
Evaluation of ticagrelor pharmacodynamic interactions with reversibly binding or non-reversibly...
7
Regular Article Evaluation of ticagrelor pharmacodynamic interactions with reversibly binding or non-reversibly binding P2Y 12 antagonists in an ex-vivo canine model ☆ Anna Ravnefjord a, ⁎, Jessika Weilitz b , Britt-Marie Emanuelsson c , J.J.J. van Giezen d a Department of Bioscience, AstraZeneca R&D Mölndal, Sweden b Global DMPK-IM, Regulatory Bioanalysis, AstraZeneca R&D Mölndal, Sweden c Global DMPK-IM, Centre of Excellence, AstraZeneca R&D Mölndal, Sweden d TA CV/GI, AstraZeneca R&D Mölndal, Sweden abstract article info Article history: Received 12 April 2012 Received in revised form 13 June 2012 Accepted 20 July 2012 Available online 19 August 2012 Keywords: Ticagrelor Cangrelor Clopidogrel Antiplatelet therapy Preclinical Introduction: As ticagrelor, clopidogrel and cangrelor therapies may be used in the same clinical setting, their potential pharmacodynamic interactions are of interest. Hence, we investigated possible interactions be- tween these agents in dogs using a variety of switching protocols. Methods: Six male dogs all received 7 different dosing regimens separated by 1–5 week washout periods: cangrelor (1 μg/kg/min, intravenous infusion); ticagrelor (0.8 mg/kg, oral); clopidogrel (3 mg/kg, intrave- nous injection); cangrelor together with ticagrelor initiated 10 minutes after cangrelor infusion start or clopidogrel given 30 minutes after cangrelor infusion start; ticagrelor followed by clopidogrel given 3 or 7 hours after ticagrelor dosing. ADP-induced whole blood platelet aggregation was measured by impedance aggregometry. Results: Mean maximum inhibition of platelet aggregation (IPA) was 81–87% at 6 minutes (cangrelor), 3 hours (ticagrelor) and 4 hours (clopidogrel) postdosing and platelet function recovered after 1.5 hours, 12 hours, and 9 days, respectively. IPA at 2 hours post clopidogrel was reduced to 39% when clopidogrel was given during cangrelor infusion versus 69% for clopidogrel alone. With clopidogrel dosed 3 hours after ticagrelor, IPA was reduced after washout of ticagrelor to 38% at 24 hrs vs. 68% for clopidogrel alone, but an interaction was not seen when clopidogrel was dosed 7 hours after ticagrelor. No pharmacodynamic in- teraction occurred between ticagrelor and cangrelor. Conclusions: The extent of the pharmacodynamic drug-drug interactions observed between clopidogrel and cangrelor or ticagrelor apparently depends on the level of receptor occupancy when clopidogrel is adminis- tered. Importantly, no significant pharmacodynamic interaction occurred between ticagrelor/clopidogrel when clopidogrel was given at clinical trough IPA levels with ticagrelor. No significant pharmacodynamic in- teraction occurred with cangrelor and ticagrelor. © 2012 Elsevier Ltd. All rights reserved. Introduction Standard dual antiplatelet therapy for reducing thrombotic compli- cations in patients with acute coronary syndromes (ACS) is clopidogrel with aspirin [1,2]. Clopidogrel (a thienopyridine) is a pro-drug, and is converted in the liver to the active metabolite. This metabolite has a free thiol group that binds irreversibly to the P2Y 12 receptor, and forma- tion of disulfide bridges with extracellular cysteine residues leads to in- activation of the receptor [3]. Clopidogrel has several clinical limitations, the need for metabolic activation results in a delayed onset of the inhibition of platelet aggregation (IPA), and the irreversible binding of its active metabolite to the P2Y 12 receptor delays the offset of IPA [4]. Potential drug-drug interactions may also occur, e.g. inhibition of relevant CYP enzymes could reduce the metabolism of clopidogrel [5]; as the active metabolite has a short half life other factors could com- pete for the P2Y12 receptor. Ticagrelor is an orally active, direct acting, reversibly binding P2Y 12 re- ceptor antagonist that belongs to a new class of compounds, cyclopentyl- triazolo-pyrimidines [6,7]. Ticagrelor has recently gained approval for use in the European Union [8] and the U.S. [9] in adult patients with acute cor- onary syndromes. Ticagrelor binds reversibly to the P2Y 12 receptor in an Thrombosis Research 130 (2012) 622–628 Abbreviations: ACS, acute coronary syndromes; ADP, adenosine diphosphate; AU, aggregation units; AUC 0−∞ , area under the plasma concentration-time curve from zero to infinity; AUC 0−t , area under the plasma concentration-time curve from zero to last measur- able time point; AUC AU , area under the aggregation curve; C max , maximum plasma concen- tration; C t , predicted plasma concentration at last measurable time point; IPA, inhibition of platelet aggregation; LLOQ, lower limit of quantification; SEM, standard error of the mean; T, time of sample; t, time postdosing; t ½ , terminal elimination half-life; t max , time to C max ; λ z , terminal-phase elimination rate constant. ☆ Previous presentation: The data reported in this manuscript were presented at the XXII Congress of the International Society on Thrombosis and Haemostasis, July 11–16, 2009; Boston, MA, USA. ⁎ Corresponding author at: Department of Bioscience, AstraZeneca R&D Mölndal, S-431 83 Mölndal, Sweden. Tel.: +46 31 7762954; fax: +46 31 7763701. E-mail address: [email protected] (A. Ravnefjord). 0049-3848/$ – see front matter © 2012 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.thromres.2012.07.021 Contents lists available at SciVerse ScienceDirect Thrombosis Research journal homepage: www.elsevier.com/locate/thromres
Transcript of Evaluation of ticagrelor pharmacodynamic interactions with reversibly binding or non-reversibly...

Thrombosis Research 130 (2012) 622–628
Contents lists available at SciVerse ScienceDirect
Thrombosis Research
j ourna l homepage: www.e lsev ie r .com/ locate / thromres
Regular Article
Evaluation of ticagrelor pharmacodynamic interactions with reversibly binding ornon-reversibly binding P2Y12 antagonists in an ex-vivo canine model☆
Anna Ravnefjord a,⁎, Jessika Weilitz b, Britt-Marie Emanuelsson c, J.J.J. van Giezen d
a Department of Bioscience, AstraZeneca R&D Mölndal, Swedenb Global DMPK-IM, Regulatory Bioanalysis, AstraZeneca R&D Mölndal, Swedenc Global DMPK-IM, Centre of Excellence, AstraZeneca R&D Mölndal, Swedend TA CV/GI, AstraZeneca R&D Mölndal, Sweden
Abbreviations: ACS, acute coronary syndromes; ADPaggregation units; AUC0−∞, area under the plasma conceninfinity; AUC0−t, area under the plasma concentration-timeable time point; AUCAU, area under the aggregation curve;tration; Ct, predicted plasma concentration at last measuraplatelet aggregation; LLOQ, lower limit of quantification; ST, time of sample; t, timepostdosing; t½, terminal eliminatioterminal-phase elimination rate constant.☆ Previous presentation: The data reported in this maXXII Congress of the International Society on Thrombosi2009; Boston, MA, USA.⁎ Corresponding author at: Department of Bioscienc
S-431 83 Mölndal, Sweden. Tel.: +46 31 7762954; fax:E-mail address: [email protected] (
0049-3848/$ – see front matter © 2012 Elsevier Ltd. Allhttp://dx.doi.org/10.1016/j.thromres.2012.07.021
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 12 April 2012Received in revised form 13 June 2012Accepted 20 July 2012Available online 19 August 2012Keywords:TicagrelorCangrelorClopidogrelAntiplatelet therapyPreclinical
Introduction: As ticagrelor, clopidogrel and cangrelor therapies may be used in the same clinical setting, theirpotential pharmacodynamic interactions are of interest. Hence, we investigated possible interactions be-tween these agents in dogs using a variety of switching protocols.Methods: Six male dogs all received 7 different dosing regimens separated by 1–5 week washout periods:cangrelor (1 μg/kg/min, intravenous infusion); ticagrelor (0.8 mg/kg, oral); clopidogrel (3 mg/kg, intrave-nous injection); cangrelor together with ticagrelor initiated 10 minutes after cangrelor infusion start orclopidogrel given 30 minutes after cangrelor infusion start; ticagrelor followed by clopidogrel given 3 or7 hours after ticagrelor dosing. ADP-induced whole blood platelet aggregation was measured by impedanceaggregometry.Results: Mean maximum inhibition of platelet aggregation (IPA) was 81–87% at 6 minutes (cangrelor),3 hours (ticagrelor) and 4 hours (clopidogrel) postdosing and platelet function recovered after 1.5 hours,
12 hours, and 9 days, respectively. IPA at 2 hours post clopidogrel was reduced to 39% when clopidogrelwas given during cangrelor infusion versus 69% for clopidogrel alone. With clopidogrel dosed 3 hours afterticagrelor, IPA was reduced after washout of ticagrelor to 38% at 24 hrs vs. 68% for clopidogrel alone, butan interaction was not seen when clopidogrel was dosed 7 hours after ticagrelor. No pharmacodynamic in-teraction occurred between ticagrelor and cangrelor.Conclusions: The extent of the pharmacodynamic drug-drug interactions observed between clopidogrel andcangrelor or ticagrelor apparently depends on the level of receptor occupancy when clopidogrel is adminis-tered. Importantly, no significant pharmacodynamic interaction occurred between ticagrelor/clopidogrelwhen clopidogrel was given at clinical trough IPA levels with ticagrelor. No significant pharmacodynamic in-teraction occurred with cangrelor and ticagrelor.© 2012 Elsevier Ltd. All rights reserved.
Introduction
Standard dual antiplatelet therapy for reducing thrombotic compli-cations in patients with acute coronary syndromes (ACS) is clopidogrel
, adenosine diphosphate; AU,tration-time curve from zero tocurve from zero to lastmeasur-Cmax, maximumplasma concen-ble time point; IPA, inhibition ofEM, standard error of the mean;nhalf-life; tmax, time to Cmax;λz,
nuscript were presented at thes and Haemostasis, July 11–16,
e, AstraZeneca R&D Mölndal,+46 31 7763701.A. Ravnefjord).
rights reserved.
with aspirin [1,2]. Clopidogrel (a thienopyridine) is a pro-drug, and isconverted in the liver to the active metabolite. This metabolite has afree thiol group that binds irreversibly to the P2Y12 receptor, and forma-tion of disulfide bridges with extracellular cysteine residues leads to in-activation of the receptor [3]. Clopidogrel has several clinicallimitations, the need for metabolic activation results in a delayedonset of the inhibition of platelet aggregation (IPA), and the irreversiblebinding of its activemetabolite to the P2Y12 receptor delays the offset ofIPA [4]. Potential drug-drug interactions may also occur, e.g. inhibitionof relevant CYP enzymes could reduce the metabolism of clopidogrel[5]; as the activemetabolite has a short half life other factors could com-pete for the P2Y12 receptor.
Ticagrelor is an orally active, direct acting, reversibly binding P2Y12 re-ceptor antagonist that belongs to a new class of compounds, cyclopentyl-triazolo-pyrimidines [6,7]. Ticagrelor has recently gained approval for usein the EuropeanUnion [8] and theU.S. [9] in adult patientswith acute cor-onary syndromes. Ticagrelor binds reversibly to the P2Y12 receptor in an

Table 1Summary of dosing regimens (n=6/regimen).
Compound(s) Dosing regimen
Cangrelor Intravenous infusion 1 μg/kg/min for 1 hourTicagrelor Single oral dose of 0.8 mg/kgClopidogrel Intravenous injection of 3 mg/kgCangrelor+clopidogrel Intravenous infusion of cangrelor (1 μg/kg/min) for
2 hours plus clopidogrel (intravenous injection) of3 mg/kg) 30 minutes after the start of cangrelor infusion
Ticagrelor+clopidogrel Single oral dose of ticagrelor (0.8 mg/kg) plusintravenous injection of clopidogrel (3 mg/kg) 3 hourspost-ticagrelor dose
Ticagrelor+clopidogrel Single oral dose of ticagrelor (0.8 mg/kg) plusintravenous injection of clopidogrel (3 mg/kg) 7 hourspost-ticagrelor dose
Cangrelor+ticagrelor Intravenous infusion of cangrelor (1 μg/kg/min) for2 hours (0.01 ml/kg/min) plus single oral dose ofticagrelor (0.8 mg/kg) 10 minutes after the start ofcangrelor infusion
623A. Ravnefjord et al. / Thrombosis Research 130 (2012) 622–628
apparent non-competitive manner versus adenosine diphosphate (ADP)[10]. In humans, ticagrelor has a rapid onset of effect with near-complete IPA achieved 2 hours after administration [11], with IPA offsetoccurring over 24 hours [11,12].
Cangrelor is a direct acting, reversibly binding P2Y12 receptor an-tagonist, which is administered intravenously [13,14]. It binds to thesame site on the receptor as ticagrelor (AstraZeneca, data on file).Due to its short half-life (b9 minutes [15]), intravenous cangrelor in-fusion results in rapid and extensive IPA accompanied by almost fullrecovery of platelet activity 60–90 minutes after withdrawal [16].
Several investigative studies have explored cangrelor and clopidogrelinteractions. For example, the low IPA response to clopidogrel in healthyvolunteers or patientswas enhanced by the ex-vivo addition of cangrelor[13,17,18]. However, in healthy volunteers, cangrelor and clopidogrelco-administration reduced the sustained IPA expected with clopidogrelalone [19]. This result suggests that if cangrelor is present at the sametime as clopidogrel's active metabolite, cangrelor may prevent the activemetabolite from binding irreversibly to the P2Y12 receptor. Furthermore,4 hours after cangrelor withdrawal, clopidogrel was still unable to exertan effect on platelet aggregation [19].
Patients with ACS can be transitioned from clopidogrel to ticagrelorwithout interruption of antiplatelet effect [8,9]. However, given the po-tential for ticagrelor, clopidogrel and cangrelor to be used in the sameclinical settings, further understanding of potential pharmacodynamicinteractions between all these antiplatelet agents are of great interest.The objectives of the present ex-vivo canine study were to evaluatethe effects of cangrelor, ticagrelor, and clopidogrel on ADP-inducedIPA and to assess potential pharmacodynamic interactions betweenthese agents. The influence of clopidogrel on ticagrelor's pharmacoki-netics was also explored.
Materials and methods
Test agents and dosing preparations
Cangrelor was supplied by AstraZeneca R&D, Charnwood, UK.Ticagrelor was provided by AstraZeneca R&D, Södertälje, Sweden.Clopidogrel was purchased from Sequoia Research Products Limited,Pangbourne, UK.
Dosing solutions of cangrelor (0.1 mg/ml) were prepared in 0.9% sa-line. Ticagrelor suspensions (0.4 mg/ml) were made in 1% (w/v) sodiumcarboxymethylcellulose/0.1% (v/v) Tween 80. Clopidogrel dosing solu-tions (3 mg/ml) were prepared in 28% hydroxypropyl-beta-cyclodextrinwith pH adjustment to 5–6 using sodium hydroxide. All solutions werefilter-sterilized before use.
Animals
Seven male beagle dogs, aged 10 months to 5 years, with a weightrange of 12.4–17.8 kg, were obtained from Rååhöjden, Örkelljunga,Sweden. They were pair-housed under standard conditions of tempera-ture (18–22 °C), humidity (30–60%) and light (12-hour light/dark cycle),with access to indoor and outdoor runs. Animalswere fed Löwens specif-ic GLP diet (Vet XX,Malmö, Sweden) and had free access to tapwater. Alldogs were acclimatized for at least 5 days before the study. For each ex-perimental phase, dogs were housed within the laboratory during theperiod of frequent blood sampling.
All animal procedures were reviewed and approved by the LocalEthics Review Committee on Animal Experiments, Gothenburg, Sweden.
Experimental design
The dosing regimens are listed in Table 1. To achieve almost com-plete inhibition of ADP-induced platelet aggregation the dosing regi-mens selected for this study were: intravenous infusion of cangrelorat 1 μg/kg/min for 1 or 2 hours; a single oral dose of ticagrelor
(0.8 mg/kg); an intravenous bolus injection of clopidogrel (3 mg/kg).The ticagrelor dose was selected based upon previous experience inour lab to obtain maximum platelet aggregation and complete reversalwithin one experimental day, raher than to mimic the clinically ob-served off-set time. Two dosing regimens were selected to evaluatethe potential pharmacodynamic interaction between ticagrelor andclopidogrel; clopidogrel was given 3 or 7 hours after ticagrelor to coin-cide with the peak and trough IPA responses to ticagrelor, respectively.To evaluate interactions with cangrelor, clopidogrel or ticagrelor weredosed during the cangrelor infusion at 30 minutes or 10 minutes afterthe start of cangrelor infusion, respectively.
All dogswere fasted for 12 hours prior to dosing. A total of seven dogswere used and three to seven dosing regimens were tested in each dog.Based on previous experience, a sample size of six dogs in each regimenwas sufficient to achieve stable data on platelet aggregation.
Assessment of platelet aggregation
ADP-induced platelet aggregation in whole blood samples wasassessed by impedance aggregometry [20,21]. Blood samples of approxi-mately 1 ml were collected from the vena jugularis or vena cephalica intoheparinized tubes (Becton Dickinson, Franklin Lakes, NJ, USA). Within10 minutes, 0.3 ml blood was added to 0.3 ml 0.9% saline in a test cellof a Multiplate® analyzer (Dynabyte, Munich, Germany) and incubatedfor 3 minutes at 37 °C with constant stirring. Platelet aggregation wasstimulated by adding ADP (Dynabyte, Munich, Germany) to a final con-centration of 6.5 μM, and the increase in impedance was measured over10 minutes. Blood samples were collected at regular intervals starting atbaseline (predose) and sampling continued until the aggregation re-sponse had returned to baseline values. Actual blood collection timesare shown in the Results.
Ticagrelor and AR-C124910XX analyses
In order to better characterize the nature of the potential interactionbetween ticagrelor and clopidogrel, the pharmacokinetics of ticagrelorand its metabolite, AR-C124910XX, were investigated in dogs. For bloodsamples collected postdosing with ticagrelor, the remaining blood (afterthe IPA test) was placed on ice immediately. Within 30 minutes, thesesamples were centrifuged (2000 g, 10 minutes, 4 °C), and the plasmastored frozen at−20 °C until analyzed.
A modified liquid chromatography with mass spectrometry meth-od was used to analyze plasma concentrations of ticagrelor andAR-C124910XX; the lower limit of quantification (LLOQ) was 10 nMfor both analytes. The method was similar to a fully validated methodused for human plasma [22].
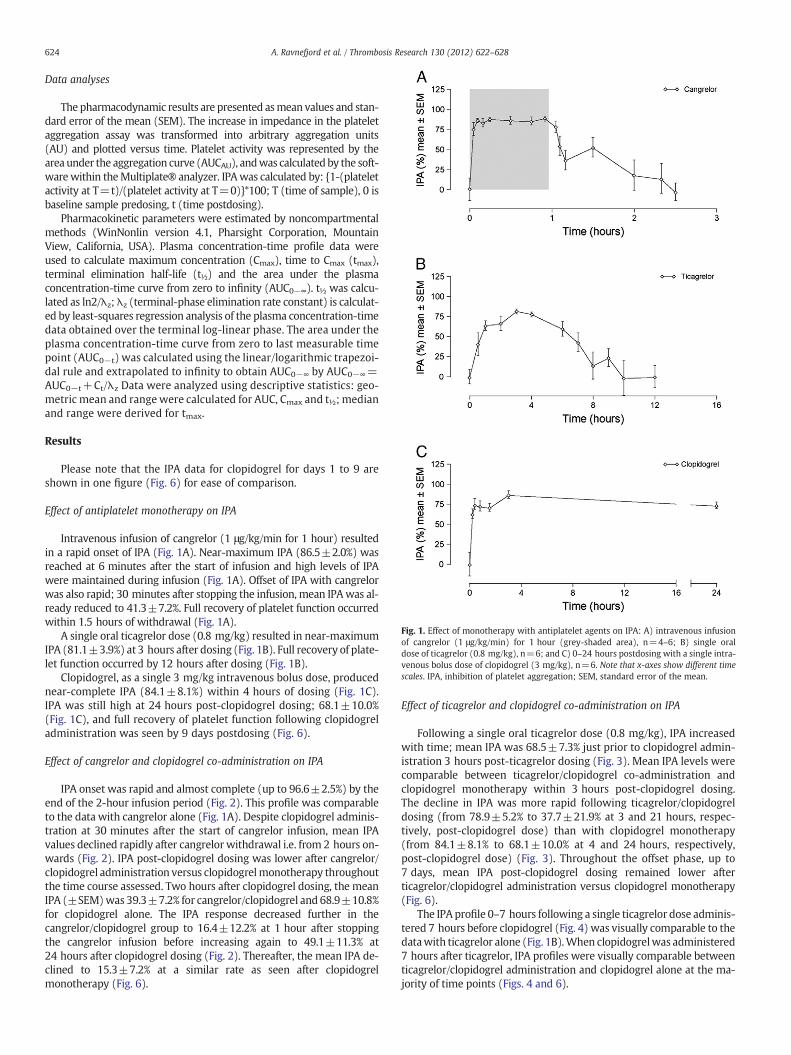
Fig. 1. Effect of monotherapy with antiplatelet agents on IPA: A) intravenous infusionof cangrelor (1 μg/kg/min) for 1 hour (grey-shaded area), n=4–6; B) single oraldose of ticagrelor (0.8 mg/kg), n=6; and C) 0–24 hours postdosing with a single intra-venous bolus dose of clopidogrel (3 mg/kg), n=6. Note that x-axes show different timescales. IPA, inhibition of platelet aggregation; SEM, standard error of the mean.
624 A. Ravnefjord et al. / Thrombosis Research 130 (2012) 622–628
Data analyses
The pharmacodynamic results are presented asmean values and stan-dard error of the mean (SEM). The increase in impedance in the plateletaggregation assay was transformed into arbitrary aggregation units(AU) and plotted versus time. Platelet activity was represented by thearea under the aggregation curve (AUCAU), andwas calculatedby the soft-warewithin theMultiplate® analyzer. IPAwas calculated by: {1-(plateletactivity at T=t)/(platelet activity at T=0)}*100; T (time of sample), 0 isbaseline sample predosing, t (time postdosing).
Pharmacokinetic parameters were estimated by noncompartmentalmethods (WinNonlin version 4.1, Pharsight Corporation, MountainView, California, USA). Plasma concentration-time profile data wereused to calculate maximum concentration (Cmax), time to Cmax (tmax),terminal elimination half-life (t½) and the area under the plasmaconcentration-time curve from zero to infinity (AUC0−∞). t½ was calcu-lated as ln2/λz;λz (terminal-phase elimination rate constant) is calculat-ed by least-squares regression analysis of the plasma concentration-timedata obtained over the terminal log-linear phase. The area under theplasma concentration-time curve from zero to last measurable timepoint (AUC0−t) was calculated using the linear/logarithmic trapezoi-dal rule and extrapolated to infinity to obtain AUC0−∞ by AUC0−∞=AUC0−t+Ct/λz Data were analyzed using descriptive statistics: geo-metric mean and rangewere calculated for AUC, Cmax and t½; medianand range were derived for tmax.
Results
Please note that the IPA data for clopidogrel for days 1 to 9 areshown in one figure (Fig. 6) for ease of comparison.
Effect of antiplatelet monotherapy on IPA
Intravenous infusion of cangrelor (1 μg/kg/min for 1 hour) resultedin a rapid onset of IPA (Fig. 1A). Near-maximum IPA (86.5±2.0%) wasreached at 6 minutes after the start of infusion and high levels of IPAwere maintained during infusion (Fig. 1A). Offset of IPA with cangrelorwas also rapid; 30 minutes after stopping the infusion, mean IPAwas al-ready reduced to 41.3±7.2%. Full recovery of platelet function occurredwithin 1.5 hours of withdrawal (Fig. 1A).
A single oral ticagrelor dose (0.8 mg/kg) resulted in near-maximumIPA (81.1±3.9%) at 3 hours after dosing (Fig. 1B). Full recovery of plate-let function occurred by 12 hours after dosing (Fig. 1B).
Clopidogrel, as a single 3 mg/kg intravenous bolus dose, producednear-complete IPA (84.1±8.1%) within 4 hours of dosing (Fig. 1C).IPA was still high at 24 hours post-clopidogrel dosing; 68.1±10.0%(Fig. 1C), and full recovery of platelet function following clopidogreladministration was seen by 9 days postdosing (Fig. 6).
Effect of cangrelor and clopidogrel co-administration on IPA
IPA onset was rapid and almost complete (up to 96.6±2.5%) by theend of the 2-hour infusion period (Fig. 2). This profile was comparableto the data with cangrelor alone (Fig. 1A). Despite clopidogrel adminis-tration at 30 minutes after the start of cangrelor infusion, mean IPAvalues declined rapidly after cangrelor withdrawal i.e. from 2 hours on-wards (Fig. 2). IPA post-clopidogrel dosing was lower after cangrelor/clopidogrel administration versus clopidogrelmonotherapy throughoutthe time course assessed. Two hours after clopidogrel dosing, the meanIPA (±SEM)was 39.3±7.2% for cangrelor/clopidogrel and 68.9±10.8%for clopidogrel alone. The IPA response decreased further in thecangrelor/clopidogrel group to 16.4±12.2% at 1 hour after stoppingthe cangrelor infusion before increasing again to 49.1±11.3% at24 hours after clopidogrel dosing (Fig. 2). Thereafter, the mean IPA de-clined to 15.3±7.2% at a similar rate as seen after clopidogrelmonotherapy (Fig. 6).
Effect of ticagrelor and clopidogrel co-administration on IPA
Following a single oral ticagrelor dose (0.8 mg/kg), IPA increasedwith time; mean IPA was 68.5±7.3% just prior to clopidogrel admin-istration 3 hours post-ticagrelor dosing (Fig. 3). Mean IPA levels werecomparable between ticagrelor/clopidogrel co-administration andclopidogrel monotherapy within 3 hours post-clopidogrel dosing.The decline in IPA was more rapid following ticagrelor/clopidogreldosing (from 78.9±5.2% to 37.7±21.9% at 3 and 21 hours, respec-tively, post-clopidogrel dose) than with clopidogrel monotherapy(from 84.1±8.1% to 68.1±10.0% at 4 and 24 hours, respectively,post-clopidogrel dose) (Fig. 3). Throughout the offset phase, up to7 days, mean IPA post-clopidogrel dosing remained lower afterticagrelor/clopidogrel administration versus clopidogrel monotherapy(Fig. 6).
The IPA profile 0–7 hours following a single ticagrelor dose adminis-tered 7 hours before clopidogrel (Fig. 4) was visually comparable to thedatawith ticagrelor alone (Fig. 1B).When clopidogrelwas administered7 hours after ticagrelor, IPA profiles were visually comparable betweenticagrelor/clopidogrel administration and clopidogrel alone at the ma-jority of time points (Figs. 4 and 6).

Fig. 2. Effect of cangrelor and clopidogrel co-administration on IPA. Cangrelor (1 μg/kg/min)was administered by intravenous infusion for 2 hours (grey-shaded area). Clopidogrel wasadministered as a single intravenous bolus dose (3 mg/kg) 30 minutes after the start ofcangrelor infusion (indicated by the arrow). Time 0=start of cangrelor dosing(cangrelor+clopidogrel group), and start of clopidogrel dosing (clopidogrel group).n=3–6. IPA, inhibition of platelet aggregation; SEM, standard error of the mean.
Fig. 4. Effect of ticagrelor and clopidogrel co-administration on IPA. Ticagrelor was ad-ministered as a single oral dose (0.8 mg/kg). Clopidogrel was administered as a singleintravenous bolus dose (3 mg/kg) 7 hours postdosing with ticagrelor (indicated by thearrow). Time 0=start of ticagrelor dosing (ticagrelor+clopidogrel group), and start ofclopidogrel dosing (clopidogrel group). n=5–6. IPA, inhibition of platelet aggregation;SEM, standard error of the mean.
625A. Ravnefjord et al. / Thrombosis Research 130 (2012) 622–628
Effect of cangrelor and ticagrelor co-administration on IPA
For the cangrelor/ticagrelor co-administration experiment, baselinevalues (t=0 hours) were unexpectedly low (784±115 AU*min) com-paredwith the baseline values from the same animals in the 6 other ex-periments, which ranged from 1150±108 to 1298±160 AU*min.Thus, the AUCAU value after full recovery at t=10 hours (1159±194 AU*min)was used to normalize these data since completewashoutof both cangrelor and ticagrelor would be expected at this time point.
IPA increased rapidly (86.7±6.7% at 6 minutes) during the first10 minutes of cangrelor infusion (no ticagrelor) (Fig. 5). Mean IPAvalues remained high after ticagrelor administration (10 minutes afterthe start of cangrelor infusion) during the remaining cangrelor infusionperiod (72.7±8.7% to 85.7±6.7%) (Fig. 5). Following cangrelor with-drawal, mean IPA levels declined over time (Fig. 5) comparable withticagrelor monotherapy: 67.1±9.0% versus 81.1±3.9%, 50.5±3.0%versus 59.3±7.0%, and 15.6±6.2% versus 17.3±13.2% at approximate-ly 3, 6 and 8 hours post-ticagrelor dosing (Fig. 5).
Ticagrelor pharmacokinetics
Following a single oral dose of 0.8 mg/kg, ticagrelor was rapidlyabsorbed (Fig. 7A). Mean Cmax was 0.19 μmol/l, median tmax was2.5 hours, and mean t½ was 2 h (Table 2). The major metabolite,AR-C124910XX, was rapidly formed (Fig. 7B), with a mean Cmax of0.031 μmol/l and the median tmax was 2 hours (Table 2).
Administration of clopidogrel (3 mg/kg, intravenously) 3 hours afterticagrelor had no effect on ticagrelor plasma levels (Fig. 7A) or pharmaco-kinetic parameters (Table 2). When clopidogrel was given 7 hours afterticagrelor, elimination of ticagrelor was slightly prolonged (Fig. 7A). All
Fig. 3. Effect of ticagrelor and clopidogrel co-administration on IPA. Ticagrelor was ad-ministered as a single oral dose (0.8 mg/kg). Clopidogrel was administered as a singleintravenous bolus dose (3 mg/kg) 3 hours postdosing with ticagrelor (indicated by thearrow). Time 0=start of ticagrelor dosing (ticagrelor+clopidogrel group), and start ofclopidogrel dosing (clopidogrel group). n=5–6. IPA, inhibition of platelet aggregation;SEM, standard error of the mean.
available plasma samples were analyzed for AR-C124910XX. However,AR-C124910XX concentrations were below the LLOQ in the majority ofplasma samples collected from approximately 6 hours after ticagrelordosing. Mean concentrations were only calculated if ≥60% of sampleshad detectable levels of AR-C124910XX. Thus, as clopidogrel was dosedeither 3 or 7 hours after ticagrelor administration, the mean plasma con-centrations of AR-C124910XX could not be calculated for samples collect-ed after clopidogrel administration (Fig. 7B).
Intravenous infusion of cangrelor (1 μg/kg/min for 2 hours, 10 mi-nutes prior to ticagrelor dosing) had no apparent effect on the plasmaconcentration profiles of ticagrelor (Fig. 7A) or AR-C124910XX (Fig. 7B).
Discussion
Ticagrelor and cangrelor are direct-acting, reversibly-binding P2Y12
receptor antagonists [10,13], whereas clopidogrel requires conversionto an active metabolite [23] which binds irreversibly to the receptor[24,25]. We investigated possible pharmacodynamic interactions aftersingle dose administration of these agents in dogs.
Comparison between the dog model results and pharmacodynamiceffects in humans
The cangrelor dosing regimen (1 μg/kg/min for 1 hour) was selectedbased on published data [13]. The current cangrelor IPA results in dogsclosely agreewith those in healthy volunteers inwhom therewas exten-sive IPA within 2 minutes of infusion and near full recovery of plateletfunction 60–90 minutes after withdrawal [16] versus 6 and 90 minutesin dogs, respectively.
Fig. 5. Effect of cangrelor and ticagrelor co-administration on IPA. Cangrelor (1 μg/kg/min)was administered by intravenous infusion for 2 hours (grey-shaded area). Ticagrelorwas ad-ministered as a single oral dose (0.8 mg/kg) 10 minutes after the start of cangrelor infusion(indicated by the arrow), n=3–6. Time 0=start of ticagrelor dosing (cangrelor+ticagrelorgroup), and start of ticagrelor dosing (ticagrelor group). Note: cangrelor/ticagrelor IPA datanormalized to t=10 hours (see text). IPA, inhibition of platelet aggregation; SEM, standarderror of the mean.

Fig. 6. Effect of co-administration of clopidogrel with cangrelor or ticagrelor on IPA for days 1 to 9 post-dosing.
626 A. Ravnefjord et al. / Thrombosis Research 130 (2012) 622–628
In a dose-findingdog study, a single oral ticagrelor dose of 0.4 mg/kgresulted in limited IPA in all animals (AstraZeneca, data on file); where-as 0.8 mg/kg provided an IPA pattern comparable with that seen withsingle dose administration in humans [11]. Thus, the ticagrelor dose se-lected for these studieswas 0.8 mg/kg. A single oral dose of ticagrelor indogs produced near-maximum IPA approximately 3 hours postdosing,which was slightly longer than previously seen in humans, i.e. within2 hours [11]. A difference in IPA offset with ticagrelorwas also apparentbetween dogs and humans. Full platelet recovery was seen by 12 hoursin dogs (0.8 mg/kg ticagrelor), whilst in humans the mean IPA (range)was 35% (0–100%) and 74% (51–98%) at 12 hours post dosing with sin-gle oral doses of ticagrelor of 30 and 100 mg (approximately equivalentto 0.4 and 1.3 mg/kg) [11]. This apparent difference in pharmacody-namic response may be explained by species differences in ticagrelorpharmacokinetics. For example, the t½ of ticagrelor was approximately2 hours in dogs (present study) in contrast with 4–9 hours reported in
Fig. 7.Mean (±standard deviation) plasma concentration-timeprofiles of A) ticagrelor, n=5–6, and B) AR-C124910XX, n=4–5, following administration of ticagrelor (0.8 mg/kg)alone or in combination with clopidogrel (3 mg/kg) or cangrelor (1 μg/kg/min for2 hours). Time 0=ticagrelor dosing. Note: mean plasma concentrations of AR-C124910XXwere only calculated if ≥60% of samples had values>LLOQ. The majority of samples collectedafter clopidogrel administration were bLLOQ, so mean AR-C124910XX concentrations couldnot be calculated.
healthy volunteers [11,12]. Also, Cmax in the present study was lowercompared than that shown in humans after a single dose of 50 mg,equivalent to approximately 0.7 mg/kg (0.42 μmol/l) [12].
IPA variability due to drug absorption, metabolism and new plateletgeneration
Clopidogrel is administered orally in the clinical setting [1,2], and var-iability in IPA occurs in patientswhich ismainly due to differences in drugabsorption [26] and themetabolismof clopidogrel to its activemetabolite,which is dependent on the genetic variation in cytochrome P450 2C19[27]. To avoid differences in drug exposure due to drug absorption, intra-venous administration has previously been used for clopidogrel in dogsand results in almost complete P2Y12 antagonism in individual animals[28]. In the present study, after a single intravenous dose of clopidogrel(3 mg/kg) in dogs, maximum platelet inhibition was seen within4 hours after dosing, with a slow recovery over 7 days. Given differencesin clopidogrel dose and route of administration, our data in dogs are notdirectly comparable to earlier data in humans. However, themore consis-tent level of IPA observed using this dosing regimen allowed us to study apotential pharmacodynamic interaction in a limited number of animals.The slow offset of IPA is consistent with irreversible inhibition of P2Y12receptors, with recovery being dependent upon the generation of newplatelets; the platelet life span is approximately 5–6 days in dogs [29]and approximately 10 days in humans [30].
In the present study, pretreatment with cangrelor before clopidogreladministration in dogs reduced IPA versus clopidogrel alone. This findingis consistent with data from a healthy volunteer study, in whichco-administration of cangrelor reduced the sustained IPA expected in re-sponse to clopidogrel [19]. The similarity of the results in dogs andhumans support the validity of our canine model to study the effects ofcombining P2Y12 antagonists. Interestingly, in the present dog study,after an initial decline in IPA during the first hour post cangrelor with-drawal, IPA apparently increased for approximately 24 hours afterclopidogrel administration. The reason for this increase in the pharmaco-dynamic effect is unknown. However, we speculate that the inactive acidmetabolite of clopidogrel could form a glucuronide conjugate thatwouldthen be excreted in the bile, hydrolyzed, reabsorbed and subsequentlymetabolized to the active thiol metabolite resulting in increased IPAover a longer period of time i.e. up to 24 hours. As the human volunteerstudy reported by Steinhubl et al. only evaluated IPA over a 6-hour peri-od [19], it is of potential interest to evaluate the IPA profile withcangrelor/clopidogrel in humans over 24 hours for comparison withthe present data in dogs. Our study demonstrated that the decline ofIPA post the 24 hour timepoint was similar between the cangrelor/clopidogrel and clopidogrel alone regimens, which reflects theturn-over velocity of platelets irreversibly bound to clopidogrel.

Table 2Summary of ticagrelor and AR-C124910XX pharmacokinetic parameters following a single oral dose of ticagrelor (0.8 mg/kg) alone or in combination with clopidogrel or cangrelor.Clopidogrel (intravenous bolus, 3 mg/kg) dosed at 3 or 7 hours post-ticagrelor dose. Cangrelor administered as an intravenous infusion (1 μg/kg/min) for 2 hours, ticagrelor dosegiven 10 minutes after the start of cangrelor infusion.
Dosing regimen§ AUC(h⋅μmol/l)*†
Cmax
(μmol/l)*tmax (h)** t½ (h)*
TicagrelorTicagrelor 0.90 (0.57–1.21) 0.19 (0.11–0.29) 2.5 (0.5–3) 2.0 (1.6–2.5)Ticagrelor+clopidogrel at 3 h 0.86 (0.58–1.10) 0.17 (0.10–0.27) 1.5 (1–2) 2.0 (1.8–2.2)Ticagrelor+clopidogrel at 7 h†† 1.02 (0.84–1.43) 0.18 (0.14–0.25) 2 (1–2) 3.8 (2.3–5.3)Cangrelor+ticagrelor 0.96 (0.87–1.10) 0.23 (0.16–0.42) 0.83 (0.83–2.33) 2.4 (2.0–2.7)
AR-C124910XXTicagrelor 0.08 (0.03–0.22) 0.03 (0.02–0.09) 2 (1–3) NCTicagrelor+clopidogrel at 3 h 0.07 (0.02–0.16) 0.03 (0.01–0.05)† 1 (1–2) NCTicagrelor+clopidogrel at 7 h†† 0.07 (0.02–0.22) 0.03 (0.01–0.08) 1 (1–2) NCCangrelor+ticagrelor†† 0.05 (0.01–0.12) 0.03 (0.01–0.06) 1.8 (1.8–2.3) NC
§Number of samples=6 except where indicated; *values are geometric mean (range); †AUC0−∞ for ticagrelor and AUC0−t for AR-C124910XX; **values are median (range); ††number ofsamples=5 for AUC and t½; h hours; NC not calculated.
627A. Ravnefjord et al. / Thrombosis Research 130 (2012) 622–628
Reversible versus non-reversible P2Y12 receptor binding
Following intravenous administration of clopidogrel during infusionof cangrelor, the active metabolite of clopidogrel would be expected tobind irreversibly to P2Y12 receptors not occupied by cangrelor. Due toits very short half-life [15], cangrelor will be cleared rapidly from theplasma after the infusion has been withdrawn. Furthermore, sincecangrelor binds reversibly, this drug would dissociate from the P2Y12
receptors allowing them to become available for binding clopidogrel'sactive metabolite. The apparent increase in IPA in response toclopidogrel after cangrelor withdrawal would indicate the prolongedpresence or formation of the active metabolite of clopidogrel. It isknown that the conversion of clopidogrel to the active thiol metaboliteis a two-step process involving cytochrome P450 isoenzymes [31]. Ascangrelor was withdrawn approximately 1.5 hours post-clopidogreladministration, it is feasible that clopidogrel metabolismwould contin-ue to occur during and after this time period. Indeed, previous data haveshown that following intravenous administration of the active thiolme-tabolite of clopidogrel (0.42 mg/kg) its half-life was 1.27±0.07 hoursin dogs [31]. This finding supports the hypothesis that this active me-tabolite may still be available after cangrelor withdrawal at 1.5 hourspost-clopidogrel dosing in the present study. However, further investi-gations would be required to address this hypothesis.
Ticagrelor, like cangrelor, also binds reversibly to P2Y12 receptors andthus, as ticagrelor and its active metabolite AR-C124910XX are eliminat-ed, the receptors become available for binding [10,13]. When clopidogrelwas administered 3 hours after ticagrelor, coinciding with the peakticagrelor IPA response (with relatively few receptors available for bind-ing clopidogrel's active metabolite), the maximum IPA response toclopidogrel was reduced versus clopidogrel alone. However, the magni-tude of this reduction was less than that seen with cangrelor/clopidogrelco-administration. In contrast, administration of clopidogrel 7 hours afterticagrelor to coincide with the trough ticagrelor IPA response (withmorereceptors available for binding clopidogrel's active metabolite) showedno difference in the IPA response to clopidogrel compared withclopidogrel alone.
Mechanism of interaction
The mechanism of interaction between clopidogrel and ticagrelor orcangrelor may be explained by considering the nature of the binding ofthese agents to the P2Y12 receptor. Cangrelor and ticagrelor reversiblybind to the same site on the receptor, which is distinct from theADP-binding site [AstraZeneca, data on file; 7,32]. In contrast,clopidogrel's active metabolite binds irreversibly to the P2Y12 receptor,and is likely to involve cysteine-97. Subsequent receptor assembly andmembrane localization are thereby disrupted, preventing ADP binding[33]. We therefore postulate that, for the dosing regimens evaluated in
our study, high, intermediate and low receptor occupancy was achievedat steady-state for cangrelor, and 3 or 7 hours post-ticagrelor dosing, re-spectively. Moreover, our IPA results indicate that the higher the level ofreceptor occupancy by a reversibly-binding inhibitor the less effectiveclopidogrel appears to be in subsequently inducing a sustained IPA re-sponse. The exact mechanism(s) of how cangrelor and ticagrelor reducethe action of clopidogrel are unknown. However, it has been hypothe-sized that ticagrelor binding to the P2Y12 receptor inhibits conformationalchanges induced by ADP binding [7,32]. By reducing the flexibility of theP2Y12 receptor, reversibly-binding receptor antagonistsmay also alter ac-cessibility of the cysteine-97 residue considered to be involved in the in-hibition of ADP-induced platelet aggregation by clopidogrel [33].Observations from a recently published in vitro study suggesting compe-tition between cangrelor and the clopidogrel active metabolite are inagreement with our hypothesis that high levels of receptor occupancyby these reversible antagonists could reduce access to the clopidogrel ac-tive metabolite binding site [34].
Our study also demonstrated that high levels of IPAwere achieved bythe co-administration of cangrelor with ticagrelor. After cangrelor with-drawal, the IPA profile was visually comparable to that achieved withticagrelor monotherapy, indicating that there was no significant phar-macodynamic interaction between these agents. A lack of interaction be-tween cangrelor and ticagrelor is perhaps not unexpected, as IPA shouldreflect plasma drug concentrations of reversible inhibitors [32] Thus,when cangrelor is withdrawn and cleared rapidly from the plasma,ticagrelor should bind to the receptors as they become available inorder to maintain antagonism.
Limitations
The present study in dogs had several limitations. These include: smallnumber of dogs evaluated; use of intravenous clopidogrel rather than oraldosing; short duration of dosing; only one dose level per compound wasevaluated; assessment of only a limitednumber of time intervals betweenadministration of thefirst and second agents. In addition, the applicabilityof these findings to humans remains to be confirmed in clinical studies.
Conclusion
In summary, using an ex-vivo canine model, this study demon-strated the importance of the timing of clopidogrel dosing followingticagrelor administration; no interaction between ticagrelor andclopidogrel was seen if the latter was dosed at declining ticagrelorIPA levels. Although a pharmacodynamic drug-drug interaction wasseen between cangrelor and clopidogrel, no significant pharmacody-namic interaction occurred with cangrelor and ticagrelor.

628 A. Ravnefjord et al. / Thrombosis Research 130 (2012) 622–628
Conflict of Interest Statement
All authors are employees of AstraZeneca.
Acknowledgements
The authors acknowledge the hard work and support from the fol-lowing personnel at AstraZeneca R&D Mölndal, Sweden: MargaretaElg, Petra Delavaux and Johanna Tornvall (Department of Bioscience),Niclas Clemmensen (Formulation Science OCR), Jonas Bäckström,Göran Ljungkvist, and Anna Carlsson (Global DMPK-IM, RegulatoryBioanalysis). Editorial support in the preparation of this manuscriptwas provided by Jackie Phillipson (medical writer, Gardiner-CaldwellCommunications); this support was funded by AstraZeneca.
References
[1] Bassand JP, Hamm CW, Ardissino D, Boersma E, Budaj A, Fernandez-Aviles F, et al.Guidelines for the diagnosis and treatment of non-ST-segment elevation acutecoronary syndromes. Eur Heart J 2007;28:1598-660.
[2] Yusuf S, Zhao F, Mehta SR, Chrolavicius S, Tognoni G, Fox KK. Effects of clopidogrelin addition to aspirin in patients with acute coronary syndromes withoutST-segment elevation. N Engl J Med 2001;345:494-502.
[3] Pereillo J-M, Maftouh M, Andrieu A, Uzabiaga MF, Fedeli O, Savi P, et al. Structureand stereochemistry of the active metabolite of clopidogrel. Drug Metab Dispos2002;30:1288-95.
[4] Gurbel PA, Bliden KP, Butler K, Tantry US, Gesheff T, Wei C, et al. Randomizeddouble-blind assessment of the ONSET and OFFSET of the antiplatelet effects ofticagrelor versus clopidogrel in patients with stable coronary artery disease, theONSET-OFFSET study. Circulation 2009;120:2577-85.
[5] Boulenc X, Djevli N, Shi J, Perrin L, Brian W, Van Horn R, et al. Effects of omeprazoleand genetic polymorphism of CYP2C19 on the clopidogrel active metabolite. DrugMetab Dispos 2012;40:187-97.
[6] Springthorpe B, Bailey A, Barton P, Birkinshaw TN, Bonnert RV, Brown RC, et al.From ATP to AZD6140: the discovery of an orally active reversible P2Y12 receptorantagonist for the prevention of thrombosis. Bioorg Med Chem Lett 2007;17:6013-8.
[7] Husted S, van Giezen JJ. Ticagrelor: the first reversibly binding oral P2Y12 receptorantagonist. Cardiovasc Ther 2009;27:259-74.
[8] Brilique, summary of product characteristics, 2010. Available at http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/001241/WC500100494.pdf; 2010Last accessed 7 December 2011.
[9] Brilinta TM. US full prescribing information, July 2011. Available at: http://www.accessdata.fda.gov/drugsatfda_docs/label/2011/022433s000lbl.pdf Last accessed7 December 2011.
[10] van Giezen JJ, Nilsson L, Berntsson P, Wissing BM, Giordanetto F, Tomlinson W,et al. Ticagrelor binds to human P2Y12 independently from ADP but antagonizesADP-induced receptor signaling and platelet aggregation. J Thromb Haemost2009;7:1556-65.
[11] Teng R, Butler K. Pharmacokinetics, pharmacodynamics, tolerability, and safetyof single ascending doses of ticagrelor, a reversibly binding oral P2Y12 receptorantagonist, in healthy subjects. Eur J Clin Pharmacol 2010;66:487-96.
[12] Butler K, Teng R. Pharmacokinetics, pharmacodynamics and safety and tolerabilityof multiple ascending doses of ticagrelor in healthy volunteers. Br J Clin Pharmacol2010;70:65-77.
[13] van Giezen JJ, Humphries RG. Preclinical and clinical studies with selective reversibledirect P2Y12 antagonists. Semin Thromb Hemost 2005;31:195-204.
[14] Wang K, Xhou X, Zhou Z, Tarakji K, Carneiro M, Penn MS, et al. Blockade of theplatelet P2Y12 receptor by AR-C69931MX sustains coronary artery recanalizationand improves the myocardial tissue perfusion in a canine thrombosis model.Arterioscler Thromb Vasc Biol 2003;23:357-62.
[15] Storey RF, Oldroyd KG, Wilcox RG. Open multicenter study of the P2T receptorantagonist AR-C69931MX assessing safety, tolerability and activity in patientswith acute coronary syndromes. Thromb Haemost 2001;85:401-7.
[16] AkersWS, Oh JJ, Oestreich JH, Ferraris S,WethingtonM, Steinhubl SR. Pharmacokineticsand pharmacodynamics of a bolus and infusion of cangrelor: a direct, parenteral P2Y12
receptor antagonist. J Clin Pharmacol 2010;50:27-35.[17] Storey RF, Wilcox RG, Heptinstall S. Comparison of the pharmacodynamic effects of
the platelet ADP receptor antagonists clopidogrel and AR-C69931MX in patientswith ischaemic heart disease. Platelets 2002;13:407-13.
[18] Bouman HJ, van Werkum JW, Hackeng CM, Clappers N, ten Berg JM. Cangrelorincreases the magnitude of platelet inhibition and reduces interindividual variabilityin clopidogrel-pretreated subjects. Neth Heart J 2009;17:195-8.
[19] Steinhubl SR, Oh JJ, Oestreich JH, Ferraris S, Charnigo R, Akers WS. Transitioningpatients from cangrelor to clopidogrel: pharmacodynamic evidence of a competitiveeffect. Thromb Res 2008;121:527-34.
[20] Tóth O, Calatzis A, Penz S, Losonczy H, Siess W. Multiple electrode aggregometry:a new device to measure platelet aggregation in whole blood. Thromb Haemost2006;96:781-8.
[21] Sibbing D, Braun S, Jawansky S, Vogt W, Mehilli J, Schömig A, et al. Assessment ofADP-induced platelet aggregation with light transmission aggregometry and multipleelectrode platelet aggregometry before and after clopidogrel treatment. ThrombHaemost 2008;99:121-6.
[22] Sillén H, CookM, Davis P. Determination of ticagrelor and twometabolites in plasmasamples by liquid chromatography and mass spectrometry. J Chromatogr B AnalytTechnol Biomed Life Sci 2010;878:2299-306.
[23] Mega JL, Close SL, Wiviott SD, Shen L, Hockett RD, Brandt JT, et al. CytochromeP-450 polymorphisms and response to clopidogrel. N Engl J Med 2009;360:354-62.
[24] Savi P, Pereillo JM, UzabiagaMF, Combalbert J, Picard C, Maffrand JP, et al. Identificationand biological activity of the active metabolite of clopidogrel. Thromb Haemost2000;84:891-6.
[25] Savi P, Labouret C, Delesque N, Guette F, Lupker J, Herbert JM. P2Y(12), a newplatelet ADP receptor, target of clopidogrel. Biochem Biophys Res Commun2001;283:379-83.
[26] Taubert D, Kastrati A, Harlfinger S, Gorchakova O, Lazar A, von Beckerath N, et al.Pharmacokinetics of clopidogrel after administration of a high loading dose.Thromb Haemost 2004;92:311-6.
[27] Hulot J-S, Bura A, Villard E, Azizi M, Remones V, Goyenvalle C, et al. CytochromeP450 2C19 loss-of-function polymorphism is a major determinant of clopidogrelresponsiveness in healthy subjects. Blood 2006;108:2244-7.
[28] van Giezen JJ, Berntsson P, Zachrisson H, Björkman JA. Comparison of ticagrelor andthienopyridine P2Y12 binding characteristics and antithrombotic and bleeding effectsin rat and dog models of thrombosis/hemostasis. Thromb Res 2009;124:565-71.
[29] Dale GL, Wolf RF, Hynes LA, Friese P, Burstein SA. Quantitation of platelet life spanin splenectomized dogs. Exp Hematol 1996;24:518-23.
[30] Giuliani DC, Ford EH, Morse BS. A rapid method for estimating mean platelet survivaltime. J Nucl Med 1989;30:1550-3.
[31] Hagihara K, Kazui M, Ikenaga H, Nanba T, Fusegawa K, Takahashi M, et al. Comparisonof formation of thiolactones and active metabolites of prasugrel and clopidogrel inrats and dogs. Xenobiotica 2009;39:218-26.
[32] van Giezen JJJ. Optimizing platelet inhibition. Eur Heart J 2008;10(Suppl. D):D23-9.[33] Savi P, Zachayus J-L, Delesque-Touchard N, Labouret C, Hervé C, Uzabiaga MF,
et al. The active metabolite of clopidogrel disrupts P2Y12 receptor oligomers andpartitions them out of lipid rafts. Proc Natl Acad Sci U S A 2006;103:11069-74.
[34] Dovlatova NL, Jakubovski JA, Sugidachi A, Heptinstall S. The reversible P2Y12 antagonistcangrelor influences the ability of the activemetabolites of clopidogrel and prasugrel toproduce irreversible inhibition of platelet function. J Thromb Haemost 2008;6:1153-9.


















