Evidence profile: urinary incontinence...1 Evidence profile: urinary incontinence ICOPE guidelines...
32
Integrated care for older people (ICOPE) Guidelines on community-level interventions to manage declines in intrinsic capacity Evidence profile: urinary incontinence Scoping question: Do non-pharmacological interventions (prompted voiding, timed voiding, toilet training, habit retraining, pelvic floor muscle training) produce any benefit and/or harm for older people with urinary incontinence? The full ICOPE guidelines and complete set of evidence profiles are available at who.int/ageing/publications/guidelines-icope Painting: “Wet in Wet” by Gusta van der Meer. At 75 years of age, Gusta has an artistic style that is fresh, distinctive and vibrant. A long-time lover of art, she finds that dementia is no barrier to her artistic expression. Appreciated not just for her art but also for the support and encouragement she gives to other artists with dementia, Gusta participates in a weekly art class. Copyright by Gusta van der Meer. All rights reserved
Transcript of Evidence profile: urinary incontinence...1 Evidence profile: urinary incontinence ICOPE guidelines...

Integrated care for older people (ICOPE) Guidelines on community-level interventions to manage declines in intrinsic capacity
Evidence profile: urinary incontinence Scoping question: Do non-pharmacological interventions (prompted voiding, timed voiding, toilet training, habit retraining, pelvic floor muscle training) produce any benefit and/or harm for older people with urinary incontinence? The full ICOPE guidelines and complete set of evidence profiles are available at who.int/ageing/publications/guidelines-icope
Painting: “Wet in Wet” by Gusta van der Meer. At 75 years of age, Gusta has an artistic style that is fresh, distinctive and vibrant. A long-time lover of art, she finds that dementia is no barrier to her artistic expression. Appreciated not just for her art but also for the support and encouragement she gives to other artists with dementia, Gusta participates in a weekly art class. Copyright by Gusta van der Meer. All rights reserved
Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
Contents
Background ........................................................................................................................................................................................................ 1
Part 1: Evidence review ..................................................................................................................................................................................... 2 Scoping question in PICO format (population, intervention, comparison, outcome) .............................................................................................. 2 Search strategy .................................................................................................................................................................................................... 3 List of systematic reviews identified by the search process .................................................................................................................................. 3 PICO table ........................................................................................................................................................................................................... 4 Narrative description of the systematic reviews included in the analysis .............................................................................................................. 5 Brief descriptions of the included non-pharmacological interventions ................................................................................................................... 6 GRADE table 1: Prompted voiding versus no prompted voiding for adults with urinary incontinence ................................................................... 8 GRADE table 2: Pelvic floor muscle training (PFMT) with or without biofeedback plus other interventions versus no active control for older people with urinary incontinence ........................................................................................................................................................................ 10 GRADE table 3: Habit retraining plus others compared with usual care for older people (men and women) with urinary incontinence .............. 12 GRADE table 4: Pelvic floor muscle training (PFMT) compared with no treatment for older women with urinary incontinence ........................... 13 GRADE table 5: Bladder training versus no treatment for older people with urinary incontinence ...................................................................... 15 GRADE table 5.1: Bladder training versus other behavioural interventions for older people with other incontinence .......................................... 16 GRADE table 6: Timed voiding plus other versus usual care for older people with urinary incontinence ............................................................ 17
Part 2: From evidence to recommendations .................................................................................................................................................. 18 Summary of evidence ........................................................................................................................................................................................ 18 Evidence-to-recommendations table .................................................................................................................................................................. 20
Guideline development group recommendation and remarks ..................................................................................................................... 24
References ....................................................................................................................................................................................................... 26
Annex 1: Search strategy ................................................................................................................................................................................ 28
Annex 2: PRISMA 2009 flow diagram for non-pharmacological intervention for managing urinary incontinence .................................. 30
© World Health Organization 2017
Some rights reserved. This work is available under the Creative Commons Attribution-
NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO;
https://creativecommons.org/licenses/by-nc-sa/3.0/igo)

1 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
Background
Urinary incontinence, the involuntary loss of urine, is a highly
prevalent condition in older people aged 60 years and over (1).
The common types of urinary incontinence in older people are
stress incontinence and urge incontinence. Stress incontinence is
the involuntary leaking of urine during efforts or exertion, or while
sneezing or coughing. Urge incontinence, or overactive bladder
syndrome, involves a constellation of symptoms including
frequency, urgency and leakage immediately preceded by urgency.
The prevalence of urinary incontinence reported in population-
based studies ranges from 9.9% to 36.1% (2–4), and is twice as
high in older women as in older men. Urinary incontinence has a
profound impact on the quality of life of older people, their
subjective health status (5, 6), levels of depression (7) and need
for care (8).
Several chronic conditions and environmental factors increase
the risk of urinary incontinence in older people. Chronic diseases
that are associated with urinary incontinence include diabetes
mellitus, Parkinson’s disease, dementia, stroke, prostatic cancer,
chronic obstructive pulmonary disease (COPD) and arthritis.
Environmental factors such as inaccessible or unsafe toilet
facilities, and the absence of caregivers for toileting assistance
are also associated with urinary incontinence. Non-
pharmacological interventions are mostly preferred and remain
the mainstay of urinary incontinence management for patients
with mild urinary incontinence. The primary goal of urinary
incontinence interventions is to improve continence by reducing
the frequency of urinary incontinence episodes. The non-
pharmacological interventions addressed in this guideline include
pelvic floor muscle training (PFMT), bladder training and habit
retraining, and timed or prompted voiding.

2 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
Part 1: Evidence review
Scoping question in PICO format (population,
intervention, comparison, outcome)
Population
• Older people with urgency or stress or mixed urinary incontinence
Interventions
• Prompted voiding
• Timed voiding
• Bladder training
• Habit retraining
• Pelvic floor muscle training (PFMT)
Comparison
• No intervention/usual care
Outcomes
• Critical: Proportion of mean change in frequency of urinary
incontinence, change in mean proportion of hourly checks that are
wet, number of patients with reductions in incidence of daytime
incontinence, number of patients with reductions in incidence of
night-time incontinence, incontinent episodes in 24 hours, mean
urinary incontinence incidence per 24 hours, urinary incontinence
symptoms
• Important: Perceived cure, self-initiated toileting, median percentage
of checks wet, number of incontinent episodes, urinary incontinence
urgency, urinary incontinence frequency, nocturia, quality of life

3 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
Search strategy
A systematic literature search for reviews was conducted in Ovid
MEDLINE, Embase, PsycINFO and Cochrane databases. The
details of the search terms used for retrieving studies are provided
in Annex 1. The search retrieved 188 reviews and 798 randomized
controlled trials (RCTs). After initial screening for eligibility, 111
reviews and 161 RCTs were considered for full-text review.
Ultimately, five systematic reviews that included 25 RCTs and two
additional studies investigating the benefits of non-pharmacological
interventions were included in this review (see Annex 2).
List of systematic reviews identified by the search
process
Included in GRADE1 tables
— Wallace SA, Roe B, Williams K, Palmer M. Bladder training for
urinary incontinence in adults. Cochrane Database Syst Rev.
2004;(1):CD001308. Updated in 2009. [Systematic review was
updated by WHO in 2015] (9)
— Ostaszkiewicz J, Johnston L, Roe B. Habit retraining for the
management of urinary incontinence in adults. Cochrane Database
Syst Rev. 2004;(2):CD002801. Updated in 2009. [Systematic
review was updated by WHO in 2015] (10)
— Eustice S, Roe B, Paterson J. Prompted voiding for the
management of urinary incontinence in adults. Cochrane Database
Syst Rev. 2000;(2):CD002113. Updated in 2006. [Systematic
review was updated by WHO in 2015] (11)
— Ostaszkiewicz J, Johnston L, Roe B. Timed voiding for the
management of urinary incontinence in adults. Cochrane Database
Syst Rev. 2004;(1):CD002802. Updated in 2009. [Systematic
review was updated by WHO in 2015] (12)
— Dumoulin C, Hay-Smith EJC, Mac Habée-Séguin G. Pelvic floor
muscle training versus no treatment, or inactive control treatments,
for urinary incontinence in women. Cochrane Database Syst Rev.
2014;(5):CD005654 (13)
_______________________________ 1 GRADE: Grading of Recommendations Assessment, Development and Evaluation. More information: http://gradeworkinggroup.org

4 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
PICO table
Intervention/
comparison
Outcomes Studies used for GRADE
1 Timed voiding plus others
vs usual care
• Number of patients with reductions in incidence of
daytime urinary incontinence
• Number of patients with reductions in incidence of
night-time incontinence
• Number of patients whose pad test indicates
reduction in the volume of incontinence
Ostaszkiewicz J, Johnston L, Roe B. Timed
voiding for the management of urinary
incontinence in adults. Cochrane Database
Syst Rev. 2004;(1):CD002802. Updated in
2009. (12)
2 Prompted voiding vs no
prompted voiding
• Number of patients with no improvement in urinary
incontinence episodes
• Change in mean proportion of hourly checks that are
wet
• urinary incontinence episodes in 24 hours
• Self-initiated toileting
Eustice S, Roe B, Paterson J. Prompted
voiding for the management of urinary
incontinence in adults. Cochrane Database
Syst Rev. 2000;(2):CD002113. Updated in
2006. (11)
3 Habit retraining plus
others vs usual care
• Number of incontinent episodes
• Incontinent volume
Ostaszkiewicz J, Johnston L, Roe B. Habit
retraining for the management of urinary
incontinence in adults. Cochrane Database
Syst Rev. 2004;(2):CD002801. Updated in
2009. (10)
4 Bladder training vs no
treatment or active
treatment controls
• Cure rate
• Number of micturition episodes
Wallace SA, Roe B, Williams K, Palmer M.
Bladder training for urinary incontinence in
adults. Cochrane Database Syst Rev.
2004;(1):CD001308. Updated in 2009. (9)
(continued next page)

5 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
5 Pelvic floor muscle
training plus bladder
retraining vs control
• Mean urinary incontinence incidence per 24 hours
• Urinary incontinence urgency
• Urinary incontinence frequency
• Nocturia
Dumoulin C, Hay-Smith EJC, Mac Habée-
Séguin G. Pelvic floor muscle training versus
no treatment, or inactive control treatments,
for urinary incontinence in women. Cochrane
Database Syst Rev. 2014;(5):CD005654. (13)
Narrative description of the systematic reviews
included in the analysis
The Cochrane systematic review by Wallace et al. (updated in
2009) aimed to synthesise evidence for effectiveness of bladder
training for urinary incontinence in adults (9). Relevant trials were
identified from the Cochrane Incontinence Review Group’s
specialized register of controlled trials, which contains trials
identified from MEDLINE, the Cumulative Index to Nursing and
Allied Health Literature (CINAHL) and the Cochrane Central
Register of Controlled Trials (CENTRAL). The specialized register
was searched using the Review Group’s own keywords and
medical search terms. The review included 12 RCTs (total of 1473
participants). The participants were predominantly female (75%).
Eight included trials had useable data but only four of them included
older people aged over 60 years. Three of the trials were conducted
in the United States of America and another study is a multicentre
trial that included participants from Denmark, Norway and Sweden.
The Cochrane systematic review by Ostaszkiewicz et al aimed to
investigate the benefit of habit retraining in the management of
urinary incontinence in adults (10). Trials were identified from the
search conducted in the Cochrane Incontinence Review Group’s
specialized register of controlled trials, MEDLINE, Embase,
CINAHL, PsycINFO, Biological Abstracts, Current Contents and the
reference lists of relevant articles. Experts in the field were also
contacted for potential papers. The search included relevant
websites and hand searches of journals and conference
proceedings. Four trials with a total of 378 participants met the
inclusion criteria. Participants in these trials (mean age 80 years)
were mainly women and they were physically and/or cognitively
impaired, dependent on caregivers and residing either in nursing
homes or in their own homes. Three trials tested habit retraining
combined with other treatment, compared with usual care (14–16)
and another trial compared the combination treatment with habit
retraining alone (17).
The Cochrane systematic review by Eustice et al. (updated in 2006)
aimed mainly to examine the effectiveness of prompted voiding in
the management of urinary incontinence in adults (11). The search
for trials was conducted in the Cochrane Incontinence Review
Group’s specialized register of controlled trials (31 January 2006)
as well as the reference lists of relevant articles. Investigators in the
field were also contacted for additional studies. As a result, nine
trials with a total 674 participants (mean age 84 years) were
included in the review. The majority of participants included in the
trials were older women. Prompted voiding was compared with no
(continued next page)

6 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
prompted voiding in nine trials. One trial was excluded as the ages
of the trial participants were not reported (18).
Ostaszkiewicz et al. (updated in 2009) is a Cochrane systematic
review on timed voiding for the management of urinary incontinence
in adults (12). The search for trials was conducted in Cochrane
Incontinence Review Group’s specialized register of controlled trials
(searched 2 April 2009), MEDLINE (January 1966 to November
2003), Embase (January 1980 to Week 18 2002), CINAHL (January
1982 to February 2001), PsycINFO (January 1972 to August 2002),
Biological Abstracts (January 1980 to December 2000), Current
Contents (January 1993 to December 2001) and the reference lists
of relevant articles. Experts in the field were contacted for potential
studies. The search included relevant websites and conference
proceedings. Hand searches were also conducted in relevant
journals. Two trials with a total of 298 participants met the inclusion
criteria (19, 20). Both compared timed voiding plus additional
intervention with usual care. Most of the participants from the two
selected trials were cognitively impaired elderly women (mean age
86.7 years) and all resided in facilities that provided nursing care.
The majority of participants (82%) in one study were older
women (19) while the other study did not report the sex of
participants (20).
Dumoulin et al. is a Cochrane systematic review of pelvic floor
muscle training (PFMT) versus no treatment, or inactive control
treatments, for urinary incontinence in women (13). The search for
relevant trials was conducted in the Cochrane Incontinence Review
Group’s specialized register of controlled trials, which contains trials
identified from CENTRAL (1999 onwards), MEDLINE (1966
onwards) and MEDLINE In-Process (2001 onwards). Conference
proceedings were searched (15 April 2013), and hand searches
were done in the journals and reference lists of relevant articles to
identify potential studies. Twenty-one trials involving 1281 women
(665 PFMT, 616 controls) met the inclusion criteria. Seven of them
recruited older people aged over 60 years or had mean participant
age of more than 60 years (21–27).
Two additional RCTs, not listed in the above-mentioned Cochrane
systematic reviews, were identified in an independent literature
search and were also included (28, 29).
Brief descriptions of the included non-
pharmacological interventions
Prompted voiding is administered for older people with or without
cognitive impairment to initiate their own toileting through requests
for help, and includes the use of positive reinforcement from carers
when they do this. This is distinct from some other therapies
because of the participation of the individual in the process. In
contrast, habit retraining attempts to determine the micturition
pattern for an individual, which can be used to achieve continence
but does not necessarily rely on the individual’s participation.
Timed voiding is fixed by time or event, and is carer led and is not
an individualized intervention. Bladder training actively includes the
individual in attempting to increase the interval between the desire
to void and the actual void, and hence would not be suitable for
those who are cognitively impaired. It comprises three components:
(a) patient education – information about the bladder and how
continence is usually maintained; (b) scheduled voiding – a
“timetable for voiding” which may be fixed or flexible to suit the
participant’s rate of increase in the interval between voids (the aim
is usually to achieve an interval of 3–4 hours between voids); and
(c) positive reinforcement – psychological support and
(continued next page)

7 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
encouragement is generally considered important and is usually
provided by a health care professional. Pelvic floor muscle training
(PFMT) is an exercise programme of repeated pelvic floor muscle
contractions taught and supervised by a health care professional, at
times combined with bladder training for individuals with mixed
urinary incontinence.
Other physical exercise interventions – such as
functional incidental training, mobility and toileting training – focus
on improving the ability of older people to reach the toilet or
developing related skills (e.g. getting up from bed or a chair,
walking 5 metres, undoing clothing hooks, zippers and buttons,
letting down the garment, sitting down on the toilet, rising up from
the toilet seat and adjusting the garment) to improve toilet timing.
Functional incidental training combines prompted voiding with
functionally oriented, low-intensity endurance exercises (e.g. timed
sit-to-stands, walking or wheelchair mobility) and strengthening
exercises (e.g. bicep curls, straight-arm raises, knee extensions
and hip abductions and flexions).
Treatment adherence. There is limited evidence on adherence to
non-pharmacological treatments. Adherence reported in four
included RCTs ranges from 72% to 89% (30–33).
Adverse events. The included trials neither performed explicit
assessment for adverse events nor reported any major risks.
8 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
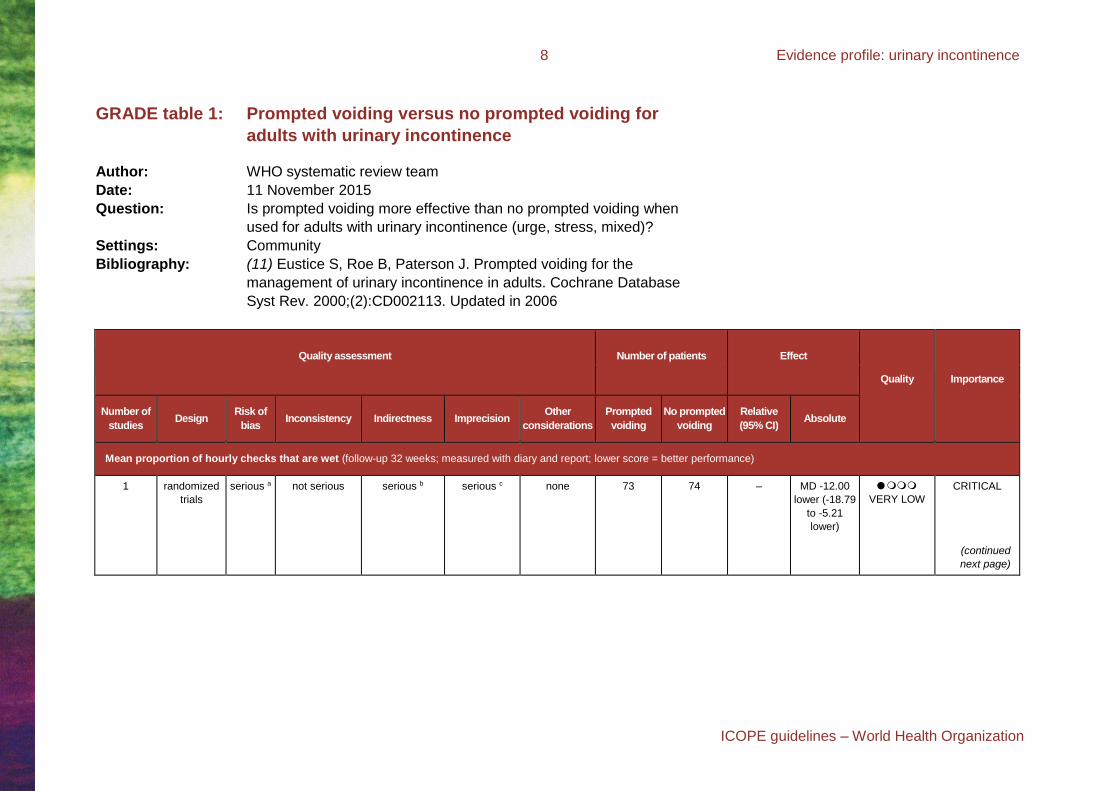
GRADE table 1: Prompted voiding versus no prompted voiding for
adults with urinary incontinence
Author: WHO systematic review team
Date: 11 November 2015
Question: Is prompted voiding more effective than no prompted voiding when
used for adults with urinary incontinence (urge, stress, mixed)?
Settings: Community
Bibliography: (11) Eustice S, Roe B, Paterson J. Prompted voiding for the
management of urinary incontinence in adults. Cochrane Database
Syst Rev. 2000;(2):CD002113. Updated in 2006
Quality assessment Number of patients Effect
Quality Importance
Number of
studies Design
Risk of
bias Inconsistency Indirectness Imprecision
Other
considerations
Prompted
voiding
No prompted
voiding
Relative
(95% CI) Absolute
Mean proportion of hourly checks that are wet (follow-up 32 weeks; measured with diary and report; lower score = better performance)
1 randomized
trials
serious a not serious serious b serious c none 73 74 – MD -12.00
lower (-18.79
to -5.21
lower)
VERY LOW
CRITICAL
(continued
next page)

9 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
Change in mean proportion of hourly checks that are wet (follow-up 8 weeks; measured with diary and self-report; lower score = better performance)
1 randomized
trials
serious d no serious
imprecision
no serious
indirectness
very serious e none 9 10 – MD 17.60
higher (-14.58
lower to 49.78
higher)
VERY LOW
CRITICAL
Number of incontinent episodes in 24 hours (follow-up 3–13 weeks; measured with diary and self-report; lower score = better performance)
2 randomized
trials
serious f serious g serious h no serious
imprecision
none 127 130 – MD –0.92
lower (-1.32-
to –0.53
lower)
VERY LOW
CRITICAL
Self-initiated toileting (follow-up 3 weeks; measured with self-report; lower score = better performance)
1 randomized
trials
serious i no serious
imprecision
serious j serious k none 63 63 – MD –1.90
lower (-2.29
to -1.51
lower)
LOW
IMPORTANT
CI: confidence interval; MD: mean difference a. Risk of bias: Downgraded once as allocation concealment was unclear in one trial. b. Indirectness: Downgraded once as trial was conducted in nursing home setting, and generalizing the evidence to other settings is doubtful. c. Imprecision: Downgraded once as sample size was small (smaller than 200). d. Risk of bias: Downgraded once as method applied for allocation concealment was unclear. e. Imprecision: Downgraded twice as sample size was very small (smaller than 50). f. Risk of bias: Downgraded once as allocation concealment method was unclear in two trials. g. Inconsistency: Downgraded once as considerable heterogeneity was observed: Chi2 = 18.07, df = 1 (P = 0.00002); I2 = 94%. h. Indirectness: Downgraded once as included trials were conducted in nursing home settings and generalizing the interventions to other settings is doubtful. i. Risk of bias: Downgraded once as allocation concealment was unclear. j. Indirectness: Downgraded once as trial was conducted in nursing home setting and generalizing the interventions to other settings is doubtful. k. Imprecision: Downgraded once as sample size was small (smaller than 200).

10 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
GRADE table 2: Pelvic floor muscle training (PFMT) with or without biofeedback plus
other interventions versus no active control for older people with
urinary incontinence
Author: WHO systematic review team
Date: 11 November 2015
Question: Is multicomponent behavioural interventions (PFMT with or without biofeedback, bladder
control strategy, education and self-monitoring) more effective than no active control when
used for older people (women and men) with urinary incontinence?
Setting: Community
Bibliography: (34) McFall SL, Yerkes AM, Cowan LD. Outcomes of a small group educational
intervention for urinary incontinence: episodes of incontinence and other urinary
symptoms. J Aging Health. 2000;12(2):250–67.
(21) Burgio KL, Locher JL, Goode PS, Hardin JM, McDowell BJ, Dombrowski M et al.
Behavioral vs drug treatment for urge urinary incontinence in older women: a
randomized controlled trial. JAMA. 1998;280(23):1995–2000.
(35) Goode PS, Burgio KL, Locher JL, Umlauf MG, Lloyd LK, Roth DL. Urodynamic
changes associated with behavioral and drug treatment of urge incontinence in older
women. J Am Geriatr Soc. 2002;50(5):808–16.
(36) Subak LL, Quesenberry CP, Posner SF, Cattolica E, Soghikian K. The effect of
behavioral therapy on urinary incontinence: a randomized controlled trial. Obstet
Gynecol. 2002;100(1):72–8.
(37) Dougherty MC, Dwyer JW, Pendergast JF, Boyington AR, Tomlinson BU, Coward
RT et al. A randomized trial of behavioral management for continence with older rural
women. Res Nurs Health. 2002;25(1):3–13.
(38) Johnson TM, Burgio KL, Redden DT, Wright KC, Goode PS. Effects of behavioral
and drug therapy on nocturia in older incontinent women. J Am Geriatr Soc.
2005;53(5):846–50.
(continued next page)

11 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
Quality assessment Number of patients Effect
Quality Importance Number
of
studies
Design Risk of
bias Inconsistency Indirectness Imprecision
Other
considerations
Multicomponent
behavioural
interventions (PFMT
with or without
biofeedback plus
bladder control
strategy and self-
monitoring)
No active
control
Relative
(95% CI) Absolute
Total number of incontinent episodes per week (post treatment) (follow-up 6–24 weeks; assessed with bladder diary; lower score = better performance)
5 randomized
trials
serious a no serious
inconsistency
no serious
indirectness
no serious
imprecision
none 382 327 – WMD -3.63
lower (-5.19
to -0.99
lower)
MODERATE
CRITICAL
Patients’ perception of improvement in urinary incontinence (follow-up 6–8 weeks; assessed with self-report and bladder diary; improvement was
defined as self-reported improvement or no restriction in daily activities)
3 randomized
trials
serious b no serious
inconsistency
no serious
indirectness
no serious
imprecision
none 165/234
(70.5%)
65/174
(37.4%) RR 4.15
(2.70 to 6.37)
339 more per
1000 (from
243 more to
418 more)
MODERATE
IMPORTANT
CI: confidence interval; RR: relative risk; WMD: weighted mean difference a. Risk of bias: Downgraded once as method applied for allocation concealment was unclear in all five included trials b. Risk of bias: Downgraded once as method applied for allocation concealment was not clear in all three included trials.

12 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
GRADE table 3: Habit retraining plus others compared with usual care for older
people (men and women) with urinary incontinence
Author: WHO systematic review team
Date: 11 November 2015
Question: Is habit retraining plus others more effective than usual care when used for older
people (men and women) with urinary incontinence?
Setting: Community
Bibliography: (10) Ostaszkiewicz J, Johnston L, Roe B. Habit retraining for the management of
urinary incontinence in adults. Cochrane Database Syst Rev. 2004;(2):
CD002801. Updated in 2009. [Systematic review was updated by WHO in 2015].
Quality assessment Number of patients Effect
Quality Importance
Number
of
studies
Design Risk of
bias Inconsistency Indirectness Imprecision
Other
considerations
Habit retraining
plus other
Usual
care
Relative
(95% CI) Absolute
Number of incontinent episodes (follow-up 6–36 weeks; assessed with bladder diary; lower score = better performance)
2 randomized
trials
serious a no serious
inconsistency
no serious
indirectness
serious b none 76 54 – SMD 0.12
lower (0.47
lower to 0.23
higher)
LOW
CRITICAL
CI: confidence interval; MD: mean difference a. Risk of bias: Downgraded once as allocation concealment was unclear in one of the included trial. b. Imprecision: Downgraded once as sample size was small (smaller than 200).

13 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
GRADE table 4: Pelvic floor muscle training (PFMT) compared with no treatment for
older women with urinary incontinence
Author: WHO systematic review team
Date: 11 November 2015
Question: Is PFMT more effective than no treatment or placebo when used for older women with
urinary incontinence?
Settings: Primary care or community
Bibliography: (13) Dumoulin C, Hay-Smith EJC, Mac Habée-Séguin G. Pelvic floor muscle training
versus no treatment, or inactive control treatments, for urinary incontinence in women.
Cochrane Database Syst Rev. 2014;(5):CD005654.
Quality assessment Number of patients Effect
Quality Importance
Number of
studies Design
Risk of
bias Inconsistency Indirectness Imprecision
Other
considerations
Pelvic floor
muscle
training
No treatment
or education
Relative
(95% CI) Absolute
Participant perceived cure (all types of urinary incontinence) (follow-up 12 weeks; assessed with self-reported information)
3 randomized
trials
serious a serious b no serious
indirectness
no serious
imprecision
none 50/144
(34.7%)
9/146
(6.2%)
RR 5.34 (2.78
to 10.26)
268 more per
1000 (from 110
more to 571
more)
LOW
IMPORTANT
Quality of life (follow-up 6 weeks; measured with King’s Health Questionnaire (KHQ)/severity measure after treatment; lower score = better performance)
1 randomized
trials
serious c not serious
applicable
no serious
indirectness
very serious d none 30 15 – MD -24.92
lower (-39.06
lower to -10.78
lower)
VERY LOW
IMPORTANT
(continued
next page)

14 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
Urinary incontinence symptoms (follow-up 6 weeks; measured with: King’s health questionnaire; Better indicated by lower values)
2 randomized
trials
serious e not serious no serious
indirectness
very serious d none 30 30 – MD -34.16
lower
(-47.45 lower
to -20.88 lower)
VERY LOW
CRITICAL
CI: confidence interval; MD: mean difference; RR: relative risk. a. Risk of bias: Downgraded once as allocation concealment method and procedure for masking outcome assessor was unclear in one trial. b. Inconsistency: Downgraded once as moderate heterogeneity was observed: Chi2 = 7.56, df = 2 (P = 0.02); I2 = 74%. c. Risk of bias: Downgraded once as outcome assessor was not masked and method applied for allocation concealment was unclear. d. Imprecision: Downgraded twice as sample size was very small (smaller than 100). e. Risk of bias: Downgraded once as allocation concealment method was unclear in one trial.

15 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
GRADE table 5: Bladder training versus no treatment for older people with
urinary incontinence
Author: WHO systematic review team
Date: 11 November 2015
Question: Is bladder training more effective than no treatment, placebo or control when
used for older people (male and female) with urinary incontinence?
Settings: Community
Bibliography: (9) Wallace SA, Roe B, Williams K, Palmer M. Bladder training for urinary
incontinence in adults. Cochrane Database Syst Rev. 2004;(1):CD001308.
Updated in 2009. [Systematic review was updated by WHO in 2015]
Quality assessment Number of patients Effect
Quality Importance
Number of
studies Design
Risk of
bias Inconsistency Indirectness Imprecision
Other
considerations
Bladder
training
No treatment
control
Relative
(95% CI) Absolute
Cure of incontinent episodes (follow-up 6 weeks; assessed with diary, number of participants cured, immediately after treatment)
1 randomized
trials
serious a not serious no serious
indirectness
serious b none 7/60
(11.7%)
2/63
(3.2%)
RR 3.68
(0.79 to
16.99)
85 more per
1000 (from 7
fewer to 508
more)
LOW
CRITICAL
Number of micturition episodes per week (daytime) (follow-up 6 weeks; assessed with diary immediately after the treatment phase; lower score = better performance)
1 randomized
trials
serious c not serious no serious
indirectness
very serious d none 45 43 – MD -0.31
lower (-0.73
lower to 0.11
higher)
VERY
LOW
IMPORTANT
CI: confidence interval; MD: mean difference; RR: relative risk. a. Risk of bias: Downgraded once as method applied for allocation concealment was unclear. b. Imprecision: Downgraded once as sample size was small (smaller than 200). c. Risk of bias: Downgraded once as information on incomplete data not described adequately. d. Imprecision: Downgraded twice as sample size was very small (smaller than 100).

16 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
GRADE table 5.1: Bladder training versus other behavioural interventions for
older people with other incontinence
Author: WHO systematic review team
Date: 11 November 2015
Question: Is bladder training more effective than other behavioural, physical,
psychological treatments when used for older people with other incontinence?
Settings: Primary care or community
Bibliography: (9) Wallace SA, Roe B, Williams K, Palmer M. Bladder training for urinary
incontinence in adults. Cochrane Database Syst Rev. 2004;(1):CD001308.
Updated in 2009. [Systematic review was updated by WHO in 2015]
Quality assessment Number of patients Effect
Quality Importance
Number of
studies Design Risk of bias Inconsistency Indirectness Imprecision
Other
considerations
Bladder
training
Other behavioural,
physical,
psychological
treatment
Relative
(95% CI) Absolute
Participant’s perception of improvement: improved, cured vs unchanged, worse; minimum of 2 months post-treatment (follow-up 12 weeks)
1 randomized
trials
serious a not serious no serious
indirectness
serious b none 37/60
(61.7%)
45/60
(75%)
RR 0.88
(0.68 to 1.13)
90 fewer
per 1000
(from 240
fewer to 97
more)
LOW
IMPORTANT
CI: confidence interval; RR: relative risk. a. Risk of bias: Downgraded once as outcome assessor was not masking in the trial and incomplete data was not managed adequately. b. Imprecision: Downgraded once as sample size was smaller than 200.

17 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
GRADE table 6: Timed voiding plus other versus usual care for older people with
urinary incontinence
Author: WHO systematic review team
Date: 11 November 2015
Question: Is timed voiding plus other more effective than usual care when used for older
people (men and women) with urinary incontinence?
Settings: Primary care or community
Bibliography: (12) Ostaszkiewicz J, Johnston L, Roe B. Timed voiding for the management of
urinary incontinence in adults. Cochrane Database Syst Rev. 2004;(1):CD002802.
Updated in 2009. [Systematic review updated by WHO in 2015]
Quality assessment Number of patients Effect
Quality Importance
Number of
studies Design
Risk of
bias Inconsistency Indirectness Imprecision
Other
considerations
Timed
voiding plus
other
Usual care Relative
(95% CI) Absolute
Number of patients with reductions in incidence of daytime incontinence (follow-up 8 weeks)
1 randomized
trials
serious a not serious serious b serious 4 none 40/120
(33.3%)
26/89
(29.2%)
RR 1.34 (0.9
to 2.01)
99 more per
1000 (from
29 fewer to
295 more)
VERY LOW
CRITICAL
Number of patients with reductions in incidence of night-time incontinence (follow-up 8 weeks)
1 randomized
trials a
serious c not serious serious b serious d none 39/95
(41.1%)
18/79
(22.8%)
RR 1.80
(1.12 to 2.89)
182 more
per 1000
(from 27
more to 431
more)
VERY LOW
CRITICAL
CI: confidence interval; RR: relative risk
a. Risk of bias: Downgraded once as trial method was quasi-experimental design.
b. Indirectness: Downgraded once as trial was conducted in nursing home settings in high income country and generalizing the evidence to other settings is doubtful.
c. Risk of bias: Downgraded once as allocation concealment method and procedure for masking of outcome assessor was unclear in the trial.
d. Imprecision: Downgraded once as sample size was small.

18 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
Part 2: From evidence to recommendations
Summary of evidence
Outcome Effect size
Prompted voiding
vs no promoted
voiding
Habit retraining
plus other vs
usual care
Pelvic-floor
muscle training
(PFMT) with or
without
biofeedback,
bladder
retraining and
self-monitoring
vs control
PFMT vs no
treatment,
placebo,
controls
Bladder training
vs no treatment
control
Timed voiding vs
usual care
GRADE table 1
Eustace et al. (11)
Mean proportion of
hourly checks that are
wet
MD -12 lower
(-18.79 lower to -5.21
lower)
Favours treatment
VERY LOW
Change in mean
proportion of hourly
checks that are wet
MD -17.60 higher
(-14.58 lower to 49.78
higher)
VERY LOW
Total number of urinary
incontinence episodes
MD -0.92 lower
(-1.32 lower to -0.53
lower)
Favours treatment
VERY LOW
SMD -0.12 lower
(-0.47 lower to
0.23 higher)
LOW
WMD -3.63 lower
(-5.19 lower
to -0.99 lower)
Favours treatment
MODERATE
(continued next page)

19 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
Self-initiated toileting MD -1.9 lower
(-2.29 lower to -1.51
lower)
Favours treatment
LOW
GRADE table 5
Wallace et al. (9)
Patients’ perception of
improvement in urinary
incontinence
RR 4.15
(2.70 to 6.37)
Favours treatment
MODERATE
RR 0.88
(0.68 to 1.13)
LOW
Cure of incontinent
episodes
RR 3.68
(0.79 to 16.99)
LOW
Number of micturition per
week (daytime)
MD -0.31 lower
(-0.73 lower to 0.11
higher)
VERY LOW
GRADE table 6
Ostaszkiewicz et al. (12)
Number of patients with
reductions in incidence
of daytime incontinence
RR 1.34
(0.90 to 2.01)
VERY LOW
Number of patients with
reductions in incidence
of nighttime incontinence
RR 1.80
(1.12 to 2.89)
Favours treatment
VERY LOW
GRADE table 4 Dumoulin et al. (13)
Participant perceived cure
RR 5.34
(2.78 to 10.26)
Favours treatment
LOW
(continued next page)

20 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
Urinary incontinence symptoms
MD -34.16 lower
(-47.45 to -20.88
lower)
Favours treatment
VERY LOW
Quality of life
MD -24.92 lower
(-39.06 lower
to -10.78 lower)
Favours treatment
VERY LOW
Evidence-to-recommendations table
Problem Explanation
Is the problem a priority?
Yes No Uncertain
✓
The prevalence of urinary incontinence reported in population-based studies ranges from 9.9%
to 36.1%, and is twice as high in older women as in older men. Urinary incontinence has a
profound impact on the quality of life of older people, their subjective health status, levels of
depression and need for care.
Benefits and harms Explanation
Do the desirable effects outweigh the
undesirable effects?
Yes No Uncertain
✓
No studies reported harm associated with non-pharmacological management of urinary
incontinence.
There is limited low-quality evidence which suggests that prompted voiding may benefit older
people in managing urinary incontinence. Eight trials included in this analysis investigated the
benefit of prompted voiding compared with no prompted voiding for older people with urinary
incontinence. All of the analysed trials were conducted in the United States. Seven of the eight
studies were carried out in nursing home settings. The duration of the interventions ranged from
(continued next page)
21 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
(continued from previous page)
Do the desirable effects outweigh the
undesirable effects?
Yes No Uncertain
✓
20 days to 32 weeks. Two trials reported the effectiveness of prompted voiding in terms of
reducing the number of urinary incontinence episodes in 24 hours. Both Hu et al. (39) and
Schnelle et al. (40) found a reduction in the number of incontinent episodes per day in the
prompted voiding group. The pooled result was statistically significant (weighted mean
difference [WMD]: -0.92, CI: 95% -1.32 to -0.53). Two other trials reported a similar outcome,
but could not be included in the meta-analysis. One of them reported a substantial reduction in
the number of incontinent episodes (60% lower) in the treatment group compared with the
control group (37%). Another trial found a significant decrease in incontinence, falling from 80%
to 20%, in the treatment group, whereas the control group remained almost the same.
There is adequate moderate-quality evidence suggesting that pelvic floor muscle training
(PFMT) combined with bladder training benefits older women to manage urinary incontinence.
Six randomized controlled trials (RCTs), with a total of 1132 participants, investigated the
benefit of PFMT combined with bladder training with or without biofeedback. All six RCTs
recruited older people living in the community; five of them recruited older people aged over 55
years, while in the other trial, participants were aged 65 years and over. The intervention was
delivered at home or in clinical settings. The mean age of the study participants ranged from
65.4 to 74.7 years. In one trial, nearly 34% of study participants were older men; all other
studies only recruited older women.
Three of the six trials tested PFMT with biofeedback and a bladder control strategy with or
without self-monitoring. One RCT examined PFMT without biofeedback, bladder training or self-
monitoring. Two other RCTs combined PFMT with other behavioural interventions: one used a
group education approach consisting of bladder training, a strategy to manage the urge to
urinate, and group support for PFMT, while the other trial administered PFMT and bladder
training with individualized voiding schedules. Apart from one trial that offered a self-help
booklet to the control group, the control groups in all the other trials received no active
intervention.
Five of the analysed trials reported outcome data on the number of incontinence episodes per
week. The overall pooled effect of PFMT plus bladder training, with or without biofeedback, was
(continued next page)

22 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
(continued from previous page)
Do the desirable effects outweigh the
undesirable effects?
Yes No Uncertain
✓
WMD: -3.63 (-5.19 to -0.99 lower), favouring the treatment (P < 0.001). Three trials reported
data on participants’ perception of improvement in urinary incontinence. The pooled estimate for
this outcome was relative risk [RR]: 4.14 (95% CI: 2.70 to 6.37) in favour of the treatment group.
No trial has reported adverse effects, and the guideline development group guideline
development group believed that the potential for harm is likely to be minimal.
Values and preferences/ acceptability Explanation
Is there important uncertainty or
variability about how much people value
the options?
Major
variability
Minor
variability
Uncertain
✓
Urinary incontinence in older people is associated with significant societal cost, and it impacts
older people and family caregivers profoundly. The magnitude of the problem is larger in low-
and middle-income countries (LMICs): 9% to 36% of older people suffer from urinary
incontinence. The majority of them receive care from a close family member, who may be at risk
of caregiver strain and burden.
Is the option acceptable to key
stakeholders?
Major
variability
Minor
variability
Uncertain
✓
Although there is an absence of evidence from low- and middle-income countries, the evidence
reported in high-income countries indicates that non-pharmacological interventions may be
acceptable to older people in low-resource settings.
(continued next page)

23 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
Feasibility/resource use Explanation
How large are the resource
requirements?
Major Minor Uncertain
✓
Non-pharmacological interventions recommended for urinary incontinence are not resource
intensive.
Is the option feasible to implement?
Yes No Uncertain
✓
The feasibility of these interventions is not an important limitation; these interventions can be
safely administered by family caregivers. Delivery of care through non-specialist health workers
seems to be a successful model for low- and middle-income countries. Delivering an
educational intervention has been shown to be feasible and to have promising results. Drawing
on these experiences, the guideline development group believed the recommendation was
feasible to implement in high- and low-resource settings.
Equity Explanation
Would the option improve equity in
health?
Yes No Uncertain
✓
The guideline development group strongly believed that this recommendation would increase
equity in health.

24 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
Guideline development group recommendation and remarks
Recommendation
Prompted voiding for the management of urinary incontinence can be offered for older
people with cognitive impairment.
Strength of the recommendation: Conditional
Quality of evidence: Very low
Pelvic floor muscle training (PFMT), alone or combined with bladder control strategies
and self-monitoring, should be recommended for older women with urinary
incontinence (urge, stress or mixed).
Strength of the recommendation: Strong
Quality of evidence: Moderate
Remarks
• Apart from one study, all of the trials were conducted in high-income countries.
• Although the majority of PFMT trials involved older women, the recommendation for
PFMT may be applicable to older men.
• The duration of the PFMT intervention trials ranged from 6 to 12 weeks and most of the
trials administered the interventions on a daily regimen.
• Using continence products should be considered for older people who are bedridden or
experiencing severe declines in mental and/or physical capacities.
• Health care providers should take a detailed history and ask specific questions about
urinary incontinence, such as the time of onset, symptoms and frequency.
(continued next page)

25 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
• At least half of women with urinary incontinence do not report this issue to their general
practitioner; therefore, health care professionals should routinely check for urinary
incontinence in older women and men.
• Identifying and managing conditions that may cause urinary incontinence, including
urinary tract infections, metabolic disorders, excess fluid intake and impaired mental
conditions (e.g. delirium), are important and should not be neglected.
• Clinicians should review current medications that may cause or worsen urinary
incontinence.
• Although pharmacological therapy can reduce urinary incontinence and even provide
complete continence, many older people discontinue medication because of adverse
effects. Specialist care providers should be consulted when initiating pharmacological
treatment.
• As a first-line treatment, provide advice on bladder training for a minimum of six weeks.
Bladder training involves advising the older people to follow a strict schedule for bathroom
visits. The schedule starts with bathroom visits every 2 hours, but the time between visits
should be gradually increased to improve bladder control.

26 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
References
1. Ageing and health: a health promotion approach for developing countries. Manila: World Health Organization (WHO) Regional Office for the Western Pacific; 2003 (http://www.wpro.who.int/publications/pub_9290610662/en/, accessed 26 July 2017).
2. Prince M, Acosta D, Ferri CP, Guerra M, Huang Y, Jacob KS et al. The association between common physical impairments and dementia in low and middle income countries, and, among people with dementia, their association with cognitive function and disability. A 10/66 Dementia Research Group population-based study. Int J Geriat Psychiatr. 2011;26(5):511–9.
3. Sims J, Browning C, Lundgren-Lindquist B, Kendig H. Urinary incontinence in a community sample of older adults: prevalence and impact on quality of life. Disabil Rehabil. 2011;33(15–16):1389–98.
4. Smith AL, Wang PC, Anger JT, Mangione CM, Trejo L, Rodriguez LV et al. Correlates of urinary incontinence in community-dwelling older Latinos. J Am Geriatr Soc. 2010;58(6):1170–6.
5. Tamanini JTN, Santos JLF, Lebrão ML, Duarte YAO, Laurenti R. Association between urinary incontinence in elderly patients and caregiver burden in the city of Sao Paulo/Brazil: Health, Wellbeing, and Ageing Study. Neurourol Urodyn. 2011;30(7):1281–5.
6. DuBeau CE, Kuchel GA, Johnson T, Palmer MH, Wagg A. Incontinence in the frail elderly: report from the 4th International Consultation on Incontinence. Neurourol Urodyn. 2010;29(1):165–78.
7. Mohd SS. The prevalence of urinary incontinence among the elderly in a rural community in Selangor. Malays J Med Sci. 2010(2):18–23.
8. Chen YM, Hwang SJ, Chen LK, Chen DY, Lan CF. Urinary incontinence among institutionalized oldest old Chinese men in Taiwan. Neurourol Urodyn. 2009;28(4):335–8.
9. Wallace SA, Roe B, Williams K, Palmer M. Bladder training for urinary incontinence in adults. Cochrane Database Syst Rev. 2004;(1):CD001308. Updated in 2009. [Systematic review was updated by WHO in 2015]
10. Ostaszkiewicz J, Johnston L, Roe B. Habit retraining for the management of urinary incontinence in adults. Cochrane Database Syst Rev. 2004(2):CD002801.
11. Eustice S, Roe B, Paterson J. Prompted voiding for the management of urinary incontinence in adults. Cochrane Database Syst Rev. 2000;(2):CD002113.
12. Ostaszkiewicz J, Johnston L, Roe B. Timed voiding for the management of urinary incontinence in adults. Cochrane Database Syst Rev. 2004;(1):CD002802.
13. Dumoulin C, Hay-Smith EJ, Mac Habee-Seguin G: Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database Syst Rev. 2014;(5):CD005654.
14. Colling J, Ouslander J, Hadley BJ, Eisch J, Campbell E. The effects of patterned urge-response toileting (PURT) on urinary incontinence among nursing home residents. J Am Geriatr Soc. 1992;40(2):135–41.
15. Colling J, Owen TR, McCreedy M, Newman D: The effects of a continence program on frail community-dwelling elderly persons. Urologic nursing 2003, 23(2):117–22, 127–31.
16. Jirovec MM, Templin T: Predicting success using individualized scheduled toileting for memory-impaired elders at home. Research in nursing & health 2001, 24(1):1–8.
17. Nikoletti S, Young J, King M. Evaluation of an electronic monitoring device for urinary incontinence in elderly patients in an acute care setting. J Wound Ostomy Continence Nurs. 2004;31(3):138–49.
18. Linn JG. Prompted voiding in the treatment of urinary incontinence. In: Rehabilitation: R & D Progress Reports, Vol. 32. Washington (DC): United States Department of Veterans Affairs, Rehabilitation Research and Development Service; 1995.
19. Tobin GW, Brocklehurst JC. The management of urinary incontinence in local authority residential homes for the elderly. Age Ageing. 1986;15(5):292–8.
20. Smith DA, Newman DK, McDowell BJ, Burgio LD. Reduction of incontinence among elderly in a nursing home setting. In: Funk SG, Tornquist EM, Champagne MT, Wiese RA, editors. Key aspects of elder care: managing falls, incontinence, and cognitive impairment.
(continued next page)

27 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
New York (NY): Springer Publishing; 1992:196–204. 21. Burgio KL, Locher JL, Goode PS, Hardin JM, McDowell BJ,
Dombrowski M, Candib D. Behavioral vs drug treatment for urge urinary incontinence in older women: a randomized controlled trial. JAMA. 1998;280(23):1995–2000.
22. Burns PA, Pranikoff K, Nochajski TH, Hadley EC, Levy KJ, Ory MG. A comparison of effectiveness of biofeedback and pelvic muscle exercise treatment of stress incontinence in older community-dwelling women. J Gerontology. 1993;48(4):M167–74.
23. Kim H, Suzuki T, Yoshida Y, Yoshida H. Effectiveness of multidimensional exercises for the treatment of stress urinary incontinence in elderly community-dwelling Japanese women: a randomized, controlled, crossover trial. J Am Geriatr Soc. 2007;55(12):1932–9.
24. Kim H, Yoshida H, Suzuki T. The effects of multidimensional exercise treatment on community-dwelling elderly Japanese women with stress, urge, and mixed urinary incontinence: a randomized controlled trial. Int J Nurs Stud. 2011;48(10):1165–72.
25. Miller JM, Ashton-Miller JA, DeLancey JO. A pelvic muscle precontraction can reduce cough-related urine loss in selected women with mild SUI. J Am Geriatr Soc. 1998;46(7):870–4.
26. Pereira VS, Correia GN, Driusso P. Individual and group pelvic floor muscle training versus no treatment in female stress urinary incontinence: a randomized controlled pilot study. Eur J Obstet Gynecol Reprod Biol. 2011;159(2):465–71.
27. Goode PS, Burgio KL, Kraus SR, Kenton K, Litman HJ, Richter HE, Urinary Incontinence Treatment N. Correlates and predictors of patient satisfaction with drug therapy and combined drug therapy and behavioral training for urgency urinary incontinence in women. Int Urogynecol J Pelvic Floor Dysfunct. 2011;22(3):327–34.
28. Pereira VS, de Melo MV, Correia GN, Driusso P. Vaginal cone for postmenopausal women with stress urinary incontinence: randomized, controlled trial. Climacteric. 2012;15(1):45–51.
29. Lee HH, Lee SW, Song CH,. The influence of pelvic muscle training program on lower urinary tract symptom, maximum vaginal contraction pressure, and pelvic floor muscle activity in aged women with stress urinary incontinence. Korean J Sport Sci. 2009;20(3):466–74.
30. Engberg S, Sereika SM, McDowell BJ, Weber E, Brodak I. Effectiveness of prompted voiding in treating urinary incontinence in
cognitively impaired homebound older adults. J Wound Ostomy Continence Nurs. 2002;29(5):252–65.
31. McDowell BJ, Engberg S, Sereika S, Donovan N, Jubeck ME, Weber E et al. Effectiveness of behavioral therapy to treat incontinence in homebound older adults. J Am Geriatr Soc. 1999;47(3):309–18.
32. Tobin GW, Brocklehurst JC. The management of urinary incontinence in local authority residential homes for the elderly. Age Ageing. 1986;15(5):292–8.
33. Ouslander JG, Griffiths PC, McConnell E, Riolo L, Kutner M, Schnelle J. Functional incidental training: a randomized, controlled, crossover trial in Veterans Affairs nursing homes. J Am Geriatr Soc. 2005;53(7):1091–100.
34. McFall SL, Yerkes AM, Cowan LD. Outcomes of a small group educational intervention for urinary incontinence: episodes of incontinence and other urinary symptoms. J Aging Health. 2000;12(2):250–67.
35. Goode PS, Burgio KL, Locher JL, Umlauf MG, Lloyd LK, Roth DL. Urodynamic changes associated with behavioral and drug treatment of urge incontinence in older women. J Am Geriatr Soc. 2002;50(5):808–16.
36. Subak LL, Quesenberry CP, Posner SF, Cattolica E, Soghikian K. The effect of behavioral therapy on urinary incontinence: a randomized controlled trial. Obstet Gynecol. 2002;100(1):72–8.
37. Dougherty MC, Dwyer JW, Pendergast JF, Boyington AR, Tomlinson BU, Coward RT et al. A randomized trial of behavioral management for continence with older rural women. Res Nurs Health.2002;25(1):3–13.
38. Johnson TM, Burgio KL, Redden DT, Wright KC, Goode PS. Effects of behavioral and drug therapy on nocturia in older incontinent women. J Am Geriatr Soc. 2005;53(5):846–50.
39. Hu TW, Igou JF, Kaltreider DL, Yu LC, Rohner TJ, Dennis PJ et al. A clinical trial of a behavioral therapy to reduce urinary incontinence in nursing homes: outcome and implications. JAMA. 1989;261(18):2656–62.
40. Schnelle JF, Traughber B, Sowell VA, Newman DR, Petrilli CO, Ory M. Prompted voiding treatment of urinary incontinence in nursing home patients. A behavior management approach for nursing home staff. J Am Geriatr Soc. 1989;37(11):1051–7.

28 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
Annex 1: Search strategy
MEDLINE database
1. exp behavior therapy/
2. (behav$ adj25 therapy).mp. [mp=protocol supplementary
concept, rare disease supplementary concept, title, original title,
abstract, name of substance word, subject heading word, unique
identifier]
3. exp cognitive therapy/
4. (cognit$ adj25 therapy).mp. [mp=protocol supplementary
concept, rare disease supplementary concept, title, original title,
abstract, name of substance word, subject heading word, unique
identifier]
5. (conservat$ adj25 intervention$).mp. [mp=protocol
supplementary concept, rare disease supplementary concept, title,
original title, abstract, name of substance word, subject heading
word, unique identifier]
6. toilet training.mp. [mp=protocol supplementary concept, rare
disease supplementary concept, title, original title, abstract, name
of substance word, subject heading word, unique identifier]
7. (habit training or habit retraining).mp. [mp=protocol
supplementary concept, rare disease supplementary concept, title,
original title, abstract, name of substance word, subject heading
word, unique identifier]
8. timed void$.mp. [mp=protocol supplementary concept, rare
disease supplementary concept, title, original title, abstract, name
of substance word, subject heading word, unique identifier]
9. prompted void$.mp. [mp=protocol supplementary concept, rare
disease supplementary concept, title, original title, abstract, name
of substance word, subject heading word, unique identifier]
10. (nursing homes and urinary incontinence).mp. [mp=protocol
supplementary concept, rare disease supplementary concept, title,
original title, abstract, name of substance word, subject heading
word, unique identifier]
11. 1 or 2 or 3 or 4 or 5 or 6 or 7 or 9 or 10
12. exp Urinary Incontinence/ or urinary incontinence.mp.
[mp=protocol supplementary concept, rare disease
supplementary concept, title, original title, abstract, name of
substance word, subject heading word, unique identifier]
13. 11 and 12
14. 13 not child.mp. [mp=protocol supplementary concept, rare
disease supplementary concept, title, original title, abstract, name
of substance word, subject heading word, unique identifier]
15. exp randomized controlled trials/
16. randomized controlled trial.pt.
17. exp random allocation/
18. exp double blind method/
19. exp single blind method/
20. exp Clinical Trial/
21. clinical trial.pt.
22. (clin$ adj25 trial$).ti,ab.
23. ((singl$ or doubl$ or treb$ or tripl$) adj25 (blind$ or
mask$)).ti,ab.
24. placebo$.ti,ab.
25. random$.ti,ab.
26. research design/
27. placebos.mp. [mp=protocol supplementary concept, rare
disease supplementary concept, title, original title, abstract, name
of substance word, subject heading word, unique identifier]
28. or/15-27
29. 14 and 28
(continued next page)

29 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
30. exp Aged/ or exp Aging/
31. exp Frail Elderly/
32. 30 or 31
33. 29 and 32
Embase database
1. Randomized Controlled Trial/
2. controlled study/
3. clinical study/
4. major clinical study/
5. prospective study/
6. meta-analysis/
7. exp clinical trial/
8. randomization/
9. crossover procedure/ or double blind procedure/ or parallel
design/ or single blind procedure/
10. Placebo/
11. latin square design/
12. exp comparative study/
13. follow up/
14. pilot study/
15. family study/ or feasibility study/ or pilot study/ or study/
16. placebo$.tw.
17. random$.tw.
18. (clin$ adj25 trial$).tw.
19. ((singl$ or doubl$ or trebl$ or tripl$) adj25 (blind$ or
mask$)).tw.
20. factorial.tw.
21. crossover.tw.
22. latin square.tw.
23. (balance$ adj2 block$).tw.
24. or/1-23
25. (nonhuman not human).sh.
26. 24 not 25
27. behavior modification/ or behavior therapy/
28. (conservat$ adj25 (intervention$ or therap$)).tw.
29. conservative treatment/
30. (behav$ adj25 (therap$ or train$ or treatment$ or
intervention$)).tw.
31. (habit adj2 (train$ or retrain$)).tw.
32. (void$ adj2 (time$ or prompt$ or schedul$)).tw.
33. toilet$.tw.
34. or/27-33
35. bladder disease/ or bladder dysfunction/ or detrusor
dyssynergia/ or neurogenic bladder/
36. (continen$ or incontinen$).tw.
37. exp Incontinence/
38. 37 or 35 or 36
39. 26 and 34 and 38
40. limit 39 to (embryo or infant or child or preschool child <1 to 6
years> or school child <7 to 12 years> or adolescent <13 to 17
years>)
41. limit 39 to (adult <18 to 64 years> or aged <65+ years>)
42. 40 not 41
43. 39 not 42
44. aging/ or aging.mp.
45. frail elderly.mp. or frail elderly/
46. 44 or 45
47. 43 and 46

30 Evidence profile: urinary incontinence
ICOPE guidelines – World Health Organization
Annex 2: PRISMA2 2009 flow diagram for non-pharmacological intervention
for managing urinary incontinence
_______________________________ 2 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). For more information: http://www.prisma-statement.org
Records identified through database
searching (n = 1893)
Records after duplicates removed (n = 986)
Records excluded (n = 714)
• Conference abstract (n = 146)
• Pharmacological intervention (n = 568)
Full-text articles assessed for eligibility (n = 272)
• Systematic reviews (SR) = 111
• Randomized controlled trials (RCTs) = 161
Full-text articles excluded, with reasons (n = 265) Reasons for RCT exclusion:
• Inappropriate age group (n = 123)
• Insufficient information on outcomes (n = 36) Reasons for review exclusion:
• Not SR (n = 54)
• Quality assessment not performed (n = 29)
• More recent reviews available (n = 23)
Studies included in qualitative synthesis
• SR = 111
• RCTs = 161
Studies included in quantitative synthesis (meta-analysis) (n = 27)
• SR = 25 RCTs
• Additional studies = 2 RCTs
Additional records identified through
other sources (n = 19)
Records screened (n = 986)
Inclu
sio
n
Scre
en
ing
Elig
ibili
ty
Iden
tificatio
n