
Evaluation of the first 5 years of a national eye health programme in Vanuatu
7
PDFlib PLOP: PDF Linearization, Optimization, Protection Page inserted by evaluation version www.pdflib.com – [email protected]
-
Upload
carmel-williams -
Category
Documents
-
view
237 -
download
2
Transcript of Evaluation of the first 5 years of a national eye health programme in Vanuatu
PDFlib PLOP: PDF Linearization, Optimization, Protection
Page inserted by evaluation versionwww.pdflib.com – [email protected]

Original Article
Evaluation of the first 5 years of a national eye healthprogramme in VanuatuCarmel Williams MA,1 John L Szetu MSc(Ophth),1,2 Jacqueline Ramke MPH,1 Anna Palagyi BOptom,1
Renee du Toit MPH1 and Garry Brian FRANZCO1
1The Fred Hollows Foundation New Zealand, Auckland, New Zealand; and 2The Pacific Eye Institute, Suva, Fiji
ABSTRACT
Purpose: To evaluate against its objectives the achievementsof the first 5 years of a national eye health programme inVanuatu.
Methods: Programme clinical activity data were collatedfrom surgical logs, clinic and outreach reports, and patientregister books. Cataract surgical outcomes were retrievedfrom monitoring software. Programme annual reportsprovided information about management, infrastructureimprovements, equipment supplied, repaired or replaced,the supply and use of consumables, and human resourcedevelopment and deployment. Costs were determinedfrom project budgets and acquittals.
Results: The programme promoted eye health, includingthrough the integration of eye care into existing healthservices; established adequate facilities, at referral hospitals,provincial hospitals and rural health clinics, with equipmentand manpower to provide eye care appropriate to thelocation; established a primary eye care programme;strengthened cataract services, although its effect on anycataract backlog is unknown; developed a diabetic eyedisease diagnosis and treatment service, but its reach andeffectiveness are unknown; provided accessible comprehen-sive eye care, but its effect on the prevalence of visionimpairment is unknown; and established medical recordsand data collection systems, but these need more attention.
Discussion: This programme achieved much. However,the evaluation highlighted the limitations of inadequateproject design and that, without addressing further humanresource development and the Ministry of Health’s waveringfinancial commitment, there are potential risks to ongoing
services.That revenue generating capacity was not incorpo-rated into this programme may prove to be a flaw that willlimit ongoing access to eye care, especially in rural areas.
Key words: blindness, evaluation, national eye health pro-gramme, Vanuatu, Vision 2020.
INTRODUCTION
The Melanesian archipelago of Vanuatu has 80 islands, 65 ofwhich are inhabited by a total population of 211 000. Morethan 30 000 people live in Port Vila, the capital, on the islandof Efate. The only other urban centre, Luganville, on Santo,the largest island, has 15 000 people. In addition to a referralhospital in each of these two locations, Vanuatu has threeprovincial hospitals and 25 health centres across its six prov-inces. Access to these health services is difficult for the 76% ofthe population that is rural dwelling.1,2 The low annual grossnational income per capita of US$16003 exacerbates accessproblems, as the cost of land and sea transport is high.2
A 1989 survey estimated the prevalence of blindness(better eye visual acuity worse than 3/60, best corrected) was0.37%,4 and recommendations were made to establish anational eye service. This did not occur.
A situation analysis was conducted in 2000 by the FredHollows Foundation, an international non-governmentaldevelopment organization (INGDO). Santo Hospital had aneye clinic with functioning ophthalmoscope, slitlamp, oper-ating microscope and cataract surgical sets, all donated byvisiting teams. There were no facilities or equipment in PortVila. Between 1989 and 2000, those who needed eye caredepended on one local part-time nurse, based on Santo, and35 visits made by foreign eye care teams, providing 482cataract operations, the outcomes of which were not docu-mented. There was no resident eye doctor. It is likely that theprevalence of vision impairment (presenting better eye visualacuity worse than 6/18) increased during this period.
� Correspondence: Dr Garry Brian, The Fred Hollows Foundation NZ, Private Bag 56908, Dominion Road, Auckland 1030, New Zealand. E-mail:
Received 16 September 2007; accepted 14 December 2007.
Clinical and Experimental Ophthalmology 2008; 36: 162–167doi: 10.1111/j.1442-9071.2008.01685.x
© 2008 The AuthorsJournal compilation © 2008 Royal Australian and New Zealand College of Ophthalmologists

A national eye care programme was commenced in 2001.This was based on the principles of Vision 2020: The Right toSight,5 and informed by the 2000 situation analysis, the expe-rience of a Melanesian ophthalmologist recognized as aregional leader in blindness prevention, and theobjectives of the Vanuatu Ministry of Health (MoH), whichrequired integration with existing public sector healthsystems and rural service provision. The aim was to improveeye health and reduce the prevalence of blindness (present-ing visual acuity worse than 3/60) and low vision (presentingvisual acuity 3/60 or better, but worse than 6/18), throughthe development of a sustainable comprehensive eye careservice, principally by training personnel to provide primaryand other eye care at appropriately equipped facilities. Incor-poration of eye care into health planning and services wasaccepted as the responsibility of the MoH. However, imple-mentation of an agreed 5-year plan (2001–2005) dependedon a partnership between the MoH and the INGDO.
This paper reports an evaluation of achievements at theend of both the 5-year work plan and the government/INGDO partnership, and speculates on the likelihood of thenational eye care programme continuing without ongoingINGDO support.
METHODS
Baseline data were extracted from a situation analysis con-ducted in 2000. These concerned nationwide clinical activ-ity, infrastructure and personnel. The contribution made byvisiting teams was included.
In 2006, programme clinical activity data were collatedfrom annual surgical logs, clinic and outreach reports, andpatient register books for the preceding 5 years. Cataractsurgical outcomes were retrieved from ‘OUTCOME’, thefree and downloadable Vision 2020 monitoring software.Clinical data were then disaggregated by gender, place ofservice and diagnosis.
Programme annual reports to the INGDO and MoH pro-vided detailed information about management, infrastructureimprovements, equipment supplied, repaired or replaced, thesupply and use of consumables, and human resource devel-opment and deployment. Costs were determined from theINGDO’s project budgets and their acquittals.
This paper audit was supplemented with specific informa-tion sought from the MoH, the INGDO and eye careworkers as required.
The data were used to evaluate the programme against itsobjectives.
RESULTS
Objective 1: To promote eye health, includingthrough the integration of eye care intoexisting health services
A prevention of blindness committee was formed, eye healthservices were promoted regularly in the media, and on World
Sight Day in 2003, Vanuatu signed up to the World HealthAssembly declaration of support to overcome avoidableblindness.6
Eye clinic space has been provided in general healthfacilities. Government-salaried medical and nursing person-nel were made available to be trained for roles in eye servicedelivery.
Eye service data have been included in the national healthstatistics.
Ophthalmic pharmaceuticals and consumables have beenobtained both through the MoH’s procurement systems andthrough donation. However, there was no certainty of supplyuntil 2004, when they were included on the EssentialMedicines List.
Objective 2: To establish adequate facilities, atreferral hospitals, provincial hospitals and ruralhealth clinics, with equipment and manpowerto provide eye care appropriate to the location
The programme leader, a Solomon Islands ophthalmologistwith experience in managing a national eye health pro-gramme and training eye care providers, was jointlyemployed by the INGDO and MoH. The MoH employedall others recruited to an increased eye care workforce.
Over the 5 years, 10 nurses graduated from 9-month full-time clinic-based training courses in primary eye care (PEC),minor surgical procedures and refraction. On completion oftraining, three nurses were deployed to each of the referralhospitals, one to each of three provincial hospitals and oneto a health centre. Subsequently, one nurse left clinicalservice to take a management position elsewhere. The othernurses had continuing duties at their assigned base facilities,as well as independently providing intermittent services toadjacent rural areas. Also, as members of an outreach teamthat included the programme’s medical officers, they periodi-cally visited more remote locations without resident services.
One Ni-Vanuatu doctor underwent basic ophthalmictraining, initially in-service, and then completing the 1-yearDiploma of Ophthalmology course at the University ofPapua New Guinea, Port Moresby, in 2004. He returned toservice delivery in Vanuatu in 2005.
Annual refresher training workshops were conductedfrom 2003. These promoted collegiality and support for eyehealth workers.
In 2001, the eye programme shared an operating theatreand consultation room in Santo hospital, and had no pres-ence in Vila. By 2005, both hospitals had stand-alone eyeclinics that included outpatient operating theatres. Theseand four other clinics were built and paid for through theefforts of donor agencies, local and international serviceclubs and non-governmental organizations (NGOs). TheINGDO purchased equipment for these facilities.
Objective 3: To establish a PEC programme
In 2000, there was only one eye nurse and no PEC service.By the end of the third year, the programme had trained
Evaluation of an eye programme in Vanuatu 163
© 2008 The AuthorsJournal compilation © 2008 Royal Australian and New Zealand College of Ophthalmologists

sufficient eye nurses to provide permanent PEC and refrac-tion services at six clinics, one in each province. Patientsrequiring additional care were referred to the ophthalmolo-gist, either at Santo or Port Vila hospitals, or arrangementsmade for treatment during annual ophthalmologist outreachvisits to provincial centres.
Eye nurses provided basic PEC training to communityhealth workers. Anecdotally, this improved the appropriate-ness of referrals.
School screening, which had not occurred previously, wasconducted in four of the six provinces. No outcome datawere available, so the benefit or otherwise of this activitycould not be assessed.
Objective 4: To identify and eliminate anycataract backlog, and further strengthencataract services
The eye nurses visited rural areas to screen for cataracts. Theophthalmologist, assisted by the local eye doctor in 2003and 2005, provided surgery for these patients at the provin-cial hospitals and selected health centres. NGOs collabo-rated to transport patients to and from surgery during theseoutreach visits.
The cataract surgical rate increased from approximately200 cataract surgeries per million people in 2000 to about1330 in 2005, with 98.9% receiving intraocular lenses. Thepercentage of surgery performed at rural clinics ranged from19.9 (62/312) in 2002 to 69.8 (210/301) in 2003, returning toabout 50% in 2004 and 2005 (Fig. 1). In total, 1409 cataractsurgeries occurred during the 5 years. Women accounted for39% (549/1409) of these, increasing from 33.2% (79/238) in2001 to 43.9% (123/280) in 2005.
Cataract surgery outcomes exceeded the World HealthOrganization (WHO) recommended minimum standards,
with presenting vision of 6/18 or better in 90.6% of cases,and 94.4% attaining this with pinhole, at 12 weeks or later.Only 1.3% had acuity worse than 6/60.
Objective 5: To develop a diabetic eye diseasediagnosis and treatment service
There was no eye component to the care of people withdiabetes in Vanuatu before 2001.
Diabetic retinopathy screening was included in eye nursetraining, and encouraged in the PEC setting. In all, over the5 years, 141 diabetics were found to have retinopathy. Thesepeople were referred to the ophthalmologist. Laser photo-coagulation was provided for 51 patients, 25 of whomrequired multiple treatments.
The service suffered a set back in 2004 when the laser unitwas shipped overseas for repair. It remained out of commis-sion for 9 months.
Objective 6: To provide accessiblecomprehensive eye care, with the aim ofreducing the national blindness rate
There were 28 109 outpatient consultations recorded,increasing from 3187 in 2001 to 7111 in 2005. Womenaccounted for 44.2% (12 438) of the total, being 43.8% and44.5% of urban and rural visits, respectively. In the first year,38.8% of total visits were by women, rising to 47.4% in2005.
During the 5 years, 24.8% (6962) of consultations tookplace in rural clinics. The outreach team provided 58.7%(4085) of these, with rural eye nurses conducting the remain-der unsupervised.
The diagnosis and management of cataract were respon-sible for 21% of the total outpatient workload as measured
0
50
100
150
200
250
Year
Nu
mb
er o
f ca
tara
ct s
urg
erie
s p
erfo
rmed
0
20
40
60
80
Per
cen
t ru
ral (
%)
Male
Female
Percent rural
2000 20022001 20042003 2005
Figure 1. Cataract surgery inVanuatu (2000–2005): number,gender and location.
164 Williams et al.
© 2008 The AuthorsJournal compilation © 2008 Royal Australian and New Zealand College of Ophthalmologists

by number of patient visits. Eleven per cent of consultationsconcerned the care of pterygia and their symptoms (Fig. 2).
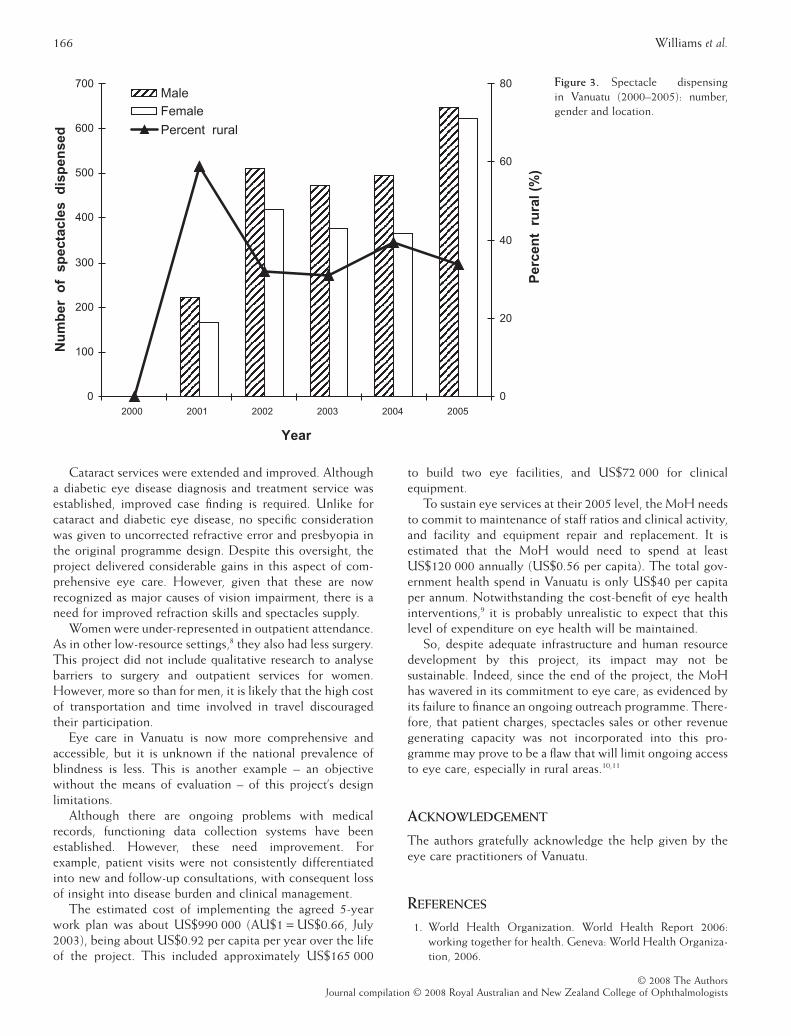
Refractive error and presbyopia accounted for 23% ofpatient visits (Fig. 2). Eye nurses performed best sphericalrefraction and presbyopic correction, and referred astigmaticrefractions to the medical officers. Ready-made spectacleswere available through the six eye clinics and during out-reach visits. In total, 4298 spectacles were dispensed: 33.6%to urban males, 30.1% to urban females, 21.0% to rural malesand 15.2% to rural females (Fig. 3).
The total number of ophthalmic surgical proceduresincreased from 508 in 2001 to 809 in 2005. Overall, 40.4%(1337/3307) of these interventions were delivered in ruralclinics. Cataract surgery accounted for 42.6% of procedures,with 25.7% for pterygium and 8.3% for corneal foreign bodyremoval. Eye care nurses performed 11.9% (395/3307) ofprocedures, most for foreign bodies.
Cost considerations prevented prevalence studies beingconducted before and after the 5 years under review. There-fore, the national blindness prevalence is not known, nor theimpact of the programme on this.
Objective 7: To establish functioning medicalrecords and data collection systems
Patient personal medical history documents were retained bythe clinics, and not, as occurs in some Pacific countries,released to the custody of the patient. However, an audit ofrecords at the end of the project revealed the unavailabilityof notes for at least 1616 patients.
Outpatient and surgical data were kept in daily updatedfacility record books. A service summary, including patientnumbers, gender, ocular condition and treatment, wasgenerated and submitted annually to the MoH. This wasincluded in national health statistics.
From 2002, a database in Excel was used to record cataractsurgeries and vision outcomes. The information wastransferred to OUTCOMES in 2005. This cataract outcomesmonitoring software was used thereafter.
Starting in mid 2005, data on people with best correctedvision less than 6/18 were entered into an Excel spreadsheet.A register of people with best corrected vision less than 3/60was developed in conjunction with the Vanuatu Society forDisabled People.
DISCUSSION
The government/INGDO partnership aimed to create a sus-tainable national comprehensive eye health service toimprove eye health and reduce the prevalence of blindnessand low vision. At the end of the partnership, the project wasevaluated to assess achievements against the stated objec-tives of the plan. This proved difficult because the objectiveswere broad, and generally without specific targets. Also, noevaluation methodology had been agreed at inception.Further, although ongoing collection of service data hadoccurred and been made available to the MoH, fulfilling oneproject objective, information concerning programme devel-opment and execution processes had not been specificallyaccumulated against the objectives. Despite these limitationsand the lack of antecedent and post-project Vanuatu visionimpairment prevalence data, the evaluation reveals consider-able achievement. However, it also highlights the difficultiescreated by inadequate project design.
The objective to promote eye health, including throughthe integration of eye care into existing health services, waspartially successful. The MoH has yet to recognize trainedeye nurses as specialist nurses and provide commensuratesalaries. More community education about eye health anddisease, and use of services, particularly by women, wouldlikely have been beneficial. However, the impact of sucheducation on service utilization was not monitored.
Equipped facilities adequate to provide required andanticipated need were established. However, issues of equip-ment maintenance and replacement need addressing. Thatthe retinal laser was unavailable for 9 months is unacceptableand emphasizes the difficulties of geographical isolationwithout local technical capacity or service contracts.
Human resource development targets were met. The ratioof eye nurses to the population is now 1:23 500, but more areneeded to improve access for rural dwellers. At the end of theproject, the expatriate ophthalmologist returned to theSolomon Islands, leaving the recently qualified indigenouseye doctor to oversee continuing services and provide clini-cal care; this reduced the medical manpower to half thatrecommended by the WHO.7 There is a risk to ongoingservice with only one eye doctor managing all aspects of anational eye programme for a population of this size andgeographical spread.
A PEC programme was set up. Basic eye care training forall health-care personnel would improve this, as would morecommunity-based service.
Cataract21%
Presbyopia17%
Pterygium11%
Other external disease
8%
Refractive error6%
Corneal ulcer5%
Conjunctivitis5%
Eye injury4%
Uveitis3%
Other / No abnormality
20%
Figure 2. Outpatient consultations in Vanuatu (2001–2005):diagnoses.
Evaluation of an eye programme in Vanuatu 165
© 2008 The AuthorsJournal compilation © 2008 Royal Australian and New Zealand College of Ophthalmologists
Cataract services were extended and improved. Althougha diabetic eye disease diagnosis and treatment service wasestablished, improved case finding is required. Unlike forcataract and diabetic eye disease, no specific considerationwas given to uncorrected refractive error and presbyopia inthe original programme design. Despite this oversight, theproject delivered considerable gains in this aspect of com-prehensive eye care. However, given that these are nowrecognized as major causes of vision impairment, there is aneed for improved refraction skills and spectacles supply.
Women were under-represented in outpatient attendance.As in other low-resource settings,8 they also had less surgery.This project did not include qualitative research to analysebarriers to surgery and outpatient services for women.However, more so than for men, it is likely that the high costof transportation and time involved in travel discouragedtheir participation.
Eye care in Vanuatu is now more comprehensive andaccessible, but it is unknown if the national prevalence ofblindness is less. This is another example – an objectivewithout the means of evaluation – of this project’s designlimitations.
Although there are ongoing problems with medicalrecords, functioning data collection systems have beenestablished. However, these need improvement. Forexample, patient visits were not consistently differentiatedinto new and follow-up consultations, with consequent lossof insight into disease burden and clinical management.
The estimated cost of implementing the agreed 5-yearwork plan was about US$990 000 (AU$1 = US$0.66, July2003), being about US$0.92 per capita per year over the lifeof the project. This included approximately US$165 000
to build two eye facilities, and US$72 000 for clinicalequipment.
To sustain eye services at their 2005 level, the MoH needsto commit to maintenance of staff ratios and clinical activity,and facility and equipment repair and replacement. It isestimated that the MoH would need to spend at leastUS$120 000 annually (US$0.56 per capita). The total gov-ernment health spend in Vanuatu is only US$40 per capitaper annum. Notwithstanding the cost-benefit of eye healthinterventions,9 it is probably unrealistic to expect that thislevel of expenditure on eye health will be maintained.
So, despite adequate infrastructure and human resourcedevelopment by this project, its impact may not besustainable. Indeed, since the end of the project, the MoHhas wavered in its commitment to eye care, as evidenced byits failure to finance an ongoing outreach programme. There-fore, that patient charges, spectacles sales or other revenuegenerating capacity was not incorporated into this pro-gramme may prove to be a flaw that will limit ongoing accessto eye care, especially in rural areas.10,11
ACKNOWLEDGEMENT
The authors gratefully acknowledge the help given by theeye care practitioners of Vanuatu.
REFERENCES
1. World Health Organization. World Health Report 2006:working together for health. Geneva: World Health Organiza-tion, 2006.
0
100
200
300
400
500
600
700
Year
Nu
mb
er o
f s
pec
tacl
es d
isp
ense
d
0
20
40
60
80
Per
cen
t r
ura
l (%
)
MaleFemale
Percent rural
2000 20022001 20042003 2005
Figure 3. Spectacle dispensingin Vanuatu (2000–2005): number,gender and location.
166 Williams et al.
© 2008 The AuthorsJournal compilation © 2008 Royal Australian and New Zealand College of Ophthalmologists

2. Szetu JL. Vanuatu national eye care program. J Comm Eye Health2005; 18: 95.
3. World Bank. World Development Indicators Database. WashingtonDC: World Bank, 2005.
4. Newland H, Harris M, Walland M et al. Epidemiology of blind-ness and visual impairment in Vanuatu. Bull World Health Organ1992; 70: 369–72.
5. World Health Organization. Global Initiative for the Elimination ofAvoidable Blindness. Geneva: WHO, 1997.
6. World Health Assembly. Resolution WHA 56.26 Elimination ofAvoidable Blindness. Geneva: World Health Assembly, 2003.
7. World Health Organization. Strategic Plan for Vision 2020: TheRight to Sight; Elimination of Avoidable Blindness in the South-East Asia
Region. New Delhi: WHO, Regional Office for South-East Asia,2000.
8. Lewallen S, Courtright P. Gender and use of cataract surgicalservices in developing countries. Bull World Health Organ 2002;80: 300–3.
9. Frick K, Foster A. The magnitude and cost of global blindness:an increasing problem that can be alleviated. Am J Ophthalmol2003; 135: 471–6.
10. Rao GN. Self sustainability in eye care. Indian J Ophthalmol 1996;44: 129.
11. Brian G, Taylor H. Cataract blindness – challenges for the 21stcentury. Bull World Health Organ 2001; 79: 249–56.
Evaluation of an eye programme in Vanuatu 167
© 2008 The AuthorsJournal compilation © 2008 Royal Australian and New Zealand College of Ophthalmologists


















