Evidence-based Practices (EBPs) in Community Treatment Programs: EBPs are just one piece of the pie...
39
Evidence-based Practices (EBPs) in Community Treatment Programs: EBPs are just one piece of the pie American Psychological Association Conference San Francisco 2007 Michael S. Levy, Ph.D. Michael S. Levy, Ph.D. CAB Health & Recovery Services, Inc. CAB Health & Recovery Services, Inc. Peabody, MA Peabody, MA
-
Upload
elaine-burke -
Category
Documents
-
view
216 -
download
0
Transcript of Evidence-based Practices (EBPs) in Community Treatment Programs: EBPs are just one piece of the pie...

Evidence-based Practices (EBPs) in Community Treatment Programs: EBPs are just one piece of the pie
American Psychological Association ConferenceSan Francisco 2007
Michael S. Levy, Ph.D.Michael S. Levy, Ph.D.
CAB Health & Recovery Services, Inc.CAB Health & Recovery Services, Inc.
Peabody, MAPeabody, MA

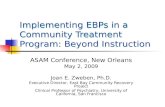
Extratherapeutic Change, 40%
Techniques, 15%
Expectancy (placebo effects),
15%
Therapeutic Relationship, 30%
Key Factors Relevant to Client Change Processes
Lambert, M.J. (1992). Implications of Outcome Research for Psychotherapy Integration. In J.C. Norcross & M. R. Goldstein (Eds.), Handbook of Psychotherapy Integration (pp. 94-129). New York: Basic Books.

• ““Psychotherapy manuals are helpful for Psychotherapy manuals are helpful for training and research. In particular, they training and research. In particular, they enhance the internal validity of comparative enhance the internal validity of comparative outcome studies, facilitate treatment integrity, outcome studies, facilitate treatment integrity, ensure the possibility of replication, and ensure the possibility of replication, and provide a systematic way of training and provide a systematic way of training and supervising therapists. At the same time, supervising therapists. At the same time, manuals are also associated with some untold manuals are also associated with some untold negative effects. There is no conclusive negative effects. There is no conclusive evidence that manuals improve treatment evidence that manuals improve treatment outcomes or that they should be required in outcomes or that they should be required in practice.” (Norcross, Beutler, & Levant, practice.” (Norcross, Beutler, & Levant, Evidence-based Practice in Mental Health, Evidence-based Practice in Mental Health, 2006)2006)

• ““Manualizing psychological Manualizing psychological interventions as if they were interventions as if they were independent of those administering and independent of those administering and receiving them does not reflect what is receiving them does not reflect what is known about psychotherapy outcome.” known about psychotherapy outcome.” (Duncan & Miller, 2006).(Duncan & Miller, 2006).

• In looking at individual drug counseling In looking at individual drug counseling (IDC) in NIDA’s Collaborative Cocaine (IDC) in NIDA’s Collaborative Cocaine Treatment Study, it was found that in Treatment Study, it was found that in cases when the alliance was strong, cases when the alliance was strong, counselor adherence did not much counselor adherence did not much matter; those patients typically improved. matter; those patients typically improved. However, for cases in which the alliance However, for cases in which the alliance was weak, adherence did matter. Those was weak, adherence did matter. Those patients improved more when their patients improved more when their counselors adhered moderately to IDC counselors adhered moderately to IDC principles than when the counselors were principles than when the counselors were either minimally or highly adherent either minimally or highly adherent (Barber, et al., Psychotherapy Research, (Barber, et al., Psychotherapy Research, 16, 229-240, 2006).16, 229-240, 2006).

• ““It makes good sense to give It makes good sense to give priority to EBTs, particularly within priority to EBTs, particularly within this era of fiscal austerity. We owe this era of fiscal austerity. We owe it to our clients to provide the best it to our clients to provide the best possible treatment within available possible treatment within available resources.” (Miller, Zweben, and resources.” (Miller, Zweben, and Johnson, JSAT, 29, 267-276, 2005).Johnson, JSAT, 29, 267-276, 2005).

• “…“…in community-based settings in community-based settings there is often not enough money to there is often not enough money to recruit and maintain a workforce recruit and maintain a workforce qualified to provide evidence-qualified to provide evidence-based treatments” (Expert Panel based treatments” (Expert Panel on Juvenile Justice and Adolescent on Juvenile Justice and Adolescent Substance Abuse Treatment, April Substance Abuse Treatment, April 2007).2007).

• NIDA’s Principles of Drug Addiction Treatment:NIDA’s Principles of Drug Addiction Treatment:• No single treatment is appropriate for all No single treatment is appropriate for all
individuals.individuals.• Treatment needs to be readily available.Treatment needs to be readily available.• Effective treatment attends to multiple needs Effective treatment attends to multiple needs
of the individual, not just his or her drug use.of the individual, not just his or her drug use.• An individual’s treatment and services plan An individual’s treatment and services plan
must be assessed continually and modified as must be assessed continually and modified as necessary to ensure that the plan meets the necessary to ensure that the plan meets the person’s changing needs.person’s changing needs.
• Remaining in treatment for an adequate Remaining in treatment for an adequate period of time is critical for treatment period of time is critical for treatment effectiveness.effectiveness.
• Counseling (individual and/or group) and Counseling (individual and/or group) and other behavioral therapies are critical other behavioral therapies are critical components of effective treatment for components of effective treatment for addiction.addiction.
• Medications are an important element of Medications are an important element of treatment for many patients, especially treatment for many patients, especially when combined with counseling and when combined with counseling and other behavioral therapies.other behavioral therapies.
• Addicted or drug-abusing individuals with Addicted or drug-abusing individuals with coexisting mental disorders should have both coexisting mental disorders should have both disorders treated in an integrated way.disorders treated in an integrated way.
• Medical detoxification is only the first stage of Medical detoxification is only the first stage of addiction treatment and by itself does little to addiction treatment and by itself does little to change long-term drug use.change long-term drug use.

• Treatment does not need to be Treatment does not need to be voluntary to be effective.voluntary to be effective.
• Possible drug use during treatment Possible drug use during treatment must be monitored continuously.must be monitored continuously.
• Treatment programs should provide Treatment programs should provide assessment for HIV/AIDS, Hepatitis B assessment for HIV/AIDS, Hepatitis B and C, tuberculosis and other infectious and C, tuberculosis and other infectious diseases, and counseling to help diseases, and counseling to help patients modify or change behaviors patients modify or change behaviors that place themselves or others at risk that place themselves or others at risk of infection.of infection.
• Recovery from drug addiction can be a Recovery from drug addiction can be a long-term process and frequently long-term process and frequently requires multiple episodes of treatment.requires multiple episodes of treatment.

Network for the Improvement of Addiction Treatment (NIATx )
Focuses on:Focuses on:• Decreasing time to obtain treatment.Decreasing time to obtain treatment.• Increasing admissions.Increasing admissions.• Decreasing no show rates.Decreasing no show rates.• Increasing treatment retention.Increasing treatment retention.• Uses rapid cycle plan-do-study-act Uses rapid cycle plan-do-study-act
projects,projects, as opposed to evidence-as opposed to evidence-based practices.based practices.

• Most all EBPs focus on the outpatient realm, so Most all EBPs focus on the outpatient realm, so what about residential treatment which can what about residential treatment which can offer 90 -250 different groups during a offer 90 -250 different groups during a treatment experience, not to mention that treatment experience, not to mention that group size can vary from 15 to 30 to 40 and group size can vary from 15 to 30 to 40 and even more. even more.
• And what about a detoxification program with And what about a detoxification program with a length of stay of 4-6 days?a length of stay of 4-6 days?
List of OMHAS Approved Evidence-Based Practices• CYT: Family Support Network (FSN) for Adolescent Cannibis CYT: Family Support Network (FSN) for Adolescent Cannibis
UsersUsers• CYT: Multidimensional Family Therapy for Adolescent CYT: Multidimensional Family Therapy for Adolescent
Cannabis Users (MDFT)Cannabis Users (MDFT)• Dialectical Behavioral Therapy (DBT) ApproachesDialectical Behavioral Therapy (DBT) Approaches• DBT adapted for adolescentsDBT adapted for adolescents• DBT for Substance Abuse (DBT-S)DBT for Substance Abuse (DBT-S)• Supported EmploymentSupported Employment• Co-occurring Disorders: Integrated Dual Diagnosis Treatment Co-occurring Disorders: Integrated Dual Diagnosis Treatment
(IDDT)(IDDT)• Illness Management and RecoveryIllness Management and Recovery• Family PsychoeducationFamily Psychoeducation• Assertive Community Treatment (ACT)Assertive Community Treatment (ACT)• Medication Management Approaches in Psychiatry (MedMAP)Medication Management Approaches in Psychiatry (MedMAP)• Stimulant Treatment of ADHD (methylphenidate, Stimulant Treatment of ADHD (methylphenidate,
dextroamphetamine, mixed salts emphetamine, pemoline)dextroamphetamine, mixed salts emphetamine, pemoline)

List of OMHAS Approved Evidence-Based Practices• Multisystemic Therapy MST)Multisystemic Therapy MST)• Cognitive Behavior Treatment for Childhood Anxiety Cognitive Behavior Treatment for Childhood Anxiety
DisordersDisorders• Trauma Focused Cognitive Behavioral TherapyTrauma Focused Cognitive Behavioral Therapy• Parent Management TrainingParent Management Training• Multi-Dimension Treatment Foster Care (MTFC)Multi-Dimension Treatment Foster Care (MTFC)• Brief Strategic Family TherapyBrief Strategic Family Therapy• Wraparound (a treatment planning process model, not a Wraparound (a treatment planning process model, not a
treatment modeltreatment model• Functional Family TherapyFunctional Family Therapy• Seeking Safety: “a present-focused therapy to help Seeking Safety: “a present-focused therapy to help
people attain safety from trauma/PTSD and substance people attain safety from trauma/PTSD and substance abuse”abuse”
• Communities that CareCommunities that Care• LifeSkills TrainingLifeSkills Training• Incredible YearsIncredible Years
List of OMHAS Approved Evidence-Based Practices• ASAM Patient Placement Criteria 2ASAM Patient Placement Criteria 2ndnd Edition-Revised Edition-Revised• The Matrix Model: Outpatient Stimulant TreatmentThe Matrix Model: Outpatient Stimulant Treatment• Methadone MaintenanceMethadone Maintenance• Motivational Enhancement Therapy Motivational Enhancement Therapy • Twelve-Step Facilitation Therapy Twelve-Step Facilitation Therapy • Cognitive Behavioral Therapy Cognitive Behavioral Therapy • Motivational InterviewingMotivational Interviewing• Motivational Enhancement Therapy/Cognitive Behavioral Motivational Enhancement Therapy/Cognitive Behavioral
Therapy (MET/CBT) for Adolescent Cannibis Users: 5 Therapy (MET/CBT) for Adolescent Cannibis Users: 5 SessionsSessions
• CYT: Motivational Enhancement Therapy and Cognitive CYT: Motivational Enhancement Therapy and Cognitive Behavioral Therapy Supplement: 7 Sessions of Cognitive Behavioral Therapy Supplement: 7 Sessions of Cognitive Behavioral Therapy for Adolescent UsersBehavioral Therapy for Adolescent Users
• CYT: The Adolescent Community Reinforcement CYT: The Adolescent Community Reinforcement Approach for Adolescent Cannibis Users (ACRA)Approach for Adolescent Cannibis Users (ACRA)
List of OMHAS Approved Evidence-Based Practices
• Motivational InterviewingMotivational Interviewing• Seeking SafetySeeking Safety

NREPP’s Evidence-based Practices• Behavioral Couples Therapy for Alcoholism and Drug AbuseBehavioral Couples Therapy for Alcoholism and Drug Abuse• Border Binge-Drinking Reduction ProgramBorder Binge-Drinking Reduction Program• Brief Marijuana Dependence CounselingBrief Marijuana Dependence Counseling• Challenging College Alcohol AbuseChallenging College Alcohol Abuse• Clinician-Based Cognitive Psychoeducational Intervention Clinician-Based Cognitive Psychoeducational Intervention
for Familiesfor Families• Cognitive Behavioral Social Skills TrainingCognitive Behavioral Social Skills Training• Cognitive Behavioral Therapy for Adolescent DepressionCognitive Behavioral Therapy for Adolescent Depression• Cognitive Behavioral Therapy for Late-Life DepressionCognitive Behavioral Therapy for Late-Life Depression• Coping CatCoping Cat• Critical Time InterventionCritical Time Intervention• DARE to be YouDARE to be You• Dialectical Behavior TherapyDialectical Behavior Therapy• Family MattersFamily Matters• Functional Adaptation Skills Training (FAST)Functional Adaptation Skills Training (FAST)• Lions Quest Skills for AdolescentsLions Quest Skills for Adolescents

NREPP’s Evidence-based Practices
• Matrix ModelMatrix Model• Multisystemic Therapy (MST) for Juvenile OffendersMultisystemic Therapy (MST) for Juvenile Offenders• Network TherapyNetwork Therapy• New Beginnings ProgramNew Beginnings Program• Parenting Through ChangeParenting Through Change• Prevention and Relationship Enhancement Program Prevention and Relationship Enhancement Program
(PREP)(PREP)• Primary ProjectPrimary Project• Program to Encourage Active, Rewarding Lives for Seniors Program to Encourage Active, Rewarding Lives for Seniors
(PEARLS)(PEARLS)• Project ALERTProject ALERT• Project EXProject EX• Project NorthlandProject Northland• Project Towards No Drug AbuseProject Towards No Drug Abuse• Responding in Peaceful and Positive Ways (RiPP)Responding in Peaceful and Positive Ways (RiPP)• Safe DateSafe Date

NREPP’s Evidence-based Practices
• Second StepSecond Step• Seeking SafetySeeking Safety• SMARTteamSMARTteam• SOS Signs of SuicideSOS Signs of Suicide• Success in Stages: Build Respect, Stop BullyingSuccess in Stages: Build Respect, Stop Bullying• Trauma Recovery and Empowerment Model (TREM)Trauma Recovery and Empowerment Model (TREM)• United States air Force Suicide Prevention ProgramUnited States air Force Suicide Prevention Program
NREPP’s Evidence-based Practices
• Motivational InterviewingMotivational Interviewing• Seeking SafetySeeking Safety

A sample of specific treatments and evidence-based practices for the treatment of addiction.• Acceptance and Commitment Therapy, Acupuncture, Affective Contra-Acceptance and Commitment Therapy, Acupuncture, Affective Contra-
Attribution Therapy, Assertive Community Treatment, Aversive Counter-Attribution Therapy, Assertive Community Treatment, Aversive Counter-conditioning, BAC Discrimination Training, Behavior Contracting, conditioning, BAC Discrimination Training, Behavior Contracting, Behavioral Marital Therapy, Behavioral Self-Control Training, Bibliotherapy, Behavioral Marital Therapy, Behavioral Self-Control Training, Bibliotherapy, Brief Intervention, Brief Strategic Family Therapy, Biofeedback, Client- Brief Intervention, Brief Strategic Family Therapy, Biofeedback, Client-Centered Therapy, Cognitive Therapy, Community Reinforcement Centered Therapy, Cognitive Therapy, Community Reinforcement Approach, Contingency Management, Covert Sensitization, Cue Exposure, Approach, Contingency Management, Covert Sensitization, Cue Exposure, Dialectical Behavior Therapy, Existential Therapy, Functional Analysis, Dialectical Behavior Therapy, Existential Therapy, Functional Analysis, Functional Family Therapy, Group Psychotherapy, Guided Self-Change, Functional Family Therapy, Group Psychotherapy, Guided Self-Change, Hypnosis, Matrix Model, Medical Management, Mindfulness, Minnesota Hypnosis, Matrix Model, Medical Management, Mindfulness, Minnesota Model, Moderation Management, Motivational Enhancement Therapy, Model, Moderation Management, Motivational Enhancement Therapy, Motivational Interviewing, Multidimensional Family Therapy, Multisystemic Motivational Interviewing, Multidimensional Family Therapy, Multisystemic Therapy, Problem Solving, Psychodynamic Psychotherapy, Therapy, Problem Solving, Psychodynamic Psychotherapy, Psychoeducation, Rational Emotive Therapy, Rational Recovery, Psychoeducation, Rational Emotive Therapy, Rational Recovery, Recreational Therapy, Relapse Prevention Relaxation Training, Secular Recreational Therapy, Relapse Prevention Relaxation Training, Secular Organization for Sobriety, Self-Monitoring, Social Skills Training, Stress Organization for Sobriety, Self-Monitoring, Social Skills Training, Stress Management, Solution-Focused Therapy, Supportive-Expressive Management, Solution-Focused Therapy, Supportive-Expressive Psychotherapy, Systematic Desensitization, Therapeutic Community, Psychotherapy, Systematic Desensitization, Therapeutic Community, Transcendental Meditation, Twelve-Step Facilitation Therapy, Women for Transcendental Meditation, Twelve-Step Facilitation Therapy, Women for Sobriety. Sobriety.
(From Miller, W., 2006, Presentation at 2006 Blending Conference, Seattle, (From Miller, W., 2006, Presentation at 2006 Blending Conference, Seattle, WA)WA)

• There must be some commonalities There must be some commonalities among EBPs that attempt to treat among EBPs that attempt to treat clients who suffer from addictive clients who suffer from addictive disorders.disorders.
• If this is true, how much energy If this is true, how much energy should be placed on training should be placed on training regarding specific EBPs or instead, regarding specific EBPs or instead, could energy be better spent on other could energy be better spent on other things?things?

EBPs that are Implemented
• Motivational interviewingMotivational interviewing• MethadoneMethadone• BuprenorphineBuprenorphine• Naltrexone, Acamprosate, Vivitrol (Soon)Naltrexone, Acamprosate, Vivitrol (Soon)• Contingency ManagementContingency Management• Matrix ModelMatrix Model• Adolescent Community Reinforcement Adolescent Community Reinforcement
Approach – Assertive Continuing Care Approach – Assertive Continuing Care (ACRA/ACC)(ACRA/ACC)
• Harm ReductionHarm Reduction• Seeking SafetySeeking Safety

Train ALL staff in overriding principles of quality treatment of addiction.• Address motivation and reinforcing factors of using Address motivation and reinforcing factors of using
drugs, and help clients to develop non-drug reinforcing drugs, and help clients to develop non-drug reinforcing activities.activities.
• Don’t be confrontational and meet clients where they Don’t be confrontational and meet clients where they are at.are at.
• Teach specific coping skills and ways to avoid a return Teach specific coping skills and ways to avoid a return to drug use.to drug use.
• Attend to the client’s social environment.Attend to the client’s social environment.• Think about psychopharmacological intervention.Think about psychopharmacological intervention.• Your relationship to the client is critical and extremely Your relationship to the client is critical and extremely
important.important.• You must attend to the multiple treatment needs that You must attend to the multiple treatment needs that
clients have.clients have.
Client Satisfaction
• An extreme focus on the importance of An extreme focus on the importance of client satisfaction and at all times, treating client satisfaction and at all times, treating clients with dignity and respect. This clients with dignity and respect. This includes nursing staff, clinical staff, and includes nursing staff, clinical staff, and milieu staff, as well as non-clinical staff.milieu staff, as well as non-clinical staff.
• Power and powerlessness trainings.Power and powerlessness trainings.• Client satisfaction surveys are given in all Client satisfaction surveys are given in all
programs, which are reviewed with all staff.programs, which are reviewed with all staff.

• All satisfaction surveys are reviewed by our All satisfaction surveys are reviewed by our senior management team and the CEO senior management team and the CEO writes a note to every staff member who writes a note to every staff member who was mentioned in a positive way.was mentioned in a positive way.
• In residential programs, there are less In residential programs, there are less negative comments about “staff attitude” negative comments about “staff attitude” or “disrespect from staff” and more positive or “disrespect from staff” and more positive comments about the “professionalism of comments about the “professionalism of staff” and “staff’s helpfulness”.staff” and “staff’s helpfulness”.
• As client satisfaction goes up, more clients As client satisfaction goes up, more clients complete treatment, go on to aftercare, and complete treatment, go on to aftercare, and less are administratively discharged.less are administratively discharged.
• If clients do not receive treatment, they will not get If clients do not receive treatment, they will not get betterbetter
• In our outpatient office, half of clients did not show for In our outpatient office, half of clients did not show for their intake appointment and another half did not come their intake appointment and another half did not come back for a second appointment.back for a second appointment.
• By beginning treatment engagement over the By beginning treatment engagement over the telephone, instituting centralized scheduling so all telephone, instituting centralized scheduling so all clinician schedules are overseen by intake staff, clinician schedules are overseen by intake staff, ensuring that all clients leave with a scheduled ensuring that all clients leave with a scheduled appointment, and conducting appt. reminder calls, we appointment, and conducting appt. reminder calls, we decreased intake no-show rates to 19% and increased decreased intake no-show rates to 19% and increased the percentage of people who return for a second the percentage of people who return for a second appointment to 95%.appointment to 95%.
Treatment engagement and Treatment engagement and decreasing no show rates.decreasing no show rates.

Administrative Discharges
• A huge issue in residential treatment.A huge issue in residential treatment.• Often for ongoing drug use, but other factors are Often for ongoing drug use, but other factors are
treatment non-compliance and getting into treatment non-compliance and getting into disagreements with staff, which can often be staff disagreements with staff, which can often be staff initiated.initiated.
• Have made this an important issue with program Have made this an important issue with program managers.managers.
• Administrative discharges must be approved by Administrative discharges must be approved by program manager.program manager.
• Review data monthly.Review data monthly.• In many cases, a return to drug use does not result in In many cases, a return to drug use does not result in
a discharge.a discharge.

Individualized Care
• Attending to the multiple needs of clients.Attending to the multiple needs of clients.• Instituted a modified ASI in all programs.Instituted a modified ASI in all programs.• Chart audits review the ASI Severity Index Chart audits review the ASI Severity Index
and ensure that identified problems are and ensure that identified problems are noted in the treatment plan and progress noted in the treatment plan and progress notes address identified problems.notes address identified problems.
• Results are given to the clinicians, in an Results are given to the clinicians, in an effort to ensure that care is individualized.effort to ensure that care is individualized.

A focus on practice-based evidence
• Obtaining feedback from clients on the Obtaining feedback from clients on the treatment that is received may be a treatment that is received may be a powerful way to enhance care.powerful way to enhance care.
• A formalized process of asking clients:A formalized process of asking clients:• Are they getting their needs met?Are they getting their needs met?• How is the quality of the How is the quality of the
therapeutic therapeutic alliance? alliance?

• Have begun an initiative on training Have begun an initiative on training clinicians to ask clients if the treatment is clinicians to ask clients if the treatment is useful and if not, what would make it more useful and if not, what would make it more useful.useful.
• In one program, clients reported that in In one program, clients reported that in many groups, there was too much cross-talk many groups, there was too much cross-talk and that more structure/information would and that more structure/information would be useful.be useful.
• Feedback was given to the clinicians and Feedback was given to the clinicians and they are working to modify their approach.they are working to modify their approach.

• Developed a survey that asked clients why they relapsed.
• Survey results were aggregated and discovered the most relevant reasons why our clients relapsed.
• Developed groups that addressed these specific reasons and trained staff.

• Are these groups evidence-based?
• No....or not yet.....
• Are these groups relevant and have they enhanced the quality of care?
• We think so........
A Culture of Continuous Performance Improvement
• All programs are involved in All programs are involved in ongoing performance ongoing performance improvement activities using rapid improvement activities using rapid cycle plan-do-study-act (PDSA) cycle plan-do-study-act (PDSA) projects.projects.
• Can focus on anything!Can focus on anything!

• Decreasing no show rates.Decreasing no show rates.• Increasing treatment retention rates.Increasing treatment retention rates.• Increasing the number of clients who get Increasing the number of clients who get
involved in an educational or vocational involved in an educational or vocational program.program.
• Decreasing episodes of aggressive acting-out.Decreasing episodes of aggressive acting-out.• Increasing referrals to the program.Increasing referrals to the program.• Increasing overall treatment compliance.Increasing overall treatment compliance.• Increasing satisfaction with group therapy.Increasing satisfaction with group therapy.

• In a short term residential treatment In a short term residential treatment program (LOS about 15-30 days), it was program (LOS about 15-30 days), it was found that 75% of people who left found that 75% of people who left treatment early did so in the first five days treatment early did so in the first five days of treatment.of treatment.
• Developed a new client fact sheet that Developed a new client fact sheet that reviewed what would occur in treatment reviewed what would occur in treatment and what to expect.and what to expect.
• Worked with Case Managers to try to meet Worked with Case Managers to try to meet with their clients more quickly.with their clients more quickly.
• Reduced the % of clients who left treatment Reduced the % of clients who left treatment early within the first five days to 37%.early within the first five days to 37%.

• In a working halfway house, we found In a working halfway house, we found that only 38% of clients were able to that only 38% of clients were able to obtain work within the first 30 days of obtain work within the first 30 days of treatment.treatment.
• Trained staff in a Job Seekers Workshop.Trained staff in a Job Seekers Workshop.• Extended the time clients needed to Extended the time clients needed to
return to the program.return to the program.• Over four months, 81% of clients were Over four months, 81% of clients were
able to obtain work within the first 30 able to obtain work within the first 30 days of treatment.days of treatment.
Summary
• The goal of evidence-based practices is The goal of evidence-based practices is to enhance the effectiveness of care and to enhance the effectiveness of care and to provide clients the best possible to provide clients the best possible treatment. treatment.
• However, the delivery of evidence-based However, the delivery of evidence-based practices is just one piece of the pie. practices is just one piece of the pie.
• Let us not forget the many other ways to Let us not forget the many other ways to enhance the quality of care that is enhance the quality of care that is delivered for clients with SUDs.delivered for clients with SUDs.