EUCAST Key factors to success - BD
32
EUCAST Conversion: Key factors to success Dewi van der Vegt, MD Radboud University Nijmegen Medical Center, Nijmegen, the Netherlands
Transcript of EUCAST Key factors to success - BD

EUCAST Conversion: Key factors to successDewi van der Vegt, MD
Radboud University Nijmegen Medical Center, Nijmegen, the Netherlands

EUCAST Tasks
• To harmonise clinical breakpoints for new and existing antimicrobial agents
• To define wild type MIC distributions and epidemiological cut‐off values for all antimicrobials
• Provide European standardised and harmonised methods
for antisuscebtibility testing (AST)

EUCAST Disk diffusion
• 2007: No plans for EUCAST disk diffusion method, but….
• Most countries preferred to retain the same methodology (Kirby‐Bauer type methods) calibrated to
EUCAST breakpoints
• 2008: development of a EUCAST disk diffusion method
• Disk diffusion is calibrated to the MIC

EUCAST implementation: The Netherlands
• 2009: decision of the NVMM
(Dutch society of Medical Microbiology)
to implement EUCAST in all Dutch laboratories
• Transition time till the 1st of January 2011:≈
30% of the Dutch laboratories converted

EUCAST implementation: National level
• Create awareness about the coming transition to the EUCAST‐method:
– 2009 + 2010 Papendal:National meetings Dutch Society of Medical Microbiology
– 2009 Zoo Blijdorp, Rotterdam:Chief laboratory technicians
– 2009‐2010 Local laboratory visits

EUCAST implementation: National level
• Create the possibility of one national contact person to answer questions and deal with local
problems
• Convince the local professionals about the reason why to implement EUCAST antimicrobial
susceptibility testing in their laboratory

Why not? We live in EUROPE !! !!

Why EUCAST‐AST?
• Based on EMEA approved indications and outcome evaluation, Pk/Pd, multiple MIC distributions, and modern
principles of determining breakpoints
• Related to European minimum and maximum dosages
• Decisions not based on proposals made by Industry
• ”Case definitions”
for antimicrobial resistance surveillance
• Reviewed at intervals: with new member of class or on initiative of the profession
• Transparent, rationale documents provided
• In the public domain and free of charge

EUCAST implementation: Local level
• Identify a “champion”
to implement the method
• Ensure that your (semi‐) automated system can provide support for EUCAST breakpoints:
– Contact the manufacturers in time!
• Ensure availability of necessary “AST materials”:– Media, disks, supplies, zone‐reader setup
• Automated systems currently available in Europe are incorporating the EUCAST breakpoints

EUCAST implementation: Local level
• Teach and train laboratory personnel in advance – education, demonstrations, practical experience
– February 2010: General session for external
+ internal microbiologists
– October 2010: Introduction session for internal personnel– December 2010: 3 training sessions for internal personnel
• Adapt local SOPs before the day of implementation manual for laboratory personnel

EUCAST implementation: Local level
• Liaise with other laboratories which has already implemented EUCAST
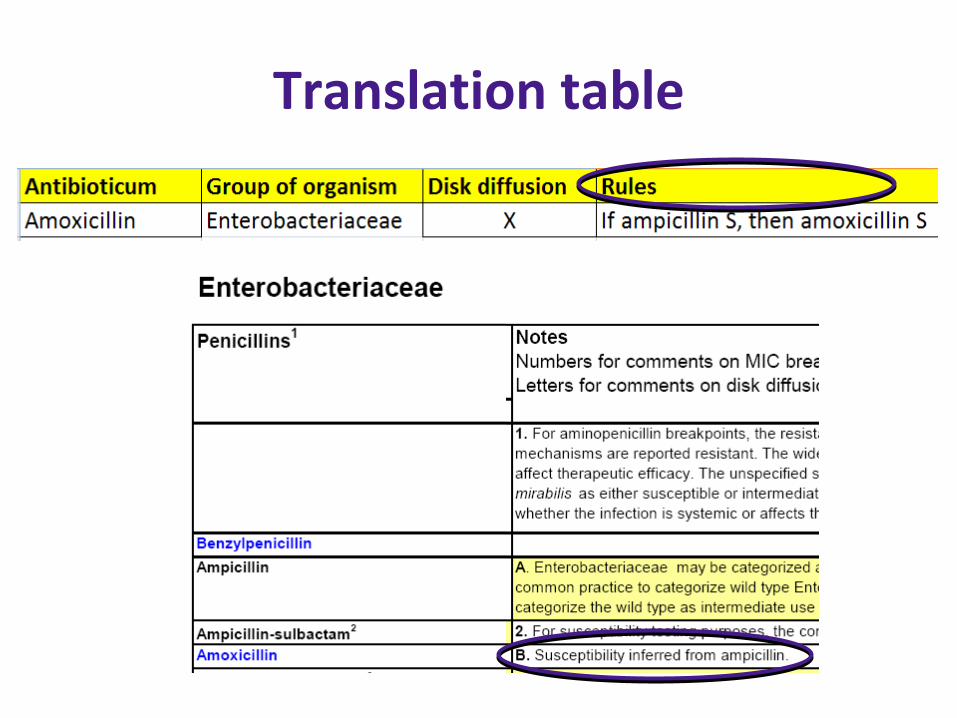
• Import of EUCAST breakpoints and expert rules in electronic laboratory system: create a ‘translation table’
• EUCAST expert rules must be implemented with EUCAST breakpoints and not with CLSI breakpoints!

www.eucast.com


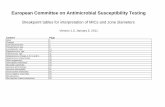
Clinical breakpoint table
–
(dash):
• Species is a poor target for therapy: susceptibility testing is not recommended
Report isolates as R without prior testing or
do not report

Clinical breakpoint table
IE (insufficient evidence):
• Insufficient clinical evidence that the species is a good target with the drug;
Report MIC without S/I/R categorization

Expert rules

Translation table
Antibiotic Group of organismDisk
diffusionLow cut off (<=) High cut off(>=)
"I" includes low
cut off"I" includes high cut
offIntrinsic R If reportedRules
Ampicillin Citrobacter koseri R
Ampicillin Citrobacter freundii R
Ampicillin Enterobacter cloacae R
Ampicillin Enterobacter aerogenes R
Ampicillin Escherichia hermannii R
Ampicillin Hafnia alvei R
Ampicillin Klebsiella spp. R
Ampicillin Morganella morganii R
Ampicillin Proteus vulgaris R
Ampicillin Proteus penneri R
Ampicillin Providencia rettgeri R
Ampicillin Providencia stuartii R
Ampicillin Elizabehtkingia meningoseptica R
Ampicillin Enterobacteriaceae 8 8,1 X
Ampicillin Enterobacteriaceae X 13,9 14
Ampicillin Pseudomonas spp. R
Ampicillin Acinetobacter spp. R
Ampicillin Staphylococcus saprophyticus X 14,9 15
Ampicillin Enterococcus faecium 4 8 X If ampicillin R, then carbapenems R
Ampicillin Enterococcus faecium X 8 10 X If ampicillin R, then carbapenems R
Ampicillin Streptococcus pneumoniae 0,5 2 X If benzylpenicilline or oxacillin S, then ampicillin S. If benzylpenicillin or oxacillin R, then determine ampicilline
Ampicillin Streptococcus pneumoniae X 20 23 X If benzylpenicilline or oxacillin S, then ampicillin S. If benzylpenicillin or oxacillin R, then determine ampicilline
Ampicillin Other Streptococci X 15 21 X
Ampicillin Haemophilus influenzae X 15,9 16 If b‐lactamase positive, then ampicillin R
Ampicillin Non species 2 8 X

Translation table
Antibiotic Group of organismDisk
diffusion
Low cut off value
(<=)
High cut off value
(>=)
"I" includes
low cut off
value
"I" includes
high cut off
value
If
reported
Ampicillin Enterococcus spp. 4 8 X
Ampicillin Enterococcus spp. X 8 10 X

Translation table
Antibiotic Group of organismDisk
diffusion
Low cut off value
(<=)
High cut off value
(>=)
"I" includes
low cut off
value
"I" includes
high cut off
value
If
reported
Ampicillin Pseudomonas spp. R
Ampicillin Acinetobacter spp. R

Translation table
Antibiotic Group of organismDisk
diffusion
Low cut off (<=)
High cut off (>=)
"I"
includes
low cut
off
"I"
includes
high cut
off
Intrinsic
R
Ampicillin Citrobacter koseri R
Ampicillin Citrobacter freundii R
Ampicillin Enterobacter cloacae R
Ampicillin Enterobacter aerogenes R
Ampicillin Escherichia hermannii R
Ampicillin Hafnia alvei R
Ampicillin Klebsiella spp. R
Ampicillin Morganella morganii R
Ampicillin Proteus vulgaris R
Translation table

Issues with EUCAST disk diffusion method
1.
Media
2.
Disk contents
3.
Inoculum suspension
4.
Reading inhibition zone diameters

Media
1.
Mueller‐Hinton agar (MH)
2.
Mueller‐Hinton‐Fastidious (MH‐F) MH + 5% defibrinated horse blood + 20 mg/L β‐NAD
→
Internal quality control; – Use EUCAST recommended strains and inhibition
zones– Daily until performance is satisfactory (≈
1 month) →
– Each new batch of media ≈
weekly

Use the correct disk contentsAntibiotic CLSI (ug) EUCAST (ug)
Piperacillin 100 30
Pip‐tazobactam 100‐10 30‐6
Cefotaxime 30 5
Ceftazidime 30 10
Vancomycin 30 5
Gentamicin HLR 120 30
Nitrofurantoin 300 100
Fusidic acid 15 10
Linezolid 30 10
Mupirocin 5 200

Inoculum suspension
• Inoculum suspension: 0.5 McFarland
• Exception: Streptococcus pneumoniae– 0.5 McFarland from blood agar
– 1.0 McFarland from chocolate agar

Incubation of plates Organism Incubation‐condition
Enterobacteriaceae 35±1 °C 16‐20h
Pseudomonas
spp. 35±1 °C 16‐20h
Stenotrophomonas maltophilia 35±1 °C 16‐20h
Acinetobacter
spp. 35±1 °C 16‐20h
Staphylococcus
spp. 35±1 °C 16‐20h
Enterococcus
spp.
35±1 °C 16‐20hGlycopeptides:35±1 °C 24h
Streptococcus pneumoniae 35±1 °C, 4‐6% CO2 16‐20h
Other streptococci 35±1 °C, 4‐6% CO2 16‐20h
Haemophilus spp. 35±1 °C, 4‐6% CO2 16‐20h
Moraxella catarrhalis 35±1 °C, 4‐6% CO2 16‐20h
Helicobacter pylori
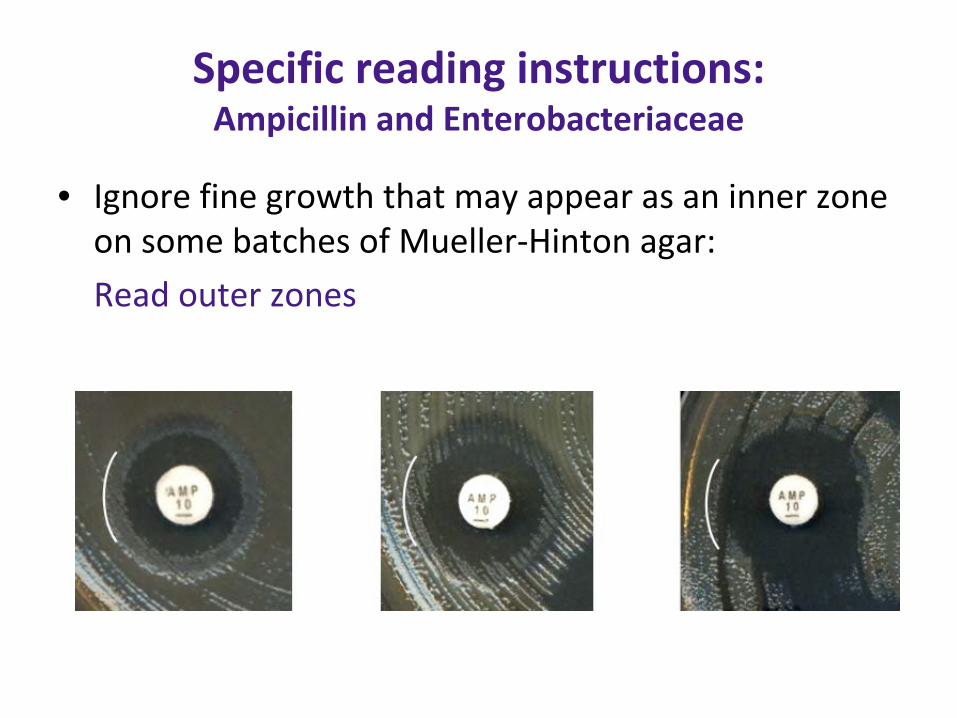
Specific reading instructions: Ampicillin and Enterobacteriaceae
• Ignore fine growth that may appear as an inner zone on some batches of Mueller‐Hinton agar:
Read outer zones

Specific reading instructions: Trimethoprim and
trimethoprim/sulfamethoxazole
• Read inner zones when double zones appear
• Ignore faint growth up to the disk within a zone with otherwise clear zone edges

EUCAST implemenation‐ Remaining issues
Missing breakpoints:• Use of non‐species related breakpoints (Pk/Pd)
• Only based on pharmacokinetic and pharmacodynamic data
• Only MIC breakpoints• Compare MIC with the MIC distribution for the species

EUCAST implemenation‐ Remaining issues
Missing breakpoints (in preperation):• Campylobacter spp.• Burkholderia
cepacia
• Corynebacterium
spp.• Listeria
monocytogenes
• Nocardia
spp.• Actinomycetes
spp.
• Pasteurella
spp.

EUCAST implementation at local level; After implementation
• Keep the method up‐to‐date– EUCAST committee: 5 meetings/year– From 2012; 1 update/year (period from Sept‐Oct)
• Report problems to the national contact person
• Report issues about the lay out/comments on the contents of the documents to EUCAST

Preguntas?




![l>lf·· E ·B; -I,:,C-·-1·1V · cat. no.i bd lj.657 bd lj.6]5 bd 4630 bd 4·627 bd 4628 bd 4886 bd 4546 bd 4·545 bd 4544 bd 4542 bd lj,588 bd lj.593 bd 0102 bd 4636 bd 4632 bd](https://static.fdocuments.in/doc/165x107/5f7c69bb7d840d18665ab1e6/llf-e-b-ic-11v-cat-noi-bd-lj657-bd-lj65-bd-4630-bd-4627-bd-4628-bd.jpg)