Evaluation and Management of Patients with · PDF fileEvaluation and Management of Patients...
30
Evaluation and Management of Evaluation and Management of Patients with Gastroparesis John I Allen, MD, MBA, AGAF Minnesota Gastroenterology PA University of Minnesota School of Medicine Vice President – American Gastroenterological Association Vice President American Gastroenterological Association
Transcript of Evaluation and Management of Patients with · PDF fileEvaluation and Management of Patients...

Evaluation and Management of Evaluation and Management of Patients with Gastroparesis
John I Allen, MD, MBA, AGAF
Minnesota Gastroenterology PAgy
University of Minnesota School of Medicine
Vice President – American Gastroenterological AssociationVice President American Gastroenterological Association

Major Take Home Points
Definition and Facts About Gastric Emptyingp y g
Practical Evaluation for Gastroparesis
Initial Stepped Approach to TreatmentInitial Stepped Approach to Treatment
How to Manage the Patients that are not easy
When to consider an enteral feeding tube or Gastric Electrical Stimulation

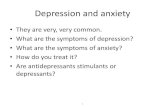
Digestive Mechanism - Simplified
UESFood bolus Food bolus transported along esophagus
(7-10”, 25 cm long)
Gravity &Peristalsis
LES
LES relaxes to allow food to pass into the stomach
Impulses generate gastric peristalsisLES
PacemakerImpulse
Impulses generate gastric peristalsis
HClHClFood is mixed and ground, chemically broken-down, ingested microbes killed
Pylorus Closed
Sphincter of Oddi
Bile Digestive
Pylorus controls the emptying of the food into the duodenum
gJuice
Via sphincter of Oddi, bile emulsifies fats, pancreas secretes digestive juice and transports wastes into the rectum
Anal SphincterClosed


Gastric Motility
In its resting state, the stomach is small and contains gabout 50 ml of fluid
Swallowing causes the fundus to relax (receptive l ti ) t i b l f f d f th relaxation) to receive a bolus of food from the
esophagus
Relaxation is coordinated by vagal fibers and is Relaxation is coordinated by vagal fibers and is facilitated by gastrin and cholecystokinin (two polypeptide hormones secreted by the GI mucosa)

Gastric Motility
Mixing occurs as food is propelled to the g p pantrum
As food approaches the pylorus, peristaltic pp py , pwaves force contents back toward the body (retropulsion)
Mixes food with digestive juices and breaks down large food Mixes food with digestive juices and breaks down large food particlesPylorus = 1.5 cm long/always open about 2.0 mm
Opens wider during antral contractionNormally no regurgitation from duodenum to antrum

Gastric Emptying
Rate depends on:200 Kcal/hourVolume
Osmotic pressureChemical composition of gastric contents
200 Kcal/hour
p g
Larger volumes of food increase gastric pressure peristalsis and rate of emptyingpressure, peristalsis, and rate of emptying
Solids, fats, and non-isotonic solutions delay t i t igastric emptying
Certain hormones inhibit gastric motility gthereby delaying emptying

Gastric Emptying Ratesp y g
Camilleri M. NEJM 2007; 356:820

Patient # 1: “I throw up” 44 year old man with Type II Diabetes is referred from the ED with recurrent vomiting. 18 ED visits in the last 6 months for pain and sedation medications fluids and months for pain and sedation medications, fluids and anti-emetics. He complains of abdominal pain, constant nausea and vomiting at least 8 times weekly. His HgbA1c is 9.4. Endoscopy, RUQ US, HIDA Scan and CT (with is 9.4. Endoscopy, RUQ US, HIDA Scan and CT (with Enterography) all were normal. A solid phase Gastric Emptying Study was abnormal.
Consider the key points from his history, physical exam, initial laboratory values and imaging.
Camilleri et al Epidemiology Mechanisms and Management of Diabetic Camilleri et al. Epidemiology, Mechanisms and Management of Diabetic Gastroparesis. Clin Gastro Hep 2011; 9:5-12.

Diabetic Gastroparesis Delayed gastric emptying in absence of mechanical obstruction.
P t di l f ll iti ( ft f ld f d) d Post-prandial fullness, nausea, vomiting (often of old food) and bloating.
Diabetes = 1/3 of all GP/
5-12% of patients with diabetes have symptoms of GP.
Prevalence of definite GP in the population (2007) was 24/100 000Prevalence of definite GP in the population (2007) was 24/100,000
Diabetics with GP – worse with poor glycemic control but persists4.8% Type I4.8% Type I1% Type IIO.1% of non-diabetics

Additional Causes
Post-viral
Anorexia nervosa
Meds (narcotics, anti-cholinergics)Bentyl, Antivert, Phenergan, Cogentin, Atrovent, Ditropan
Amyloid and scleroderma
ddiAddisons
Migraines
Hypothyroidism

Evaluation of Symptoms
History and physical examinationMedications and past treatments
E d d SBFT (CT MR E t h )Endoscopy and SBFT (CT or MR Enterography)
Lactose, Fructose, Glucose Breath Tests
Ultrasound and possible Nuclear GB Scan
Solid phase Gastric Emptying Study or Capsule Motility
Evaluation for Central causes (Neurological, Tumor)

Scintiscans of Residual Gastric Contents
Camilleri M. N Engl J Med 2007;356:820-829


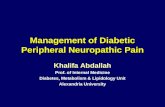
Blood Sugar SignalsLow Blood Sugar High Blood Sugar = Insulin
CravingsDepression
Increased Gastroparesis ActivityInflammation
g g
DepressionFatigue
InsomniaLack of Focus
Irritable
Fat StorageWeight gain
High CholesterolHigh Triglycerides
High Blood Pressure
Blood Sugar Levels
200Balanced Blood Sugar
80
100
120
140
160
180
Suga
r Lev
el
Decrease in Gastroparesis ActivityIncreased Energy
Weight LossEven Moods
0
20
40
60
80
1/2 1.0 1 1/2 2.0 2 1/2 3.0 3 1/2 4.0 4 1/2
Bloo
d Eliminate CravingsLower Cholesterol
Sense of Well-Being
Hours Since Last Meal/Snack
Balanced Blood Sugar Fluctuations Erratic Blood Sugar Fluctuations
© 2/2011 Minnesota Gastroenterology, PA. (612) 871-1145

Management ProgressionManagement ProgressionLeast invasive/risky
Lif t lLifestyle
Pharmacologya aco ogy
Tube feeding
Gastric Pacing
SMost invasive/risky
Surgery
Total parental nutritionTotal parental nutrition

Lifestyle Changes
Mild (Gastric Retention 10-15% at 4 hours)Low fatSmall mealsTobacco cessation
Moderate (16-35%)Periodic homogenized food
Severe (>35%)Homogenized foodOften with J tube (10% weight loss in 6 months)( g )

Medical Treatments
Reverse underlying conditionsOptimize glucose and electrolyte levels
Medication ReviewMedication ReviewAnti-hypertensive meds (calcium channel blockers)Anti-cholinergics (anti-depressants)Exenatide and pramlintide (hyperglycemia meds)Exenatide and pramlintide (hyperglycemia meds)

Anti-emeticsTricyclic Anti-depressants
86% at least moderate improvementAmitriptyline or nortriptylineAmitriptyline or nortriptyline
10-100 mg dailyStart with 10-20 mg at bedtime and work up in 10 mg increments over several weeksSedative side effects
BenzodiazepinesLorazepam (Ativan) – anxiety – 1-2 mg PO q day
Cannabinol (Marinol) 2 5 5 mg BIDCannabinol (Marinol) 2.5 – 5 mg BIDApepritant (Emend) 80 mg dailyAcupuncture (P6) or Relief BandAcupuncture (P6) or Relief Band

Prokinetics
Promote antral contractility
Antiemetic qualities
Metoclopramide (acetylcholine release and inhibition of Metoclopramide (acetylcholine release and inhibition of dopamine receptor)
Proximal gut onlySide effects 50% - Medical Legal Riskg
Parkinsons, somnolence, tardive dyskinesia, depression, breast engorgementDetailed documentation needed10 mg 30 minutes prior to meals (20 mg QID)

ProkineticsDomperidone (Motilium) – peripheral acting dopamine-2 antagonist
Does not cross BB barrieroes o c oss ba e10 mg before meals and q HS (max 30 mg QID)Need at least 3 months of therapyBreast engorgement, irregular mensesCanada New Zealand TexasCanada, New Zealand, Texas
www.fda.gov/cder/news/domperidone.htm
Tegaserod – withdrawn March 2007Macrolide antibiotics
Erythromycin 2-3 mg/kg IV q 6 or 125-250 mg TID (suspension)

Abdominal Pain
89% of patients with gastroparesisp g p
Acetaminophen and NSAIDʼs
IV ketorolac can be used to interrupt gastric dysrythmias IV ketorolac can be used to interrupt gastric dysrythmias in DM hospitalized for gastroparesis
15-30 mg IV q 6 hours
Tramadol 50-100 mg PO q 6
Gabapentin 100-1200 mg TID (Neurontin)

Abdominal Pain
Tricyclic Anti-depressantsSSRIʼs
Panic attacks – Paroxetine (Paxil) Remeron – increase appetite and sedationEffexor and Cymbalta chronic painEffexor and Cymbalta – chronic pain
Short acting narcotics – oxycodone, ms, dilaudidLong acting narcotics – oxycontin, MScontin or Long acting narcotics oxycontin, MScontin or transdermal fentanyl (or Actique lozenges – 400 micrograms of fentanyl)Alvimopan(Entereg) 6 mg/day –blocks intestinal effects of narcotics (recently withdrawn)effects of narcotics (recently withdrawn)


Jejunal Feeding Tube Gastrostomy or GJ Tubey

Enterra Therapy: U. S. Indication
“Enterra Therapy is indicated for the Enterra Therapy is indicated for the treatment of patients with chronic, intractable (drug
refractory) nausea and vomiting secondary to gastroparesis of diabetic or idiopathic origin.”g g

Gastric Electrical StimulationGastric Electrical Stimulation

Lead FixationLead Fixation

Stimulator PocketStimulator Pocket

Conclusion: What are we missing and How Can we Help?How Can we Help?