Evidence Supporting Aggressive Glycemic Control. Treatment of Type 2 Diabetes.
49
Evidence Supporting Aggressive Glycemic Control
-
Upload
amie-bruce -
Category
Documents
-
view
223 -
download
2
Transcript of Evidence Supporting Aggressive Glycemic Control. Treatment of Type 2 Diabetes.

Evidence Supporting Aggressive Glycemic
Control

Treatment of Type 2 Diabetes

Sites of Action of Therapeutic Options for
Type 2 Diabetes

DCCT: Effects of Intensive vs Conventional Glycemic Control

UKPDS: Design

UKPDS: Effects of Intensive (Sulfonylurea/Insulin) Treatment

UKPDS: Effects of Intensive (Metformin)
Treatment*

UKPDS: Effects of Glycemia Exposure
Over Time

UKPDS: Risk Reduction in Diabetes-
Related Complications (A1c)

Diabetes Prevention Program: Protocol Design

Diabetes Prevention Program: Reduction in Diabetes Incidence

Structures of Thiazolidinediones

Thiazolidinediones: Mechanism of Insulin
Sensitization

PPAR α vs. gamma
• PPAR α (fibrates) work mostly in the liver and lower VLDL triglycerides and increase HDL-C but do not affect FFA, glucose, or insulin sensitivity
• PPAR gammas (TZDs such as rosiglitazone or pioglitazone) promote new fat cells in subcutaneous tissue and decrease intramuscular and visceral fat.

Thiazolidinediones:Rationale for Type 2 Diabetes
Therapy

ACTOS, an Insulin Sensitizer

Reduced Insulin Resistance Suggested by HOMA Analysis of
Pioglitazone Therapy

Improved β-Cell Response Suggested by HOMA Analysis of
Pioglitazone Therapy

Changes in A1c From Baseline in All Treated Patients

Endpoint Changes in Patients With
Lower Baseline A1c (Mean 9.0%)*

Change in FPG From Baseline in All Treated Patients

Change in Lipid Profile at Endpoint:
ACTOS 26-Week Monotherapy

DREAM Study for Prevention of Diabetes
• 5,269 persons with pre-diabetes randomized to rosiglitazone (8 mg daily) vs. placebo and ramipril vs. placebo for median of 3 years
• 10.6% of those on rosiglitazone progressed to type 2 diabetes vs. 25% on placebo, a 62% risk reduction (p<0.0001).
• Primary endpoint of development of diabetes or death from any cause reduced by 60%
• 51% of those on rosiglitazone vs. 30% on placebo returned to normal blood sugar
• No significant difference in future cardiovascular events, but higher rate of new heart failure in those on rosiglitazone (0.5%) vs. placebo (0.1%). Body weight increased 2.2kg more in the rosiglitazone vs. placebo group.

PROACTIVE Study: Secondary Prevention of Macrovascular Events in Persons with Diabetes
from Pioglitazone 5238 patients with type 2 diabetes who had evidence of
macrovascular disease assigned to oral pioglitazone titrated from 15 mg to 45 mg (n=2605) or matching placebo (n=2633), taken w/existing drugs.
Primary endpoint: combined all-cause mortality, non fatal myocardial infarction (including silent myocardial infarction), stroke, acute coronary syndrome, endovascular or surgical intervention in the coronary or leg arteries, and amputation above the ankle.
Over an average of 34.5 months. 514 of 2605 patients in the pioglitazone group and 572 of 2633 patients in the placebo group achieved the primary endpoint (HR 0.90, 95% CI 0.80-1.02, p=0.095).
Lancet 2005; 366: 1279-89


Cholesterol Treatment Trialists’ (CCT) Collaboration: Efficacy and safety of cholesterol-lowering treatment:
prospective meta-analysis fo data from 90,056 participants in 14 randomized trials of statins
(The Lancet 9/27/05)• Over average 5 year treatment period (per mmol/L
reduction—approx 40 mg/dl in LDL-C):– 12% reduction in all-cause mortality– 19% reduction in coronary mortality– 23% reduction in MI or CHD death– 17% reduction in stroke– 21% reduction in major vascular events– No difference in cancer incidence (RR=1.00).
• Statin therapy can safely reduce 5-year incidence of major coronary events, revascularization, and stroke by about 20% per mmol/L (about 38 mg/dl) reduction in LDL-C

Collaborative Atorvastatin Diabetes Study (CARDS)
• 2838 patients aged 40-75 with type 2 diabetes, no prior CVD, but at least 1 of the following: retinopathy, albuminuria, smoking, or hypertension
• Randomization to 10 mg atorvastatin or placebo• Mean follow-up 3.9 years• Reduction in all CVD events of 37% (p=0.001), all
cause mortality 27% (p=0.059). CHD events reduced 36% and stroke 48%.
Colhoun HM et al., The Lancet 2004; 364: 685-696

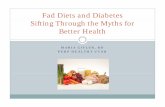
Relative Risk of Events in 4S Study
RR = 0.6895% CI = 0.59-0.79
P <0.001 n = 1631/1606
RR = 0.62 95% CI = 0.46-0.85 P <0.003 n = 335/343
NFG IFG DMRR = 0.58 95% CI = 0.41-0.80P <0.001 n = 232/251
RR = 0.67 95% CI = 0.55-0.80P <0.001 n = 1631/1606
RR = .57 95% CI = 0.37-.87P <0.01 n = 335/343
RR = 0.52 95% CI = 0.32-0.82P <0.005 n = 232/251
RR = 0.72 95% CI = 0.57-0.90P <0.005 n = 1631/1606
RR = 0.57 95% CI = 0.35-0.93 P <0.02 n = 335/343
16.4
7.7 7.312.810.4 13.1
05
10152025
RR = 0.79 95% CI = 0.49-1.27P <0.34 n = 232/251
NFG IFG DM
NFG IFG DM
Patients (%)
CAD Events
Revascularization
Total Mortality
21.1
11.5 10.2 11.616.6 16.7
05
10152025
Patients (%)
30.437.5
18.6 19.523.526.2
010203040
Patients (%)
Placebo Simvastatin

Reduction in CHD Event Rates With Statin Treatment (WOSCOPS)
Sattar N, et al. Circulation. 2003;108:414-419
10.4
6.2
7.7
4.4
0
2
4
6
8
10
12
CH
D e
ven
t ra
te (
%)
Patients WithMetabolic Syndrome
Patients WithoutMetabolic Syndrome
PlaceboPravastatin

Are LDL and HDL Effects Additive?
R2 = 0.8512
0
20
40
60
80
100
0 10 20 30 40 50 60 70 80
% Absolute Change in LDL+HDL
% C
V E
ven
t R
RR
HATS
FATS
FATS F/U
4SVA HIT DAIS
BIP
AFCAPS/TexCAPS
WOSCOPS
LIPIDCARE, HPS
HHS
CDP
ASCOT
ALLHAT
PROSPER
2nd Order Relationship

Hypertension Optimal Treatment (HOT): Outcomes in Patients
With Diabetes

UKPDS: Effects of Tight vs Less-Tight Blood Pressure
Control

Most CHD Events May be Preventable by Control of Blood Pressure, HDL-C, LDL-C to “Optimal” Levels
in Persons with the Metabolic Syndrome (Wong et al., Am J Cardiol 2003; 91: 1421-26)
28.2
51.2 50.646.2
38.1
80.5 82.1
45.1
0
10
20
30
40
50
60
70
80
90
Men Women
Pro
po
rtio
n o
f C
HD
Ev
en
ts P
rev
en
ted
(P
AR
%)
BP only HDL-C only LDL-C only All 3 factors
***
* p<0.05, ** p<0.01 compared to men

The endocannabinoid system
• An endogenous signaling system which contributes to physiologic regulation of energy balance, food intake, and lipid and glucose metabolism through both central and peripheral effects




Effects of cannabinoid-1 receptor blocker rimonabant on weight reduction and
cardiovascular risk factors over 1 year: RIO Europe Study
• 1,507 pts with BMI >=30 or >27 with dyslipidemia and/or hypertension randomized to placebo, 5mg or 20 mg rimonabant, w/hypocaloric diet
• Weight loss at 1 year: -3.4 kg w/5mg, -6.6 kg w/10 mg rimonabant vs. placebo (-1.8 kg)
• Rimonabant 20 mg produced greater improvements in waist circumference, HDL-C, triglycerides, LDL-C, insulin, and prevalence of metabolic syndrome (reduced by 34% w/placebo vs. 64.8% with rimonabant)
Van Gaal LF, et al. Lancet 2005; 365: 1389-97



Metabolic Syndrome: Lifestyle Management
• Obesity / weight management: low fat – high fiber diet resulting in 500-1000 calorie reduction per day to provide a 7-10% reduction on body weight over 6-12 mos, ideal goal BMI <25
• Physical activity: at least 30, pref. 60 min moderate intensity on most or all days of the week as appropriate to individual
• Nutritional recommendations per ATP III guidelines: low intake of saturated fats, trans fats, and cholesterol, reduced consumption of simple sugars, and increased intakes of fruits, vegetables, and whole grains are reasonable
Grundy SM, Hansen B, Smith SC, et al. Clinical management of metabolic syndrome. Report of the American Heart Association / National Heart, Lung, and Blood Institute / American Diabetes Association Conference on Scientific Issues Related to Management. Circulation 2004; 109: 551-556



Therapeutic Lifestyle ChangesNutrient Composition of TLC Diet
Nutrient Recommended Intake
• Saturated fat Less than 7% of total calories
• Polyunsaturated fat Up to 10% of total calories
• Monounsaturated fat Up to 20% of total calories
• Total fat 25–35% of total calories
• Carbohydrate 50–60% of total calories
• Fiber 20–30 grams per day
• Protein Approximately 15% of total calories
• Cholesterol Less than 200 mg/day
• Total calories (energy) Balance energy intake and expenditure to maintain desirable body weight/
prevent weight gain

Effect of Mediterranean-style diet in the metabolic syndrome
• 180 pts with metabolic syndrome randomized to Mediterranean-style vs. prudent diet for 2 years
• Those in intervention group lost more weight (-4kg) than those in the control group (+0.6kg) (p<0.01), and significant reductions in CRP and Il-6.
• After 2 years, 40 pts in intervention group still had features of metabolic syndrome compared to 78 pts in the control group
Esposito K et al. JAMA 2004; 292(12): 1440-6.

Therapeutic Goals and Recommendations for Clinical Management of Metabolic Syndrome (Grundy et al.
Circulation 2005; 112 (epub) Oct 18)Dyslipidemia
LDL-C, HDL-C, TG, non-HDL-C
Elevated Blood Pressure
Elevated Glucose
Prothrombotic and Proinflammatory States

ABC’s of Metabolic Syndrome Management
Intervention Goals / Treatment
A Antiplatelet agent Treat all high-risk patients with low-dose aspirin (or clopidogrel in those with CVD if aspirin is contraindicated) and consider low-dose aspirin in moderately high-risk patients.
B BP Control Aim for BP <130/85 mm Hg, or <130/80 mm Hg for type 2 diabetes. Consider ACE-I or ARBs and low dose diuretics in combination rx.

ABC’s of Metabolic Syndrome Management
Intervention
Goals
C Cholesterol Management
LDL-C targets, ATP III guidelines
–High Risk: CHD, CHD risk equivalents (incl. >20% 10-year risk): <100 mg/dL (option <70 mg/dl if CVD present)
– Moderately High Risk (10-20% risk or subclinical disease) 2 RF: <130 mg/dL, option <100 mg/dL
– Moderate Risk (2+ RF, <10%) <130 mg/dL
-- Low Risk: 0-1 RF: <160 mg/dL
Non-HDL-C targets 30 mg/dL higher
HDL-C: >40 mg/dL (men)
>50 mg/dL (women)
TG: <150 mg/dL
Cigarette Smoking
Long term smoking cessation

Goals for Elevated Glucose • For IFG delay progression to type 2 diabetes; for diabetes,
HgbA1c <7.0%• For IFG encourage weight reduction and increased physical
activity• For type 2 diabetes, lifestyle therapy and if necessary,
pharmacologic therapy to achieve near normal HgbA1c <7%; modify other risk factors and behaviors.
• Limited clinical trial data on treatment to reduce CVD events; neither metformin or thiazolidinediones recommended just for prevention of diabetes because cost-effectiveness and long-term safety not yet documented.
Grundy et al. AHA/NHLBI scientific statement on diagnosis and management of metabolic syndrome. Circulation Oct 18, 2005; 112 (e pub)