Evaluation of esophageal varices in liver disease by splenic-pulp manometry, splenoportography, and...
9
Evaluation of Esophageal Varices in Liver Disease by Splenic-Pulp Manometry, Splenoportography, and Esophagogastroscopy Diagnostic Discrepancies LAWRENCE GREENE, M.D., HERBERT WEISBERG, M.D.,* WILLIAM S. ROSENTHAL, M.D., PETER A. DOUVRES, M.D., and DAVID KATZ, M.D. T HE DISCREPANCY between levels of portal pressure and the presence of collateral circulation in patients with liver disease is unexplained. The problem is further complicated by the difficulty in accurately detect- ing portosystemic collateral circulation. With rare exception, 1, 2 previous studies have employed a single diagnostic procedure (endoscopy a, 4, 5 or barium swallow 6) or the combination of portal-pressure measurements and splenoportography. ~, s, 9 In this study, we combined esophagogas- troscopy, splenic-pulp manometry, and splenoportography in a prospec- tive investigation of a series of patients with liver disease. We used this approach to investigate the relationship between portal pressure, the splenoportographic demonstration of portosystemic collaterals, and rhe endoscopic visualization of esophageal varices. MATERIALS AND METHODS Each of 112 patients with documented liver disease was investigated by means of esophagogastroscopy, splenic-pulp manometry, and spleno- portography between December 1961 and November 1963. Only 60 pa- tients were selected for inclusion in the present report because all three procedures were successfully carried out within 6 days and a diagnosis of liver disease was available on the basis of histologic examination. Esopha- From the Section of Gastroenterology, Department of Medicine, New York Medical College-Metropolitan Hospital Medical Center, New York, N. Y. Supported in part by Graduate Training Grant TI-AM-5237 and Clinical Research Center Grant AM-05576-02 from the National Institute of Arthritis and Metabolic Dis- eases, N.I.H, U. S. Public Health Ser~Sce, and Contract U 1373 of the Health Research Council of the City of New York. *Former U, S. Public Health Service Trainee in Gastroenterology. 284 American Journal of Digestive Diseases
-
Upload
lawrence-greene -
Category
Documents
-
view
212 -
download
0
Transcript of Evaluation of esophageal varices in liver disease by splenic-pulp manometry, splenoportography, and...

Evaluation of Esophageal Varices in Liver Disease by Splenic-Pulp Manometry, Splenoportography, and Esophagogastroscopy Diagnostic Discrepancies
LAWRENCE GREENE, M.D., HERBERT WEISBERG, M.D.,* WILLIAM S. ROSENTHAL, M.D., PETER A. DOUVRES, M.D.,
and DAVID KATZ, M.D.
T HE DISCREPANCY between levels of portal pressure and the presence of collateral circulation in patients with liver disease is unexplained.
T h e p rob lem is fur ther complicated by the difficulty in accurately detect- ing portosystemic collateral circulation. With rare exception, 1, 2 previous studies have employed a single diagnostic procedure (endoscopy a, 4, 5 or ba r ium swallow 6) or the combinat ion of portal-pressure measurements and splenoportography. ~, s, 9 In this study, we combined esophagogas- troscopy, splenic-pulp manometry, and splenopor tography in a prospec- tive investigation of a series of patients with liver disease. We used this approach to investigate the relat ionship between por ta l pressure, the splenoportographic demonstra t ion of portosystemic collaterals, and rhe endoscopic visualization of esophageal varices.
M A T E R I A L S AND M E T H O D S
Each of 112 patients with documented liver disease was investigated by means of esophagogastroscopy, splenic-pulp manometry , and spleno- por tography between December 1961 and November 1963. Only 60 pa- tients were selected for inclusion in the present repor t because all three procedures were successfully carried out within 6 days and a diagnosis of liver disease was available on the basis of histologic examinat ion. Esopha-
From the Section of Gastroenterology, Department of Medicine, New York Medical College-Metropolitan Hospital Medical Center, New York, N. Y.
Supported in part by Graduate Training Grant TI-AM-5237 and Clinical Research Center Grant AM-05576-02 from the National Institute of Arthritis and Metabolic Dis- eases, N.I.H, U. S. Public Health Ser~Sce, and Contract U 1373 of the Health Research Council of the City of New York.
*Former U, S. Public Health Service Trainee in Gastroenterology.
284 American Journal of Digestive Diseases

GREENE ET AL. : DIAGNOSTIC DISCREPANCIES
goscopy was carried out with tile Eder-Hufford flexible esophagoscope.* The diagnosis of esophageal varices at endoscopy was determined by two or more experienced endoscopists participating in the procedure.
The diameter of varices, expressed in millimeters, was estimated by comparison with the 9-mm. lumen of tim esophagoscope. Patients with upper gastrointestinal hemorrhage were judged to be bleeding from esophageal varices only if active bleeding from the varix was demon- strated by endoscopic examination. Immediately following esophagos- copy, gastroscopy was carried out with the Eder-Chamberlain* or Eder- Pahner gastroscope 'x= to determine the presence of gastric varices. Splenic- pulp manometry and splenoportography were always carried out follow- ing endoscopy. The standard contraindications and usual precautions for these procedures were observed, s-I0 Splenic-pulp pressure was measured using an open-water manometer connected by polyethylene tubing to a needle introduced percutaneously into the spleen. The accepted splenic- pulp pressure was the average of three successive manometric readings corrected to the level of the right atrium. Splenoportography was carried out immediately following the measurement of splenic-pulp pressure. Sodium diatrizoate (50 nil., 70%) was injected manually in less than l0 sec. After the first 30 ml., 6 films were taken at 1-sec. intervals using a Sanchez-Perez automatic casette changer.} Following a 5-sec. interval, 6 more exposures were made at 1-sec. intervals.
Splenoportograms were evaluated according to the following criteria: (1) minimal cotlateralization: reflux of the contrast medium into the in-
ferior mesenteric vein and small splenic radicals, and delayed emptying of splenic and portal veins; (9) moderate collateralization: opacification of coronary, short gastric, inferior mesenteric, or superior mesenteric veins; and (3) marhed collateralization: marked diversion of the contrast me- dium into esophageal varices via the coronary and short gastric veins or into large mesenteric collaterals, with poor visualization or lack of filling of the portal vein.
RESULTS Endoscopic Studies
Esophagoscopy demonstrated esophageal varices in 54 (90%) of the 60 patients studied (Fig. 1 and 2). The size of the varices ranged from 1 to 7 ram. in diameter. Of the 20 patients who were actively bleeding from the upper gastrointestinal tract during endoscopy (Fig. 3), 11 (55%) were bleeding from esophageal w~rices. Of the actively bleeding patients,
eEder Instrument Company, Chicago, Ill. J-Automatic Scriograph Corporation, College Park, Md.
New Series, Vol. 10, No. 4, 1965 ~

NEW YORK MEDICAL COLLEGE ISSUE
9 (45%) proved to be bleeding from nonvariceal sites--as determined by means of endoscopy, surgical exploration, and/or gross pathological ex- amination. Four of the 9 were bleeding from duodenal ulcer, 3 from erosive gastritis, and in 2 the site of bleeding was not established. In this group of 9 patients, 8 had esophageal varices which were not bleeding.
Splenic-Pulp Pressure
The range of splenic-pulp pressure in 54 patients with esophageal varices (demonstrated by endoscopy) was 80 to 540 mm. of water. Of
14
12
P- io bJ
8 P, 6
ICl :E 4 #=
2
• L • N O VARICES VISUALIZED
-- ~ NON-BLEEDING VARICES
- - I BLEEDING VARICES
0-9'9 I00- 150- 2 0 0 - 250- 3 0 0 - 5 5 0 - 4 0 0 - 4 5 0 - 5 0 0 + 149 199 2 4 9 299 :349 3 9 9 4 4 9 4 9 9
SPLENIC PULP PRESSURE
Fig. 1. Relationship between splenic-pulp pressure (ram. H20) and presence of endoscopically visualized bleeding and nonbleeding esophageal varices (60 patients).
7
6
7 E S
(D E: 4 x 3 3
2
• Non-bleedlng Varices o Bleeding Varices
*o o *o o
- • o .*
o
50 I00 150 200 250 300 350 400 450
SPLENIC PULP PRESSURE ( mm H20)
50O
Fig. 2. Relationship between splenic-pulp pressure and variceal size (diameter in ram,) estimated by endoscopy (47 patients).
2,86 American Journal of Digestive Diseases

G R E E N E E T A L . : D I A G N O S T I C D I S C R E P A N C I E S
these, 15 patients (28%) had splenic-pulp pressures below 270 mm. of water--of whom 9 (17%) had splenic-pulp pressures below 200 ram. of water (Fig. 1). In 6 patients in whom no varices were noted endoscopical- ty, the pressure range was 190 to 340 ram.
I 0
P_
4
2 z
0
[ - ~ BLEEDING,NO VARICES DEMONSTRATEO
~ BLEEDING,NOT FROM DEMONSTRATED VARtCES
BLEEDING VARICES DEMONSTRATED
50-99, I00- 150- 200- 250- 300- '350- 400- 450- 500+ 149 199 249 299 349 399 449 499
SPLENIC PULP PRESSURE
Fig. 3. Splenic.pulp pressure (mm. H.O) in patients with upper GI hemorrhage: variceal vs. nonvariceal bleeding (20 patients).
Of the 11 patients in whom endoscopy revealed bleeding from esopha- geal varices, 3 had splenic-pulp pressures below 270 mm. of water. Of the 9 patients who were actively bleeding from nonvariceal sites, 8 had splenic pulp pressures above 270 inrn. of water (Fig. 3).
Splenoportographic Studies
Splenoportography demonstrated collateral circulation in 27 (50%) of the patients with esophageal varices previously revealed by endoscopy. In no instance did splenoportography demonstrate collateral circulation not previously visualized by endoscopy (Fig. 4). Splenoportography did not demonstrate collateral circulation in 20 patients whose splenic-pulp pres- sures were less than 270 mm. of water (Fig. 5), despite the fact that 15 (75%) in this group had varices demonstrated by esophagoscopy. Spleno-
portogxaphic collaterals were found in 27 of the 40 patients (67.5%) whose splenic-pulp pressure exceeded 270 mm. of water (Fig. 5). There- fore, of the 40 patients whose splenic-pulp pressures were over 270 mm. of water, 13 (32.5%) had no collaterals demonstrable by splenoportog- raphy and 3 (7.5~) had no collaterals revealed by esophagoscopy and splenoportography. Three patients in whom endoscopy revealed bleeding esophageal varices had splenic-pulp pressures below 270 mm. of water and no splenoportographic collaterals. In the remaining 8 patients with bleeding esophageal varices and pressures above 270 ram. of water, 6 had splenoportographically established evidence of collateral circulation. In the group of 9 patients bleeding from nonvariceal sites, 5 showed spleno- portographic evidence of collateral circulation.
blew Series, Vol. I0, No. 4, 1965 287
N E W Y O R K M E D I C A L C O L L E G E I S S U E
INTERRI~3LATIONStnPS
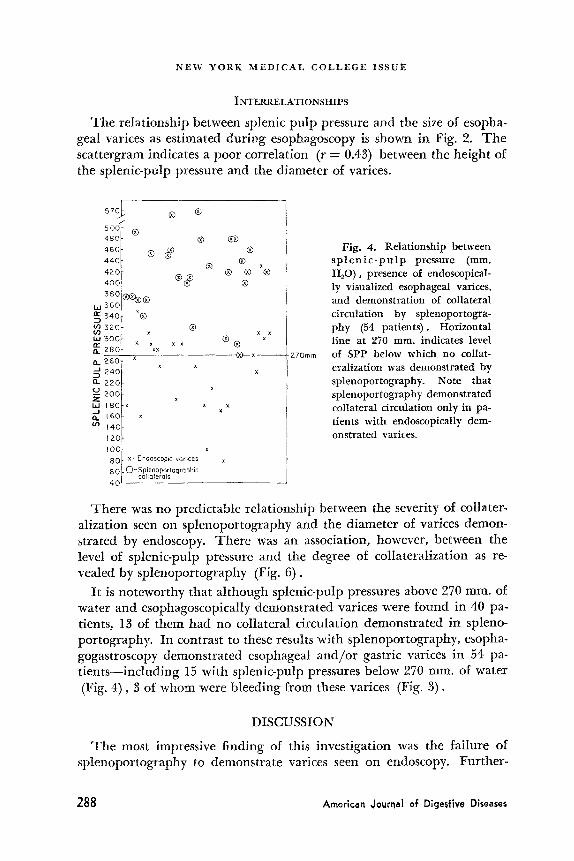
The relationship between splenic pulp pressure and the size of esopha- geal varices as estimated during esophagoscopy is shown in Fig. 2. The scattergram indicates a poor correlation (r = 0.43) between the height of the splenic-pulp pressure and the diameter of varices.
574 50C 48O
46O
44O
42C 40C
$8C
I.~ 56C
~ $ 4 0
u') 320 U')
3 0 0
~ 2 8 C
e. 2 6 0 J 2 4 c
22C
2 0 0 Z jw 18C
~. 16C
t20
I00
8C 6C 4C
® ®
® ® d#
® ®
® ®
×® ®
× × ×
x ~xx x x ® ®
x ® ~ - x -
x x x
x
x x x
x
x - Endoscopic vGrJces x
O-Splenoporlographic collaterals
~®
-270mm
Fig. 4. Relationship between s p l e n i c - p u l p pressure (mm. H~O), presence of endoscopical- ly visualized esophageal varices, and demonstration of collateral circulation by splenoportogra- phy (54 patients). Horizontal line at 270 ram. indicates level of SPP below which no collat- eralization was demonstrated by splenoportography. Note that splenopor tography demonstrated collateral circulation only in pa- tients with endoscopically dem- onstrated varices.
There was no predictable relationship between the severity of collater- alization seen on splenoportography and the diameter of varices demon- strated by endoscopy. There was an association, however, between the level of splenic-pulp pressure and the degree of collateralization as re- vealed by splenoportography (Fig, 6).
It is noteworthy that although splenic-pulp pressures above 270 ram. of water and esophagoscopically demonstrated varices were found in 40 pa- tients, 13 cff them had no collateral circulation demonstrated in spleno- portography. In contrast to these results with splenoportography, esopha- gogastroscopy demonstrated esophageal and/or gastric varices in 54 pa- tients-including 15 with splenic-pulp pressures below 270 ram. of water (Fig. 4), 3 of whom were bleeding from these varices (Fig. 3).
DISCUSSION
The most impressive finding of this investigation was the failure of splenoportography to demonstrate varices seen on endoscopy. Further-
288 American Journal of Dige~'~ive Diseases

G R E E N E E T A L . : D I A G N O S T I C D I S C R E P A N C I E S
more, portal pressure (reflected by splenic-pulp pressure), correlated i~oorly with the diameter of varices seen endoscopically. In patients with ~q)l)er gastrointestinal hemorrhage, an elevated splenic-pulp pressure was :~ poor index of the site of bleeding. Several patients with severe portal
12
o 1 0
- - 8
11. u- 6 0
,.'5, 4 Ill =E
Z 2
5 0 - 9 9 I 0 0 - 1 5 0 - 2 0 0 - 2 7 I - ,300- ,350- 4 0 0 - 4 5 0 - 5 0 0 + 149 199 2 7 0 2 9 9 ,3'49 3 9 9 4 4 9 4 9 9
SPLENIC PULP PRESSURE
Fig. 5. Relationship between splenic-pulp pressure and demonstration of porto- systemic collerateral circulation by splenoportography (60 patients).
hypertension and esophageal varices were bleeding from nonvariceal sites (Fig. 8).
Splenoportography was emphasized by T u r n e r et a l2 and since then by others 7, s, 10 as an excellent method of demonstrating portosystemic col- lateral circulation and especially esophageal varices. This has recently been questioned by several authors 1~, 12, Ia who have described bleeding and nonbleeding varices in the presence of a normal splenoportogram. This phenomenon has not been fully explained, but it may be due to such factors as density of the contrast medium, positioning of the patient, and flow characteristics of the portal system--as has been suggested by Bergstrand and Ekman. 1~, 15 Other purely technical factors, such as using a small amount of contrast medium, prolonged injection time, and an inadeqnate number or durat ion of exposures were eliminated in our study because of the technique employed. Since no splenoportographic col- laterals were visualized with a splenic-pulp pressure below 270 mm., it is suggested that a portal pressure in this range is necessary before collater- alization will be demonstrated by the method.
T h e poor correlation between portal pressure and variceal diameter confirms the work of Palmer 3, 1~ and de Castro Silva et al. 1 Our findings further underscore the difficulty involved in numerically defining the limits of normal portal pressure. This is illustrated by the wide range of normal values found by others (Table 1) and, in our study, by the wide range of splenic-pulp pressures noted in patients with liver disease
New Ser~es, Vol. 10, No. 4, 1965 ~ - ~

N E W YORK M E D I C A L C O L L E G E I S S U E
and endoscopically demonstrated bleeding and nonbleeding esophageal varices (Fig. I ) .
The fact that endoscopically demonstrated esophageal varices were found over a wide range of splenic-pulp pressures and in the presence of normal splenoportograms is particularly significant. Endoscopically vis- ualized esophageal varices have been described in the absence of liver disease and portal hypertension 5 and may account for such a discrepancy in a small number of cases. Furthermore, we recognize that there are technical limitations in the endoscopic diagnosis of esophageal varices and particularly in the accurate estimation o[ variceal size. a, 20 Nevertheless.
600
500
~ 300
- Standord error T ~o 200 -Jr Me~ ~j - Stondord error
[
C~mper~so~ o! S~mc P~p ¢a3 Pressure in eoch Co{egory :
I 0 0 • StatislicaI Signific(/n ce Min Mod. Sev.
NONE p ':01 p (01 p (.0~
O N O N E M I N I M A [ - MOO S E V E R E
DEGREE OF C O L L A T E R A L I Z A T I O N
Fig. 6. Relat ionship between splenic-pulp pressure and degree of collateraiization on splenoportography (54 pa t ients ) . Significant differences between mean SPP in each category of col la teral izat ion--none vs. minimal , modera te ; and severe; severe vs. mini- mal and moderate collateralization are also shown.
TABLE 1. N O R M A L VALUES OF SPLENIC-PULP PRESSURE (SPP) D E T E R M I N E D IN PREVIOUS STUDIES
SPP Authors Year (ram. HsO)
Atkinson and Sherlock ~7 1954 41--231 T u r n e r et al? 1957 108± 54 Leevy et alY 1960 82--136 Zeid et at? ° 1960 <200 Rousselot and BurchelW 1963 <290
200 American Journal of Digestive Diseases
G R E E N E E T A L . : D I A G N O S T I C D I S C R E P A N C I E S
il would appear from our results that esophagogastroscopy is a more re- liable method of demonstrating esophageal varices and determining whether or not they are bleeding.
In the management of patients with nonvariceal upper gastrointestinal bleeding and coexisting elevated splenic-pulp pressures and esophageal varices, the reliance upon a specific level of splenic-pulp pressure as an indicator of the site of bleeding seems untenable. Furthermore, it may lead to errors in case management.
From the present study it is evident that different methods of demon- strating portal hypertension and collateral circulation may give varying results. While splenoportography has an established place in defining the patency of the portal vein and demonstrating large spontaneous or sur- gical portosystemic shunts, v-x0 esophagogastroscopy is a better method for detecting esophageal varices. I t is also of greater value in determining the site of upper gastrointestinal bleeding, whether variceal or nonvari- teal.
The height of the splenic pulp pressure was of little value in predicting the size of esophageal varices or whether they were bleeding.
SUMMARY AND CONCLUSION
Esophagogastroscopy, splenic-pulp manometry, and splenoportography were combined in a prospective study of 60 patients with documented liver disease and suspected portal hypertension. All three procedures were performed on each of the patients within a 6-day period. Twenty patients were actively bleeding at the time of endoscopic examination.
Esophagogastroscopy demonstrated varices in 90% of the patients studied. Sptenoportography, however, demonstrated collateral circula- tion in only 50% of the patients with endoscopically demonstrated varices. In no instance did splenoportography demonstrate collateral cir- culation not previously seen on endoscopy. Splenoportography failed to demonstrate collateral circulation in all patients whose splenic-pulp pres- sure was less than 270 ram. water.
In 20 patients with upper gastrointestinal bleeding, the height of the splenic-puIp pressure was a poor index of the site of bleeding. Eight pa- tients with portal hypertension and esophageal varices were found to be bleeding from nonvariceal sites. Conversely, 5 patients with active bleed- ing from endoscopicalIy demonstrated varices had no collateral circula- tion revealed by splenoportography.
It is evident from this study that splenic-pulp manometry, spleno- portography, and esophagogastroscopy will frequently yield divergent results in the evaluation of portal hypertension and portosystemic col- lateral circulation in patients with liver disease. While splenoportography
New Series, Vol. I0, No. 4, 1965 2 9 ]
NEW YORK MEDICAL COLLEGE ISSUE
m a y be u s e f u l i n d e t e r m i n i n g t h e p a t e n c y of t h e p o r t a l v e i n a n d d e m o n -
s t r a t i n g l a rge s p o n t a n e o u s o r su rg ica l p o r t o s y s t e m i c shun t s , e s o p h a g o -
ga s t ro scopy is a b e t t e r m e t h o d fo r d e t e c t i n g e s o p h a g e a l var ices a n d de te r -
m i n i n g w h e t h e r t h e y a re b l e e d i n g . T h e h e i g h t of t h e s p l e n i c - p u l p pres-
su re is of l i t t l e v a l u e i n i n d i c a t i n g the s i te o f u p p e r g a s t r o i n t e s t i n a l
b l e e d i n g .
New York Medical College Fifth Ave. 6" 106th St,
New York, N. Y.
R E F E R E N C E S
1. DE CASTRO SILVA, L., Gor~i, F., SCHMIDT, L., and SAO TreAt, O, J. B. EIiicacy of esophagography, esophagoscopy, and splenoportal venography in the diagnosis of esophageal varices. Rev. paulista reed. 64:10, 1964.
2. JACKSON, F. C. "Directional" flow patterns in portal hypertension. Arch. Surg. 87:307, 1963.
3. PALM~, E. D. On the natural history of esophageal varices which are secondary to portal cirrhosis. Ann. Int. Med. 47:18, 1957.
4. BENNETt, H. D., LORrNTCEN, C., and BAUER, C. A. Transient esophageal varices in hepatic cirrhosis. Arch. Int. Med. 92:507, 1953.
5. PALMER, E. D. The problem of unexplainable esophageal varices. South. M. J. 56: 1317, 1963.
6. EVANS, K. T. Oesophageal and gastric varices. Brit. J. Radiol. 32:233, 1959. 7. LEEVY, C. M., CHEggICK, G. R., and DAWDSON, C. S. Portal hypertension. New Eng-
land J. Med. 262:397, 1960. 8. PANKE, W. F., MOm~NO, A. H., and ROUSSELOT, L. M. The diagnostic study of the
portal venous system. Med. Clinics North America 44:727, 1960. 9. TURNER, M. D., SHERLOCK, S., and STEINER, R. E. Splenic venography and intra-
splenic pressure measurement in the clinical investigation of the portal venous system. Am. J. Med. 23:846, 1957.
10. ZEID, S. S., FELSON, B., and SCruFF, L Percutaneous spleuoportat venography with additional comments on transhepatic venography. Ann. Int. Med. 52:782, 1960.
11. CASaXO, M. R. The value of splenic pulp manometry and splenoportography in the diagnosis of bleeding esophageal varices. Acta medica phill ipina 19:91, 1962.
12. DOPPMAN, J. L., and SHAPIRO, R. L. Bleeding esophageal varices in presence of a normal splenoportogram. Am. ]. Roentgenol. 86:1103, 1961.
13. SCHAEVER, J., BRAUSCHIREIBER, J., MISTILIS, S., and SCHIF~', L Gastroesophageal variceal bleeding in the absence of hepatic cirrhosis or portal hypertension. Gastro- enterology 46:583, 1964.
14. BERGSTRAND, I., and •KMAN, C. A. Percutaneous lieno portal venography. Acta radiol. 47:269, 1957.
15. BERCSTRAND, L, and EKMAN, C. A. Portal circulation in portal hypertension. Acta radiol. 47:1, 1957.
16. PALMER, E. D. On the correlation between portal venous pressure and the size and extent of esophageal varices in portal cirrhosis. Ann. Surg. 138:741, 1953.
17. ATKINSON, M., and SHERLOCK, S. Intrasplenic pressure as an index of portal pres- sure. Lancet t:1325, 1954.
18. ROUSSELOT, L. M., and BURCHELL, A. R. "Portal Venography and Manometry." In Diseases of the Liver. L. Schiff, Ed. 2nd. ed., pp. 284-328. Lippincott, Philadelphia, 1963.
19. KATZ, D., DOUVRES, P., WEISBERG, H., CHARM, R., and McKINNON, W. Sources of bleeding in upper gastrointestinal hemorrhage: A re-evaluation. Am. J. Digest. Dis. 9:447, 1964.
292 American Journal of Diges¢ive Diseases