Updates on management of Adolescent PCOS An evidence based approach

Evidence-Based Updates on the FirstWeek of Exclusive BreastfeedingAmong Infants $35 WeeksLori Feldman-Winter, MD, MPH,a Ann Kellams, MD, IBCLC,b Sigal Peter-Wohl, MD, MS,c Julie Scott Taylor, MD, MSc,d,e
Kimberly G. Lee, MD, MSc, IBCLC,f Mary J. Terrell, MD, IBCLC,g Lawrence Noble, MD,h Angela R. Maynor, MPH, RD, LDN, CSP,i
Joan Younger Meek, MD, MS, IBCLC,j Alison M. Stuebe, MD, MSck,l
abstractThe nutritional and immunologic properties of human milk, along with clearevidence of dose-dependent optimal health outcomes for both mothers andinfants, provide a compelling rationale to support exclusive breastfeeding. USwomen increasingly intend to breastfeed exclusively for 6 months. Becauseestablishing lactation can be challenging, exclusivity is often compromised inhopes of preventing feeding-related neonatal complications, potentiallyaffecting the continuation and duration of breastfeeding. Risk factors forimpaired lactogenesis are identifiable and common. Clinicians must be able torecognize normative patterns of exclusive breastfeeding in the first weekwhile proactively identifying potential challenges. In this review, we providenew evidence from the past 10 years on the following topics relevant toexclusive breastfeeding: milk production and transfer, neonatal weightand output assessment, management of glucose and bilirubin, immunedevelopment and the microbiome, supplementation, and health systemfactors. We focus on the early days of exclusive breastfeeding in healthynewborns $35 weeks’ gestation managed in the routine postpartum unit.With this evidence-based clinical review, we provide detailed guidance inidentifying medical indications for early supplementation and can informbest practices for both birthing facilities and providers.
Exclusive breastfeeding significantlyimproves maternal and childhealth. Although US pediatricians’recommendations are increasinglyaligned with American Academy ofPediatrics (AAP) policies, theiroptimism about the potential forbreastfeeding success has declined.1
To maintain familiarity with thebenefits of breastfeeding and theskills necessary to promote thispositive health intervention,providers caring for neonatesand/or new mothers need updatedevidence-based information andtools to assess and managebreastfeeding.
In this review, we provide newevidence from the past 10 years on thefollowing topics relevant to exclusivebreastfeeding: milk production andtransfer, neonatal weight and outputassessment, glucose stabilization,hyperbilirubinemia, immunedevelopment and the microbiome,supplementation, and health systeminterventions. We focus on the earlydays of exclusive breastfeeding inhealthy newborns $35 weeks’gestation managed in the routinepostpartum unit.2–6 Tables 1 through3 and Fig 1 provide summariesbased on evidence and authors’recommendations to provide concise
aDepartment of Pediatrics, Cooper Medical School, RowanUniversity and Children’s Regional Hospital at Cooper,Cooper University Health Care, Camden, New Jersey;bDepartment of Pediatrics, School of Medicine, University ofVirginia, Charlottesville, Virginia; cDivision of Neonatology,Departments of Pediatrics and kObstetrics and Gynecology,School of Medicine and lDepartment of Maternal and ChildHealth and Carolina Global Breastfeeding Institute, GillingsSchool of Global Public Health, University of North Carolinaat Chapel Hill, Chapel Hill, North Carolina; dAmericanUniversity of the Caribbean School of Medicine, SintMaarten, Netherlands Antilles; eDepartment of FamilyMedicine, Warren Alpert Medical School, Brown University,Providence, Rhode Island; fDivision of Neonatology,Department of Pediatrics, Medical University of SouthCarolina, Charleston, South Carolina; gDivision ofNeonatology, Department of Pediatrics, University of NorthCarolina Hospitals, Chapel Hill, North Carolina; hDepartmentof Pediatrics, Icahn School of Medicine at Mount Sinai, NewYork, New York; iDepartment of Food and Nutrition,University of North Carolina Health Care, Chapel Hill, NorthCarolina; and jDepartment of Clinical Sciences, College ofMedicine, Florida State University, Tallahassee, Florida
Drs Feldman-Winter, Kellams, and Stuebeconceptualized and designed the review of theliterature, conducted the literature review andanalysis, drafted the initial manuscript, and reviewedand revised the manuscript; Dr Peter-Wohl madesubstantial contributions to the acquisition of dataand to the analysis and interpretation of data, draftedthe article, and revised it critically for importantintellectual content; Dr Taylor made substantialcontributions to conception and design and madecritical revisions; Drs Lee and Terrell made substantialcontributions to the design and to the acquisition ofdata and made critical revisions for importantintellectual content; Drs Meek and Noble and MsMaynor made substantial contributions to theconception, design, and analysis and interpretation ofdata and revised the article critically for importantintellectual content; and all authors approved the finalmanuscript as submitted and agree to be accountablefor all aspects of the work.
To cite: Feldman-Winter L, Kellams A, Peter-WohlS, et al. Evidence-Based Updates on the FirstWeek of Exclusive Breastfeeding Among Infants$35 Weeks. Pediatrics. 2020;145(4):e20183696
PEDIATRICS Volume 145, number 4, April 2020:e20183696 STATE-OF-THE-ART REVIEW ARTICLE by guest on October 15, 2021www.aappublications.org/newsDownloaded from

and clear bullets on optimalmanagement. The search strategy andtables of evidence for milk productionand transfer, neonatal weight andoutput assessment, management ofglucose, and hyperbilirubinemia aresummarized in the SupplementalInformation.
MILK PRODUCTION AND TRANSFER
Three stages of milk production,lactogenesis I to III, are defined onthe basis of volume and compositionof milk. For volume, Fig 2 showsestimated daily milk production.16 Inrelation to composition, human milkchanges dramatically over the firstweek of lactation. Colostrum, which isproduced during the initial stage oflactation (lactogenesis I) in the firstdays after birth, contains moreprotein than mature milk. This highlydense early milk has a highconcentration of immunoglobulins,activated macrophages, lymphocytes,
neutrophils, and growth factors withessential roles in development of gut-associated lymphoid tissue.17 As milkvolume increases (lactogenesis II),sodium concentration and thesodium/potassium ratio declinerapidly with increased secretoryactivity of the lactocytes and closureof tight cellular junctions.18
Production of fat-rich, higher-caloriemature milk typically occurs by∼10 days post partum(lactogenesis III).
Most, but not all, women experiencelactogenesis II, referred to as “milkcoming in,” by 72 hours post partum.In the Infant Feeding Practices SurveyII, 19% of multiparous women and35% of primiparous women reportedmilk coming in on day 4 or later.19
Reasons for delayed lactogenesis IIinclude primiparity, cesarean delivery,and BMI . 27.20–22 Conditionsassociated with obesity, such asadvanced maternal age (possibly
related to reduced fertility associatedwith obesity-variant polycysticovarian syndrome) and excessivegestational weight gain, may also leadto a delay.23,24 Delayed lactogenesis IIis associated with neonatal weightloss .10%.20
Occasionally, a woman does notexperience lactogenesis II and onlyproduces small volumes of milk(prevalence 5%–8%).19,25 Thedifferential diagnosis includes breastpathology, previous breast surgery(with damage to ducts oraugmentation for hypoglandularbreasts), developmental anomaliesof the breast tissue, hormonaldisruptions (such as retainedplacental fragments and pituitaryinsufficiency, including Sheehan’ssyndrome, hypothyroidism, polycysticovarian syndrome, or theca-luteinovarian cysts), and toxins (such asexcessive tobacco exposure).26
Occasionally, strategies described
TABLE 1 Breastfeeding Assessment During the First Postnatal Week
Inpatient Hospital Discharge Outpatient
Schedule for observed feeding bytrained health professional(physician, midwife, or a physician-supervised, breastfeeding-trainedhealth care provider) to evaluatebreastfeeding effectiveness7
• At least once every 8–12 hduring the hospitalization
• At least once within 8 h beforehospital discharge
• Within 24–48 h of hospital discharge formother-infant pairs with:○ Infants ,37 wk gestation8
○ Any risk factors for breastfeedingdifficulties (Table 2)
○ Mothers who are experiencing any painwith breastfeeding
○ Infants with greater-than-expected wtloss (.75th percentile on NEWT curve)
○ Infants #48 h of age at discharge6,9
○ Infants with risk factors forhyperbilirubinemia
• Within 48–72 h of discharge for allother breastfed infants2,6
Key components of breastfeedingassessment and documentation10,11
• Risk factors for breastfeedingproblems (Table 2)
• Latch (including maternalcomfort)
• Milk transfer• Clinical jaundice• Urine output and notation ofuric acid crystals if present
• Stool output, color, andtransition
• Evidence of milk transfer such as audiblemilk swallowing, level of maternalcomfort while feeding, satisfaction ofinfant after a feed, and softening ofbreasts after feeding compared withbefore feeding (softening is difficult toassess before lactogenesis II)
• With equivocal physical findings, obtainpre- and postfeeding weights on anaccurate (65 g) infant scale12
• Mother: nipple pain, nippletrauma, compression,engorgement, and mastitisrequire thorough assessment andmanagement
• Infant: infants with wt loss$7% ofbirth wt at 5–6 d after birthshould be monitored every24–48 h in the outpatient settinguntil wt gain is well established2
Clinical pearls • Before discharge, infant’s wtand percentage wt loss shouldbe documented by using NEWT(https://www.newbornweight.org)
• Telemedicine (telelactationconsultation), hospital- or home-basedbreastfeeding follow-up clinics mayoffset lack of available weekendvisits13,14
• Mothers with persistentbreastfeeding problems should beassessed for a latch problem
—, not applicable.
2 FELDMAN-WINTER et al by guest on October 15, 2021www.aappublications.org/newsDownloaded from

here to improve milk production andtransfer are not effective, and long-term supplementation with eitherdonor milk or infant formula ismedically necessary.
Milk expression is safely andeffectively achieved by both manualand mechanical methods and can beused to maintain milk supply in theevent of separation from the infant.27
Hand expression also facilitates milktransfer for the infant learning tobreastfeed; both latch and an effectivesuckling pattern are key. Amongmothers of term infants who werefeeding poorly, those randomlyassigned to hand expression versuselectric pumps were more likely tostill be breastfeeding at 2 months(96.1% vs 72.7%; P = .02).28
Infrequent or inadequate signalingdue to ineffective or infrequentbreastfeeding or milk expression maytrigger the autocrine-paracrinemechanisms of halting milkproduction and dismantling themammary gland architecture.29
Milk removal, either via directbreastfeeding or expression, isessential for continuation of milkproduction.
Some women experienceengorgement with lactogenesis II.There is limited evidence regardingthe optimal management ofengorgement. However, becausesevere engorgement can impedeinfant removal of milk, breastfeedingmothers should learn handexpression and reverse pressuresoftening, which is positive pressureto the central subareolar region,30
before discharge from maternitycare.31,32 If a mother is unable tohand express or her infant is unableto latch, she may require a breastmassage33 and/or use of an electricbreast pump.
The components of a comprehensivebreastfeeding assessment aredescribed in Table 1.12,34 It isimportant to note that a mother’spumped milk volume may be an
TABLE 2 Mother, Infant, and Systems-Level Risk Factors for Breastfeeding Difficulties
Risk Factors for Breastfeeding Difficulties
PrenatalPast medical historyMaternal obesity (BMI $ 30)Significant medical problems (eg, thyroid disease, diabetes or insulin resistance, cystic fibrosis,
polycystic ovarian syndrome)Extremes of maternal age (eg, adolescent mother or older than 40 y)15
Any previous breast surgery, including cosmetic procedures (important to ask, not always obviouson examination)
Previous breast abscessLack of noticeable breast enlargement or tenderness during puberty or pregnancy
Past gynecology historyHistory of infertilityConception by assisted reproductive technology
Past obstetrics historyPrimiparityHistory of previous breastfeeding problems, early breastfeeding cessation, or breastfed infant
with slow wt gainPostpartum plansIntention to both breastfeed and bottle-feed or formula feed at ,6 wkIntention to use pacifiers or dummies and/or artificial nipples or teats at ,6 wkEarly intention or necessity to return to school or workIntended use of hormonal contraceptives before breastfeeding is well established (6 wk)
MedicationsInadequate counseling on maternal medication safety in lactation
Social historyPsychosocial problems (eg, depression, anxiety, lack of social support for breastfeeding)
Physical examination findingsVariation in breast appearance (marked asymmetry, hypoplastic, tubular)Flat, inverted, or large nipples
IntrapartumProlonged laborLong induction or augmentation of laborUse of medications during labor (benzodiazepines, morphine, or others) that can cause drowsiness
in the newbornPeripartum complications (eg, maternal hyperglycemia in labor, postpartum hemorrhage,
hypertensive disorders of pregnancy, infection)Infant initial assessmentLow birth wt, small for gestational age, or premature birth (,37 wk)Early-term birth (37 1 0/7–38 1 6/7 wk)MultiplesOral anatomic abnormalities (eg, cleft lip or palate, macroglossia, micrognathia, tight frenulum or
ankyloglossia)Medical problems (eg, hypoglycemia, infection, jaundice, respiratory distress, birth trauma, birth
asphyxia)Neurologic problems (eg, genetic syndromes, hypertonia, hypotonia)
Early postnatal careMother signs and symptomsPerceived inadequate milk supplySore nipples or evidence of nipple compression with feedingsFailure of secretory activation or lactogenesis stage II (milk did not noticeably come in by 72 h
post partum); this may be difficult to evaluate if the mother and infant are discharged from thehospital in the first 24–48 h post partum
Mother unable to hand express colostrumNeed for breastfeeding aids or appliances (such as nipple shields, breast pumps, or supplemental
nursing systems) at the time of hospital dischargeUse of breast milk substitutes during hospital stayUse of opiate pain medications
Infant signs and symptomsPersistently sleepy infantDifficulty in latching on to 1 or both breastsIneffective or unsustained suckling
PEDIATRICS Volume 145, number 4, April 2020 3 by guest on October 15, 2021www.aappublications.org/newsDownloaded from

inaccurate estimate of milk transferbecause transfer also depends on theinfant’s capabilities. Associated riskfactors for suboptimal milk transferare listed in Table 2.
Painful latching deserves specialattention as a contributor to lowsupply, impaired milk transfer, andearly cessation of breastfeeding.35 Inan ultrasound study in whichbreastfeeding mothers with nipplepain were compared with thosewithout, nipple pain was associatedwith abnormal infant tonguemovement, restricted nipple
expansion, and lower rates of milktransfer.36 In a retrospective audit ofan Australian breastfeeding center,36% of visits were for nipple pain.37
A US study revealed that nipple painand trauma were among the mostfrequently cited reasons for earlyweaning. In a study of .1600 womenwith singleton births, ∼10% hadnipple pain that persisted atpostpartum day 7; 72% wasattributed to inappropriatepositioning and latching, 23% totongue-tie in the infant, and 4% tooversupply. Women who receivedtreatment recovered within 1 to 2
weeks, and 6-week exclusivebreastfeeding rates were no differentfrom those of mothers without nipplepain.38 Although high-qualityrandomized controlled trials (RCTs)are needed, frenotomy has beenshown to reduce maternal nipplepain in infants with congenitalankyloglossia.39 There is no evidencethat any one topical treatment issuperior40; the mainstay ofmanagement for nipple pain andfissuring is assistance withpositioning and latching.41
NEONATAL WEIGHT AND OUTPUTASSESSMENT
Healthy newborns experiencephysiologic weight loss afterbirth,42,43 which, in the exclusivelybreastfed infant, typically plateaus asthe mother’s milk transitions fromlactogenesis I to lactogenesis II. Theaddition of infant formula, either asa supplement or in the form ofexclusive formula feeding, isassociated with rapid weight gain.This nonphysiologic weight trajectoryis associated with childhoodobesity.44 Exclusive directbreastfeeding is inversely associatedwith the velocity of weight gainthroughout the first year of life.45
In one prospective cohort study of.300 newborns, weight gain .100 gduring the first week after birth wasindependently associated withoverweight status at age 2 (adjustedodds ratio [aOR] 2.3; 95% confidenceinterval [CI] 1.1 to 4.8).44
Early infant weight loss should beevaluated in the context of the clinicalstatus of the infant and the mother.Nomograms for newborn weight havebeen developed by using data from.100000 healthy, exclusivelybreastfed infants in California.46
Individual infant weights can beplotted against these nomograms byusing the Newborn Early WeightTool (NEWT) (https://www.newbornweight.org). Weight losstrajectory over time, combined withclinical information, provides a robust
TABLE 2 Continued
Risk Factors for Breastfeeding Difficulties
Excessive infant wt loss (.7%–10% of birth wt in the first 48 h or .75th percentile for age andmode of delivery on NEWT curves [https://www.newbornweight.org/])
Supplementation with breast milk substitutesEarly pacifier useSigns of infant dehydration:Lack of bowel movementsUrate crystals in diaperDry mucous membranesLoss of skin turgorSunken eyesDepressed anterior fontanelleThready radial pulseCold extremities
Health systemMother-infant separationNonadherence to BFHI-based maternity practicesHospital discharge before effective breastfeeding establishedDischarge from the hospital at ,48 h of age
Adapted from Evans A, Marinelli KA, Taylor JS; Academy of Breastfeeding Medicine. ABM clinical protocol #2: guidelines forhospital discharge of the breastfeeding term newborn and mother: “The going home protocol,” revised 2014. BreastfeedMed. 2014;9(1):4.
TABLE 3 Risk Factors for Hypoglycemia
Risk Factors
Large for gestational ageSmall for gestational ageInfant of a mother with diabetes (including gestational diabetes)Premature (,37 wk) or postmature delivery (.41 wk 6 d)Symptoms of hypoglycemia (jitteriness, cyanosis, seizures, apneic episodes, tachypnea, weak or high-pitched cry, floppiness or lethargy, poor feeding, and eye-rolling)
Family history of congenital errors in metabolism that may be associated with hypoglycemiaCongenital syndromes (eg, Beckwith-Wiedemann syndrome), abnormal physical features (eg, midlinefacial malformations, microphallus) that may be associated with hypoglycemia
Perinatal stress (asphyxia)
Adapted from Thornton PS, Stanley CA, De Leon DD, et al; Pediatric Endocrine Society. Recommendations from the PediatricEndocrine Society for evaluation and management of persistent hypoglycemia in neonates, infants, and children. J Pediatr.2015;167(2):241 and Adamkin DH; Committee on Fetus and Newborn. Postnatal glucose homeostasis in late-preterm andterm infants. Pediatrics. 2011;127(3):576.
4 FELDMAN-WINTER et al by guest on October 15, 2021www.aappublications.org/newsDownloaded from

context for evidence-based decision-making.47 Weight loss in the .75thpercentile on NEWT nomograms formode of delivery and infant ageshould prompt a thorough evaluation.
A term newborn’s weight is 75%water, compared with 60% for anadult. Urine output is usually low inthe first 1 to 2 days after birth, afterwhich a physiologic diuresis andloss of up to 7% to 10% of birthweight occurs.48,49 Insufficient milkproduction and/or transfer in theexclusively breastfed newborn cancontribute to excessive weight loss inthe first few days of life. Low milksupply, often exacerbated by poorfeeding or difficulty in suckling,correlates with elevated milk sodiumlevels.50 Exclusively breastfed infants,especially those born via cesareandelivery, are at increased risk forgreater weight loss, dehydration, andhypernatremia.51,52 In a systematic
review of hypernatremia amongbreastfed infants, significant riskfactors included weight loss .10%,cesarean delivery, primiparity, breast
anomalies, reported breastfeedingproblems, excessive prepregnancymaternal weight, delayed firstbreastfeeding, lack of previous
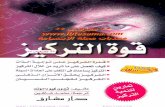
FIGURE 1Supplementation decision algorithm.
FIGURE 2Milk volume estimated by breast milk transfer over the first 6 days in vaginal and cesarean births.*Adjusted difference P , .05. Adapted from Evans KC, Evans RG, Royal R, Esterman AJ, James SL.Effect of caesarean section on breast milk transfer to the normal term newborn over the first weekof life. Arch Dis Child Fetal Neonatal Ed. 2003;88(5):F382.
PEDIATRICS Volume 145, number 4, April 2020 5 by guest on October 15, 2021www.aappublications.org/newsDownloaded from

breastfeeding experience, and lowmaternal education.53 Preventionstrategies included daily weightscoupled with lactation support duringthe first 4 to 5 days after birth.
Early weight loss nomograms forexclusively breastfed newborns canhelp identify those infants at risk forhypernatremic dehydration (HD),54,55
a rare condition characterized bylethargy, restlessness, hyperreflexia,spasticity, hyperthermia, andseizures, with an estimated incidenceof 20 to 70 per 100 000 births and upto 223 per 100 000 births amongprimiparous mothers.56 Use of chartsfor weight loss with SD scoresspecifically to detect HD, combinedwith a policy of weight checks ondays 2, 4, and 7 of life, had highsensitivity (97%) and specificity(98.5%) to detect HD.47 However,given the low incidence of HD, thepositive predictive value (PPV) ofrepeated weight checks alone wasonly 4.4%.56
Importantly, elimination patternsduring the first 2 days of life areneither sensitive nor specific asmeasures of infant intake.49 Infantsmay be voiding and stooling despiteinsufficient intake or, morecommonly, have decreased voidingand stooling compared withexclusively formula-fed infantsdespite adequate intake. In a cohortstudy of 313 infants, the frequencyof urination and stooling wassignificantly decreased amongexclusively breastfed infantscompared with exclusively formula-fed infants during the first 3 days oflife then rose and significantlysurpassed that of exclusively formula-fed infants by day 6 of life.49
Another prospective cohort study of280 mother-infant pairs examinedelimination patterns in relation toexcessive weight loss (.10%)between 72 and 96 hours afterbirth.48 The strongest associationwith weight loss .10% was with,4 stools after 72 hours or maternalperception of delayed lactogenesis II.
Although term and late-preterminfants generally pass meconiumwithin 48 hours (76%–83% ina study of 198 infants), delayedpassage of meconium can be a markerfor insufficient milk intake.57
Correlations between infants’ intakeand elimination are more reliableafter the first 3 days (lactogenesis II).
GLUCOSE STABILIZATION
To prepare for transitional energyneeds, the third-trimester fetusstores glycogen, manufacturescatecholamines, and deposits brownfat. Healthy newborns use thesestores to maintain thermoregulationand meet their energy needs throughmetabolism of brown fat and therelease of counterregulatoryhormones such as glucagon,epinephrine, cortisol, and growthhormone. Combined with declininginsulin secretion, these hormonesmobilize glucose and alternativefuels, such as lactate and ketonebodies, to support organfunctions.58,59
Because oral intake is not the mainenergy source for healthy termneonates in the first days after birth,physiologic volumes of colostrum(16 kcal/oz) are sufficient to meetmetabolic demands. As glycogenstores are depleted, coinciding withthe transition from colostrum tomature milk, newborns transitionfrom a catabolic state to reliance onenteral feeds, with approximatelyhalf of the caloric content derivedfrom fat.60
After placental detachment, neonatalglucose levels reach a physiologicnadir in the first hours after birth andthen typically rise to adult levelsa few days later. The threshold forneonatal glucose that is associatedwith neurotoxicity is unclear;a 2008 National Institutes of Healthworkshop concluded that “there is noevidence-based study to identify anyspecific plasma glucose concentration(or range of glucose values) to define
pathologic hypoglycemia.”61 Inone cohort study, treatment ofasymptomatic newborn hypoglycemiato maintain blood glucose levels.47 mg/dL had no effect oncognitive performance at 2 years;however, at 4.5 years, there weredose-dependent concerns regardingvisual motor and executive function,with the highest risk in childrenexposed to severe (,36 mg/dL),and recurrent ($3 episodes)hypoglycemia.62,63
In the first hours after birth, healthyterm neonates compensate forrelatively low glucose levels bydecreasing insulin productionand increasing glycolysis,gluconeogenesis, and ketoneproduction. Among at-risk newborns,early skin-to-skin care plus earlyfeeding and blood glucose assessmentat 90 minutes supports glucosehomeostasis and is associated withdecreased risk of hypoglycemia andNICU admission.64 In a Cochranereview, early skin-to-skin contactincreased glucose levels by 10.49(95% CI 8.39 to 12.59) mg/dL or 0.6(0.5 to 0.7) mmol/L.65 Conversely,practices that separate the motherand infant and delay the first feedingincrease hypoglycemia risk.
Glucose monitoring is recommendedfor infants with risk factors (Table 3)and for any infant who exhibitssymptoms of hypoglycemia.66
Because operational thresholds fortreating hypoglycemia and targetglucose levels are not defined, clinicalrecommendations vary. Infants whorequire early or more frequentfeedings should be supported tobreastfeed and/or receive expressedmilk. Authors of multiple studiesconfirm the benefits of using glucosegel rather than formula as an initialtreatment of low glucose levels, andthis practice has become increasinglycommonplace.67–73 Some institutionsuse pasteurized donor humanmilk (PDHM) as a treatment ofhypoglycemia; however, there are, asyet, no published studies describing
6 FELDMAN-WINTER et al by guest on October 15, 2021www.aappublications.org/newsDownloaded from

outcomes of this practice. The optionof antenatal milk expression forlower-risk women with preexisting orgestational diabetes may also beconsidered because this techniquemay preserve exclusive breastfeedingwithout adversely affecting perinataloutcomes.74 Infants requiringintravenous glucose shouldbreastfeed, when able, during thetherapy.
Persistent or late-onset hypoglycemia(.48 hours after birth) can occur inthe setting of congenital endocrinedisorders or, more commonly,perinatal stress due to birth asphyxia,intrauterine growth restriction,maternal preeclampsia,75 orpersistent problems establishingbreastfeeding.76 Infants with theserisk factors may be more vulnerableto insufficient feeding, so skilledassessment is essential.
HYPERBILIRUBINEMIA
Management of hyperbilirubinemia inthe exclusively breastfed newborndepends on whether the excess inbilirubin is pathologic or physiologic.Neonatal bilirubin levels rise afterbirth because of physiologicimmaturity of glucuronyl transferase,which is exaggerated with eachdecreasing week of gestational age.Exclusively breastfed infants havehigher serum bilirubin levels thanformula-fed infants, possibly becauseof differences in fluid intake andbilirubin excretion and increasedenterohepatic resorption ofbilirubin.77 Some individuals mayalso have a genetic predisposition tohigher bilirubin levels.78,79 Bilirubinis an antioxidant, and it has beenhypothesized that moderate increasesin bilirubin levels may be protectivefor the transition to extrauterinelife.77,80
In contrast, pathologichyperbilirubinemia resulting frominsufficient breastfeeding, sometimesreferred to as breastfeeding jaundice,is better defined as suboptimal intake
jaundice.77 In the United States andCanada, it is recommended that allneonates undergo bilirubin riskscreening at least once beforehospital discharge.81 The Academy ofBreastfeeding Medicine and the AAPadvise the use of Bhutani curves toassess risk and need for treatment ofhyperbilirubinemia; clinical tools areavailable on mobile deviceapplications.77,81,82 This approach hasled to a decrease in severe pathologichyperbilirubinemia83; however,concerns for overtreatment and thepotential harm of phototherapy havearisen recently.84 Using subthresholdbilirubin levels to initiatephototherapy as a mechanism toprevent readmission is notrecommended because this approachincreases length of stay and results inmany infants receiving unnecessarytreatment to reduce each case ofreadmission.85
Breastfed infants withhyperbilirubinemia requireassessment of milk production andtransfer, feeding frequency, andneonatal weight loss.86–91 If there ispathologic hyperbilirubinemia, andinfant intake at the breast issufficient, exclusive breastfeedingshould be continued while the infantreceives phototherapy. Althoughsupplementation with infant formulamay decrease the bilirubin leveland risk of readmission forphototherapy,85 it will also interferewith the establishment andcontinuation of breastfeeding.92 Ifintake at the breast is insufficientand supplementation is medicallynecessary, expressed maternal milk ispreferred. Despite the current lack ofdata on its benefits in reducinghyperbilirubinemia in term infants,the use of PDHM to preserveexclusive human-milk feeding isincreasing.93
Phototherapy for neonatal jaundiceand concerns about insufficient milkcan be anxiety provoking for parents,even in a supportive environment,and can be disruptive to successful
breastfeeding.94 Practices tominimize mother-infant separation,including providing phototherapy inthe same room and maintaining safeskin-to-skin care with the infant’smother, also promote exclusivebreastfeeding.95
IMMUNE DEVELOPMENT AND THEMICROBIOME
Early colostrum and exclusivebreastfeeding establish an optimaland intact immune system. Unlikeinfant formula, human milk hasa dynamic composition of bothmacro- and micronutrients that varieswithin a feed, diurnally, and over thecourse of lactation. Protectiveproteins abound in human milk,including lactoferrin, secretoryimmunoglobulin A, transforminggrowth factor-b, and a-lactalbumin.These factors promote developmentof the infant’s immune system.96
Additionally, lactoferrin has uniqueantibacterial properties important inthe prevention of sepsis. Uniquenonnutritive oligosaccharides that arespecific to the mother-infant pair’sshared environment and exposuresprevent binding of pathogenicbacteria and promote a healthymicrobiome in the gut.97 Differencesin immune cell distributions based onneonatal diet can be detected through6 months of age, with natural killercells most significantly affected.98
During vaginal birth, the newborn’sintestine and mucosal surfaces arecolonized with maternal microbesthat act synergistically with bioactivefactors in mother’s milk to establisha robust lymphoid follicle repletewith a healthy balance of T helpercells.99,100 Surgical delivery isassociated with aberrant colonization,which may lead to differences in themother’s milk microbiome101 onlypartially restored by vaginalsecretions.102 Formulasupplementation may effect themost change in the newborn’smicrobiome103,104 and immunedevelopment. These basic science
PEDIATRICS Volume 145, number 4, April 2020 7 by guest on October 15, 2021www.aappublications.org/newsDownloaded from

findings are supported by clinicalstudies.
Given the multiple mechanismsthrough which exclusive human milkimpacts gut development, formulasupplementation should always beavoided when the mother’s ownmilk is available. Although anexploratory study of early limitedsupplementation with extensivelyhydrolyzed formula followed bya return to exclusive breastfeedingdid not reveal differences in thedeveloping microbiome (N = 15),105
a longitudinal study among infantsexclusively breastfeeding at 3 months(N = 579) revealed alterations in themicrobiome among infants exposedto formula as neonates (n = 179).106
Just as antimicrobial stewardshiprequires appropriate use ofantibiotics,107 supplementationstewardship requires judicious use offormula when medically indicated.
SUPPLEMENTATION
A systematic review of healthy, term,breastfed newborns revealed nobenefit from routine supplementationwith foods or fluids in the earlypostpartum period.108 These findingsare consistent with consensusrecommendations for exclusivebreastfeeding for the first 6 months,followed by continued breastfeedingwith the addition of complementaryfoods until at least 12 months ofage.2,109–111 Early introduction ofsupplemental formula is associatedwith a greater than twofold increasein risk of early cessation ofbreastfeeding even when controllingfor confounding variables.112–114
Among almost 1500 women in theInfant Feeding Practices Study II, onlyearly exclusive breastfeedingremained significant for achievingintended breastfeeding duration (aOR2.3; 95% CI 1.8 to 3.1) afteradjustment for relevant hospitalpractices.113 This finding may be duein part to the supply and demandnature of milk production and the
role of suckling, oxytocin release, andmilk removal in establishing lactation.
If supplemental feeds are medicallyindicated, they should beaccompanied by manual ormechanical milk expression,recognizing that direct breastfeedingusually provides more complete milkremoval.115 In a pilot RCT (N = 40),early limited formulasupplementation for infants with$5% weight loss increased exclusivebreastfeeding at 3 months postpartum.116 In a subsequent largerstudy (N = 164), early limitedsupplementation did not affectoverall breastfeeding at 1 or6 months but slightly increased ratesof formula use at 1 month (36.7% vs22.4%; P = .08),105 decreasedbreastfeeding at 12 months (30% vs48%; risk difference 218% [CI234% to 23%]), and shortened thetime to breastfeeding cessation(hazard ratio 0.65; 95% CI 0.43 to0.97).117
Because evidence continues to accruethat supplementation in the first daysafter birth has major healthrisks,103,106 judicious use ofsupplementation is a critical goal,with a return to exclusivity wheneverpossible. If supplementation isindicated (Fig 1), options in order ofpreference are (1) expressed milkfrom the infant’s own mother,4 (2)PDHM, and (3) commercial infantformulas. The potential risks andbenefits of these options should beconsidered in the context of theinfant’s age, the volume required, andthe impact on the establishment ofbreastfeeding.4
Methods of supplemental feedinginclude spoon or cup feeds,supplemental nursing systems,syringe feeds, and paced bottle feeds.Methods should be tailored to stafftraining and family preferences.7
Among late-preterm newborns, thereis evidence that some may be moresusceptible to feeding problems whensupplemented via a bottle; in an RCT
in which the 2 methods werecompared, cup feeding wasassociated with a longer duration ofexclusive breastfeeding comparedwith bottle-feeding.118 Among termnewborns, the manner in whichsupplementation is delivered,whether a bottle or alternativedevices, has no apparent impact oncontinuation of breastfeeding.119 Ifthe supplement is the mother’s ownexpressed milk, avoidance of bottlesand nipples may preserve a longerduration of breastfeeding, especiallyamong late-preterm newborns.120
To ensure milk removal, which is keyto establishing a milk supply,a mother should be assisted toexpress milk each time her infant issupplemented, even if the infant isalso “practicing” at the breast.4
“Hands on” pumping, combiningbreast massage with pumping, hasbeen shown to increase milkproduction in mothers of preterminfants who are hospitalized.121
HEALTH SYSTEM INTERVENTIONS: THEBABY-FRIENDLY HOSPITAL INITIATIVE
Physiologic early infant feeding isfacilitated by keeping mothers closeto their infants, beginning with skin-to-skin care immediately after birthand continuing with 24-hourrooming-in and feeding on cue. Theseare core practices of the recentlyupdated World Health Organization’sTen Steps to Successful Breastfeedingof the Baby-Friendly HospitalInitiative (BFHI).7 Feeding on cue or“responsive feeding” is associatedwith more frequent breastfeedingthroughout the day, more exclusivebreastfeeding up to 6 months andbeyond,122–124 and decreasedlikelihood of abnormal rapid weightgain in infancy.125
Several major health organizations,including the US Preventive ServicesTask Force and the Agency forHealthcare Research and Quality, havegenerated systematic reviews andquality improvement (QI) reports
8 FELDMAN-WINTER et al by guest on October 15, 2021www.aappublications.org/newsDownloaded from

that demonstrate the positive impactof the BFHI on breastfeedingoutcomes.10,13,14 Implementation ofmaternity care practices aligned withany component of the BFHI isassociated with improved in-hospitaland postdischarge breastfeedingrates.11,13,126 Best Fed Beginningsincreased exclusive breastfeedinginitiation from 39% to 61% (t = 9.72;P , .001) at 89 hospitals over2 years.127 The Community andHospitals Advancing Maternity CarePractices initiative reported that theBFHI helped to reduce racialdisparities in breastfeeding insouthern US states.128
Since the initial implementation ofthe BFHI, safety concerns haveemerged, including case reports ofinadvertent bed-sharing, suffocation,falls, and increased risk of neonataljaundice.3,129 In this context, theWorld Health Organization conductedan extensive evidence-basedreview.7,130 Key differences in therevised Ten Steps include highlightingthe Code of Marketing of BreastmilkSubstitutes, the need to collectongoing data, a focus on safety andsurveillance (especially as it relatesto skin-to-skin care and rooming-in),and acknowledgment that thereis insufficient evidence to limitpacifiers and other artificialnipples.
Step 10 of the BFHI requires a directconnection between the deliveryhospital and the community forongoing support. Referral foroutpatient support as well asprovision of contact information for
those who can manage breastfeedingproblems is paramount.
LIMITATIONS AND IMPLICATIONS FORFUTURE RESEARCH
Given the importance of exclusivebreastfeeding for maternal and childhealth, both intent and initiation areincreasing. However, maternalconditions linked with delayedlactogenesis, such as advancedmaternal age, obesity, and fertilitytreatment, are increasingly common.Priority research areas to helpfamilies meet their breastfeedinggoals include accurate identificationof women with risk factors for delayor absence of lactogenesis, moresensitive methods of identifying at-risk newborns, and exploration of theimplications of early limited formulasupplementation on infant outcomessuch as ontogeny of the immunesystem and the microbiome, maternalself-efficacy, and continuedbreastfeeding.
CONCLUSIONS
Health care professionals’ support iscritical for families to meet theirinfant feeding goals and achieveoptimal health outcomes. Allphysicians who care for new mothersand infants need skills to evaluateearly breastfeeding, performmaternal and infant risk stratification,understand the range of potentialinterventions in the context of therisk/benefit ratio of supplementation,and ensure appropriate follow-up.
Most mothers can produce adequatecolostrum and mature milk, and most
newborns are able to breastfeedexclusively. Nevertheless, conditionsthat require medical supplementationare common and important torecognize. The decision tosupplement with infant formularequires thoughtful analysis of therisks and benefits, with considerationof the family’s informed choice. Early-term and late-preterm newborns areat a higher risk of complications.Therefore, more careful monitoring,detailed assessments, and case-basedinterventions are warranted. Furtherresearch is needed to identify the bestmethods to support exclusivebreastfeeding in high-riskpopulations.
ACKNOWLEDGMENT
We thank Delali Lougou fororganizing the articles used in thisarticle to provide the originalframework for the authors’ review.
ABBREVIATIONS
AAP: American Academy ofPediatrics
aOR: adjusted odds ratioBFHI: Baby-Friendly Hospital
InitiativeCI: confidence intervalHD: hypernatremic dehydrationNEWT: Newborn Early
Weight ToolPDHM: pasteurized donor
human milkPPV: positive predictive valueQI: quality improvementRCT: randomized controlled trial
DOI: https://doi.org/10.1542/peds.2018-3696
Accepted for publication Aug 6, 2019
Address correspondence to Lori Feldman-Winter, MD, MPH, Department of Pediatrics, Cooper Medical School, Rowan University and Children’s Regional Hospital at
Cooper, Cooper University Health Care, 401 Haddon Ave, Room 366, Camden, NJ 08103. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2020 by the American Academy of Pediatrics
PEDIATRICS Volume 145, number 4, April 2020 9 by guest on October 15, 2021www.aappublications.org/newsDownloaded from

FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Feldman-Winter L, Szucs K, Milano A,Gottschlich E, Sisk B, Schanler RJ.National trends in pediatricians’practices and attitudes aboutbreastfeeding: 1995 to 2014.Pediatrics. 2017;140(4):e20171229
2. Section on Breastfeeding.Breastfeeding and the use of humanmilk. Pediatrics. 2012;129(3). Availableat: www.pediatrics.org/cgi/content/full/129/3/e827
3. Feldman-Winter L, Goldsmith JP;Committee on Fetus and Newborn;Task Force on Sudden Infant DeathSyndrome. Safe sleep and skin-to-skincare in the neonatal period for healthyterm newborns. Pediatrics. 2016;138(3):e20161889
4. Kellams A, Harrel C, Omage S, GregoryC, Rosen-Carole C. ABM clinicalprotocol #3: supplementary feedingsin the healthy term breastfed neonate,revised 2017. Breastfeed Med. 2017;12(4):188–198
5. Wight N, Marinelli KA; Academy ofBreastfeeding Medicine. ABM clinicalprotocol #1: guidelines for bloodglucose monitoring and treatment ofhypoglycemia in term and late-preterm neonates, revised 2014.Breastfeed Med. 2014;9(4):173–179
6. Evans A, Marinelli KA, Taylor JS;Academy of Breastfeeding Medicine.ABM clinical protocol #2: guidelinesfor hospital discharge of thebreastfeeding term newborn andmother: “The going home protocol,”revised 2014. Breastfeed Med. 2014;9(1):3–8
7. World Health Organization; UnitedNations Children’s Fund.Implementation Guidance: Protecting,Promoting and SupportingBreastfeeding in Facilities ProvidingMaternity and Newborn Services – TheRevised Baby-Friendly HospitalInitiative. Geneva, Switzerland: WorldHealth Organization; 2018
8. Crippa BL, Colombo L, Morniroli D,et al. Do a few weeks matter? Late
preterm infants and breastfeedingissues. Nutrients. 2019;11(2):E312
9. Tjora E, Karlsen LC, Moster D,Markestad T. Early severe weight lossin newborns after discharge fromregular nurseries. Acta Paediatr. 2010;99(5):654–657
10. Feltner C, Weber RP, Stuebe A,Grodensky CA, Orr C, Viswanathan M.Breastfeeding Programs and Policies,Breastfeeding Uptake, and MaternalHealth Outcomes in DevelopedCountries. Rockville, MD: Agency forHealthcare Research and Quality (US);2018
11. Pérez-Escamilla R, Hromi-Fiedler AJ,Gubert MB, Doucet K, Meyers S, DosSantos Buccini G. Becomingbreastfeeding friendly index:development and application forscaling-up breastfeeding programmesglobally. Matern Child Nutr. 2018;14(3):e12596
12. Haase B, Barreira J, Murphy PK, MuellerM, Rhodes J. The development of anaccurate test weighing technique forpreterm and high-risk hospitalizedinfants. Breastfeed Med. 2009;4(3):151–156
13. Pérez-Escamilla R, Martinez JL, Segura-Pérez S. Impact of the Baby-friendlyHospital Initiative on breastfeeding andchild health outcomes: a systematicreview. Matern Child Nutr. 2016;12(3):402–417
14. Patnode CD, Henninger ML, Senger CA,Perdue LA, Whitlock EP. Primary careinterventions to support breastfeeding:updated evidence report andsystematic review for the US PreventiveServices Task Force [publishedcorrection appears in JAMA. 2016;316(20):2155]. JAMA. 2016;316(16):1694–1705
15. Colombo L, Crippa BL, Consonni D, et al.Breastfeeding determinants in healthyterm newborns. Nutrients. 2018;10(1):E48
16. Evans KC, Evans RG, Royal R, EstermanAJ, James SL. Effect of caesareansection on breast milk transfer to thenormal term newborn over the firstweek of life. Arch Dis Child FetalNeonatal Ed. 2003;88(5):F380–F382
17. Munblit D, Treneva M, Peroni DG, et al.Immune components in human milk areassociated with early infantimmunological health outcomes:a prospective three-country analysis.Nutrients. 2017;9(6):E532
18. Lai CT, Gardner H, Geddes D.Comparison of inductively coupledplasma optical emission spectrometrywith an ion selective electrode todetermine sodium and potassiumlevels in human milk. Nutrients. 2018;10(9):E1218
19. Division of Nutrition, Physical Activity,and Obesity, National Center for ChronicDisease Prevention and HealthPromotion, Centers for Disease Controland Prevention. Results: breastfeedingand infant feeding practices. 2014.Available at: https://www.cdc.gov/breastfeeding/data/ifps/results.htm.Accessed February, 11, 2019
20. Dewey KG, Nommsen-Rivers LA, HeinigMJ, Cohen RJ. Risk factors forsuboptimal infant breastfeedingbehavior, delayed onset of lactation,and excess neonatal weight loss.Pediatrics. 2003;112(3 pt 1):607–619
21. de Jersey SJ, Mallan K, Forster J,Daniels LA. A prospective study ofbreastfeeding intentions of healthyweight and overweight women aspredictors of breastfeeding outcomes.Midwifery. 2017;53:20–27
22. Matias SL, Nommsen-Rivers LA, Creed-Kanashiro H, Dewey KG. Risk factors forearly lactation problems amongPeruvian primiparous mothers. MaternChild Nutr. 2010;6(2):120–133
23. Preusting I, Brumley J, Odibo L, SpatzDL, Louis JM. Obesity as a predictor ofdelayed lactogenesis II. J Hum Lact.2017;33(4):684–691
10 FELDMAN-WINTER et al by guest on October 15, 2021www.aappublications.org/newsDownloaded from

24. Nommsen-Rivers LA. Does insulinexplain the relation between maternalobesity and poor lactation outcomes?An overview of the literature. Adv Nutr.2016;7(2):407–414
25. Hurst NM. Recognizing and treatingdelayed or failed lactogenesis II.J Midwifery Womens Health. 2007;52(6):588–594
26. Neifert M, Bunik M. Overcoming clinicalbarriers to exclusive breastfeeding.Pediatr Clin North Am. 2013;60(1):115–145
27. Becker GE, Smith HA, Cooney F. Methodsof milk expression for lactating women.Cochrane Database Syst Rev. 2016;(9):CD006170
28. Flaherman VJ, Gay B, Scott C, Avins A,Lee KA, Newman TB. Randomised trialcomparing hand expression with breastpumping for mothers of termnewborns feeding poorly. Arch Dis ChildFetal Neonatal Ed. 2012;97(1):F18–F23
29. Weaver SR, Hernandez LL. Autocrine-paracrine regulation of the mammarygland. J Dairy Sci. 2016;99(1):842–853
30. YouTube. Reverse pressure softening(RPS). 2019. Available at: https://www.youtube.com/watch?v=cbBTyG3grt4.Accessed February 5, 2020
31. Cotterman KJ. Reverse pressuresoftening: a simple tool to prepareareola for easier latching duringengorgement. J Hum Lact. 2004;20(2):227–237
32. Berens P, Brodribb W. ABM clinicalprotocol #20: engorgement, revised2016. Breastfeed Med. 2016;11(4):159–163
33. Witt AM, Bolman M, Kredit S. Mothersvalue and utilize early outpatienteducation on breast massage and handexpression in their self-management ofengorgement. Breastfeed Med. 2016;11(9):433–439
34. Meier P, Patel AL, Wright K, Engstrom JL.Management of breastfeeding duringand after the maternity hospitalizationfor late preterm infants. Clin Perinatol.2013;40(4):689–705
35. Odom EC, Li R, Scanlon KS, Perrine CG,Grummer-Strawn L. Reasons for earlierthan desired cessation ofbreastfeeding. Pediatrics. 2013;131(3).
Available at: www.pediatrics.org/cgi/content/full/131/3/e726
36. McClellan HL, Kent JC, Hepworth AR,Hartmann PE, Geddes DT. Persistentnipple pain in breastfeeding mothersassociated with abnormal infant tonguemovement. Int J Environ Res PublicHealth. 2015;12(9):10833–10845
37. Kent JC, Ashton E, Hardwick CM, et al.Nipple pain in breastfeeding mothers:incidence, causes and treatments. IntJ Environ Res Public Health. 2015;12(10):12247–12263
38. Puapornpong P, Paritakul P,Suksamarnwong M, Srisuwan S,Ketsuwan S. Nipple pain incidence, thepredisposing factors, the recoveryperiod after care management, and theexclusive breastfeeding outcome.Breastfeed Med. 2017;12(3):169–173
39. O’Shea JE, Foster JP, O’Donnell CP, et al.Frenotomy for tongue‐tie in newborninfants. Cochrane Database Syst Rev.2017;(3):CD011065
40. Dennis CL, Jackson K, Watson J.Interventions for treating painfulnipples among breastfeeding women.Cochrane Database Syst Rev. 2014;(12):CD007366
41. Niazi A, Rahimi VB, Soheili-Far S, et al. Asystematic review on prevention andtreatment of nipple pain and fissure:are they curable? J Pharmacopuncture.2018;21(3):139–150
42. Chantry CJ, Nommsen-Rivers LA,Peerson JM, Cohen RJ, Dewey KG.Excess weight loss in first-bornbreastfed newborns relates tomaternal intrapartum fluid balance.Pediatrics. 2011;127(1). Available at:www.pediatrics.org/cgi/content/full/127/1/e171
43. Grossman X, Chaudhuri JH, Feldman-Winter L, Merewood A. Neonatal weightloss at a US Baby-Friendly Hospital.J Acad Nutr Diet. 2012;112(3):410–413
44. Feldman-Winter L, Burnham L,Grossman X, Matlak S, Chen N,Merewood A. Weight gain in the firstweek of life predicts overweight at2 years: a prospective cohort study.Matern Child Nutr. 2018;14(1):e12472
45. Azad MB, Vehling L, Chan D, et al; CHILDStudy Investigators. Infant feeding andweight gain: separating breast milk
from breastfeeding and formula fromfood. Pediatrics. 2018;142(4):e20181092
46. Flaherman VJ, Schaefer EW, KuzniewiczMW, Li SX, Walsh EM, Paul IM. Earlyweight loss nomograms for exclusivelybreastfed newborns. Pediatrics. 2015;135(1). Available at: www.pediatrics.org/cgi/content/full/135/1/e16
47. van Dommelen P, Boer S, Unal S, vanWouwe JP. Charts for weight loss todetect hypernatremic dehydration andprevent formula supplementing. Birth.2014;41(2):153–159
48. Nommsen-Rivers LA, Heinig MJ, CohenRJ, Dewey KG. Newborn wet and soileddiaper counts and timing of onset oflactation as indicators of breastfeedinginadequacy. J Hum Lact. 2008;24(1):27–33
49. Chen CF, Hsu MC, Shen CH, et al.Influence of breast-feeding on weightloss, jaundice, and waste elimination inneonates. Pediatr Neonatol. 2011;52(2):85–92
50. Murase M, Wagner EA, J Chantry C,Dewey KG, Nommsen-Rivers LA. Therelation between breast milk sodium topotassium ratio and maternal report ofa milk supply concern. J Pediatr. 2017;181:294–297.e3
51. Manganaro R, Mamì C, Marrone T,Marseglia L, Gemelli M. Incidence ofdehydration and hypernatremia inexclusively breast-fed infants. J Pediatr.2001;139(5):673–675
52. Ferrández-González M, Bosch-Giménez V,López-Lozano J, Moreno-López N,Palazón-Bru A, Cortés-Castell E. Weightloss thresholds to detect earlyhypernatremia in newborns. J Pediatr(Rio J). 2019;95(6):689–695
53. Lavagno C, Camozzi P, Renzi S, et al.Breastfeeding-associatedhypernatremia: a systematic review ofthe literature. J Hum Lact. 2016;32(1):67–74
54. Bilgin LK, Akcay F, Altinkaynak K,Altindag H. Hypernatremia in breastfednewborns: a review of 149 cases. J TropPediatr. 2012;58(4):332–334
55. Oddie SJ, Craven V, Deakin K, WestmanJ, Scally A. Severe neonatalhypernatraemia: a population basedstudy. Arch Dis Child Fetal Neonatal Ed.2013;98(5):F384–F387
PEDIATRICS Volume 145, number 4, April 2020 11 by guest on October 15, 2021www.aappublications.org/newsDownloaded from

56. Boer S, Unal S, van Wouwe JP, vanDommelen P. Evidence based weighingpolicy during the first week to preventneonatal hypernatremic dehydrationwhile breastfeeding. PLoS One. 2016;11(12):e0167313
57. Bekkali N, Hamers SL, Schipperus MR,et al. Duration of meconium passage inpreterm and term infants. Arch DisChild Fetal Neonatal Ed. 2008;93(5):F376–F379
58. Ward Platt M, Deshpande S. Metabolicadaptation at birth. Semin FetalNeonatal Med. 2005;10(4):341–350
59. Aylott M. The neonatal energy triangle.Part 1: metabolic adaptation. PaediatrNurs. 2006;18(6):38–42, quiz 43
60. Deshpande S, Ward Platt M. Theinvestigation and management ofneonatal hypoglycaemia. Semin FetalNeonatal Med. 2005;10(4):351–361
61. Hay WW Jr., Raju TN, Higgins RD, KalhanSC, Devaskar SU. Knowledge gaps andresearch needs for understanding andtreating neonatal hypoglycemia:workshop report from Eunice KennedyShriver National Institute of ChildHealth and Human Development.J Pediatr. 2009;155(5):612–617
62. McKinlay CJ, Alsweiler JM, Ansell JM,et al; CHYLD Study Group. Neonatalglycemia and neurodevelopmentaloutcomes at 2 years. N Engl J Med.2015;373(16):1507–1518
63. McKinlay CJD, Alsweiler JM, Anstice NS,et al; Children With Hypoglycemia andTheir Later Development (CHYLD) StudyTeam. Association of neonatal glycemiawith neurodevelopmental outcomes at4.5 years. JAMA Pediatr. 2017;171(10):972–983
64. LeBlanc S, Haushalter J, Seashore C,Wood KS, Steiner MJ, Sutton AG. Aquality-improvement initiative to reduceNICU transfers for neonates at risk forhypoglycemia. Pediatrics. 2018;141(3):e20171143
65. Moore ER, Bergman N, Anderson GC,Medley N. Early skin-to-skin contact formothers and their healthy newborninfants. Cochrane Database Syst Rev.2016;(11):CD003519
66. Adamkin DH; Committee on Fetus andNewborn. Postnatal glucosehomeostasis in late-preterm and terminfants. Pediatrics. 2011;127(3):575–579
67. Ter M, Halibullah I, Leung L, Jacobs S.Implementation of dextrose gel in themanagement of neonatalhypoglycaemia. J Paediatr Child Health.2017;53(4):408–411
68. Stewart CE, Sage EL, Reynolds P.Supporting ‘Baby Friendly’: a qualityimprovement initiative for themanagement of transitional neonatalhypoglycaemia. Arch Dis Child FetalNeonatal Ed. 2016;101(4):F344–F347
69. Barber RL, Ekin AE, Sivakumar P,Howard K, O’Sullivan TA. Glucose gel asa potential alternative treatment toinfant formula for neonatalhypoglycaemia in Australia. IntJ Environ Res Public Health. 2018;15(5):E876
70. Harding JE, Hegarty JE, Crowther CA,Edlin R, Gamble G, Alsweiler JM.Randomised trial of neonatalhypoglycaemia prevention with oraldextrose gel (hPOD): study protocol.BMC Pediatr. 2015;15:120
71. Hegarty JE, Harding JE, Gamble GD,Crowther CA, Edlin R, Alsweiler JM.Prophylactic oral dextrose gel fornewborn babies at risk of neonatalhypoglycaemia: a randomisedcontrolled dose-finding trial (the pre-hPOD study). PLoS Med. 2016;13(10):e1002155
72. Harris DL, Weston PJ, Signal M, ChaseJG, Harding JE. Dextrose gel forneonatal hypoglycaemia (the SugarBabies Study): a randomised, double-blind, placebo-controlled trial. Lancet.2013;382(9910):2077–2083
73. Newnam KM, Bunch M. Glucose gel asa treatment strategy for transientneonatal hypoglycemia. Adv NeonatalCare. 2017;17(6):470–477
74. Forster DA, Moorhead AM, Jacobs SE,et al. Advising women with diabetes inpregnancy to express breastmilk in latepregnancy (Diabetes and Antenatal MilkExpressing [DAME]): a multicentre,unblinded, randomised controlled trial.Lancet. 2017;389(10085):2204–2213
75. Thornton PS, Stanley CA, De Leon DD,et al; Pediatric Endocrine Society.Recommendations from the PediatricEndocrine Society for evaluation andmanagement of persistenthypoglycemia in neonates, infants, andchildren. J Pediatr. 2015;167(2):238–245
76. Singh P, Upadhyay A, Sreenivas V,Jaiswal V, Saxena P. Screening forhypoglycemia in exclusively breastfedhigh-risk neonates. Indian Pediatr. 2017;54(6):477–480
77. Flaherman VJ, Maisels MJ; Academy ofBreastfeeding Medicine. ABM clinicalprotocol #22: guidelines formanagement of jaundice in thebreastfeeding infant 35 weeks or moreof gestation-revised 2017. BreastfeedMed. 2017;12(5):250–257
78. Huang A, Tai BC, Wong LY, Lee J, Yong EL.Differential risk for early breastfeedingjaundice in a multi-ethnic Asian cohort.Ann Acad Med Singapore. 2009;38(3):217–224
79. Sato H, Uchida T, Toyota K, et al.Association of neonatalhyperbilirubinemia in breast-fed infantswith UGT1A1 or SLCOs polymorphisms.J Hum Genet. 2015;60(1):35–40
80. Hansen R, Gibson S, De Paiva Alves E,et al. Adaptive response of neonatalsepsis-derived group B Streptococcusto bilirubin. Sci Rep. 2018;8(1):6470
81. American Academy of PediatricsSubcommittee on Hyperbilirubinemia.Management of hyperbilirubinemia inthe newborn infant 35 or more weeksof gestation. Pediatrics. 2004;114(1):297–316
82. Bhutani VK; Committee on Fetus andNewborn; American Academy ofPediatrics. Phototherapy to preventsevere neonatal hyperbilirubinemia inthe newborn infant 35 or more weeksof gestation. Pediatrics. 2011;128(4).Available at: www.pediatrics.org/cgi/content/full/128/4/e1046
83. Mah MP, Clark SL, Akhigbe E, et al.Reduction of severe hyperbilirubinemiaafter institution of predischargebilirubin screening. Pediatrics. 2010;125(5). Available at: www.pediatrics.org/cgi/content/full/125/5/e1143
84. Newman TB, Wu YW, Kuzniewicz MW,Grimes BA, McCulloch CE. Childhoodseizures after phototherapy. Pediatrics.2018;142(4):e20180648
85. Wickremasinghe AC, Kuzniewicz MW,McCulloch CE, Newman TB. Efficacy ofsubthreshold newborn phototherapyduring the birth hospitalization inpreventing readmission for
12 FELDMAN-WINTER et al by guest on October 15, 2021www.aappublications.org/newsDownloaded from

phototherapy. JAMA Pediatr. 2018;172(4):378–385
86. Chang RJ, Chou HC, Chang YH, et al.Weight loss percentage prediction ofsubsequent neonatalhyperbilirubinemia in exclusivelybreastfed neonates. Pediatr Neonatol.2012;53(1):41–44
87. Chen YJ, Chen WC, Chen CM. Riskfactors for hyperbilirubinemia inbreastfed term neonates. Eur J Pediatr.2012;171(1):167–171
88. Chen YJ, Yeh TF, Chen CM. Effect ofbreast-feeding frequency onhyperbilirubinemia in breast-fed termneonate. Pediatr Int. 2015;57(6):1121–1125
89. Hassan B, Zakerihamidi M. Thecorrelation between frequency andduration of breastfeeding and theseverity of neonatal hyperbilirubinemia.J Matern Fetal Neonatal Med. 2018;31(4):457–463
90. Huang HC, Yang HI, Chang YH, et al.Model to predict hyperbilirubinemia inhealthy term and near-term newbornswith exclusive breast feeding. PediatrNeonatol. 2012;53(6):354–358
91. Salas AA, Salazar J, Burgoa CV, De-Villegas CA, Quevedo V, Soliz A.Significant weight loss in breastfedterm infants readmitted forhyperbilirubinemia. BMC Pediatr. 2009;9:82
92. Chantry CJ, Dewey KG, Peerson JM,Wagner EA, Nommsen-Rivers LA. In-hospital formula use increases earlybreastfeeding cessation among first-time mothers intending to exclusivelybreastfeed. J Pediatr. 2014;164(6):1339–1345.e5
93. Sen S, Benjamin C, Riley J, et al. Donormilk utilization for healthy infants:experience at a single academic center.Breastfeed Med. 2018;13(1):28–33
94. Chu KH, Sheu SJ, Hsu MH, Liao J, ChienLY. Breastfeeding experiences ofTaiwanese mothers of infants withbreastfeeding or breast milk jaundicein certified baby-friendly hospitals.Asian Nurs Res (Korean Soc Nurs Sci).2019;13(2):154–160
95. Szucs KA, Rosenman MB. Family-centered, evidence-based phototherapydelivery. Pediatrics. 2013;131(6).
Available at: www.pediatrics.org/cgi/content/full/131/6/e1982
96. Munblit D, Boyle RJ, Warner JO. Factorsaffecting breast milk composition andpotential consequences fordevelopment of the allergic phenotype.Clin Exp Allergy. 2015;45(3):583–601
97. Pacheco AR, Barile D, Underwood MA,Mills DA. The impact of the milkglycobiome on the neonate gutmicrobiota. Annu Rev Anim Biosci. 2015;3(1):419–445
98. Andersson Y, Hammarström ML,Lönnerdal B, Graverholt G, Fält H,Hernell O. Formula feeding skewsimmune cell composition towardadaptive immunity compared tobreastfeeding. J Immunol. 2009;183(7):4322–4328
99. Stiemsma LT, Michels KB. The role of themicrobiome in the developmentalorigins of health and disease.Pediatrics. 2018;141(4):e20172437
100. Tamburini S, Shen N, Wu HC, ClementeJC. The microbiome in early life:implications for health outcomes. NatMed. 2016;22(7):713–722
101. Cabrera-Rubio R, Mira-Pascual L, MiraA, Collado MC. Impact of mode ofdelivery on the milk microbiotacomposition of healthy women. J DevOrig Health Dis. 2016;7(1):54–60
102. Dominguez-Bello MG, De Jesus-LaboyKM, Shen N, et al. Partial restoration ofthe microbiota of cesarean-born infantsvia vaginal microbial transfer. Nat Med.2016;22(3):250–253
103. Carvalho-Ramos II, Duarte RTD, BrandtKG, Martinez MB, Taddei CR.Breastfeeding increases microbialcommunity resilience. J Pediatr (Rio J).2018;94(3):258–267
104. Stewart CJ, Ajami NJ, O’Brien JL, et al.Temporal development of the gutmicrobiome in early childhood from theTEDDY study. Nature. 2018;562(7728):583–588
105. Flaherman VJ, Narayan NR, Hartigan-O’Connor D, Cabana MD, McCulloch CE,Paul IM. The effect of early limitedformula on breastfeeding, readmission,and intestinal microbiota: a randomizedclinical trial. J Pediatr. 2018;196:84–90.e1
106. Forbes JD, Azad MB, Vehling L, et al;Canadian Healthy Infant LongitudinalDevelopment (CHILD) StudyInvestigators. Association of exposureto formula in the hospital andsubsequent infant feeding practiceswith gut microbiota and risk ofoverweight in the first year of life. JAMAPediatr. 2018;172(7):e181161
107. MacDougall C, Schwartz BS, Kim L,Nanamori M, Shekarchian S, Chin-HongPV. An interprofessional curriculum onantimicrobial stewardship improvesknowledge and attitudes towardappropriate antimicrobial use andcollaboration. Open Forum Infect Dis.2017;4(1):ofw225
108. Smith HA, Becker GE. Early additionalfood and fluids for healthy breastfedfull-term infants. Cochrane DatabaseSyst Rev. 2016;(8):CD006462
109. American Academy of FamilyPhysicians. Breastfeeding, familyphysicians supporting (position paper).2014. Available at: https://www.aafp.org/about/policies/all/breastfeeding-support.html. Accessed April 24, 2018
110. American College of Obstetricians andGynecologists’ Committee on ObstetricPractice; Breastfeeding Expert WorkGroup. Committee opinion No. 658:optimizing support for breastfeeding aspart of obstetric practice. ObstetGynecol. 2016;127(2):e86–e92
111. Chantry CJ, Eglash A, Labbok M. ABMposition on breastfeeding-revised 2015.Breastfeed Med. 2015;10(9):407–411
112. Hall RT, Mercer AM, Teasley SL, et al. Abreast-feeding assessment score toevaluate the risk for cessation ofbreast-feeding by 7 to 10 days of age.J Pediatr. 2002;141(5):659–664
113. Perrine CG, Scanlon KS, Li R, Odom E,Grummer-Strawn LM. Baby-friendlyhospital practices and meetingexclusive breastfeeding intention.Pediatrics. 2012;130(1):54–60
114. Nguyen TT, Withers M, Hajeebhoy N,Frongillo EA. Infant formula feeding atbirth is common and inverselyassociated with subsequentbreastfeeding behavior in Vietnam.J Nutr. 2016;146(10):2102–2108
115. Alekseev NP, Ilyin VI. The mechanics ofbreast pumping: compression stimuli
PEDIATRICS Volume 145, number 4, April 2020 13 by guest on October 15, 2021www.aappublications.org/newsDownloaded from

increased milk ejection. BreastfeedMed. 2016;11(7):370–375
116. Flaherman VJ, Aby J, Burgos AE, Lee KA,Cabana MD, Newman TB. Effect of earlylimited formula on duration andexclusivity of breastfeeding in at-riskinfants: an RCT. Pediatrics. 2013;131(6):1059–1065
117. Flaherman VJ, Cabana MD, McCullochCE, Paul IM. Effect of early limitedformula on breastfeeding duration inthe first year of life: a randomizedclinical trial. JAMA Pediatr. 2019;173(8):729–735
118. Yilmaz G, Caylan N, Karacan CD, Bodur _I,Gokcay G. Effect of cup feeding andbottle feeding on breastfeeding in latepreterm infants: a randomizedcontrolled study. J Hum Lact. 2014;30(2):174–179
119. Howard CR, Howard FM, Lanphear B,et al. Randomized clinical trial ofpacifier use and bottle-feeding orcupfeeding and their effect onbreastfeeding. Pediatrics. 2003;111(3):511–518
120. Flint A, New K, Davies MW. Cup feedingversus other forms of supplementalenteral feeding for newborn infants
unable to fully breastfeed. CochraneDatabase Syst Rev. 2016;(8):CD005092
121. Morton J, Hall JY, Wong RJ, Thairu L,Benitz WE, Rhine WD. Combining handtechniques with electric pumpingincreases milk production in mothersof preterm infants. J Perinatol. 2009;29(11):757–764
122. Little EE, Legare CH, Carver LJ.Mother–infant physical contactpredicts responsive feeding among U.S.Breastfeeding mothers. Nutrients. 2018;10(9):E1251
123. Radwan H. Patterns and determinantsof breastfeeding and complementaryfeeding practices of Emirati mothers inthe United Arab Emirates. BMC PublicHealth. 2013;13(1):171
124. Spaeth A, Zemp E, Merten S, Dratva J.Baby-Friendly Hospital designation hasa sustained impact on continuedbreastfeeding. Matern Child Nutr. 2018;14(1):e12497
125. Mihrshahi S, Battistutta D, Magarey A,Daniels LA. Determinants of rapidweight gain during infancy: baselineresults from the NOURISH randomisedcontrolled trial. BMC Pediatr. 2011;11(1):99
126. Barrera CM, Beauregard JL, Nelson JM,Perrine CG. Association of maternitycare practices and policies with in-hospital exclusive breastfeeding in theUnited States. Breastfeed Med. 2019;14(4):243–248
127. Feldman-Winter L, Ustianov J, AnastasioJ, et al. Best fed beginnings:a nationwide quality improvementinitiative to increase breastfeeding.Pediatrics. 2017;140(1):e20163121
128. Merewood A, Bugg K, Burnham L, et al.Addressing racial inequities inbreastfeeding in the southern UnitedStates. Pediatrics. 2019;143(2):e20181897
129. Shan KH, Wang TM, Lin MC. Associationbetween rooming-in policy andneonatal hyperbilirubinemia. PediatrNeonatol. 2019;60(2):186–191
130. World Health Organization. Guideline:protecting, promoting and supportingbreastfeeding in facilities providingmaternity and newborn services. 2017.Available at: www.who.int/nutrition/publications/guidelines/breastfeeding-facilities-maternity-newborn/en/.Accessed December 20, 2018
14 FELDMAN-WINTER et al by guest on October 15, 2021www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2018-3696 originally published online March 11, 2020; 2020;145;Pediatrics
Alison M. StuebeandG. Lee, Mary J. Terrell, Lawrence Noble, Angela R. Maynor, Joan Younger Meek
Lori Feldman-Winter, Ann Kellams, Sigal Peter-Wohl, Julie Scott Taylor, Kimberly35 Weeks≥Infants
Evidence-Based Updates on the First Week of Exclusive Breastfeeding Among
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/145/4/e20183696including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/145/4/e20183696#BIBLThis article cites 111 articles, 22 of which you can access for free at:
Subspecialty Collections
_subhttp://www.aappublications.org/cgi/collection/preventative_medicinePreventive Medicinehttp://www.aappublications.org/cgi/collection/breastfeeding_subBreastfeedinghttp://www.aappublications.org/cgi/collection/nutrition_subNutritionfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on October 15, 2021www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2018-3696 originally published online March 11, 2020; 2020;145;Pediatrics
Alison M. StuebeandG. Lee, Mary J. Terrell, Lawrence Noble, Angela R. Maynor, Joan Younger Meek
Lori Feldman-Winter, Ann Kellams, Sigal Peter-Wohl, Julie Scott Taylor, Kimberly35 Weeks≥Infants
Evidence-Based Updates on the First Week of Exclusive Breastfeeding Among
http://pediatrics.aappublications.org/content/145/4/e20183696located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2020/03/09/peds.2018-3696.DCSupplementalData Supplement at:
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2020has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on October 15, 2021www.aappublications.org/newsDownloaded from







![TRAINING - LS ACADEMY...Filling data gaps: methodology, updates and insights in Real World Evidence REAL WORLD DATA AND REAL WORLD EVIDENCE U 4622 [ TRAINING CALENDAR - 2020 ] PAGE](https://static.fdocuments.in/doc/165x107/5f04ddf67e708231d4101b3e/training-ls-academy-filling-data-gaps-methodology-updates-and-insights-in.jpg)