Evolving role of diet in the pathogenesis and...
13
1726 Levine A, et al. Gut 2018;67:1726–1738. doi:10.1136/gutjnl-2017-315866 Recent advances in clinical practice Evolving role of diet in the pathogenesis and treatment of inflammatory bowel diseases Arie Levine, 1,2 Rotem Sigall Boneh, 1,2 Eytan Wine 3 ABSTRACT Recent advances in basic and clinical science over the last 3 years have dramatically altered our appreciation of the role of diet in inflammatory bowel diseases (IBD). The marked increase in incidence of these diseases along with the important role of non-genetic susceptibility among patients with IBD has highlighted that these diseases have a strong environmental component. Progress in the field of microbiome and IBD has demonstrated that microbiome appears to play an important role in pathogenesis, and that diet may in turn impact the composition and functionality of the microbiome. Uncontrolled clinical studies have demonstrated that various dietary therapies such as exclusive enteral nutrition and newly developed exclusion diets might be potent tools for induction of remission at disease onset, for patients failing biologic therapy, as a treatment for disease complications and in reducing the need for surgery. We review these advances from bench to bedside, along with the need for better clinical trials to support these interventions. INTRODUCTION The basic understanding of how and why IBD develop has been the focus of research of many disciplines over the last few decades, especially given the complex, multifactorial nature of these conditions. The discovery of NOD2 as the first, and most important, susceptibility gene 1 2 was then followed by identification of over 200 other loci, 3 4 but these genetic contributions together likely only explain 19%–26% of the hereditary variance of IBD. 5 Genetic studies have identified defects in innate immunity in Crohn disease (CD) and altered barrier function in Ulcerative Colitis (UC) as some of the key players in disease susceptibility. 6 7 The intestinal barrier comprises the mucous layer, epithelial cells and the tight junctions between cells, rendering the mucosa relatively imperme- able to bacteria. Some of the early changes in the sequence of events, leading to IBD are seen in the epithelial and mucus layers, 8–10 which is particu- larly evident in patients with UC. 11 12 The mucous layer is a critical barrier separating commensal and pathogenic bacteria from the epithelium, thereby decreasing immune activation. Both CD and UC are characterised by high penetration of the mucous layer by bacteria and increased barrier permea- bility. 11 13 Increased barrier dysfunction during remission has been associated with clinical relapse of the disease. 14 15 CD and UC are characterised by the presence of mucosal bacteria 16 that differs from healthy human hosts, in which bacteria for the most part do not reside adjacent to the mucosal epithelium (figure 1A, B). 13 In fact, increased epithelial cell shedding, high vascular flow, depletion of the small bowel mucus layer and presence of mucosa-associated bacteria have been demonstrated in non-inflamed duodenum and ileum of children with UC. 17–19 Both CD and UC appear to involve translocation of bacteria through the epithelium. 20 Thus, impaired barrier function, defects in innate immunity, changes in microbial composition and the presence of mucosa-associated and translocating bacteria have all been described in IBD. However, differences do exist between CD (figure 1A) and UC (figure 1B). Dysbiosis is more prominent in CD. 21 The predominance of Proteobacteria, specifically indi- vidual Escherichia coli strains, especially in CD, has been known for many years 22 23 ; however, whether or not this reflects a true role in driving disease To cite: Levine A, Sigall Boneh R, Wine E. Gut 2018;67:1726–1738. 1 Pediatric Gastroenterology and Nutrition Unit, Edith Wolfson Medical Center, Holon, Israel 2 Tel Aviv University, Tel Aviv, Israel 3 Department of Pediatrics, University of Alberta, Edmonton, Alberta, Canada Correspondence to Professor Arie Levine, Paediatric Gastroenterology and Nutrition Unit, Wolfson Medical Center, Holon 58100 Israel; arie.levine. [email protected] Received 2 January 2018 Revised 16 April 2018 Accepted 17 April 2018 Published Online First 18 May 2018 Significance of this study What is already known? ► Diet has been implicated in the pathogenesis of Crohn disease (CD) and Ulcerative Colitis (UC). Dietary factors may have a plausible role in altering the microbiota, metabolome, host barrier function and innate immunity. What is new? ► Exclusive enteral nutrition has demonstrated efficacy for induction of remission, as well as treatment of complications such as inflammatory strictures, intrabdominal abscess and enterocutaneous fistulae in Crohn disease. Use or preoperative exclusive enteral nutrition for ≥4 weeks may reduce the need for surgical resections. ► Preliminary reports from uncontrolled studies suggest that specific exclusion diets based on partial enteral nutrition and specific whole foods may induce remission and can be used as a salvage therapy after loss of response to biologics or combination therapy. How might it impact on clinical practice? ► Dietary interventions ranging from dietary education of patients to exclusive enteral nutrition and newer elimination diets may have the potential to better control disease or avoid complications, pending better clinical trials. There are insufficient data at the present time to suggest that dietary therapy may be useful in UC; this is an important research gap. on 4 March 2019 by guest. Protected by copyright. http://gut.bmj.com/ Gut: first published as 10.1136/gutjnl-2017-315866 on 18 May 2018. Downloaded from
Transcript of Evolving role of diet in the pathogenesis and...

1726 Levine A, et al. Gut 2018;67:1726–1738. doi:10.1136/gutjnl-2017-315866
Recent advances in clinical practice
Evolving role of diet in the pathogenesis and treatment of inflammatory bowel diseasesArie Levine,1,2 Rotem Sigall Boneh,1,2 Eytan Wine3
AbstRActRecent advances in basic and clinical science over the last 3 years have dramatically altered our appreciation of the role of diet in inflammatory bowel diseases (IBD). The marked increase in incidence of these diseases along with the important role of non-genetic susceptibility among patients with IBD has highlighted that these diseases have a strong environmental component. Progress in the field of microbiome and IBD has demonstrated that microbiome appears to play an important role in pathogenesis, and that diet may in turn impact the composition and functionality of the microbiome. Uncontrolled clinical studies have demonstrated that various dietary therapies such as exclusive enteral nutrition and newly developed exclusion diets might be potent tools for induction of remission at disease onset, for patients failing biologic therapy, as a treatment for disease complications and in reducing the need for surgery. We review these advances from bench to bedside, along with the need for better clinical trials to support these interventions.
IntRoductIonThe basic understanding of how and why IBD develop has been the focus of research of many disciplines over the last few decades, especially given the complex, multifactorial nature of these conditions. The discovery of NOD2 as the first, and most important, susceptibility gene1 2 was then followed by identification of over 200 other loci,3 4 but these genetic contributions together likely only explain 19%–26% of the hereditary variance of IBD.5 Genetic studies have identified defects in innate immunity in Crohn disease (CD) and altered barrier function in Ulcerative Colitis (UC) as some of the key players in disease susceptibility.6 7
The intestinal barrier comprises the mucous layer, epithelial cells and the tight junctions between cells, rendering the mucosa relatively imperme-able to bacteria. Some of the early changes in the sequence of events, leading to IBD are seen in the epithelial and mucus layers,8–10 which is particu-larly evident in patients with UC.11 12 The mucous layer is a critical barrier separating commensal and pathogenic bacteria from the epithelium, thereby decreasing immune activation. Both CD and UC are characterised by high penetration of the mucous layer by bacteria and increased barrier permea-bility.11 13 Increased barrier dysfunction during remission has been associated with clinical relapse of the disease.14 15
CD and UC are characterised by the presence of mucosal bacteria16 that differs from healthy human
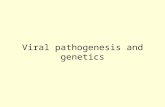
hosts, in which bacteria for the most part do not reside adjacent to the mucosal epithelium (figure 1A, B).13 In fact, increased epithelial cell shedding, high vascular flow, depletion of the small bowel mucus layer and presence of mucosa-associated bacteria have been demonstrated in non-inflamed duodenum and ileum of children with UC.17–19 Both CD and UC appear to involve translocation of bacteria through the epithelium.20 Thus, impaired barrier function, defects in innate immunity, changes in microbial composition and the presence of mucosa-associated and translocating bacteria have all been described in IBD. However, differences do exist between CD (figure 1A) and UC (figure 1B).
Dysbiosis is more prominent in CD.21 The predominance of Proteobacteria, specifically indi-vidual Escherichia coli strains, especially in CD, has been known for many years22 23; however, whether or not this reflects a true role in driving disease
to cite: Levine A, Sigall Boneh R, Wine E. Gut 2018;67:1726–1738.
1Pediatric Gastroenterology and Nutrition Unit, Edith Wolfson Medical Center, Holon, Israel2Tel Aviv University, Tel Aviv, Israel3Department of Pediatrics, University of Alberta, Edmonton, Alberta, Canada
correspondence toProfessor Arie Levine, Paediatric Gastroenterology and Nutrition Unit, Wolfson Medical Center, Holon 58100 Israel; arie. levine. dr@ gmail. com
Received 2 January 2018Revised 16 April 2018Accepted 17 April 2018Published Online First 18 May 2018
significance of this study
What is already known? ► Diet has been implicated in the pathogenesis of Crohn disease (CD) and Ulcerative Colitis (UC). Dietary factors may have a plausible role in altering the microbiota, metabolome, host barrier function and innate immunity.
What is new? ► Exclusive enteral nutrition has demonstrated efficacy for induction of remission, as well as treatment of complications such as inflammatory strictures, intrabdominal abscess and enterocutaneous fistulae in Crohn disease. Use or preoperative exclusive enteral nutrition for ≥4 weeks may reduce the need for surgical resections.
► Preliminary reports from uncontrolled studies suggest that specific exclusion diets based on partial enteral nutrition and specific whole foods may induce remission and can be used as a salvage therapy after loss of response to biologics or combination therapy.
How might it impact on clinical practice? ► Dietary interventions ranging from dietary education of patients to exclusive enteral nutrition and newer elimination diets may have the potential to better control disease or avoid complications, pending better clinical trials. There are insufficient data at the present time to suggest that dietary therapy may be useful in UC; this is an important research gap.
on 4 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2017-315866 on 18 M
ay 2018. Dow
nloaded from

1727Levine A, et al. Gut 2018;67:1726–1738. doi:10.1136/gutjnl-2017-315866
Recent advances in clinical practice
or just a change in the gut setting (eg, due to higher oxygen tension, related to inflammation) remains controversial; it is safe to say that both processes are likely and that the diversity of disease presentation and course likely represent different levels of microbial involvement in different individuals.24 The pres-ence or decline in specific mucosal genera have been identified in children and adults with IBD.21 25 26 Several researchers have demonstrated that patients with UC appear to have diminished ability to produce short chain fatty acids (SCFA), even with an abundant supply of substrates,27 28 suggesting that microbial metabolic dysfunction may play an important role in UC.
background: diet and IbdDiet is one of the key players in the normal gut microenvironment, impacting microbial composition, function, the gut barrier and host immunity. Alterations in single food groups have far ranging implications. For example, depriving colonic microbes from fibre in rodent models will favour taxa that can use alternative carbon sources found within the colonic mucus; this then leads to depletion of the mucus layer, disruption of the barrier, immune activation and tissue damage.29 Changing from a plant-based to an animal-based diet radically changes bacterial taxa and metabolism, leading to alterations in bile acids and sulfide metabolism, both of which may play a role in IBD.30 Recent data suggest that the most important
factors regulating compositional changes are access to calorie, carbohydrate and protein intake.31 Since diet has such an important role in gut homeostasis, and interacts with the microbiome, host barrier and immunity, we will explore the possible and plausible role of dietary factors in the pathogenesis of IBD.
clues from epidemiologyNumerous epidemiological studies with inconsistent methodolog-ical quality have demonstrated associations between the intake of specific dietary components or dietary patterns and the risk of developing IBD.32–39 One of the earliest epidemiological associ-ations with IBD is the strong protective role of breast feeding. Although recall bias needs to be considered, almost all studies from various regions support this dose-dependent association, which is also demonstrated for other immune-mediated conditions.40 The results from other epidemiological studies should be considered with caution due to a recall bias and possible dietary modification before the diagnosis of IBD.41 A statistical association between specific dietary factors and disease does not necessarily imply causation. In any complex disease with dietary triggers, it may be difficult to unravel the role of individual dietary risk factors since dietary patterns often involve exposures to clusters of foods. In addition, certain dietary ingredients are likely to cluster together due to industrial processing of food. For example, fat exposure
Figure 1 Western diet and pathogenesis of IBD. (A) Proposed pathogenesis of Crohn disease and effects of western diet. (B) Proposed pathogenesis of UC and effects of western diet observations that can be associated with western diet appear in the marked boxes. Tregs, regulatory T cells.
on 4 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2017-315866 on 18 M
ay 2018. Dow
nloaded from

1728 Levine A, et al. Gut 2018;67:1726–1738. doi:10.1136/gutjnl-2017-315866
Recent advances in clinical practice
will likely be associated with emulsifier exposure, processed meats with preservatives, dairy products with thickening agents and emulsifiers, etc. In addition, food frequency questionnaires may be insufficient to address longitudinal exposures.
D’Souza et al conducted a case-control study to assess the dietary patterns of Canadian children and the risk of developing CD. They evaluated multiple dietary patterns including western diet and a prudent diet. A dietary pattern characterised by meats, fatty foods and desserts (western diet) increased the risk for CD in females (OR 4.7, 95% CI 1.6 to 14.2), whereas the consumption of vegetables, fruits, olive oil, fish, grains and nuts (prudent diet) was associated with a decreased risk for developing CD in both males and females (females: OR 0.3, 95% CI 0.1 to 0.9; males: OR 0.2, 95% CI 0.1 to 0.5).33 A recent Australian population-based study of environ-mental risk factors demonstrated an increased risk for CD with frequent consumption of fast food (western diet) before diagnosis.42
Several studies have associated protein with increased risk for IBD.32 35 36 As part of the E3N prospective study, which included 67 581 French women, high animal protein was associated with a significantly increased risk of IBD (OR 3.03, 95% CI 1.45 to 6.34), particularly with UC (OR 3.29, 95% CI 1.34 to 8.04).32 Vegetable protein intake was not associated with either disease. However, other smaller studies have not confirmed this.43 In a separate study evaluating dietary intake and relapse of UC, red meat was found to have the strongest association (OR 5.19, 95% CI 2.09 to 12.9) with relapse.36
Data regarding the associations between increased intakes of carbohydrates and the risk for IBD are inconsistent. The E3N study did not identify carbohydrate intake as a risk factor for IBD, CD or UC.32 Racine et al, evaluated 366 351 participants with IBD from theEuropean Prospective Investigation into Cancer and Nutrition (EPIC) study cohort and found no correla-tion between dietary intake patterns and CD.34 They did find an association between high-sugar and low-fibre intake and UC (OR 1.68, 95% CI 1.00 to 2.82).
More recent data from the EPIC study found no associa-tion between alcohol consumption and the risk for CD.44 This contrasted with the study by Jowett et al,36 who tried to find dietary products associated with the relapse of UC. High alcohol consumption was associated with an increased risk of relapse (OR 2.71, 95% CI 1.1 to 6.67).
Dietary fats are associated with an increase or decrease risk for IBD, depending on the type of fat. Among 170 805 women followed over 26 years, a high intake of dietary long-chain n-3 polyunsaturated fatty acids was associated with a reduced risk of UC. In contrast, high intake of transunsaturated fats was associ-ated with an increased risk of UC.37
Perhaps the dietary component with the greatest agreement in epidemiological studies is dietary fibre, which is also represented in the prudent dietary patterns mentioned above. Multiple studies reported a negative association between dietary fibre intake from fruits or fruits and vegetables and subsequent risk for CD.33 37 Data from the Nurses’ Health Study among 170 776 participants showed that higher long-term intake of fruit was associated with lower risk of CD but not UC.37
Several research gaps remain in this field, including more data about exposure to industry-added ingredients, such as emulsi-fiers, preservatives and thickening agents, including maltodex-trins and carrageenans.
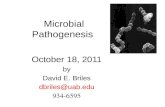
diet and altered host immunityHost factors that may play an important role in pathogenesis or active inflammation include defects in barrier function, depletion
of the intact mucous layer, decreased regulatory T cells (Tregs) and impaired bacterial clearance mechanisms (figure 1A, B). A major limitation to date is that most of the evidence comes from animal models and human cell lines, which makes extrapolation difficult. Dietary factors that may affect host immunity are presented in table 1 and figure 2. Western diet is characterised by alterations in the amount of exposure to natural dietary ingredients such as high fat (HF), high sugar (HS), high wheat and high dairy expo-sure, accompanied by low fibre exposure, and by high exposure to multiple food additives.45 46 We will focus our discussion on the dietary products with the most evidence from animal models, which include fibre, animal fat, wheat and food additives.
Low dietary fibre, identified through epidemiological studies as a possible risk factor,33 37 could affect host immunity via multiple pathways. Fibres and starches found in fruits and vege-tables are a vital substrate for the production of butyrate and other SCFAs. Butyrate plays an important role in downregulating inflammation by suppressing transcription of cytokines and increasing differentiation and the population of lamina propria Tregs.47 48 Butyrate can also enhance innate immunity by upreg-ulating defensins and cathelicidins in animal models.47 48 Low dietary fibre may cause catabolism of the mucous layer, leading to increased permeability of the mucous layer, and allowing increased contact between luminal bacteria and the epithelium.29
HF or HF/HS diets may act synergistically to a low fibre diet as they may exert many of the same effects described above for low fibre exposure. An HF/HS diet in a CEACAM 10 rodent model has been shown to decrease MUC2 expression and goblet cell mucous while increasing intestinal permeability.49 These diets have been demonstrated to decrease both butyrate produc-tion and expression of the butyrate GPR43 receptor, which is underexpressed in CD.49 Finally, HF diets (without HS) have been shown to increase tumour necrosis factor (TNF)-α and interferon-γ expression and decrease levels of colonic Tregs.50
Exposure to gluten may promote an inflammatory state, impair innate immunity or increase intestinal permeability. Dietary gluten significantly decreased intestinal Tregs in non-obese diabetic mice fed gluten compared with standard chow.51 Dietary gluten was also shown to induce ileitis in TNFΔARE/WT mice via an increase in intestinal permeability,52 which has been iden-tified as a factor associated with relapse in CD.14
Alpha-amylase/trypsin inhibitors, found in wheat, may have a pro-inflammatory role. They are activators of human dendritic cells and macrophages, driving intestinal inflammation in rodents.53 54
Multiple food additives, commonly present in western diet, may affect host barrier function or immunity. Chassaing et al, demonstrated that IL-10−/− mice exposed to two common emul-sifiers, carboxymethylcellulose and polysorbate-80, developed increased intestinal permeability and significant thinning of the mucous layer, leading to increased proximity of the microbiota to the intestinal epithelium.55 Maltodextrins, used as thickeners and sweeteners, have demonstrated the ability to affect mucosal proximity (by a presumed effect on mucous layer thickness) and to impair clearance of intracellular Salmonella.56 57 Carra-geenans, used for texture and as thickening agents in the dairy and sauce industry, may induce intestinal permeability.58 59 Other factors, which may promote intestinal permeability are listed in table 1 and are beyond the scope of this paper.
diet and microbiotaDietary components linked to changes in the microbiome that have been associated with IBD appear in table 2 and figure 3. For example, adherent invasive E. coli (AIEC) strains cannot induce inflammation under normal conditions. Pathogenicity may arise
on 4 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2017-315866 on 18 M
ay 2018. Dow
nloaded from

1729Levine A, et al. Gut 2018;67:1726–1738. doi:10.1136/gutjnl-2017-315866
Recent advances in clinical practice
table 1 Dietary factors potentially affecting host barrier and immunity
dietary component Reference Model Effect
Natural components
High fat+high sugar diet Martinez-Medina. Gut, 201449
CEABAC 10 mice ► Decreased MUC2 expression ► Depleted Goblet cells ► Increased intestinal permeability ► Increased TNF-α secretion
High fat+high sugar diet Agus. Sci Rep, 201660 CEABAC 10 mice ► Decreased FoxP3 Tregs in mesenteric lymph nodes ► Decreased butyrate production ► Reducedexpression of the butyrate GPR43 receptor ► Dysbiosis ► Significantly decreased SCFA concentrations
High fat diet Ma. Clin Exp Immunol, 200850
WT C57BL/6 mice ► Higher numbers of non-CD1d-restricted natural killer T cells in the colonic IEL
► Increased TNF-α and IFN-γ expression ► Decreased levels of colonic Tregs
High fat diet Suzuki. Nutri & Metab, 2010101
LETO andOLETF rats (mutant obese Long-Evans)Human intestinal Caco-2 cells
► Increased intestinal permeability ► Decreased tight junction proteins expression (claudin-1, claudin-3, occludin
and junctional adhesion molecule-1)
High fat diet Gruber. PLoS One, 2013102 TNFΔARE/WT mouse and WT C57BL/6 ► Aggravation of ileal inflammation ► Reduced expression of occludin ► Increasedtranslocation of endotoxin ► Increased pro-inflammatory markers ► Recruitment of dendritic cells and Th17-biased lymphocyte into the lamina
propria
Sodium caprate (constituent of milk fat)
Söderholm. Dig Dis Sci, 1998103
Rat ileum ► Increased tight junction permeability
Söderholm. Gut, 2002104 Specimens from the distal ileum of patients with CD
► Rapid increased in paracellular permeability
Gluten Ejsing-Duun. Scand J Immunol, 200851
NOD and BALB/c mice ► Decreased the occurrence of Tregs by 10%–15% (p<0.05)
Gluten Wagner. Inflamm Bowel Dis, 201352
TNFΔARE/WT mouse ► Increased intestinal permeability ► Reduced occludin expression ► Induced chronic ileitis
Gluten (gliadin) Lammers. Gastroenterology, 2008105
Human intestinal epithelial cell, Caco2 cellsIEC6 cells
► Zonulin released, causedtight junction disassembly
Gluten (gliadin) Hollon. Nutrients, 2015106 Ex vivo human duodenal biopsies ► Increased intestinal permeability ► Higher concentration of IL-10 in controls compared with coeliac disease in
remission or gluten sensitivity
Wheat (ATIs) Junkers. J Exp Med, 201254
Human cells and biopsies ► ATIs are potent activators of human innate immune responses in monocytes, macrophages and dendritic cells
Wheat (ATIs) Zevallos. Gastroenterology, 201753
TLR4-responsive mouse and human cell lines
► Activation of dendritic cells in mesenteric lymph nodes ► Released inflammatory mediators
Soluble fibres and resistant starch
Bassaganya-Riera. J Nutr, 2011107
C57BL/6J WT miceIL-10−/− mice
► Decreased ileal and colonic inflammatory lesions ► Decreased IFN-γ production by effector CD4+ T cells from Peyer’s patches ► Resistant starch increased the IL-10-expressing cells ► Suppressed gut inflammation
Dietary pectin Ye. J Agric Food Chem, 2010108
IL-10−/− mice ► Reduced expression of TNF-R and GATA-3 ► Lower levels of IgE, IgG and IgM expression ► Modulation of production of pro-inflammatory cytokines and
immunoglobulins
Fermentable fibre (guar gum, partially hydrolysed GG)
Hung. J Nutr, 2016109 BALB/c mice aged 7 weeks ► Increased expression of occludin and claudin-3, claudin-4 and claudin-7 (reduced permeability)
► Greater total faecal SCFA concentrations ► Reduced inflammation score
Multifibre mix diet Wang. JCC, 201647 IL-10−/− mice ► Reduced disease activity index score ► Decreased CD4+CD45+ lymphocytes, IFN-γ/IL-17A, TNF-α/TNF-R2 mRNA
expression ► Increased Tregs and SCFA production ► Increased epithelial expression and correct localisation of tight junction
proteins
Alcohol Forsyth. Alcohol Clin Exp Res, 2017110
Mice ► Colonic (but not small intestinal) hyperpermeability ► Decreased butyrate/total SCFA ratio in stool
Dietary salt Tubbs. J Immunol, 2017111 IL-10−/− murine model of colitis ► Exacerbation of inflammatory pathology ► Enhanced expression of numerous pro-inflammatory cytokines ► TLR4 activation
Continued
on 4 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2017-315866 on 18 M
ay 2018. Dow
nloaded from

1730 Levine A, et al. Gut 2018;67:1726–1738. doi:10.1136/gutjnl-2017-315866
Recent advances in clinical practice
if the ligand CEACAM 6 is presented by intestinal epithelial and M cells. Under these conditions, AIEC may form small intestinal biofilms, adhere and translocate via M cells, and then invade the associated epithelium. An HF/HS diet may promote colonisation with IBD-associated pathobionts. CEABAC 10 mice, expressing CEACAM 6, fed HF/HS but not standard chow were rapidly colonised by mucosa-associated AIEC and presented higher degrees of crypt abscesses when compared with the standard chow group.49 Transplantation of faeces from HF/HS-treated mice to germ free mice increased susceptibility to AIEC.60 A study that compared HF with HS diet in a mouse model demon-strated that HF but not HS induced dysbiosis, characterised
by an increase in Proteobacteria and a decrease in Firmicutes, similar to that seen in CD.61 HF diets result in accumulation of secondary bile acids, such as deoxycholic acid, which in turn can inhibit the growth of members of the Bacteroidetes and Firmic-utes phyla, characteristic of the dysbiosis found in CD.62
Maltodextrins have been shown to promote AIEC biofilm formation independent of the presence of the ligand CEACAM 6, while AIEC growth in medium was enhanced particularly with polysaccharides used as thickening agents, such as maltodextrin and xanthan gum, but not by glucose or sucrose.63
The source of dietary fat may play an important role in promoting colitogenic bacteria. Devkota et al reported an
dietary component Reference Model Effect
Food additives
Carboxymethylcellulose (E466) and polysorbate-80 (E433)
Chassaing. Nature, 201555
IL-10−/− mice ► Increased intestinal permeability ► Mucous layer depletion led to increased proximity of the microbiota to the
intestinal epithelium
Carboxymethylcellulose (E466)
Swidsinski. Inflamm Bowel Dis, 2009112
IL-10−/− mice ► Distension of spaces between villi, with bacteria filling these spaces
Maltodextrin Miyazato. Biosci Microbiota Food Health, 2016113
BALB/c mice ► Increasedtotal IgA levels in the intestinal tract
Carrageenan (E407) Choi. Toxicol Lett, 201259 HCT-8, HT-29 and Caco-2 cells ► Lowered transepithelial resistance ► Discontinuous and irregular ZO-1 expression
Fahoum. Mol Nutr Food Res, 201758
Caco-2 cell model ► Redistribution of the tight-junction protein ZO-1 ► Increased intestinal permeability
Titanium dioxide (TiO2) Ruiz. Gut, 2017114 WT and NLRP3−/− mice with DSS ► Oral administration of TiO2 worsened acute colitis through a mechanism involving the NLRP3 inflammasome
► Induced reactive oxygen species generation ► Increased epithelial permeability in IEC monolayers
ATI, α-a mylase/trypsin inhibitors; CD, Crohn disease; IFN, interferon; IL, interleukin; SCFA, short chain fatty acids; Th, T helper; TNF, tumour necrosis factor; Tregs, T regulatory cells; WT, wild-type; ZO, zonula occludens. IEL (intrepithelial lymphocyes), DSS (dextran sulfate sodium).
table 1 Continued
Figure 2 Possible effects of dietary factors on host barrier and immunity leading to IBD (based on cell lines and animal models). Tregs, regulatory T cells.
on 4 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2017-315866 on 18 M
ay 2018. Dow
nloaded from

1731Levine A, et al. Gut 2018;67:1726–1738. doi:10.1136/gutjnl-2017-315866
Recent advances in clinical practice
increase in colitis severity after exposure to milk fat diet but not to isocaloric polyunsaturated fatty acid diet or a low fat diet in IL-10−/− mice.64 Colitis was associated with the bloom of coli-togenic Bilophila wadsworthia in the milk fat group, which was dependent on milk fat, and induced taurine conjugated bile acids.
Interestingly, emulsifiers may affect the microbiome as well as the host. The emulsifier polysorbate-80 was associated with increased translocation of AIEC through M cells and the follicular associated epithelium; this effect was suppressed by certain dietary fibres.65 Emulsifiers appear to affect compositional changes associated with inflammation. Polysorbate-80 induced inflammation and flagellin expression via alteration of microbial dysbiosis, whereas the emul-sifier carboxymethylcellulose rapidly induced flagellin and alter-ations in gene expression for flagellin in a model for gut dysbiosis.66 Exclusion of western diet by exclusive enteral nutrition (EEN) or an exclusion diet in children with CD were shown to cause a marked reduction in Proteobacteria and in taxa associated previously with CD including Escherichia, Haemophilus, Veillonella and Fusobac-teria (Van Limbergen and Dunn, unpublished data).
The metabolic activity of the microbiota may be as important, or even more important than compositional changes, especially in UC. Both CD and UC are characterised by a decrease in SCFA-pro-ducing genera, which are stimulated by the presence of dietary fibre. However, UC seems to be characterised by deficient production of SCFA, even when substrates such as resistant starch are provided.27 28 Sulfide-reducing bacteria and increased sulfide production have been reported in UC.27 Animal protein-based diets favour production of sulfide reductases and sulfide-reducing bacteria.30
In summary, high animal or dairy fat, animal protein, wheat, emulsifiers and thickeners appear to top the list of candidate foods associated with intestinal inflammation in animal models.
diet as a therapeutic interventionRecent studies have expanded our understanding of the possible roles for dietary therapy, primarily in CD. Dietary therapies, such as EEN, were traditionally and primarily used to induce remis-sion in early or new-onset CD67 or as supportive therapy in chil-dren and adults with malnutrition or in the preoperative setting.
table 2 Dietary factors potentially affecting the microbiota in IBD
dietary component Reference Model Effect
Natural components
High fat+high sugar diet Martinez-Medina. Gut, 201449 CEABAC 10 mice ► AIEC Colonisation ► Low diversity ► Dysbiosis ► Higher degree of crypt abscesses
High fat+high sugar diet Agus. Sci Rep, 201660 CEABAC 10 mice ► Intestinal mucosa dysbiosis ► Decreased butyrate production ► Reduced expression of the butyrate GPR43 receptor ► Overgrowth of Escherichia coli ► Significantly decreased SCFA concentrations
High fat vs high sugar Lai. Environ Pollut, 201661 CD1 mice ► High fat but not high sugar induced dysbiosis characterised by an increase in Proteobacteria and a decrease in Firmicutes and Clostridia
► Growth induction of the family Helicobacteraceae
Milk fat (saturated fat) Devkota. Nature, 201264 IL-10−/− mice ► Promoted expansion of sulfite-reducing pathobiont, Bilophila wadsworthia
► Induced pro-inflammatory Th1 immune response ► Increased incidence of colitis ► Low diversity ► Dysbiosis
High fibre diet Silveira. Eur J Nutr, 2017115 BALB/c female mice ► High fibre diet protected from acute colitis
Fibre James. GUT, 201528 Patients with UC and controls
► High fibre diet did not increased SCFA production in patients with UC
Animal vs plant diet David. Nature, 201430 Healthy volunteers ► Animal-based diet increased the abundance of bile-tolerant microorganisms and decreased the levels of Firmicutes
Alcohol Forsyth. Alcohol Clin Exp Res, 2017110
Mice ► Decreased butyrate/total SCFA ratio in stool
Food additives
Carboxymethylcellulose (E466) and polysorbate-80 (E433)
Chassaing. Nature, 201555 IL-10–/– miceHuman intestinal microbial ecosystem (M-SHIME)
► Increased mucosal-associated bacteria ► Increased Flagellin expression ► P-80 altered species composition
Chassaing. GUT, 201766
Carboxymethylcellulose (E466)
Swidsinski. Inflamm Bowel Dis, 2009112
IL-10–/– mice ► Bacterial overgrowth ► Distension of spaces between villi, with bacteria filling these spaces ► Adherence of bacteria to the mucosa ► Migration of bacteria to the bottom of the crypts of Lieberkühn
Polysorbate-80 (E433)
Roberts. Gut, 201065 M cellsCaco-2 cellsHuman Peyer’s patches
► Increasedtranslocation of E. coli across M cells
Plantain and broccoli fibre ► Reduction in translocation of E. coli across M cells
Maltodextrin Nickerson. PLoS One, 201263 Human intestinal epithelial cell monolayers
► Biofilm formation AIEC ► Enhanced E. coli adhesion independent of the cellular receptor CEACAM 6Nickerson. Gut Microbes, 201556
Carrageenan (E407) Munyaka. Front Microbiol, 2016116
Piglet model of IBD ► Decreased bacterial species richness ► Shifted community composition. ► Bacterial dysbiosis
AIEC, adherent invasive E. coli ; SCFA, short chain fatty acids; Th, T helper.
on 4 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2017-315866 on 18 M
ay 2018. Dow
nloaded from

1732 Levine A, et al. Gut 2018;67:1726–1738. doi:10.1136/gutjnl-2017-315866
Recent advances in clinical practice
EEN involves the exclusive use of a liquid nutrition in the form of medical formulas, without exposure to other foods, usually for 6–8 weeks (table 3). This effect does not depend on the protein source (type of formula), but is very dependent on exclusion of ordinary table food.68 69 Newer open-label studies have demon-strated that existing and new dietary strategies may have a wider role and can be employed to maintain remission, induce remission in patients failing biologics and for patients with complicated disease (figure 4). As data from randomised controlled trials (RCTs) are absent or pending, we will confine ourselves to more recent studies that have expanded our understanding beyond the use of EEN at diagnosis for induction of remission, which is reviewed elsewhere.67
Induction of remissionSeveral recent paediatric studies have demonstrated and confirmed that EEN may induce remission in 60%–86% of children accom-panied by a significant decrease in inflammatory markers such as erythrocyte sedimentation rate (ESR), C reactive protein (CRP) and faecal calprotectin.69–73 This recent body of literature has evaluated long-term benefits associated with use of EEN in mild-to-moderate paediatric CD. In comparison to use of steroids and corrected for disease severity, EEN was associated with higher remission rates, better growth and longer steroid-free periods,71 72 but did not differ with regard to other outcomes such as relapse. Cohen-Dolev et al demonstrated that EEN was superior to corticosteroids for induction of remission and linear growth in a multicentre prospective inception cohort of mild-to-moderate CD at diagnosis. EEN was not superior with respect to other outcomes such as time to relapse or complications over 2 years.72 Grover et al performed a prospective trial to assess mucosal healing by performing colonoscopy before and after 8 weeks of EEN with azathioprine. At the end of 8 weeks, complete mucosal healing was observed in 33%, near complete in another 19% of patients.73 Patients who achieved complete mucosal healing had better sustained remission over 3 years of follow-up.
Use of EEN poses challenges to physicians and patients alike, as patients have to deal with monotony of food and taste fatigue. Furthermore, up to 50% of patients may require nasogastric tubes and many might refuse to start therapy due to these issues.74 75 This limits access and availability of the therapy. Therefore, it is no surprise that the last 3 years have seen several attempts to achieve the effect of EEN while allowing access to whole foods. Investigators from three centres in the USA and Canada compared outcomes from three cohorts treated with either: 1) high volume partial enteral nutrition (PEN) using a mean of 77% of estimated energy requirements from PEN with free access to food; 2) EEN and 3) infliximab. Clinical remission rates were similar between infliximab and EEN (73%–76%) and lower (50%) in the PEN group. Faecal calprotectin <250 g/dL as an inflammatory end point was found only in 14% of patients treated with PEN and ad libitum diet, compared with 45% with EEN and 62% treated with infliximab at week 8. This suggests that high-volume PEN with access to free diet is ineffective at improving inflammation compared with EEN or infliximab, reaffirming the principle of exclusivity.67 68
Other research groups have employed a different strategy based on the combination of PEN with a specific exclusion diet that allows access to whole foods. This review will be confined only to studies that evaluated clinical remission and objective markers of inflammation or mucosa healing. The Crohn’s disease exclusion diet was developed based on the principles outlined in figures 1–3, by excluding foods that have been associated with altered host barrier or bacterial clearance, dysbiosis and virulence factors that may allow bacteria to become mucosa-associated and enable translocation, based on the bacterial penetration cycle hypothesis for CD first proposed by the authors.76 The premise behind this theory is that CD is caused by mucosal and translocating bacteria. This diet was evaluated initially in 47 children and adults with mild-to-moderate disease. Clinical remission was achieved in
Figure 3 Possible effects of dietary factors on microbiota leading to IBD (based on cell lines and animal models).
on 4 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2017-315866 on 18 M
ay 2018. Dow
nloaded from

1733Levine A, et al. Gut 2018;67:1726–1738. doi:10.1136/gutjnl-2017-315866
Recent advances in clinical practice
table 3 Key studies and recent advances with EEN in children and adults
study design Populationduration of EEn comparator number of patients outcome Key findings Reference
Randomised controlled trial
Adults 3–6 Weeks EEN vs CS and sulfasalazine
EEN: 51 ptsDrugs: 44 pts
Improvement in CDAI:EEN: 41%Drugs: 72%p<0.05
Equal effectiveness of EEN compared with drugs per protocol
Malchow. Scand J Gastroenterol, 1990117
Randomised ccontrolled trial
Adults 4–6 Weeks EEN vs CS and sulfasalazine
EEN: 52 ptsDrugs: 55 pts
Remission:EEN: 55%Drugs: 74%p<0.01
Comparison to medications
Lochs. Gastroenterology, 1991118
Randomised ccontrolled trial
Adults 4 Weeks EEN: n-6 PUFA vs MUFA vs CS with ward diet
MUFA: 20 ptsPUFA: 23 ptsCS: 19 pts
Remission rates (ITT):MUFA EEN: 20%PUFA EEN: 52%CS: 79%p=0.001
Composition of fat Gassull. Gut, 2002119
Randomised ccontrolled trial
Paediatric CD 6 Weeks Elemental formula vs polymeric formula
Elemental fomula: 16 ptsPolymeric formula: 17 pts
Remission:Elemental: 69%Polymeric: 82%p=0.44
Polymeric equivalent to elemental
Ludvigsson. Acta Paediatr, 2004120
Randomised ccontrolled trial
Paediatric CD 6 Weeks EEN vs 50% PEN with free diet
EEN:24 ptsPEN: 26 pts
Remission:PEN: 15%EEN: 42%p=0.035
Principle of exclusivity Johnson. GUT, 200668
Randomised ccontrolled trial
Newly diagnosed paediatric CD
10 Weeks Polymeric formula vs CS
EEN: 19 ptsCS: 18 pts
Remission:polymeric EEN: 79%CS: 67%p=0.4Mucosal healing EEN: 74%CS: 33%p<0.05
Mucosal healing comparing EEN with CS
Borrelli. Clin Gastroenterol Hepatol, 2006121
Retrospective Paediatric CD 8 Weeks Oral vs continues enteral feeding
Oral: 45 ptsEnteral: 61 pts
Remission:Oral EEN: 75%Tube EEN: 85%p=0.157
Oral equivalent to enteral feeding
Rubio. Aliment Pharmacol Ther, 2011122
Prospective uncontrolled
Adults 4 Weeks – EEN: 13 pts Significant improvement in quality of lifeClinical remission: 84.6%
Improvement of quality of life
Gou. Nutr Clin Pract, 2013123
Prospective inception cohort
Newly diagnosed children
6–8 Weeks EEN vs CS mild-to-moderate CD
5-ASA: 29 ptsEEN: 43 ptsCS: 114 pts
CS-free remission week 12:EEN: 71%CS: 46%5-ASA: 55%p=0.0006NCR:EEN: 39%CS: 25%5-ASA: 24%
EEN superior to CS for reduction of inflammation
Levine. IBD, 201470
Prospective cohort Paediatric CD 6 Weeks EEN vs healthy control
EEN: 15 ptsHC: 21 pts
EEN: decreased butyrate, decreased diversity, Faecalibacterium prausnitzii concentration decreased
EEN mechanism Gerasimidis. IBD, 2014124
Prospective cohort Newly diagnosed paediatric CD
6 Weeks Mild-to-moderate EEN with thiopurine
34 Children Clinical remission: 84%Early good endoscopic response: 58%Complete transmural healing ileal CD: 21%
Mucosal healing Grover. J Gastroenterol, 2014125
Prospective cohort Paediatric CD 8 Weeks EEN vs anti-TNF vs PEN with ad libitum diet
Anti-TNF: 52 ptsEEN: 22 ptsPEN: 16 pts
Clinical response: PEN- 64%EEN- 88%Anti-TNF - 84%p=0.08 FCP<250 mg/g:PEN: 14%EEN -45%Anti-TNF- 62%p=0.001
Comparison with anti-TNFEEN reduced calprotectin
Lee. IBD, 201569
Retrospective Newly diagnosed paediatric CD
8–16 Weeks EEN vs CS EEN:76 ptsCS 35 pts
EEN: 86.6% remission vs CS: 58.1%p<0.01
Reduced need for steroids
Connors. JCC, 201771
Prospective inception cohort
Newly diagnosed children
6–8 Weeks EEN vs CS EEN: 60 ptsCS: 87 pts
Remission:CS: 47%EEN: 63%p=0.036
EEN superior to CS Cohen Dolev. JCC, 201872
5-ASA, 5-aminosalicylic acid; CD, Crohn disease; CDAI, Crohn’s Disease Activity Index; CS, corticosteroids; EEN, exclusion enteral nutrition; FCP, faecal calprotectin; ITT, intention to treat; MUFA, monounsaturated fatty acids; NCR, normal C reactive protein remission; PEN, partial enteral nutrition; PUFA, polyunsaturated fatty acids.
on 4 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2017-315866 on 18 M
ay 2018. Dow
nloaded from

1734 Levine A, et al. Gut 2018;67:1726–1738. doi:10.1136/gutjnl-2017-315866
Recent advances in clinical practice
70% of patients; this was accompanied by a significant drop in ESR and CRP and was associated with mucosal healing among patients who achieved remission and were evaluated during the maintenance phase of the diet.77 The diet is low in animal fat, rich in complex carbohydrates, with moderate exposure to soluble fibre. It excludes wheat and dairy, emulsifiers, maltodextrins, cara-geenans and sulfites. This diet was subsequently evaluated for induction of remission in children and adults failing biologics. Among 21 patients with active disease after loss of response to biologics despite dose escalation or combination therapy, 61% achieved clinical remission, again with a significant drop in inflam-matory markers.78 While limited by design, these two retrospec-tive studies reported remission with an exclusion diet at both ends of the spectrum of clinical disease, suggesting that diet may be an important tool for controlling active disease even in established disease and among biologic unresponsive patients. These reports should be viewed as preliminary data that need to be validated in prospective controlled trials. Several RCTs using this method are ongoing at the present time (NCT01728870, NCT02843100, NCT02231814). The specific carbohydrate diet restricting carbo-hydrates and processed foods has been advocated for CD and UC. This was previously evaluated in 10 children with very mild CD (mean Harvey Bradshaw Index (HBI) 3.3, mean ESR 9.7), of whom 6 achieved clinical remission.79 However, another small study published this year demonstrated that this diet was not asso-ciated with mucosal healing.80 Clinical trials to assess this diet are underway at the present time (NCT02213835, NCT01749813), but randomised controlled studies evaluating patients with more significant disease are required. Fibre and prebiotics supplements have been evaluated as interventions in CD. A systematic review including 10 eligible studies with clinical outcomes found no evidence for use of fibre or prebiotics to induce or maintain remis-sion in CD.81 Importantly, these papers concluded that there was no evidence for restriction of fibre in the absence of obstructive symptoms or stricturing disease.
Maintenance of remissionThe idea of maintaining remission with diet is compelling and challenging at the same time. On the one hand, once remission
is established, it is certainly possible that diet will be sufficient to maintain homeostasis and prevent the cascade of pro-inflamma-tory events leading to flare; however, long-term studies are chal-lenging to perform and adherence becomes a serious concern. Nevertheless, several studies have assessed PEN for maintenance of remission, some showing promising results.
One of the first studies to suggest the merit of PEN was published in Gut in 1996. Wilschanski et al82 followed 28 children who responded to EEN induction therapy for up to 12 months and agreed to receive nightly nasogastric PEN; they were less likely to flare than the 19 patients who chose not to receive PEN. A review, which included 10 published studies, most of which were not randomised, demonstrated some endoscopic improvement with PEN, but the overall quality of these studies was limited, high-lighting the need for large, prospective RCTs.83
A retrospective, single-centre study from Israel followed 42 children who responded to EEN and then went on PEN (50% liquid formula, 50% free diet) for a median of 40 months. Although a survival analysis was not included, median time for remaining in remission was 6 months; however, the median time in remission without need for additional therapy was 0 months (0–16 months). Eighty-six percent of patients started on PEN as maintenance therapy required additional therapy by 6 months.84 There is insufficient evidence to recommend PEN as the only maintenance therapy in children based on existing data.
Another approach, mainly based on studies in adults from Japan, has focused on partial elemental diet (ED), providing a minimum of 900 kcal/day combined with a free diet. An RCT comparing this approach to a fully free diet showed lower relapse rates at a mean follow-up of 1 year (34.6% vs 64%).85 More recent retrospective studies have indicated a potential advan-tage for partial ED in reducing loss of response to infliximab and adalimumab.86 87 PEN has also been shown to be effective in preventing postoperative recurrence of CD. Twenty adults who were compliant to EN were treated with nightly ED and a low fat diet during the day and were followed for 5 years; remarkably, 16 maintained the diet. Only two had disease recurrence (vs 9/20 in a normal-diet control group; p=0.03) and 1 (vs 5) required addi-tional surgery.88 Japanese researchers randomised adult patients
Figure 4 New targets for dietary interventions in Crohn disease (CD).
on 4 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2017-315866 on 18 M
ay 2018. Dow
nloaded from

1735Levine A, et al. Gut 2018;67:1726–1738. doi:10.1136/gutjnl-2017-315866
Recent advances in clinical practice
with CD in remission on maintenance 5-aminosalicylic acid (ASA) to additional 6-mercaptopurine (MP), PEN with 900 kcal/day from an ED, or no additional therapy. At the end of 2 years, sustained remission was present in 60% of patients on 6-MP, 47% of patients on PEN and only 27% of patients on 5-ASA. Both 6-MP and PEN were significantly superior to 5-ASA.89 Fernán-dez-Bañares et al demonstrated that combining fibre supplements with mesalamine was more effective than mesalamine alone for maintenance of remission.90 A systematic review found that there was no evidence for an effect of dietary fibre on disease outcomes in UC.81
dietary therapy for complicated cdCD is associated with several complications that eventually can lead to surgery. Treatment of complicated disease, such as stric-tures, abscesses and fistulae has traditionally been either medical or surgical. Recent studies have demonstrated that dietary therapy with EEN may have the potential to treat complications and have a ‘surgery sparing effect’.
Two studies conducted by a group from China evaluated the efficacy of EEN in complicated CD. Hu et al conducted a prospec-tive, observational study to examine the effects of 12 weeks of EEN on inflammatory bowel strictures. They performed cross-sec-tional CT before and after therapy. Sixty-five per cent of patients achieved clinical remission, while 54% achieved radiologic remis-sion. This was accompanied by a significant increase in luminal diameter and a significant decrease in bowel wall thickness.91 Yan et al conducted a prospective study to identify the predictors of response to 12 weeks of EEN in patients with CD who had entero-cutaneous fistulae. They demonstrated that 30/48 (62.5%) had a successfully closure of fistula after EEN therapy with average closure time of 32.4±8.85 days. They found that decreased CRP and elevated body mass index levels were associated with response to EN in patients with CD with enterocutaneous fistulae.92
EEN has also been demonstrated to reduce the need for surgery in complicated disease. Heerasing et al demonstrated in a retro-spective case-control study that EEN for a period of 6 weeks could lead to avoidance of surgery in (13/51) 25% of patients who were scheduled for an elective surgical resection.93 They also showed by multivariable logistic regression analysis that patients who went to surgery without EEN had a ninefold increase in the incidence of postoperative abscess and/or anastomotic leak (OR 9.1; 95% CI 1.2 to 71.2, p=0.04). An additional recent retrospective study conducted by a group from China reported that patients with CD with intra-abdominal abscesses who were treated with 4 weeks of EEN and antibiotics were less likely to require surgical interven-tion compared with those who did not use EEN (26.1% vs 56.3%, p=0.01).94 Several studies have confirmed that perioperative EEN can improve surgical outcomes, reduce complications and the need for immune suppression.95 96 Use of preoperative EEN may have long-lasting effects. Wang et al found that EEN prior to resection was accompanied by a significant reduction of endoscopic recur-rence rates after resection for CD after 6 months.96 In addition, a large retrospective study demonstrated that administration of EEN for approximately 4 weeks led to lower rates of stoma creation (p<0.05), a decrease in urgent operation requirement (p<0.05) and extended preoperative drug-free intervals (p<0.001).97
diet for functional symptomsPatients with IBD may experience GI symptoms even during remission without underlying inflammation. Recent studies have demonstrated that restriction of several groups of fermentable
carbohydrates (low fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAP) diet) is effective in the management of functional symptoms. Prince et al found that 78%, p<0.001 with IBD reported satisfactory relief of func-tional symptoms after 6 weeks of low FODMAP diet.98 A recent meta-analysis concluded that a low FODMAP diet is beneficial for reducing GI symptoms in patients with quiescent IBD.99 Halmos et al100 showed that the low FODMAP diet had no effect on the calprotectin results in patients with CD. Furthermore, altering dietary FODMAP intake was associated with possible detrimental changes in faecal microbiota and therefore is not recommended for extended periods of time.
summaryIn summary, there seems to be a growing body of evidence to suggest that dietary factors may play an important role in the patho-genesis of CD. Use of EEN has expanded from a tool for induction of remission in children at disease onset, to a tool with potential to treat very complicated long duration disease in adults (figure 4). Use of perioperative EEN has the potential to avoid the need for surgery, reduce poor surgical outcomes and delay postoperative recurrence in CD. Perhaps the most exciting development is the potential to induce and maintain remission by use of exclusion diets and PEN, which would enable wider use of dietary therapy across the spectrum. However, the field still has insufficient high-quality evidence due to the small number of well-designed trials performed to date, but the future appears to be bright in CD. RCTs with newer dietary interventions or indications are warranted. Perhaps the largest research gaps at the present are in the field of UC. Although there are emerging clues linking diet to UC as well, researchers have yet to make the jump from bench to bedside in UC, and we still do not know if dietary therapy would be effective in UC.
contributors All authors contributed to the writing of the manuscript.
Funding This study was funded by grants from Nestle and the Azrieli Foundation.
competing interests None declared.
Patient consent Not required.
Provenance and peer review Commissioned; externally peer reviewed.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
REFEREncEs 1 Ogura Y, Bonen DK, Inohara N, et al. A frameshift mutation in NOD2 associated with
susceptibility to Crohn’s disease. Nature 2001;411:603–6. 2 Hugot J-P, Chamaillard M, Zouali H, et al. Association of NOD2 leucine-rich repeat
variants with susceptibility to Crohn’s disease. Nature 2001;411:599–603. 3 Luo Y, de Lange KM, Jostins L, et al. Exploring the genetic architecture of
inflammatory bowel disease by whole-genome sequencing identifies association at ADCY7. Nat Genet 2017;49:186–92.
4 Huang H, Fang M, Jostins L, et al. Fine-mapping inflammatory bowel disease loci to single-variant resolution. Nature 2017;547:173–8.
5 Peters LA, Perrigoue J, Mortha A, et al. A functional genomics predictive network model identifies regulators of inflammatory bowel disease. Nat Genet 2017;49:1437–49.
6 Jostins L, Ripke S, Weersma RK, et al. Host–microbe interactions have shaped the genetic architecture of inflammatory bowel disease. Nature 2012;491:119–24.
7 Bording-Jorgensen M, Alipour M, Danesh G, et al. Inflammasome Activation by ATP Enhances Citrobacter rodentium Clearance through ROS Generation. Cell Physiol Biochem 2017;41:193–204.
8 Teshima CW, Goodman KJ, El-Kalla M, et al. Increased intestinal permeability in relatives of patients with crohn’s disease is not associated with small bowel ulcerations. Clinical Gastroenterology and Hepatology 2017;15:1413–8.
9 Buhner S, et al. Genetic basis for increased intestinal permeability in families with Crohn’s disease: role of CARD15 3020insC mutation? Gut 2006;55:342–7.
on 4 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2017-315866 on 18 M
ay 2018. Dow
nloaded from

1736 Levine A, et al. Gut 2018;67:1726–1738. doi:10.1136/gutjnl-2017-315866
Recent advances in clinical practice
10 Kevans D, Turpin W, Madsen K, et al. Determinants of intestinal permeability in healthy first-degree relatives of individuals with crohnʼs disease. Inflamm Bowel Dis 2015;21:879–87.
11 Johansson MEV, Gustafsson JK, Holmén-Larsson J, et al. Bacteria penetrate the normally impenetrable inner colon mucus layer in both murine colitis models and patients with ulcerative colitis. Gut 2014;63:281–91.
12 McCole DF. IBD candidate genes and intestinal barrier regulation. Inflamm Bowel Dis 2014;20:1829–49.
13 Kleessen B, Kroesen AJ, Buhr HJ, et al. Mucosal and invading bacteria in patients with inflammatory bowel disease compared with controls. Scand J Gastroenterol 2002;37:1034–41.
14 Kiesslich R, Duckworth CA, Moussata D, et al. Local barrier dysfunction identified by confocal laser endomicroscopy predicts relapse in inflammatory bowel disease. Gut 2012;61:1146–53.
15 Vogelsang H. Do changes in intestinal permeability predict disease relapse in crohnʼs disease? Inflamm Bowel Dis 2008;14(Suppl 2):S162–3.
16 Gevers D, Kugathasan S, Knights D, et al. A microbiome foundation for the study of crohn’s disease. Cell Host Microbe 2017;21:301–4.
17 Zaidi D, Bording-Jorgensen M, Huynh HQ, et al. Increased epithelial gap density in the noninflamed duodenum of children with inflammatory bowel diseases. J Pediatr Gastroenterol Nutr 2016;63:644–50.
18 Zaidi D, Churchill L, Huynh HQ, et al. Capillary flow rates in the duodenum of pediatric ulcerative colitis patients are increased and unrelated to inflammation. J Pediatr Gastroenterol Nutr 2017;65:306–10.
19 Alipour M, Zaidi D, Valcheva R, et al. Mucosal barrier depletion and loss of bacterial diversity are primary abnormalities in paediatric ulcerative colitis. Journal of Crohn's and Colitis 2016;10:462–71.
20 Vrakas S, Mountzouris KC, Michalopoulos G, et al. Intestinal bacteria composition and translocation of bacteria in inflammatory bowel disease. PLoS One 2017;12:e0170034.
21 Pascal V, Pozuelo M, Borruel N, et al. A microbial signature for Crohn’s disease. Gut 2017;66:813–22.
22 Mazzarella G, Perna A, Marano A, et al. Pathogenic role of associated adherent-invasive Escherichia coli in Crohn’s Disease. J Cell Physiol 2017;232:2860–8.
23 Darfeuille-Michaud A, Boudeau J, Bulois P, et al. High prevalence of adherent-invasive Escherichia coli associated with ileal mucosa in Crohn’s disease. Gastroenterology 2004;127:412–21.
24 Sartor RB, Wu GD, Gd W. Roles for intestinal bacteria, viruses, and fungi in pathogenesis of inflammatory bowel diseases and therapeutic approaches. Gastroenterology 2017;152:327–39.
25 Gevers D, Kugathasan S, Denson LA, et al. The treatment-naive microbiome in new-onset crohn’s disease. Cell Host Microbe 2014;15:382–92.
26 Machiels K, Sabino J, Vandermosten L, et al. Specific members of the predominant gut microbiota predict pouchitis following colectomy and IPAA in UC. Gut 2017;66:79–88.
27 Khalil NA, Walton GE, Gibson GR, et al. In vitro batch cultures of gut microbiota from healthy and ulcerative colitis (UC) subjects suggest that sulphate-reducing bacteria levels are raised in UC and by a protein-rich diet. Int J Food Sci Nutr 2014;65:79–88.
28 James SL, Christophersen CT, Bird AR, et al. Abnormal fibre usage in UC in remission. Gut 2015;64:562–70.
29 Desai MS, Seekatz AM, Koropatkin NM, et al. A dietary fiber-deprived gut microbiota degrades the colonic mucus barrier and enhances pathogen susceptibility. Cell 2016;167:1339–53.
30 David LA, Maurice CF, Carmody RN, et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature 2014;505:559–63.
31 Holmes AJ, Chew YV, Colakoglu F, et al. Diet-Microbiome interactions in health are controlled by intestinal nitrogen source constraints. Cell Metab 2017;25:140–51.
32 Jantchou P, Morois S, Clavel-Chapelon F, et al. Animal protein intake and risk of inflammatory bowel disease: the E3N prospective study. Am J Gastroenterol 2010;105:2195–201.
33 DʼSouza S, Levy E, Mack D, et al. Dietary patterns and risk for Crohnʼs disease in children. Inflamm Bowel Dis 2008;14:367–73.
34 Racine A, Carbonnel F, Chan SS, et al. Dietary Patterns and risk of inflammatory bowel disease in Europe: results from the EPIC Study. Inflamm Bowel Dis 2016;22:345–54.
35 Shoda R, Matsueda K, Yamato S, et al. Epidemiologic analysis of Crohn disease in Japan: increased dietary intake of n-6 polyunsaturated fatty acids and animal protein relates to the increased incidence of Crohn disease in Japan. Am J Clin Nutr 1996;63:741–5.
36 Jowett SL, et al. Influence of dietary factors on the clinical course of ulcerative colitis: a prospective cohort study. Gut 2004;53:1479–84.
37 Ananthakrishnan AN, Khalili H, Konijeti GG, et al. A prospective study of long-term intake of dietary fiber and risk of crohn’s disease and ulcerative colitis. Gastroenterology 2013;145:970–7.
38 Costea I, Mack DR, Lemaitre RN, et al. Interactions between the dietary polyunsaturated fatty acid ratio and genetic factors determine susceptibility to pediatric crohn’s disease. Gastroenterology 2014;146:929–31.
39 Chan SSM, Luben R, van Schaik F, et al. Carbohydrate intake in the etiology of crohnʼs disease and ulcerative colitis. Inflamm Bowel Dis 2014;20:2013–21.
40 Xu L, Lochhead P, Ko Y, et al. Systematic review with meta-analysis: breastfeeding and the risk of Crohn’s disease and ulcerative colitis. Aliment Pharmacol Ther 2017;46:780–9.
41 Loftus EV. Clinical epidemiology of inflammatory bowel disease: incidence, prevalence, and environmental influences. Gastroenterology 2004;126:1504–17.
42 Niewiadomski O, Studd C, Wilson J, et al. Influence of food and lifestyle on the risk of developing inflammatory bowel disease. Intern Med J 2016;46:669–76.
43 Hou JK, Abraham B, El-Serag H. Dietary intake and risk of developing inflammatory bowel disease: a systematic review of the literature. Am J Gastroenterol 2011;106:563–73.
44 Bergmann MM, Hernandez V, Bernigau W, et al. No association of alcohol use and the risk of ulcerative colitis or Crohn’s disease: data from a European Prospective cohort study (EPIC). Eur J Clin Nutr 2017;71:512–8.
45 Moubarac J-C, Batal M, Martins APB, et al. Processed and ultra-processed food products: consumption trends in Canada from 1938 to 2011. Canadian Journal of Dietetic Practice and Research 2014;75:15–21.
46 Roberts CL, Rushworth SL, Richman E, et al. Hypothesis: Increased consumption of emulsifiers as an explanation for the rising incidence of Crohn’s disease. Journal of Crohn's and Colitis 2013;7:338–41.
47 Wang H, Shi P, Zuo L, et al. Dietary non-digestible polysaccharides ameliorate intestinal epithelial barrier dysfunction in IL-10 Knockout Mice. Journal of Crohn's and Colitis 2016;10:1076–86.
48 Furusawa Y, Obata Y, Fukuda S, et al. Commensal microbe-derived butyrate induces the differentiation of colonic regulatory T cells. Nature 2013;504:446–50.
49 Martinez-Medina M, Denizot J, Dreux N, et al. Western diet induces dysbiosis with increased E coli in CEABAC10 mice, alters host barrier function favouring AIEC colonisation. Gut 2014;63:116–24.
50 Ma X, Torbenson M, Hamad ARA, et al. High-fat diet modulates non-CD1d-restricted natural killer T cells and regulatory T cells in mouse colon and exacerbates experimental colitis. Clinical & Experimental Immunology 2008;151:130–8.
51 Ejsing-Duun M, Josephsen J, Aasted B, et al. Dietary gluten reduces the number of intestinal regulatory t cells in mice. Scand J Immunol 2008;67:553–9.
52 Wagner SJ, Schmidt A, Effenberger MJP, et al. Semisynthetic diet ameliorates crohn’s Disease–Like Ileitis in TNFΔARE/WT mice through antigen-independent mechanisms of gluten. Inflamm Bowel Dis 2013;19:1285–94.
53 Zevallos VF, Raker V, Tenzer S, et al. Nutritional Wheat Amylase-Trypsin Inhibitors Promote Intestinal Inflammation via Activation of Myeloid Cells. Gastroenterology 2017;152:1100–13.
54 Junker Y, Zeissig S, Kim S-J, et al. Wheat amylase trypsin inhibitors drive intestinal inflammation via activation of toll-like receptor 4. J Exp Med 2012;209:2395–408.
55 Chassaing B, Koren O, Goodrich JK, et al. Dietary emulsifiers impact the mouse gut microbiota promoting colitis and metabolic syndrome. Nature 2015;519:92–6.
56 Nickerson KP, Chanin R, McDonald C. Deregulation of intestinal anti-microbial defense by the dietary additive, maltodextrin. Gut Microbes 2015;6:78–83.
57 Nickerson KP, Homer CR, Kessler SP, et al. The dietary polysaccharide maltodextrin promotes salmonella survival and mucosal colonization in mice. PLoS One 2014;9:e101789.
58 Fahoum L, Moscovici A, David S, et al. Digestive fate of dietary carrageenan: evidence of interference with digestive proteolysis and disruption of gut epithelial function. Mol Nutr Food Res 2017;61:16.
59 Choi HJ, Kim J, Park S-H, et al. Pro-inflammatory NF-κB and early growth response gene 1 regulate epithelial barrier disruption by food additive carrageenan in human intestinal epithelial cells. Toxicol Lett 2012;211:289–95.
60 Agus A, Denizot J, Thévenot J, et al. Western diet induces a shift in microbiota composition enhancing susceptibility to Adherent-Invasive E. coli infection and intestinal inflammation. Sci Rep 2016;6:19032.
61 Lai K-P, Chung Y-T, Li R, et al. Bisphenol A alters gut microbiome: Comparative metagenomics analysis. Environ Pollut 2016;218:923–30.
62 Islam KBMS, Fukiya S, Hagio M, et al. Bile acid is a host factor that regulates the composition of the cecal microbiota in rats. Gastroenterology 2011;141:1773–81.
63 Nickerson KP, McDonald C. Crohn’s disease-associated adherent-invasive escherichia coli adhesion is enhanced by exposure to the Ubiquitous Dietary Polysaccharide Maltodextrin. PLoS One 2012;7:e52132.
64 Devkota S, Wang Y, Musch MW, et al. Dietary-fat-induced taurocholic acid promotes pathobiont expansion and colitis in Il10 −/− mice. Nature 2012;487:104–8.
65 Roberts CL, Keita AV, Duncan SH, et al. Translocation of Crohn’s disease Escherichia coli across M-cells: contrasting effects of soluble plant fibres and emulsifiers. Gut 2010;59:1331–9.
66 Chassaing B, Van de Wiele T, De Bodt J, et al. Dietary emulsifiers directly alter human microbiota composition and gene expression ex vivo potentiating intestinal inflammation. Gut 2017;66:1414–27.
67 Ruemmele FM, Veres G, Kolho KL, et al. Consensus guidelines of ECCO/ESPGHAN on the medical management of pediatric Crohn’s disease. Journal of Crohn's and Colitis 2014;8:1179–207.
68 Johnson T, Macdonald S, Hill SM, et al. Treatment of active Crohn’s disease in children using partial enteral nutrition with liquid formula: a randomised controlled trial. Gut 2006;55:356–61.
on 4 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2017-315866 on 18 M
ay 2018. Dow
nloaded from

1737Levine A, et al. Gut 2018;67:1726–1738. doi:10.1136/gutjnl-2017-315866
Recent advances in clinical practice
69 Lee D, Baldassano RN, Otley AR, et al. Comparative effectiveness of nutritional and biological therapy in north american children with active crohnʼs disease. Inflamm Bowel Dis 2015;21:1786–93.
70 Levine A, Turner D, Pfeffer Gik T, et al. Comparison of outcomes parameters for induction of remission in new onset pediatric Crohn’s disease: evaluation of the porto IBD group "growth relapse and outcomes with therapy" (GROWTH CD) study. Inflamm Bowel Dis 2014;20:278–85.
71 Connors J, Basseri S, Grant A, et al. Exclusive enteral nutrition therapy in paediatric crohn’s disease results in long-term avoidance of corticosteroids: results of a propensity-score matched cohort analysis. Journal of Crohn's and Colitis 2017;11:1063–70.
72 Cohen-Dolev N, Sladek M, Hussey S, et al. Differences in outcomes over time with exclusive enteral nutrition compared with steroids in children with mild to moderate crohn’s disease: results from the GROWTH CD Study. Journal of Crohn's and Colitis 2018;12:306–12.
73 Grover Z, Burgess C, Muir R, et al. Early mucosal healing with exclusive enteral nutrition is associated with improved outcomes in newly diagnosed children with luminal crohn’s disease. Journal of Crohn's and Colitis 2016;10:1159–64.
74 Buchanan E, Gaunt WW, Cardigan T, et al. The use of exclusive enteral nutrition for induction of remission in children with Crohn’s disease demonstrates that disease phenotype does not influence clinical remission. Aliment Pharmacol Ther 2009;30:501–7.
75 Van Limbergen J, Haskett J, Griffiths AM, et al. Toward enteral nutrition in the treatment of pediatric crohn disease in canada: a workshop to identify barriers and enablers. Canadian Journal of Gastroenterology and Hepatology 2015;29:351–6.
76 Levine A, Wine E. Effects of enteral nutrition on Crohn’s disease: clues to the impact of diet on disease pathogenesis. Inflamm Bowel Dis 2013;19:1322–9.
77 Sigall-Boneh R, Pfeffer-Gik T, Segal I, et al. Partial enteral nutrition with a Crohn’s disease exclusion diet is effective for induction of remission in children and young adults with Crohn’s disease. Inflamm Bowel Dis 2014;20:1353–60.
78 Sigall Boneh R, Sarbagili Shabat C, Yanai H, et al. Dietary therapy with the crohn’s disease exclusion diet is a successful strategy for induction of remission in children and adults failing biological therapy. J Crohns Colitis 2017;11:1205–12.
79 Cohen SA, Gold BD, Oliva S, et al. Clinical and mucosal improvement with specific carbohydrate diet in pediatric Crohn disease. J Pediatr Gastroenterol Nutr 2014;59:516–21.
80 Wahbeh GT, Ward BT, Lee DY, et al. Lack of Mucosal Healing From Modified Specific Carbohydrate Diet in Pediatric Patients With Crohn Disease. J Pediatr Gastroenterol Nutr 2017;65:289–92.
81 Wedlake L, Slack N, Andreyev HJ, et al. Fiber in the treatment and maintenance of inflammatory bowel disease: a systematic review of randomized controlled trials. Inflamm Bowel Dis 2014;20:576–86.
82 Wilschanski M, Sherman P, Pencharz P, et al. Supplementary enteral nutrition maintains remission in paediatric Crohn’s disease. Gut 1996;38:543–8.
83 Yamamoto T, Nakahigashi M, Umegae S, et al. Enteral nutrition for the maintenance of remission in Crohn’s disease: a systematic review. Eur J Gastroenterol Hepatol 2010;22:1–8.
84 Schulman JM, Pritzker L, Shaoul R. Maintenance of remission with partial enteral nutrition therapy in pediatric crohn’s disease: a retrospective study. Can J Gastroenterol Hepatol 2017;2017:1–7.
85 Takagi S, Utsunomiya K, Kuriyama S, et al. Effectiveness of an ’half elemental diet’ as maintenance therapy for Crohn’s disease: A randomized-controlled trial. Aliment Pharmacol Ther 2006;24:1333–40.
86 Sugita N, Watanabe K, Kamata N, et al. Efficacy of a concomitant elemental diet to reduce the loss of response to adalimumab in patients with intractable Crohn’s disease. J Gastroenterol Hepatol 2018;33:631-637.
87 Kamata N, Oshitani N, Watanabe K, et al. Efficacy of concomitant elemental diet therapy in scheduled infliximab therapy in patients with Crohn’s disease to prevent loss of response. Dig Dis Sci 2015;60:1382–8.
88 Yamamoto T, Shiraki M, Nakahigashi M, et al. Enteral nutrition to suppress postoperative Crohn’s disease recurrence: a five-year prospective cohort study. Int J Colorectal Dis 2013;28:335–40.
89 Hanai H, Iida T, Takeuchi K, et al. Nutritional therapy versus 6-mercaptopurine as maintenance therapy in patients with Crohn’s disease. Dig Liver Dis 2012;44:649–54.
90 Fernández-Bañares F, Hinojosa J, Sánchez-Lombraña JL, et al. Randomized clinical trial of Plantago ovata seeds (dietary fiber) as compared with mesalamine in maintaining remission in ulcerative colitis. Spanish Group for the Study of Crohn’s Disease and Ulcerative Colitis (GETECCU). Am J Gastroenterol 1999;94:427–33.
91 Hu D, Ren J, Wang G, et al. Exclusive enteral nutritional therapy can relieve inflammatory bowel stricture in Crohn’s disease. J Clin Gastroenterol 2014;48:790–5.
92 Yan D, Ren J, Wang G, et al. Predictors of response to enteral nutrition in abdominal enterocutaneous fistula patients with Crohn’s disease. Eur J Clin Nutr 2014;68:959–63.
93 Heerasing N, Thompson B, Hendy P, et al. Exclusive enteral nutrition provides an effective bridge to safer interval elective surgery for adults with Crohn’s disease. Aliment Pharmacol Ther 2017;45:660–9.
94 Zheng XB, Peng X, Xie XY, et al. Enteral nutrition is associated with a decreased risk of surgical intervention in Crohn’s disease patients with spontaneous intra-abdominal abscess. Rev Esp Enferm Dig 2017;109:109.
95 Li G, Ren J, Wang G, et al. Preoperative exclusive enteral nutrition reduces the postoperative septic complications of fistulizing Crohn’s disease. Eur J Clin Nutr 2014;68:441–6.
96 Wang H, Zuo L, Zhao J, et al. Impact of Preoperative Exclusive Enteral Nutrition on Postoperative Complications and Recurrence After Bowel Resection in Patients with Active Crohn’s Disease. World J Surg 2016;40:1993–2000.
97 Li Y, Zuo L, Zhu W, et al. Role of exclusive enteral nutrition in the preoperative optimization of patients with Crohn’s disease following immunosuppressive therapy. Medicine 2015;94:e478.
98 Prince AC, Myers CE, Joyce T, et al. Fermentable Carbohydrate Restriction (Low FODMAP Diet) in clinical practice improves functional gastrointestinal symptoms in patients with inflammatory bowel disease. Inflamm Bowel Dis 2016;22:1129–36.
99 Zhan YL, Zhan YA, Dai SX. Is a low FODMAP diet beneficial for patients with inflammatory bowel disease? A meta-analysis and systematic review. Clin Nutr 2018;37:123–9.
100 Halmos EP, Christophersen CT, Bird AR, et al. Consistent prebiotic effect on gut microbiota with altered FODMAP intake in patients with crohn’s disease: a randomised, controlled cross-over trial of well-defined diets. Clin Transl Gastroenterol 2016;7:e164.
101 Suzuki T, Hara H. Dietary fat and bile juice, but not obesity, are responsible for the increase in small intestinal permeability induced through the suppression of tight junction protein expression in LETO and OLETF rats. Nutr Metab 2010;7:19.
102 Gruber L, Kisling S, Lichti P, et al. High fat diet accelerates pathogenesis of murine crohn’s disease-like ileitis independently of obesity. PLoS One 2013;8:e71661.
103 Soderholm JD, Oman H, Blomquist L, et al. Reversible increase in tight junction permeability to macromolecules in rat ileal mucosa in vitro by sodium caprate, a constituent of milk fat. Dig Dis Sci 1998;43:1547–52.
104 Soderholm JD, et al. Augmented increase in tight junction permeability by luminal stimuli in the non-inflamed ileum of Crohn’s disease. Gut 2002;50:307–13.
105 Lammers KM, Lu R, Brownley J, et al. Gliadin induces an increase in intestinal permeability and zonulin release by binding to the chemokine receptor CXCR3. Gastroenterology 2008;135:194–204.
106 Hollon J, Puppa E, Greenwald B, et al. Effect of gliadin on permeability of intestinal biopsy explants from celiac disease patients and patients with non-celiac gluten sensitivity. Nutrients 2015;7:1565–76.
107 Bassaganya-Riera J, DiGuardo M, Viladomiu M, et al. Soluble fibers and resistant starch ameliorate disease activity in interleukin-10–deficient mice with inflammatory bowel disease. J Nutr 2011;141:1318–25.
108 Mb Y, Lim BO. Dietary pectin regulates the levels of inflammatory cytokines and immunoglobulins in interleukin-10 knockout mice. Journal of agricultural and food chemistry 2010;58:11281–6.
109 Hung TV, Suzuki T. Dietary Fermentable Fiber Reduces Intestinal Barrier Defects and Inflammation in Colitic Mice. J Nutr 2016;146:1970–9.
110 Forsyth CB, Shaikh M, Bishehsari F, et al. Alcohol feeding in mice promotes colonic hyperpermeability and changes in colonic organoid stem cell fate. Alcoholism: Clinical and Experimental Research 2017;41:2100–13.
111 Tubbs AL, Liu B, Rogers TD, et al. Dietary salt exacerbates experimental colitis. The Journal of Immunology 2017;199:1051–9.
112 Swidsinski A, Ung V, Sydora BC, et al. Bacterial overgrowth and inflammation of small intestine after carboxymethylcellulose ingestion in genetically susceptible mice. Inflamm Bowel Dis 2009;15:359–64.
113 Miyazato S, Kishimoto Y, Takahashi K, et al. Continuous intake of resistant maltodextrin enhanced intestinal immune response through changes in the intestinal environment in mice. Biosci Microbiota Food Health 2016;35:1–7.
114 Ruiz PA, Morón B, Becker HM, et al. Titanium dioxide nanoparticles exacerbate DSS-induced colitis: role of the NLRP3 inflammasome. Gut 2017;66:1216–24.
115 Silveira ALM, Ferreira AVM, de Oliveira MC, et al. Preventive rather than therapeutic treatment with high fiber diet attenuates clinical and inflammatory markers of acute and chronic DSS-induced colitis in mice. Eur J Nutr 2017;56:179–91.
116 Munyaka PM, Sepehri S, Ghia J-E, et al. Carrageenan gum and adherent invasive Escherichia coli in a piglet model of inflammatory bowel disease: impact on intestinal mucosa-associated microbiota. Front Microbiol 2016;7:462.
117 Malchow H, Steinhardt HJ, Lorenz-Meyer H, et al. Feasibility and effectiveness of a defined-formula diet regimen in treating active Crohn’s disease. European Cooperative Crohn’s Disease Study III. Scand J Gastroenterol 1990;25:235–44.
118 Lochs H, Steinhardt HJ, Klaus-Wentz B, et al. Comparison of enteral nutrition and drug treatment in active Crohn’s disease. Results of the European Cooperative Crohn’s Disease Study. IV. Gastroenterology 1991;101:881–8.
119 Gassull MA, Fernandez-Banares F, Cabre E, et al. Fat composition may be a clue to explain the primary therapeutic effect of enteral nutrition in Crohn’s disease: results of a double blind randomised multicentre European trial. Gut 2002;51:164–8.
on 4 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2017-315866 on 18 M
ay 2018. Dow
nloaded from

1738 Levine A, et al. Gut 2018;67:1726–1738. doi:10.1136/gutjnl-2017-315866
Recent advances in clinical practice
120 Ludvigsson JF, Krantz M, Bodin L, et al. Elemental versus polymeric enteral nutrition in paediatric Crohn’s disease: a multicentre randomized controlled trial. Acta Paediatr 2004;93:327–35.
121 Borrelli O, Cordischi L, Cirulli M, et al. Polymeric diet alone versus corticosteroids in the treatment of active pediatric crohn’s disease: a randomized controlled open-label trial. Clinical Gastroenterology and Hepatology 2006;4:744–53.
122 Rubio A, Pigneur B, Garnier-Lengliné H, et al. The efficacy of exclusive nutritional therapy in paediatric Crohn’s disease, comparing fractionated oral vs. continuous enteral feeding. Aliment Pharmacol Ther 2011;33:1332–9.
123 Guo Z, Wu R, Zhu W, et al. Effect of Exclusive enteral nutrition on health-related quality of life for adults with active crohn’s disease. Nutrition in Clinical Practice 2013;28:499–505.
124 Gerasimidis K, Bertz M, Hanske L, et al. Decline in presumptively protective gut bacterial species and metabolites are paradoxically associated with disease improvement in pediatric crohn’s disease during enteral nutrition. Inflamm Bowel Dis 2014;20:861–71.
125 Grover Z, Muir R, Lewindon P. Exclusive enteral nutrition induces early clinical, mucosal and transmural remission in paediatric Crohn’s disease. J Gastroenterol 2014;49:638–45.
on 4 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gutjnl-2017-315866 on 18 M
ay 2018. Dow
nloaded from