Evidence-Based Practice Project Paper - Alicia Nix, …...evidence based project. This is a level...
41
Running head: EVIDENCE-BASED PRACTICE PROJECT PAPER 1 Reducing Insulin Levels and Type Two Diabetes in Children and Adolescents Evidence-Based Practice Project Paper Alicia Nix Auburn University
Transcript of Evidence-Based Practice Project Paper - Alicia Nix, …...evidence based project. This is a level...

Running head: EVIDENCE-BASED PRACTICE PROJECT PAPER 1
Reducing Insulin Levels and Type Two Diabetes in Children and Adolescents
Evidence-Based Practice Project Paper
Alicia Nix
Auburn University

EVIDENCE-BASED PRACTICE PROJECT PAPER 2
Evidence-Based Practice Project Paper
Abstract
This paper looks at an evidence based project to reduce insulin levels in type 2 diabetes
among children and adolescents. Type 2 diabetes is a potentially devastating disease that is on
the rise among youth. Identifying this potential progression of disease in insulin resistance
youth enables intervention before the development of type 2 diabetes. This paper explores the
best related evidence in lowering insulin resistance. The most recent literature regarding insulin
resistance and adolescent was obtained and applied. For this project, the Iowa model was
implemented as a framework to guide us to the best evidence based practice. In researching for
this project the evidence narrows on three possible interventions. A healthy diet is shown to
lower insulin levels. Exercise lowers the body’s need for insulin thus lowering insulin resistance.
Although not recognized as acceptable treatment, Pharmacological intervention is also shown to
lowering insulin resistance. For this purpose of this project, we chose to focus on reducing the
insulin levels by implementing moderate 30 minutes of exercise daily. This was a grade one
recommendation. This small test of change was conducted on adolescents with elevated insulin
levels at a privately owned pediatric practice in North Alabama. . The participants signed consent
forms and 14 adolescents with elevated insulin levels were instructed and educated on daily
moderate exercise. They were contacted weekly to provide support and education. At the end of
6 weeks, they returned for a recheck on their BMI and insulin levels .Based on the outcomes of
this project, the average insulin level and BMI were reduced. Based on the outcomes, Tennessee

EVIDENCE-BASED PRACTICE PROJECT PAPER 3
Valley Pediatrics adapted their recommendations for the insulin resistant adolescent to include
the evidence based recommendation of daily moderate activity. This protocol change will greatly
benefit the insulin resistant adolescent in this practice.
Introduction
Insulin resistance is the leading cause of diabetes. Diabetes is the sixth leading cause of
death according to the CDC (2012). Type 2 diabetes is on the rise among children and
adolescents. An article regarding obesity and cardiovascular risk factors in children and
adolescents. (2008) advises on the growing number of obese adolescents. The author
notes that according to the National Center for Health Statistics, the percentage of
overweight and obese children and adolescents in the year 2000 was 15%. This figure
has quadrupled from 1963 to 1970 when the percentage was 4% in children 6 to 11 years
old and 5% in adolescents 12 to 19 years old. The article also states that up to 80% are
still obese in adulthood. This is a staggering statistic that is concerning in that obesity
frequently leads to type 2 diabetes. This is in part due to the increasing BMI among the
adolescent population. In fact two million children ages 12-19 years of age in the United States
have pre-diabetes. The alarming thing is that this is a preventable disease. If caught early type 2
diabetes is reversible (Scott, 2013). Another staggering statistic is that type diabetics are
suspected of having impaired glucose tolerance for 7-10 years prior to diagnosis (Scott, 2013, p.
190). One important fact regarding this subject is if insulin resistance is diagnosed, there is
currently no recognized treatment for children (Quinn, Baur, Garnett, & Cowell, 2010, p. 722).
There are many factors that can influence insulin resistance. Children with elevated BMI are
at risk for the development of insulin resistance (Simmons, Alexander, Ewing, & Whetzel 2012
para. 1). Unfortunately, there is an increase in BMI among the adolescent population. If

EVIDENCE-BASED PRACTICE PROJECT PAPER 4
adolescents are identified with elevated BMI’s, measures can be taken to reduce the BMI. This
intervention can either prevent diabetes or reduce insulin levels. According to the Center for
Disease control 17% of children age 2-19 year olds are above the 95th
percentile for weight
(2012). This project will explore reducing BMI with diet and exercise. For this project, the main
focus will be on children and adolescents who have elevated insulin levels to develop a treatment
plan to lower insulin levels based on the best evidence.
Exercise is an intervention that can lower insulin levels. Exercise has been proven to lower
the bodies need for insulin. Studies have shown that even exercising 30 minute a day can lower
blood sugar significantly (Farias, 2012). Most children and adolescents do not get enough
exercise therefore the body’s need for insulin may increase. In this project, educating the patient
on exercise as a way of lowering the bodies’ requirement for insulin will be explored as one
option. This will also help develop healthy lifestyles changes that may continue into adulthood.
Diet is another factor that contributes to insulin resistance in children and adolescents. Many
take in more calories than their body uses. Adolescents as a group do not make the best food
choices. Health disparity may play a role in this issue. Healthy food is more expensive than fast
food ( Niklas, 2008). If a family is on a limited budget, they may not be able to afford healthy
foods. Habits and potential causes will need to be identified and educated accordingly. Many
times this can be something that the entire family needs to have addressed. After identifying
ways to reduce insulin levels, the project focuses on education of those concepts. The children
and adolescent patient needs to understand the ramifications of the disease. The parents will also
need education regarding diabetes.
PICO Question:

EVIDENCE-BASED PRACTICE PROJECT PAPER 5
In patients under age 18 that have elevated insulin levels, what evidence-based interventions
most affect insulin levels and future risk of type 2 diabetes?
P-The population of focus is children or adolescents who had their insulin level checked due to
obesity or elevated BMI.
I-“evidence-based dietary changes, education and daily exercise” The intervention in this
population will come from evidence-based interventions for dietary changes and exercise. It will
also instruct the patient on information regarding the possible progression of insulin resistance.
C- “Compared to routine care” The current office-based instruction.
O-“lowering insulin levels and BMI” The desired outcome measurement is a lowered insulin
level and BMI. .
Framework
The Iowa Model Characteristics
The Iowa model was chosen to help implement strategies and guide development on the
entire project. After identifying the problem, the first step in the Iowa model is to examine the
research evidence. After researching the the evidence, the Iowa model recommends combining

EVIDENCE-BASED PRACTICE PROJECT PAPER 6
the evidence found along with past clinical experiences with assessment of the setting. This
allows the researcher to then set a goal based on the evidence found. This also determines
whether there is enough evidence needed to implement a practice change. The Iowa model
recommends implementing the test of change and to set a timeline to evaluate data.
In identifying the problem, labs from insulin resistant patients are easily recognized. In
searching data bases related to obesity and insulin resistance in teenagers, the research does
support a correlation between the two. The Iowa model looks at education deficits and solving
the problem at hand. Insulin resistance is often due to lack of education on the subject. It also
walks the Practitioner through the steps of the evidence-based process (Melnyk & Finout-
Overholt, 2005, p. 254). With the Iowa model, being able to reevaluate the BMI of the patient as
well as recheck their insulin level will tell us if the change is appropriate. This model will
provide the steps necessary to implement a practice change (Melnyk & Finout-Overholt, 2005).
The Iowa model has proven to be effective in a variety of settings. The Iowa model’s application
results are also consistent even when the user has little experience (Schaffer, Sandau, &Diedrik,
2012).
Iowa Model Rationale
In looking at the PICO question “In patients under age 18 that have elevated insulin levels,
what evidence-based interventions most affect insulin levels and future risk of type 2 diabetes?”
The Iowa model will question whether insulin resistance is an area of concern for a practice. A
large part of the intervention for this project is educating on diet and exercise. . The Iowa model
focuses on educational deficits. With the Iowa model, being able to reevaluate the BMI of the

EVIDENCE-BASED PRACTICE PROJECT PAPER 7
patient as well as recheck their insulin level will tell us if the change is appropriate. This model
will provide the steps necessary to implement a change (Melnyk & Fineout-Overholt, 2005). The
focus by the Iowa model on education is ideal in this particular EBP project.
Review of literature
In reviewing the Literature, an extensive search was conducted looking through Auburn
University Library. CINAHL, EBSCO and The Cochrane data bases were used. Also The
American Academy of Pediatrics website provided additional articles related to this paper. The
search terms that were used consisted of: obesity, diabetes, insulin resistance, and adolescents.
CINAHL and The American Academy of Pediatrics provided the bulk of the articles. In
searching the AAP website, 10 articles were obtained by searching “insulin resistance” The first
article is a systematic review by Quinn, Baur, Garnett, and Cowell (2010). This study looked at
five electronic databases in search of randomized trial that lasted over two months. The study
looked at using metformin alone or with lifestyle changes. This systematic review and meta-
analysis results show that Metformin along with lifestyle changes has lowering outcome on BMI
and fasting insulin. This is true in looking at children and adolescents with insulin resistance or
diabetes. With this article dealing with specific treatment of insulin resistance, this relates to the
evidence based project. This is a level one article.
A meta-analysis by Fedewa, Gist, Evans, Dishman (2013) concluded that exercise reduces
insulin resistance in children and adolescents. This randomized trial included children and
adolescents in the trial from 546 sources. One interesting fact regarding this study is that dietary
changes along with exercise were excluded from this study. This provides more concrete

EVIDENCE-BASED PRACTICE PROJECT PAPER 8
evidence on the effects of exercise on insulin resistance. It is also important to note that this
study involved all genders and races. Incorporating exercise into adolescents and children who
are either at risk or have insulin resistance was shown to have a small to moderate effect on
lowering insulin levels. This meta-analysis is relevant to this project and is a level 1 article.
An RCT by Davis. Pollock, Waller, Allison, Dennis, Gowler (2012) looked at the effects of
exercise on visceral fat and insulin resistance. This study took place in Georgia and included
counties near Augusta. The participants included in the study were adolescents who had an
elevated BMI and reported a sedentary lifestyle. The span of this study was four years. This was
a large study with 222 participants. The participants were assigned to either a 20 or a 40 minute
per day exercise regimen. After 13 weeks insulin levels and BMI were obtained. At the end of
13 weeks results showed that both groups had a lowered fasting insulin level as well as visceral
fat. This was without any dietary restrictions. This article is a level one article.
In a 12 week quasi-experimental study Monzavi, Dreimane, ,Geffner, Braun, Conrad,
Klier, Kaufman (2006) 109 adolescents that had been referred to weight management and also
had insulin resistance were invited to participate in a 12 week program. The program involved
education from a dietitian once a week on healthy eating. The program also involved
participating for 90 minutes of physical activity per week. Although not statistically significant,
there was a reduction in insulin levels in the participants. This is a level two article.
An article discussing obesity and glucose levels Lee, Yoo, Kim, Lee, Kim, Lim, Yang
(2011) focuses on connecting the relationship between the two. The purpose of this study was to
to compare the fasting serum proinsulin levels of children with normal BMI to prepubertal
overweight or obese children. This is a correlational study. A total of 109 prepubertal children

EVIDENCE-BASED PRACTICE PROJECT PAPER 9
(mean age, 8.6 years) were included in this study. The data suggested that obesity itself or insulin
resistance may independently cause fasting hyperproinsulinemia in proportion to
hyperinsulinemia in children. This result was with children that had normal glucose tolerance but
had insulin resistance. Since the project is lowering insulin resistance levels and decreasing the
incidence in development of type 2 diabetes, it is important to understand the relationship
between elevated pro insulin levels and the development of insulin resistance. This is a level IV
evidence article It is supported by other articles and therefore is relevant the project.
The key component to this EBP project is reducing insulin resistance. In an article by
Sumanmo, Schellenberg, Dryden, Vandermeer Ha, Korowynk (2014) insulin resistance and
physical activities are examined. This article provides evidence regarding how much exercise is
needed to reduce insulin levels. The purpose of this recommendation is to provide a guideline for
physical activity in children and adolescent children. These guidelines sets a precedence in the
amount of physical activity needed to help prevent type two diabetes and insulin resistance. This
is a critical guideline review. The guideline is providing a recommendation for physical activity
which is a goal of my EBP. This is an acceptable screening tool that could be used in my EBP
project. This is a level 1 article.
A cross-sectional design by Oftedal, Bru, Bjorg (2011) supports that diet and exercise
habits can improve with education. This article examines type 2 diabetes and how exercise and
diet expectations relate to the behaviors developed. This study included a postal questionnaire
that investigated diet and exercise management. This questionnaire also looked at other factors of
motivation including expectations of lab values. A sample comprising 425 adults with type two
diabetes aged between 30 and 70 completed the questionnaire. The results suggest that the
subjects had a high level of expectation of being able to follow the diet and exercise

EVIDENCE-BASED PRACTICE PROJECT PAPER 10
recommendation. It should be noted that the participants followed diet recommendations to a
greater extent than those pertaining to physical activity. The results showed that with education
subjects are motivated to improve their diet and exercise habits. This article relates to the EBP
project in that education as a factor in reducing insulin resistance. This article helps prove that
with education on the disease most subjects want to make better lifestyle choices. This is a level
IV article.
Multiple articles show a connection between type two diabetes, diet and exercise. A meta-
analysis and systematic review Sumanmo, Schellenberg, Dryden, Vandermeer, Ha, Korowynk
(2014) is a level one article that provide this evidence. Five data bases were pooled together for
the data given. The study included nine randomized controlled trials. This study show diet and
exercise can have a real impact on the prevention of type 2 diabetes demonstrating a change in
metabolic risk factors and abnormal glucose levels. The duration of the interventions ranged
from 6 to 72 months, with follow-ups between 3 and 20 years. The lifestyle interventions
included diet and exercise. The subjects also received individual and group counseling. The
studies reported positive outcomes. Most studies reported positive effects for secondary
outcomes, including changes in body composition, metabolic variables, physical activity, and
dietary intake. This is relevant to my EBP project.
Critical Appraisal of Evidence
Quality
The evidence from guidelines, meta-analysis, RCT’s and systematic reviews provide
significant evidence and relevance for my topic of lowering insulin resistance and prevention of

EVIDENCE-BASED PRACTICE PROJECT PAPER 11
type two diabetes in children and adolescents. In evaluating the use of Metformin daily on
children and adolescents with insulin resistance, we see two systematic reviews that support this
recommendation. Two systematic reviews Quinn et al. (2010) and Sumanmo et al. (2014)
support the use of Metformin to lower insulin resistance. Both of these articles provide level one
evidence. They also have supportive data relating to diet and exercise. Diet and exercise were
shown to decrease in insulin resistance and diabetes. The articles give a clinical recommendation
of engaging in daily exercise and health eating habits to lower insulin levels. The evidence in
these articles provides information that strongly suggests a correlation between diet, exercise and
pharmacological management and the treatment and prevention of insulin resistance. Both of the
above studies involved prescribing medications and lifestyles changes. The studies are clearly
stated and contain strong evidences. The possible concern of Quinn et al. (2010) is the relatively
small sample size. Another concern with Sumanmo et al. (2014) is that this study focused on
measures such a weight change and blood pressure to measure positive outcomes. There was
limited study bias in that both reviews contained a meta-analysis.
Two articles show strong evidence for the use of exercise alone. The first was a meta-
anaylsis by Fedewa et al. (2010) that provides sufficient evidence that exercise and physical
activity produces the desired result. Resistance training and aerobic exercise provided the same
outcomes of lowered insulin levels. This article combined peer-reviewed research that ranged
from 1999-2013. The second article that provided recent quality evidence regarding exercise was
a randomized controlled trial by Davis et al. (2013). In this RCT conducted from 2003-2007
physical activity of 20-40 minutes per day decreased insulin resistance in adolescents. This was
consistent regardless of race or sex.

EVIDENCE-BASED PRACTICE PROJECT PAPER 12
Quantity
In researching insulin resistance in adolescents, eight quality articles provided consistent
evidence regarding what factors provide the best evidence to lower insulin resistance. Many of
the articles overlapped in terms of recommending the three components of exercise, diet, and
pharmacological intervention. While three articles focused on diet alone. Two levels I articles
provide sufficient evidence to feel confident in making the recommendation regarding exercise.
Many of the articles provided large samples sizes which added validity to the project. The
timeframe that was reviewed varied from 6 months to a 13 year follow up.
One study showed a correlation between insulin resistance and obesity. (Lee, 2011) This
study compared fasting insulin levels in lean, overweight and obese children.
Metformin with dietary changes were shown to lower insulin sensitivity in a study by Quinn et
al. (2010). In Monzavi et al. (2006) the quasi-experimental looked at family oriented lifestyle
changes such as exercise and dietary changes to reduces insulin levels in youth. Another study
that states the benefits of diet and exercise to reduce insulin levels is Oftedal et al. (2011)
In Fedewa et al. (2013) exercise was the focus of reducing insulin resistance. The physical
activity duration ranged from 30 minutes to 90 minutes. This was based on 2-4 times weekly.
This study ranged from 6-52 weeks. An RCT by Davis et al (2012) also showed that exercise
reduces the insulin resistance in obese children and adolescents. A clinical guidelines regarding
recommendation of exercise provided expert advice in the prevention of type 2 diabetes (2000).
Another article showed that exercise and dietary changes slows the progression of type 2
diabetes Sumanmo et al. (2013).

EVIDENCE-BASED PRACTICE PROJECT PAPER 13
Consistency
The collective and combined results span over 10 years of study. The RCT’s, Systematic
reviews and Meta-analysis that are included in the both level one study provide sufficient
evidence. This ensures that multiple sources yield the same results on this subject. These studies
were conducted by Medical doctors, nurse educators, and nurses with doctorates. The common
thread among the studies was that insulin dependence and diabetes can be prevented. The
evidence shows that type 2 diabetes can be prevented. Also adolescents with elevated insulin
levels can take steps to lower them. The evidence shows that exercise will reduce insulin levels
in adolescents. The evidence also supports exercise with conjunction of diet and pharmacological
measures.
Summary of Evidence
The strongest points of the appraisal of the literature suggest that medications, education, diet,
and exercise can lower insulin levels. This project will implicate a plan based on the evidence
collected to implement changes in this population .Through these recommendations we will
strive to have the outcome of a decrease insulin level. This project will also promote healthy
lifestyle changes that will carry throughout the lifespan.
Recommendations
From the review of literature and critical appraisal of the level I and level II evidence
contained in Appendix A, key recommendations are graded. The recommendations from the
critical appraisal in Table 1 provide a synthesis of the best evidence to develop the EBP practice

EVIDENCE-BASED PRACTICE PROJECT PAPER 14
change. The clinical question intervention element can be further developed into the practice
setting for testing based on the recommendations.
Table 1
Recommendations from Critical Appraisal
PICO QUESTION: In patients under age 18 that has elevated insulin levels, what evidence-
based interventions most affect insulin levels and future risk of type 2 diabetes?
Grade Recommendations
A Engage in daily exercise at least 30 minutes to lower insulin levels:
Participate in 30 minutes of moderate activity daily
. Evidence Level 1
Davis,C.L., Pollock,N.K., Waller,J.L., Allison, J.D., Dennis, B.A.,....Gowler,

EVIDENCE-BASED PRACTICE PROJECT PAPER 15
B.A.(September, 2012) Exercise dose and diabetes risk in obese children; A
randomized trial JAMA (308)1103-1121 Retrieved from
https://www.academia.edu/1853577
Evidence Level 1
Fedewa, M.V., Gist, N. H., Evans, E.M., Dishman, R. K. (2013) Exercise and insulin
resistance in youth: A meta-analysis. Pediatrics Official Journal of the American
Academy of Pediatrics 133 (1) 163-173 doi: 10.1542/peds.2013-2718
(Evidence Level I)
Sumanmo,E.,Schellenberg,B.S, Dryden,D.,Vandermeer,M.S., Ha,C.,
Korowynk,C.(2014) Lifestyle interventions for patients with and at risk for type 2
diabetes. Annals of Internal Medicine 159 (8) 543-551 doi: 2013;159:543-551.
A Begin adolescents and children with elevated insulin levels on the drug Metformin
500 mg twice daily.
Ensure the patient understands the dosage, side effects, frequency, purpose and
possible interaction.
.(Evidence Level I) Quinn, S. M., Baur, L. A., Garnett, S. P., & Cowell, C. T. (2010,
October). Treatment of clinical insulin resistance in children: a systematic
review [article]. Obesity Reviews: An Official Journal Of The International
Association For The study Of Obesity, 11(10), 722-730.
http://dx.doi.org/10.1111/j.1467-789X.2009.00697.x
(Evidence Level I)Sumanmo,E.,Schellenberg,B.S, Dryden,D.,Vandermeer,M.S.,
Ha,C., Korowynk,C.(2014) Lifestyle interventions for patients with and at risk for

EVIDENCE-BASED PRACTICE PROJECT PAPER 16
type 2 diabetes. Annals of Internal Medicine 159 (8) 543-551 doi: 2013;159:543-551
A Increase fruits and vegetables and to decrease the sugar intake (Evidence Level I)
Sumanmo,E.,Schellenberg,B.S, Dryden,D.,Vandermeer,M.S., Ha,C.,
Korowynk,C.(2014) Lifestyle interventions for patients with and at risk for type 2
diabetes. Annals of Internal Medicine 159 (8) 543-551 doi: 2013;159:543-551.
Clinical Setting Assessment
This is a large pediatric practice that serves patients ranging from birth to college age. The
practice is made of of three pediatricians and four nurse practitioners. Three of the practitioners
are family nurse practitioners, while the fourth is a pediatric nurse practitioner. The practice is
made of a diverse range of patients. Approximately forty percent have private insurance. The
remaining sixty percent have Alabama Medicaid. Every social class is represented. The practice
is multi-racial with Caucasian, Hispanic, African-Americans, Indians and Asian Americans. The
practice has around 10,000 active patients. The practice sees about 150 patients per day. Of this
number, approximately 30 patients per day are adolescents. This leads to the conservative
number of around 7000 adolescents seen and treated per year.

EVIDENCE-BASED PRACTICE PROJECT PAPER 17
This project focuses on the treatment of insulin resistance and obesity in hopes of changing
lifestyles and preventing type 2 diabetes. This is an area of concern in this pediatric practice.
There is a mutual consensus by all providers that obesity and insulin resistance has become an
epidemic among their patients. The challenges in treatment at this clinic occur after the initial
visit. After identifying insulin resistance in lab results, the child’s caretaker is called one time
and educated regarding treatment and follows up. The fast pace nature of the office hinders the
providers from giving more education and making sure that the patient comes back in for follow
up. Also, the practice does not have a policy in place of speaking to the actual patient.
The administrator of the office states that the providers always speak to the caregiver regarding
education. Another concern is related to the follow up appt. Even though the office has a call
back system for follow ups appointment, the providers usually verbally tell the caregiver to call
back and schedule. This leaves the office with no way to ensure an appointment is ever made.
There are some potential barriers identified by the staff. Even though education is needed for
both the patient and the caretaker, families may want to convey the education to their children.
Also, many of their patients are difficult to reach. Another possible barrier is the unwillingness to
change lifestyles in a large portion of their patients. The plan itself will not cost the practice.
However, if this plan is successful they anticipate needing an RN to spend approximately two
hours per week calling patients and making follow up appointments. At the current rate that their
nurses are compensated this would add around 2,600 dollars to their yearly budget. The
administration states that the only required approval for this project would be a signed HIPPA
agreement.

EVIDENCE-BASED PRACTICE PROJECT PAPER 18
Implementation Plan
Two million children age 12 to 19 years in the United States have pre-diabetes. (Scott, 2013,
p. 190) According to the American Diabetes Association, diabetes is the 6th leading cause of
death. Another staggering statistic is that type 2 diabetics are suspected of having impaired
glucose tolerance for 7-10 years prior to diagnosis. (Scott, 2013, p. 190). That statistic includes
many adolescents. Another concern for the adolescent population is treatment if it does progress.
There is currently no recognized treatment for pre-diabetes in children. (Quinn, Baur, Garnett, &
Cowell, 2010, p. 722). Tennessee Valley Pediatrics is a large privately owned pediatric practice
in North Alabama. The facility has around 8000 active patients ranging in age from newborn to
18 years. Having worked in pediatrics for 18 years, I am alarmed at the increasing number of
insulin resistance. Implementing a program that focused on educating patients on insulin
resistance and type two diabetes could greatly impact the patients. This change could become a
lifestyle change that can continue throughout adulthood.
At well check ups and sick visits patients with elevated BMI’s will be identified as potentially
at risk for insulin resistance. Every patient’s weight and height is obtained at each visit. The EHR
system at the facility automatically calculates the BMI which makes identifying the patients
simple. A weekly email will be sent to remind providers and nurses to help identify patients at
risk for insulin resistance. Providers seeing the patient will discuss their concern for potential
insulin resistance. A good rapport with the patient will be essential for this stage of the process.
This group will then have insulin levels drawn to access their risk.
Patients with elevated insulin levels will contacted regarding their results. This will occur
after the provider has reviewed the labs. The telephone triage RNs will be responsible for making

EVIDENCE-BASED PRACTICE PROJECT PAPER 19
contact with the patient. This will require approximately one hour of extra work per week for
these nurses. This also increases their pay by 400 dollars per month for a total cost of 4800
dollars per year. Patients unable to be contacted by phone will be mailed a letter to contact the
office .Initially, they will be educated on the potential progression of insulin resistance. They
will be advised that insulin resistance can lead to type two diabetes. Patients will be told that
insulin resistance is thought to be caused from the insulin’s inability to regulate sugar. They will
further be educated on the evidence-based discovery that dietary changes, exercise and
supportive medications can help lower insulin resistance. The target population consists of three
evidence based choices. . The group will be advised to engage in moderate physical activity for
at least 30 minutes per day. Another intervention is dietary changes. Reducing sugar intake
along with increasing fruits and vegetables will be the recommended dietary change. This is in
contrast to the current recommendations by the facility which were to decrease greasy foods and
lower caloric intake. Also, fruits and vegetables typically cost more than other food.
There are potential barriers for this plan. Many families do not come in for regular well visits.
This would make it vital to identify these patients at sick visits. Another barrier is that when we
are addressing adolescents, their parents must be on board with the recommendations. The
parents must be willing to not only encourage but also bring the patient back in for follow up
Weather conditions can be another factor when you are recommending exercise.
The next step in the EBP process involves continuing education and encouragement of the
patient. Weekly the patient and caregiver will be contacted. This will also be implemented by the
telephone triage nurses. They will answer any questions that the patient has regarding diet and
exercise. Having supportive nurses that develop a relationship and essentially become
“cheerleaders” to this group will be vital in the outcome of this project. Hard to reach patients

EVIDENCE-BASED PRACTICE PROJECT PAPER 20
may cause more time than allotted for the EBP project. Initially, it will be important to make
sure we have good contact information for the patient.
Once a month the patient will return to the office to recheck their weight and BMI. This will
give the provider a chance to assess their progress. A potential barrier is that some insurance may
not cover frequent rechecks. Also, two months after the first lab draw the patient will come back
into the office for a recheck. The telephone triage nurses will need to schedule this appointment.
The office does have an automated system that will remind the patient of their appointment.
Potentially, some patients may be hard to contact or may not come for a follow up visit. Patients
that feel they might have a poor outcome may be reluctant to follow up. At this visit their weight,
height and a BMI will be taking upon arrival and before they are examined by the provider. The
provider will examine the patient and order an insulin level. They will also be available to
answer any questions or concerns regarding their disease process. Patients will be questioned
regarding their dietary changes and their eating habits. Additional education will be provided if
needed. Although the insulin levels will not be readily available, this visit will provide either
positive or negative clinical information. A decrease in BMI and weight would be a positive
finding and encouraging for the patient. This will be presented on a flow chart through the EHR
system.
The insulin level will take approximately 24 hours to result. The providers will review the
labs and give recommendations to the nurse. The telephone triage nurse will then contact the
patient and specifically discuss their progress if the results are favorable. Patients who have no
change or an increase in insulin level will also be contacted. Patients with decreased insulin
levels will be encouraged to continue their current regimen. They will continue to be followed
for an additional 5 months for the EBP project. Patient’s that have the same or an increase in

EVIDENCE-BASED PRACTICE PROJECT PAPER 21
insulin levels will be interviewed by the telephone triage nurses to identify potential problems in
the implementation of the recommendations. Further education will be provided and they will
also be followed for an additional 5 months.
An evaluation plan will be needed to determine the success of the EBP project. A long term
goals would be to successfully develop a protocol at this facility for insulin resistant teens. This
plan aims to establish this protocol for anyone that either has insulin resistance or is at risk for
insulin resistance. The long term goal that is imperative for the implementation of this protocol
is the decrease in insulin resistance among the test patients. Another long term goal would be a
decrease in insulin levels on the patients that are in the project. There are several short term goals
for this plan. One short term goal would be to successfully educate the patient and the parent on
the insulin resistance. It is important to have the patient and the caregiver working together to
obtain the same outcome. Another short term goal would be the weight loss or a drop in BMI at
their monthly visit. Yet another goal would be the patient reporting that their attitude regarding
exercise had improved since the beginning of the project.
Several tools will be used to measure outcomes. Interviewing the patient to discuss their
current eating habits and exercise habits will add subjective data. Height and weight will be
measured and graphed on a growth chart provided by the AAP. BMI will be recorded on a BMI
calculator. The insulin level requires venous access. Insulin levels greater than 24mcu/ml will be
reported as elevated by the lab.
Providers will identify patients that are at risk for elevated insulin levels. The provider will
obtain the baseline labs, weight and BMI at the initial visit. Upon receiving labs that confirm that
the patient has insulin resistance, the provider will notify the RNs and the patient. The EBP
project manager will be contacted and given the demographic information regarding the patient.

EVIDENCE-BASED PRACTICE PROJECT PAPER 22
Patients that are selected for the small test of change will be monitored weekly and rechecked in
the office monthly. Data will be collected by reviewing the EHR record. Another important
factor in monitoring the data is the ability to track the patient’s progress. The EHR system in
place allows the facility to search patients based on diagnosis only. Patients who have had the
diagnosis of insulin resistance will be printed to provide a list of patients that need intervention.
Phone calls to the telephone triage nurse will be made weekly to evaluate the progress of the
EBP project. Also, the facility will be able to contact the EBP project manager during the
process. The EBP project manager will also be available to assist in any step of the process.
Small Test of Change
After looking at all the evidence provided from research, one area was chosen to implement.
The recommendation of 30 minutes of moderate exercise was selected for my small test of
change. The IRB was submitted and approved through Auburn University This involved
recruiting adolescents that already had elevated insulin levels. The office was able to run a
report based on the diagnosis of obesity and insulin resistance. This was very helpful in that it
provided a list of potential adolescents with insulin resistance. Patients with current insulin
resistance were brought into the office for a recheck. They had their weight and height taken to
calculate. Their BMI was recorded. Out of 29 patients scheduled, 22 signed consent for the
small test of change. Patients that consented were told to use a fitness app such as my fitness pal
to keep track of their activity. Patients were given suggestion of exercise from the American
Academy of Pediatrics. Patients and their parents were told to incorporate moderate daily
exercise of 30 minutes daily. This was in addition to dietary changes which were previously
recommended during their initial visit. We contacted the patient and or parent weekly to provide

EVIDENCE-BASED PRACTICE PROJECT PAPER 23
encouragement and answer any arising questions. At the end of 6 weeks they were brought back
into the office for a recheck on their BMI and insulin levels
Financially, the small test of change total is currently unknown. Initially the cost to the
practice was the cost of paying a registered nurse for two extra hours weekly. However, it is yet
to be known how often insurances will pay for insulin levels to be rechecked. Another concern is
the office recheck. How often is acceptable to recheck and manage patients with insulin
resistance? Currently, the practice was only rechecking these patients yearly. It is yet to be
determined if these visits will be covered under insurance.
While performing the small test of change, some participants did not complete the process
Only 14 actually returned to the office for their recheck. This was 8 males and 5 females. Also
there were 8 Caucasian and 5 African Americans. The mean age was 14.71. In measuring the
short term goals, patients were measured on their receptiveness to being educated. Short term,
successfully making weekly contact provides another short term goal. The return visit provided
objective ways of measuring the success of the small test of change. The patient came in to the
office and met with a provider. There they had their height and weight calculated to measure
their BMI. An insulin level was also redrawn. This provided the answers to the effectiveness of
the small test of change. The measuring tool was did they have a 15 percent reduction on their
insulin level.

EVIDENCE-BASED PRACTICE PROJECT PAPER 24
Results
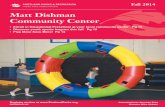
Category 1 grey Pre BMI
Category 1 orange post BMI
Category 3 grey Pre Insulin
Category 2 orange Post Insulin

EVIDENCE-BASED PRACTICE PROJECT PAPER 25
After calculating the information collected using SPSS, we found the following results. The
mean BMI dropped from 39.29 down to 37.93. The mean insulin level changed from a 34.21 pre
small test of change to 30.64. Although the results were not statistically significant, we do see a
trend that moderate exercise does lower BMI and insulin resistance. The owner and providers in
this pediatric practice feel this is a worthwhile recommendation and in the future will
recommend daily moderate exercise to their current recommendations.
Application in Overall Project
During this process I learned that it is difficult for one person to manage the project. In the
future, it would be easier if each nurse was responsible for their provider’s patients that had
insulin resistance. This would prevent frustration and time concerns. The process was too short
in length; ideally the change should be evaluated after 4-6 months to see any major changes. This
might also increase the likeliness of insurances covering the visit. I learned that adolescents also
do not like talking on the phone. In the future, a simple reminder text might be a better idea for
this age group. This project also reiterated that education can and does make a difference. In
applying this project in the future, I would include more education in the initial visit. This
education should include the disease process diabetes and potential complications that arise from
being a diabetic.
Conclusions

EVIDENCE-BASED PRACTICE PROJECT PAPER 26
In concluding this small test of change, it is evident that this project did provide future skills
for an advanced practice nurse. Understanding and being able to conduct sound research on
topics is a valuable skill for an advanced practice nurse. The importance of distinguishing the
difference in the level of evidence is crucial to health care providers. Presenting this small test of
change promotes confidence and independence. The discovery of reducing insulin resistance in
adolescents is a worthy topic that will continue to be visited. As an advanced practice nurse with
plans to work in a pediatric setting that my small test of change was conducted will provide
insight as one change roles from an RN to a nurse practitioner.

EVIDENCE-BASED PRACTICE PROJECT PAPER 27
References
CDC provides national estimates, general information on diabetes. (2012).chart10(4)5-8
retrieved from http://www.cdc.gov.
Clinical practice guidelines: Physical fitness and activity in schools. [Journal]. (2000).
Pediatrics, The Official Journal of the American Academy of Pediatrics, (105), 1156. doi:
10.1542/peds.105.5.1156
Davis,C.L., Pollock,N.K., Waller,J.L., Allison, J.D., Dennis, B.A.,....Gowler, B.A.(September,
2012) Exercise dose and diabetes risk in obese children; A randomized trial JAMA
(308)1103-1121 Retrieved from https://www.academia.edu/1853577
Evaluating obesity and cardiovascular risk factors in children and adolescents. (2008).
Retrieved June 10, 2014, from
https://www.pediatriccareonline.org/pco/ub/view/Bright-
Futures/135046/0/Adolescence_11_to_21_Years?amod=aapea&login=true&nfstatus
Farias, J. M. (2012, October 10th). Exercise training performed simultaneously to a high-fat diet
reduces the degree of insulin resistance and improves adipoR1-2/APPL1 protein levels in
mice. [Article]. Lipids in Health and Disease, 11, 34. http://dx.doi.org/10.1186/1476-
511X-11-134

EVIDENCE-BASED PRACTICE PROJECT PAPER 28
Fedewa, M.V., Gist, N. H., Evans, E.M., Dishman, R. K. (2013) Exercise and insulin resistance
in youth: A meta-analysis. Pediatrics Official Journal of the American Academy of
Pediatrics 133 (1) 163-173 doi: 10.1542/peds.2013-2718
Garnett, S. P., Baur, L. A., Noakes, M., Steinbeck, K., Woodhead, H. J., Burrell, S., ... Cowell,
C. T. (2010, September 25). Researching Effective Strategies to Improve Insulin
Sensitivity in Children and Teenagers - RESIST. A Randomized control trial
investigating the effects of two different diets on insulin sensitivity in young people with
insulin resistance and/or pre-diabetes. [article]. BMC Public Health, 10, 575.
http://dx.doi.org/10.1186/1471-2458-10-575
Garnett, Sarah P.; Gow, Megan; Ho, Mandy; Baur, Louise A.; Noakes, Manny; Woodhead,
Helen J.; Broderick, Carolyn R.; Burrell, .... Cowell, Chris T. (2013, May) Optimal
acmronutrient content of the diet for Adolescents with prediabetes; RESIST a
Randomised Control Trial . The Journal of Clinical Endocrinology & Metabolism,
98(5),2116-2125 doi: 10.1210/jc.2012-4251
Lee, Y. A., Yoo, J. H., Kim, J. H., Lee, S. H., Kim, J. H., Lim, L. H., ... Yang, S. W. (2011,
May). Independent relationships of obesity and insulin resistance with serum proinsulin
level in prepubertal children with normal glucose tolerance. [Article]. Pediatric Diabetes,
12(3), 235-241. http://dx.doi.org/10.1111/j.1399-448.2010.00696.x
Melnyk, B., & Fineout-Overholt, E. (2011). Evidence-Based Practice in Nursing and
Healthcare (2 ed.). Philadelphia: Lippincott Williams & Wilkins
Monzavi,R.,Dreimane,D.,Geffner, M.E., Braun,S., Conrad, B., Klier,
M.Kaufman,F.R.(June,2006) Improvement in risk factors for metabolic syndrome and
insulin resistance in overweight youth who are treated with lifestyle interventions.

EVIDENCE-BASED PRACTICE PROJECT PAPER 29
Pediatrics Official Journal of the American Academy of Pediatrics (117)1111-1118 doi:
10.1542/peds.2005-1532
Niklas, T. S. (2008, June). Association between 100% juice consumption and nutrient intake and
weight of children aged 2 to 11 years. [Comparitive study]. Pediatric and Adolescent
Medicine, 162(6), 557-565. http://dx.doi.org/10.1001/archpedi.162.6.557
Oftedal,B.,Bru,E. Bjorg,K.,(2011) Motivation for diet and exercise management among adults
with type 2 diabetes,Scandianavia Caring Science (25)2, 735-744 doi: 10.1111/j.1471-
6712.2011.00884
Simmons, S., Alexander, J. L., Ewing, H., & Whetzel, S. (2012, November 23). SNAP
participation in preschool-aged children and prevalence of overweight and obesity
[Journal article]. Journal of School Health, 1(23), 548-552. http://dx.doi.org/
10.1111/j.1746-1561.2012.00735
Sumanmo,E.,Schellenberg,B.S, Dryden,D.,Vandermeer,M.S., Ha,C., Korowynk,C.(2014)
Lifestyle interventions for patients with and at risk for type 2 diabetes. Annals of Internal
Medicine 159 (8) 543-551 doi: 2013;159:543-551
Wilson, V. (2013, March). Type 2 diabetes: an epidemic in children. [Article]. Nursing Children
and Young People, 25(2), 14-17. Retrieved from
Quinn, S. M., Baur, L. A., Garnett, S. P., & Cowell, C. T. (2010, October). Treatment of clinical
insulin resistance in children: a systematic review [article]. Obesity Reviews: An Official
Review Of The International Foundation For The Study of Obesity. 11(10) 722-730 doi:
11(10), 722-730. http://dx.doi.org/10.1111/j.1467-789X.2009.00697.x

EVIDENCE-BASED PRACTICE PROJECT PAPER 30
Alicia Nix Evidence grid
Level1
Sumanmo,E.,Schellenberg,B.S,
Dryden,D.,Vandermeer,M.S.,
Ha,C., Korowynk,C.(2014)
Lifestyle interventions for
patients with and at risk for type
2 diabetes. Annals of Internal
Medicine 159 (8) 543-551 doi:
2013;159:543-551
Purpose
To
systematically
review the
effectiveness of
lifestyle
interventions
on minimizing
progression to
diabetes in
high-risk
patients
or progression
to clinical
Design A Systematic
Review and
Meta-analysis
sampling
5 electronic
databases
(1980 to June
2013),
reference
lists, and gray
literature.
Two
Major findings
relevant to
project
Comprehensive
lifestyle
interventions
effectively
decrease
the incidence of
type 2 diabetes
in high-risk
patients. In
patients who
already have
Critique of
validity, bias and
significance for
your project
Most trials focused
on surrogate
measures (such as
weight change,
blood pressure, and
lipids) for which
clinical relevance
was unclear.
Significance
This is relevant to

EVIDENCE-BASED PRACTICE PROJECT PAPER 31
outcomes (such
as
cardiovascular
disease and
death) in
patients with
type 2 diabetes.
The literature
search
identified 1289
citations.
The lifestyle
intervention
had to
include an
exercise
component, a
diet component,
and at
least 1 other
component
(such as
counseling,
smoking
cessation,
and behavior
modification
reviewers
independently
identified
randomized,
controlled
trials of
lifestyle
interventions
(_3 months’
duration)
that included
exercise, diet,
and at least 1
other
component;
the
comparator
was standard
care.
The literature
search
identified
1289
citations.
Twenty
unique studies
in 58
publications
were included
Nine studies
addressed
patients at
increased risk
for type 2
diabetes; 11
studies
addressed
patients
diagnosed
with type
2 diabetes
type 2 diabetes,
there is no
evidence of
reduced all-
cause mortality
and insufficient
evidence to
suggest
benefit on
cardiovascular
and
microvascular
outcomes
my EBP project in
that my project’s
aim is to prevent
diabetes.
Level 1
Level1
Quinn, S. M., Baur, L. A.,
Garnett, S. P., & Cowell,
C. T. (2010, October).
The objective
of this study
was to evaluate
the
Design: randomized
controlled
trial (True
6 months of
metformin with
or without
lifestyle
The review question
was clearly stated.
The search strategy
was effective.

EVIDENCE-BASED PRACTICE PROJECT PAPER 32
Treatment of clinical
insulin resistance in
children: a systematic
review [article]. Obesity
Reviews: An Official
Journal Of The
International
Association For The
study Of Obesity, 11(10),
722-730.
http://dx.doi.org/10.1111
/j.1467-
789X.2009.00697.x
effectiveness of
interventions
aimed at
improving
clinical insulin
resistance
and/or pre-
diabetes in
children
experimental)
Sampling
method Five
electronic
databases
were searched
for
randomized
controlled
trials of at
least 2-
months’
duration
Sample size
four trials
were eligible
for inclusion
in the
systematic
review.
Interventions
none
Outcomes
Fasting
insulin,
HOMA-IR
BMI
interventions
showed a
statistical
difference in
fasting insulin
After 6 months
when using
metformin the
subjects had a
decrease in BMI
with or without
physical activity
The combined
effect of
metformin and
individualized
lifestyle
intervention
resulted in the
greatest decrease
in fasting insulin
and had the
additional effect
of decreasing
BMI
this systematic
review shows
that
metformin,
whether used
alone or in
combination
with lifestyle
interventions,
improves
markers of
insulin
sensitivity,
fasting insulin
and HOMA and
reduces BMI.
Comprehensive
search methods and
appropriate
databases were
used.
The review methods
are clearly
documented, as well
as the search
strategy, inclusion
criteria, and
methods used.
The sample size
was extremely
small, with only 3
being acceptable to
be included in the
meta-analysis so the
statistical power
after the pooling of
data is low.
Second, of the three
trials that provided
sufficient detail
to determine
attrition rate (15–
17), the mean value
was
20%, with more
people in the
control group (25%)
compared
with the
intervention group
(16%) discontinuing
trial participation.
This highlights the
difficulties with
implementing
treatment regimens
in this age group.
One study (17) had
a particularly high
attrition rate in both
the control (36%)

EVIDENCE-BASED PRACTICE PROJECT PAPER 33
and intervention
arm (33%); the
authors attributed
this to the
prolonged dose
loading regimen of
2 months decreasing
the impact of the
intervention on
weight
loss and
consequently
resulting in
participant
dissatisfaction with
the treatment.
Significance-
Although no trials
on lifestyle
interventions alone
were identified, this
systematic review
shows that
metformin, whether
used alone or in
combination with
lifestyle
interventions,
improves markers
of insulin
sensitivity, fasting
insulin and HOMA
and reduces BMI.
Several features of
clinical insulin
resistance, including
In applying
to my
project,
starting
patients on
metformin
might be a
recommenda
tion added

EVIDENCE-BASED PRACTICE PROJECT PAPER 34
to diet and
exercise
when the
goal is
lowering
insulin
levels
.
-
Level 1
Clinical practice guidelines:
Physical fitness and
activity in schools.
[Journal]. (2000).
Pediatrics, The Official
Journal of the American
Academy of Pediatrics,
(105), 1156. doi:
10.1542/peds.105.5.1156
Purpose
To provide a
guideline for
physical
activity in
children and
adolescents
with certain risk
factors can
detect insulin
resistance and
diabetes early
in the disease
progression.
design Clinical
Guideline
Review of
Published
Meta-
Analyses
Systematic
Review
No
interventions
Outcomes
this guideline
was put in
place to give
clinicians and
parents a
guideline as
to how much
physical
activity for
optimal health
in children
Major findings
relevant to
project
These guidelines
sets a
precedence in
the amount of
physical activity
needed to help
prevent type 2
diabetes and
insulin
resistance.
Validity
This is a valid study
in that it used expert
consensus
Significance. It was
also weighted
according to the
weighted scheme.
with no bias
The guideline is
providing a
recommendation for
physical activity in
is also the ultimate
goal of my EBP.
An acceptable
screening tool
would be a tool that
could be used in my
EBP project

EVIDENCE-BASED PRACTICE PROJECT PAPER 35
and
adolescents
while in a
school setting
Article Level 1
Fedewa, M.V., Gist, N. H., Evans,
E.M., Dishman, R. K. (2013)
Exercise and insulin resistance in
youth: A meta-analysis. Pediatrics
Official Journal of the American
Academy of Pediatrics 133 (1) 163-
173 doi: 10.1542/peds.2013-2718
This
systematic
review and
meta-analysis
provides a
quantitative
estimate of the
effectiveness
of exercise
training on
fasting insulin
and insulin
resistance in
children and
adolescents.
.
Design RCT
Sampling
method
Analysis was
limited to
randomized
controlled
trials by
using
combinations
of the terms
adolescent,
child,
pediatric,
youth,
exercise
training,
physical
activity,
diabetes,
insulin,
randomized
trial, and
randomized
controlled
trial. Sample
size:The
authors
assessed 546
sources, of
which 4.4%
(24 studies)
were eligible
for inclusion.
Major findings
These results
support the use of
exercise training in
the
prevention and
treatment of type 2
diabetes.
Critique of
validity, bias
Analysis was
limited to
randomized
controlled
trial. Only 24
studies were
included in
the trial. Also
effects were
independently
calculated by
multiple
authors.

EVIDENCE-BASED PRACTICE PROJECT PAPER 36
Thirty-two
effects were
used to
estimate the
effect of
exercise
training on
fasting
insulin, with
15 effects
measuring the
effect on
insulin
resistance.
Outcomes:
Based on the
cumulative
results from
these studies,
a small
to moderate
effect was
found for
exercise
training on
fasting
insulin
and
improving
insulin
resistance in
youth -
Level 3
Oftedal,B.,Bru,E. Bjorg,K.,(2011)
Motivation for diet and exercise
management among adults with type
2 diabetes,Scandianavia Caring
The aim of this
study was to
investigate diet
and
exercise
A cross-
sectional
design
including a
postal
Reported diet
management was
more in accordance
with
recommendations
Large sample
size But a
questionnaire
was mailed to
obtain data.

EVIDENCE-BASED PRACTICE PROJECT PAPER 37
Science (25)2, 735-744 doi:
10.1111/j.1471-6712.2011.00884
management
and how
indicators of
intrinsic
motivation
such as ability
expectations
and values are
associated
with diet and
exercise
management
among
adults with
type 2
diabetes.
Background:
Motivational
problems are
probably one
questionnaire
that
investigated
diet and
exercise
management
as well as
intrinsic
motivational
factors such
as ability
expectations
and values
related to
these
behaviors
was used to
collect the
data. A
sample
comprising
425 adults
with type 2
diabetes aged
between 30
and 70
completed the
questionnaire.
than reported
exercise
management. Yet
results indicated
equally high ability
expectations and
positive values for
exercise and diet
management.
This might
have been in
one small
area of the
country so
not a true
random study
Also self
reported data
This provides
evidence to
my project
due to the
promotion of
diabetes and
exercise
among type 2
diabetics
Level IV
Lee, Y. A., Yoo, J. H., Kim, J. H.,
Lee, S. H., Kim, J. H., Lim, L.
H., ... Yang, S. W. (2011,
May). Independent
relationships of obesity and
insulin resistance with serum
proinsulin level in prepubertal
children with normal glucose
tolerance. [Article]. Pediatric
Diabetes, 12(3), 235-241.
http://dx.doi.org/10.1111/j.13
99-
448.2010.00696.x
Purpose of
study. to
compare the
fasting serum
proinsulin
levels in lean,
overweight,
and obese
prepubertal
children with
normal
glucose
tolerance
and also
evaluated the
relationship
- Design
Coorelational
- Sampling
method
118
prepubertal
children (80
males, 38
females) who
were assessed
between
December
2007 and
January 2009.
- sample size
data suggest that
obesity itself or
insulin resistance
may independently
cause fasting
hyperproinsulinemia
in proportion to
hyperinsulinemia in
prepubertal
children with
normal glucose
tolerance test.
. Measuring the
serum
level of proinsulin
might be useful as a
Strength; This study had a large sampling population which contributes to the validity of the study Statistical analysis was used.

EVIDENCE-BASED PRACTICE PROJECT PAPER 38
between
fasting
proinsulin
level
and indices of
insulin
resistance
to compare the
fasting serum
proinsulin
levels in lean,
overweight,
and obese
prepubertal
children with
normal
glucose
tolerance
and also
evaluated the
relationship
between
fasting
proinsulin
level
and indices of
insulin
resistance
A total of 109
prepubertal
children
(mean age,
8.6 years)
were included
in this study
- Brief
description
of
interventions
(if any)
None
- outcomes
measured
(30 points)
Determining
the patients
insulin level
helps
determine b-
cell overload
in children
marker of β-cell
overload in obese
children.
Weakness- the fasting insulin levels were only collected once. A limitation of this cross-sectional study was that we could not investigate what is the value of using both proinsulin and insulin in screening vs. the use of insulin alone to predict the development of T2DM or metabolic syndrome later. Significance. Since my project is lowering insulin resistance levels and decreasing the incidence in development of type 2

EVIDENCE-BASED PRACTICE PROJECT PAPER 39
diabetes, it is important to understand the relationship between elevated pro insulin levels and the development of insulin resistance.
Level 2
Monzavi,R.,Dreimane,D.,Geffner,
M.E., Braun,S., Conrad, B., Klier,
M.Kaufman,F.R.(June,2006)
Improvement in risk factors for
metabolic syndrome and insulin
resistance in overweight youth who
are treated with lifestyle
interventions. Pediatrics Official
Journal of the American Academy of
Pediatrics (117)1111-1118 doi: 10.1542/peds.2005-1532
Quasi-
experimental
To evaluate
the prevalence
of risk factors
that are
associated
with the
metabolic
syndrome and
insulin
resistance in
overweight
youth and to
determine
the effect of a
short-term,
family-
centered,
lifestyle
intervention on
various
associated
anthropometric
and metabolic
measures
Overweight
youth who were
between 8 and 16
years of age
participated
in a 12-week,
family-centered,
lifestyle
intervention
program.
Anthropometric
and metabolic
measures were
assessed before
the program in
all participants (n
_ 109) and after the
program in a
subset of the
participants (n _ 43).
Overweight youth have
multiple risk factors
associated with the
metabolic
syndrome. A 12-week
lifestyle program may
have a positive effect on
reducing risk factors for
the metabolic syndrome
and insulin resistance in
overweight
youth. www
Possible recruitment bias. The primary care physician referred the patient So it was not a blind study. Also there was a small number of participants
Level 1 Davis,C.L., Pollock,N.K., Waller, J.L., Allison, J.D., Dennis,
The Aim of the study is to test the
Design: RCT Sampling
In this trial, after 13 weeks, 20 or 40 min/d of
Although there was an adequate

EVIDENCE-BASED PRACTICE PROJECT PAPER 40
B.A.,....Gowler, B.A.(September, 2012) Exercise dose and diabetes risk in obese children A randomized controlled trial JAMA (308)1103-1121 Retrieved from https://www.academia.edu/1853577
effect of different doses of aerobic training on insulin resistance, fatness, visceral fat, and fitness in overweight, sedentary children and to test moderation by sex and
race.
size and Method Randomized controlled efficacy trial conducted from 2003 through 2007 in which 222 overweight or obese sedentary children (mean age, 9.4 years; 42% male; 58% black) were recruited from 15 public schools in the Augusta, Georgia, area
aerobic training improved fitness and demonstrated dose-response benefits for insulin resistance and general and visceral adiposity in sedentary overweight or obese children, regardless of sex or race
sample size, the recruitment came from one city of one state This study specifically relates to my project. This provides evidence that physical activity reduces insulin resistance This is relevant to my project in that we are looking at exercise reducing the risk of type 2 diabetes. Insulin resistance is the leading cause of type 2 diabetes.

EVIDENCE-BASED PRACTICE PROJECT PAPER 41