
Evaluation framework to assess benefits and harms of...
70
Evaluation framework to assess benefits and harms of bone-anchored prosthesis 2015. 6th International Conference Advances in Orthopaedic Osseointegration Page 1 of 4 Evaluation framework to assess benefits and harms of bone-anchored prosthesis Frossard Laurent Queensland University of Technology, Brisbane, QLD, Australia University of the Sunshine Coast, Maroochydore, QLD, Australia Frossard L. Evaluation framework to assess benefits and harms of bone-anchored prosthesis. 6th International Conference Advances in Orthopaedic Osseointegration. 2015. Las Vegas, Nevada, USA. p 2 Introduction Bone-anchored prostheses are increasingly acknowledged as viable alternative method of attachment of artificial limb compared to socket-suspended prostheses. To date, a few osseointegration fixations are commercially available. Several devices are at different stages of development particularly in Europe and the US. [1-15] Clearly, the current momentum experienced worldwide is creating a need for a standardized evaluation framework to assess the benefits and safety of each procedure. Methods The proposed evaluation framework was extracted from a systematic review of the literature including seminal studies focusing on clinical benefits and safety of procedures involving screw-type implant (e.g., OPRA) and press-fit fixations (e.g., EEFT, ILP, OPL). [16-25] Results The literature review highlighted that a standard and replicable evaluation framework should focus on: The clinical benefits with a systematic recording of health- related quality of life (SF-26, Q- TFA), mobility predictor (e.g., AMPRO), ambulation abilities (TUG, 6MWT), walking abilities (e.g., characteristic spatio-temporal) and actual activity level at baseline and follow-up post Stage 2 surgery, The potential harms with systematic recording of residuum care, infection, implant stability, implant integrity, injuries (e.g., falls) after Stage 1 surgery. Discussion There was a general consensus around the instruments to monitor most of the benefits and harms. The benefits could be assessed using a wide spectrum of complementary assessments ranging from subjective patient self-reporting to objective measurements of physical activity. However, this latter was assessed using a broad range of measurements (e.g., pedometer, load cell, energy consumption). More importantly, the lack of consistent grading of infections was sufficiently noticeable to impede cross- fixation comparisons. Clearly, a more universal grading system is needed. In the meanwhile, investigators are encouraged to implement an evaluation framework featuring the domains and instruments proposed above using a single database to facilitate robust prospective studies about potential benefits and harms of their procedure. References 1. Kang, N.V., D. Morritt, C. Pendegrass, and G. Blunn, Use of
Transcript of Evaluation framework to assess benefits and harms of...

Evaluation framework to assess benefits and harms of bone-anchored prosthesis
2015. 6th International Conference Advances in Orthopaedic Osseointegration Page 1 of 4
Evaluation framework to assess benefits and harms of bone-anchored
prosthesis
Frossard Laurent
Queensland University of Technology, Brisbane, QLD, Australia
University of the Sunshine Coast, Maroochydore, QLD, Australia
Frossard L. Evaluation framework to assess benefits and harms of bone-anchored
prosthesis. 6th International Conference Advances in Orthopaedic Osseointegration. 2015.
Las Vegas, Nevada, USA. p 2
Introduction
Bone-anchored prostheses are increasingly
acknowledged as viable alternative method
of attachment of artificial limb compared to
socket-suspended prostheses. To date, a few
osseointegration fixations are commercially
available. Several devices are at different
stages of development particularly in Europe
and the US. [1-15]
Clearly, the current
momentum experienced worldwide is
creating a need for a standardized evaluation
framework to assess the benefits and safety
of each procedure.
Methods
The proposed evaluation framework
was extracted from a systematic review of
the literature including seminal studies
focusing on clinical benefits and safety of
procedures involving screw-type implant
(e.g., OPRA) and press-fit fixations (e.g.,
EEFT, ILP, OPL). [16-25]
Results
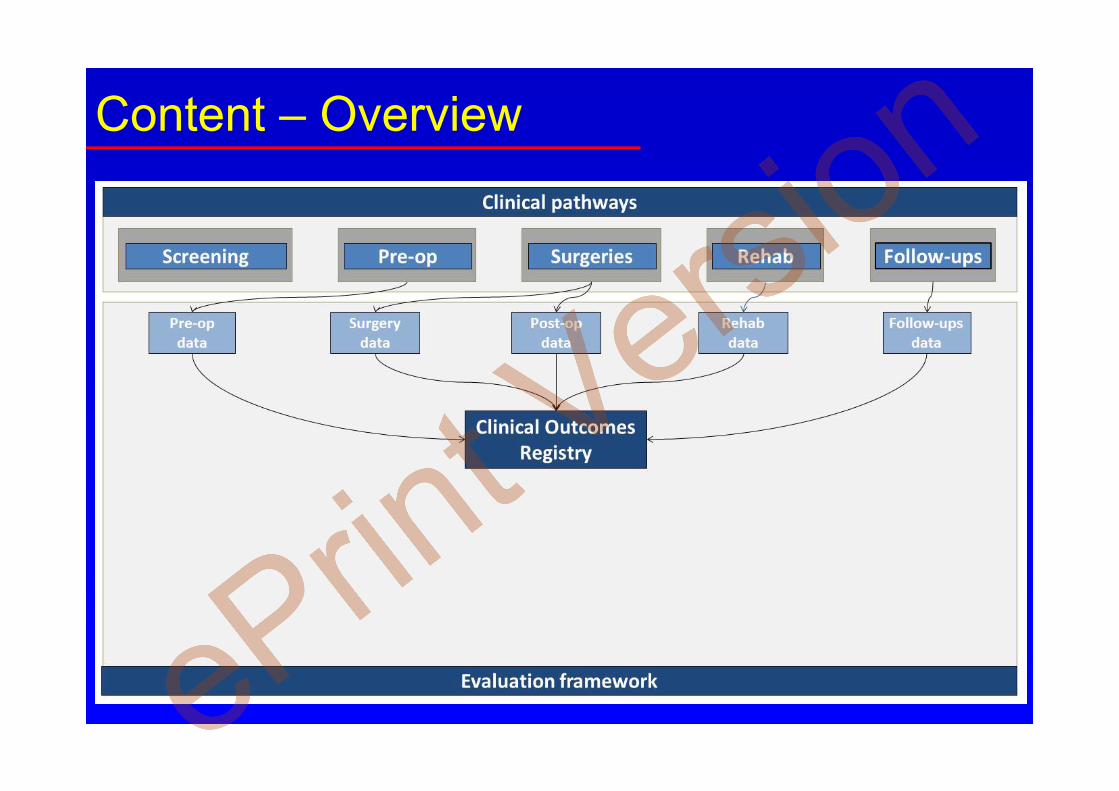
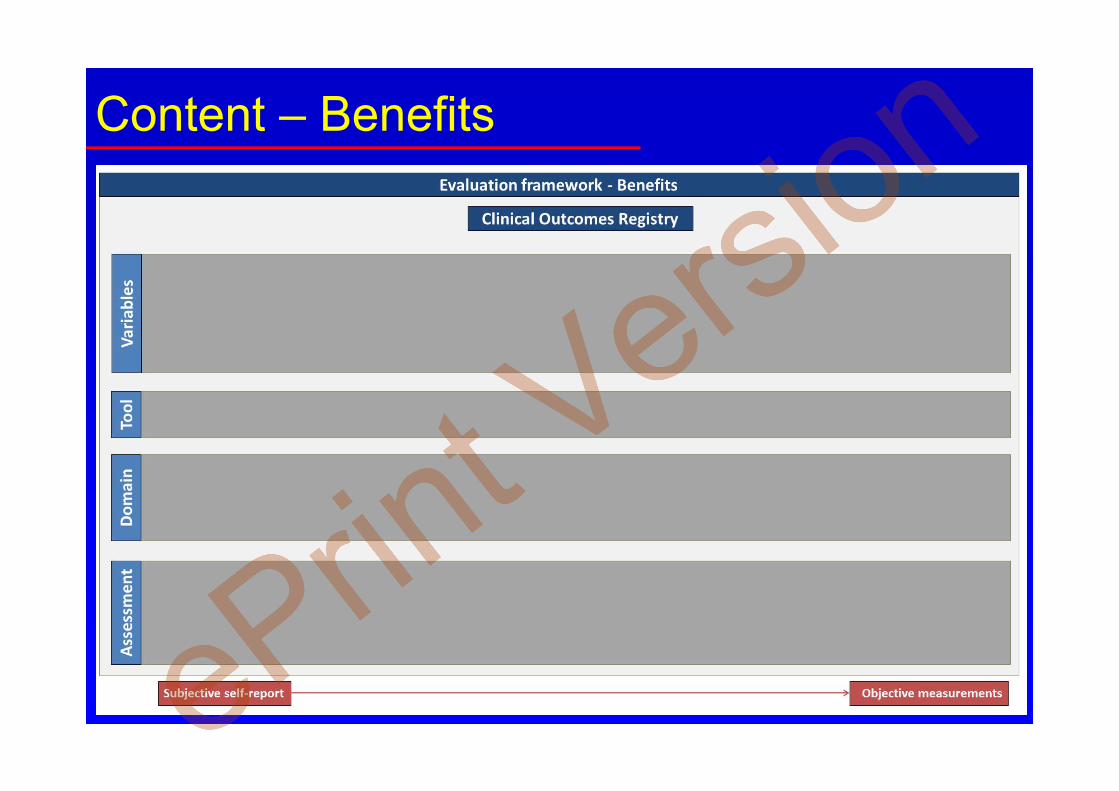
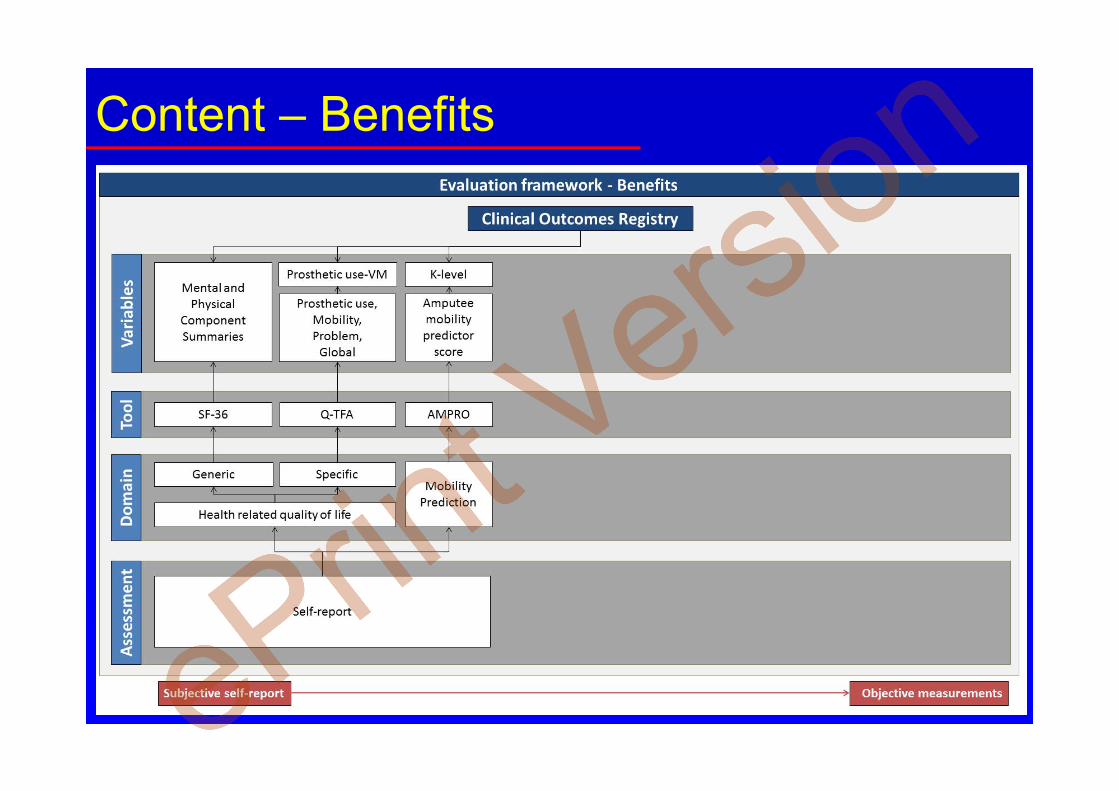
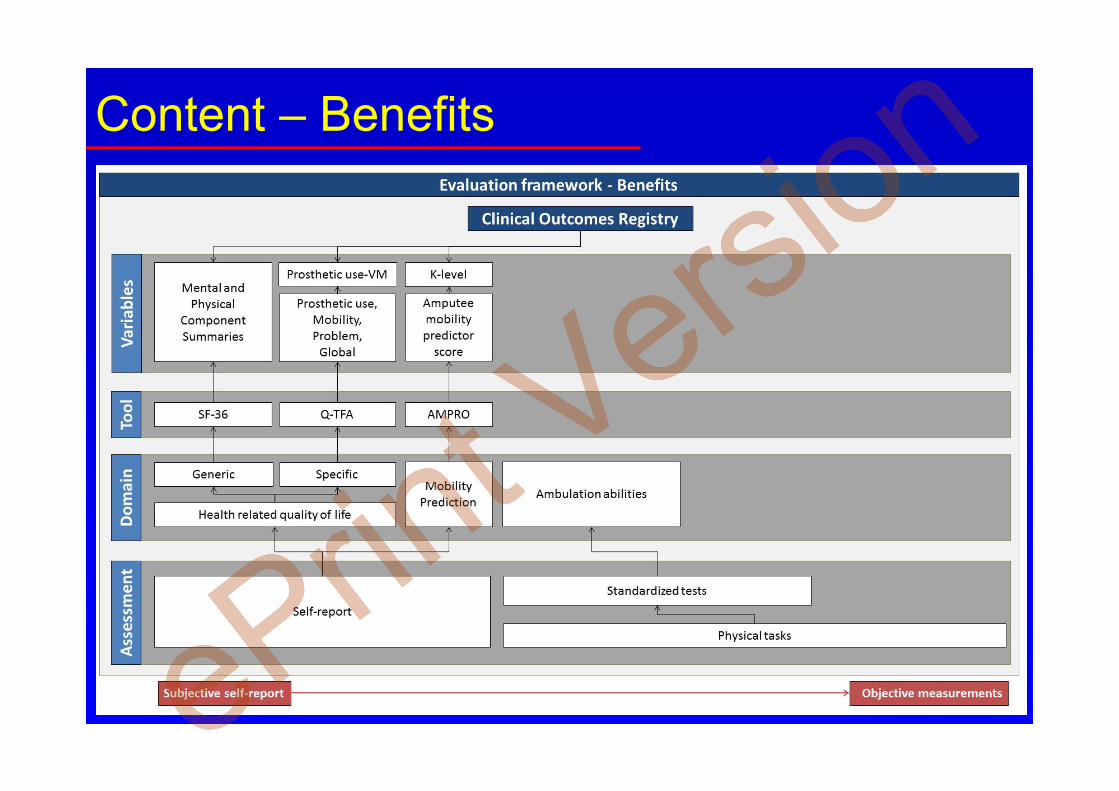
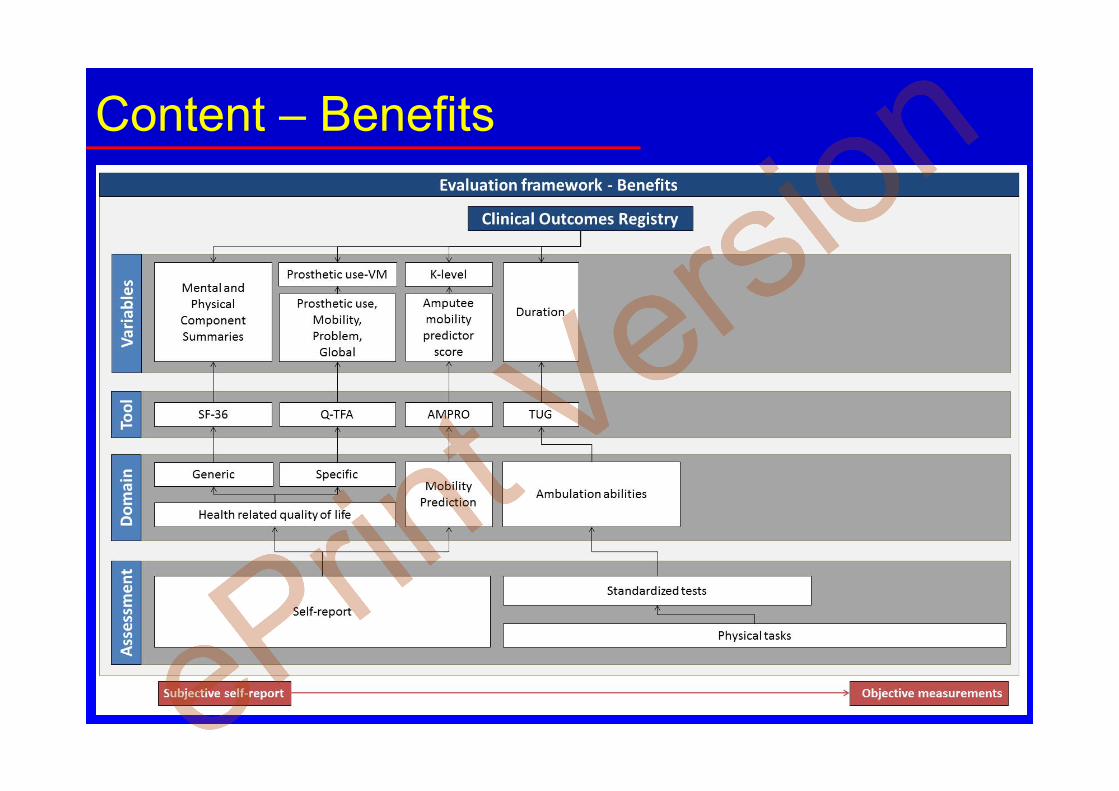
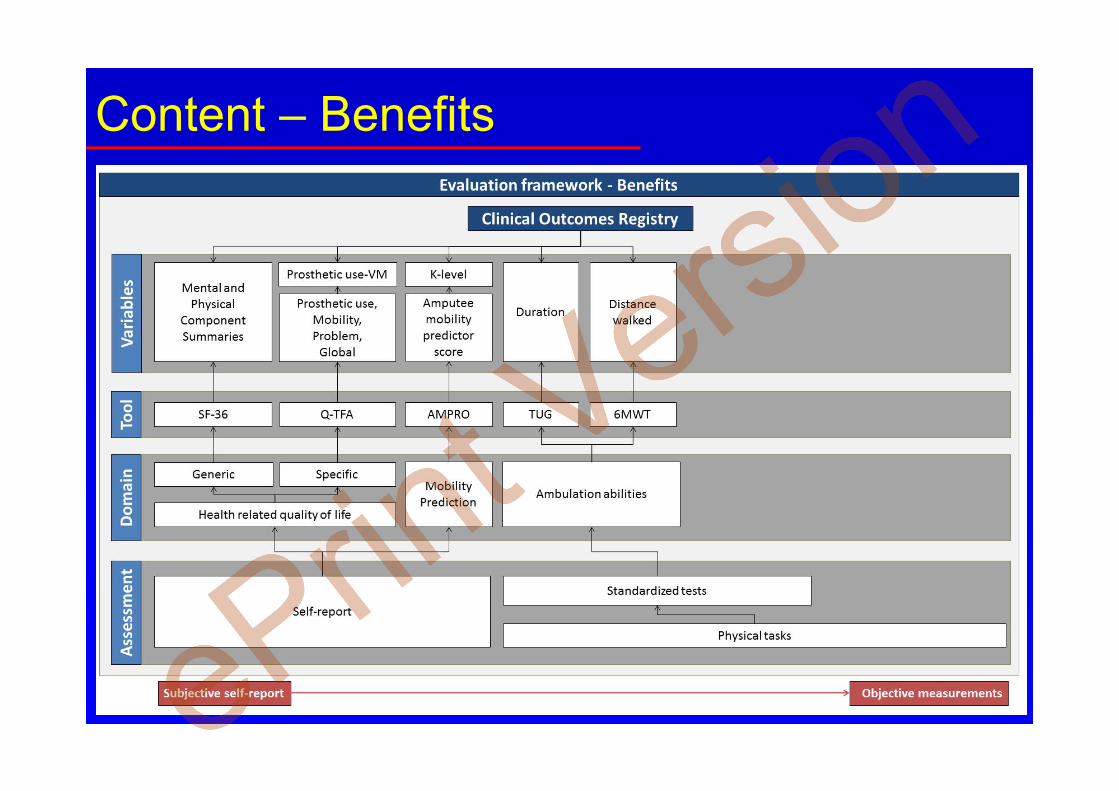
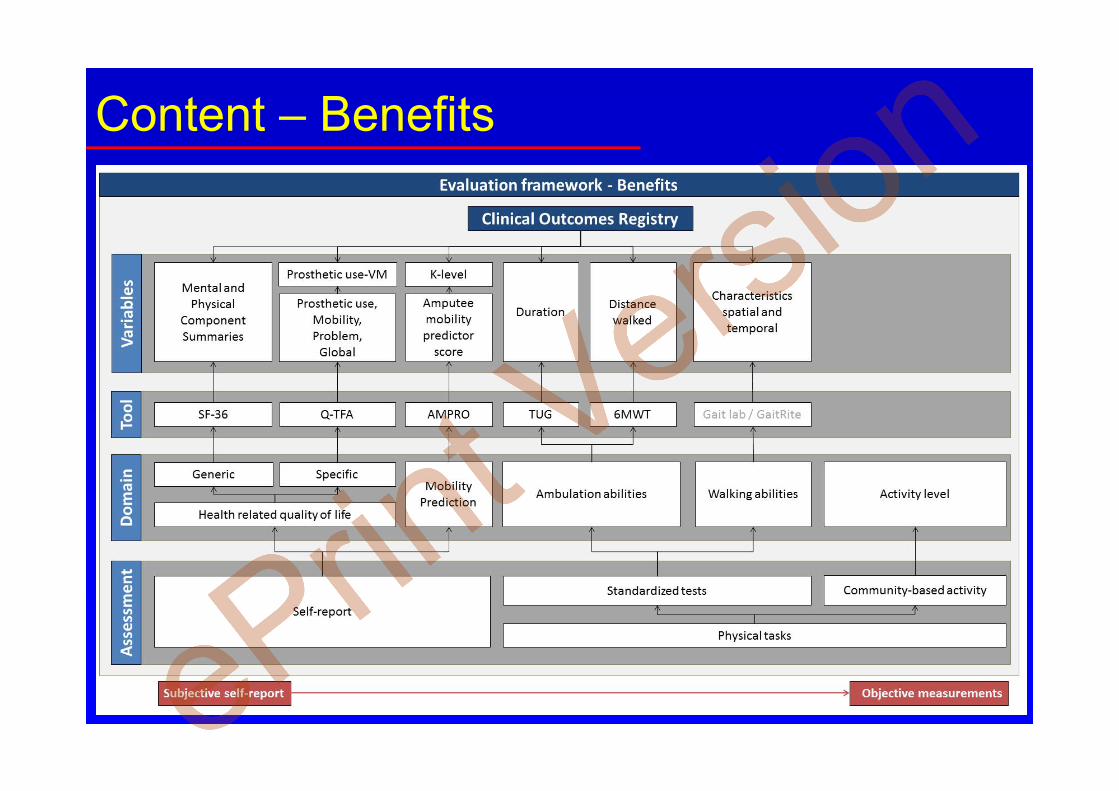
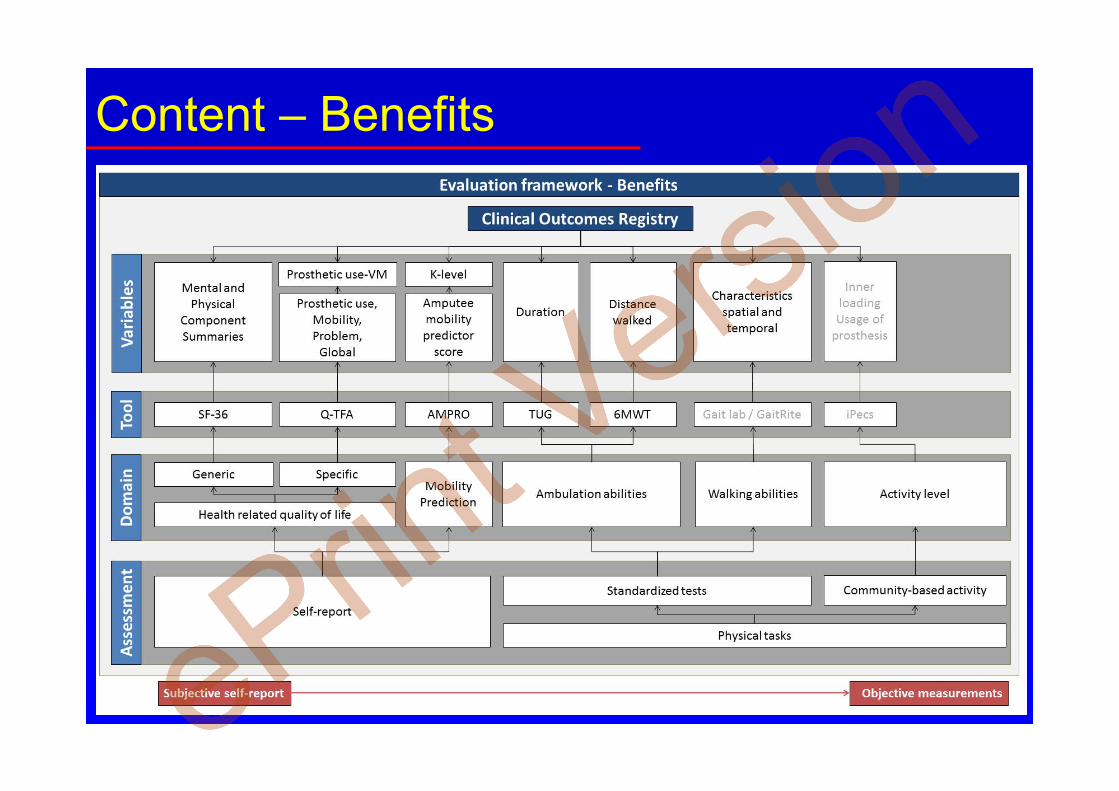
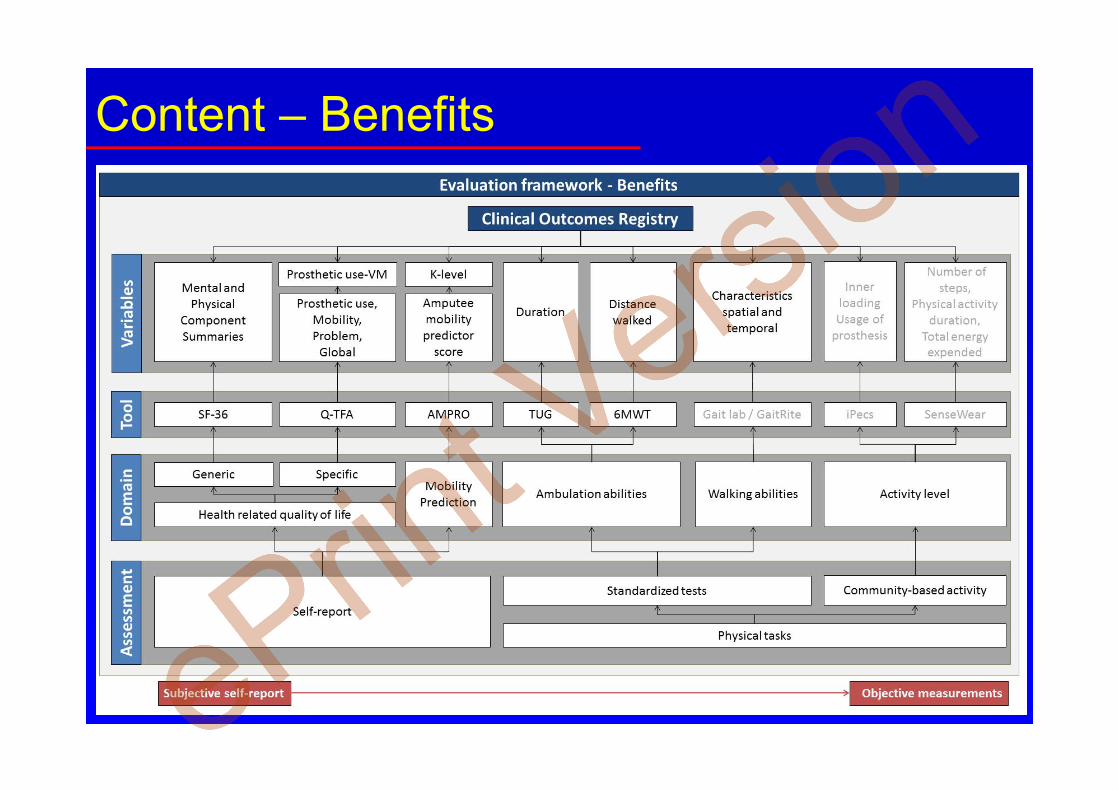
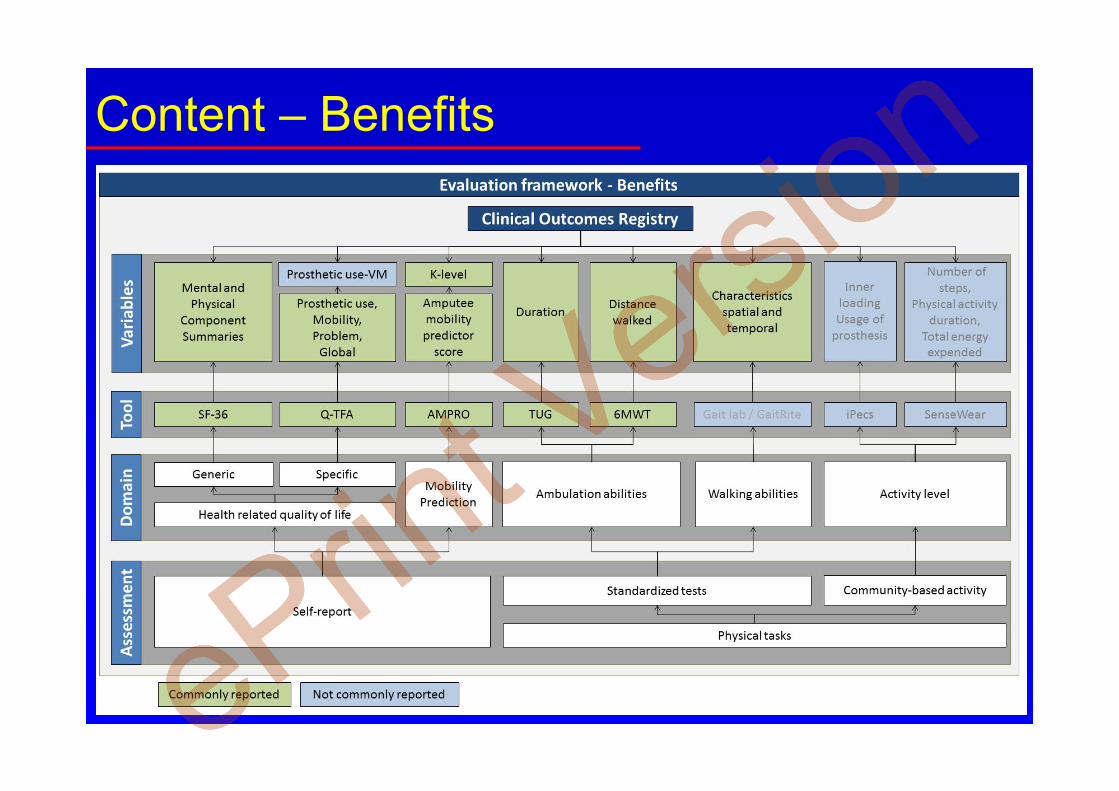
The literature review highlighted that a
standard and replicable evaluation
framework should focus on:
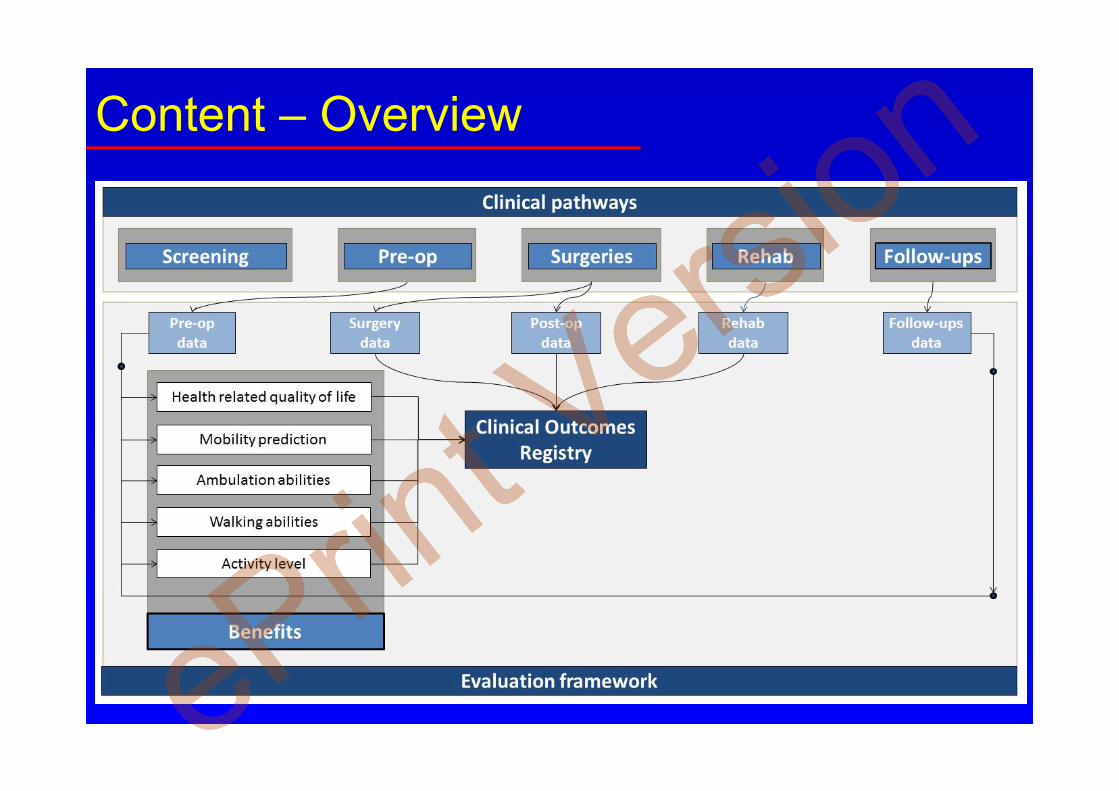
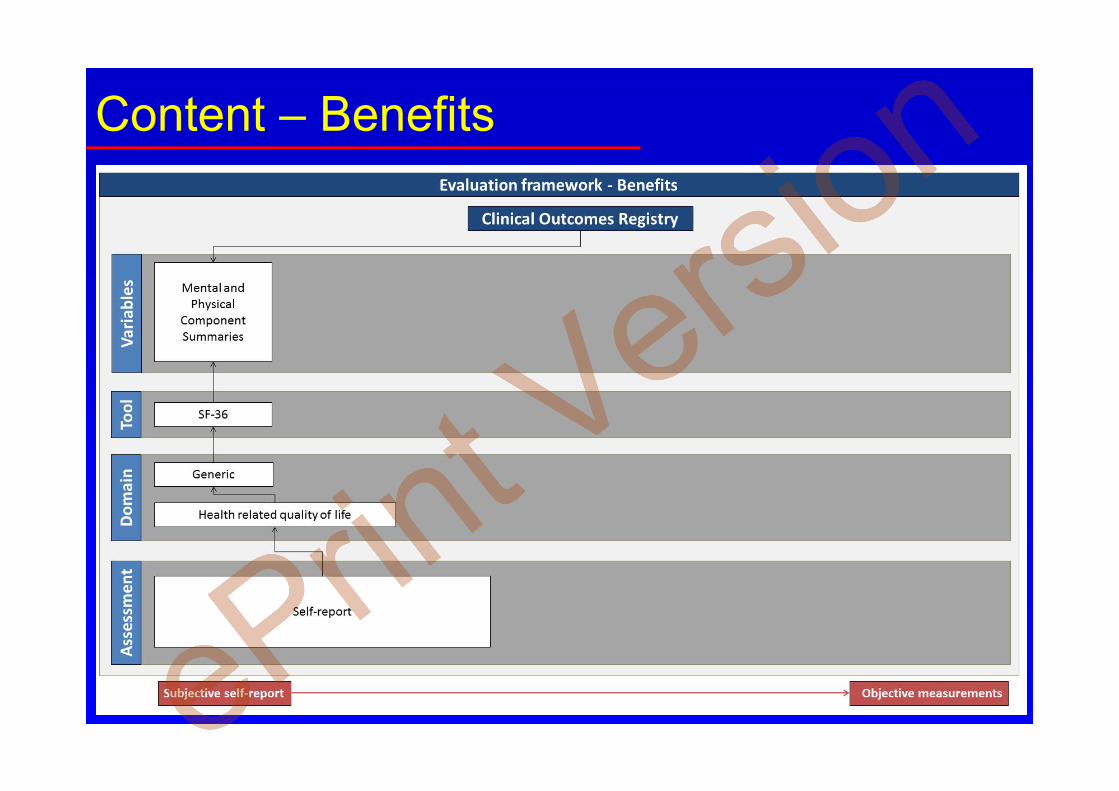
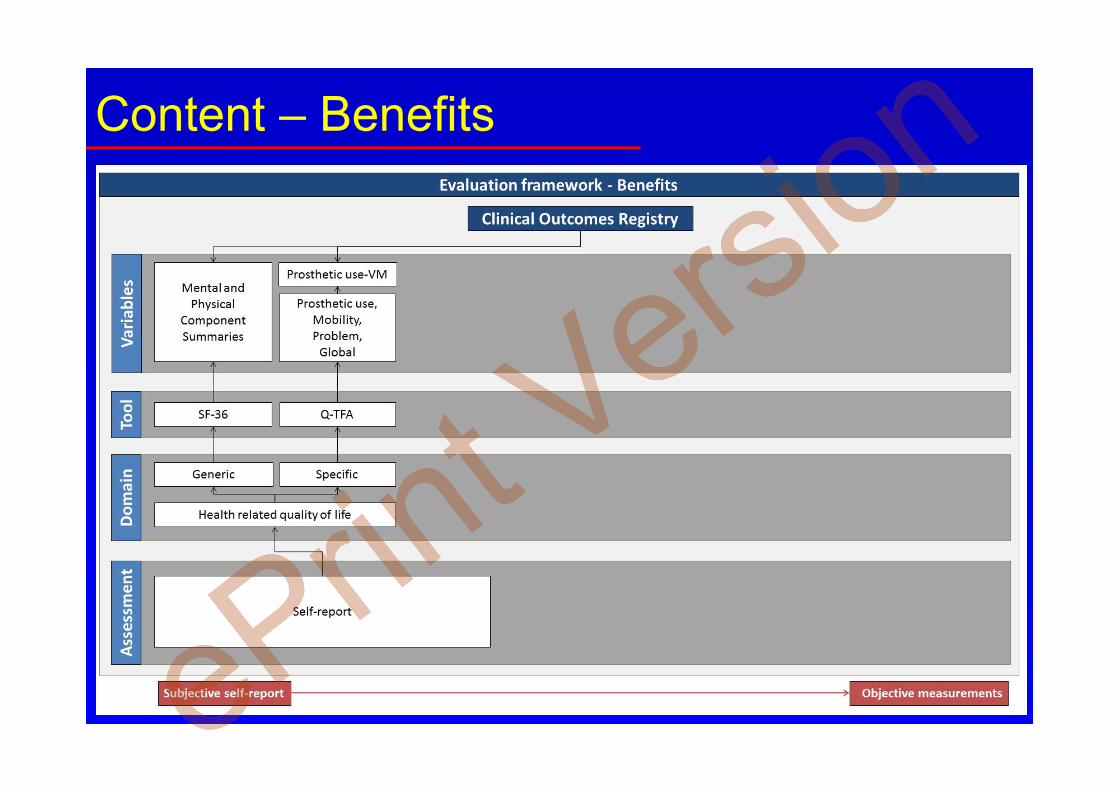
The clinical benefits with a
systematic recording of health-
related quality of life (SF-26, Q-
TFA), mobility predictor (e.g.,
AMPRO), ambulation abilities
(TUG, 6MWT), walking abilities
(e.g., characteristic spatio-temporal)
and actual activity level at baseline
and follow-up post Stage 2 surgery,
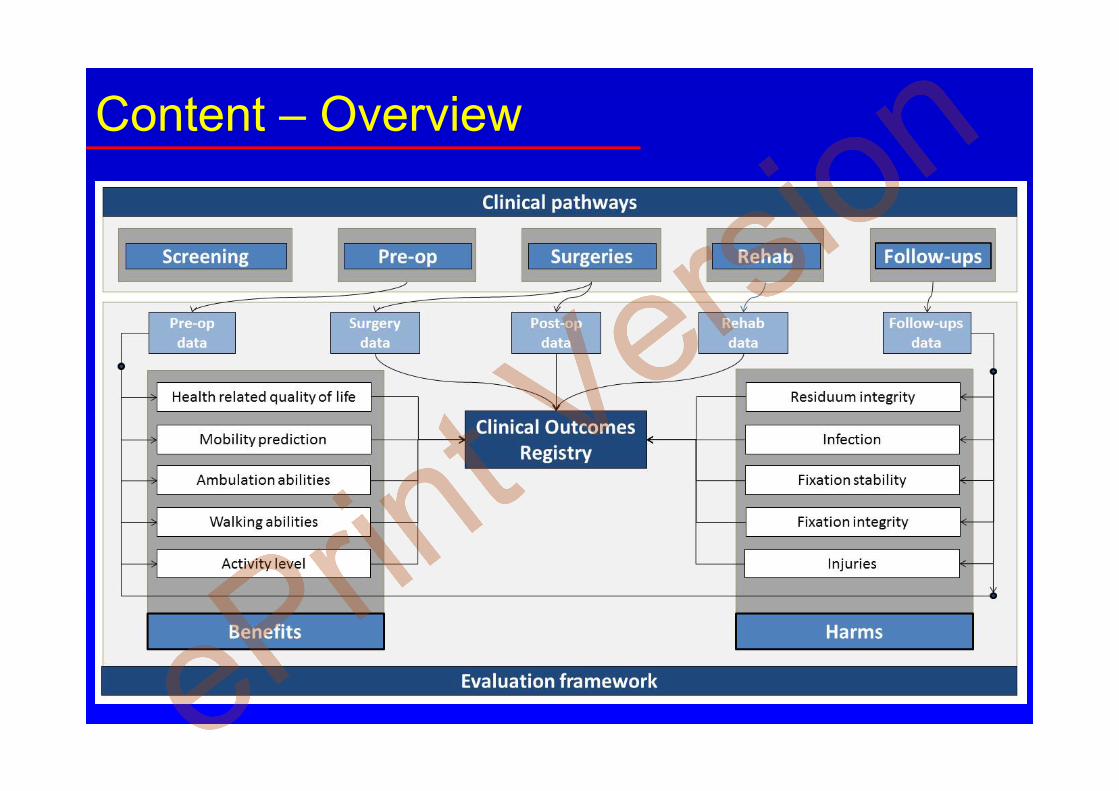
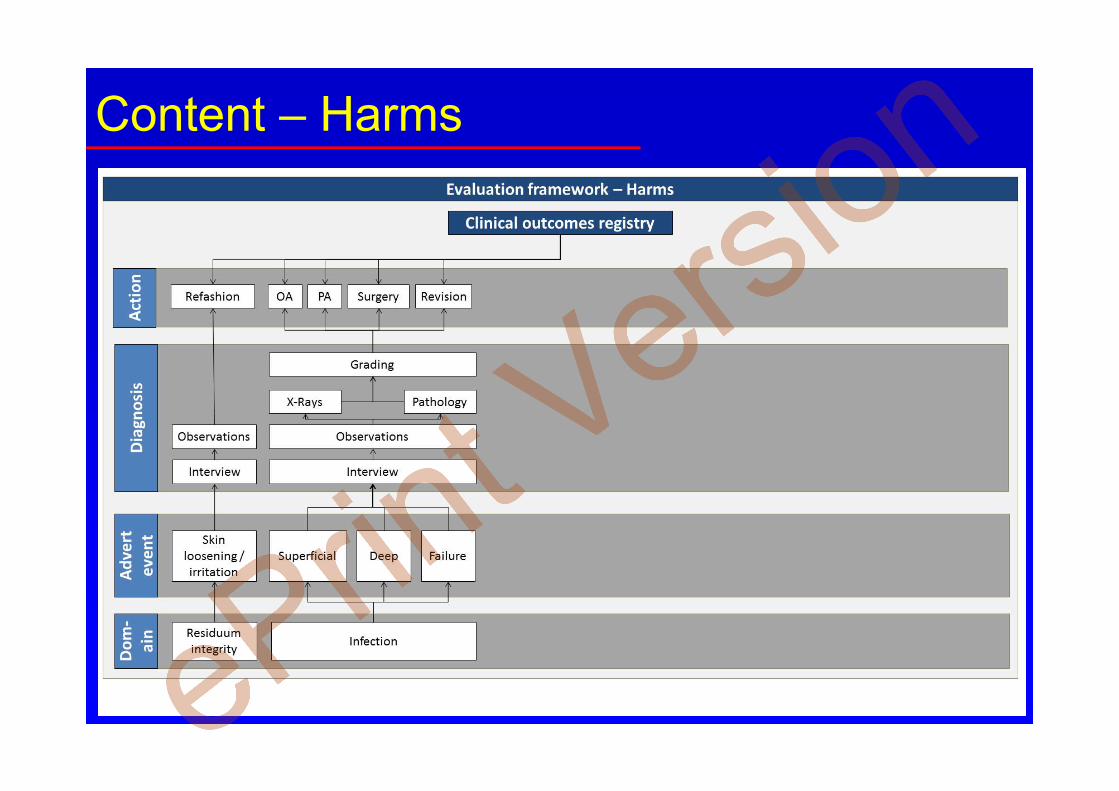
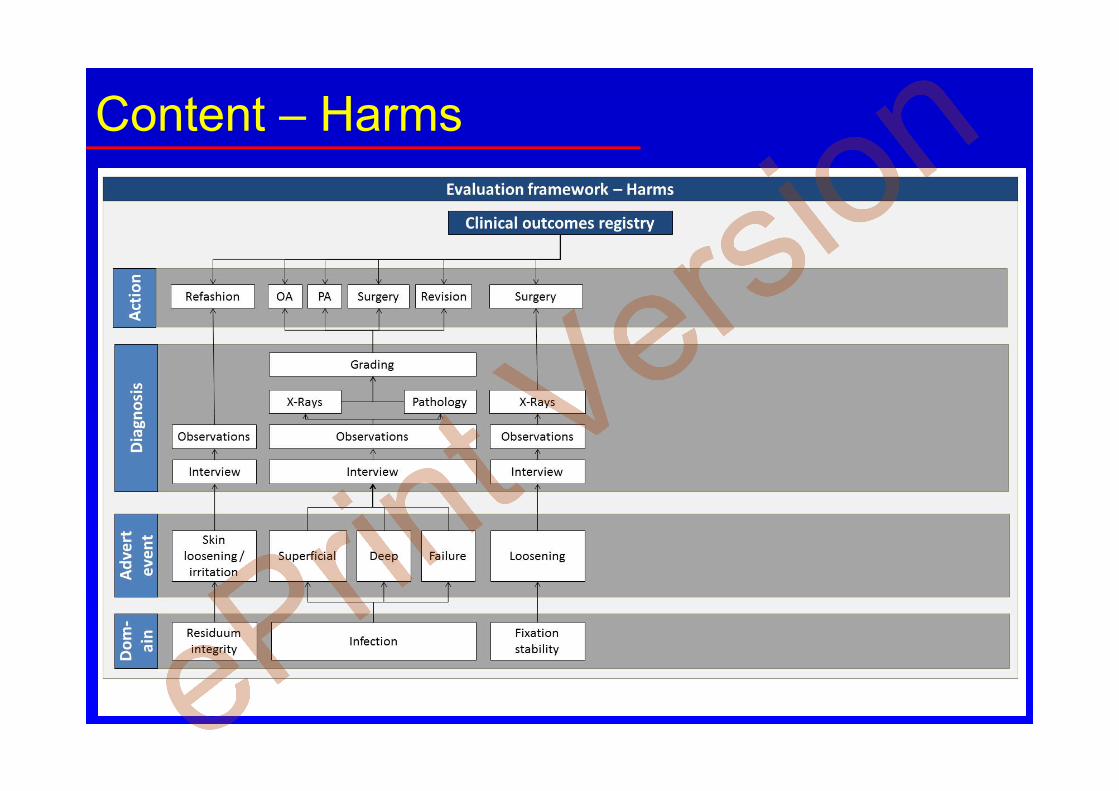
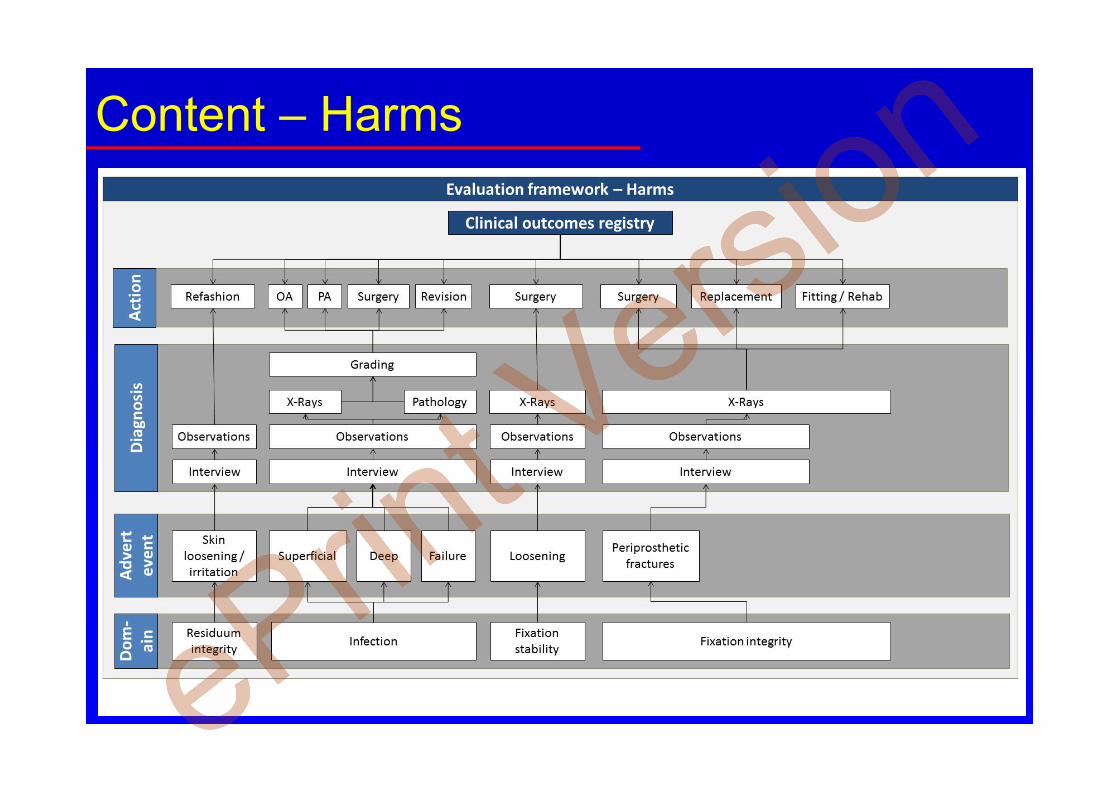
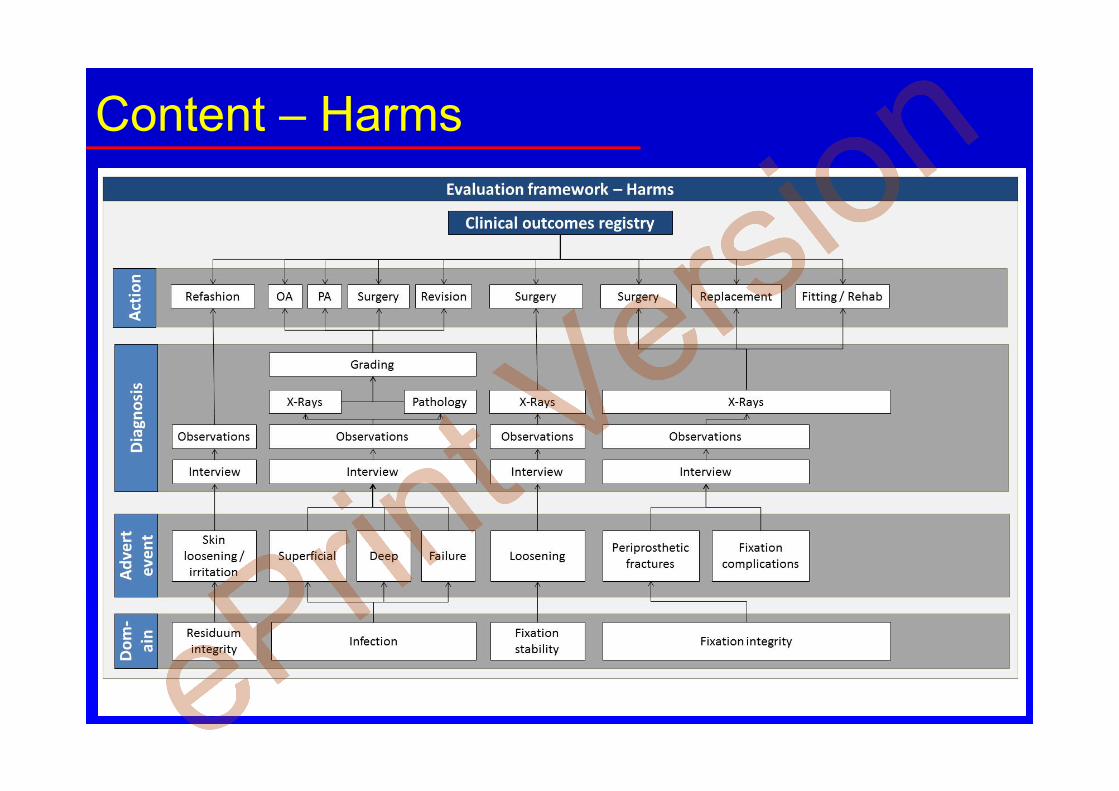
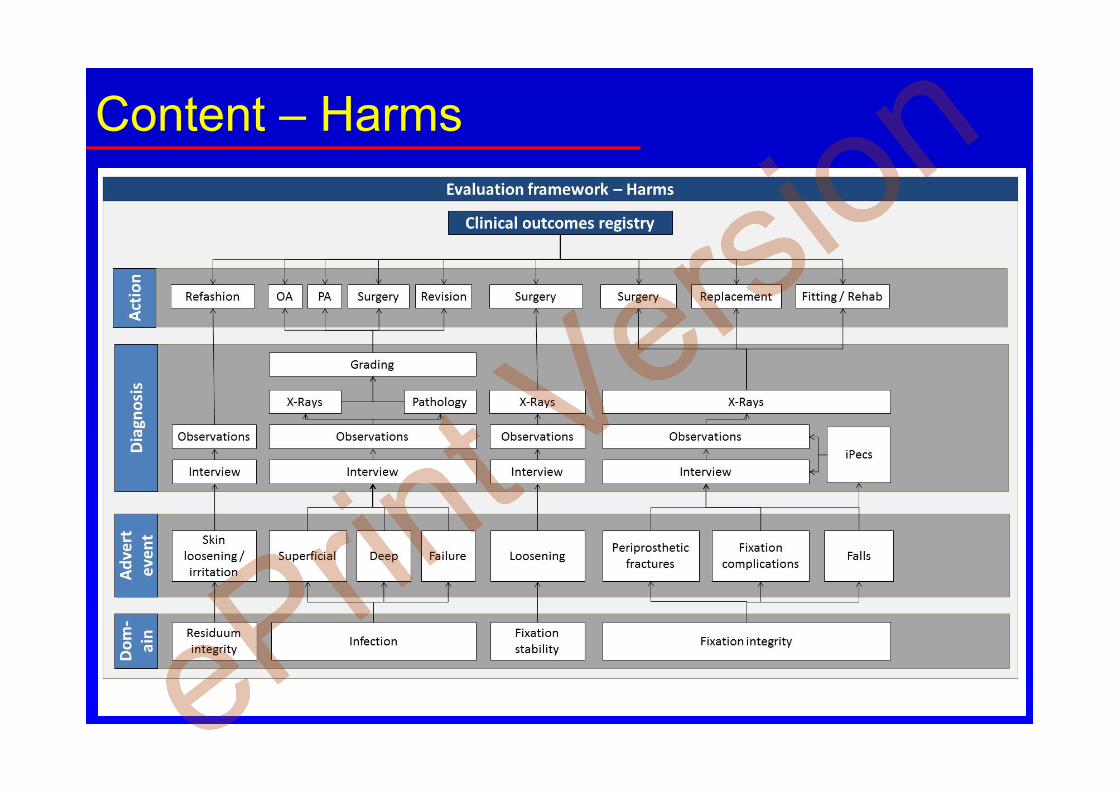
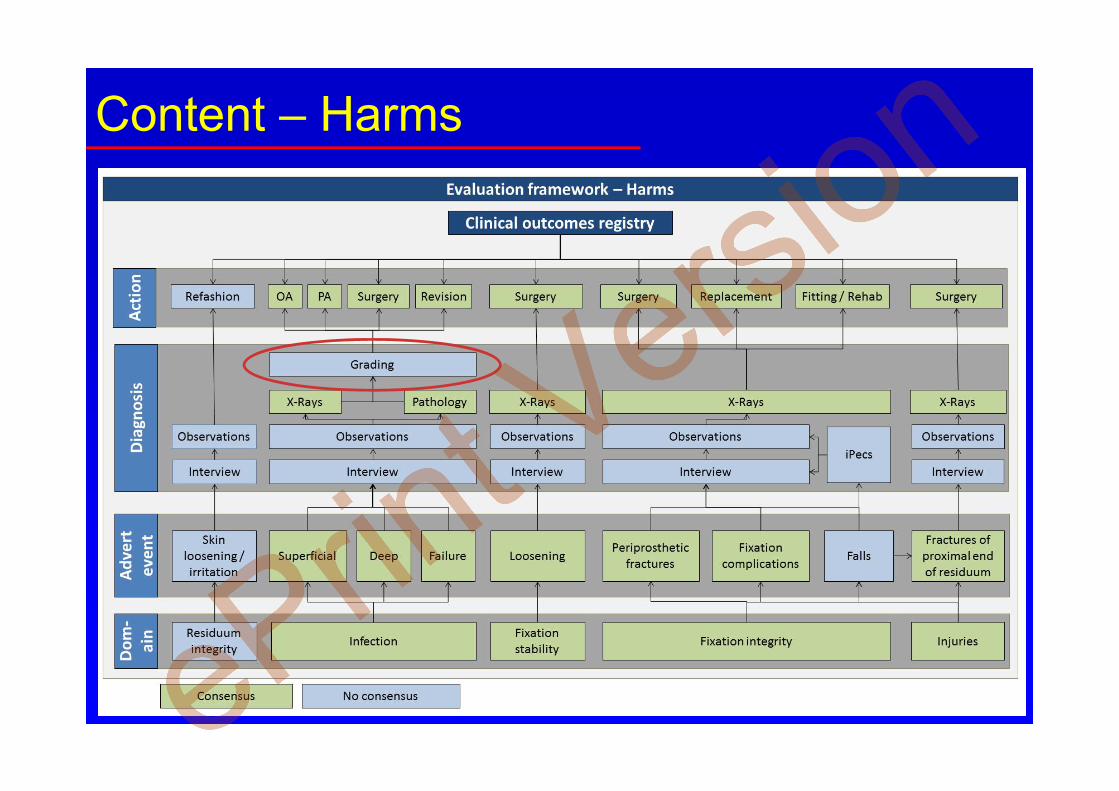
The potential harms with systematic
recording of residuum care,
infection, implant stability, implant
integrity, injuries (e.g., falls) after
Stage 1 surgery.
Discussion
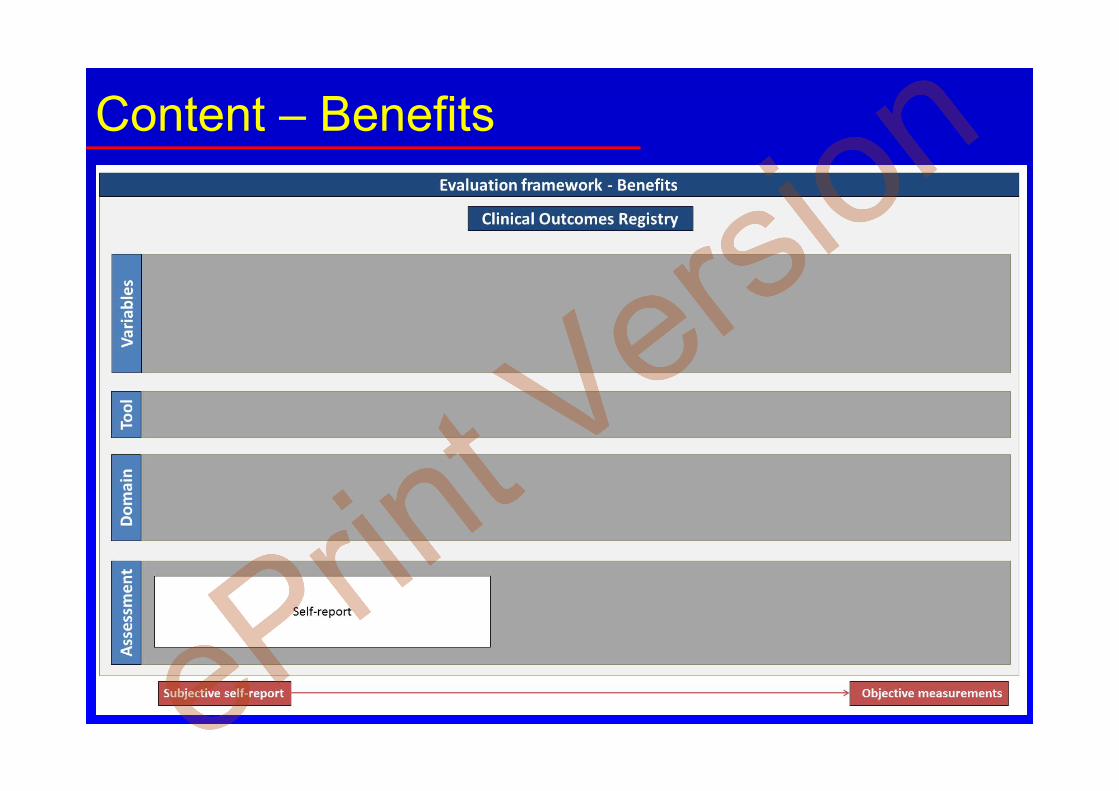
There was a general consensus around the
instruments to monitor most of the benefits
and harms. The benefits could be assessed
using a wide spectrum of complementary
assessments ranging from subjective patient
self-reporting to objective measurements of
physical activity. However, this latter was
assessed using a broad range of
measurements (e.g., pedometer, load cell,
energy consumption). More importantly, the
lack of consistent grading of infections was
sufficiently noticeable to impede cross-
fixation comparisons. Clearly, a more
universal grading system is needed. In the
meanwhile, investigators are encouraged to
implement an evaluation framework
featuring the domains and instruments
proposed above using a single database to
facilitate robust prospective studies about
potential benefits and harms of their
procedure.
References
1. Kang, N.V., D. Morritt, C.
Pendegrass, and G. Blunn, Use of

Evaluation framework to assess benefits and harms of bone-anchored prosthesis
2015. 6th International Conference Advances in Orthopaedic Osseointegration Page 2 of 4
ITAP implants for prosthetic
reconstruction of extra-oral
craniofacial defects. J Plast Reconstr
Aesthet Surg, 2013. 66(4): p. 497-
505.
2. Kang, N.V., C. Pendegrass, L.
Marks, and G. Blunn,
Osseocutaneous integration of an
intraosseous transcutaneous
amputation prosthesis implant used
for reconstruction of a transhumeral
amputee: Case report. The Journal of
Hand Surgery, 2010. 35(7): p. 1130-
1134.
3. Pendegrass, C., C. Fontaine, and G.
Blunn, Intraosseous transcutaneous
amputation prostheses vs dental
implants: a comparison between
keratinocyte and gingival epithelial
cell adhesion in vitro. Journal of
Bone & Joint Surgery, British
Volume, 2012. 94-B(SUPP
XXXVI): p. 10.
4. Aschoff, H.H., R.E. Kennon, J.M.
Keggi, and L.E. Rubin,
Transcutaneous, distal femoral,
intramedullary attachment for above-
the-knee prostheses: an endo-exo
device. J Bone Joint Surg Am, 2010.
92 Suppl 2(Supplement 2): p. 180-6.
5. Aschoff, H.-H. and R. McGough,
The Endo-Exo Femoral Prosthesis: a
new rehabilitation concept following
above knee amputation. Journal of
Bone & Joint Surgery, British
Volume, 2012. 94-B(SUPP
XXXIX): p. 77.
6. Hillock, R., J. Keggi, R. Kennon, E.
McPherson, T. Clyburn, D. Brazil,
and T. McTighe, A Global
Collaboration - Osteointegration
Implant (OI) for Transfemoral
Amputation - Case Report.
Reconstructive review - Joint
Implant Surgery & Research
Foundation, 2013. 3(2): p. 50-54.
7. Rubin, L., L. Kennon, J. Keggi, and
H. Aschoff, Surgical management
of trans-femoral amputation with a
transcutaneous, press-fit distal
femoral intra-medullary device:
analysis with minimum 2 year
follow-up. Journal of Bone & Joint
Surgery, British Volume, 2012. 94-
B(SUPP XXI): p. 95.
8. Van de Meent, H., M.T. Hopman,
and J.P. Frolke, Walking ability and
quality of life in subjects with
transfemoral amputation: a
comparison of osseointegration with
socket prostheses. Arch Phys Med
Rehabil, 2013. 94(11): p. 2174-2178.
9. Tomaszewski, P.K., B. Lasnier, G.
Hannink, G.J. Verkerke, and N.
Verdonschot, Experimental
assessment of a new direct fixation
implant for artificial limbs. J Mech
Behav Biomed Mater, 2013. 21: p.
77-85.
10. Tomaszewski, P.K., M. van Diest,
S.K. Bulstra, N. Verdonschot, and
G.J. Verkerke, Numerical analysis of
an osseointegrated prosthesis
fixation with reduced bone failure
risk and periprosthetic bone loss. J
Biomech, 2012. 45(11): p. 1875-80.
11. Tomaszewski, P.K., N. Verdonschot,
S.K. Bulstra, J.S. Rietman, and G.J.
Verkerke, Simulated bone
remodeling around two types of
osseointegrated implants for direct
fixation of upper-leg prostheses. J
Mech Behav Biomed Mater, 2012.
15(0): p. 167-75.
12. Tomaszewski, P.K., N. Verdonschot,
S.K. Bulstra, and G.J. Verkerke, A
New Osseointegrated Fixation
Implant for Amputated Patients.
Journal of Biomechanics, 2012.
45(0): p. S322.
13. Jeyapalina, S., J.P. Beck, K.N.
Bachus, O. Chalayon, and R.D.
Bloebaum, Radiographic Evaluation
of Bone Adaptation Adjacent to
Percutaneous Osseointegrated
Evaluation framework to assess benefits and harms of bone-anchored prosthesis
2015. 6th International Conference Advances in Orthopaedic Osseointegration Page 3 of 4
Prostheses in a Sheep Model. Clin
Orthop Relat Res, 2014: p. 1-12.
14. Shelton, T.J., J.P. Beck, R.D.
Bloebaum, and K.N. Bachus,
Percutaneous osseointegrated
prostheses for amputees: Limb
compensation in a 12-month ovine
model. J Biomech, 2011. 44(15): p.
2601-6.
15. Shevtsov, M.A., O.V. Galibin, N.M.
Yudintceva, M.I. Blinova, G.P.
Pinaev, A.A. Ivanova, O.N.
Savchenko, D.N. Suslov, I.L.
Potokin, E. Pitkin, G. Raykhtsaum,
and M.R. Pitkin, Two-stage
implantation of the skin and bone
integrated pylon (SBIP) seeded with
autologous fibroblasts induced into
osteoblast differentiation for direct
skeletal attachment of limb
prostheses. Journal of Biomedical
Materials Research Part A, 2013: p.
n/a-n/a.
16. Frossard, L., D.L. Gow, K. Hagberg,
N. Cairns, B. Contoyannis, S. Gray,
R. Branemark, and M. Pearcy,
Apparatus for monitoring load
bearing rehabilitation exercises of a
transfemoral amputee fitted with an
osseointegrated fixation: a proof-of-
concept study. Gait Posture, 2010.
31(2): p. 223-8.
17. Frossard, L., K. Hagberg, E.
Haggstrom, and R. Branemark,
Load-relief of walking aids on
osseointegrated fixation: instrument
for evidence-based practice. IEEE
Trans Neural Syst Rehabil Eng,
2009. 17(1): p. 9-14.
18. Frossard, L., K. Hagberg, E.
Häggström, D.L. Gow, R.
Brånemark, and M. Pearcy,
Functional Outcome of Transfemoral
Amputees Fitted With an
Osseointegrated Fixation: Temporal
Gait Characteristics. JPO Journal of
Prosthetics and Orthotics, 2010.
22(1): p. 11-20.
19. Frossard, L., N. Stevenson, J.
Smeathers, E. Haggstrom, K.
Hagberg, J. Sullivan, D. Ewins, D.L.
Gow, S. Gray, and R. Branemark,
Monitoring of the load regime
applied on the osseointegrated
fixation of a trans-femoral amputee:
a tool for evidence-based practice.
Prosthet Orthot Int, 2008. 32(1): p.
68-78.
20. Frossard, L., N. Stevenson, J.
Smeathers, D. Lee Gow, S. Gray, J.
Sullivan, C. Daniel, E. Häggström,
K. Hagberg, and R. Brånemark,
Daily activities of a transfemoral
amputee fitted with osseointegrated
fixation: continuous recording of the
loading for an evidence-based
practice. Kinesitherapie Revue,
2006. 6(56-57): p. 53-62.
21. Frossard, L., R. Tranberg, E.
Haggstrom, M. Pearcy, and R.
Branemark, Fall of a transfemoral
amputee fitted with osseointegrated
fixation: loading impact on
residuum. Gait & Posture, 2009.
30(Supplement 2): p. S151-S152.
22. Frossard, L.A., R. Tranberg, E.
Haggstrom, M. Pearcy, and R.
Branemark, Load on osseointegrated
fixation of a transfemoral amputee
during a fall: loading, descent,
impact and recovery analysis.
Prosthet Orthot Int, 2010. 34(1): p.
85-97.
23. Lee, W., L. Frossard, K. Hagberg, E.
Haggstrom, and R. Brånemark,
Kinetics analysis of transfemoral
amputees fitted with osseointegrated
fixation performing common
activities of daily living. Clinical
Biomechanics, 2007. 22(6): p. 665-
673.
24. Lee, W.C., L.A. Frossard, K.
Hagberg, E. Haggstrom, D.L. Gow,
S. Gray, and R. Branemark,
Magnitude and variability of loading
on the osseointegrated implant of
Evaluation framework to assess benefits and harms of bone-anchored prosthesis
2015. 6th International Conference Advances in Orthopaedic Osseointegration Page 4 of 4
transfemoral amputees during
walking. Med Eng Phys, 2008.
30(7): p. 825-833.
25. Vertriest, S., P. Coorevits, K.
Hagberg, R. Branemark, E.
Haggstrom, G. Vanderstraeten, and
L. Frossard, Static Load Bearing
Exercises of Individuals With
Transfemoral Amputation Fitted
With an Osseointegrated Implant:
Reliability of Kinetic Data. IEEE
Trans Neural Syst Rehabil Eng,
2014. In press.
Adj/Prof Laurent Frossard
Las Vegas, Nevada, USA
26/03/2015
Queensland University of Technology, Brisbane, QLD, Australia
University of the Sunshine Coast, Maroochydore, QLD, Australia
Evaluation framework to assess benefits and harms of bone-anchored
prosthesis
www.LaurentFrossard.com
6th International Conference Advances in Orthopaedic Osseointegration

Background
What is an evaluation framework?• Toolbox including a set of instruments to monitor the treatment and to assess the benefits and harms of bone-anchored prosthesis

• Reflective and evidence-based practice• Speed-up publications• Facilitate approvals (FDA, ISO norm)• Convince decision-makers
Background
Why an evaluation framework is needed?• Quick access to critical data• Systematic way to report progresses
Background
How to design an evaluation framework?• Purpose 1: The content
• Choice of evaluation domains• Choice of instruments
• Purpose 2: The structure • Choice of technical platform
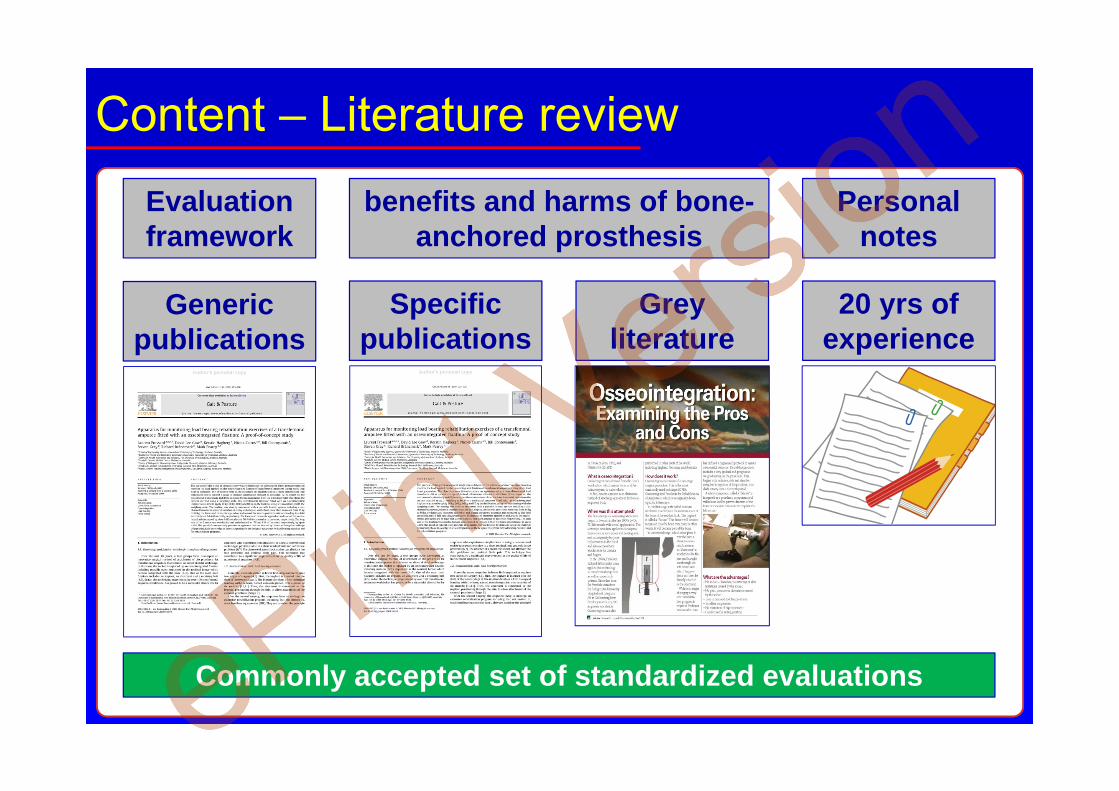
Content – Literature review
benefits and harms of bone-anchored prosthesis
Grey literature
Specific publications
20 yrs of experience
Generic publications
Evaluation framework
Commonly accepted set of standardized evaluations
Personal notes
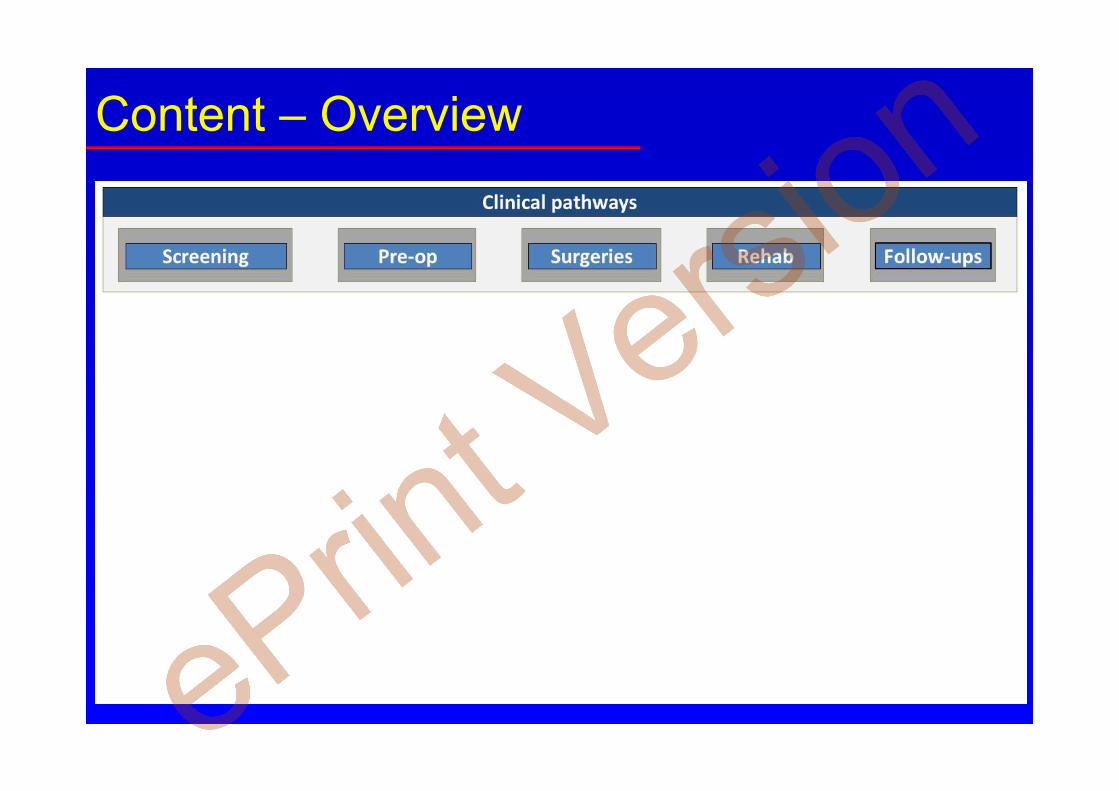
Content – Overview
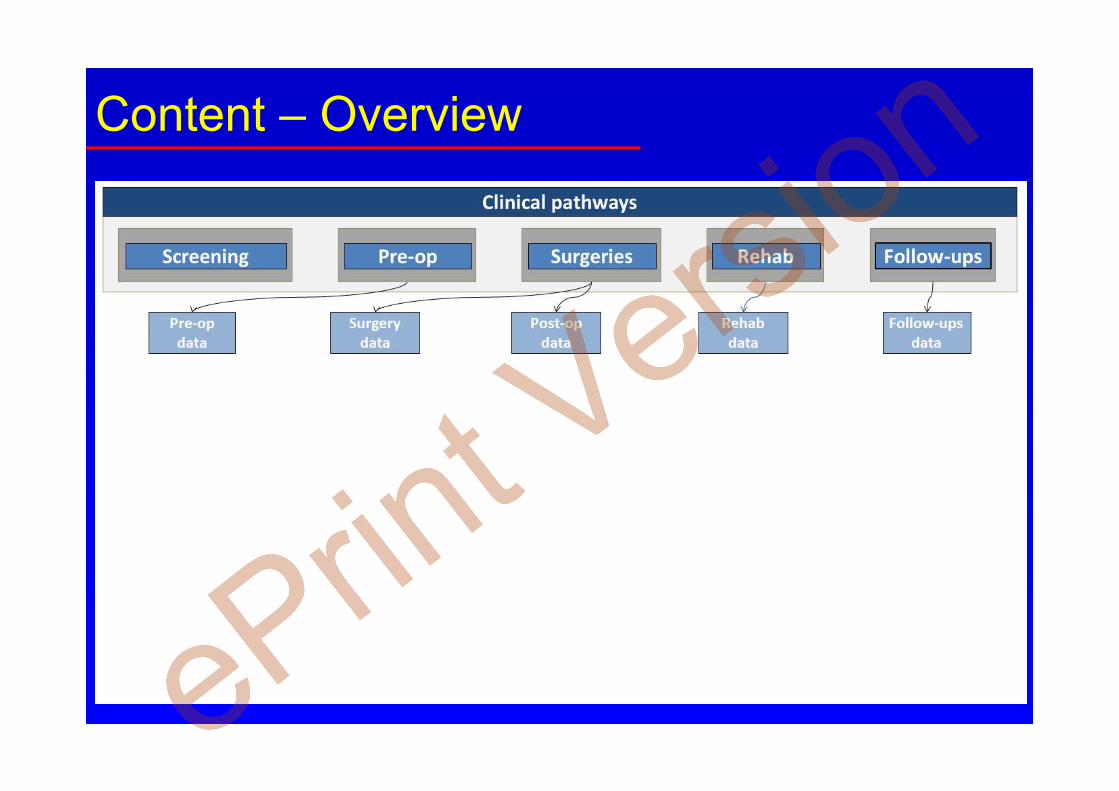
Content – Overview
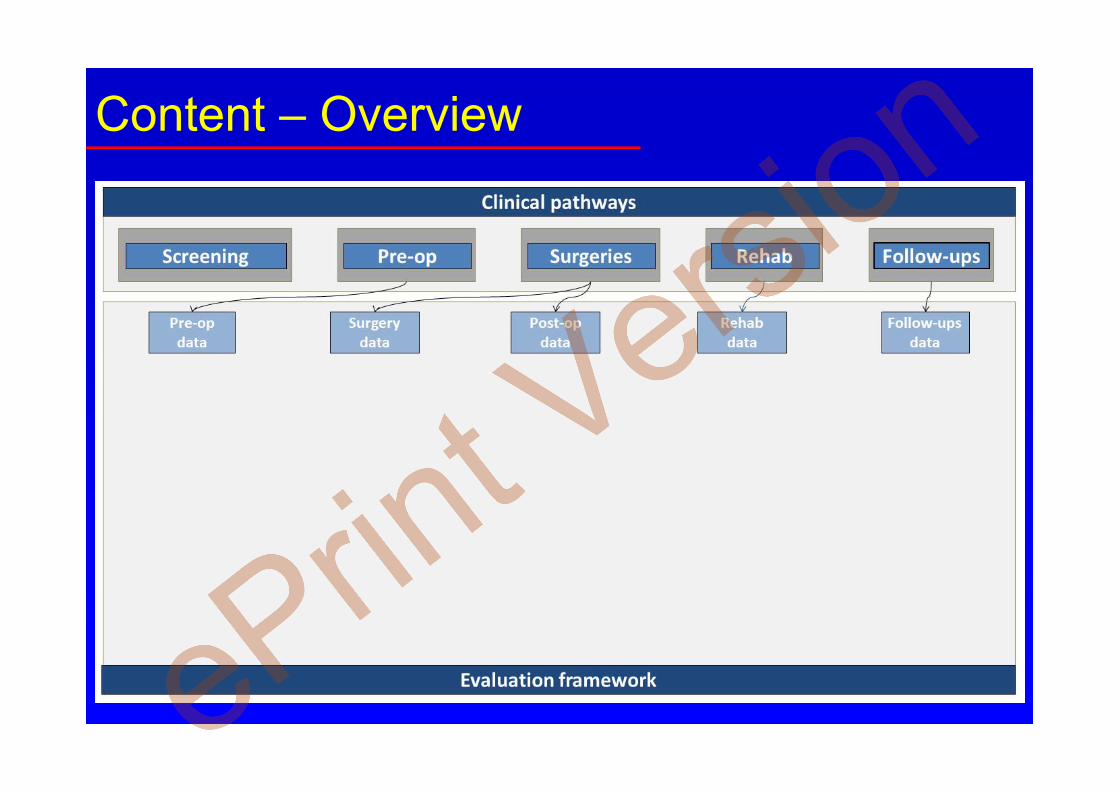
Content – Overview
Content – Overview
Content – Overview
Content – Overview
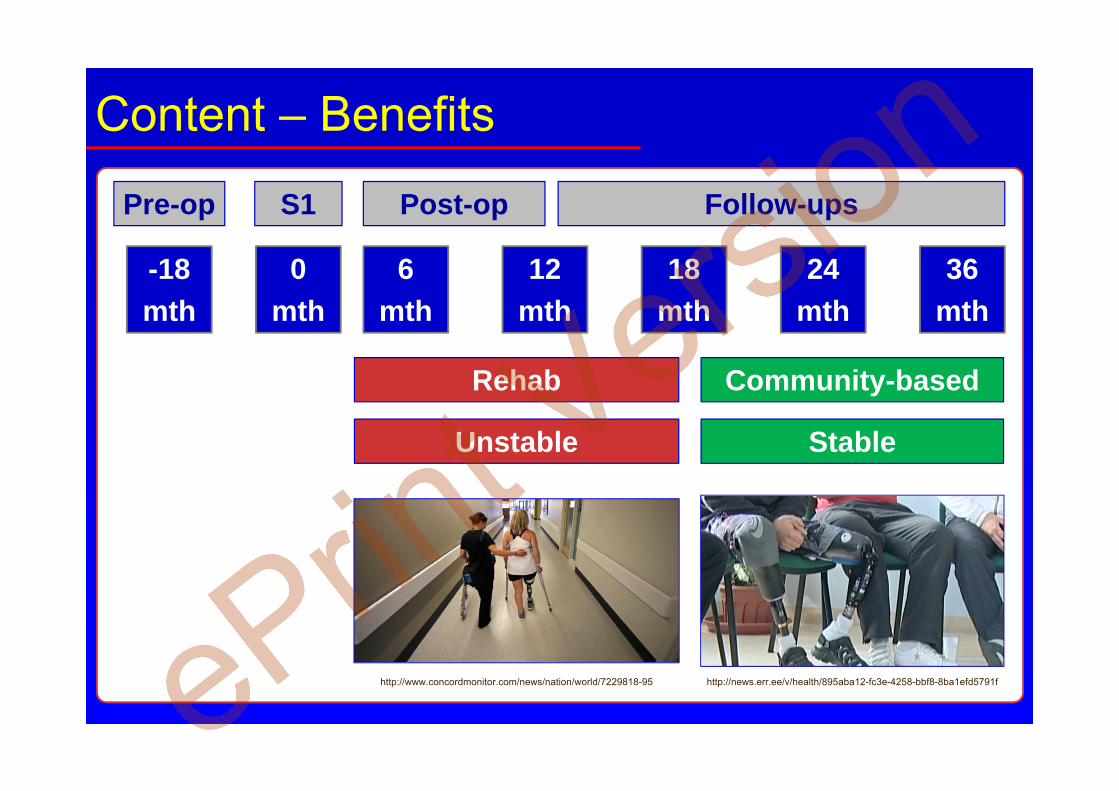
Content – Benefits
Pre-op S1 Post-op
-18mth
0mth
6mth
12mth
24mth
36mth
18mth
Rehab Community-based
Unstable Stable
Follow-ups
http://news.err.ee/v/health/895aba12-fc3e-4258-bbf8-8ba1efd5791fhttp://www.concordmonitor.com/news/nation/world/7229818-95
Content – Benefits

Content – Benefits
Content – Benefits
Content – Benefits
Content – Benefits
Content – Benefits
Content – Benefits
Content – Benefits
Content – Benefits
Content – Benefits
Content – Benefits
Content – Benefits
Content – Benefits

Content – Benefits
Content – Benefits
Content – Benefits
Content – Benefits
Content – Benefits
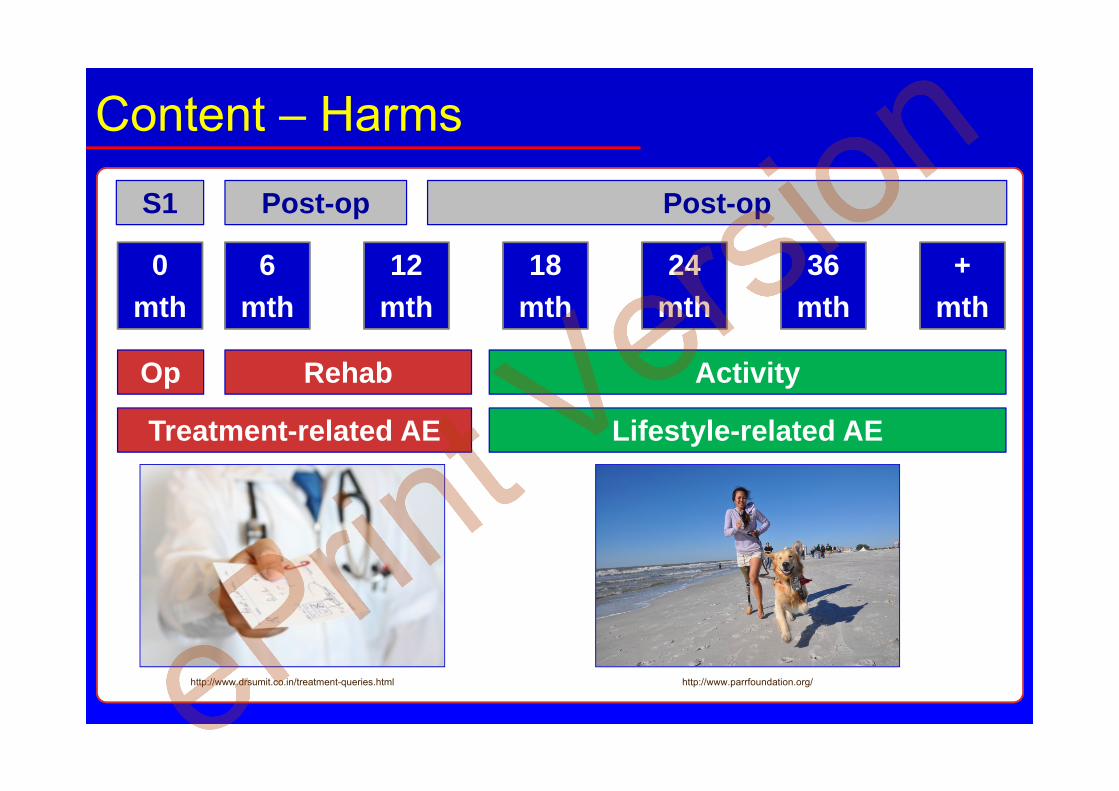
Content – Harms
S1 Post-op
0mth
6mth
12mth
24mth
36mth
18mth
Rehab Activity
Treatment-related AE Lifestyle-related AE
Op
Post-op
+mth
http://www.parrfoundation.org/http://www.drsumit.co.in/treatment-queries.html
Content – Harms
Content – Harms

Content – Harms

Content – Harms

Content – Harms
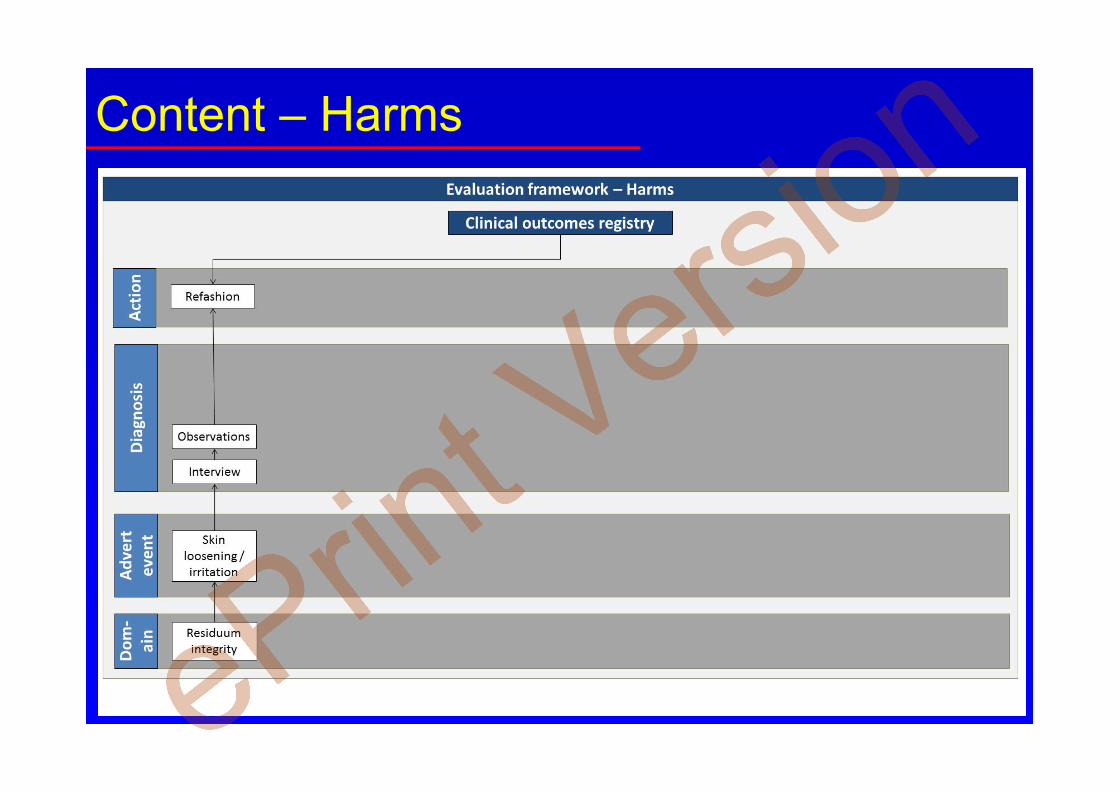
Content – Harms
Content – Harms
Content – Harms
Content – Harms
Content – Harms
Content – Harms

Content – Harms
Content – Harms
Structure - Technical platform
Medical information
X-ray, MRI, Scans, etc…
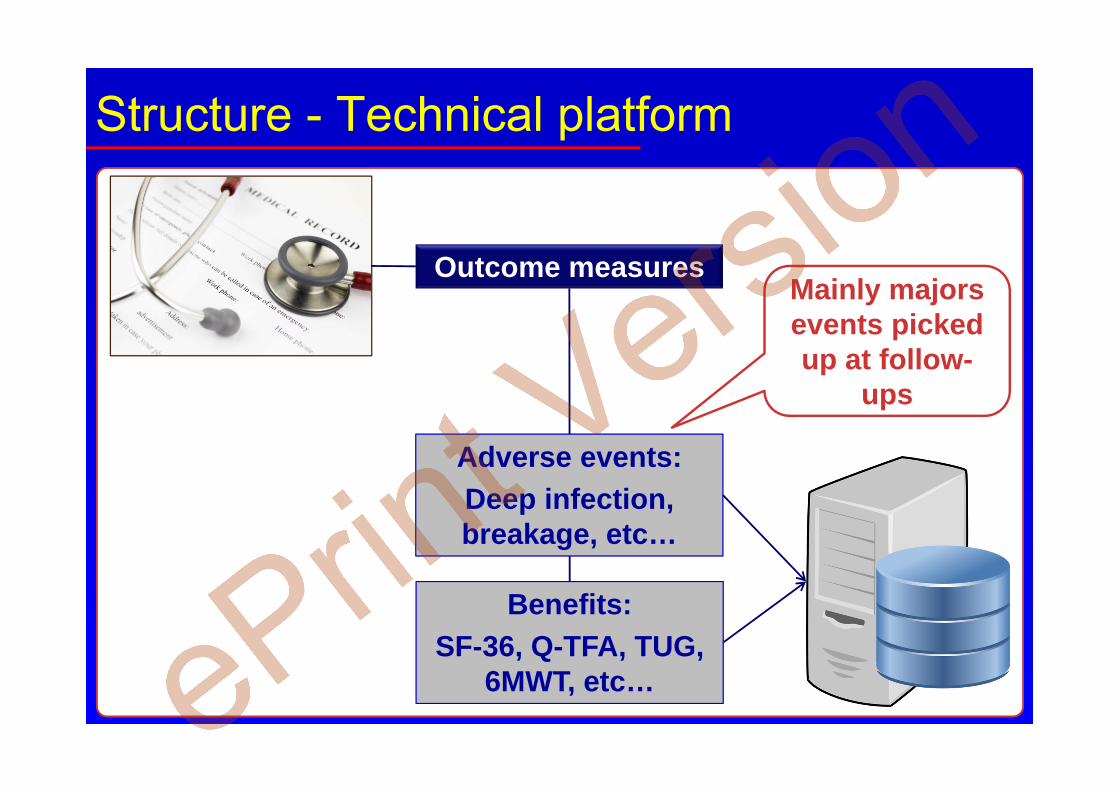
Structure - Technical platform
Outcome measures
Benefits:SF-36, Q-TFA, TUG,
6MWT, etc…
Adverse events:Deep infection, breakage, etc…
Mainly majors events picked up at follow-
ups

Structure - Technical platform
https://www.pinterest.com/brothertedd/the-good-the-bad-and-the-ugly/
Structure - Technical platform
Patient journey
e.g., Static and dynamics load
bearing progression, first
walk, etc…
Structure - Technical platform
Incidental events
e.g., Fall, new components, etc…
Structure - Technical platform
Minor events
Minor infections treated by GP,
Self-adjustment of fixation, etc…
Not typically pickup at
follow-ups
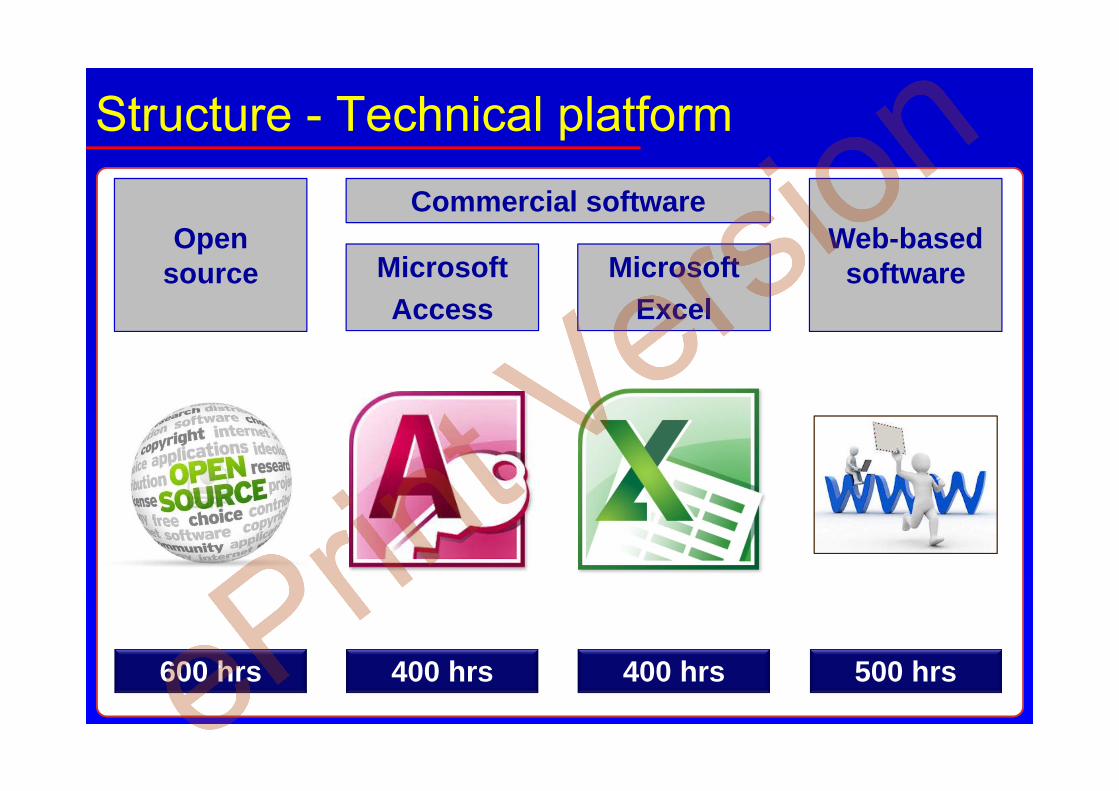
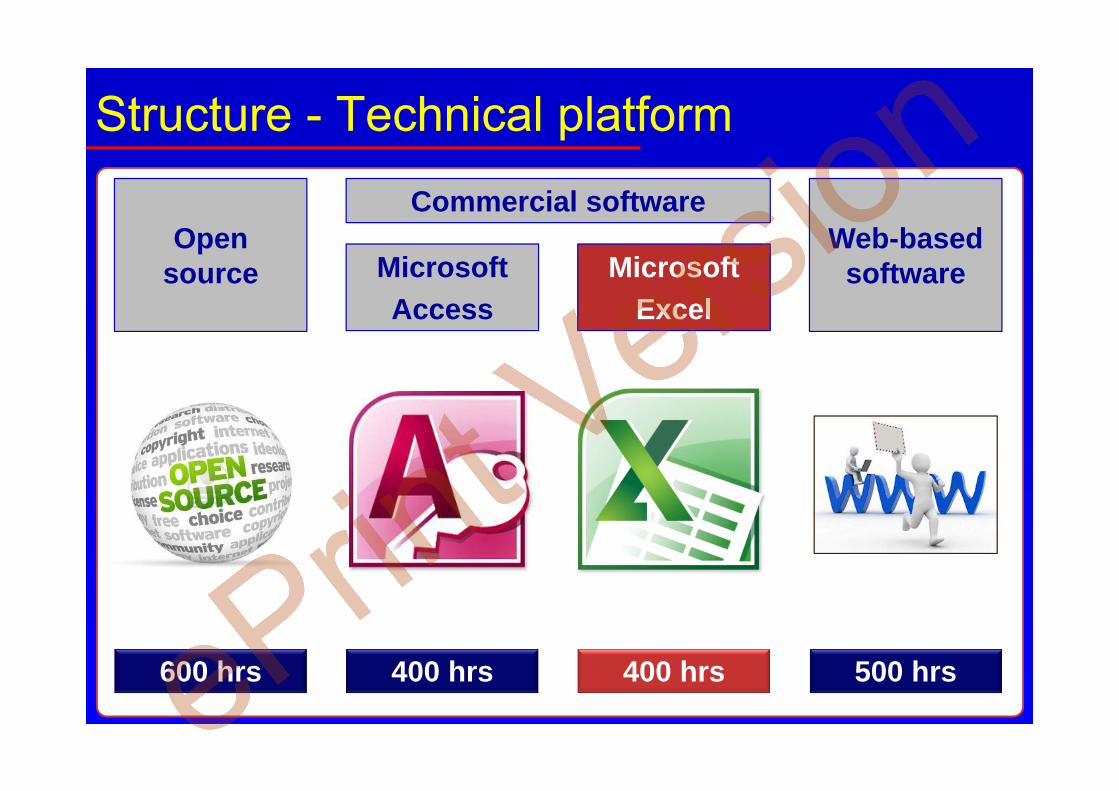
Structure - Technical platform
Commercial software
MicrosoftExcel
MicrosoftAccess
Web-based software
400 hrs 400 hrs 500 hrs
Open source
600 hrs
Structure - Technical platform
Commercial software
MicrosoftExcel
MicrosoftAccess
Web-based software
400 hrs 400 hrs 500 hrs
Open source
600 hrs

Structure - Technical platform
cloud-based system
800 hrshttp://www.soshawaii.com/services/cloud-computing-for-oahu-businesses/.

Structure - Organisation
Easy to import and export data sets (SF-36)
https://skyvia.com/connectors/salesforce.
Structure - Organisation
Cross-correlations between cofounders and outcomes
http://gibraltardatabases.com/database_portfolio.html

Structure - Organisation
Reporting overall and individual data
http://theunboundedspirit.com/
Conclusion – Tips
1. Identify all your outcome measures first
Do the “thinking” before the “doing”!
Conclusion – Tips
1. Identify all your outcome measures first2. Implement at least the common outcomes
Make sure you are using validated instruments providing publishable data!
Conclusion – Tips
1. Identify all your outcome measures first2. Implement at least the common outcomes3. Choose a commonly used platform
Do you want to “build” or to “drive” the car?
Conclusion – Tips
1. Identify all your outcome measures first2. Implement at least the common outcomes3. Choose a commonly used platform4. Choose a flexible platform
Needs and standards change: make sure you can accommodate adjustments
Conclusion – Tips
1. Identify all your outcome measures first2. Implement at least the common outcomes3. Choose a commonly used platform4. Choose a flexible platform 5. Start building your DB with Case 1
Entering back-log of data could take a long time!
Conclusion – Tips
1. Identify all your outcome measures first2. Implement at least the common outcomes3. Choose a commonly used platform4. Choose a flexible platform 5. Start building your DB with Case 16. Generate statistically-ready outcomes
Data matter… but statistical analyses matter more!
Conclusion – To know more
Publication submitted to
APMR:
• Al Muderis M, Khemka A,
Lord S, Bosley B, Frossard
L. Clinical pathways and evaluation framework for bone-anchored prostheses: The Osseointegration Group of Australia Accelerated Protocol. 2015.
http://www.archives-pmr.org/
Conclusion – To know more
Presentation at 2nd Australasian
Osseointegrated for Amputees
Conference :
• Frossard L, Formosa D,
Quincey T, Berg D, Burkett B.
Cost effectiveness of osseointegration. 2015.
Brisbane, Australia. p 3
http://eprints.qut.edu.au/82497/
Adj/Prof Laurent Frossard
Las Vegas, Nevada, USA
26/03/2015
Queensland University of Technology, Brisbane, QLD, Australia
University of the Sunshine Coast, Maroochydore, QLD, Australia
Evaluation framework to assess benefits and harms of bone-anchored
prosthesis
www.LaurentFrossard.com
6th International Conference Advances in Orthopaedic Osseointegration

Websitewww.laurentfrossard.com
www.YourResearchProject.com
LinkedInwww.ca.linkedin.com/pub/laurent-frossard/5/4b4/b59/
Google+www.plus.google.com/#113083134851353167716/about
Facebookwww.facebook.com/YourResearchProject












![Don Harms V1[1]](https://static.fdocuments.in/doc/165x107/54b4bd0b4a79592a668b45b5/don-harms-v11.jpg)





