
Evidence-Based Shoulder Assessment - Cloud Object …€¦ · EVIDENCE-BASED SHOULDER ASSESSMENT...
49
EVIDENCE-BASED SHOULDER ASSESSMENT AOTA CONFERENCE 2016 DANA WASHBURN, MS, OTR/L, CKTP TM Netter 2011
Transcript of Evidence-Based Shoulder Assessment - Cloud Object …€¦ · EVIDENCE-BASED SHOULDER ASSESSMENT...

E V I D E N C E - B A S E D S H O U L D E R A S S E S S M E N T A O TA C O N F E R E N C E 2 0 1 6
DANA WASHBURN, MS, OTR/ L, CKTP T M
Netter 2011

LEARNING OBJECTIVES
• Gain evidence-based knowledge in at least five areas of
shoulder assessment
• Be aware of at least five evidence-based special tests for
the shoulder
• Be able to construct a comprehensive strategy for
evidence-based assessment of shoulder dysfunction

INTRODUCTION: SHOULDER PAIN IS A COMMON
MEDICAL CONDITION
• Shoulder pain is the third most common musculoskeletal
reason for seeking medical care (Hermans et al 2013)
• Rotator cuff disease is the most common cause of shoulder
pain seen by physicians (Hermans et al 2013)
• 1% of adults over the age of 45 present with present with
shoulder pain each year (Donnelly et al 2013)

SHOULDER DYSFUNCTION IS COMPLEX
• The shoulder has the greatest range of motion of any joint
in the body (Cooper 2014) and restriction of it can have a
significant effect on functional ability (Donnelly 2013)
• The etiology of shoulder dysfunction is often complex and
difficult to assess clinically (Donnelly 2013)
• Causality of shoulder dysfunction is difficult to quantify
yet occupational therapists are asked do this every day by
general practice doctors
COMMON TYPES OF SHOULDER DYSFUNCTION
• Acute: fracture, dislocation, muscular injury, glenoid labral
tears
• Chronic: osteoarthritis, rotator cuff tears, recurrent
dislocations (instability), biceps long head tendonitis,
rotator cuff tendonitis, adhesive capsulitis, impingement
• Neuropathic: cervical spine pathology, herpes zoster
infection, or brachial neuritis
• (Donnelly et al 2013, Durall 2013)

UPPER EXTREMITY ANATOMY REVIEW: SHOULDER COMPLEX
(COOPER 2014)
• Has the greatest range of motion (ROM) in the entire body
• Has three bones: the humerus, the clavicle, and the scapula
• Has three joints: glenohumeral, acromioclavicular, and
sternoclavicular
• Has one pseudojoint: the scapulothoracic articulation

Downloaded from: StudentConsult (on 30 January 2012 01:41 AM)
© 2005 Elsevier

Downloaded from: StudentConsult (on 30 January 2012 01:41 AM)
© 2005 Elsevier

IMPORTANCE OF ROTATOR CUFF (RC)
• Primary mover of GH joint
• Supraspinatus, infraspinatus, subscapularis, and teres minor
• Accessory muscles can be very important as well: e.g., serratus anterior causes scapular winging; lower trapezius weakness can cause elevation of the shoulder
• Supraspinatus most frequently injured

ROTATOR CUFF MUSCLES H T T P : / / P H Y S IO W O R K S . C O M . A U/ IM A G E S / IN J U R IE S -
C O N D IT IO N S / R O T A T O R% 2 0 C U F F % 2 0 M U S C L E S % 2 0 IN J U R Y . J P G

EVIDENCE-BASED SHOULDER ASSESSMENT STRATEGY:
OVERVIEW
• History of shoulder dysfunction: occupational history,
onset process (or event) and symptoms
• “Look, Feel, Move”: inspect for abnormalities during
clinical examination
• Special tests & individual muscle testing

STEP 1: PATIENT HISTORY OF SHOULDER DYSFUNCTION
(DONNELLY ET AL 2013)
• Onset: gradual or sudden?
• Symptoms: pain at rest & with movement, neurological
complaints (e.g., sensation), kinematics (joint issues and/or
instability), stiffness, & when symptoms occur, pain
pattern?

H T T P : / / W W W . T H E B O X M A G . C O M / C O N T E N T / C O N T E N T / 1 1 8 3 0 / S H O U L D E R - P A I N . J P G

H T T P : / / A T H L E T E C U L T U R E . C O M /W P -C O N T E N T / U P L O A D S / 2 0 1 3 /0 3 / 1 6 -S H O U L D E R -P A IN -6 2 0 X 3 5 0 . J P G ? B 9 3 D B 2

STEP 1: PATIENT HISTORY OF SHOULDER DYSFUNCTION
(DONNELLY ET AL 2013)
• Occupational history: ADL and IADL (especially work)
• Results of history should begin to suggest etiology

STEP 2: CLINICAL EXAMINATION
• “Look”: Check for abnormalities (bilateral shoulders are
exposed) (Limb & Limb 2014)
– Redness or swelling
– Bony prominences (e.g., scapula, clavicle)
– Muscle wasting and/or asymmetry
– Postural abnormalities: Rounded shoulders, forward head,
kyphotic thoracic spine, shoulder height differential,
bilateral shoulder elevation
– Scapular winging
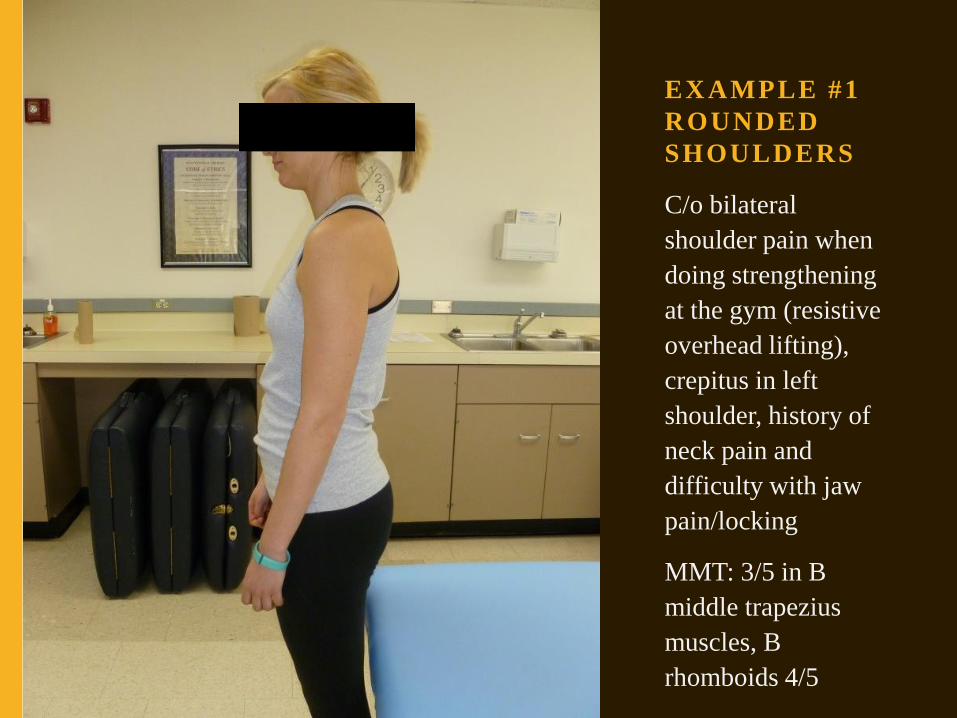
EX AMPLE #1
ROUNDED
SHOULDERS
C/o bilateral
shoulder pain when
doing strengthening
at the gym (resistive
overhead lifting),
crepitus in left
shoulder, history of
neck pain and
difficulty with jaw
pain/locking
MMT: 3/5 in B
middle trapezius
muscles, B
rhomboids 4/5

EX AMPLE #2
MUSCLE
ASYMMETRY
C/o right shoulder pain
when washing dishes
using bilateral UE’s;
Left upper trapezius
and infraspinatus are
larger than right, is a
student. Carries grocery
bags on left side.
MMT: middle trapezius
R 3+/5, L 3/5; lower
trapezius R 4/5, L 4+/5

EX AMPLE #3
SHOULDER
HEIGHT
DIFFERENTIAL
Student’s left shoulder is
higher than right, history
of initial right shoulder
injury 5 years ago during
heavy lifting with no
medical treatment; second
injury was during resistive
right shoulder horizontal
abduction with pain in
deltoid (snapping sound);
no complaints at present.
MMT results: 3+/5 R
posterior deltoid & middle
trapezius vs. 3/5 LUE

STEP 2: CLINICAL EXAMINATION
• “Feel”: Bony landmarks are palpated systematically
(Limb & Limb 2014)
– AC, SC & GH joints
– Overall palpation during movement especially when
patient reports ‘crunching’ (helps to localize crepitus as
specific region/joint)
– Neuro signs are noted

EX AMPLE #4
SCAPULAR
WINGING
Student has winging L
greater than R with
“pinching” on L side at
times with trunk
movement and
protracted kyphotic
posture; history of
dancing 15 years until
18 years old (now 25
yrs); palpation of T12 is
painful on left, no neuro
signs

STEP 2: CLINICAL EXAMINATION
• “Move”: Assess fluidity, quality, & quantity (AROM,
then PROM) (Donnelly et al 2013)
– Sternoclavicular (SC) movement: palpate SC joint &
clavicle
– Acromioclavicular (AC) movement: note any
dyskinesis especially with shoulder abduction and
horizontal abduction/adduction
– Scapulothoracic (ST) movement: note that GH to ST
movement should be 5:4 after 30 degrees of abduction
– Glenohumeral (GH) movement: all planes

STEP 2 TO STEP 3 TRANSITION
• Once analysis of Step 2 is complete the clinician should select special tests (Donnelly et al, 2013) and/or individual manual muscle testing to investigate abnormalities such as:
– Abnormal posture
– Muscle wasting
– Abnormal bone position
– Abnormal movement and joint structure
– A/PROM deficits
– Pain and neurological signs

STEP 3: SPECIAL TESTS & MMT
• Please note that to select special tests and individual muscle testing
effectively one must have basic knowledge of common shoulder
conditions for which these tests are given
• Recommended readings:
– Fundamentals of Hand Therapy: Clinical Reasoning and
Treatment Guidelines for Common Diagnoses of the Upper
Extremity (2nd Ed.), Cooper (2014), Chapter 22
– Special Tests for Orthopedic Examination (4th Ed.) by Konin et al.
(2016), Sections 1 & 2
– Muscles: Testing and Function with Posture and Pain (5th Edition)
by Kendall et al. (2005)

STEP 3: SPECIAL TESTS
• Review of research/statistical terms
– Sensitivity: Ability of a test to identify people who
have a condition
– Specificity: Ability of a test to identify people who
don’t have a condition
• Both sensitivity and specificity range from 0 to 1 with
values closer to 1 being considered more accurate
• Remember, no clinical test is 100% accurate

STEP 3: SPECIAL TESTS FOR CERVICAL SCREENING
• Note that if your patient has signs of cervical spine dysfunction you should do special tests to screen for this
• Symptoms that suggest cervical dysfunction:
– Forward head posture
– Dizziness
– Headaches (frequent – can be daily or multiple per day)
– Unilateral or bilateral shoulder pain & numbness
– Limited and/or painful cervical A/PROM
– Pain referral pattern for cervical spine dysfunction

Downloaded from: StudentConsult (on 30 January 2012 01:41 AM)
© 2005 Elsevier
CERVICAL RADICULOPATHY PATTERNS

CERVICAL DISC PAIN REFERRAL PATTERNS
Grubb, et al
2000

STEP 3: SPECIAL TESTS (CERVICAL RADICULOPATHY)
(WAINNER R. ET AL., 2003)
• Patients referred for shoulder pain sometimes have cervical radiculopathy that has been misdiagnosed
• If neuro symptoms are present special tests can be done:
– Spurling’s Test
– Distraction Test
– Upper Limb Tension Test for Median Nerve
– Ipsilateral cervical rotation AROM < 60 degrees
• If all four of the above are positive this indicates .99 specificity that patient has cervical radiculopathy and he/she could be referred to PT for cervical treatment if needed

EX AMPLE #5
C/o pain in C5-6 disc
distribution with
corresponding forward
head posture
History: Aggressive
exercise program with
“plyometric” pushups,
thoracic spine “went
out”; cervical rotation is
70 degrees to R, 80
degrees to L
Special Tests:
Spurling’s – negative;
Distraction – positive;
ULTT - negative

STEP 3: SPECIAL TESTS (SHOULDER)
• Special tests for the shoulder should be selected based on
history, clinical exam and symptomatology
• The following is a summary of common types of shoulder
dysfunction and evidence-based special tests for each
• Sensitivity and specificity have been converted to
percentages for ease of understanding
• Remember, special tests are positive only if specific test
criteria are met

STEP 3: SPECIAL TESTS (SHOULDER)
• AC Joint Pathology
– Sensitive Test (rules-out when negative)
• AC Joint Palpation (97%), Walton et al. 2004
– Specific Tests (rules-in when positive)
• Cross-Body Adduction (79%), Chronopoulos et al. 2004
• Active Compression Test (~95%), Chronopoulos et al. 2004,
Walton et al. 2004

STEP 3: SPECIAL TESTS (SHOULDER)
• Shoulder Impingement
– Sensitive Test (rules-out when negative)
• Neer Test (~80%), Calis et al. 2000, MacDonald et al. 2000,
Park et al. 2005
• Hawkins-Kennedy Test (~80%), Calis et al. 2000,
MacDonald et al. 2000, Park et al. 2005
– Specific Tests (rules-in when positive)
• Hawkins-Kennedy Test + painful arc + ER weakness in
neutral (~95%) Park et al. 2005

STEP 3: SPECIAL TESTS (SHOULDER)
• Anterior Instability
– Sensitive Test (rules-out when negative)
• Release/Surprise Test (~64%) Lo et al. 2004
– Specific Tests (rules-in when positive)
• Apprehension Test (>90%) Lo et al. 2004, Farber et al. 2006
• Relocation Test (>90%) Lo et al. 2004, Farber et al. 2006
• Release/Surprise Test (~64%) Lo et al. 2004, Gross &
Distefano 1997

STEP 3: SPECIAL TESTS (SHOULDER)
• Biceps Tendonitis/Pathology
– Sensitive Tests (rule-out when negative)
• Upper cut (77%) Kibler et al. 2009
– Specific Tests (rule-in when positive)
• Speed’s test (~83%) Kibler et al. 2009
• Belly Press (~83%) Kibler et al. 2009
• Anterior-Inferior Labral Pathology
– Specific Tests (rules-in when positive)
• Crank Test + history of popping, clicking, or catching (91%) Walsworth et al. 2008

STEP 3: SPECIAL TESTS (SHOULDER)
• Supraspinatus Tear
– Specific Tests (rules-in when positive)
• Drop Arm Test (~90%) Calis et al. 2000, Murrell &
Walton 2001, Park et al. 2005
• Infraspinatus Tear
– Specific Tests (rules-in when positive)
• External Rotation Lag Sign (~90%), Park et al.
2005, Miller et al. 2008, Walch et al. 1998

STEP 3: SPECIAL TESTS (SHOULDER)
• Subscapularis Tear
– Sensitive Test (rules-out when negative)
• Bear Hug Test (82%) Barth et al. 2012
– Specific Test (rules-in when positive)
• Lift-Off Test (~70%) Leroux et al. 1995, Barth et
al. 2012

EX AMPLE #6
C/o pain after 5 months of
working as a waitress,
postural asymmetry with left
scapula higher than right;
states “it doesn’t feel like it’s
in the right place”
History: Waitress for 10
months, carries trays on left
side but is right dominant
Special Tests/MMT: Negative
Hawkins-Kennedy & Drop
Arm but lower trapezius
MMT is 2/5, rhomboid MMT
4/5

EX AMPLE #7
C/o brief shoulder pain on
waking in the AM,
hypermobility, can’t do
standard push-up
History of Pottenger’s Saucer,
nursemaid’s elbow; brief 7/10
pain in morning if sleeping
with right shoulder in external
rotation and will get “stuck”;
received exercises from
chiropractor for improving
thoracic spine flexibility
MMT: Rhomboids R 4/5, L
5/5; Middle Trapezius R 4/5,
L 3/5; Lower Trapezius R
3+/5, L 3+/5

EX AMPLE #8
C/o pain in right UT,
deltoid & scapula at times,
forward head posture, slight
right scapular winging,
lacks fluidity of movement
during shoulder abduction
History of violin playing on
and off for 7 years
Special Tests/MMT:
Hawkins-Kennedy & Drop
Arm negative; lower traps
R 2+/5 L 3/5, rhomboids B
3+/5

PRESENTATION REVIEW: EVIDENCE-BASED OT
ASSESSMENT OF SHOULDER PATIENTS
• Step 1: Patient history of shoulder dysfunction
• Step 2: Clinical examination: “Look, Feel, Move”
• Step 3: Special tests & individual muscle tests

ACKNOWLEDGEMENTS
• A big thank you to my UWM occupational therapy students who
agreed to be photographed for this presentation
• My appreciation to my UWM colleagues and my family for their
guidance regarding this presentation

QUESTIONS? EMAIL: [email protected]


REFERENCES
• Barth, J., Audebert, S., Toussaint, B., Charousset, C., Godeneche, A., Graveleau, N., Joudet, T., Lefebvre, Y., Nove-Josserand, L., Petroff, E., Solignac, N. Scymanski, C., Pitermann, M., Thelu, C.E. (2012). Diagnosis of subscapularis tendon tears: Are available diagnostic tests pertinent for a positive diagnosis? Orthopaedics & Traumatology: Surgery & Research (98S): S178-S185
• Calis, M., Akgun, K., Birtane, M., Karacan, I., Calis, I., Tuzun, R. (2000). Diagnostic values of clinical diagnostic tests in subacromial impingement syndrome. Annals of the Rheumatic Diseases 59(1): 44-47.
• Chronopoulos, E., Kim, T., Park, H., Ashenbrenner, D., McFarland, E. (2004). Diagnostic value of physical tests for isolated chronic acromioclavicular lesions. American Journal of Sports Medicine 32: 655-661.
• Cooper, Cynthia (Ed.). (2014). Fundamentals of hand therapy: clinical reasoning and treatment guidelines for common diagnoses of the upper extremity (2nd Ed.). St. Louis: Mosby Elsevier.

REFERENCES
• Donnelly, T., Ashwin, S., MacFarlane, R., Waseem, M. (2013). Clinical assessment of
the shoulder. Open Orthopaedics Journal, 7 (Suppl 3: M3): 310-315.
• Durall, C. (2013). Evidence-based clinical examination of the shoulder complex. From
North American Seminars, Inc. continuing education course, “Comprehensive
Examination and Treatment of Shoulder Disorders: What are you missing?” Kenosha,
WI.
• Farber, A., Castillo, R., Clough, M., Bahk, M., McFarland, E. (2006). Journal of Bone
& Joint Surgery 88(7): 1467-74.
• Gross, M., Distefano, M. (1997). Anterior release test: a new test of occult shoulder
instability. Clinical Orthopaedics and Related Research Jun; (339): 105-8.
• Grubb, S., Kelly, C. (2000). Cervical discography: clinical implications from 12 years
of experience. Spine 25 (11): 1382-1389.

REFERENCES
• Hermans, J., Luime, J., Meuffels, D., Reijman, M., Simel, D., Bierma-Zeinstra, S.
(2013). Does this patient with shoulder pain have rotator cuff disease? The rational
clinical examination systematic review. Journal of the American Medical Association
310(8): 837-847.
• Kilber, W., Sciascia, A., Hester, P., Dome, D., Jacobs, C. (2009). Clinical utility of
traditional and new tests in the diagnosis of biceps tendon injuries and superior labrum
anterior and posterior lesions in the shoulder. American Journal of Sports Medicine 37:
1840-1847.
• Leroux, J., Thomas, E., Bonnell, F., Blotman, F. (1995). Diagnostic value of clinical
tests for shoulder impingement syndrome. Revue du Rheumatisme, English Edition 62:
423-8.
• Limb, D., Limb, R. (2014). Clinical assessment of the shoulder. Archives of
Orthopaedic & Trauma Surgery 28(6): 355-364.

REFERENCES
• Lo, I., Nonweiler, B., Woolfrey, M., Litchfield, R., Kirkley, A. (2004). An evaluation of
the apprehension, relocation, and surprise tests for anterior shoulder instability.
American Journal of Sports Medicine 32(2): 301-307.
• MacDonald, P., Clark P., Sutherland, K. (2000). An analysis of the diagnostic accuracy
of the Hawkins and Neer subacromial impingement signs. Journal of Shoulder and
Elbow Surgery 9(4): 299-301.
• Miller, C., Forrester, G., Lewis, J. (2008). The validity of the lag signs in diagnosing
full-thickness tears of the rotator cuff: a preliminary investigation. Archives of
Physical Medicine and Rehabilitation Jun; 89(6): 1162-8.
• Murrell, G., Walton, J. (2001). Diagnosis of rotator cuff tears. Lancet Mar 10; 357
(9258): 769-70.
• Netter, F. (2011). Atlas of human anatomy (5th Ed.) Philadelphia: Saunders Elsevier.

REFERENCES
• Park, H., Yokota, A., Gill, H., El Rassi, G., McFarland E. (2005). Diagnostic accuracy of clinical tests for the different degrees of subacromial impingement syndrome. Journal of Bone & Joint Surgery (American) Jul; 87(7): 1446-55.
• Wainner r. et al. (2003). Reliability and Diagnostic Accuracy of the Clinical Examination and Patient Self-Report Measures for Cervical Radiculopathy. Spine 1 January 2003, Vol.28(1), pp.52-62.
• Walch, G., Boulahia, A., Calderone, S. (1998). The ‘dropping’ and ‘hornblower’s’ signs in evaluation of rotator-cuff tears. Journal of Bone & Joint Surgery (British) 80: 624-8.
• Walsworth, M. Doukas, W., Murphy, K., Mielcarek, B., Michener, L. (2008). Reliability and diagnostic accuracy of history and physical examination for diagnosing glenoid labral tears. American Journal of Sports Medicine Jan; 36(1): 162-8.
• Walton, J. Mahajan, S. Paxinos, A., Marshall, J., Bryant, C., Shnier, R., Quinn, R., Murrell, G. (2004). Diagnostic values of tests for acromioclavicular joint pain. Journal of Bone & Joint Surgery (American) 86: 807-812.


















