical Practicen TNP is an effective treatment for deep sternal infec-
tion after cardiac surgeryn TNP is associated with low failure rate, and reduced
short- and mid-term mortalityn TNP should be widely accepted as a first-line treat-
ment strategy for DSWI in cardiac surgery
Further Researchn Multi-centre prospective randomized trials compar-
ing TNP with the conventional therapy need to be undertaken
n Influences of individual wound-healing risk factors and microbiological agents on the effectiveness of TNP therapy need to be examined m
Table 2. Therapy characteristics and outcomesTNP (n=50)
Primary therapyNo. of revisions/dressing changes 5.0±2.1Length of primary therapy (days) 10.8±7.9Failure of primary therapy (%) 6.0
Complications after the chest closureDSWI (%) 4.0Flap necrosis (%) 2.0SSWI/dehiscence (%) 8.0Fistula (%) 14.0
Overall therapyOverall length of therapy (days) 12.6±8.0Overall No. of revision/dressing changes 5.4±2.5In-ICU stay (hours) 204.4±320.1In-hospital stay (days) 38.1±14.6
Mortality30-day mortality (%) 4.0In-hospital mortality (%) 8.0Multiple organ failure (%) 6.0Intractable bleeding (%) 2.01-year mortality (%) 14.0
ICU – intensive care unit
Figure 2. Kaplan-Meier survival analysis
Literature
1. Lepelletier D, Perron S, Bizouarn P, et al. Surgical-site infection after cardiac surgery: Incidence, microbiology, and risk factors. Infect Control Hosp Epidemiol 2005;26:466-72.
2. Schimmer C, Sommer P, Bensch M, Elert M, Leyh R. Management of poststernotomy mediastinitis: experience and results of different therapy modalities. Thorac Cardiovasc Surg 2008;56:200-4.
3. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. The hospital infection control practise advisory committee. Guidelines for prevention of surgical site infection. Infect Control Hosp Epidemiol 2002;20:247-78.
4. Raja SG, Berg GA. Should vacuum-assisted closure therapy be routinely used for management of deep sternal wound infection after cardiac surgery. Interactive Cardiovasc Thorac Surg 2007;6:523–27.
5. Sjögren J, Gustafsson R, Nilsson J, Malmsjö M, Ingemansson R. Clinical outcome after postster-notomy mediastinitis: Vacuum-assisted closure versus conventional treatment. Ann Thorac Surg 2005;79:2049-55.
6. Simek M, Hajek R, Fluger I, et al. Topical negative pressure versus conventional treatment of deep sternal infection in cardiac surgery. EWMA Journal 2008;8:19-22.
7. De Feo M, Vicchio M, Nappi G, Contrufo M. Role of Vacuum in Meticillin-Resistant Deep Sternal Wound Infection. Asian Cardiovasc Thorac Ann 2010;18:360-363.
8. Petzina R, Hoffman J, Navasardyan A, Mamsjoe S, Ubenhaun A, Hetzer R. Negative pressure wound therapy for post-sternotomy mediastinitis reduces mortality rate and sternal re-infection rate compared to conventional treatment. Eur J Cadiothoracic Surg 2010;38:110-113
9. Mokhari A, Sjögren J, Nilsson J, Gustafsson R, Malmsjö M, Ingemansson R. The cost of vacuum-assisted closure in treatment of deep sternal wound infection. Scand Cardiovasc J 2007;42:85-89.
10. Banwell PE, Musgrave M. Topical negative pressure therapy: mechanisms and indications. Int Wound J 2004;1:95-106.
11. Ubbink DT, Westerbos SJ, Nelson EA, Vermeulen H. A systematic review of topical negative pressure therapy for acute and chronic wounds. Brit J Surg 2008;95:685-692.
12. Argenta LC, Morykvas MJ, Marks MW, DeFranzo AJ, Molnar JA, David LR. Vacuum-assisted closure: State of art. Plast Reconstruct Surg 2006;117: 127-42S.
13. Petzina R, Gustafsson L, Mokhtari A, Ingemansson R, Malmsjö M. Effect of vacuum-assisted closure on blood flow in the peristernal thoracic wall after internal mammary artery harvesting. Eur J Cardiotho-rac Surg 2006;30:85-9.
14. Mouës CM, Vos MC, van den Bemd GJ, Stijnen T, Hovius SE. Bacterial load in relation to vacuum-assisted closure wound therapy: a prospective randomized trial. Wound Repair Regen 2004;12:11-7.
15. Mouës CM, van Toorenenbergen AW, Heule F, Hop WC, Hovius SE. The role of topical negative pressure in wound repair: expression of biochemical markers in wound fluid during wound healing. Wound Repair Regen 2008;6:488-94.
16. Timmers MS, Steenvoorde P, Bernards AT, van Dissel JT, Jukema GN. Negative pressure wound treatment with polyvinyl alcohol foam and polyhexanide antiseptic solution instillation in posttraumatic osteomyelitis.Wound Repair Regen. 2009;17:278-86.
17. Timmers MS, Le Cessie S, Banwell P, Jukema GN: The effects of varying degrees of pressure delivered by negative pressure wound therapy on skin/tissue perfusion. Ann Plast Surg 2005:55:665-671.
Science, Practice and Education
EWMA Journal 2011 vol 11 no 2 41

Phyt
oceu
tica
ls L
td. |
800
8 Z
uri
ch |
Swit
zerl
and
WWW.1WOUND.INFO
SIMPLE. NATURAL. EFFECTIVE.

Karen Lamb1 Nikki Stubbs1 Jo Dumville2 Nicky Cullum2
Dr Susan O’Meara2
1NHS Leeds Community Healthcare, St. Marys Hospital, Leeds, LS12 3QE
2Department of Health Sciences, University of York, York, YO10 5DD
Conflict of interest: None
Scientific Communication
BACKGROUNDThe Wounds Research for Patient Benefit (WRPB) programme commenced in 2008 and will receive £1.75 million of funding from the Programme Grants for Applied Research funding stream of the National Institute for Health Research (NIHR), over five years. The research programme is a multidisciplinary col-laboration between NHS Leeds Community Healthcare and the University of York. The large and diverse population of Leeds offers an ideal laboratory for research, ensuring the de-livery of useful and valid information regard-ing complex wound care and the University of York is home to the Wounds Research Group which has an international reputation for its expertise in a range of research methodologies applied to wound care.
The WRPB programme is specifically fo-cused on researching complex wounds which we define as wounds which involve superficial, partial or full thickness skin loss and which are healing by secondary intention. They are wounds with an underlying cause or which occur in pa-tients where underlying disease may impact upon healing e.g. pressure ulcers, leg ulcers and dehisced surgical wounds. Currently good information regarding the nature, treatment, costs and outcomes for people with complex wounds is very limited and this research programme will plug some of these knowledge gaps, re-duce clinical uncertainty and enable decision makers to prioritise future research and areas for service development. We wanted to take this opportunity to provide an overview of the work that is being carried out as part of this programme and to invite you to share your clinical uncertainties with us.
The research programme is split into three distinct, but integrated workstreams which we will describe in turn.
WORKSTREAM 1: Data capture and epidemiology Workstream 1 is focused on collecting high qual-ity information about complex wounds and their care. There is a real lack of basic, yet important, information about the treatment of complex wounds in the UK; a fact we have confirmed in a recently completed literature review of wound prevalence surveys/audits. Whilst we included fifty studies in the review, problems of study design meant that many of these studies were at high risk of bias and likely to under- or over-estimate wound prevalence. These biases result in large differences in the pub-lished estimates of complex wound prevalence. Our literature review helped inform the design of a new large and comprehensive survey of people with com-plex wounds in Leeds. The survey took place over a two-week period in March 2011 and included all settings in which people with complex wounds are treated including health clinics for people with no fixed abode and prisons. This comprehensive data collection and the inclusion of hard-to-reach groups such as IV drug users mean that we are confident in the results and the estimate of wound prevalence this study will bring. This survey also recorded who is delivering health care, how often and what treat-ments are being provided so we will have important new insights into the impact of wounds on all health care services. Data are currently being analysed and will be published late 2011.
Wounds Research for Patient Benefit:
A five year programme of research in wound care
EWMA Journal 2011 vol 11 no 2 43

Scientific Communication
Become a Member of EWMA
Make a difference in clinical practice
Benefits of your EWMA Membership:n You make a difference in clinical practice within wound management in Europe
n Right to vote and stand for EWMA Council
n EWMA Journal send directly to you three times a year
n EWMA news and statements send directly to you
n A discount on your registration fee for EWMA Conferences
n Right to apply for EWMA travel grants
n Yearly membership fee € 25
n Yearly membership fee for members of cooperating organisations € 10
Please register as a EWMA member at WWW.EWMA.ORG
EWMA SecretariatNordre Fasanvej 113,2000 Frederiksberg,DenmarkTel: +45 7020 0305Fax: +45 7020 [email protected]
Finally, within this workstream we are exploring whether we can routinely collect high quality data about people with complex wounds, for use in both service planning and research. Such a system, a type of register, would record the number of patients affected; the ongoing impact of wounds on quality of life; actual treatments received and healing rates achieved. Additionally, such a system could facilitate on-going assessment of costs and benefits, as well as monitoring the diffusion of new-to-market medical de-vices into practice. Such data will contribute to health technology assessment via the tentative application of ad-vance methodologies that may generate information on the clinical and cost effectiveness of wound treatments. This work is on-going and more information about this and all aspects of workstream 1 can be found at: www.york.ac.uk/healthsciences/wounds-patientbenefit/wone/
WORKSTREAM 2: Understanding what matters most to patients, carers and health professionals in complex wound careWorkstream two acknowledges that those researching and delivering wound care should fully understand what outcomes matters most to patients and carers. Wound healing is frequently reported in trials, whilst some have argued for alternative outcomes1, so we are asking patients and clinicians. Other possible outcomes of interest could include debridement, the number of dressing changes, resource use, exudate, odour, pain, dressing comfort and product durability. To find out we are undertaking in-depth interviews with patients, carers and healthcare staff about the relative importance of different wound treat-
ment outcomes to them. The study includes patients who have leg ulcers, diabetic foot ulcers, pressure ulcers and dehisced surgical wounds and the findings will provide missing information for researchers and health care staff on what matters most to different patients experiencing wound care. Additionally, in collaboration with the James Lind alliance (JLA)2, we are convening groups of patients, carers and citizens who are interested in helping to set the research agenda for the treatment specific wounds.
The JLA was established in 2004 to encourage patients, carers and clinicians to work together to identify and prioritise important healthcare uncertainties that can be translated into research priorities. Where there is no clear evidence about the effectiveness of treatments, clinicians and patients are left with uncertainty and are reliant on the opinions of health care professionals which can be flawed. In our experience public involvement in, and awareness of, wounds research is minimal. Given the lack of patient involvement in research agenda setting and the limited ev-idence-base informing clinical decisions in wound care3-5, the JLA is supporting the development of a partnership of patients, carers and clinicians to identify research priorities in the prevention and management of pressure ulcers. The objective is to discover the research questions that matter most to stakeholders. The initial meeting of the James Lind Alliance Pressure Ulcer Partnership (JLAPUP) took place in York in Spring 2011 and was participated in with much enthusiasm by delegates. Further information on the JLAPUP can be found at www.york.ac.uk/healthsciences/wounds-patientbenefit/jla-pressureulcerpartnership/
EWMA Journal 2011 vol 11 no 2 44

Hyiodine®Activates Healing …Naturally
Hyaluronic Acid & Iodine Safely Delivered to The Wound Bed
Tissue repair Antimicrobial protection Reduced scarring
Promotes healing in all wound types, especially hard to heal wounds. Suitable for wounds with varying degrees of exudate, sinuses and fi stulae.
Contipro C, a. s.Dolní Dobrouč 401 561 02 Dolní Dobrouč Czech RepublicT: 00420 465 519 582 e-mail: [email protected]
Unlocking the Secretsof Biotechnology
WEEK 0
WEEK 3
WEEK 14
Hyiodine_inzerát_A4.indd 3 6.4.2011 13:55:05

Scientific Communication
WORKSTREAM 3: Evidence synthesisWorkstream 3 brings together existing research to answer questions about which wound treatments work best. In or-der that our reviews tackle questions of high priority to the NHS, we consulted with clinicians, including nurses and podiatrists and compiled a list of 27 potential questions which can be viewed on our website (www.york.ac.uk/healthsciences/wounds-patientbenefit/wthree ). Questions included: What is the relationship between debridement and healing in foot ulcers and other complex/chronic wounds? and What is the best way to diagnose osteomyelitis?
For each topic we have scoped the literature in order to identify existing summaries of research and we have noted those topics that seem ‘ripe’ for further investigation. It is important to note that this list is not closed and we welcome further suggestions from readers of this journal (please submit suggestions via our Programme website or by contacting Susan O’Meara, [email protected]). The main focus here is clinical effectiveness questions (i.e., those that explore how well an intervention works) or what the most accurate method of diagnosis is.
Our consultation with clinicians has resulted in us initi-ating a new review on dressings for healing diabetic foot ulcers where we are using a more sophisticated method of evidence synthesis (mixed treatment comparison) to make the most of existing published data.6-8 We are also working on updating existing Cochrane reviews in wound care. We have completed one update (Antibiotics and an-tiseptics for venous leg ulcers9) and another (Compression for venous leg ulcers) is underway. We also have a new review in progress which explores the influence of the type of research funding on the quality of wound treatment trials. Additional new reviews and review updates will be undertaken as the research programme progresses. A fur-ther component of this Workstream will investigate how we might best present the results of evidence synthesis, including quantitative information and uncertainty, to make them most useful for health professionals.
CONCLUSIONS Good clinical management of complex wounds promotes positive outcomes and reduces wound recurrence. The lack of good quality research evidence for wound treatments should concern us all — only approximately 10% of rec-ommendations in National institute of Health and Clini-cal Excellence and the Royal Collage of Nursing wound care guidelines are supported by Level 1 evidence. The Wound Research for Patient Benefit research programme is encouraging the production of more relevant and better quality research evidence on the effectiveness and cost-effectiveness of wound prevention and treatment. This evidence has the potential to improve the quality of care, patient outcomes and reduce costs. If you wish to contrib-ute to discussion on treatment uncertainties or have any other wound care-related research questions please con-tact us via our website: www.york.ac.uk/healthsciences/wounds-patientbenefit/research-question/ m
Disclaimer All authors receive funding from the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research funding scheme (RP-PG-0407-10428). The views expressed in this review are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
References
1. Gottrup F. Debridement: another evidence problem in wound healing. Wound Repair and Regeneration 2009; 17:294-95.
2. The James Lind Alliance. www.lindalliance.org/ Accessed 19th April 2011
3. NICE (2005) The management of pressure ulcers in primary and secondary care: A Clinical Practice Guideline. Available at http://guidance.nice.org.uk/CG29/Guidance/pdf/English . (Accessed 06/01/2010).
4. NPUAP-EPUAP Guidelines for Pressure Ulcer Prevention and Treatment (2009). Available at www.npuap.org (accessed 20 April 2011).
5. Reddy M, Gill SS, Kalkar SR, Wu W, Anderson PJ, Rochon PA (2008) Treatment of Pressure Ulcers: A Systematic Review JAMA 300 22: 2647-2662
6. Sutton A, Ades AE, Cooper N, Abrams K. Use of indirect and mixed treatment comparisons for technology assessment. Pharmacoeconomics. 2008;26(9):753-67.
7. Lu G, Ades AE. Combination of direct and indirect evidence in mixed treatment comparisons. Stat Med. 2004 Oct 30;23(20):3105-24
8. Glenny AM, Altman DG, Song F, Sakarovitch C, Deeks JJ, D’Amico R, Bradburn M, Eastwood AJ; International Stroke Trial Collaborative Group. Indirect comparisonsof competing interventions. Health Technol Assess. 2005 Jul;9(26):1-134, iii-iv.
9. O’Meara S, Al-Kurdi D, Ologun Y, Ovington LG. Antibiotics and antiseptics for venous leg ulcers. Cochrane Database of Systematic Reviews 2010, Issue 1. Art. No.: CD003557. DOI: 10.1002/14651858.CD003557.pub3. Available from www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD003557/frame.html
Are you interested in submitting an article or paper for EWMA Journal?
Read our author guidelines at www.ewma.org/english/authorguide
EWMA Journal 2011 vol 11 no 2 46

Are You Doing Everything You Can For Your Patients?Heal Chronic Wounds - Completely.
For more information or to schedule your evaluation visit us at www.aotinc.net or email us at [email protected]
www.aotinc.net
Greater than 80% Wound Closure Rate Unprecedented closure rates in various stage 2, 3 and 4 wounds.
Stimulates Angiogenesis and Collagen ProductionSigni� cantly increases indigenous growth factors stimulating angiogenesis, capillary budding and collagen production.
Infection ControlE� ectively eliminates wound pathogens including; Staphylo-coccus Aurous, Streptococci, Pseudomonas Aeruginosa and MRSA.
Signi� cant Pain ReductionRapid reduction in wound related pain by over 75% within 3-4 weeks of commencing treatment.
Non Invasive Safe TherapyEasily applied and integrated into any Acute, Long Term and Home Care setting.
Cost Savings Less labor intensive and less costly then Negative Pressure Wound Therapy (NPWT). The ability to reduce healing times and complications can lead to signi� cant cost savings.
EWMA2011Brussels · Belgium
www.ewma2011.org

EWMA Journal Previous Issues
The EWMA Journals can be downloaded free of charge from www.ewma.org
Other JournalsThe section on International Journals is part of EWMA’s attempt to exchange information on wound healing in a broad perspective.
Advances in Skin & Woundcare, vol. 24, no 5, 2011www.aswcjournal.com
A Morphological and Biochemical Analysis Comparative Study of Collagen ProductsJeffrey C. Karr, Anna Rita Taddei, Simona Picchietti, Gabriella Gambellini, Anna Maria Fausto, Franco GiorgiA Case of Refractory Pyoderma Gangrenosum Treated with a Combination of Apligraf and Systemic Immunosuppressive AgentsGiacomo Duchini, Peter Itin, Andreas ArnoldOvercoming Lower-Extremity Wound Defects Using Hydrocolloid FramingBruce M. Goldstein
English
Journal of Wound Care, vol. 20, no 4, 2011www.journalofwoundcare.com
A clinical evaluation of the efficacy and safety of singlet oxygen in cleansing and disinfecting stagnating woundsG. Kammerlander, O. Assadian, T. Eberlein, P. Zweimeller, S. Luchsinger, A. AndriessenRole of oxygen in wound healing: A review of the evidence A.C. Chambers, D.J. LeaperWound healing following combined radiation and cetuximab therapy in head and neck cancer patientsN.R. Dean, L. Sweeny, P.M. Harari, J.A. Bonner, V. Jones, L. Clemons, H. Geye, E.L. Rosenthal
English
Helcos, vol. 22, no. 1, 2011
Pressure ulcers risk assessment scales for childrenFP García-Fernandez, PL Pancorbo-Hidalgo, JJ Soldevilla-AgredaMeasue healing in perssure ulcers. What do we have?JC Restrepo-Medrano, J VerdúThe skin has a symbolic characteristic because it is where the body and the spirit uniteJA Marina
Spanish
Haava, no. 4, 2010www.shhy.fi
Thema: BurnsBurns – Classification and treatmentLeena BergOperative treatment of burnsHeli KukkoElectricity damages – What they are?Leena BergTreatment of burns in history and today in HYK burn centerSari IlmarinenPaavo’s 1. day in intensive care unitLiisa Sikkilä
Finnish
Volume 10, no 1, January 2010
Systematic review of Repositioning for the Treatment of Pressure UlcersZena Moore, Seamus Cowman Analysis of wound care in nursing care homes as part of a district-wide wound care auditPeter Vowden, Kathryn VowdenChronic leg ulcers among the Icelandic population Guðbjörg Pálsdóttir, Ásta Thoroddsen Cross-sectional Survey of the Occurrence of Chronic Wounds within Capital Region in FinlandAnita MäkeläThe EWMA Teach the Teacher ProjectZena Moore
Volume 10, no 3, October 2010
Rationale for compression in leg ulcers with mixed, arterial and venous aetiologyHugo PartschPressure ulcers in Belgian hospitals: What do nurses know and how do they feel about prevention?D. Beeckman, T. Defloor, L. Schoonhoven, K. Vanderwee Nutritional Supplement is Associated with a Reduction in Healing Time and Improvement of Fat Free Body Mass in Patients with Diabetic Foot UlcersP. Tatti, A.E. Barber, P. di Mauro, L. MasselliChronic wounds, non-healing wounds or a possible alternative?M. BriggsSilver-impregnated dressings reduce wound closure time in marsupialized pilonidal sinusA. Koyuncu, H. Karadaˇ, A. Kurt, C. Aydin, O. TopcuVenous leg ulcer patients with low ABPIs: How much pressure is safe and tolerable?J. Schuren, A. Vos, J.O. Allen,Adherence to leg ulcer treatment: Changes associated with a nursing intervention for community care settingsA. Van Hecke, M. Grypdonck, H. Beele, K. Vanderwee, T. DefloorA Social Model for Lower Limb Care: The Lindsay Leg Club ModelM. Clark
Volume 10, no 2, May 2010
Hyperbaric Oxygen and Wounds: A tale of two enzymesThomas K. HuntHBOT in evidence-based wound healingMaarten J. LubbersComparative analysis of two types of gelatin microcarrier beads Mohamed A Eldardiri et al.Evidence based guidelines – how to channel relevant knowledge into the hands of nurses and carersSusan F. Jørgensen, Rie NygaardLack of due diligence in the prophylaxis of pressure ulcers?Dr. Beate Weber, Hans-Joachim CastrupSix prevalence studies for pressure ulcers – Snapshots from Danish HospitalsSusan Bermark et al.The Ransart Boot – An offloading device for every type of Diabetic Foot Ulcer?I.J.Dumont et al.The Haitian Earthquake, January 2010 John M Macdonald
Acta Vulnologica, vol. 9, no 1, 2011www.vulnologia.it
Daptomycin in the disinfection of complicated infected skin ulcers of the lower limbs in geriatric patients and candidates for reconstructive and/or regenerative surgeryCampitiello F., et al.Foam adhesive dressing in the treatment of leg skin ulcersBucalossi M., et al.Classification of peristomal skin changes:multicentric observational studyPisani F., et al.Chronic infected skin lesions, micro-organismsand bacterial resistanceNebbioso G., et al.Chronic skin ulcers in elderly patients: What are the outcomes?Peruzza S., et al.
Italian
Volume 1, no 1, January 2011 Who will take onAli Barutcu, Aydin O. Enver, Top Husamettin, Violeta Zatrigi Diabetic foot ulcer pain: The hidden burdenSarah E Bradbury, Patricia E PriceThe reconstructive clockwork as a 21st century concept in wound surgeryKarsten Knobloch, Peter M. VogtAnaemia in patients with chronic woundsLotte M. Vestergaard, Isa Jensen, Knud Yderstraede A survey of the provision of education in wound management to undergraduate nursing studentsZena Moore, Eric ClarkeCaring for Patients with Hard-to-Heal Wounds – Homecare Nurses’ NarrativesCamilla Eskilsson
EWMA Journal 2011 vol 11 no 2 48

EWMA
Wound Repair and Regeneration, vol. 19, no 3, 2011www.wiley.com
Time course of the angiogenic response during normotrophic and hypertrophic scar formation in humansWillem M. van der Veer, et al.Formulated collagen gel accelerates healing rate immediately after application in patients with diabetic neuropathic foot ulcersPeter Blume, et al.Development of the DESIGN-R with an observational study: An absolute evaluation tool for monitoring pressure ulcer wound healingYuko Matsui, et.alHow to assess scar hypertrophy – A comparison of subjective scales and Spectrocutometry: A new objective methodIlkka S. Kaartinen, et al.A novel noncontact method to assess the biomechanical properties of wound tissueClare Y. L. Chao, et al.Evaluation of effects of nutrition intervention on healing of pressure ulcers and nutritional states (randomized controlled trial)Takehiko Ohura, et al.
English
Wund Management, vol. 5, no 2, 2011 English abstracts are available from www.mhp-verlag.de
Classification of wounds at risk (W.A.R. score) and their anti-microbial treatment with polihexanide ó A practice-oriented expert recommendationJ. Dissemond, O. Assadian, V. Gerber, A. Kingsley, A. Kramer, D. J. Leaper, G. Mosti, A. Piatkowski, G. Riepe, A. Risse, M. Romanelli, R. Strohal, J. Traber, A. Vasel-Biergans,T. Wild, T. Eberlein Electrotherapy of chronic wounds: Evidence of clinical effectiveness and benefitK. Herberger, T. Kornek, E. S. Debus, H. Diener, M. Augustin
German
Wounds (SÅR) vol. 19, no 1, 2011www.saar.dkWill systematic actions for improvement of wound bed preparation, edema control and treatment of malnutrition lead to a better wound healing? A review of 33 treatment casesArne Langøen, Tove Sandvoll VeeDressings: Super absorbents in the treatment of woundsAnne HindhedeSoap is not recommended in the treatment of woundsJette Skiveren, Britta ÿstergaard Melby, Lis Kirkedal Bunder, Heidi Nordahl Larsen, Katja Safin Gudmundsen, Susan BermarkWound Management for Diabetic Patients: a Holistic ApproachSanne Wichmann
Scandinavian
Phlebologie, no 2, 2011www.schattauer.de
Outpatient varicose vein surgeryNeller5-year results for 980 nm endovenous laser obliteration of Beinvarizen. First comparisons with 1470 nm laser and laser radial probe.Pinzetta et al.Caliber reduction of the great saphenous vein and the femoral artery after CHIVAMendoza et al. Analgesic effect of topical sevoflurane on venous leg ulcer with intractable painGeronimo-Pardo et al. The CALISTO-studyBauersachsDifferential diagnoses of venous leg ulcersGallenkemper, Schimmelpfennig, Dissemond
English
Lietuvos chirurgija, vol. 8, no 4, 2010www.chirurgija.lt
Anal fistula plug for the treatment of complex fistula-in-anoPalubinskas E, Samalavicius NE, Gudelyte LAloplasty in inguinal hernia repair in LithuaniaNarmontas D, Gradauskas AComparative analysis of chronic hemorrhoids surgical treatmentDenisenko VLInjection of methylene blue solution into the inferior mesenteric artery of resected rectal specimens for rectal cancer as a method to increase lymph node harvestKlepsyte E, Samalavicius NEEarly results of incarcerated abdominal wall hernia repairStanaitis J, Saltanavicius R, Povilavicius J, Stasinskas AAcute mesenteric ischemia following cardiac surgeryAndrejaitiene JIncarcerated obturator hernia in 49 year old women: A case report and review of the literatureMarkevicius M, Lunevicius R, Markovas V, Stanaitis J
English
Leczenie Ran, Issue 1, Volume 8, 2011
Osteoprotegerin – a new marker of atherosclerosis helpful in selecting patients at amputation risk?Aleksandra Rumianowska, et al.The Doreen Norton scale for assessing risk of pressure ulcersKatarzyna Cierzniakowska, et al.Risk factors of lower limb amputation in diabetic foot syndromeBeata Mrozikiewicz-Rakowska, et al.The efficacy of selected antiseptics against CNS isolated from chronic wound infections examined in in vitro conditions and in conditions imitating the wound environmentMarzenna Bartoszewicz, et al.
Int. Journal of Lower Extremity Wounds vol. 10, no, 3, 2011http://ijlew.sagepub.com
Diabetic Foot Amputations in Greece: Where Do We Go From Here?N. Papanas,M.K. LazaridesImpact of Diabetic Foot Related Complications on the Health Related Quality of Life(HRQol) of Patients – A Regional Study in SpainE. García-Morales, et al.A Chronic, Destructive Mycetoma Infection in a Diabetic Foot in Saudi ArabiaM. Malone, Al Gannass, F. BowlingReview: The Diabetic Bone: A Cellular and Molecular PerspectiveRobert Blakytny, Maximilian Spraul, Edward B. JudeSeminar Review: A Review of the Basis of Surgical Treatment of Diabetic Foot InfectionsJavier Aragón-Sánchez
English
EWMA values your opinion and would like to invite all readers to
participate in shaping the organisation.Please submit possible topics for
future conference sessions.EWMA is also interested in receiving
book reviews, articles etc.
Please contact the Journal Secretariat at [email protected]
EWMA Journal 2011 vol 11 no 2 49

The Belgian Federation of Woundcare (BEFE-WO) was established in
2004 as the umbrella organisation of two major wound management associations in Belgium. Belgium is a bilingual country where both French and Flemish (Dutch) are spoken. The two wound management associa-tions existing at that time were CNC Wound Management Association and AFISCeP. An outcome of this joint partnership was the Bel-gian National Bilingual wound management conference in 2006 in Brussels. The success of this initiative has now resulted in an an-nual BEFEWO conference with over 450 par-ticipants each year. In 2011 the BEFEWO conference will be held during the EWMA conference at the SQUARE in Brussels. It is a great privilege in 2011 for BEFEWO to host EWMA’s conference in Brussels, the Euro-pean Capital, as it is also the fifth anniversary of the Belgian Bilingual National Conference.
The organisations not only collaborate with conferences but also in relation to liaising with the Belgian Government. Here the organisa-tions undertake common initiatives and rep-resent each other as BEFEWO members in diverse international organisations as EWMA, ECET, EPUAP and ETRS. BEFEWO is a joint organisation representing the strength, multilingualism and unity of Belgium and its wound management associations. Besides the interest in wound management both or-ganisations have a specific interest in ostomy care which is closely combined with wound management in Belgium.
CNC Wound Manage-ment Association (CNC WMA)Fifteen years ago CNC
WMA was established as a charity. The founding members of CNC WMA were Jan Vandeputte and Luc Gryson, both masters in Nursing Sciences and still active in wound management. Today CNC WMA has a board of managers, a council and an executive to fulfil all activities now delivered by CNC WMA. CNC WMA started as a very small specialised wound care nurses’ association but gradually healthcare professionals of different specialities also became interested in membership. Nowadays the healthcare professionals offer a val-uable contribution in the society’s activities and nurses of all specialities with an interest in wound management are becoming members.
The main purpose of CNC WMA is to promote education in wound care among doctors, nurses and other health care professionals. To this end, CNC WMA has a strong and firm collaboration with several University colleges making it possible to organise more than six basic wound manage-ment courses and two postgraduate courses for nurses each year. As a result of this CNC WMA has contributed to the education of over 3,000 nurses in modern wound care. In addition, CNC WMA, together with partners, offers over 25 different educational specialised pro-grams in wound management for nurses and doc-tors in Flanders. Since 1999 CNC WMA, together with The HUB University College of Brussels, has organised the post graduate course in wound management. In 2004 the same collaboration was set up with the KATHO University College. An-other joint activity with HUB University College Brussels will be the master class being launched in
INTRODUCING
The Belgian Federation of Woundcare
Brigitte Crispin President of AfiScep
and Befewo
Luc GrysonPresident of C.N.C.
and Befewo
EWMA Journal 2011 vol 11 no 2 50

April 2011. This is a new initiative on which there hopefully will be a lot of focus in the fu-ture.
Since 2000 an annual Flemish wound sympo-sium has been organised and in 2008 the sympo-sium became the Flemish Wound Management Conference. Held in Kortrijk with its mirror symposium in Hasselt –Genk the conference annually attracts over 700 doctors and nurses to attend.
Besides education and promotion of wound management, CNC WMA believes in collabora-tion between organisations to promote wound care issues. CNC WMA collaborates with NVKVV (Nationaal Verbond van Katholieke Vlaamse Verpleegkundigen) Flanders, a major Nurses organisation, regarding a joint member-ship at reduced annual fee opportunity; with VLAS, the Flemish ostomy organisation, re-garding educational activities and also with a steering committee of 21 local wound manage-ment companies to establish better education and awareness towards wound-care in Belgium.
In 2001, CNC WMA started a preliminary UCM (University Conference Model) concept at the EWMA conference for its postgradu-ate students. Since then CNC WMA has been proud to be able to send students to the confer-ence each year.
In 2011 the updated website, www.woundcare.be, will be launched which is a reference for Flemish students and nurses seeking compre-hensive and accessible information concerning wound management. Together with the paper version wondzorg.be this is the major reference source for the Flemish nurses and doctors.
INTRODUCING
The Belgian Federation of WoundcareAFISCeP.be – Association Francophone d’Infirmiers(ères) en Stomathérapie, Cicatrisation et Plaies Belgique
Nearly twenty years ago an association named ARIAS was established. This association handled the distribution of infor-mation regarding ostomised patients to nurses and attending doctors etc. for the more professional treatment of ostomised patients.
Five years later ABISCEP was established with the inten-tion to train stoma therapy nurses in Belgium. Over time, this association expanded into wound care and healing.
In 2007, these two francophone associations joined to-gether under one name: AFISCeP.be.
This association is very active. It organizes an annual confer-ence and roundtable meeting. In addition, some members are responsible for informing home care providers and future nurses in schools. It participates in the INAMI (Institut Na-tional Assurance Maladie Invalidité – National Institute for Disability Health Insurance) work group and defends patients for the reimbursement of equipment used in stoma care. The association works for the recognition of stoma therapy nurses and nurses specializing in wound care. In addition, AFISCeP.be also organises supplementary training events for certified stoma therapy nurses.
An additional project was a 900 hour stoma therapy and wound care training course that was organised to meet the Belgian legislation in the field. Our association works with CNC WMA to organise the BEFEWO conference which bring together the French and Flemish communities.
To support and complement its activities the AFISCeP.be publishes a quality journal twice a year that is respected and valued by all professionals. Its website, www.afiscep.be, also keeps members up-to-date on the latest news in the field. These projects all contribute to the dissemination of information and training to maintain a high skill level of caregivers in patient support and care. m
EWMA
EWMA201125-27 May
Brussels · Belgium
EWMA Journal 2011 vol 11 no 2 51

Patient Outcome Group (POG) is currently working on disseminating the messages for-mulated in the POG document “Outcomes
in controlled and comparative studies on non-healing wounds – Recommendations to improve quality of evidence in wound management”.
POG is currently initiating several projects to meet the general objectives: 1. Identify barriers: n With a starting point in the current debate
on evidence in wound healing and the Co-chrane levels of evidence, the group will de-fine the primary barriers (as experienced by clinicians and companies) related to the crea-tion and implementation of evidence-based guidelines in wound healing.
2. Propose guidelines for clinical data collection:
n The objective will be to define how exist-ing guidelines for clinical trials (e.g. RCTs or more “practical” studies (real life studies etc.)) can be adapted to wound manage-ment, by including, for example, other end points such as number of dressing changes, health economics, QOL, education of staff and structure of treatment.
3. Participate in the public debate / policy making:
n The working group should present a com-mon viewpoint on clinical trials of wound management products in relation to the de-bate on both national and European levels. A primary goal will be to influence the deci-sion making processes concerning approval and reimbursement of wound management products. EWMA will act as shareholder and work to influence the national agendas in order to put chronic wounds on the agenda.
n A central European HTA unit is assumed to be established. The working group should approach involved institutions in order to present the work and conclusions of the group in relation to evidence in HTA of wound management products.
4. Create and implement consensus: n Other interested parties (clinicians, compa-
nies, reimbursement authorities, European collaborative groups and institutions) should be involved in order to establish consensus within the area. A pan-European consensus with a national implementation strategy has been proposed.
POG conducted a Health Economics Course in Copenhagen which can be read about elsewhere in this Journal edition. Furthermore, the group is currently preparing EWMA Industry Course to be held on October 13-14th, 2011 in Budapest. The group is also working on translating the es-sential document into German and French in order to spread the messages of the work. Cur-rently there is a Polish translation of the docu-ment, which is available on the website.
Furthermore, the group is continuing to dis-seminate the messages of the POG document by addressing relevant concerns to the authorities in the EU and member states in order to enhance research in wound care and, in turn, create a better treatment of wounds for patients all over Europe.
POG currently consists of: Clinical:
Patricia Price, Chair (EWMA Council)Jan Apelqvist (EWMA Council)Finn GottrupLuc Gryson (EWMA Council)Hugo PartschRobert Strohal (EWMA Council)
Industry: Abbott Nutrition, B Braun, ConvatecLohmann and Rauscher, Mölnlycke
For further information about EWMA Patient Outcome Group, please visit ewma.org/english/patient-outcome-group.html. Any questions con-cerning Patient Outcome Group or the document can be sent to EWMA Secretariat: [email protected] m
·PAT
IENT OUTCOME GROUP·EUR
OPEAN
· WOUND ·MANAGEMENT· A
SSO
CIA
TIO
N
Patricia Price PhD, CHPsychol,
Chair of the EWMA Patient
Outcome Group
Dean and Head of School of Healthcare
Studies
EWMA Patient Outcome Group
EWMA update
EWMA
EWMA Journal 2011 vol 11 no 2 52

Bionect®Start
Start well, faster heal!
BIONECT® START is the bioactive solution for necrotic and fibrinous wounds. Fidia’s collagenase, developed from Vibrio Alginolitycus (non pathogenic bacterial strain), has a high purity grade to assure the respect of periwound skin. Hyaluronic acid provides an ideal wound environment and promotes wound healing. Hyaluronic acid + Collagenase

EWMA and the EWMA Patient Outcome Group introduce the EWMA Industry Courses 2011.
The two courses are held over two days. One course focuses onEvidence and Outcome and the other focuses on Health Economics.
The courses are primarily targeted at industry representatives, but will also be of relevance to clinicians and others interested in research and wound care economics.
·PAT
IENT OUTCOME GROUP·EUR
OPEAN
· WOUND ·MANAGEMENT· ASS
OC
IAT
ION
13-14 October 2011Generating Evidence in wound careThe course aims to give an introduction to clinical trials in addition to the use of alternative end points and outcomes in wound care. The course will provide the participants with an understanding of what the essential considerations and limitations are when conducting research in wound care. Furthermore, the participants will be provided with the necessary information on how to conduct evidence based research in wound care, taking the right measures into consideration.
13-14 October 2011Health EconomicsThis course aims to give an introduction to health economics and evaluation as applied to wound care. The course will provide the participants with an understanding of how to evaluate the economic benefits and challenges in prevention, diagnosis and treatment. The participants will aquire basic knowledge about economic analysis and training in the tools of how to conduct economic evaluation. The entry point is wound care, but the principles are general.
For more information and registration please visit www.ewma.org/industrycourse
EWMA INDUSTRY COURSES13 -14 October 2011 · Budapest, Hungary

Facilitated by the internationally recognised health economist John Posnett, the course took place on 7-8 April 2011 in Copenha-
gen, Denmark. The course was considered a pilot for future similar courses with the next EWMA Health Economics Course scheduled to take place in Budapest on 13-14 October 2011.
The main objective of the course is to pro-vide training in health economics principles and health economics analysis applied in wound care. Participants are, among other things, introduced to methods of how to elaborate and present argu-ments on modern wound care products and the organization of the treatment.
Learning objectives:n To understand why an economic approach
to wound care is essential for both clinicians and for the industry in the face of demo-graphic and technological trends;
n To understand how to demonstrate the value of good treatment to senior managers and other decision-makers, through audit and other forms of observational research;
n To learn how to undertake or to inter-pret the results of economic evaluations of healthcare interventions.
Feedback and evaluation by course participantsThe course attracted a mixed group of 30 par-ticipants including international clinicians (phy-sicians and nurses), industry representatives and EWMA Council members. The following feedback is based on the responses to an online evaluation questionnaire after the course.n 100% of the respondents expressed that the
course had met their expectationsn 100% of the respondents would recommend
the course to others.n The social & networking aspects of partici-
pation in the course were considered relevant by all participants.
Background for the course and contentThe EWMA Health Economics Course is a new activity under the auspices of the EWMA Patient Outcome Group (POG).
Meeting the objectives of EWMA POG, focus on the need for knowledge about health econom-ics is increasing due to the changing demographics and the continuing rise in the cost of health care provision across Europe.
Health Economics is based on the concept of scarcity, which suggests that there will never be sufficient resources to meet the ever growing need for health care by society. Thus, the under-lying premise is that the delivery of health care should be founded on equity and efficiency; in other words, making the best use of the resources available (Phillips 2005).
EWMA wants to contribute to maintain focus on the severe costs of wounds, thereby strengthen-ing the importance of wound care investments in order to improve conditions for patients.
Further information about the next EWMA Health Economy Course is available at:www.ewma.org/industrycourse m
References
Phillips CJ (2005); Introduction; In Health Economics an Introduction for Health Professionals (Phillips CJ ed.). British Medical Journal, Oxford, pp. 1-17.
Finn GottrupMD, DMSci
Professor of Surgery, Former Chair of the EWMAPatient Outcome Group
1st EWMA Health Economics Courseorganised by the EWMA Patient Outcome Group
·PAT
IENT OUTCOME GROUP·EUR
OPEAN
· WOUND ·MANAGEMENT· A
SSO
CIA
TIO
N
Participants at the 1st EWMA Health Economics Coursein Copenhagen, April 2011.
EWMA
EWMA Journal 2011 vol 11 no 2 55

INTRODUCTION The Eucomed AWCS group (www.eucomed.org) was founded back in June 2007, and since then we have had sixteen regular meetings. At present there are eight companies in the group: B. Braun, Co-vidien, ConvaTec, KCI, Mölnlycke Health Care, Paul Hartmann, Smith & Nephew and 3M. In addition, we also work in active partnership with EWMA and Policy Action.
The purpose of this paper is to give an update of our activities during the latest nine months, from July 2010 to March 2011.
STATUS REPORTQuestionnaire about Patient Safety sent out by the European Commission to the Member StatesWith short notice, the AWCS group together with EWMA was offered an opportunity to contribute to a questionnaire that was being finalized by the European Commission. This questionnaire, about Patient Safety, was sent by the Commission to the Member States by the end of March 2011. The purpose of the exercise was to support the European Commission in its review of the Coun-cil Recommendation on Patient Safety (approved June 2009). Our recommendation ended up in
nine distinct questions. Please see below for a list of the questions posed. While it is not certain that any questions submitted to the EC will in fact be used in the questionnaire for the Member States, the engagement alerts the Commission to AWCS/EWMA’s interest in this dossier and provides an avenue for future discussions with the Commission – particularly regarding the use of adequate wound care treatment to increase the patient safety.
Eucomed AWCS (Advanced Wound Care Sector)The 16th Eucomed AWCS meeting took place on 17-18 January 2011 at the B.Braun offices in Paris, commensurate with the CPC. This was a 1½ day session with a goal & strategy meeting followed by a normal meeting. The budget for the year 2011 will be €30,000 which means €5,000 per company. The priorities of the group during 2011 will be: n The European Commission AHAIP (Active
and Healthy Ageing Innovation Partner-ship), knowing that diabetes is a chronic dis-ease with a hidden potential for DFUs and thus a public health issue.
Hans Lundgren
Chair of the Eucomed Advanced Wound Care
Sector Group
Advanced Wound Care Sector (AWCS)
Status Report
EC Patient Safety Questionnaire to Member States
The European Wound Management Association (EWMA) and the Eucomed based Advanced Wound Care Sector Group (AWCS) recommends to the European Commission that the following questions be incorporated into the planned questionnaire sent to member states on Patient safety.
1. Does the member state have in place guide-lines for diagnosis and effective treatment of chronic/non-healing wounds?
Yes/no: ___If yes, which programmes/policies/performance para meters/quality measures are in place (home-care or hospital targeted)? ___
2. Do national targets exist for the prevention of wounds? Yes/no: ___ • Pressure ulcers (tic x): __ • Leg ulcers: __ • Diabetic foot ulcers: __ • Healthcare associated infections in wounds: __If yes, which programmes/policies/performance parameters/quality measures are in place? (please elaborate below): homecare or hospital targeted? ___
3. Do national targets exist for education and training specific to wound care and prevention with regards to adverse events, hereunder health care workers specialisation in wound prevention and treatment?
Yes/no: ___ • Pressure ulcers (tic x): __ • Leg ulcers: __ • Diabetic foot ulcers: __ • Healthcare associated infections in wounds: __If yes, which programmes/policies/performance parameters/quality measures are in place? (please elaborate below): homecare or hospital targeted? ___
Patient Safety in the EU
By Zena Moore
I am happy to announce that EWMA and the Eucomed based Advanced Wound Care Sector Group (AWCS) got a unique opportunity to be heard prior the European Commission Questionnaire to be send to all Member States on Patient safety.
EWMA recommended together with AWCS to the European Commission that the following questions be in-corporated into the planned question-naire sent to member states.
EWMA Journal 2011 vol 11 no 2 56

n “Patient Safety”, continue to be involved with this campaign through the risk of wound infections.
n “Continue the dialogue with national associations: SDMA and ABHI (UK), BvMed (Germany), Appamed (France), Assobiomedica (Italy) and Fenin (Spain).
n Work in active partnership with Policy Action and EWMA including the POG (Patient Outcomes Group).
Wound Care contribution to the European Commis-sion campaign on ‘Active and Healthy Ageing’Based on the EU2020 strategy for a smart, sustainable and inclusive Europe, the European Commission (EC) in October 2010 launched the Innovation Union Strategy. A key pillar of that strategy is the pilot Innovation Partner-ship on Active and Healthy Ageing. Eucomed answered to the EU public consultation by providing four proposals to the ‘Active and Healthy Ageing Partnership’ which revolve around:1. Developing procurement systems that focus on pro-
curing innovation. The UK and Sweden have devel-oped new approaches around this objective.
2. Facilitating research on the parameters that influence national and local procurement decisions.
3. Reducing risks and hospitalisation of people with cardiac problems. Raising awareness of the benefits of remote monitoring of cardiac devices and develop appropriate funding schemes.
4. Avoiding hospitalisation of people through effective community care in the areas of stoma, wounds and incontinence, conditions that have high prevalence in people with any chronic conditions.
Today, the medical technology industry is faced with a number of innovation hurdles which limit its potential
to contribute to a smart, sustainable and inclusive econo-my, ranging from limited end-user involvement, through patchy adoption of novel technology, to a lack of harmo-nisation in funding and reimbursement practices across the member states. Eucomed is of the opinion that, in partnership with other stakeholders, these innovation bar-riers can be overcome, thus contributing to the three goals the EC has set out for itself with this pilot partnership:1. Enabling EU citizens to lead healthy, active and in-
dependent lives while ageing;2. Improving the sustainability and efficiency of social
and health care systems;3. Boosting and improving the competitiveness of
the markets for innovative products and services, responding to the ageing challenge at both EU and global level, thus creating new opportunities for businesses.
Eucomed MedTech ForumOn 12-14 October 2010, the annual Eucomed MedTech Forum, organized under the patronage of Mr John Dalli, EU Health Commissionaire, took place in Brussels. The theme this year was “Europe 2020: Driving the innovation agenda” and the highlight of the event was a CEO Sum-mit. The forum attracted over 350 leaders from policy and scientific communities, along with the medical technol-ogy industry. The mission of Eucomed (www.eucomed.be) is to improve patient and clinician access to modern, innovative and reliable medical technology.
The CEO Summit welcomed representatives from both global and European industry leaders. In the first panel we saw:n Alex Gorski, Worldwide Chairman, Medical Devices
and Diagnostics Group, Johnson & Johnson n Pierre Guyot, CEO Mölnlycke Health Care n Srini Seshadri, President, Smiths Medical
4. Do national targets exist for the multidisciplinary approach to treatment and prevention of wounds?
Yes/no: ___ • Pressure ulcers (tic x): __ • Leg ulcers: __ • Diabetic foot ulcers: __ • Healthcare associated infections in wounds: __If yes, which programmes/policies/performance parameters/quality measures are in place? (please elaborate below): homecare or hos-pital targeted? ___
5. Does national targets/procedures/regulation exist for avoiding delay for patient treatment, hereunder organisation of treatments (e.g. clinical pathways)?
Yes/no: ___ • Pressure ulcers (tic x): __ • Leg ulcers: __ • Diabetic foot ulcers: __ • Healthcare associated infections in wounds: __If yes, which programmes/policies/performance parameters/quality measures are in place? (please elaborate below): homecare or hos-pital targeted? ___
6. Does national standardisation exist for wound care, hereunder national quality measures?
Yes/no: ___ • Pressure ulcers (tic x): __ • Leg ulcers: __ • Diabetic foot ulcers: __ • Healthcare associated infections in wounds: __If yes, which programmes/policies/performance parameters/quality measures are in place? (please elaborate below): homecare or hospital targeted? ___
7a. If data collection on wounds are in place which is collected and how is it reported?
• Incidence: __ • Prevalence: __ • Costs: __If yes, how is it reported? Which measures for exhaustive collection has been taken and how is it reported (e.g. clinical and/or research based collection, national/local)?
EWMA
EWMA Journal 2011 vol 11 no 2 57

The speakers gave a description of what they think the world will look like in five years and what it means for the industry and for its customers in terms of change. In his speech, Pierre Guyot started with an introduction of Mölnlycke Health Care, then continued with describing today’s challenges for the medtech industry in general, and finally asked how Europe can help to create a more innova-tive industry climate. The focal point of his presentation was on the coming shift from hospital care to community & homecare, and how government policy could help or hinder this change. The complete presentations from the MedTech Fo-rum can be found here, (www.eucomed.be/Home/por-tal/mtf2010_presentations/mtf_presentations.aspx)
IHE Forum (Swedish Institute of Health Economics)This year’s annual conference took place in Lund on 2-3 September 2010, with the theme “How can we promote innovations in healthcare? ”. There were many interesting speeches from different angles including “Innovation – what is that and how does it influence economic growth?”, “Purchase of innovations”, and “Value Based Pricing – To set the price on value or cost?”
Everyone agreed that innovations are necessary for society to grow and develop, but still public payers (government, county councils and municipalities) are reluctant to buy new innovative products. The reason for that is the care providers’ conservative idea of seeing their main goal as the care of patients and not as bringing in innovations in the healthcare process. Therefore we must apply a holistic view of health and social care. In the end it is all about customer benefits, in terms of utility for the patients, care-givers and relatives, but also in services and efficiency in the process and organization around the patient. m
8. Do national targets exist for research support on chronic/ non-healing wounds?
Yes/no: ___ • Pressure ulcers (tic x): __ • Leg ulcers: __ • Diabetic foot ulcers: __ • Healthcare associated infections in wounds: __If yes, which programmes/policies/performance parameters/quality measures are in place? (please elaborate below): homecare or hospital targeted? ___
9. Does national targets/procedures/regulation exist for patient rights to choose between treatment regimes, hereunder reimbursement of services (e.g. prevention tools)?
Yes/no: ___ • Pressure ulcers (tic x): __ • Leg ulcers: __ • Diabetic foot ulcers: __ • Healthcare associated infections in wounds: __If yes, which programmes/policies/performance parameters/quality measures are in place? (please elaborate below): homecare or hospital targeted? ___
EWMA
EWMA Journal 2011 vol 11 no 2 58
This 4 day theoretical course & practical training gives participants a thorough intro-duction to all aspects of diagnosis, manage-ment and treatment of the diabetic foot.
Lectures will be combined with practical sessions held in the afternoon at the diabetic foot clinic at the Pisa University Hospital.
Lectures will be in agreement with the International Consensus on the Diabetic Foot & Practical Guideline on the Management and Prevention on the Diabetic Foot.
·COURSE ENDORSED BY
·
EUR
OPEAN
· WOUND ·MANAGEMENT· A
SSO
CIA
TIO
N
This course is endorsed by EWMA.
Management ofthe Diabetic FootTheory & Practice4 Day Course, 3 - 6 October 2011Pisa, Italy
www.diabeticfootcourses.org

1-K158 WC11 FP Europe ad:1-K158 WC11 FP Europe ad 4/4/11 10:28 AM Page 1

BACKGROUNDResearch within wound care is fragmented and it is difficult to find validated data on the preva-lence and costs of wounds. The EWMA Patient Outcome Group has for some time been working for creating better evidence in wound care and spreading the understanding of the complex ap-proach to wound care research.
The purpose of the EWMA Wound Survey is to uncover the true resource costs of wounds to hos-pital and community care health care providers in different countries in Europe. Uncovering the prevalence of wounds, the hours and time con-sumption of health care professionals, and the costs of treatment materials and wound-related hospitalisation in specific health care providers’ organisations, serves to raise awareness of the true significance of good wound care.
Specifically the surveys will focus on:1) The prevalence of all types of wounds, in
both hospitals and in municipalities/com-munity service.
2) The costs of wound treatment in hospitals and in municipalities/community care.
3) Convey publications and discussion papers/arguments that can serve as a political tool to increase awareness among politicians of the actual prevalence of wounds and to reveal the actual resources being used to treat the wounds.
METHODSThe studies are part of a EWMA project, which will cover several European countries. The first study using this methodology was done in Hull in the UK, published in the International Wound Journal, 20081 and this methodology has been adapted for the EWMA studies.
The study is intended to be made as a “point prevalence” study. For practical reasons, data will
1 ”Drew P, Posnett J, Rusling L. The Costs of wound Care for a local population in England. International Wound Journal 2007; 4(2): 149-155
be was collected over 2 days in hospitals and over 1 week in communities. Data are collected by go-ing through all patient files in all hospital wards and in all community nursing centres as well as in all nursing homes.
The researchers all take an active role in gath-ering the data and in obtaining approval for the study with the hospital management and with the community nursing service.
The data are collected for each patient are catego-rised and represent some of the following: n Number of wounds n Condition of the woundn Type of woundn Place of origin
The nursing staff collecting the data will access the wounds and record the time consumption for each patient per dressing change, for travelling time and for documentation. Combining the time consumption with the average cost of a nursing hour, and extrapolating the data to the entire country, the total cost for the nursing time con-sumption for wound treatment can be calculated.
Similarly, the total cost for dressings and wound-related hospitalisation can be calculated, and adding these two costs together a total cost of wound care can be measured.
The data collected in a database from where the statistical analysis is taken from and thus cal-culated the costs of the wound treatment.
RESULTS The results of the survey are presented in tables with written analysis and the following is essential to prospects of the idea behind the survey.
Finn GottrupMD, DMSci
Professor of Surgery, Former Chair of the EWMA
Patient Outcome Group
EWMA Wound SurveysResource consumption for wound care
EWMA Journal 2011 vol 11 no 2 60

EWMA
As a member of EWMA, you already receive numerous bene ts in terms of access to information and advice on the latest trends in wound care practice. We would like to offer you one more.
Journal of Wound Care is a leading monthly international MEDLINE-listed wound care journal, with a loyal global audience and contributors from every continent. JWC provides a truly global perspective on wound care, from the latest in evidence-based practice to cutting-edge research from the US, Europe and elsewhere.
SUBSCRIBE TODAY and receive special rates online by visiting
www.journalofwoundcare.com/EWMA
j o u rnal of w o u nd ca r e
? ? C W
C
? ? ? v o l u m e 1 9 . n u m b e r 1 1 . n o v e m b e r 2 0 1 0
NPWT: a systematic reviewVenous reflux in delayed leg ulcer healing
A review of pilonidal sinus disease: part one
Clinical report: a new negative pressure wound therapy system
Can thermography predict delayed healing in pressure ulcers?
Antibiotic beads in a Charcot foot
JWC_19_11_frontcover.indd 1 04/11/2010 17:02
W v o l u m e 1 9 . n u m b e r 1 1 . n o v e m b e r 2 0 1 0
NPWT: a systematic reviewVenous reflux in delayed leg ulcer healing
A review of pilonidal sinus disease: part one
Clinical report: a new negative pressure wound therapy system
Can thermography predict delayed healing in pressure ulcers?
j o u rnal of w o u nd ca r e
? ? C W
C
? ? ? v o l u m e 1 9 . n u m b e r 1 2 . d e c e m b e r 2 0 1 0
Pilonidal sinus disease: a reviewPsychological profile of patients with neglected malignant wounds
Marjolin’s ulcer in the natal cleft mimics anal canal carcinoma
Reconstruction of a chronic late post-nephrectomy wound
Clinical and cost effectiveness evaluation of low friction and shear garments
International organisations update
COVER.indd 1 03/12/2010 12:25
j o u rnal l l of f f w o w o w u nd d d ca r e W
C
v o l u m e 1 9 . n u m b e r 1 2 . d e c e m b e r 2 0 1 0
Pilonidal sinus disease: a reviewPsychological profile of patients with neglected malignant wounds
Marjolin’s ulcer in the natal cleft mimics anal canal carcinoma
Reconstruction of a chronic late post-nephrectomy wound
j o u rnal of w o u nd ca r e
? ? C W
C
? ? ? v o l u m e 1 9 . n u m b e r 1 0 . o c t o b e r 2 0 1 0
Using electrical stimulation to treat scarsEffect of elasticity on sub-bandage pressure in two bandaging systems: a RCT
Why do wound dressings have a potential analgesic effect?
Predicting which organisms might cause infection in a resource-poor setting
Potential effects of honey on angiogenesis: an animal study
A bizarre presentation of necrotising fasciitis in the cervicofacial region
Severe hidradenitis suppurativa: a case report
JWC_19_10_frontcover.indd 1 07/10/2010 16:18
VISIT NOW:
www.journalofwoundcare.com/EWMA
JWC_EWMA_Offer_HP Dec10.indd 1 23/12/2010 15:15
The prevalence of the wound collected in both hospital and municipalities/community care is presented, hereun-der the following parameters are covered: n No. of Citizens covered (population)n Percentage of inhabitantsn No. of Patients with wound(s)n Prevalence per 1000 populationn Percentage of hospital patients with woundsn Calculated total no. of patients with wound(s)
The different types of wounds are presented:n Acute/surgical woundn Pressure Ulcersn Leg Ulcersn Diabetic Foot Ulcersn Other n Total no
Furthermore, the types of wounds are correlated with the resource consumption of the treatment of the wound. The results presented are: n Nursing time (minutes) per dressing changen Travelling time Documentation time (minutes)n Total, cost of nursing timen Total cost of dressingsn Total cost nursing time and dressingsn Total cost of wound-related hospitalisation
CONCLUSIONThe purpose of the surveys is to present the costs in the individual country of wound care. The results of the sur-vey will convey the ability to hospital and municipalities/community care givers to view their actual cost. This will facilitate a dialogue with policy makers and other admin-istrators and result in saved money and improvement of the quality of life for the patients.
Currently the surveys of this kind have been conducted in England and Denmark and the results are presently being processed in Denmark. Further surveys are planned in Germany, Italy and Portugal and later in France and Spain. m
The Danish Wound Survey
Nina Bækmark, MScFinn Gottrup, Professor, MD, DMSci. Eskild W. Henneberg, MDJohn Posnett, BA (Hons), DPhil (Econ). Heron HealthJan Sørensen, MDRikke Trangbæk, MSc

MSKTHungarian Wound Care Society
www.euuzlet.hu/mskt/President: Dr. Hunyadi János
Activities: – Annual congress every year
in October– Publishes the journal Sebkezelés
Sebgyógyulás– Aims at spreading of practical
and scientific knowledge regard-ing wound healing between MD’s and health care workers.
Together with the wound management associations in the Slovak Republic, Austria and Hungary, the International
Compression Club (ICC) and EWMA arrange a sequence of 3 Leg Ulcer & Compression seminars in Bratislava, Vienna and Budapest on the 10th, 11th and 13th of October 2011.
The national wound management associa-tions involved are the Austrian Wound Associa-tion (AWA), the Slovak Wound Care Associa-tion (SSOOR), the Hungarian Association for the Improvement in Care of Chronic Wounds and Incontinence (SEBINKO) and the Hungarian Wound Care Society (MSKT).
The program draws on the existing ICC con-sensus documents on compression therapy as well as results and experiences gained through the im-plementation of the EWMA Central & Eastern European Leg Ulcer Project (LUP) carried out by the wound associations and project teams in Slovenia, Poland and the Czech Republic.
The overall objective of the Leg Ulcer & Com-pression seminars is to discuss and plan for the establishment of national consensus on prevention and treatment of leg ulceration using compression therapy. In each country the seminar program is
Hugo Partsch ICC President
Finn Gottrup Former chair of
the EWMA Patient Outcome Group
National collaboration for the Leg Ulcer & Compression Seminars 2011
based on the current national situation with re-gards to the treatment of leg ulceration.
Further information and preliminary pro-gramme for the Leg Ulcer & Compression semi-nars is available at www.ewma.org/icc-ewma-seminar/
The role of the national wound associations In order to achieve the objectives of the Leg
Ulcer & Compression seminars a close collabo-ration between the local wound associations, the ICC and EWMA is essential.
Apart from chairing the Leg Ulcer & Com-pression seminars together, the national associa-tions play a key role in facilitating the involvement of national stakeholders in the seminars and the follow-up activities which may prove to be the most important result of the seminars.
In Hungary, the annual meetings of MSKT and SEBINKO will take place in connection with the Leg Ulcer & Compression seminars. The two Hungarian associations will hold their meetings with a joint exhibition on 12 October at the same venue where the seminars will take place on 13 October.
For more information about the national wound associations please see below. m
AWA Austrian Wound Association
www.a-w-a.at
No. of members: 240President: Franz Trautinger
Activities: – Annual Congress– Foster education and
research in wound care
SEBINKOHungarian Association for the Improvement in Care of Chronic Wounds and Incontinence
www.sebinko.hu
No. of members: 198President: Fokiné Karap Zsuzsanna
Activities: – Annual congress every year
in October– Publishes the SEBINKO Journal
twice a year
SSOORSlovak Wound Care Association
www.ssoor.sk
No. of members: 31President: Jozefa Košková
Activities: – Cooperation with teaching
institutions and wound care specialists
– Review the wound situation in Slovakia
EWMA
EWMA Journal 2011 vol 11 no 2 62

Organised by: EWMA & International Compression Club (ICC)
BRATISLAVA 10 OCTOBER
VIENNA 11 OCTOBER
BUDAPEST 13 OCTOBER
LEG ULCER & COMPRESSION SEMINARS 2011
LEG ULCER & COMPRESSION SEMINARS 2011
For information about the programme, registration etc. please visit the website www.ewma.org/icc-ewma-seminar The seminars will be held in local languages and English with simultaneous translation.

Wound ManagementSmith & Nephew Medical Ltd101 Hessle RoadHull, HU3 2BNUnited KingdomTel: +44 (0) 1482 225181Fax: +44 (0) 1482 328326www.smith-nephew.com/wound
Sorbion AGIm Suedfeld 1148308 Senden GermanyTel.: +49 (0) 2536 34 400 400Fax: +49 (0) 2536 34 400 410www.sorbion.com
Systagenix Wound ManagementGargraveNorth YorkshireBD23 3RXUnited KingdomTel: +44 1756 747200Fax: +44 1756 747590 www.systagenix.com
Corporate A
Abbott Nutrition200 Abbott Park RoadAbbott Park Illinois 60064USATel: +1 (614) 624-7485 Fax: +1 (614) 624-7899www.abbottnutrition.com
ConvaTec EuropeHarrington HouseMilton Road, Ickenham, UxbridgeUB10 8PUUnited KingdomTel: +44 0 1895 62 8300Fax: +44 0 1895 62 8362www.convatec.com
Covidien154, Fareham Road PO13 0AS GosportUnited KingdomTel: +44 1329 224479 Fax: +44 1329 224107www.covidien.com
Paul Hartmann AGPaul-Hartmann-StrasseD-89522 HeidenheimGermanyTel: +49 0 7321 / 36-0Fax: +49 0 7321 / 36-3636www.hartmann.info
KCI Europe Holding B.V.Parktoren, 6th floorvan Heuven Goedhartlaan 111181 LE AmstelveenThe Netherlands.Tel: +31 0 20 426 0000Fax: +31 0 20 426 0097www.kci-medical.com
Lohmann & RauscherP.O. BOX 23 43 NeuwiedD-56513 GermanyTel: +49 0 2634 99-6205Fax: +49 0 2634 99-1205www.lohmann-rauscher.com
Mölnlycke Health Care AbBox 13080402 52 Göteborg, SwedenTel: +46 31 722 30 00Fax: +46 31 722 34 01www.molnlycke.com
Ferris Mfg. Corp.16W300 83rd StreetBurr Ridge, Illinois 60527-5848 U.S.A.Tel: +1 (630) 887-9797 Toll-Free: +1 (630) 800 765-9636 Fax: +1 (630) 887-1008www.PolyMem.eu
Corporate Sponsor Contact Data
Use the EWMA Journal
to profile your company
Deadline for advertising
in the October 2011 issue is
1 September 2011
EWMA Journal 2011 vol 11 no 2 64

B. Braun Medical 204 avenue du Maréchal Juin92107 Boulogne BillancourtFranceTel: +33 1 41 10 75 66Fax: +33 1 41 10 75 69www.bbraun.com
BSN medical GmbHQuickbornstrasse 2420253 HamburgTel: +49 40/4909-909Fax: +49 40/4909-6666www.bsnmedical.comwww.cutimed.com
Curea Medical GmbHMünsterstraße 61-6548565 SteinfurtGermanyTel: +49 36071 9009500Fax: +49 36071 9009599www.curea-medical.de
Flen pharma NVBlauwesteenstraat 87 2550 KontichBelgiumTel.: +32 3 825 70 63Fax: +32 3 226 46 58www.flenpharma.com
HILL-ROM 83, Boulevard du Montparnasse 75006 Paris France Tel: +33 (0) 1 53 63 53 73Fax: +33 (0) 1 53 63 53 70www.hill-rom.com
3M Health CareMorley Street, LoughboroughLE11 1EP LeicestershireUnited KingdomTel: +44 1509 260 869Fax: +44 1 509 613326www.mmm.com
Advanced BioHealing, Inc.10933 N. Torrey Pines Road, Suite 200La Jolla, CA 92037Tel: 858.754.3705Fax: 858.754.3710www.AdvancedBioHealing.com
AOTI Ltd.Qualtech HouseParkmore Business Park WestGalway, IrelandTel: +353 91 660 310Fax: +353 1 684 9936www.aotinc.net
ArjoHuntleigh310-312 Dallow RoadLutonLU1 1TD United KingdomTel: +44 1582 413104Fax: +44 1582 745778www.ArjoHuntleigh.com
Corporate B
EWMA
Life Wave9 Hashiloach St.P.O.B. 7242Petach Tikvah 49514IsraelTel: +972-3-6095630Fax: +972-3-6095640www.life-wave.com
Nutricia Advanced Medical NutritionSchiphol Boulevard 1051118 BG Schiphol AirportThe Netherlandswww.nutricia.com
Organogenesis Switzerland GmbHBaarerstrasse 2 CH-6304 Zug SwitzerlandTel: +41 41 727 67 89www.organogenesis.com
PhytoceuticalsZollikerstrasse 448008 ZurichSwitzerlandTel: +41 58 800 58 58www.1wound.info
Argentum Medical LLCSilver Antimicrobial Dressings2571 Kaneville CourtGeneva, Illinois 60134U.S.A.Tel: +1 630-232-2507Fax: +1 630-232-8005www.silverlon.com
TEVA5 Basel St. Petach Tikva 49131IsraelTel: +972 8 932 4000Fax: +972 8 932 4001www.polyheal.co.il
Laboratoires Urgo42 rue de Longvic B.P. 15721304 Chenôve FranceTel: +33 3 80 54 50 00 Fax: +33 3 80 44 74 52www.urgo.com
Welcare Industries SPAVia dei Falegnami, 705010 Orvieto ( TR )ItaliaTel: +39 0763-316353Fax +39 0763-315210www.welcaremedical.com
EWMA Journal 2011 vol 11 no 2 65

Conference Calendar
Organisations
For web addresses please visit www.ewma.org
Conferences Theme 2011 Days City Country
Annual Meeting of the Chronic Wounds Initiative (ICW) May 11-12 Bremen Germany
Annual Meeting of the Italian Nurses’ Cutaneous Wounds Association (AISLeC)
May 12-14 Bologna Italy
21st Conference of the European Wound Management Association
Common Voice – Common Rights May 25-27 Brussels Belgium
12th EFORT Congress Jun 1-4 Copenhagen Denmark
International Lymphoedema Framework Conference Towards Global implementation of Best Practice – Opportunities and Challenges
Jun 16-18 Toronto Canada
Annual Meeting of German Society of Wound Healing and Wound Treatment (DGfW)
Guidelines and quality standards of Fascinating Biotechnology
Jun 23-25 Hannover Germany
14th Annual European Pressure Ulcer Meeting (EPUAP) Pressure Ulcer Research Achievements Translated to Clinial Guidelines
AugSep
31-2 Oporto Portugal
30th Annual meeting of the European Bone and Joint Infection Society
Biofilm and Health Economics in Bone and Joint Infections
Sep 15-17 Copenhagen Denmark
Annual meeting of Italian Association for the Study of Cutaneous Ulcers (AIUC)
Sep 21-24 Ancona Italy
Pisa International Diabetic Foot Courses Oct 3-6 Pisa Italy
Bi-Annual Conference of the Wound Management Association of Ireland
Oct 4-5 Galway Ireland
21st Annual European Tissue Repair Society Oct 5-7 Amsterdam Netherlands
EWMA Leg Ulcer and Compression Seminars Oct 10 Bratislava Slovakia
EWMA Leg Ulcer and Compression Seminars Oct 11 Vienna Austria
EWMA Leg Ulcer and Compression Seminars Oct 13 Budapest Hungary
4th Latin American Conference on Ulcers Oct 11-14 Rio de Janeiro Brazil
EWMA Master Course 2011 Is Oedema a Challenge in Wound Healing? Oct 13-14 Budapest Hungary
EWMA Industry Course 2011 Health Economics and Generating Evidence in wound healing – clinical trials, alternative end points and outcome
Oct 13-14 Budapest Hungary
The Annual Fall Symposium on Advanced Wound care (SAWC/WHS)
Oct 13-15 Las Vegas USA
First International Pediatric Wound Care Symposium Oct 27-29 Rome Italy
Biannual meeting of the Woundcare Consultant Society Nov 22-23 Utrecht Netherlands
Annual Meeting of the Danish Wound Healing Society Nov 24-25 Kolding Denmark
2012
16th National Conference of wound healing of CPC Jan 15-17 Paris France
10th National Australian Wound Management Associa-tion Conference
Mar 18-22 Sydney Australia
World Council of Enterostomal Therapists Conference Apr 19-23 Adelaide Australia
22nd Conference of the European Wound Management Association
May 23-25 Vienna Austria
4th Congress of the World Union of Wound Healing Societies
Better care – Better Life Sep 7-12 Yokohama Japan
10th Scientific Meeting of Diabetic Foot Study Group (DFSG)
Sep 28-30 Potsdam Germany
EWMA Journal 2011 vol 11 no 2 66

FUNDRAISING CAMPAIGN DURING THE EWMA BRUSSELS CONFERENCE
Support the WAWLC Podoconiosis Eradication Project in Ethiopia
AIMS OF THE WAWLC INITIATIVE:
n Training for 200 health care providers from 50 different hospitals, clinics and organisations
n Training to Health Extension Workers and local non-medical community agents, especially women
n Provision of kit (education material and supplies) for each participant to teach & treat patients
n Meeting with Ethiopian Ministry of Health in August 2011
About Podoconiosis:
n An endemic non-filarial elephantiasis,
commonly known as “Mossy Foot”.
n Affects > 1 million people in rural villages of Ethiopia.
n Listed by WHO as neglected tropical disease in 2010.
EWMA has since 2009 been part of the WAWLC initiative.
EWMA201125-27 May
Brussels · Belgium
Donations are welcomed at the EWMA Conference or at http://wawlc.org/donation.html

ienna · Austria · Österreich
Organised by the European Wound Management Association in cooperation with Die Österreichische Gesellschaft für Wundbehandlung AWA (Austrian Wound Association)
Organisiert von: der Europäischen Wound Management Organisation in Zusammenarbeit mit der Österreichische Gesellschaft für Wundbehandlung, AWA
WWW.EWMA.ORG / EWMA2012
22nd Conference of the European Wound Management Association22. Kongress der European Wound Management Association
EWMA 201223-25 May / Mai · 2012
Bilingual:
English & German
Zweisprachig:
Englisch & Deutsch
WOUND HEALING – DIFFERENT PERSPECTIVES, ONE GOAL
WUNDHEILUNG – UNTERSCHIEDLICHE PERSPEKTIVEN, EIN ZIEL

ETRSEuropean
Tissue Repair Society
Prof.dr. Gerrolt N. Jukema
Member of the EWMA council,
board member of the ETRS
Building on the long standing tradition and the rela-tionship between EWMA and the European Tissue Repair Society, the interaction between both societies has become even more intense during the last two years. To continue their established relationship and develop an even closer collaboration, a combined session was scheduled during the 20th European Tissue Repair Society Congress in Gent Belgium, 15-17 September 2010.
The local host of the meeting was the University of Gent. The congress venue was an historical building of the University (‘het Pand’) in the historical part of the old city. The congress was attended by numerous delegates from all over Europe and the United States of America.
The topic of the combined EWMA / ETRS session was ‘Management of Acute Wounds.’ This session was chaired by Finn Gottrup and Gerrolt Jukema (a member of the EWMA council and a board mem-ber of the ETRS).
Martin Koschnik highlighted in his presentation the clinical relevance of antiseptic treatment of contami-nated and infected wounds with polyhexanid (PHMB) solution.
16 Billions Approx.Health Care Budget for the year 2011
An invitation to expand and invest in the biggest market among Gulf Region
Comate Ltd.,is fully equipped with all necessary infrastructure to launch your product in Saudi Arabia.
Comate Ltd., is successfully representing many world renowned manufacturers.
Comate Ltd., is one of the leading companies in the field of Medical Equipments, Wound Care Management & Dental materials in
Kingdom of Saudi Arabia dealing with more than 100 potential customers in
Governmental & Private Sectors since 1989. [email protected]
[email protected] Office : RiyadhP.O Box 88552 Zip Code 11672Kingdom of Saudi Arabia
Conference Report ETRS
EWMA Session, 20th Annual European Tissue Repair Society Congress Gent, 15-17 September 2010
Gerrolt Jukema presented experimental clinical data on infected trauma and orthopedic wounds. In addi-tion, new modalities for treatment of acute and infected wounds were presented, including topical negative wound therapy and the installation tech-nique with polyhexanid solution. Maggot therapy for treatment of infected wounds, including data from his experimental research, was also presented.
Finn Gottrup, as the current chair of the EWMA Patient Outcome Group, shared his thoughts with the audience about problems with evidence and outcomes in wound healing studies. This session was very well attended by congress participants and featured an interactive discussion with the presenters, reflecting the close relationship between the lab and the clinician. Experimental research, based on clini-cal problems studied in relation with patients’ care-related infections, can be a map guiding us to im-proved and quality-related patient care.
A new combined, clinical-orientated session of both societies is scheduled at the 21st Annual European Tissue Repair Society Congress in Amsterdam, The Netherlands, on October 5th-7th 2011. It is sure to be both interesting and informative, and further develop the close relations between these two wound societies. m
Organisations

Anna HjerppeMD, Clinical teacher,
President
Department of Dermatology, Tampere University Hospital,
Finland
www.suomenhaavanhoitoyhdistys.fi
FWCS Finnish Wound
Care Society
In February this year, The Finnish Wound Care Society organized its fourteenth, national, two day congress on wound healing. The theme was:
Challenging and uncommon wounds
The theme was selected according to suggestions from the field. Although these wounds are rare and more seldom diagnosed than wounds such as venous leg ulcers, they pose real challenges both for the patient and for the health care system.The theme was split into four main sessions.
The first session focused on malignant fungating wounds. We had a leading Finnish dermato-pathologist to give an introductory lecture on the different manifestations of skin cancers and can-cer metastasis to the skin. This was followed by the different treatments and finally there was a nurse-led lecture on the special wound care of these extremely hard-to-heal or non-healing wounds. Caring for a patient with a malignant fungating wound is a challenge for any nurse or doctor regardless of their years of experience in wound care. The wounds cause huge distress for the patient including pain, malodour, haemor-rhage, excessive exudate and infection, altered body image and social isolation. Neglect may also play its role with patients with advanced malignant wounds. The patient and his family may fail to seek medical help even if the wound is clearly vis-ible. The stories about the patients with malignant fungating wounds were listened to attentively by our audience. The informative lecture improved both their knowledge and clinical understanding of patients with malignant fungating wounds.
The second session focused on acute traumatic wounds, especially on wounds in fragile elderly skin or traumatic amputations. This lecture was very appropriate as, at the same time as our con-ference, the Fair Centre was also hosting a big motorcycle event and many of those traumatic amputations discussed seemed to have happened to motorcyclists!
The third session about pressure ulcers (PU) was held the next morning. This theme was chosen to cover the new EPUAP and NPUAP Guidelines. The session included the presentation of the new Guidelines which the Finnish Wound Care Society has had translated into Finnish to enable health-care professionals in Finland to fully understand them; no more excuses for not preventing PUs! Our fourth session concentrated on various types of skin vasculitis, from the diagnosis to the treat-ment and to local wound care.
Along with the main sessions, we had organised practical workshops. The workshops focussed on five common wound care themes: debridement, ABI- measuring, compression therapy, how to choose a right wound care product and how to dress a difficult wound.
There were 96 participants at these workshops (fully booked). And the participants had a chance to learn “hands on” about the themes. Each work-shop included about 20 minutes introduction and 20 minutes of practical experience. Organizing workshops requires strenuous efforts from our organizing committee and is not financially profitable, but we included them as they offer a very beneficial way of learning.
The venue was in the Helsinki Fair Centre, in the congress area. We have chosen this same venue for four years now, because it is very easy to get there from all over Finland. Also the personnel of the Fair Centre are very professional and have become almost “friends” to us which made the hard work of organizing such an event easier for us all.
On the first night of the congress we always have a ‘get together’ evening party which also takes place in the Fair Centre. The event is free of charge and has a free buffet for participants. This year’s theme was “TexMex” and featured not only a buffet of food chosen to go with the theme, but also some Tequila girls who danced and served tequila for those who wanted to enjoy tequila slammers; some participants had quite a head-ache the next morning!
The 14th national wound healing congress in Helsinki, Finland
Organisations
EWMA Journal 2011 vol 11 no 2 70

The objective of the evening party is to make social contacts with other delegates and to meet friends. The company members can also attend, so it is also a good marketing possibility for them. The party has always been very successful and popular with the participants; this year we had there almost 300 partygoers!
Over all we had around 650 participants at this year’s congress. This was only about 100 fewer than the year before, so our fears about the theme were unnecessary. We had a marketing area of 280m2 for wound care companies and 37 companies attended. We are very strict about what kinds of companies are allowed to participate; only those companies that are gen-uinely involved in wound care are welcomed. This is because we want to preserve our status as professionals. We also reward our lecturers well for presenting the lectures; that way we can ensure very high standard specialist lectures and we can be sure the knowledge is always up to date and evidence based.
In all, our congress was, once again, a very successful event: the lectures were brilliant and kept to schedule, the food was good, the exhibi-tion looked very impressive and the feedback that we had was mainly positive. Next year is our 15th national congress. The planning and organizing has already started, the theme has been chosen and marketing has begun.
The congress will be built around the theme of acute wounds, so that it can serve as many healthcare professionals as possible. This theme was last presented six years ago and the event was the biggest success we’ve ever had. That time there were over 1100 participants and we are hoping to have the same amount of partici-pants next year or even more; that will be a really huge challenge for us! However, with a good program, top lecturers and the good repu-tation that we have gained over the years, the challenge will not be an impossible one! m
Since 2007, EWMA has successfully offered students of wound management from institutes of higher education across Europe the opportunity to take part of academic studies whilst participating in the EWMA Conference. In 2011 it is expected that students from the institutes listed below will participate in the EWMA UCM in Brussels.
The opportunity of participating in the EWMA UCM is available to all teaching institutions with wound management courses for health professionals.
EWMA strongly encourages teaching institutions and students from all countries to benefit from the possibilities of international networking and access to lectures by many of the most experienced wound management experts in the world.
Yours sincerely
Zena Moore, Chair of the EWMA Education Committee, EWMA President
THE EWMA UNIVERSITY CONFERENCE MODEL (UCM)
in Brussels
Participating institutions:
For further information about the EWMA UCM, please visit the Education section of the EWMA website www.ewma.org or contact the EWMA Secretariat at [email protected]
Haute École de Santé Geneva, Switzerland
HUB BrusselsBelgium
KATHO university college Roeselare
Belgium
Escola Superior de Enfermagem de LisboaPortugal
University of Hertfordshire United Kingdom
Universidade Católica Portuguesa Porto, Portugal
EWMA201125-27 May
Brussels · Belgium
EWMA Journal 2011 vol 11 no 2 71

Rytis Rimdeika
Member of EWMA Council, President of LWMA
On November 25-26th, 2010, in Kiev, the capital of Ukraine, the conference “Wounds, Wound Infections and Wound Closure” was organised by the newly established Ukrainian Wound Treatment Organization (UWTO).
This association is the first in the Ukraine that focuses on wound treatment. The instigators of UWTO have worked tremendously hard establish-ing local sections in 15 regions of the Ukraine. In the beginning the Ukrainian association was mainly based on the initiative of doctors from vari-ous specialties but there is a clear determination for the association to become open to healthcare professionals from multiple disciplines.
UWTO has a very strong council of well-known Ukrainian physicians who have been elected to the main positions. The council is represented by Professor B. M. Datsenko as President, and Professors E.J. Fistal, G. P. Kozynets and T. Tamm as vice presidents.
During the process of establishment, several con-sultations took place with EWMA Council and EWMA Secretariat. The close co-operation with EWMA is due to the fact that EWMA supports local initiatives of establishment of national wound management societies in countries across Eastern Europe.
To date Ukrainian delegates have visited the annual EWMA conference in Geneva and have also participated in national meetings in Lithuania and Belarus. The exchange of experiences with neighbouring countries regarding the establish-ment of their own associations greatly helped the Ukrainian founders during the organising process
for UWTO. More information about UWTO can be found on their web-site www.uwto.org.ua.
The conference “Wounds, Wound Infections and Wound Closure” was organised in the Academy for Postgraduate Studies of Ukraine. The proce-dure of registration was finalised in the late autumn after a long arrangement process.
The conference program included three thematic sessions: Wound Care and Debridement, Surgical Wound Reconstruction, and Modern Trends in Management of Wound and Wound Infections. EWMA was represented by the Council Member Rytis Rimdeika, who had the privilege of opening the conference with an introductory presentation on EWMA.
The conference attracted more than 200 partici-pants from various regions of the Ukraine, and neighbouring Belarus and Russia. Participants from numerous regions of the Ukraine presented papers and case reports from their clinical practic-es. In addition, round table discussions on diabetic foot issues were held by prominent lecturers from the Ukraine. The conference also featured sepa-rate poster sessions which were held in the exhibi-tion area.
During the conference there were exhibitions of wound dressings, wound care equipment, medical devices and pharmaceutical products. Representa-tives of well-known international medical compa-nies as well as local manufacturers participated actively in the exhibition and also organised con-current sessions and workshops. The conference was followed by a welcome party for all partici-pants. m
Organisations
Wound Treatment Organisation established in Ukraine
Chairing persons at the opening ceremony, from the left UWTO President Prof. B. M. Datsenko, chairman of the organizing committee Prof. G. P. Kozynets, and EWMA representative Prof. R. Rimdeika
The Exhibition
EWMA Journal 2011 vol 11 no 2 72

· EWMA MASTER COURSE·EU
RO
PEAN· WOUND ·MANAGEMENT· A
SSO
CIA
TIO
N
EWMA MASTER COURSE
www.ewma.org/woundcourse
IS OEDEMA A CHALLENGE IN WOUND HEALING?
13-14 October 2011 · Budapest, Hungary
Advanced theoretical and practical sessions related to oedema and wound healing.
Through a mixture of lectures, workshops and interactive sessions the course will bridge theory and practice, addressing a broad range of topics including: n Oedema as a problem in different types of wounds and
what impact it hasn The pathophysiology of oedeman Psycho-social impact of oedeman Methods for diagnosing different types of oedeman Prevention and managementn Development of evidence based outcome measurement
of oedema in wound healingn Infectionn Associated skin complications Credits for Continuing Medical Education (CME) will be awarded by the European Union of Medical Specialists.
For more information about the programme, registration etc. please visit

AFIScep.beFrancophone Nurses’ Association in Stoma Therapy, Wound Healing and Woundswww.afiscep.be
AISLeC Italian Nurses’ Association for the Study of Cutaneous Woundswww.aislec.it
AIUCItalian Association for the study of Cutaneous Ulcerswww.aiuc.it
APTFeridasPortuguese Association for the Treatment of Woundswww.aptferidas.com
AWAAustrian Wound Associationwww.a-w-a.at
BEFEWOBelgian Federation of Woundcarewww.befewo.org
BWABulgarian Wound Associationwww.woundbulgaria.org
CNCClinical Nursing Consulting – Wondzorgwww.wondzorg.be
CSLRCzech Wound Management Societywww.cslr.cz
CWACroatian Wound Associationwww.huzr.hr
DGfWGerman Wound Healing Societywww.dgfw.de
Danish WoundHealing Society
DSFSDanish Wound Healing Societywww.saar.dk
FWCSFinnish Wound Care Societywww.suomenhaavanhoitoyhdistys.fi
GAIF Associated Group of Research in Woundswww.gaif.net
Cooperating Organisations
GNEAUPPNational Advisory Group for the Study of Pressure Ulcers and Chronic Woundswww.gneaupp.org
ICWChronic Wounds Initiativewww.ic-wunden.de
LBAALatvian Wound Treating Organisation
LUFThe Leg Ulcer Forumwww.legulcerforum.org
LWMALithuanian Wound Management Associationwww.lzga.lt
MASCMaltese Association of Skin and Wound Carewww.mwcf.madv.org.mt/
MSKTHungarian Wound Care Societywww.euuzlet.hu/mskt/
MWMAMacedonian Wound Management Association
NATVNSNational Association of Tissue Viability Nurses, Scotland
NIFSNorwegian Wound Healing Associationwww.nifs-saar.no
NOVWDutch Organisation of Wound Care Nurseswww.novw.org
PWMAPolish Wound Management Associationwww.ptlr.pl
ROWMARomanian Wound Management Associationwww.artmp.ro
EWMA Journal 2011 vol 11 no 2 74

SAfWSwiss Association for Wound Care(German section)www.safw.ch
SAfWSwiss Association for Wound Care(French section)www.safw-romande.ch
SAWMASerbian Advanced Wound Management Associationwww.serbiawound.org
SEBINKOHungarian Association for the Improvement in Care of Chronic Wounds and Incontinentiawww.sebinko.hu
SFFPCThe French and Francophone Society of Wounds and Wound Healingwww.sffpc.org
SSiSSwedish Wound Care Nurses Associationwww.sarsjukskoterskor.se
SSOORSlovak Wound Care Associationwww.ssoor.sk
SUMSIcelandic Wound Healing Societywww.sums-is.org
SWHS Serbian Wound Healing Societywww.lecenjerana.com
SWHSSwedish Wound Healing Societywww.sarlakning.se
TVSTissue Viability Societywww.tvs.org.uk
URuBiHAssociation for Wound Management of Bosnia and Herzegovinawww.urubih.ba
V&VNDecubitus and Wound Consultants, Netherlandswww.venvn.nl
WMAKWound Management Association of Kosova
WMAOIWound Management Association of Irelandwww.wmaoi.ie
WMASWound Management Association Slovenia www.dors.si
WMATWound Management Association Turkeywww.yaradernegi.net
WMS (Belarus)Wound Management Society
For more information about EWMA’s Cooperating Organisations
please visit www.ewma.org
Associated Organisations
Leg ClubLindsay Leg Club Foundationwww.legclub.org
LSNThe Lymphoedema Support Networkwww.lymphoedema.org/lsn
International Partner Organisations
AWMA Australian Wound Management Associationwww.awma.com.au
Debra Internationalwww.debra-international.org
NZWCSNew Zealand Wound Care Societywww.nzwcs.org.nz
AAWCAssociation for the Advancement of Wound Carewww.aawconline.org
ILFInternational Lymphoedema Frameworkwww.lympho.org
SOBENFeEBrazilian Wound Management Association www.sobenfee.org.br
Organisations
EWMA Journal 2011 vol 11 no 2 75

Science, Practice and Education
Organisations
EWMA
5 EditorialCarol Dealey
7 The fight against biofilm infections: Do we have the knowledge and means?Klaus Kirketerp-Møller, Thomas Bjarnsholt, Trine Rolighed Thomsen
10 Biofilms in wounds: An unsolved problem?António Pedro Fonseca
25 Diabetic foot ulcer pain: The hidden burdenSarah E Bradbury, Patricia E Price
38 Topical negative pressure in the treatment of deep sternal infection following cardiac surgery: Five year results of first-line application protocolMartin Šimek
43 Wounds Research for Patient Benefit: A five year programme of research in wound careKaren Lamb, Nikki Stubbs, Jo Dumville, Nicky Cullum
48 EWMA Journal Previous Issues and Other Journals
50 Introducing the Belgian Federation of WoundcareBrigitte Crispin, Luc Gryson
52 EWMA Patient Outcome GroupPatricia Price
55 1st EWMA Health Economics Course organised by the EWMA Patient Outcome GroupFinn Gottrup
56 Advanced Wound Care Sector (AWCS) Status ReportHans Lundgren
60 EWMA Wound Surveys – Resource consumption for wound careFinn Gottrup
62 National collaboration for the Leg Ulcer & Compression Seminars 2011Hugo Partsch, Finn Gottrup
64 EWMA Corporate Sponsors Contact Data
66 Conference Calendar
69 Conference Report: EWMA Session, 20th Annual European Tissue Repair Society CongressGerrolt N. Jukema
70 FWCS: The 14th national wound healing congress in Helsinki, FinlandAnna Hjerppe
72 Wound Treatment Organisation established in UkraineRytis Rimdeika
74 EWMA Cooperating Organisations
75 International Partner Organisations
75 Associated Organisations
Scientific Communication