Evolutive particularities of cardiovascular disorders in children with Marfan Syndrome First author:...
27
Evolutive particularities of cardiovascular disorders in children with Marfan Syndrome First author: Adriana Crăciun Second authors: Aurica Creța, Iulia Gavrilă, Armina Mihanoș Coordinator: Conf. Dr. Amalia Făgărășan
-
Upload
juliet-atkins -
Category
Documents
-
view
214 -
download
0
Transcript of Evolutive particularities of cardiovascular disorders in children with Marfan Syndrome First author:...

Evolutive particularities of cardiovascular disorders in children with Marfan
Syndrome
First author: Adriana Crăciun
Second authors: Aurica Creța, Iulia Gavrilă, Armina Mihanoș
Coordinator: Conf. Dr. Amalia Făgărășan
Marfan syndrome is an autosomal dominant heritable disorder of fibrous connective tissue due to mutation in the fibrillin-1 gene, located on chromosome 15. It has a reported incidence of 1 in 3000 to 5000 individuals.
Marfan syndrome most often affects the connective tissue of the heart and blood vessels, eyes, bones, lungs and dura mater. Because the condition affects many parts of the body, it can cause many complications that could eventually be life threatening.

The diagnosis of Marfan syndrome relies on defined clinical criteria –The revised Ghent nosology- where special considerations are given to the diagnosis of MFS in children.

The diagnosis of MFS in familial and sporadic cases is based
upon the presence of characteristic manifestations:
1. Particularly: - Aortic root dilatation/dissection
- Ectopia lentis

2. Systemic features:
-musculoskeletal abnormalities
- mitral valve prolapse
-dural ectasia, pneumothorax and skin striae

Given the fact that the aortic root dilatation is the most
important disorder of the MFS it is paramount to surveil its size.The aortic root Z-score is used to identify aortic dilatation since aortic size varies with body size. However, use of Z score may underestimate aortic size, particularly in individuals with large body surface area.

Purpose
The aim of this study is to show a follow-up image of the cardiovascular disorder in Marfan syndrome emphasising not only over the cardiovascular aspects of the syndrome itself but also on a comparative approach which concerns the mitral valve prolapse and the mitral regurgitation.
MVP and MR is identified at all patients with Marfan syndrome so that is why the comparison aims to show if children with Marfan syndrome encounter more cardiac complications during the follow-up than those who only have mitral valve prolapse and mitral regurgitation.

Matherial and method
We conducted a retrospective study in the Pediatric Cardiology Clinic from Targu-Mures in the period 2003-2013. We had a total of 15 patients with Marfan syndrome ( all of them presenting MVP and mitral regurgitation) and a control group comprising 15 patients with chronic mitral regurgitation and mitral valve prolapse without any other cardiovascular pathologies associated.
Studied parameters were: age, sex, area, family history, the ecocardiographic status at the moment of diagnosis, periodic controls, the evolution in time, the occurence of the arrythmias and the need of surgical interventions.

RESULTS

73,33%
60%
26,66%
40%
0,00%
10,00%
20,00%
30,00%
40,00%
50,00%
60,00%
70,00%
80,00%
female male
Marfan syndrome
Control group
40%
46,66%
60%53,33%
0%
10%
20%
30%
40%
50%
60%
urban area rural area
Marfan syndrome
Control group

Control group
13,33%
86,66%
Positive family history
Negative family history
Marfan syndrome
53,33%
46,66%Positive family history
Negative family history

13%
6,66%
40%40,00%
46,66%
53,33%
0%
10%
20%
30%
40%
50%
60%
< 3 years 3 to 7 years > 7 years
Marfan syndrome
Control group
0,00%
20,00%
40,00%
60,00%
80,00%
Marfan syndrome 73,33% 20% 6,66%
Control group 66,66% 33,33% 0,00%
Regular follow-up Irregular follow-upLost from the
follow-up
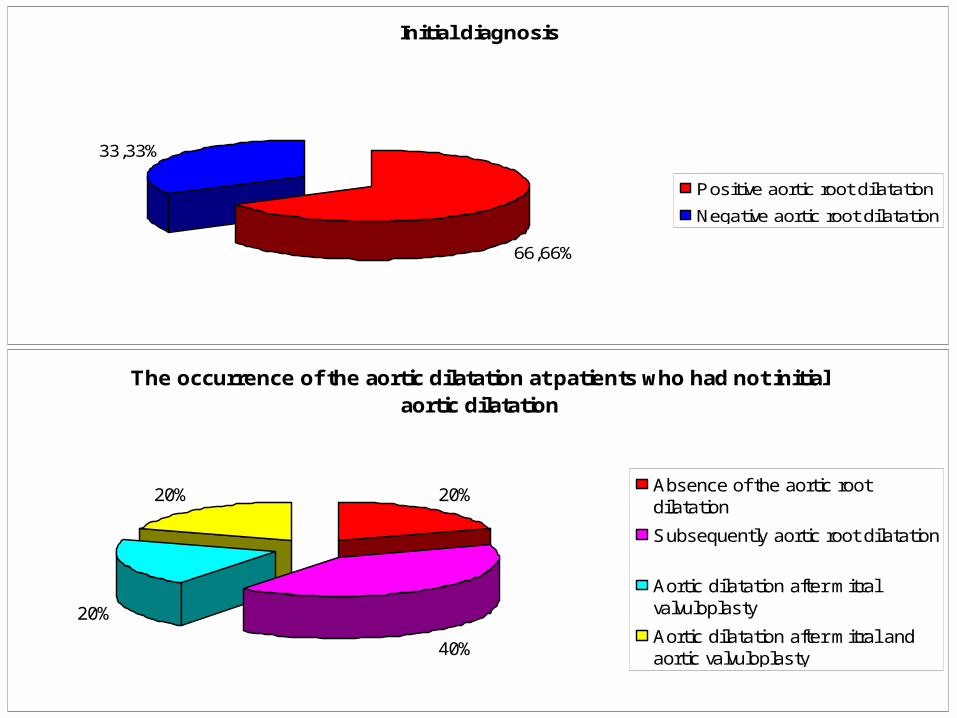
Initial diagnosis
66,66%
33,33%
Positive aortic root dilatation
Negative aortic root dilatation
The occurrence of the aortic dilatation at patients who had not initial aortic dilatation
20%
40%
20%20% Absence of the aortic rootdilatation
Subsequently aortic root dilatation
Aortic dilatation after mitralvalvuloplasty
Aortic dilatation after mitral andaortic valvuloplasty

80%
20%
0%0%
10%20%30%40%50%60%70%80%
Mild aortic rootdilatation
Medium aorticroot dilatation
Severe aorticroot dilatation
Marfan syndrome-initial diagnosis
Marfan syndrome-initial diagnosis
The age of occurrence of mild aortic root dilatation at initial diagnosis
37,50%
50,00%
12,50%
< 3 years
3-7years
>7 years
The age of occurrence of medium aortic root dilatation at initial diagnosis
0,00%
33,33%
66,66%
< 3 years
3-7years
>7 years

Evolution of the aortic root dilatation at children under 3 years old
25%
75%
Mild aortic root dilatation
Medium aortic root dilatation
Evolution of the aortic root dilatation at children aged between 3 to 7 years old
33,33%
66,66%
Mild aortic root dilatation
Medium aortic root dilatation

The progression of medium aortic root dilatation
25%
75%
Progressive medium aortic rootdilatation ( Z score > 3,5)
Stationary medium aortic rootdilatation ( 3<= Z score <= 3,5 )

Initial diagnosis: MVP and MR
60%
40%
0%
40%
60%
0%
0% 20% 40% 60% 80% 100% 120%
Mild mitralregurgitation
Medium mitralregurgitation
Severe mitralregurgitation
Marfan syndrome Control group

33,33%
0%
44,44%
16,66%22,22%
83,33%
0,00%
20,00%
40,00%
60,00%
80,00%
100,00%
< 3 years 3 to 7 years > 7 years
Initial mild mitral regurgitation
Marfan syndrome
Control group
16,66%12,50%
33,33%
50,00%55,55%
0,00%
10,00%
20,00%
30,00%
40,00%
50,00%
60,00%
< 3 years 3 to 7 years > 7 years
Initial medium mitral regurgitation
Marfan syndrome
Control group

33,33%
66,66%
55,55%
33,33%
11,11%16,66%
0,00%
10,00%
20,00%
30,00%
40,00%
50,00%
60,00%
70,00%
Mild mitralregurgitation
Medium mitralregurgitation
Mitralvalvuloplasty
Evolution of the mild mitral regurgitation
Marfan syndrome
Control group
66,66%
20,00%
44,44%
80,00%
0,00%
20,00%
40,00%
60,00%
80,00%
Medium mitral regurgitation Mitral valvuloplasty
Evolution of the medium mitral regurgitation
Marfan syndrome
Control group

0,00%
20,00%
40,00%
60,00%
80,00%
The existence of the arrythmias at the initial diagnosis
Marfan syndrome 26,66% 73,33%
Control group 40% 60%
Present Absent
0,00%
20,00%
40,00%
60,00%
80,00%
The occurence of the arrythmias during the evolution of the disease
Marfan syndrome 63,63% 36,36%
Control group 44% 56%
Present Absent
Contingency table using odds ratio function showed that:
OR=1,20 with 95% Confidence Interval

Type of arrythmia
50%
30%
20%
29%
57%
14%
TPSV
ESV+ESA
BAV
Control group
Marfan syndrome
CONCLUSIONS
1. - Mild aortic root dilatation is more often at children aged between 3 to 7 years old and more than a half
( 66,66%) develop in time medium aortic root dilatation. But a higher percentage( 75%) at developping a medium aortic root dilatation is at children who have less than 3 years old - so the earlier the aortic root dilatation the greater probability of increasing aortic root diameter.
2. - A significant percentage ( 44,44%) of children with Marfan syndrome who have initial mild mitral regurgitation are aged between 3 to 7 years old which leads us to the following:
A: We can notice that at this age group ( 3 to 7 years old) there is a significant number of patients who have both initial mild aortic root dilatation and mitral regurgitation.
B: A comparison with the control group where initial mild mitral regurgitation occurs more oftenly( 83,33%) at children aged more than 7 years.

3. - The comparative study shows a similarity between the
both groups which concerns the age of occurrence of the medium mitral regurgitation: more than 7 years old.
4. - There is a higher percentage ( 55,55%) of children with Marfan syndrome and mild mitral regurgitation at initial diagnosis who develop in time medium mitral regurgitation, than the children from the control group who have less occurrence of the medium mitral regurgitation ( 33,33%).
5. - In what concerns the severe forms of mitral regurgitation (at patients who had initial mild mitral regurgitation) who underwent surgical treatment there is un insignificant percentage difference between the both groups (11,11% Marfan syndrome - 16,66% Group control).
6. - The evolution of the initial medium mitral regurgitation shows that:
- A significant percentage of children with Marfan syndrome ( 66,66%) did not developped severe mitral regurgitation which could have required surgical treatment, in comparison with the control group where 80% of the patients presented at a certain moment severe mitral regurgitation which required surgical treatment.
7. – The value of the Odds Ratio which is 1,200 shows that there is no difference in occurrence of arrythmias between children with Marfan syndrome and children from the control group who have only mitral valve prolapse and mitral regurgitation without any other cardiac pathologies associated.

References
1. Erkula G, Jones KB, Sponseller PD: “Growth and maturation in Marfan syndrome” Am J Med genet 2002;
2. Del Mastro R , Sarfazzi M: “Genetic linkage of the Marfan syndrome, ectopia lentis, and congenital contractural arachnodactyly to the fibrillin genes on chromosomes 15 and 5”;
3. Glesby MJ, Pyeritz RE: “Association of mitral valve prolapse and systemic abnormalities of connective tissues. A phenotypic continuum”;
4. Loeys BL, Chen J: “A syndrome of altered cardiovascular , craniofacial, neurocognitive and skeletal development caused by mutations in TGFBR 1 and TGFBR 2”;
5. www.update.com “Genetics, clinical features, and diagnosis of Marfan syndrome and related disorders”;
6. www.jmg.bmj.com “ The revised Ghent nosology for the Marfan syndrome-2010”