Evidence-based impact of experiential learning Professor Ian Bates Head of Education Development...
32
Evidence-based impact of experiential learning Professor Ian Bates Head of Education Development School of Pharmacy University of London
-
Upload
melvin-white -
Category
Documents
-
view
216 -
download
2
Transcript of Evidence-based impact of experiential learning Professor Ian Bates Head of Education Development...
Evidence-based impact of experiential learning
Professor Ian BatesHead of Education Development
School of PharmacyUniversity of London

European Directive
– 3000 hours of directed study at 4-5 years’ duration
– Greater part of curriculum and not less than 50% of final year must be core
– At least 35% on actions and uses of drugs
– At least 35% on experiments and data analysis
– Research project of 3 – 6 months duration
The professional imperative
– Better health care,
– Better patient experience,
– Better value for money

– Curricular pressures Integration of pharmaceutical and
clinical sciences
– Dislocation of education and practice– Not competency-based
Performance of our graduates?
– Not a partnership With national health systems With existing health professionals
What’s holding us back?

Short term vs Long term
– Long term The science of medicines must be
foundation of education Knowledge half-life
– Short-term imperatives Understand and engage with the
health agenda

The learning experience
Syllabus – knowledge & content
Delivery & quality
Outcomes
Context – institutional, societal & cultural
Access, finance & policy
What’s holding us back……curriculum

Assessment
Goals
Independence
Good Teaching
BangladeshUSA
India
MalaysiaNetherlands
Canada
AustraliaGhana
Finland
PortugalIceland
Slovenia
JamaicaSingapore
Swiss
RomaniaTaiwan
Serbia
SpainGermany
UK
CroatiaIsrael
Czech Republic
Nepal
-0.5
0.0
0.5
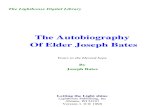
1.0Assessment
Goals
Independence
Good Teaching
Pharmacy students N = 5,243 p<0.0001
Sta
ndar
dise
d m
ean
scor
esThe Learning Experience…

– It varies
– Is this acceptable?
– How can we improve it?
The learning experience

the Knowledge problem
…pharmacy syllabus is overcrowded
chemistry pharmacology biotechnologygenetics medicine analysis formulationphysical chemistry ethics pharmacognosyphytochemistry drug design immunologypharmacokinetics therapeutics pathologyepidemiology health economics chemical analysisphysiology proteomics statisticslaw Licensing&marketing ADRsmicrobiology medicinal chemistry biochemistrytoxicology drug metabolism genomicssocial & behavioural sciences

And so…?
– Methods PBL Near to patient cases Clinical contact Experiential Subject Integration
– Designs Scientists as practitioners Adult learning & self-direction Pragmatic & meaningful in situ LLL
“Experiential” learning
– Experience We all have ‘experiences’ We often learn from an “experience”
Working or work-like
As children…. Anecdotal….
– No real mysterious or obscure theory

The real issue…
…getting the “experience” to UG and PG learners (either students or practitioners)
– Design
– Environment
– Outcomes

Competency →
Competence →
Performance
Fit to practise?
…outcomes
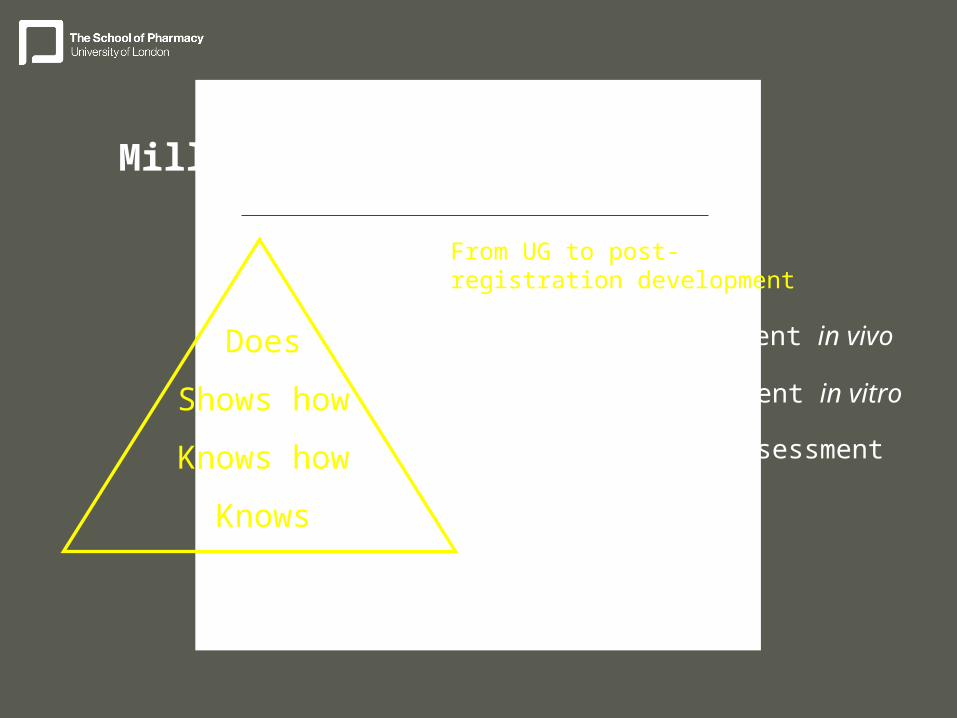
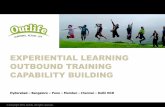
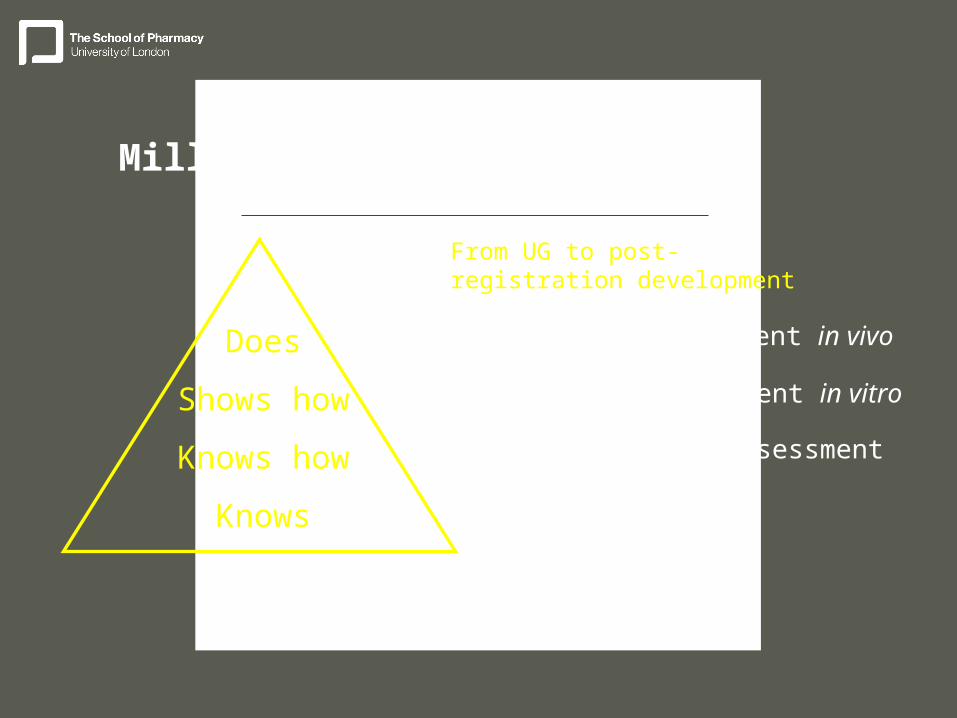
Miller’s pyramid
Does
Shows how
Knows how
Knows
performance assessment in vivo
performance assessment in vitro
clinical context assessment
factual assessment
From UG to post-registration development

Experiential learning
– Should attempt to bring relevant experience to theory
– Should therefore illustrate knowledge (working knowledge?)
– Should therefore re-enforce primary learning
…it should move learning towards the competency agenda…
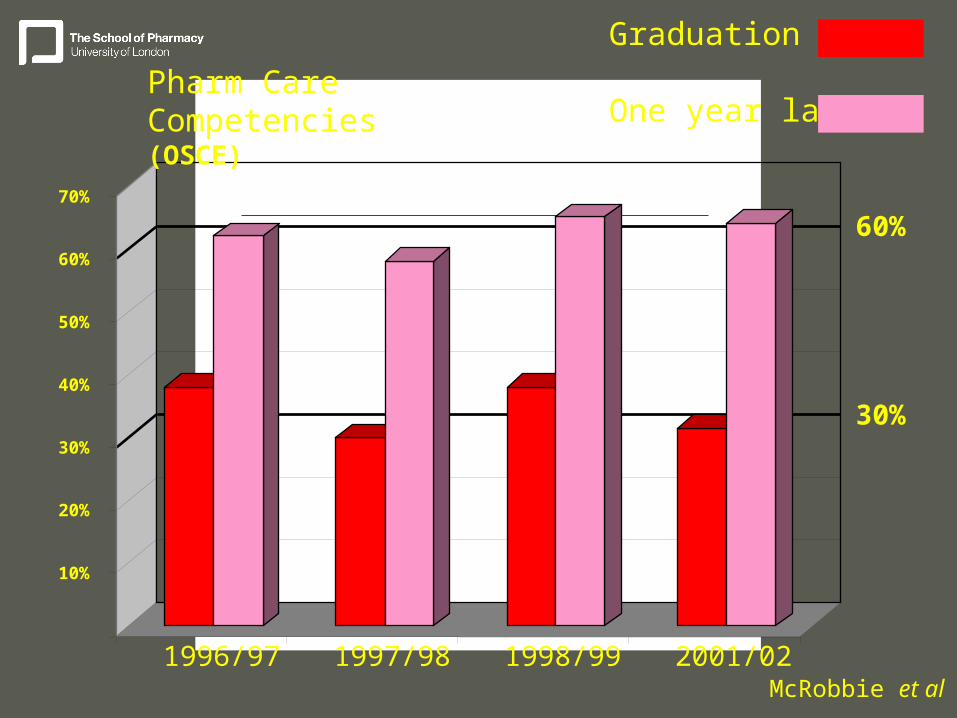
10%
20%
30%
40%
50%
60%
70%
1996/97 1997/98 1998/99 2001/02
Pharm Care Competencies(OSCE)
60%
30%
Graduation
One year later
McRobbie et al
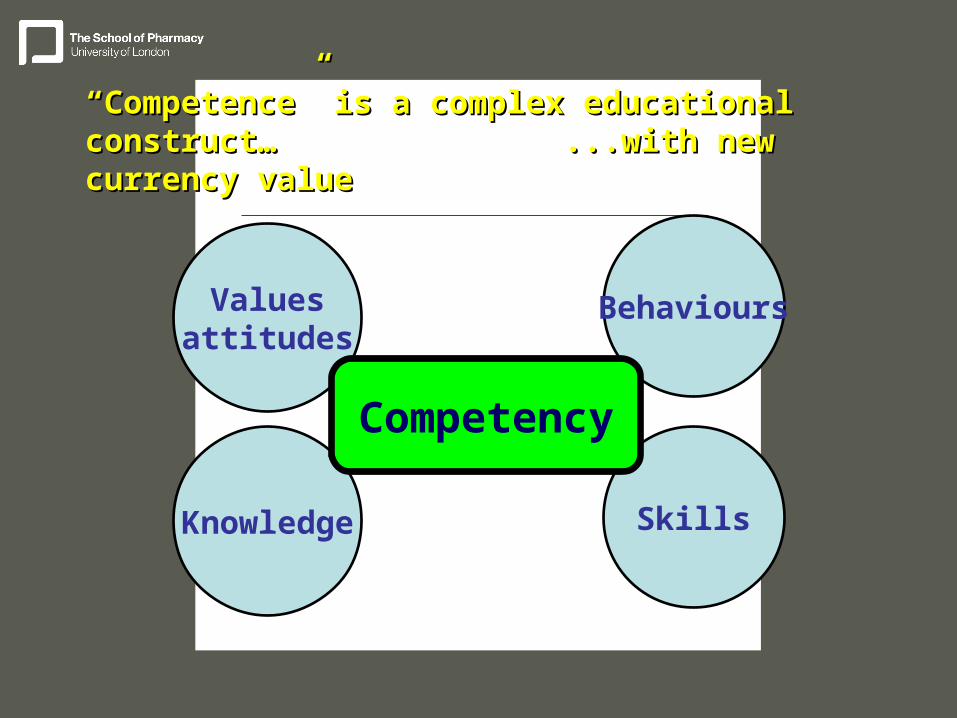
Skills
Behaviours
Knowledge
Valuesattitudes
Competency
““Competence” is a complex educational construct…Competence” is a complex educational construct…...with new currency value...with new currency value
An example..
Drug-drug interactions:-
– Theory, knowledge
– Examples (from lectures, books, case studies, etc)
– Exams and questions

Moving from “knowing” (theory)… towards …“doing” (performance)

Miller’s pyramid
Does
Shows how
Knows how
Knows
performance assessment in vivo
performance assessment in vitro
clinical context assessment
factual assessment
From UG to post-registration development
Barriers
– Assessment
– Resource
– Culture
Miller’s pyramid
Does
Shows how
Knows how
Knows
performance assessment in vivo
performance assessment in vitro
clinical context assessment
factual assessment
From UG to post-registration development

Barriers
– Assessment
– Resource– Culture
…there must be a working relationship with the university and the work environment
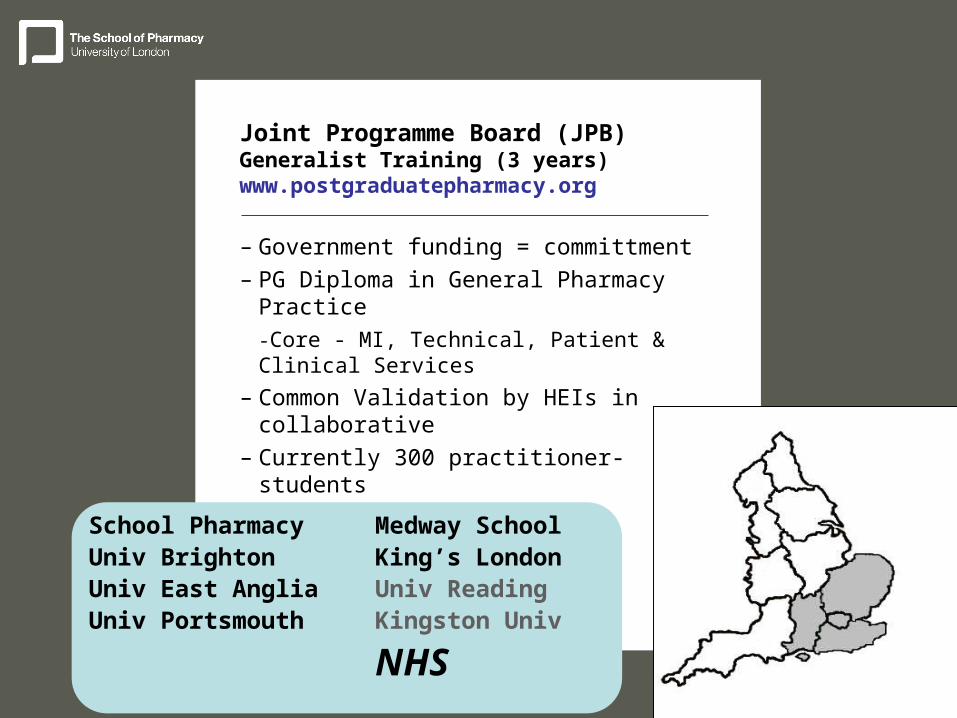
Joint Programme Board (JPB)Generalist Training (3 years)www.postgraduatepharmacy.org
– Government funding = committment
– PG Diploma in General Pharmacy Practice
-Core - MI, Technical, Patient & Clinical Services
– Common Validation by HEIs in collaborative
– Currently 300 practitioner-students
(target 2009 = 750)
School PharmacyUniv BrightonUniv East AngliaUniv Portsmouth
Medway SchoolKing’s LondonUniv ReadingKingston Univ
NHS
I tend to describe myself as a student rather than a practitionerStrongly agreeAgreeDisagreeStrongly disagree
Fre
qu
en
cy
50
40
30
20
10
0
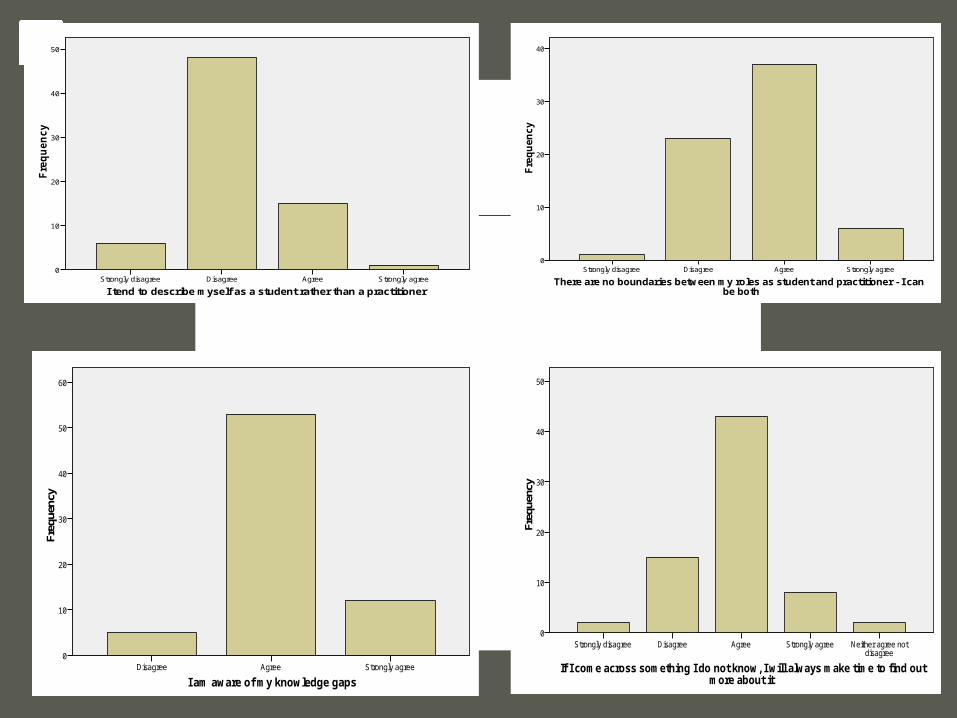
I tend to describe myself as a student rather than a practitioner
There are no boundaries between my roles as student and practitioner - I can be both
Strongly agreeAgreeDisagreeStrongly disagree
Fre
qu
en
cy
40
30
20
10
0
There are no boundaries between my roles as student and practitioner - I can be both
I am aware of my knowledge gapsStrongly agreeAgreeDisagree
Freq
uenc
y
60
50
40
30
20
10
0
I am aware of my knowledge gaps
If I come across something I do not know, I will always make time to find out more about it
Neither agree not disagree
Strongly agreeAgreeDisagreeStrongly disagree
Freq
uenc
y
50
40
30
20
10
0
If I come across something I do not know, I will always make time to find out more about it

Predominantly FDL and e-modes
Predominantly face-to-face modes
Cohort learners
Lone learnerOn-site (HEI) learning
Off-site (work) learning
FDL, e-modesoff-site, experientialIndependentCareer driven
Learning modality with time/career pathway
UG
UG/Pre
Post-reg
Higher

General and Higher level practice: Growing the next generation
The next [urgent] challenge…
– Competency frameworks for undergraduate education
– Assessment of performance at UG level (medicines-centered)

The pharmaceutical imperative
– Bring our pharmaceutical science into healthcare practice

Where is our professional ‘centre of gravity’?
Patient-focussed, medicines-centred
..can only achieve this through a partnership of universities and health care employers (systems)

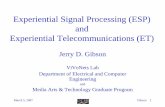
Mortality rate Index
Low Activity
High Activity
Key performance indicators F1(medical)
70 80 90 100 110 120
0
50
100
150
200
Ph
arm
acy
est
ab
lish
me
nt
WT
Es
R-Square = 0.16
R-Square = 0.76

Evidence-based impact of experiential learning
Professor Ian BatesHead of Education Development
School of PharmacyUniversity of London