Evidence of Non-Linear Associations between Frustration ...
11
Evidence of Non-Linear Associations between Frustration-Related Prefrontal Cortex Activation and the Normal:Abnormal Spectrum of Irritability in Young Children Adam S. Grabell 1 & Yanwei Li 1,2 & Jeff W. Barker 3 & Lauren S. Wakschlag 4 & Theodore J. Huppert 3 & Susan B. Perlman 1 Published online: 18 March 2017 # Springer Science+Business Media New York 2017 Abstract Burgeoning interest in early childhood irritability has recently turned toward neuroimaging techniques to better understand normal versus abnormal irritability using dimen- sional methods. Current accounts largely assume a linear re- lationship between poor frustration management, an expres- sion of irritability, and its underlying neural circuitry. However, the relationship between these constructs may not be linear (i.e., operate differently at varying points across the irritability spectrum), with implications for how early atypical irritability is identified and treated. Our goal was to examine how the association between frustration-related lateral pre- frontal cortex (LPFC) activation and irritability differs across the dimensional spectrum of irritability by testing for non- linear associations. Children (N = 92; ages 3–7) ranging from virtually no irritability to the upper end of the clinical range completed a frustration induction task while we recorded LPFC hemoglobin levels using fNIRS. Children self-rated their emotions during the task and parents rated their child’ s level of irritability. Whereas a linear model showed no rela- tionship between frustration-related LPFC activation and irri- tability, a quadratic model revealed frustration-related LPFC activation increased as parent-reported irritability scores in- creased within the normative range of irritability but decreased with increasing irritability in the severe range, with an apex at the 91st percentile. Complementarily, we found children’ s self-ratings of emotion during frustration related to concurrent LPFC activation as an inverted U function, such that children who reported mild distress had greater activation than peers reporting no or high distress. Results suggest children with relatively higher irritability who are unimpaired may possess well-developed LPFC support, a mechanism that drops out in the severe end of the irritability dimension. Findings suggest novel avenues for understanding the heterogeneity of early irritability and its clinical sequelae. Keywords Early childhood . Irritability . Emotion regulation . Lateral prefrontal cortex Irritability comprises annoyance, touchiness, angry mood, and temper outbursts (Stringaris 2011), is a feature of both inter- nalizing and externalizing disorders (Dougherty et al. 2013; Kim-Cohen et al. 2003; Nock et al. 2007; Wakschlag et al. 2015), and is one of the most common reasons young children are referred for clinical services (Avenevoli et al. 2015). In much of the clinical literature, irritability is described as a pathologic state, in which irritable mood and angry outbursts are pervasive and impairing (Leibenluft et al. 2003). However, because irritable behaviors are common in early childhood, defining clinically salient irritability is particularly Portions of the findings included in this manuscript were presented as a poster at the Congress on Pediatric Irritability and Dysregulation, University of Vermont, Burlington, VT (October 21–22, 2015). * Adam S. Grabell [email protected] 1 Department of Psychiatry, Laboratory for Child Brain Development, University of Pittsburgh School of Medicine, Loeffler Building, 121 Meyran Avenue, Pittsburgh, PA 15213, USA 2 Research Center for Learning Science, Key Laboratory of Child Development and Learning Science of Ministry of Education, Southeast University, Nanjing, Jiangsu, China 3 Department of Radiology, University of Pittsburgh School of Medicine, Pittsburgh, PA, USA 4 Department of Medical Social Sciences, Feinberg School of Medicine, and the Institute for Policy Research, Northwestern University, Chicago, IL, USA J Abnorm Child Psychol (2018) 46:137–147 DOI 10.1007/s10802-017-0286-5
Transcript of Evidence of Non-Linear Associations between Frustration ...

Evidence of Non-Linear Associationsbetween Frustration-Related PrefrontalCortex Activation and the Normal:AbnormalSpectrum of Irritability in Young Children
Adam S. Grabell1 & Yanwei Li1,2 & Jeff W. Barker3 & Lauren S. Wakschlag4 &
Theodore J. Huppert3 & Susan B. Perlman1
Published online: 18 March 2017# Springer Science+Business Media New York 2017
Abstract Burgeoning interest in early childhood irritabilityhas recently turned toward neuroimaging techniques to betterunderstand normal versus abnormal irritability using dimen-sional methods. Current accounts largely assume a linear re-lationship between poor frustration management, an expres-sion of irritability, and its underlying neural circuitry.However, the relationship between these constructs may notbe linear (i.e., operate differently at varying points across theirritability spectrum), with implications for how early atypicalirritability is identified and treated. Our goal was to examinehow the association between frustration-related lateral pre-frontal cortex (LPFC) activation and irritability differs acrossthe dimensional spectrum of irritability by testing for non-linear associations. Children (N = 92; ages 3–7) ranging fromvirtually no irritability to the upper end of the clinical rangecompleted a frustration induction task while we recorded
LPFC hemoglobin levels using fNIRS. Children self-ratedtheir emotions during the task and parents rated their child’slevel of irritability. Whereas a linear model showed no rela-tionship between frustration-related LPFC activation and irri-tability, a quadratic model revealed frustration-related LPFCactivation increased as parent-reported irritability scores in-creased within the normative range of irritability but decreasedwith increasing irritability in the severe range, with an apex atthe 91st percentile. Complementarily, we found children’sself-ratings of emotion during frustration related to concurrentLPFC activation as an inverted U function, such that childrenwho reported mild distress had greater activation than peersreporting no or high distress. Results suggest children withrelatively higher irritability who are unimpaired may possesswell-developed LPFC support, a mechanism that drops out inthe severe end of the irritability dimension. Findings suggestnovel avenues for understanding the heterogeneity of earlyirritability and its clinical sequelae.
Keywords Early childhood . Irritability . Emotionregulation . Lateral prefrontal cortex
Irritability comprises annoyance, touchiness, angry mood, andtemper outbursts (Stringaris 2011), is a feature of both inter-nalizing and externalizing disorders (Dougherty et al. 2013;Kim-Cohen et al. 2003; Nock et al. 2007; Wakschlag et al.2015), and is one of the most common reasons young childrenare referred for clinical services (Avenevoli et al. 2015). Inmuch of the clinical literature, irritability is described as apathologic state, in which irritable mood and angry outburstsare pervasive and impairing (Leibenluft et al. 2003). However,because irritable behaviors are common in early childhood,defining clinically salient irritability is particularly
Portions of the findings included in this manuscript were presented as aposter at the Congress on Pediatric Irritability and Dysregulation,University of Vermont, Burlington, VT (October 21–22, 2015).
* Adam S. [email protected]
1 Department of Psychiatry, Laboratory for Child Brain Development,University of Pittsburgh School of Medicine, Loeffler Building, 121Meyran Avenue, Pittsburgh, PA 15213, USA
2 Research Center for Learning Science, Key Laboratory of ChildDevelopment and Learning Science of Ministry of Education,Southeast University, Nanjing, Jiangsu, China
3 Department of Radiology, University of Pittsburgh School ofMedicine, Pittsburgh, PA, USA
4 Department of Medical Social Sciences, Feinberg School ofMedicine, and the Institute for Policy Research, NorthwesternUniversity, Chicago, IL, USA
J Abnorm Child Psychol (2018) 46:137–147DOI 10.1007/s10802-017-0286-5

challenging (Wakschlag et al. 2010). When their increasedgoal-oriented drive collides with environmentally imposedlimits, young children regularly experience frustration, de-fined as anger in response to a blocked goal or reward(Berkowitz 1989). The result is the common occurrence ofnormative misbehaviors such as temper tantrums.Accordingly, many investigations of irritability in early child-hood take a developmentally specified approach (Wakschlaget al. 2010), defining irritability along a dimensional spectrumpresent in all children ranging from low and normatively oc-curring to severe and atypical (Li et al. 2016; Perlman et al.2014). A major objective of the child irritability field is toidentify the point along the dimension that marks when irrita-bility crosses into the clinically significant range (Wakschlaget al. 2015). Dimensional ratings of behavioral irritabilityshow significant heterogeneity in clinical and longitudinaloutcomes of these children (Wakschlag et al. 2015). To moreprecisely characterize patterns of early abnormal irritability,the field has turned toward neuroimaging methods to betterunderstand the normal:abnormal spectrum of irritability inearly childhood (Avenevoli et al. 2015). Clinical descriptionsof irritability throughout the DSM suggest a positive linearassociation between irritability and dysregulated response tofrustration (American Psychiatric Association 2013), imply-ing higher irritability corresponds to weaker neural activationsupporting frustration regulation across the irritability dimen-sion. However, this assumption has yet to be tested in samplesof young children comprising the full dimensional spectrumof irritability. In fact, early childhood irritability andfrustration-related neural activation may follow a non-linearfunction with different implications for how typical versusatypical irritability is defined. For example, low and high irri-table young children may vary in their capacity to recruit topdown control in the face of frustration.
In the adult neuroimaging literature, evidence suggestsfrustration comprises the complex interaction of reward, reac-tive aggression, and regulatory systems (Blair 2012; Coccaroet al. 2011). Frustration may involve decreased ventral stria-tum activation, and increased amygdala, hypothalamus, ante-rior insula, and periaqueductal grey activation, coupled withincreased activation of various prefrontal cortex regions(Abler et al. 2005; Yu et al. 2014). This prefrontal cortexactivation, comprising dACC, orbitofrontal, and dorso andventro medial and lateral areas, among others, is hypothesizedto reflect decision-making, processing, and regulation strate-gies to modulate salient frustration (Blair 2016; Perlman et al.2015b). Two regions within the prefrontal cortex hypothe-sized to support frustration regulation include the dorsolateraland ventrolateral prefrontal cortex (DLPFC, VLPFC,respectively; Blair 2012; Coccaro et al. 2011).
The DLPFC is hypothesized to support frustration regula-tion via its role in myriad executive functions including rever-sal learning (Blair 2012; Coccaro et al. 2011; Ochsner et al.
2004), inhibition, attention shifting, and working memory(Carpenter et al. 2000), that may be engaged to manage emo-tional challenges, including in early childhood (Zelazo andCarlson 2012; Zelazo and Cunningham 2007). The VLPFCis hypothesized to support frustration regulation via top downconnections with subcortical structures, including the amyg-dala, that modulate the threat response (Wager et al. 2008).There is robust data showing DLPFC and VLPFC activationoccurs during various emotional challenges, however, somestudies have reported that this activation might be positivelyassociated with irritability in healthy adults. For example, in asample of healthy adults, higher self-ratings of susceptibilityto frustration were related to greaterDLPFC activation duringa frustration task (Siegrist et al. 2005). The authors postulatedthat this seemingly counter-intuitive finding may reflectchanges in DLPFC functioning that result from experiencingfrustration more regularly in every day life. In clinical adultpopulations, however, evidence suggests that severe irritabil-ity may be associated with a reduced prefrontal response tofrustration. Adults with extremely high trait aggression (phe-notypically similar to irritability) showed less VLPFC activa-tion during a frustration task compared to adults with low traitaggression (Pawliczek et al. 2013). Collectively, this literaturesuggests that, in adults, the association between irritability andprefrontal activation during frustration may not be constantacross the full irritability dimension.
Similar to adults, in early childhood the association be-tween frustration-related DL and VLPFC activation andirritability appears to depend on level of irritability severity.Perlman et al. (2014) used functional near infrared spectros-copy (fNIRS), a neuroimaging technique that measures hemo-dynamic changes in the outer cortex and has less spatial sen-sitivity compared to fMRI (Boas et al. 2014) to probe theLPFC (comprising DL and VLPFC areas) during frustrationin healthy preschoolers. Results showed that healthy pre-schoolers with higher levels of parent-rated irritability showeda greater LPFC response to frustration than peers with lowerirritability. Like previous adult findings in healthy samples, aseemingly counter-intuitive positive association betweenLPFC activation and irritability may indicate that childrenwith higher levels of normative irritability, and who do nothave psychopathology, may require greater LPFC activationto regulate frustration as well as peers. In other words, childrenin the sample with low irritability may have shown lowfrustration-related LPFC activation not because they wereworse emotion regulators, but because they experienced frus-tration less saliently and required less down-regulation thanpeers. In contrast, we hypothesize that early, severe irritabilitywill be associated with a reduced LPFC response to frustra-tion, as shown in case studies of preschoolers sustaining le-sions to regions including the LPFC (Marlowe 1992) and inevent related potential (ERP) investigations comparing chil-dren suffering from a severe form of clinically impairing
138 J Abnorm Child Psychol (2018) 46:137–147

irritability to healthy peers during a frustration task (Rich et al.2007). If irritability and frustration- related LPFC activationare positively associated in typically-developing children, andnegatively associated in clinically irritable children, it sug-gests a potential inverted U association across the full normalto abnormal dimension. Specifically, children with low irrita-bility may require less frustration- related LPFC activation,children with high but normative irritability may match salientfrustration with an enhanced LPFC response, and childrenwith clinically significant irritability may have an inadequateLPFC response to frustration.
An inverted U association between early irritability andfrustration-related neural activation has the potential to shifthow we consider the normative vs. maladaptive tipping pointof irritability across the child population. Thus, the goal of thepresent study was to examine the association betweenfrustration- related LPFC activation and irritability by testingfor non-linear patterns. We examined 92 children (ages 3–7),24% (n = 22) of whom were seeking clinical services. Allchildren completed a developmentally sensitive and well-validated frustration task (Perlman et al. 2015b; Perlmanet al. 2014) while we recorded LPFC hemoglobin levels usingfNIRS and parents rated their child’s level of irritability. Wehypothesized that frustration-related LPFC activation wouldbe positively associated with irritability at the low to norma-tive end of the dimension, and negatively associated at theimpairing end of the dimension.
Methods
Subjects
We recruited young children from the community and frompsychiatric outpatient clinics to examine the full range of lowto high irritability. Children from the community were recruit-ed via paper and internet advertisements. Community-recruited subjects were reported by their parents to have nopsychiatric diagnoses and no lifetime history of severe psychi-atric diagnoses (e.g., psychosis) in any first- degree relative.Level of irritability was allowed to vary. Based on prior workin community samples of preschoolers, we expected the non-referred children to exhibit the full spectrum of irritability(Copeland et al. 2015). Children seeking assessment or inter-vention services at an outpatient clinic were recruited viaflyers and by clinic staff, as well as through an online registry.Exclusionary criteria were diagnosis or history of autism spec-trum disorder, mental retardation, psychotic disorder, or histo-ry of head trauma with loss of consciousness. Although werecruited from clinics for the purposes of sampling at the highend of the irritability spectrum, clinically recruited childrenwere included in the study regardless of their level of irritabil-ity or diagnostic status.
Four children were excluded from analyses due to poorquality fNIRS data (1), technical error (2), and experimentererror (1). The final sample included 92 children between 3 and7 years (M = 5.3 years, SD = 1.3 years), 71 community-recruited and 22 clinic-recruited. Clinic and community- re-cruited children did not differ in Verbal IQ score on thePeabody Picture Vocabulary Test, Fourth Edition (Dunn andDunn 2012). Clinic-recruited children were more likely to beolder, male, and African American compared to community-recruited children (see Table 1). The goal of the study, how-ever, was not to compare discrete groups, but examine a di-mensional sample of children from a diverse range of back-grounds. Referral status, age, gender, and verbal IQ wereadded as covariates in all analyses.
Experimental procedures were approved by the localInstitutional Review Board.
fNIRS Instrument and Analysis
Set Up
As described in previous reports (Perlman et al. 2014), non-invasive optical imaging was performed using a CW6 real-time fNIRS system (Techen, Inc., Milford, MA). The fNIRSprobe comprised four light-source emitter positions contain-ing 690 nm (12mW) and 830 nm (8mW) laser light, and eightdetectors, mounted within a child-friendly elastic cap. Theaverage inter-optode distance was 3 cm. The probe was posi-tioned according to international 10–20 coordinates such thatthe interior medial corner of the probe was aligned with FpZ.The probe was designed to extended over Brodmann areas 10,the ventrolateral prefrontal cortex, and 46, the dorsolateralprefrontal cortex, on each hemisphere using AtlasViewer soft-ware (Aasted et al. 2015). Given the reduced spatial sensitivityof fNIRS compared to fMRI, we describe this region as theBLPFC^, consistent with our prior studies (Perlman et al.2015a; Perlman et al. 2014). As described in Okamoto et al.(2004), individual differences in head circumference have anegligible effect on how the probe is positioned over the cor-tical region of interest for each subject. Children were seatedin front of a touch-screen computer that recorded theirresponses.
Acquisition and Data Pre-Processing
Data were collected at 20 Hz and down sampled to 4 Hz usinga custom-builtMatlab-based (Mathworks, Natick, MA) acqui-sition software program (Barker et al. 2013). fNIRS data isrecorded as changes in the light from a source position inci-dent on a detector position as a function of time. Signals arefirst converted to changes in optical density (OD) over time asgiven byΔOD(t) = − log (I(t)/I0) where I(t) is the intensity ofthe signal recorded and I0 is the reference signal intensity at
J Abnorm Child Psychol (2018) 46:137–147 139

baseline. The optical density signals are converted to oxy- anddeoxy-hemoglobin estimates via the modified Beer-Lambertlaw with a partial pathlength correction of 0.1 for both wave-lengths (e.g., DPF = 6 and partial volume factor = 60). Thetime-course of hemoglobin changes for each source-detectorpair was analyzed using a general linear model Δ[Hbx] = X∗ β + ∈ where X is the design matrix encoding the timing ofstimulus events andis the coefficient (weight) of that stimuluscondition for that source-detector channel. The design matrix(X) was constructed from the convolution of the stimulustiming and duration with a canonical response model.
To reduce effects of motion artifacts and systemic physiol-ogy, we used an iteratively auto- regressively whitened,weighted least-squares (AR-iRLS) model to solve the generallinear equation. This regression model uses an nth order auto-regressive (AR) filter determined by an Akaike model-order(AIC) selection to whiten both sides of the GLM expression.Using this model, the regression coefficients (β) and theirerror-covariance (Cov) is estimated, which is used to definestatistical tests between task conditions or baseline. The re-gression model is solved sequentially for each data file foreach subject. All source-detector pairs within a file are solvedconcurrently yielding a full covariance model of the noise,which is used in group-level analysis.
Questionnaires
Parents rated their child’s irritability using the Temper Losssubscale of the Multidimensional Assessment Profile forDisruptive Behavior (MAP-DB; Wakschlag et al. 2012).This subscale was developed to differentiate normative fromclinically salient irritability, has shown good reliability and
validity, and has been shown to predict children’s brain acti-vation following frustration (Perlman et al. 2015b; Wakschlaget al. 2014; Wakschlag et al. 2012). The Temper Loss scaleprovides coverage of both irritable mood (e.g., BAct irritable^)and tantrums (e.g., BHave hot or explosive temper^) featuresof irritability rated on an objective frequency 6-point Likertscale (1 = Never in the past month; 6 =Many times each day).Temper Loss summary scores were used in all analyses. Asummary score of 42.5 corresponds to a 1.5 SD clinical cutoffbased on the MAP-DB community sample (Wakschlag, un-published data). Reliability of the Temper Loss scale was ex-cellent (α = 0.96).
The Frustration Emotion Task for Children (FETCH)
The Frustration Emotion Task for Children (FETCH; Perlmanet al. 2015a; Perlman et al. 2015b) is a frustration inductiontask tolerable to young children and stimulates frustration-related neural activation. Prior to the task, children wereshown three boxes: a blue box containing attractive toys, ared box containing small stickers, and a yellow box containinga broken crayon (Cole et al. 1994). Children were told thathow well they did in the game would determine from whichbox they would choose their final prize at the end. During thetask (see Fig. 1) children competed with Sparky, Ba verysneaky dog^, to fetch bones by touching the bone as it ap-peared on the screen. Trials were fixed where sometimes thechild could fetch the bone before Sparky (win trials), butsometimes Sparky would fetch the bone before the child’spossible reaction time (frustration trials). After win trials, ananimated drawing depicted the child grabbing the bone andplacing it within one of five boxes indicating progression
Table 1 Demographic datadescribing the study sample,children referred from thecommunity, and children referredfrom clinics
Full Sample(n = 92)
Community-Recruited(n = 70)
Clinic-Recruited(n = 22)
t/χ2
Age (Years)
Mean (SD) 5.22(1.3) 5.01(1.3) 5.86(1.2) -2.66*
Range 3–7 3–7 3–7
% Male 61% 55% 82% 5.11*
Race
% Caucasian 63.4% 69% 45.5% 6.28*
% African American 33.3% 26.8% 54.5%
% Other 3.2% 4.2% 0%
Family Income
Median $55,000 $60,000 $20,000 ns
Range $6000–$1.2 M $6000–$1.2 M $10,000–$150,000
Temper Loss Score
Mean (SD) 22.19(18.6) 18.48(16.2) 34.18(22.1) -3.64(27.17)**a
Range 0–107 0–107 1–85
* p <0 .05, ** p <0 .01aAdjusted for unequal variances
140 J Abnorm Child Psychol (2018) 46:137–147
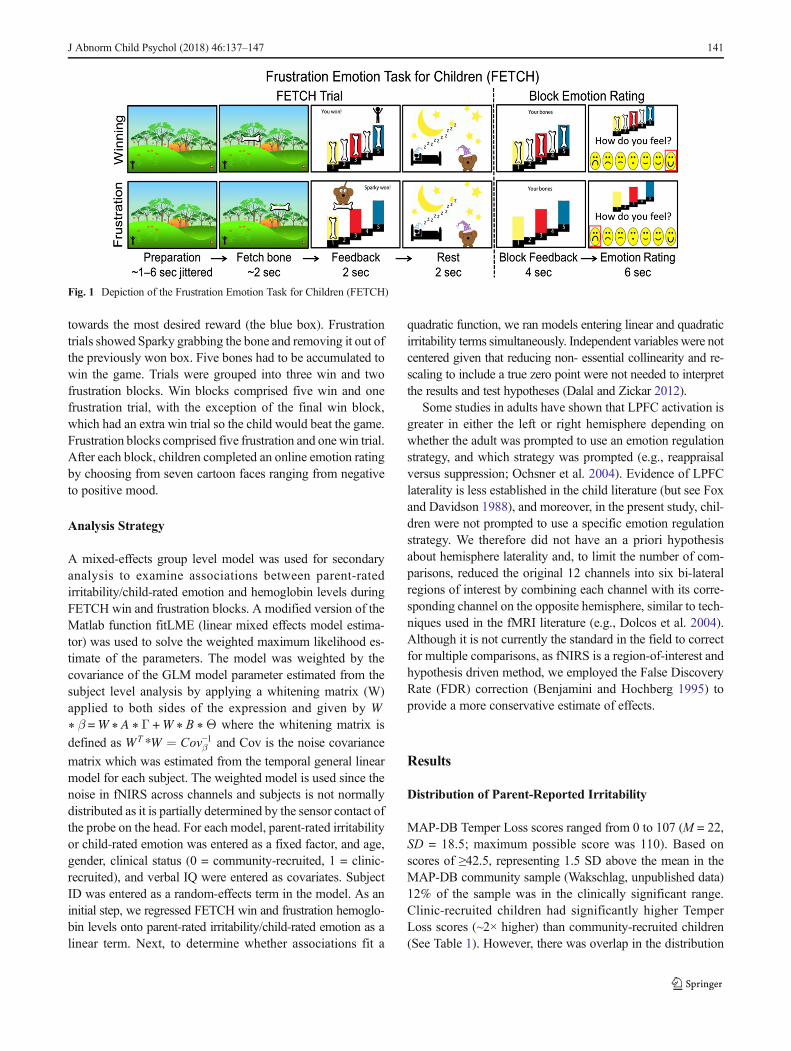
towards the most desired reward (the blue box). Frustrationtrials showed Sparky grabbing the bone and removing it out ofthe previously won box. Five bones had to be accumulated towin the game. Trials were grouped into three win and twofrustration blocks. Win blocks comprised five win and onefrustration trial, with the exception of the final win block,which had an extra win trial so the child would beat the game.Frustration blocks comprised five frustration and one win trial.After each block, children completed an online emotion ratingby choosing from seven cartoon faces ranging from negativeto positive mood.
Analysis Strategy
A mixed-effects group level model was used for secondaryanalysis to examine associations between parent-ratedirritability/child-rated emotion and hemoglobin levels duringFETCH win and frustration blocks. A modified version of theMatlab function fitLME (linear mixed effects model estima-tor) was used to solve the weighted maximum likelihood es-timate of the parameters. The model was weighted by thecovariance of the GLM model parameter estimated from thesubject level analysis by applying a whitening matrix (W)applied to both sides of the expression and given by W∗ β =W ∗ A ∗ Γ +W ∗ B ∗Θ where the whitening matrix is
defined as WT*W ¼ Cov−1β and Cov is the noise covariance
matrix which was estimated from the temporal general linearmodel for each subject. The weighted model is used since thenoise in fNIRS across channels and subjects is not normallydistributed as it is partially determined by the sensor contact ofthe probe on the head. For each model, parent-rated irritabilityor child-rated emotion was entered as a fixed factor, and age,gender, clinical status (0 = community-recruited, 1 = clinic-recruited), and verbal IQ were entered as covariates. SubjectID was entered as a random-effects term in the model. As aninitial step, we regressed FETCH win and frustration hemoglo-bin levels onto parent-rated irritability/child-rated emotion as alinear term. Next, to determine whether associations fit a
quadratic function, we ran models entering linear and quadraticirritability terms simultaneously. Independent variables were notcentered given that reducing non- essential collinearity and re-scaling to include a true zero point were not needed to interpretthe results and test hypotheses (Dalal and Zickar 2012).
Some studies in adults have shown that LPFC activation isgreater in either the left or right hemisphere depending onwhether the adult was prompted to use an emotion regulationstrategy, and which strategy was prompted (e.g., reappraisalversus suppression; Ochsner et al. 2004). Evidence of LPFClaterality is less established in the child literature (but see Foxand Davidson 1988), and moreover, in the present study, chil-dren were not prompted to use a specific emotion regulationstrategy. We therefore did not have an a priori hypothesisabout hemisphere laterality and, to limit the number of com-parisons, reduced the original 12 channels into six bi-lateralregions of interest by combining each channel with its corre-sponding channel on the opposite hemisphere, similar to tech-niques used in the fMRI literature (e.g., Dolcos et al. 2004).Although it is not currently the standard in the field to correctfor multiple comparisons, as fNIRS is a region-of-interest andhypothesis driven method, we employed the False DiscoveryRate (FDR) correction (Benjamini and Hochberg 1995) toprovide a more conservative estimate of effects.
Results
Distribution of Parent-Reported Irritability
MAP-DB Temper Loss scores ranged from 0 to 107 (M = 22,SD = 18.5; maximum possible score was 110). Based onscores of ≥42.5, representing 1.5 SD above the mean in theMAP-DB community sample (Wakschlag, unpublished data)12% of the sample was in the clinically significant range.Clinic-recruited children had significantly higher TemperLoss scores (~2× higher) than community-recruited children(See Table 1). However, there was overlap in the distribution
Fig. 1 Depiction of the Frustration Emotion Task for Children (FETCH)
J Abnorm Child Psychol (2018) 46:137–147 141

of Temper Loss scores in community and clinic-recruited chil-dren, and the total sample comprised the full dimensionalspectrum of irritability (See Fig. 2).
Child Self-Report of Frustration
On average, children selected negative faces following frus-tration blocks (M = 3.62 on a 1–7 scale with 1 being mostnegative and 7 being most positive), and positive faces fol-lowing win blocks (M = 6.21). A paired-sample t-test revealedthat emotion ratings following frustration and win blocks weresignificantly different, t(91) = −10.44, p < .001, d = 2.19.Step-wise multiple regression revealed irritability was unrelat-ed to children’s emotion ratings following frustration blockslinearly, β = −0.16, p = 0.13 or quadratically, linear irritabilityterm: β = 0.02, p = 0.93; quadratic irritability term: β = −0.19,p = 0.50. Next, linear and quadratic mixed effects models wereused to test for associations between frustration-related LPFCactivation and child self-ratings of frustration, controlling forage, gender, verbal IQ, and clinical status. A linear mixed-effects model revealed that children’s emotion ratings follow-ing frustration blocks were positively associated with LPFCactivation during frustration blocks at two bi-lateral regions ofinterest in the LPFC, t(356) = 2.97, p < .01, d = 0.31;t(356) = 3.19, p < 0.01, d = 0.34, such that children who ratedthemselves as less negative following frustration had higherLPFC activation. These associations remained significant af-ter FDR correction for multiple comparisons. In addition, thequadratic model revealed children’s emotion ratings followingfrustration blocks were associated with LPFC activation atthree bi-lateral regions of interest such that the linear termswere positive, t(354) = 2.81, p < 0.01, d = 0.30; t(354) = 2.46,p < 0.05, d = 0.26; t(354) = 2.01, p < 0.05, d = 0.21, and the
quadratic terms were negative, t(354) = −3.02, p < 0.01,d = 0.32; t (356) = −2.79, p < 0.01, d = 0.30;t(356) = −2.02, p < 0.01, d = 0.21, respectively; SeeFig. 3. After FDR correction for multiple comparisons,the inverted U association remained significant at twochannels. As shown in Fig. 4, the emotion rating associ-ated with the inverted U apex, for the most robust chan-nel, was 3.7, suggesting that children who rated them-selves as mildly distressed had greater frustration-relatedLPFC activation than peers who rated themselves as hap-py or very upset.
Parent Reported Irritability
Linear and quadratic mixed effects models were used to testfor associations between frustration- related LPFC activationand parent-rated irritability, controlling for age, gender, verbalIQ, and clinical status. When irritability was included as alinear term only, a mixed-effects model revealed no associa-tion with LPFC activation during frustration (all p-values >0.09) or winning (all p-values > 0.10). Next, we simultaneous-ly entered linear and quadratic terms into the model. As shownin Fig. 5, the linear and quadratic irritability terms were bothassociated with one region of interest in the middle LPFC,such that the linear term was positive, t(356) = 2.69,p < 0.01, d = 0.29, and the quadratic term was negative,t(356) = −2.74, p < 0.01, d = 0.29, indicating an inverted Ufunction. The inverted U finding remained significant afterFDR correction for multiple comparisons. As shown inFig. 6, at the low to moderate end of the irritability dimension,frustration-related LPFC activation increased with irritability,but at the high end of the irritability dimension, frustration-related LPFC decreased with irritability. A MAP-DB Temper
Fig. 2 Distribution of Temper Loss scores in community and clinic-recruited children
142 J Abnorm Child Psychol (2018) 46:137–147

Loss score of 32, the 91st percentile in the sample,corresponded to the inverted U apex. In comparison, theMAP DB clinical cutoff score, 42.5, corresponded to the96th percentile the current sample. There were no associationsbetween irritability and LPFC activation during win blocks inthe quadratic model (all p- values > 0.50).
Discussion
We found evidence that an inverted U function characterizedthe association between young children’s hemodynamic
response to frustration and level of irritability. Whereas a lin-ear model showed no association between frustration-relatedLPFC activation and parent-rated irritability, a quadratic mod-el revealed that frustration-related LPFC activation was posi-tively associated with irritability at the low to moderate end ofthe dimension, and negatively associated with irritability at thehigh end of the dimension. Strikingly, the LPFC activationapexwas nearly identical to the behaviorally identified clinicalthreshold on the MAP-DB. We similarly found an inverted Uassociation between frustration-related LPFC activation andchildren’s self-ratings of emotion, such that children who en-dorsed mild negative emotion following frustration had great-er activation than peers who endorsed either no or high nega-tive emotion.
Our finding that irritability and frustration-related LPFCactivation relate as an inverted U function, as opposed to alinear function, represents a potential shift in how early irrita-bility and its underlying neurophysiology might be conceptu-alized in this burgeoning field of research. Assuming a linearversus non-linear association between early irritability andfrustration regulation generates different assumptions aboutthe role of emotion regulation, and its underlying neural sys-tems, in clinical versus non-clinical early irritability. If weassume irritability and frustration-related hemodynamic acti-vation correlate as a linear function, it follows that more irri-tability is worse and linked to greater dysregulation, and thatchildren with the lowest irritability levels should show thestrongest frustration-related LPFC activation. However, thisassumption is incongruent with studies showing that higherirritability was associated with a stronger, not weaker,frustration-related LPFC response in non-impaired childrenand adults (Perlman et al. 2014; Siegrist et al. 2005). In con-trast, the present study suggests that LPFC activation duringfrustration is greatest at the inverted U apex, corresponding tomoderate irritability levels. Among non-impaired children,
Fig. 4 Scatterplot showing the inverted U fit between frustration-relatedactivation at the most significant bi-lateral region of interest and self-ratedemotion following frustration, with vertical line denoting the apex. The fitline appears in black with 95% confidence interval denoted with lightgray lines
Fig. 3 Channel-space probe super-imposed over 3Dmesh brain showingthe association between linear and quadratic self-rated emotion followingfrustration and oxygenated-hemoglobin levels during frustration. Theoriginal 12 channels were combined into 6 bi-lateral regions of interest
Fig. 5 Channel-space probe super-imposed over 3Dmesh brain showingthe association between linear and quadratic MAP-D Temper Loss scoresand oxygenated-hemoglobin levels during frustration. The original 12channels were combined into 6 bi-lateral regions of interest
J Abnorm Child Psychol (2018) 46:137–147 143

being a relatively more irritable child may be associated withwell- developed LPFC support for managing anger and frus-tration. Moreover, an inverted U association between self-reported emotion and frustration-related LPFC, such that chil-dren who rated themselves as experiencing moderate negativeemotion had the highest activation, further supports this con-tention. The inverted U apex may therefore mark the pointalong the irritability dimension when higher levels of severeirritability become associated with increasing decrements infrustration-related LPFC activation, a combination with po-tential to predict mental disorder (Lewis et al. 2006).Specifically, young children with high irritability paired withan underactive LPFC response to frustration may be most atrisk for a chronic course. The Temper Loss score correspond-ing to the apex, 32, the 91st percentile, approximated the clin-ical cutoff reported in the MAP DB community sample, 42.5,which was the 96th percentile in our sample. To our knowl-edge, this finding represents the first pathophysiologic valida-tion of a dimensional irritability scale, suggesting that highirritability scores on the MAP-DB are indicators of under-lying atypical hemodynamic activation. The present studymay therefore facilitate future research using an invertedU f ramework to more accu ra t e ly iden t i fy thenormal:abnormal irritability tipping point in early child-hood. Further, the present findings set the stage for futurework to explicate, in greater detail, the etiology of clini-cally impairing irritability and associated psychopatholo-gy. For example, children populating the descending armof the inverted U function may lack an LPFC Bbuffer^against impairing irritability that peers closer to the apexpossess, or, alternatively, it may be that irritability levelsexceeding a certain threshold interfere with LPFC activa-tion during frustration.
An inverted U association between early irritability andfrustration-related LPFC activation has potential implicationsfor a more precisionmedicine-based approach to treating earlyirritability (Insel 2014). Children referred to clinics for irrita-bility fall across a wide swath of the dimension (Drabick andGadow 2012) and may be routed to myriad treatments thatinteract with the developing LPFC. Controversial medicationsto treat severe irritability in early childhood, such asRisperidone (Biederman et al. 2005), affect mood and behav-ior, in part, by changing brain metabolism in the LPFC (Laneet al. 2004). Interventions for young children, such as cogni-tive behavioral therapy (CBT), require implementing meta-cognitive and emotion regulation skills that may only benefitirritable children with competent LPFC functioning (Graveand Blissett 2004; but note studies showing the reverse maybe true in adulthood, e.g., Siegle et al. 2006). Other interven-tions, such as parent-child interaction therapy (PCIT), are ef-ficacious in cognitively delayed children and may benefit ir-ritable children with poor LPFC functioning (Eyberg 2005).Finally, more recently developed interventions that attempt tostrengthen regulatory neural networks through executive func-tion training have shown mixed success (Morris et al. 2014).Our findings suggest that children referred to treatment forirritability may exhibit substantial variability in their LPFCactivation during frustration. Future work that further eluci-dates links between early irritability and LPFC functioninghas the potential to impact clinical decision making.
Limitations, Future Directions, and Conclusions
Although this study provides insight into the heterogeneity ofearly of irritability that could challenge the manner in whichirritability and its neural underpinnings are conceptualized,
Fig. 6 Scatterplot showing theinverted U fit between frustration-related activation at the significantbi-lateral region of interest andMAP-DB Temper Loss scores.Vertical lines denote the invertedU apex score (blue) and the 1.5SD clinical cutoff score from theMAP - DB norming sample(green). The fit line appears inblack with 95% confidence inter-val denoted with light gray lines
144 J Abnorm Child Psychol (2018) 46:137–147

some limitations must be acknowledged. Scatterplots revealeda skewed association between frustration-related LPFC activa-tion and irritability scores, such that a smaller subset of partic-ipants populated the descending arm of the inverted U.However, studies using larger samples suggest that irritabilityis similarly skewed in the general child population (Wakschlaget al. 2015). Thus, the inverted U association and irritabilityscore associated with the apex may have clinical utility in iden-tifying a subset of irritable children who are most at risk. Astrategy to oversample severely irritable children to create moreevenly distributed samples may have adversely affected theecological validity of the findings. Relatedly, distribution ofself-ratings following frustration blocks showed that nearly halfthe sample chose either the most negative or most positiverating every time, suggesting largely bimodal responding con-sistent with previous studies in this age range (Chambers andJohnston 2002). This bimodal distribution of self-reportedemotion may explain why we failed to find an associationbetween children’s self-ratings of emotion and parent-rated ir-ritability. Further, our interpretation of the inverted U functionsuggests the apex may discriminate children with elevated irri-tability that do and do not exhibit functional impairment ineveryday life. Although we were unable to directly test if chil-dren populating the descending arm of the inverted U curveshowed greater functional impairment than peers, prior workhas shown that the MAP- DB Temper Loss scale is significant-ly positively associated with measures of functional impair-ment (Wakschlag et al. 2015). An additional limitation is thatfNIRS is a technique capable only of measurement within theouter cortex and only on focused regions of interest (the LPFCin our study). However, the neural network underlying frustra-tion regulation comprises many structures projecting to andfrom the LPFC that may play a role in early irritability (Blair2012; Perlman et al. 2015b).
Irritability also has many environmental determinants (e.g.,neighborhood and family characteristics) that were not mea-sured but nonetheless shape early brain development(Hackman and Farah 2009). Future work is needed to under-stand how neural response to frustration corresponds withother biological systems, environmental factors, and differentclinical endpoints later in development. Finally, the presentfindings suggest that at the lowest point on the irritabilityspectrum irritability is coupled with low frustration-relatedLPFC activation, which may be clinically meaningful andwarrant future investigation. Increasing interest in the clinicalsignificance of early irritability, and defining clinical pheno-types, carries a risk of mislabeling irritability as a ubiqui-tously negative trait. The present study suggests rethink-ing this view. How irritability, and underlying regulatorysystems, contributes to early psychopathology may bemore complex than disorder-based criteria suggest andunpacking this complexity may lead to major strides inaddressing childhood-onset mental illness.
Acknowledgements Supported by NIMH grants K01 MH094467 PI:Susan Perlman, R21 MH100189 PI: Susan Perlman, and R01MH107540: PI Susan Perlman.
Compliance with Ethical Standards
Conflict of Interests Drs. Grabell, Barker, Wakschlag, Huppert andPerlman, and Ms. Li, report no competing interests.
Ethical Approval All procedures performed in studies involving hu-man participants were in accordance with the ethical standards of theinstitutional and/or national research committee and with the 1964Helsinki declaration and its later amendments or comparable ethicalstandards.
Informed Consent Informed consent was obtained from all individualparticipants included in the study.
References
Aasted, C. M., Yücel, M. A., Cooper, R. J., Dubb, J., Tsuzuki, D.,Becerra, L., et al. (2015). Anatomical guidance for functional near-infrared spectroscopy: AtlasViewer tutorial. Neurophotonics, 2,020801–020801.
Abler, B., Walter, H., & Erk, S. (2005). Neural correlates of frustration.Neuroreport, 16, 669–672.
American Psychiatric Association. (2013). Diagnostic and statisticalmanual of mental disorders (5th ed.). Washington, D.C.: Author.
Avenevoli, S., Blader, J. C., & Leibenluft, E. (2015). Irritability in youth:an update. Journal of the American Academy of Child andAdolescent Psychiatry, 54, 881–883.
Barker, J. W., Aarabi, A., & Huppert, T. J. (2013). Autoregressive modelbased algorithm for correcting motion and serially correlated errorsin fNIRS. Biomedical Optics Express, 4, 1366–1379.
Benjamini, Y., & Hochberg, Y. (1995). Controlling the false discoveryrate: a practical and powerful approach to multiple testing. Journalof the Royal Statistical Society. Series B (Methodological), 57, 289–300.
Berkowitz, L. (1989). Frustration-aggression hypothesis: examinationand reformulation. Psychological Bulletin, 106, 59.
Biederman, J., Mick, E., Hammerness, P., Harpold, T., Aleardi, M.,Dougherty, M., & Wozniak, J. (2005). Open-label, 8-week trial ofolanzapine and risperidone for the treatment of bipolar disorder inpreschool-age children. Biological Psychiatry, 58, 589–594.
Blair, R. (2012). Considering anger from a cognitive neuroscience per-spective.Wiley Interdisciplinary Reviews: Cognitive Science, 3, 65–74.
Blair, R. J. (2016). The neurobiology of impulsive aggression. Journal ofChild and Adolescent Psychopharmacology, 26, 4–9.
Boas, D. A., Elwell, C. E., Ferrari, M., & Taga, G. (2014). Twenty yearsof functional near-infrared spectroscopy: introduction for the specialissue. NeuroImage, 85, 1–5.
Carpenter, P. A., Just, M. A., & Reichle, E. D. (2000). Working memoryand executive function: evidence from neuroimaging. CurrentOpinion in Neurobiology, 10, 195–199.
Chambers, C. T., & Johnston, C. (2002). Developmental differences inchildren's use of rating scales. Journal of Pediatric Psychology, 27,27–36.
J Abnorm Child Psychol (2018) 46:137–147 145

Coccaro, E. F., Sripada, C. S., Yanowitch, R. N., & Phan, K. L. (2011).Corticolimbic function in impulsive aggressive behavior. BiologicalPsychiatry, 69, 1153–1159.
Cole, P. M., Zahn-Waxler, C., & Smith, K. D. (1994). Expressive controlduring a disappointment: variations related to preschoolers' behaviorproblems. Developmental Psychology, 30, 835.
Copeland, W. E., Brotman, M. A., & Costello, E. J. (2015). Normativeirritability in youth: developmental findings from the great SmokyMountains study. Journal of the American Academy of Child andAdolescent Psychiatry, 54, 635–642.
Dalal, D. K., & Zickar, M. J. (2012). Some common myths about center-ing predictor variables in moderated multiple regression and poly-nomial regression. Organizational Research Methods, 15, 339–362.
Dolcos, F., LaBar, K. S., & Cabeza, R. (2004). Interaction between theamygdala and the medial temporal lobe memory system predictsbetter memory for emotional events. Neuron, 42, 855–863.
Dougherty, L. R., Smith, V. C., Bufferd, S. J., Stringaris, A., Leibenluft,E., Carlson, G. A., & Klein, D. N. (2013). Preschool irritability:longitudinal associations with psychiatric disorders at age 6 andparental psychopathology. Journal of the American Academy ofChild and Adolescent Psychiatry, 52, 1304–1313.
Drabick, D. A., & Gadow, K. D. (2012). Deconstructing oppositionaldefiant disorder: Clinic-based evidence for an anger/irritability phe-notype. Journal of the American Academy of Child and AdolescentPsychiatry, 51, 384–393.
Dunn, L. M., & Dunn, D. (2012). Peabody picture vocabulary test,(PPVT™-4). Johannesburg: Pearson Education Inc..
Eyberg, S. M. (2005). Tailoring and adapting parent-child interactiontherapy to new populations. Education and Treatment of Children,28, 197–201.
Fox, N. A., & Davidson, R. J. (1988). Patterns of brain electrical activityduring facial signs of emotion in 10-month-old infants.Developmental Psychology, 24, 230.
Grave, J., & Blissett, J. (2004). Is cognitive behavior therapy develop-mentally appropriate for young children? A critical review of theevidence. Clinical Psychology Review, 24, 399–420.
Hackman, D. A., & Farah, M. J. (2009). Socioeconomic status and thedeveloping brain. Trends in Cognitive Sciences, 13, 65–73.
Insel, T. R. (2014). The NIMH research domain criteria (RDoC) project:precision medicine for psychiatry. American Journal of Psychiatry,171, 395–397.
Kim-Cohen, J., Caspi, A., Moffitt, T. E., Harrington, H., Milne, B. J., &Poulton, R. (2003). Prior juvenile diagnoses in adults with mentaldisorder: developmental follow-back of a prospective-longitudinalcohort. Archives of General Psychiatry, 60, 709–717.
Lane, C. J., Ngan, E. T., Yatham, L. N., Ruth, T. J., & Liddle, P. F. (2004).Immediate effects of risperidone on cerebral activity in healthy sub-jects: a comparison with subjects with first-episode schizophrenia.Journal of Psychiatry & Neuroscience: JPN, 29, 30–37.
Leibenluft, E., Blair, R. J. R., Charney, D. S., & Pine, D. S. (2003).Irritability in pediatric mania and other childhood psychopathology.Annals of the New York Academy of Sciences, 1008, 201–218.
Lewis, M. D., Granic, I., & Lamm, C. (2006). Behavioral differences inaggressive children linked with neural mechanisms of emotion regu-lation. Annals of the New York Academy of Sciences, 1094, 164–177.
Li, Y., Grabell, A. S., Wakschlag, L. S., Huppert, T. J., & Perlman, S. B.(2016). The neural substrates of cognitive flexibility are related toindividual differences in preschool irritability: a fNIRSinvestigation. Developmental Cognitive Neuroscience. doi:10.1016/j.dcn.2016.07.002.
Marlowe, W. B. (1992). The impact of a right prefrontal lesion on thedeveloping brain. Brain and Cognition, 20, 205–213.
Morris, P, Mattera, S. K., Castells, N., Bangser, M., Bierman, K., &Raver, C. (2014). Impact Findings from the Head Start CARESDemonstration: National Evaluation of Three Approaches toImproving Preschoolers’ Social and Emotional Competence.
OPRE Report 2014–44. Washington, DC: Office of Planning,Research and Evaluation, Administration for Children andFamilies, U.S. Department of Health and Human Services.
Nock, M. K., Kazdin, A. E., Hiripi, E., & Kessler, R. C. (2007). Lifetimeprevalence, correlates, and persistence of oppositional defiant disor-der: results from the National Comorbidity Survey Replication.Journal of Child Psychology and Psychiatry, 48, 703–713.
Ochsner, K. N., Ray, R. D., Cooper, J. C., Robertson, E. R., Chopra, S.,Gabrieli, J. D., & Gross, J. J. (2004). For better or for worse: neuralsystems supporting the cognitive down-and up-regulation of nega-tive emotion. NeuroImage, 23, 483–499.
Okamoto,M., Dan, H., Sakamoto, K., Takeo, K., Shimizu, K., Kohno, S.,et al. (2004). Three-dimensional probabilistic anatomical cranio-cerebral correlation via the international 10–20 system oriented fortranscranial functional brain mapping. NeuroImage, 21, 99–111.
Pawliczek, C. M., Derntl, B., Kellermann, T., Kohn, N., Gur, R. C., &Habel, U. (2013). Inhibitory control and trait aggression: neural andbehavioral insights using the emotional stop signal task.NeuroImage, 79, 264–274.
Perlman, S. B., Luna, B., Hein, T. C., & Huppert, T. J. (2014). fNIRSevidence of prefrontal regulation of frustration in early childhood.NeuroImage, 85, 326–334.
Perlman, S. B., Huppert, T. J., & Luna, B. (2015a). Functional near-infrared spectroscopy: evidence for development of prefrontal en-gagement in working memory in early through middle childhood.Cerebral Cortex, 26, 2790–2799.
Perlman, S. B., Jones, B. M., Wakschlag, L. S., Axelson, D., Birmaher,B., & Phillips,M. L. (2015b). Neural substrates of child irritability intypically developing and psychiatric populations. DevelopmentalCognitive Neuroscience, 14, 71–80.
Rich, B. A., Schmajuk,M., Perez-Edgar, K. E., Fox, N. A., Pine, D. S., &Leibenluft, E. (2007). Different psychophysiological and behavioralresponses elicited by frustration in pediatric bipolar disorder andsevere mood dysregulation. American Journal of Psychiatry, 164,309–317.
Siegle, G. J., Carter, C. S., & Thase, M. E. (2006). Use of FMRI to predictrecovery from unipolar depression with cognitive behavior therapy.American Journal of Psychiatry, 163, 735–738.
Siegrist, J., Menrath, I., Stöcker, T., Klein, M., Kellermann, T., Shah, N.J., et al. (2005). Differential brain activation according to chronicsocial reward frustration. Neuroreport, 16, 1899–1903.
Stringaris, A. (2011). Irritability in children and adolescents: a challengefor DSM-5. European Child & Adolescent Psychiatry, 20, 61–66.
Wager, T. D., Barrett, L. F., Bliss-Moreau, E., Lindquist, K., Duncan, S.,Kober, H., et al. (2008). The neuroimaging of emotion. In M. Lewis,J. M. Haviland-Jones, & L. F. Barrett (Eds.), The handbook ofemotion (3rd ed., pp. 249–271). New York: Guilford Press.
Wakschlag, L. S., Tolan, P. H., & Leventhal, B. L. (2010). Researchreview:‘Ain’t misbehavin’: towards a developmentally-specifiednosology for preschool disruptive behavior. Journal of ChildPsychology and Psychiatry, 51, 3–22.
Wakschlag, L. S., Henry, D. B., Tolan, P. H., Carter, A. S., Burns, J. L., &Briggs-Gowan, M. J. (2012). Putting theory to the test: modeling amultidimensional, developmentally-based approach to preschooldisruptive behavior. Journal of the American Academy of Childand Adolescent Psychiatry, 51, 593–604.
Wakschlag, L. S., Briggs-Gowan, M. J., Choi, S. W., Nichols, S. R.,Kestler, J., Burns, J. L., et al. (2014). Advancing a multidimensional,developmental spectrum approach to preschool disruptive behavior.Journal of the American Academy of Child and AdolescentPsychiatry, 53, 82–96.
Wakschlag, L. S., Estabrook, R., Petitclerc, A., Henry, D., Burns, J. L.,Perlman, S. B., et al. (2015). Clinical implications of a dimensionalapproach: the normal:abnormal spectrum of early irritability.Journal of the American Academy of Child and AdolescentPsychiatry, 54, 626–634.
146 J Abnorm Child Psychol (2018) 46:137–147

Yu, R., Mobbs, D., Seymour, B., Rowe, J. B., & Calder, A. J. (2014). Theneural signature of escalating frustration in humans. Cortex, 54,165–178.
Zelazo, P. D., & Carlson, S.M. (2012). Hot and cool executive function inchildhood and adolescence: development and plasticity. ChildDevelopment Perspectives, 6, 354–360.
Zelazo, P. D., & Cunningham, W. A. (2007). Executive function: mech-anisms underlying emotion regulation. In J. J. Gross (Ed.),Handbook of emotion regulation (pp. 135–158). New York:Guilford Press.
J Abnorm Child Psychol (2018) 46:137–147 147