“Evaluating an Asymptomatic patient for CAD– should we or should we not? Your role will be –...
68
“Evaluating an Asymptomatic patient for CAD– should we or should we not? Your role will be – “Yes – we should” DR H S ISSER MD DM SENIOR CARDIOLOGIST VMMC & SAFDARJANG HOSPITAL NEW DELHI.
-
Upload
shauna-mccoy -
Category
Documents
-
view
218 -
download
0
Transcript of “Evaluating an Asymptomatic patient for CAD– should we or should we not? Your role will be –...

“Evaluating an Asymptomatic patient for CAD– should we or should we not? Your role will be – “Yes – we should”
DR H S ISSERMD DMSENIOR CARDIOLOGIST VMMC & SAFDARJANG HOSPITAL NEW DELHI.

• Is asymptomatic CAD prevalent YES/NO
• Is asymptomatic CAD clinically important YES/NO
• Can asymptomatic CAD be diagnosed YES/NO
• Does treatment of asymptomatic CAD reduce future cardiovascular events YES/NO
• Clinical Implications of Risk Assessment YES/NO

Coronary Artery Disease in an Asymptomatic Population Undergoing a Multidetector Computed Tomography (MDCT) Coronary Angiography
128 (68%) demonstrated MDCT findings compatible with CAD.
111 (86.7%) had non-significant (diameter stenosis ≤ 50%) 17 (13.3%) had significant CAD (diameter stenosis ≥ 50%).
Compared with older subjects (mean age 56±8 years), younger subjects had a lower prevalence of MDCT findings of CAD 55.5% vs. 12.5%, respectively (P<0.001),
Regardless of risk factors. Males had more CAD (mostly non-significant) compared with females (109 [72.7%] vs. 19 [50.3%], respectively; P= 0.007). Subjects with ≥ 2 risk factors had a higher prevalence of CAD in general and significant CAD in particular (P<0.001).
Is asymptomatic CAD prevalent

Detection of CAD before its ‘full blown’ manifestation may have a beneficial impact on the natural course of the disease
Clinical risk-factor assessment and stress testing, are good prognostic indicators cannot serve as definitive diagnostic tools
Risk stratification based on the cardiovascular risk profile is important in identifying cohorts at risk for future cardiovascular events, these data seem to be limited for the diagnosis or exclusion of CAD.
CAD in asymptomatic population not uncommon
Using MDCT a high prevalence of non-significant and low prevalence of significant CAD was discovered in middle age asymptomatic population
Is asymptomatic CAD prevalent
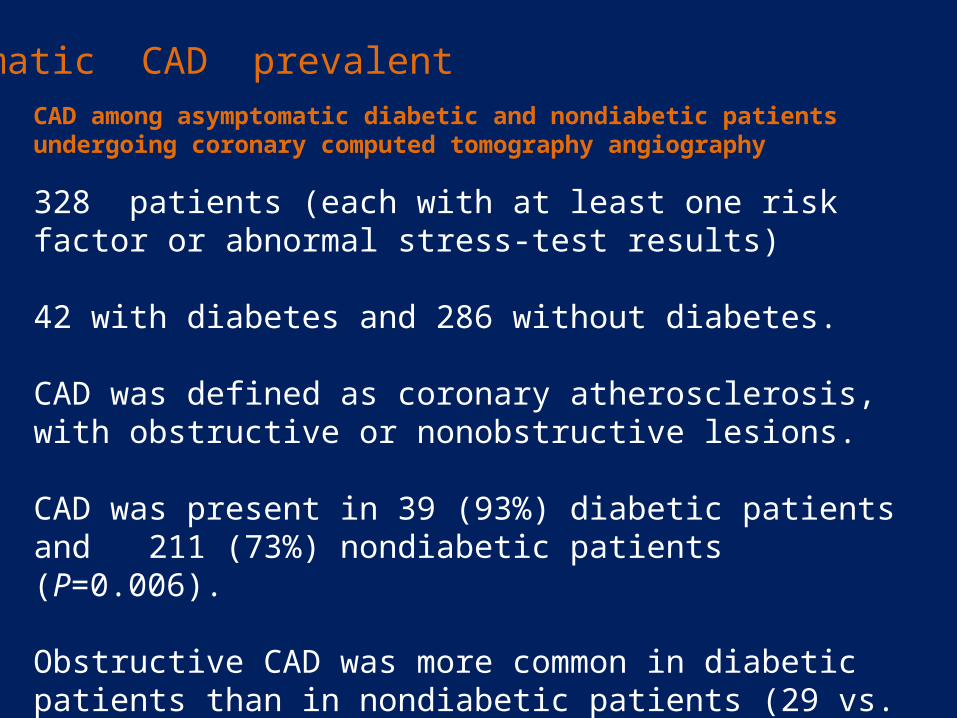
328 patients (each with at least one risk factor or abnormal stress-test results)
42 with diabetes and 286 without diabetes.
CAD was defined as coronary atherosclerosis, with obstructive or nonobstructive lesions.
CAD was present in 39 (93%) diabetic patients and 211 (73%) nondiabetic patients (P=0.006).
Obstructive CAD was more common in diabetic patients than in nondiabetic patients (29 vs. 6.6%, respectively; P<0.0001).
CAD among asymptomatic diabetic and nondiabetic patients undergoing coronary computed tomography angiography
Is asymptomatic CAD prevalent

Diabetic had more coronary segments with atherosclerosis per patient (5.5 segments/patient vs. 2.8 segments/patient in nondiabetic; P<0.0001).
Agatston score was significantly higher in diabetic patients vs. nondiabetic patients (370±96 and 79.9±16, respectively; P<0.0001).
Results indicate a high prevalence (93%) of CAD in asymptomatic diabetic patients with either nonobstructive or obstructive lesions.
CCTA may be a useful imaging modality for selecting patients at high risk who would benefit most from further evaluation for subclinical ischemia
Is asymptomatic CAD prevalent
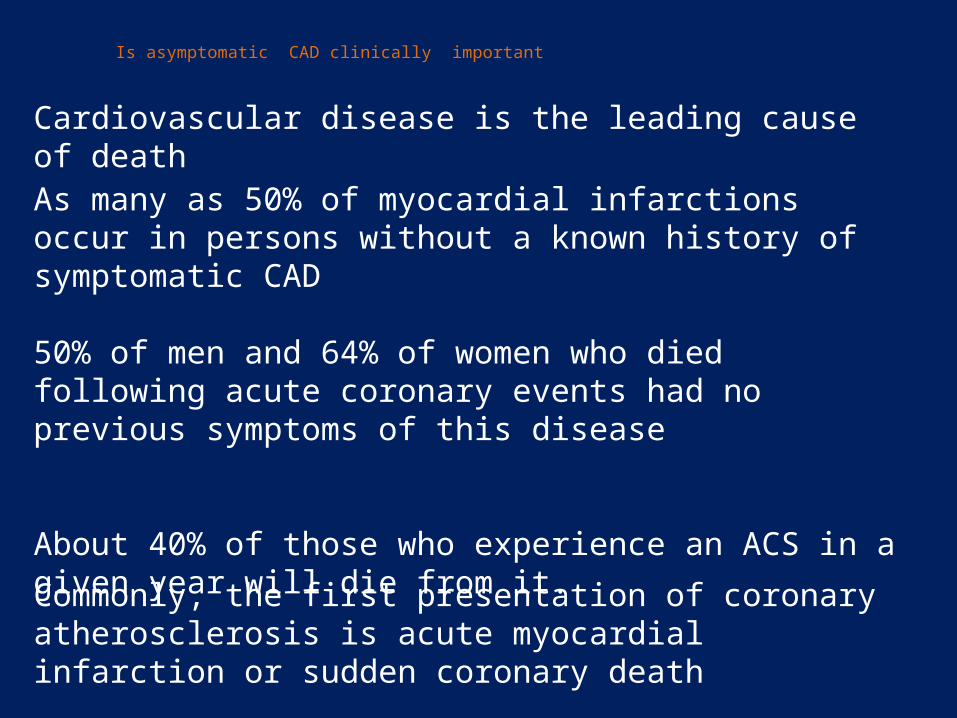
Is asymptomatic CAD clinically important
Cardiovascular disease is the leading cause of death
As many as 50% of myocardial infarctions occur in persons without a known history of symptomatic CAD
50% of men and 64% of women who died following acute coronary events had no previous symptoms of this disease
About 40% of those who experience an ACS in a given year will die from it.
Commonly, the first presentation of coronary atherosclerosis is acute myocardial infarction or sudden coronary death

Cost for treating CHD Is HUGE
Ischemic and/or symptomatic patients, are populations with advanced disease
For these reasons, early diagnosis is urgently needed.
CAD has a pre-clinical detectable phase (i.e. coronary atherosclerosis)
Early detection of CAD in apparently healthy persons may be an important substitute for or supplement to risk assessment based on the traditional risk factors.
Screening using traditional predictors misses a considerable proportion of persons who will suffer from coronary events
Can asymptomatic CAD be diagnosed

The major issue is to develop strategies to identify high-risk patients without established CHD who are candidates for aggressive medical therapies for primary prevention
(1) medical office assessment, (2) tests for silent and inducible ischemia, and (3) noninvasive tests of atherosclerotic burden
The recommended strategies will assist in expanding preventive therapies, i.e. lipid lowering, BP control, smoking cessation, diet, and exercise, in patients at risk for developing CHD.
Can asymptomatic CAD be diagnosed

Asymptomatic patients can be placed into 1 of 3 risk categories. low risk, intermediate risk, and high risk
Low-risk patients encouraged to adhere to healthy life habits.
High-risk patients can directly enter a regimen of aggressive risk reduction through a combination of nondrug and drug regimens.
Patients at intermediate risk become candidates for further risk stratification through noninvasive procedures that test for the presence of myocardial ischemia or coronary atherosclerotic burden.
The purpose is to assist the physician in better defining absolute risk of intermediate-risk patients to predict future major coronary events (unstable angina and myocardial infarction).
Can asymptomatic CAD be diagnosed

Causative risk factorsCigarette smokingElevated blood pressureElevated serum cholesterol (or LDL cholesterol)Alternative: elevated apolipoprotein BLow HDL cholesterolDiabetes mellitusCoronary plaque burden as a risk factorAgeNonspecific ST-segment changes on resting ECGConditional risk factorsTriglycerides*Small LDL particles*Lp(a)*Homocysteine*
Predisposing risk factorsOverweight and obesity (especially abdominal obesity)†Physical inactivity†Male sexFamily history of premature CHDSocioeconomic factorsBehavioral factors (eg, mental depression)Insulin resistanceSusceptibility risk factorLeft ventricular hypertrophy
*These factors are considered conditional risk factors when serum levels are abnormally high.†Obesity and physical inactivity are counted as major risk factors by the AHA.
Coagulation factors*Plasminogen activating factor inhibitor-1FibrinogenC-reactive protein
Can asymptomatic CAD be diagnosed

Account for '50% of the variability in risk in high-risk populations and explain up to 90% of the excess population risk for CHD.
Major Categorical Risk FactorsCigarette smoking (any current smoking)Hypertension (blood pressure (140/90 mm Hg)Elevated LDL cholesterol (160 mg/dL)Low HDL cholesterol (,35 mg/dL)Diabetes mellitus
Can asymptomatic CAD be diagnosed
Two Approaches to Cardiovascular EvaluationI. Diagnosis of existing diseaseII. Prognosis for future coronary events

Estimating total cardiovascular risk in the medical office.
From known risk factors for CHD
presence of multiple risk factors is sufficient to confer a high-risk status, and additional noninvasive testing for coronary atherosclerotic burden or for subclinical myocardial ischemia will be unnecessary.
In patients found to be at intermediate riskAdditional testing may be indicated to better stratify risk.
Can asymptomatic CAD be diagnosed
Could be elevated to the high-risk category by the finding of advanced subclinical atherosclerosis or myocardial ischemia

Exercise ECG Testing
Ischemic ECG response at low workloads of exercise testing is associated with a higher incidence of future events such as angina pectoris, myocardial infarction, and sudden death.
The Multiple Risk Factor Intervention Trial (MRFIT) Reported a nearly 4-fold increase in 7-year coronary mortality (7.6 versus 2.0 per 1000 person-years of risk) among middle aged men with an abnormal exercise ECG versus those with a normal exercise ECG
Can asymptomatic CAD be diagnosed
Noninvasive testing for subclinical myocardial ischemia
In the Lipid Research Clinics Coronary Primary Prevention Trial3775 asymptomatic hypercholesterolemic men
5.7 times greater risk of death due to coronary heart disease in the placebo group among those with a positive exercise test result than among those with a negative test result
Overall, during a mean follow-up period of 7.4 years, there was a 6.7% mortality rate in the group with a positive test result versus 1.3% in the group with a negative test result
Can asymptomatic CAD be diagnosed
Asymptomatic men 40 years of age with 1 risk factor Exercise testing may provide useful information as a guide to aggressive risk factor intervention or the need to evaluate further the cause of myocardial ischemia.

Exercise and Pharmacological Stress Echocardiographylimited data exist to support the use of SE as a tool to elevate the intermediate-risk, asymptomatic patient to a higher risk category
SE could be of value in the assessment of women and elderly patients who fall into the intermediate-risk category
Can asymptomatic CAD be diagnosed
Exercise and Pharmacological Myocardial Perfusion Imaging
An important question is whether stress thallium scintigraphy can be a useful addition to exercise ECG for determining risk for major coronary events in intermediate-risk asymptomatic patients.
Limited data suggest incremental value for this purpose in some populations. Such populations might include postmenopausal women and elderly men (age .75 years), in whom the use of exercise ECG testing is problematic

Positron Emission Tomography
It was not considered to provide additional quantitative risk prediction over exercise ECG in middle-aged asymptomatic men in the intermediate-risk category.
Future applications of this technique in the detection of coronary endothelial dysfunction and the noninvasive monitoring of aggressive medical therapy and risk factor modification.
Can asymptomatic CAD be diagnosed

CONCLUSION Noninvasive testing for subclinical myocardial ischemia
Detect patients who have been found to be at intermediate risk by office-based risk assessment and identify those who are candidates for more aggressive risk reduction therapies
Several studies in middle-aged men in this category have documented that exercise ECG has independent power for predicting major coronary events and may be a useful adjunct in identifying high-risk patients who otherwise would be classified as being at intermediate risk
Can asymptomatic CAD be diagnosed

Noninvasive Tests of Atherosclerotic Burden
With the physician-directed office risk assessment as a foundation, further risk stratification may be valuable, especially when the risk estimate is neither clearly low risk nor high risk (intermediate risk)
“traditional” risk factors are associated with the extent and severity of atherosclerosis. However, at every level of risk factor exposure, there is substantial variation in the amount of the atherosclerosis.
Thus, subclinical disease measurements, representing the end result of risk exposures, may be useful in improving CHD risk prediction
Can asymptomatic CAD be diagnosed
Carotid artery duplex scanning
Electron beam CT (EBCT)
Ultrasound-based endothelial function studies
Ankle/brachial blood pressure ratios, and
Magnetic resonance imaging (MRI) techniques
Can directly or indirectly measure and monitor atherosclerosis in asymptomatic people.
High-sensitivity testing for C-reactive protein (hs-CRP) may also represent a measure of atherosclerosis “burden” and potential marker of atherosclerotic disease risk.
Can asymptomatic CAD be diagnosed

Ankle/Brachial Blood Pressure Index
In population studies, people with a low ABPI have been found to have a considerably higher prevalence of CVD than individuals with a normal ABI.
At least 3 studies have reported an increased combined incidence of CVD morbidity and CVD mortality in persons with PAD detected by ABPI
ABPI values < 0.9 & >1.3 indicates arteriosclerosis of leg arteries
Can asymptomatic CAD be diagnosed
Abnormal ABPI may be an independent predictor of mortality, as it reflects the burden of atherosclerosis

ABPI is a simple, inexpensive, noninvasive measure of PAD. Follow-up studies have shown that an abnormal ABI provides incremental risk-assessment information over and above that provided by traditional risk factors.
ABPI might be a useful addition to the assessment of CHD risk in people aged 50 years and older or those who appear to be at intermediate or higher risk for CVD on the basis of traditional risk factor assessment
Patient having an abnormal ABPI, can be elevated to a higher risk category. The high relative risk in patients with abnormal ABPIs is similar to that of patients who qualify for the AHA secondary-prevention regimen
Can asymptomatic CAD be diagnosed

B-Mode UltrasoundCommon carotid IMT has been associated with cardiovascular risk factors & also with prevalence of CVD in several cross-sectional studies
At least 4 published studies found that carotid IMT measurement was a predictor of the presence of coronary atherosclerosis and its clinical sequelae Thus, carotid IMT defined by noninvasive B-mode ultrasound has been shown to be an independent risk factor for CHD events and stroke.
Measuring intima media thickness (IMT) is a reliable test for calculating the vascular age of a patient
Can asymptomatic CAD be diagnosed

Carotid artery B-mode ultrasound imaging is a safe, noninvasive, and relatively inexpensive means of assessing subclinical atherosclerosis
The technique can measure IMT, an operational measure of atherosclerosis, in a valid and reliable manner
The severity of carotid IMT is an independent predictor of transient cerebral ischemia, stroke, and coronary events such as myocardial infarction
In asymptomatic individuals older than 45 years of age, carefully performed carotid ultrasound examination with IMT measurement can add incremental information to traditional risk factor assessment
Can asymptomatic CAD be diagnosed

Coronary Calcium Scores Calcification within the coronary arterial wall is a recognized marker of atherosclerosis.
EBCT and helical CT are highly sensitive means of detecting coronary calcium and are being intensively evaluated as noninvasive means of defining coronary atherosclerotic disease and identifying the asymptomatic but high-risk CAD patient.
There are, however, relatively few prospective data linking coronary calcium scores with risk of subsequent CHD events.
Data concerning risk prediction with EBCT in asymptomatic people are sparse.
Can asymptomatic CAD be diagnosed
The greatest potential for coronary calcium scores would appear to be in the detection of advanced coronary atherosclerosis in patients at apparently intermediate risk.
Conversely, low or absent coronary calcium scores may prove valuable in determining a low CAD event risk
Until there is more definitive information about the additive value of calcium scores in the asymptomatic individual, coronary calcium measurement should not be recommended for routine risk assessment in asymptomatic populations
Selected use of coronary calcium scores when a physician is faced with a patient with intermediate coronary disease risk may be appropriate.
Can asymptomatic CAD be diagnosed

MRI and Atherosclerotic Disease
Composition of atherosclerotic plaque is important risk factor for acute coronary syndromes. MRI has been shown to characterize tissue noninvasively in many different study systems.
Therefore, research has begun to focus on the use of in vivo MRI to evaluate the vessel wall in several animal models and in humans.
MRI is a promising research tool, but its use appears limited to only a small number of research laboratories at this time.
Can asymptomatic CAD be diagnosed

Endothelial Function Studies and CAD RiskFMD of brachial artery is the test for endothelial dysfunction.( Occlude the brachial artery by inflating BP measuring cuff above 170 mm of mercury for 5 minutes. Post release, the artery should dilate > 10%; if not, this is a sign of endothelial dysfunction.)
Endothelial dysfunction is linked to presence of microalbumin in the urine and exudates in the eye.
Endothelial function, as measured by FMD of brachial artery, is a promising technique that may reflect an independent measure of CVD risk
Additional prospective research is needed . Standardization and improvement of the measurement technique are needed before this modality can become a part of routine clinical assessment of CVD risk
Can asymptomatic CAD be diagnosed

hs-CRP & other inflammatory markersPotential new markers of CAD and all-CVD risk. total plasma homocysteine (tHcy) Lipoprotein(a) [Lp(a)], Fibrinolytic function (as assessed by tissue plasminogen activator and plasminogen activator inhibitor-1 antigens), and Inflammatory parameters such as fibrinogen and CRP.
Many of these markers are not yet considered applicable for routine clinical CVD risk assessment because of
(1) lack of measurement standardization [eg, Lp(a) testing, fibrinogen, and tHcy],
(2) lack of consistency in epidemiological findings from prospective studies with CVD end points [eg, data for Lp(a) and tHcy are inconsistent], and
(3) lack of evidence that the novel marker adds to risk prediction over and above that already achievable through the use of established cardiovascular risk factors
Can asymptomatic CAD be diagnosed

Laboratory evidence and pathological studies suggest that the inflammatory process plays an important part in the atherosclerotic process.
CRP is a sensitive marker for vascular inflammation, and it has been suggested that hs-CRP may provide a novel method to assess CVD risk that is additive to the assessment of traditional CVD risk factors.
hs-CRP has been shown to predict future coronary events in several prospective studies and may add to the predictive value of lipid testing alone.
Additional studies of this approach to risk prediction are warranted and should be undertaken before this measurement can be advised for addition to the routine assessment of coronary risk.
Can asymptomatic CAD be diagnosed
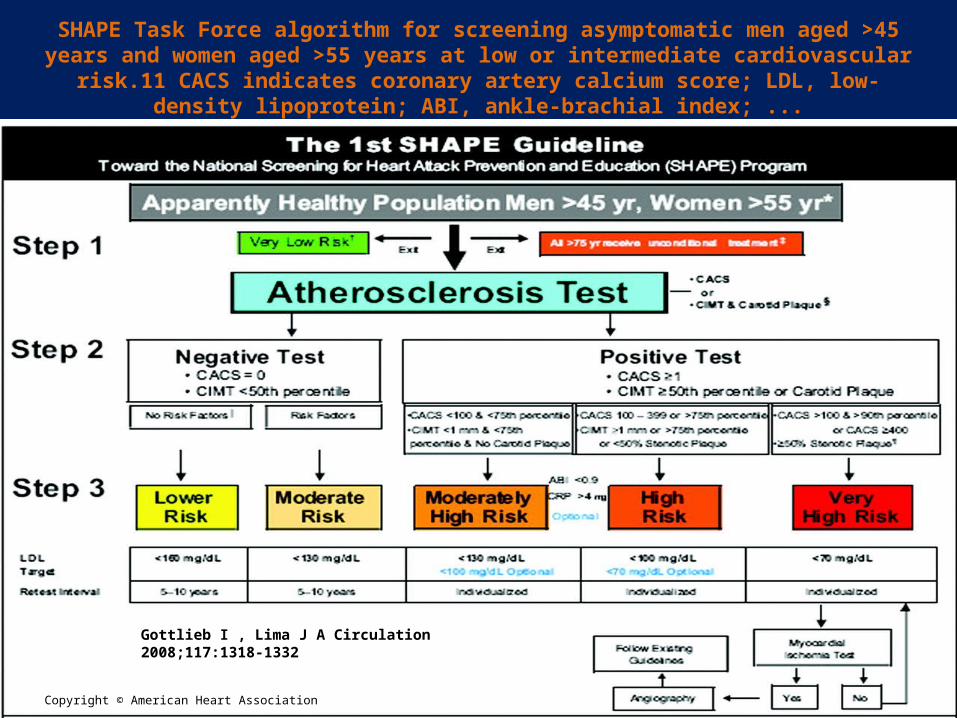
SHAPE Task Force algorithm for screening asymptomatic men aged >45 years and women aged >55 years at low or intermediate cardiovascular risk.11 CACS indicates
coronary artery calcium score; LDL, low-density lipoprotein; ABI, ankle-brachial index; ...
Gottlieb I , Lima J A Circulation 2008;117:1318-1332
Copyright © American Heart Association

Example of an asymptomatic 40-year-old man whose brother died in his 40s from coronary
occlusion.
Gottlieb I , Lima J A Circulation 2008;117:1318-1332
Copyright © American Heart Association

Gottlieb I , Lima J A Circulation 2008;117:1318-1332
Image obtained from a 27-year-old man who came with symptoms attributed to anxiety associated with the fact that his father died of a heart attack at age 27.
Except for Mild obesity and hypertension, the young man had no other risk factors,
His total calcium score was 17, high risk for complications of CAD on the basis of the calcium score alone.
2 large and soft plaques located in the proximal left anterior descending coronary artery by MDCTA suggests that this patient is at a high risk for plaque rupture with potentially disastrous consequences..

2010 ACCF/AHA Guideline for Assessment of Cardiovascular Risk in Asymptomatic Adults: Executive Summary
CHD has a long asymptomatic latent period, which provides an opportunity for early preventive interventions
Many standard risk factors New risk factors or markers are frequently identified and evaluated as potential additions to standard risk assessment strategies.
Must have an independent statistical association with risk after accounting for established readily available and inexpensive risk markers.
Evidence of “additive predictive information,”

Patients at low risk for clinical events are unlikely to gain substantial benefits from pharmaceutical interventions and therefore might best be managed with lifestyle modifications.
Conversely, patients at high risk for events are more likely to benefit from pharmacologic interventions and therefore are appropriate candidates for intensive risk factor modification efforts.
Among patients at intermediate risk, further testing may be indicated to refine risks and assess the need for treatment.
The most basic goal is to estimate the economic consequences of a decision to order a new test. The ultimate goal is to determine whether performing the test provides sufficient value to justify its use
Recommendation for Global Risk Scoring Class I
These scores are useful for combining individual risk factor measurements into a single quantitative estimate of risk that can be used to target preventive interventions
(Level of Evidence: B)
Framingham SCORE, PROCAM (Men), Reynolds (Women) Reynolds (Men)
Recommendation for Family History Class I (Level of Evidence: B) Family history of atherothrombotic CVD should be obtained for cardiovascular risk assessment in all asymptomatic adults.
Recommendation for Genomic Testing Class III Genotype testing for CHD risk assessment in asymptomatic adults is not recommended.

Recommendation for Lipoprotein and ApolipoproteinsAssessments Class III (Level of Evidence: C) Measurement of lipid parameters, including lipoproteins, apolipoproteins, particle size, and density, beyond a standard fasting lipid profile is not recommended for cardiovascular risk assessment in asymptomatic adults.
Lipoprotein-Associated Phospholipase A2 Class IIb (Level of Evidence: B) May be reasonable for cardiovascular risk assessment in intermediate-risk asymptomatic adults.

Natriuretic Peptides Class III (Level of Evidence B)
Measurement of natriuretic peptides is not recommended for CHD risk assessment in asymptomatic adults

Class I1a (Level of Evidence: B) Men 50 years of age or older or women 60 years of age or older with low-density lipoprotein cholesterol less than 130 mg/dL
Class I1b (Level of Evidence: B)In asymptomatic intermediate-risk men 50 years of age or younger or women 60 years of age or younger, measurement of CRP may be reasonable for cardiovascular risk assessment
Class III: (Level of Evidence: B) In asymptomatic high-risk adults, measurement of CRP is not recommended for cardiovascular risk assessment.
In low-risk men younger than 50 years of age or women 60 years of age or younger, measurement of CRP is not recommended for cardiovascular risk assessment.
C-Reactive Protein

Hemoglobin A1C Class Iib (Level of Evidence: B)Measurement of hemoglobin A1C may be reasonable for cardiovascular risk assessment in asymptomatic adults without a diagnosis of diabetes
Microalbuminuria Class Iia (Level of Evidence: B)In asymptomatic adults with hypertension or diabetes, urinalysis to detect microalbuminuria is reasonable for cardiovascular risk assessment
Class Iib (Level of Evidence: B) In asymptomatic adults at intermediate risk without hypertension or diabetes, urinalysis to detect microalbuminuria might be reasonable for cardiovascular risk assessment.

Resting Electrocardiogram
Class IIa (Level of Evidence: C)A resting electrocardiogram (ECG) is reasonable for cardiovascular risk assessment in asymptomatic adults with hypertension or diabetes
Class IIb (Level of Evidence: C)A resting ECG may be considered for cardiovascular risk assessment in asymptomatic adults without hypertension or diabetes

Transthoracic Echocardiography
Class IIb . (Level of Evidence: B)Echocardiography to detect left ventricular hypertrophy may be considered for cardiovascular risk assessment in asymptomatic adults with hypertension
Class III: (Level of Evidence: C)Echocardiography is not recommended for cardiovascular risk assessment of CHD in asymptomatic adults without HT
Carotid Intima-Media Thickness Class IIa (Level of Evidence: B)
Measurement of carotid artery intima-media thickness is reasonable for cardiovascular risk assessment in asymptomatic adults at intermediate risk
Ankle-Brachial Index Class IIa (Level of Evidence: B)
Measurement of ankle-brachial index is reasonable for cardiovascular risk assessment in asymptomatic adults at intermediate risk.

Specific Measures of Arterial StiffnessClass III: (Level of Evidence: C) Measures of arterial stiffness outside of research settings are not recommended for cardiovascular risk assessment in asymptomatic adults
Brachial/Peripheral Flow-Mediated Dilationtest for endothelial dysfunction. Class III: (Level of Evidence: B)Peripheral arterial flow-mediated dilation studies are not recommended for cardiovascular risk assessment in asymptomatic adults

Exercise Electrocardiography Class IIb (Level of Evidence: B)An exercise ECG may be considered for cardiovascular riskassessment in intermediate-risk asymptomatic adults (includingsedentary adults considering starting a vigorous exerciseprogram), particularly when attention is paid to non-ECG markerssuch as exercise capacity
Stress Echocardiography Class III (Level of Evidence: C)Stress echocardiography is not indicated for cardiovascular riskassessment in low- or intermediate-risk asymptomatic adults.(Exercise or pharmacologic stress echocardiography is primarilyused for its role in advanced cardiac evaluation of symptomssuspected of representing CHD and/or estimation of prognosis inpatients with known coronary artery disease or the assessmentof patients with known or suspected valvular heart disease

Class III: (Level of Evidence: C) Stress MPI is not indicated for cardiovascular risk assessment in low- or intermediate-risk asymptomatic adults. (Exercise or pharmacologic stress MPI is primarily used and studied for its role in advanced cardiac evaluation of symptoms suspected of representing CHD and/or estimation of prognosis in patients with known coronary artery disease.)
Myocardial Perfusion Imaging Class IIb (Level of Evidence: C)Stress MPI may be considered for advanced cardiovascularrisk assessment in asymptomatic adults with diabetes orasymptomatic adults with a strong family history of CHD orwhen previous risk assessment testing suggests high risk ofCHD, such as a coronary artery calcium (CAC) score of 400 orgreater

Calcium Scoring Methods
Class IIa (Level of Evidence: B)Measurement of CAC is reasonable for cardiovascular risk assessment in asymptomatic adults at intermediate risk (10% to 20% 10-year risk)
Class IIb (Level of Evidence: B)Measurement of CAC may be reasonable for cardiovascular risk assessment in persons at low to intermediate risk (6% to 10% 10-year risk)
Class III: (Level of Evidence: B)Persons at low risk (<6% 10-year risk) should not undergo CAC measurement for cardiovascular risk assessment

Coronary Computed Tomography AngiographyClass III: (Level of Evidence: C)Coronary computed tomography angiography is not recommended for cardiovascular risk assessment in asymptomatic adults
Magnetic Resonance Imaging of PlaqueClass III: (Level of Evidence: C)Magnetic resonance imaging for detection of vascular plaque is not recommended for cardiovascular risk assessment in asymptomatic adults

Clinical Implications of Risk Assessment
The assessment of risk for development of clinical manifestations of atherosclerotic CVD is designed to aid the clinician in informed decision making about lifestyle and pharmacologic interventions to reduce such risk
Patients are broadly categorized into low-, intermediate-, and high-risk subsets
Level of intensity and type of treatments are based on these differing assessments of risk

Persons at low risk Do not require further testing for risk assessment, as more intensive interventions are considered unwarranted
High risk (established CHD or coronary risk equivalents) are already candidates for intensive preventive interventions, so that added testing will not provide incremental benefit
The initial step in risk assessment in individual patients involves the ascertainment of a global risk score (Framingham, Reynolds, etc.) and the elucidation of a family history of atherosclerotic CVD.
Recommendations, which are simple and inexpensive, determine subsequent strategies to be undertaken.
For the intermediate-risk patient Guideline should help the clinician select appropriate test that can further define risk status
Tests classified as Class IIa are those shown to provide benefit that exceeds costs and risk.
Selection among these will vary with local availability and expertise, decisions regarding cost, and potential risks such as radiation exposure, etc.
Tests classified as Class IIb have less robust evidence for benefit but may prove helpful in selected patients.
Tests classified as Class III are not recommended for use in that there is no, or rather limited, evidence of their benefit in incrementally adding to the assessment of risk; therefore, these tests fail to contribute to changes in the clinical approach to therapy

THANK YOU
THANK YOU

possible limitations
only guidelines developed by national or international medical specialty organizations were reviewed. Hence, guidelines developed by local organizations, private organizations, and individual experts were not considered
An example of an often-cited guideline, therefore, not included is the Society for Heart Attack Prevention and Eradication (SHAPE).
The SHAPE guideline recommends periodic measurement of coronary calcium or carotid intima-media thickness in all asymptomatic men ages 45 to 75 years and women ages 55 to 75 years except those defined at very low risk. Such a universal screening approach is, however, not advocated by any of the guidelines included in this systematic review.
used the AGREE instrument, in theory, a solid recommendation could be createdwithin a poorly developed guideline and vice versa.
it was difficult to quantify the true degree of influence by industry relationships,also because guidelines did not report payment amounts
the ability to detect statistically significant relationships in the quantitative analyses, was limited owing to the small set of included guidelines.
Artery Disease Systematic Review of Guidelines on Imaging of Asymptomatic Coronary Artery Disease J. Am. Coll. Cardiol. 2011;
Measuring intima media thickness (IMT) is a reliable test for calculating the vascular age of a patient
Endothelial dysfunction is linked to presence of microalbumin in the urine and exudates in the eye.
The primary purpose of screening would be to identify patients whose prognosis could be improved with medical therapy or myocardial revascularization.
A consensus statement on coronary CT was issued by American College of Cardiology and the American Heart Association (ACC/AHA) [34]. According to this consensus, coronary CT may be used in “selected” patients with intermediate risk according to the Framingham Risk Score
For intermediate-risk patients, those with an absolute 10-year risk of coronary events of approximately 10 to 20 percent according to the Framingham Risk Score. Noninvasive testing with coronary CT, exercise testing, or perhaps other tests, could improve the assessment of risk and are probably cost-effective.
CAD in asymptomatic population seems to be not uncommon. Using MDCT a high prevalence of non-significant and low prevalence of significant CAD was discovered in middle age asymptomatic population

Patients with subclinical atherosclerosis identified by accurate imaging tests can be expected to benefit from preventive treatment because they are at elevated risk for anevent. Ideally, decision making as to whether imaging individual patients is beneficial should be based on RCTs comparing preventive measures guided by imaging versus not imaging and evaluating CAD event rates as outcome.
Such RCTs are, however, expensive and time-consuming and not always feasible.
In the absence of these RCTs, combine data from trials evaluating the effect of preventive measures with data from cohort studies reporting the association between imaging test results and CAD event rates.
Use of prediction models combining traditional risk factors and test results to calculate a new risk estimate. The Framingham-based intermediate risk (10% to 20% 10-year CAD risk) is reclassified to high risk (a 10-year CAD risk 20%), if the test result is positive, rather than updating the risk estimate.
As opposed to cancer screening, few large randomized controlled trials (RCTs) studying the effect of early detection of CAD on event rates within an asymptomatic populationhave been performed.

To diminish disease burden, primary prevention on the individual level is currently rendered by targeting high-risk subjects, who are identified by office based risk assessment using multiple traditional cardiovascular risk predictors: age, sex, smoking, lipid levels, and blood pressure.
In asymptomatic persons, the emphasis is on the assessment of long-term risk and primary prevention of future clinical disease.
Intensity of risk factor management should be adjusted by the severity of risk
Framingham scoring uses only the “standard” risk factors (smoking, blood pressure, serum cholesterol, HDL cholesterol, blood glucose, and age). Conditional and predisposing risk factors are not used in the Framingham risk equation
Several of the conditional and predisposing risk factors undoubtedly contribute to the development of CHD. Thus, the detection and even therapeutic modification of these risk factors may be appropriate in some patients.

High-risk state as a 10-year absolute risk for developing CHD of 20%.
This level of risk was identified as one that justifies management of risk factors in the clinical setting, particularly for the pharmacological control of elevated blood pressure and cholesterol.
Patients who have intermediate risk in the short term may still be at high risk in the long term
Global assessment for short-term (10 years) risk is the foundation of guidelines
For example, any single risk factor can produce cumulative damage and thus lead to premature clinical syndromes if left untreated for many years.
Every causative risk factor deserves modification under physician supervision once it has reached a categorical level . Clinical judgment is required as to whether risk-factor reduction is best carried out with nondrug or drug therapies.

question of whether tests that assess silent ischemia or inducible ischemia add to prognostic information gained from standard risk factors in asymptomatic patients without known coronary disease
The tests reviewed included exercise ECG, exercise and pharmacological (stress) echocardiogram (echo), exercise and pharmacological myocardial perfusion imaging, ambulatory ECG monitoring, and positron emission tomography (PET).
Their greatest application to date has been diagnostic,
A limitation of all methods used to detect stress (exercise or pharmacologically induced) myocardial ischemia is their dependence on the presence of flow-limiting coronary stenosis.
their predictive value is dependent on the prevalence of disease in the population tested.
majority of future events among patients with CHD are related to severity of obstruction, plaque instability, and total atherosclerotic burden

Figure 2. Predicted 7-year event rates for from Cox regression model for coronary heart disease death or nonfatal myocardial infarction (MI) for categories of Framingham Risk Score
or coronary artery calcium score (CACS).
Gottlieb I , Lima J A Circulation 2008;117:1318-1332
Copyright © American Heart Association

Comparative Value of Coronary Artery Calcium and Multiple Blood Biomarkers for Prognostication of Cardiovascular Events (Am J Cardiol 2012)
The value of coronary artery calcium (CAC) scoring versus multiple biomarkers in increasing risk prediction for cardiovascular disease (CVD) remains unknown
1,286 asymptomatic participants
CAC was calculated by the method of Agatston
Biomarkers measured were C-reactive protein, interleukin-6, myeloperoxidase, B-type natriuretic peptide, and plasminogen activator-1
Mean follow-up time was 4.1 0.4 years with the primary outcome of combined CVD (cardiac death, myocardial infarction, stroke, and late target vessel revascularization).

During follow-up 35 participants developed CVD events cardiac deaths (6%), myocardial infarction (23%), strokes (17%), and late revascularizations(54%). addition of CAC to risk factors was successful in risk prediction, discrimination, andreclassification for future CVD eventsAlthough a combination of biomarkers improved risk prediction, the combinationdid not discriminate or reclassify subjects at risk of future CVD events.
Addition of CAC to risk factors showed significant reclassification whereas addition of multiple biomarkers score did not show significant reclassification.
In conclusion, in this study of asymptomatic subjects without known CVD, addition of CAC but not biomarkers substantially improved risk reclassification for future CVD events beyond traditional risk factors
the most recent American College of Cardiology/American Heart Association guideline for assessment of cardiovascular risk in asymptomatic adults recommends use of CAC scanning as a class Iia indication for risk stratification of asymptomatic patients with an intermediate risk of events.4

The early discovery of CAD in the asymptomatic population may encourage and motivate these patients to be more compliant and to begin or continue to make life style changes
Coronary occlusion and myocardial infarction may, in fact, arise most frequently from mild to moderate stenosis
Angiographic studies showed that 68% of myocardial infarctions were attributable to so-called "angiographically silent" lesions (luminal narrowing <50%), whereas only 14% could be assigned to a severe stenosis (>70%)
A recent study showed that non-obstructive CAD was indeed an independent predictor of future cardiac events
Excellent correlation between the prevalence of CAD and male sex, older age, and number (≥2) of risk factors
Is asymptomatic CAD prevalent

SE appears to add little prognostic/diagnostic information to exercise ECG in middle-aged men but may have utility for adjusting risk assessment in women and older men (.75 years), in whom the predictive power of exercise ECG is uncertain.
The same can be said regarding myocardial perfusion imaging. PET scanning maydetect myocardial ischemia in the presence of less severe degrees of coronary atherosclerosis than can be detected by exercise ECG; however, its lack of availability and high cost seemingly do not justify PET scanning of intermediate-risk patients whose exercise ECGs are normal
Can asymptomatic CAD be diagnosed

ABPI value Interpretation Action Nature of ulcers, if present
above 1.2AbnormalVessel hardening from PVD
Refer routinely
Venous ulceruse full compression bandaging
1.0 - 1.2 Normal rangeNone
0.9 - 1.0 Acceptable
0.8 - 0.9 Some arterial disease Manage risk factors
0.5 - 0.8 Moderate arterial disease
Routine specialist referral
Mixed ulcersuse reduced compression bandaging
under 0.5 Severe arterial disease
Urgent specialist referral
Arterial ulcersno compression bandaging used

Patients With Diabetes Mellitus
Class IIa (Level of Evidence: B)In asymptomatic adults with diabetes, 40 years of age and older, measurement of CAC is reasonable for cardiovascular risk assessment
Class IIb (Level of Evidence: B)1. Measurement of hemoglobin A1C may be considered for cardiovascular risk assessment in asymptomatic adults with diabetes.
2. Stress MPI may be considered for advanced cardiovascular risk assessment in asymptomatic adults with diabetes or when previous risk assessment testing suggests a high risk of CHD, such as a CAC score of 400 or greater. (Level of Evidence: C)
Special Considerations In Women
Class I (Level of Evidence: B)
A global risk score should be obtained in all asymptomaticwomen
Family history of CVD should be obtained for cardiovascular risk assessment in all asymptomatic women

![[Challenge:Future] Project Baikal : We Can & We Should](https://static.fdocuments.in/doc/165x107/58824f231a28ab37158b65b7/challengefuture-project-baikal-we-can-we-should.jpg)