Ethical issues in tissue banking for research: a b
30
KEITH BAUER, SARA TAUB and KAYHAN PARSI ETHICAL ISSUES IN TISSUE BANKING FOR RESEARCH: A BRIEF REVIEW OF EXISTING ORGANIZATIONAL POLICIES ABSTRACT. Based on a general review of international, representative tissue banking policies that were described in the medical, ethics, and legal literature, this paper reviews the range of standards, both conceptually and in existing regulations, relevant to four main factors: (1) commercialization, (2) confidentiality, (3) informed consent, and (4) quality of research. These four factors were selected as reflective of some of the major ethical considerations that arise in the conduct of tissue banking research. The authors emphasize that any policy or ethical guidelines designed to regulate tissue bank research should address all four factors. Whenever this sort of research is conducted between several institutions or several countries, the paper suggests that the relevant entities work collaboratively to harmonize their standards. KEY WORDS: commercialization, confidentiality, human tissue sample, informed consent, organizational policies, quality, research, standards, tissue banking INTRODUCTION Tissue banking research increasingly is conducted in partnership between the for-profit and not-for-profit spheres, raising many ethical considerations. 1 In part, this change can be attributed to the growing sophistication of genomic technology and, in particular, the new interest it has fueled in human tissue. 2 In fact, newly established tissue banks are surfacing – many of them private, for-profit enterprises that compete with non-profit tissue banks for the recovery and pro- cessing of these tissues. 3 In addition, tissue banks in the non-profit sector are often supported by the pharmaceutical and biotech industries that help fund academic research and rely on human bio- logical samples recovered and banked by these institutions. 4 Some contend that the current system of safeguards (at least in the US) will become increasingly obsolete in protecting tissue donors; others point to a variety of cultural, organizational, and professional issues that question the ethical appropriateness of for-profit tissue banks and Theoretical Medicine 25: 113–142, 2004. Ó 2004 Kluwer Academic Publishers. Printed in the Netherlands.
Transcript of Ethical issues in tissue banking for research: a b

KEITH BAUER, SARA TAUB and KAYHAN PARSI
ETHICAL ISSUES IN TISSUE BANKING FOR RESEARCH:A BRIEF REVIEW OF EXISTING ORGANIZATIONAL
POLICIES
ABSTRACT. Based on a general review of international, representative tissue
banking policies that were described in the medical, ethics, and legal literature, thispaper reviews the range of standards, both conceptually and in existing regulations,relevant to four main factors: (1) commercialization, (2) confidentiality, (3) informedconsent, and (4) quality of research. These four factors were selected as reflective of
some of the major ethical considerations that arise in the conduct of tissue bankingresearch. The authors emphasize that any policy or ethical guidelines designed toregulate tissue bank research should address all four factors. Whenever this sort of
research is conducted between several institutions or several countries, the papersuggests that the relevant entities work collaboratively to harmonize their standards.
KEY WORDS: commercialization, confidentiality, human tissue sample, informedconsent, organizational policies, quality, research, standards, tissue banking
INTRODUCTION
Tissue banking research increasingly is conducted in partnershipbetween the for-profit and not-for-profit spheres, raising many ethicalconsiderations.1 In part, this change can be attributed to the growingsophistication of genomic technology and, in particular, the newinterest it has fueled in human tissue.2 In fact, newly established tissuebanks are surfacing – many of them private, for-profit enterprisesthat compete with non-profit tissue banks for the recovery and pro-cessing of these tissues.3 In addition, tissue banks in the non-profitsector are often supported by the pharmaceutical and biotechindustries that help fund academic research and rely on human bio-logical samples recovered and banked by these institutions.4 Somecontend that the current system of safeguards (at least in the US) willbecome increasingly obsolete in protecting tissue donors; others pointto a variety of cultural, organizational, and professional issues thatquestion the ethical appropriateness of for-profit tissue banks and
Theoretical Medicine 25: 113–142, 2004.� 2004 Kluwer Academic Publishers. Printed in the Netherlands.

academic-industry relationships.5 In response to these concerns,various governments, non-governmental organizations, and otherinstitutions have been drafting and promulgating policies to regulatetissue banks and their relationships with industry. These policiesrepresent the consensus of private associations (such as the AmericanAssociation of Tissue Banks), reflect the national policies of certaingovernments (such as Spain), and are the products of various inter-national bodies (such as the European Union). Thus, these policiesare broad in scope; we have not surveyed the institutional policies ofindividual banks, academic medical centers, or other institutions.Moreover, the enforcement mechanisms will similarly reflect theauthority of the bodies that produce such policies. For instance, aprivate association will have relatively little authority to sanctionindividual banks for violations of certain policies; on the other hand,governments will have appropriate enforcement mechanisms to en-sure compliance (although resources to achieve such compliance willvary from country to country).
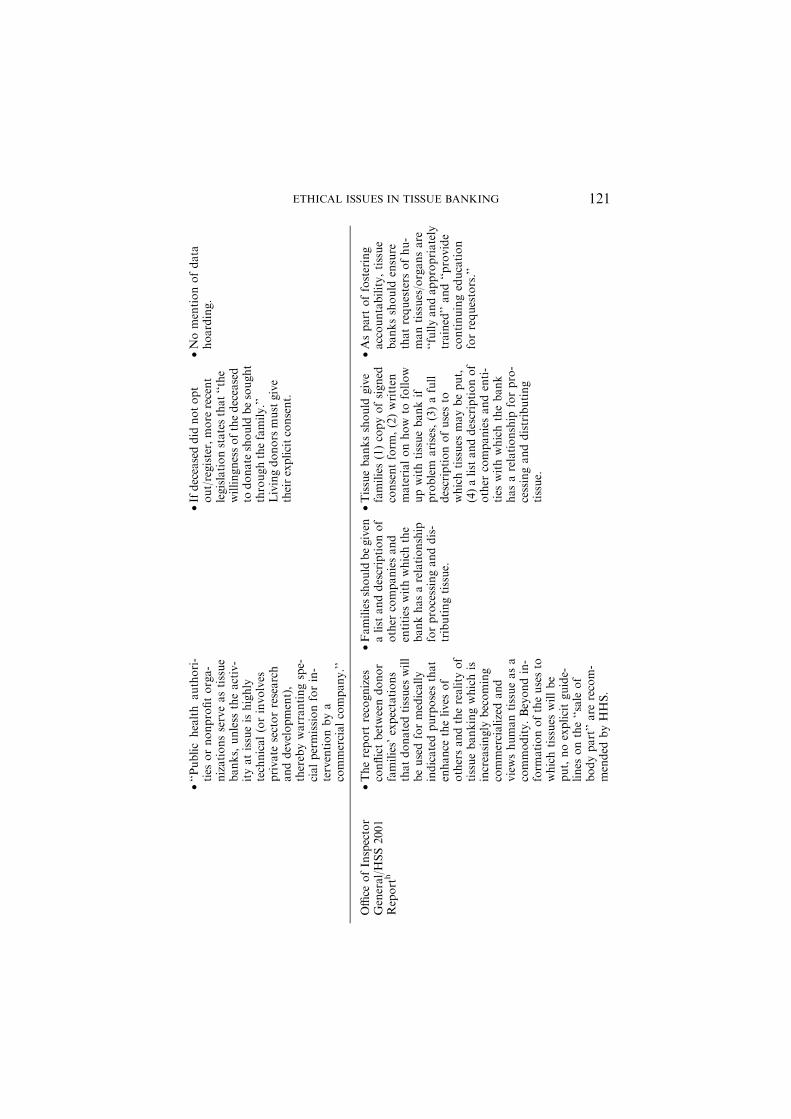
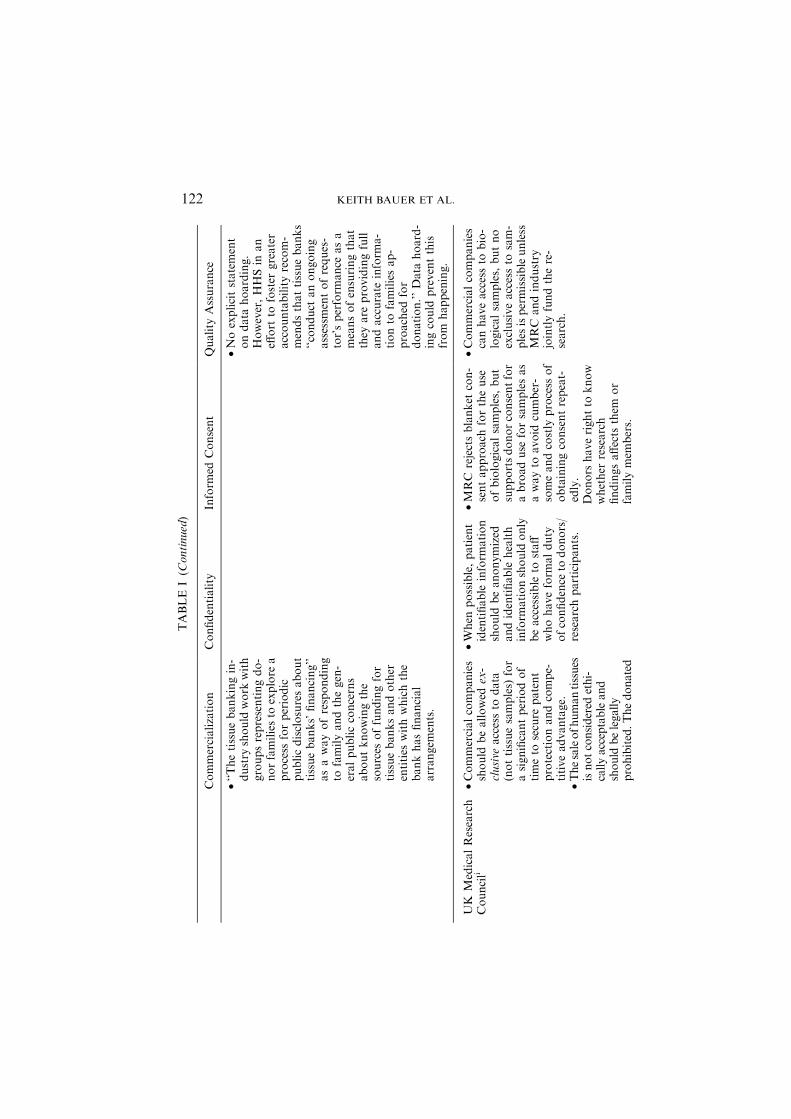
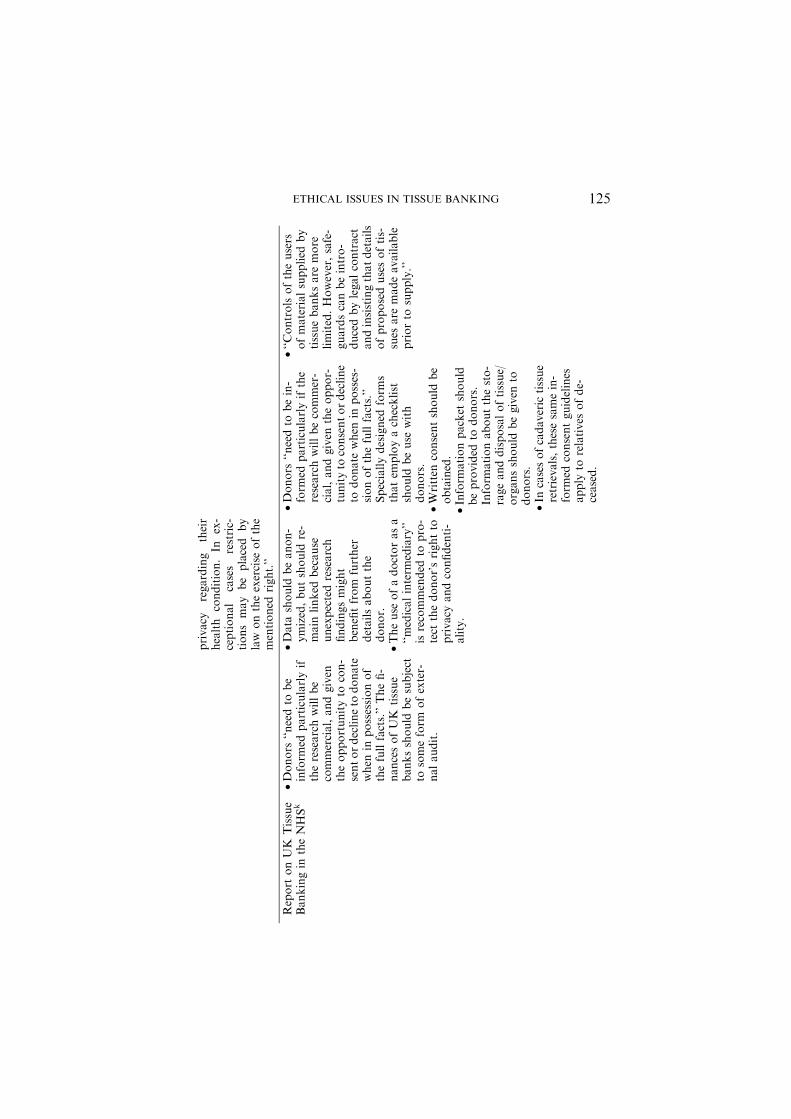
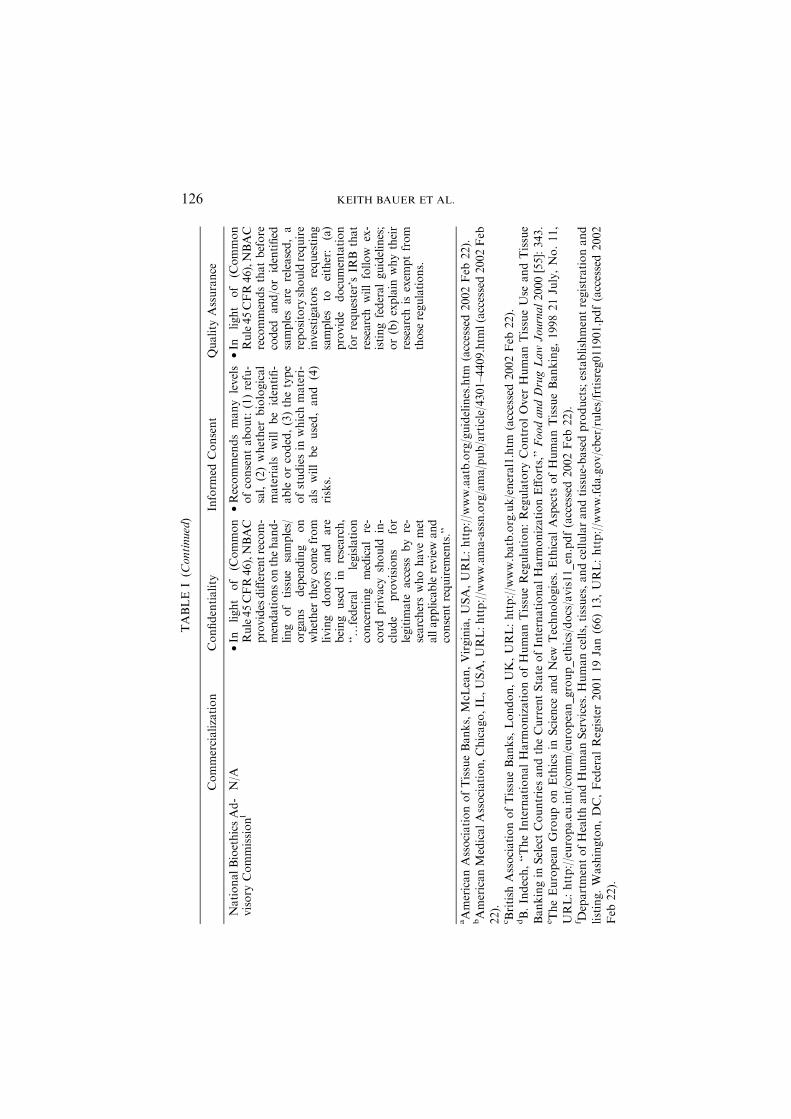
Based on a general survey of representative tissue banking policiesthat were described in the medical, ethics, and legal literature, thispaper reviews the range of standards, both conceptually and inexisting regulations, relevant to four main factors: (1) commerciali-zation, (2) confidentiality, (3) informed consent, and (4) quality ofresearch (see Table 1). These four factors were selected as reflectiveof some of the major ethical considerations that arise in the conductof tissue banking research.6 We recommend that any policy or ethicalguidelines designed to regulate tissue bank research should address allfour factors. Where this sort of research is conducted between severalinstitutions or several countries, we suggest that the relevant entitieswork collaboratively to harmonize their standards.
COMMERCIALIZATION OF HUMAN TISSUES
A number of potential benefits stem from the commercialization ofhuman tissues. For industry, the likelihood of profit based on medicalproducts derived from human tissues is an effective incentive to investin related academic research. With the judicious use of patents andother forms of intellectual property rights, industry has added reasonto support cutting-edge and sometimes financially risky academicresearch involving human tissues. From the perspective of academiccenters, the infusion of capital by industry can help to fund innovative
KEITH BAUER ET AL.114

TABLE
I
Relevantstandardsfrom
ageneralsurvey
oftissuebankingpolicies
Commercialization
Confidentiality
Inform
edConsent
Quality
Assurance
American
Associationof
TissueBanksa
•Noexplicitstatementon
thesellingofbodyparts.
Noexplicitstatement
aboutprofitsto
familiesis
made.
•If
required
bylaw
or
regulation,anexplana-
tionthatnon-profitand/
orfor-profitorganiza-
tionsmaybeinvolved
infacilitatingdonation.
•Donor’smedical
recordsmaybeaccessed
byresearchersandmay
bereleasedto
other
ap-
propriate
parties.
•Identificationofspecific
tissues
beingrequested
fordonationandan
explanationofhow
they
willbeused.
•If
required
bylaw,an
explanationthattissues
maybeusedin
amanner
differentthan
intended.
•Anexplanationof
recoveryprocess.
•Asnotto
undermine
publicconfidence
indo-
nation,tissues
should
be
distributedin
awaythat
‘‘maxim
izeusefulnessto
thepatientcommunity.’’
•Data
hoardingislikelyto
underminethisgoal.
Anexplanationofhow
donation
process
willaffect
body’sappearance
and
burialarrangem
ents.
AmericanMedical
Association
(CouncilonEthical
andJudicialAffairs)b
•Profits
from
commercial
use
ofhumantissuemay
besharedwithpatient.
•N/A
•Inform
edconsentmust
be
obtained
from
patients
for
use
oftissuein
clinical
research.
•N/A
•Potentialcommercialuse
oftissuemust
be
disclosedto
patient
before
profitisrealized.
ETHICAL ISSUES IN TISSUE BANKING 115

TABLE
I(C
ontinued)
Commercialization
Confidentiality
Inform
edConsent
Quality
Assurance
British
Associationof
TissueBanksc
•Statesthat‘‘thereshall
benocommercialdeal-
ingin
humantissue.’’
•Relatives
shallspecifi-
callyagreeto
letthe
tissuebankseek
infor-
mationaboutthedonor
from
professionalssuch
astheGPorpatholo-
gist.
•Recordswillremain
confidential.
•Recordswillbemain-
tained
foraminim
um
of11years
after
the
expirydate
ofthetissue.
•Legallyrequired
inthe
UK
toobtain
consentfor
tissuedonationfrom
per-
sonlegallyin
possessionof
thebody(cadaver).
•It
must
beestablished
that
thedeceaseddid
notobject
todonation.
•It
must
beestablished
that
survivingspouse,partner,
orlivingrelativedoes
not
object
todonation.
•It
must
beestablished
that
noreligiousobstacles
are
•‘‘Allreasonab
leeff
orts
shallbemad
eto
ensure
that
tissues
aresentto
qualified
individuals/or-
ganizationswhohave
acceptedresponsibility
fortheirproper
han
dling
anduse.’’
Nothingstated
about
datahoarding.
•Tissuebankswillin-
form
users
(clinicaland
research)thatalltissue
must
belogged
and
recipienttraceability
must
beinsured.
present.
•Deceased’sreligiousvalues
should
betaken
into
con-
sideration.
•A
written
record
ofinqui-
ries
andtheiroutcomes
•Each
unitoftissuewill
haveauniqueidentifi-
ablecodeandbetrace-
ableto
thedonorwhile
protectingthedonor’s
anonymity.
should
bekept.
•Relatives
should
bein
form
edoftestingto
be
doneonthedonorandof
anypositiveresultsthat
mayhaverelevance
totheirhealth.
KEITH BAUER ET AL.116

•If
tissues
are
notusedfor
transplantation,explicit
consentfrom
donors
or
relatives
must
beobtained
touse
materialsforre-
search.
*•Relatives
shallspecifically
agreeto
letthetissuebank
seek
inform
ationabout
thedonorfrom
profes-
sionalssuch
astheGPor
pathologist.
Belgium
d•The
Crown
Order
of
June13,1986law
for-
bidsthesale
ofbody/
body
parts
and
profit
from
donation.
•The
Crown
Order
of
1986
states
that
confiden-
tialityofdonation
must
bemaintained
–an
onym
-ityap
plies
toboth
donor
and
recipient.
However,
theCrownOrderofApril
15,1988
man
dates
the
keeping
ofdetailed
re-
cordstrackingtheorigin,
processing,
andhan
dling
ofhuman
tissueas
away
toensure
traceabilityof
tissues.
•1986lawsupportsassumed
orpresumed
consent,stat-
ing
thatanyonewho
has
lived
inBelgium
formore
than
6monthsabove
the
ageofeighteen
isapoten-
tialdonor,
unless
express
proofofthatindividual’s
oppositionisavailable.
•Living
donors
may
with-
draw
theirconsentatany-
•1988lawad
dresses
issues
oftechnicalan
dmedical
quality,accreditationof
nonprofittissuebanks.
•No
mention
of
data
hoarding.
time.Close
relativesmay
offer
guidan
ceondonation
byafamilymem
ber
ifthat
mem
ber
isunab
leto
com-
municatehis/her
wishes.
ETHICAL ISSUES IN TISSUE BANKING 117

TABLE
I(C
ontinued)
Commercialization
Confidentiality
Inform
edConsent
Quality
Assurance
•Belgium
law
permitstissue
retrievalfrom
anydeceased
Belgianwhoresided
inthe
countryunless
thereis
ex-
pressed
oppositionagainst
it(e.g.,bythefamily).
EuropeanCommis-
sione
•EU
adheres
tothe
principlethatdonations
ofhumantissues
must
befree…andthisrules
outanypaymentto
the
donor(prevents
exploi-
tationofunderprivi-
leged).
•Rejects
claim
thatdo-
nors/familiesshould
be
paid
ifprofitismade
from
donatedtissues.
•Explicitstatementre-
spectingconfidentiality.
•Codingsystem
thatbal-
ancestraceabilitywith
confidentiality.
•Tissues
maynotbere-
moved
ifpersonrefused
consentduringhis/her
lifetime.
•If
therehasbeennoex-
pressionofwillandthe
applicable
system
isthat
•‘‘In
principle,tissue
bankactivitiesshould
bereserved
topublic
healthinstitutionsor
non-profit-makingor-
ganisations.In
such
cases,thismeansthat
thedeliveryprice
of
tissues
only
coversthe
bank’sexpensesrelating
tothetissues
inques-
tion.However,given
thecurrentstate
ofde-
velopmentofthesector,
itisdiffi
cultto
exclude
tissuebankingactivities
bycommercialorgani-
sations,such
asprivate
laboratories.’’
KEITH BAUER ET AL.118

•A
rightnotto
besub-
jected
tounfairtreatm
ent
whichcould
resultfrom
therevelationofcollected
data
tothirdparties(e.g.
employersandinsurance
companies).
of‘‘presumed’’consent,
doctors
must
ensure
asfar
aspossiblethatrelatives
or
nextofkin
havetheop-
portunityto
express
the
deceasedperson’swishes,
andmust
taketheseinto
account.
•Nomentionofdata
hoarding.
•Donor/familyhavearight
topriorinform
ationonthe
conditionsofremovaland
the
expected
use
of
the
tissue
and
likely
public
healthbenefits.
FDA/H
HS2001
Reportf
•Thetissuebankingin-
dustry
should
work
withgroupsrepresent-
ingdonorfamiliesto
explore
publicdisclo-
sure
oftissuebanks’
finances.
•Noexplicitmentionof
thesale
oftissues
for
profitorofsharing
profits
withfamilies.
•Thetissuebankingindus-
tryshould
work
with
groupsrepresentingdonor
familiesto
explore
public
disclosure
oftissuebanks’
finances.
•Requires
allorganiza-
tionsthatmanufacture
humancells,tissues,and
cellularandtissue-based
productsto
registerand
list
theirproductswith
theFDA.Thismeans
thattissueprocessors
anddistributors
‘‘should
ensure
thatin-
form
ationaccompany-
ingtheirproducts
clearlyindicate
itis
derived
from
donated
humantissue.’’
ETHICAL ISSUES IN TISSUE BANKING 119

TABLE
I(C
ontinued)
Commercialization
Confidentiality
Inform
edConsent
Quality
Assurance
•Thesenew
requirem
ents
willcreate
thefirst
complete
inform
ation
database
onthetissue
bankingindustry
inthe
US.
•Manytissuebankshave
never
beeninspectedby
thefederalgovernment.
Atiered
system
ofrules
andregulationswillbe
implementedwiththe
goalsof(1)preventing
thespreadofcommu-
nicable
diseasesand(2)
requiringthepre-m
ar-
ket
approvalofsome
tissue-relatedproducts.
No
mention
of
data
hoarding.
France
g•1994law
(94-654)em
-phasizesthatthedona-
tionprocess
(donor-
tissuebankrelation-
ship)should
benon-
commercial.However,
commercialism
isnotcompletely
ruled
out.
•Donors
ofeverytissue
must
beidentified
(for
trackingandpublic
healthprotections).
•1994law
supports
assumed
orpresumed
consentfordeceased
donors,withanoptingout
optionbyregisteringwith
nationalcomputerizedda-
tabase.
•1994law
addresses
is-
sues
oftechnicaland
medicalquality,accred-
itationofnonprofittis-
suebanks.
KEITH BAUER ET AL.120
•‘‘Publichealth
authori-
ties
ornonprofitorga-
nizationsserveastissue
banks,unless
theactiv-
ityatissueishighly
technical(orinvolves
private
sectorresearch
anddevelopment),
therebywarrantingspe-
cialpermissionforin-
terventionbya
commercialcompany.’’
•Ifdeceaseddid
notopt
out/register,more
recent
legislationstatesthat‘‘the
willingnessofthedeceased
todonate
should
besought
throughthefamily.’’
Livingdonors
mustgive
theirexplicitconsent.
•Nomentionofdata
hoarding.
Office
ofInspector
General/HSS2001
Reporth
•Thereport
recognizes
conflictbetweendonor
families’expectations
thatdonatedtissues
will
beusedformedically
indicatedpurposesthat
enhance
thelives
of
othersandthereality
of
tissuebankingwhichis
increasingly
becoming
commercializedand
viewshumantissueasa
commodity.Beyondin-
form
ationoftheusesto
whichtissues
willbe
put,noexplicitguide-
lines
onthe‘‘sale
of
bodypart’’are
recom-
mended
byHHS.
•Familiesshould
begiven
alist
anddescriptionof
other
companiesand
entities
withwhichthe
bankhasarelationship
forprocessinganddis-
tributingtissue.
•Tissuebanksshould
give
families(1)copyofsigned
consentform
,(2)written
materialonhow
tofollow
upwithtissuebankif
problem
arises,(3)afull
descriptionofusesto
whichtissues
maybeput,
(4)alistanddescriptionof
other
companiesandenti-
ties
withwhichthebank
hasarelationship
forpro-
cessinganddistributing
tissue.
•Aspart
offostering
accountability,tissue
banksshould
ensure
thatrequesters
ofhu-
mantissues/organsare
‘‘fullyandappropriately
trained’’and‘‘provide
continuingeducation
forrequestors.’’
ETHICAL ISSUES IN TISSUE BANKING 121
TABLE
I(C
ontinued)
Commercialization
Confidentiality
Inform
edConsent
Quality
Assurance
•‘‘Thetissuebankingin-
dustry
should
work
with
groupsrepresentingdo-
norfamiliesto
explore
aprocess
forperiodic
publicdisclosuresabout
tissuebanks’financing’’
asawayofresponding
tofamilyandthegen-
eralpublicconcerns
aboutknowingthe
sources
offundingfor
tissuebanksandother
entities
withwhichthe
bankhasfinancial
arrangem
ents.
•Noexplicitstatement
ondata
hoarding.
However,HHSin
an
effort
tofoster
greater
accountabilityrecom-
mendsthattissuebanks
‘‘conduct
anongoing
assessm
entofreques-
tor’sperform
ance
asa
meansofensuringthat
they
are
providingfull
andaccurate
inform
a-
tionto
familiesap-
proached
for
donation.’’Data
hoard-
ingcould
preventthis
from
happening.
UK
MedicalResearch
Councili
•Commercialcompanies
should
beallowed
ex-
clusive
accessto
data
(nottissuesamples)
for
asignificantperiodof
timeto
secure
patent
protectionandcompe-
titiveadvantage.
•When
possible,patient
identifiable
inform
ation
should
beanonymized
andidentifiable
health
inform
ationshould
only
beaccessible
tostaff
whohaveform
alduty
ofconfidence
todonors/
researchparticipants.
•MRC
rejectsblanket
con-
sentapproach
fortheuse
ofbiologicalsamples,but
supportsdonorconsentfor
abroaduse
forsamplesas
awayto
avoid
cumber-
someandcostly
process
of
obtainingconsentrepeat-
edly.
•Commercialcompanies
canhaveaccessto
bio-
logicalsamples,butno
exclusiveaccessto
sam-
plesispermissibleunless
MRC
andindustry
jointlyfundthere-
search.
•Thesaleofhumantissues
isnotconsidered
ethi-
callyacceptableand
should
belegally
prohibited.Thedonated
Donors
haverightto
know
whether
research
findingsaffects
them
or
familymem
bers.
KEITH BAUER ET AL.122

bodypart
ortissuesam-
ple
isa‘‘gift’’andnota
commodityforexchange
inthemarketplace.Sam-
plesare
given
tocompa-
nieswiththeaim
of
improvingthehealthof
citizens.
•Because
biologicalsam-
plesare
gifts
toresearch-
ers,they
oughtnotto
be
sold
andresearchers
oughtnotto
profit.
However,commercial
companies(e.g.,pharm
a-
ceuticals)canprofit.
•MRC
guidelines
apply
tolivingdonors.
Asa‘‘gift,’’donors
can
place
restrictionsontheuse
ofbiologicalsamples/can
specifywhatcanandcannot
bedone.
However,MRC
statesthatmanydonors
would
nothavesufficient
understanding(scientific)
of
whatresearchmightbepos-
sible
forthisto
bemean-
ingful.
Livingdonors
should
not
beoffered
monetary
in-
ducements
todonate.
•Generally,noprofits
will
goto
donors.
Spain
j•‘‘Thehumanbodyandits
partsshall
not,
assuch,
giverise
tofinancialgain.
Activities
and
expenses
related
tohandling
and
managem
entoftissues
as
wellassubstance
orother
•‘‘Theidentity
ofthedo-
nor
isnot
relevantto
research
purposesan
dis
protected
bytherigh
tto
confidence.Theprinciple
ofconfidence
isbased
on
naturalattributesofhu-
man
beings
and
•‘‘In
the
case
of
apost-
mortem
donor,
there
are
fiveoptions:(1)
‘‘Required
consentoropt-
ing
in’’
during
life
ofthe
potentialdonorwhich
must
beexpressed
byan
N/A
ETHICAL ISSUES IN TISSUE BANKING 123

TABLE
I(C
ontinued)
Commercialization
Confidentiality
Inform
edConsent
Quality
Assurance
materialusedin
theac-
quisitionandpreserva-
tionoftissues
are
able
tobeconsidered
asabudget
tobepaid
when
atissueis
required
forresearch.At
thesametime,
theactiv-
itiesofprofessional[s].
(technicians,MD
and
other
investigators)have
therightto
bereim
bursed
accordingto
theservices
carriedout,andthepro-
fessionalqualifications.’’
onthenature
ofhuman
relationships.Eachindi
vidualhas
therigh
tto
privacy
andconfiden-
tiality.’’
•‘‘Researchusinghuman
tissues
canbringnew
in-
form
ationab
outthedo-
nor.Thismay
occureven
wherethematerialisused
inwaysnotap
parently
relatedto
that
person’s
condition.T
hepossibility
ofnew
findings
ofsign
ifi-
cance
tothefamilymem
-bersfrom
whom
material
was
taken
should
playan
importan
tpartin
the
ethicalconduct.In
this
context
theacquired
confidence
withthedo-
normay
becomeirrele-
vantandthepossibilityto
inform
aboutnew
act
ofdonation.(2)‘‘Con-
tractingoutoroptingout,’’
meaningthedonornever
expressed
objectionto
organ
donationduringlife.Ac-
cordingto
thisconceptallof
usare
possible
donors.In
Spain,thelegislationaccepts
the2ndconcept.However,
inthebrain
bankin
Barce-
lona,acombinationofthe
required
consentwiththe
consentofrelatives
orin
casesofdeaddonors,the
consentofrelatives
isalways
required.
findingscould
betaken
into
account.TheCon-
ventiononHuman
Rights
andBiomedicine
hasestablished
that
everyonehastherightto
KEITH BAUER ET AL.124
privacy
regarding
their
health
condition.In
ex-
ceptional
cases
restric-
tionsmay
be
placed
by
law
ontheexercise
ofthe
mentioned
right.’’
Report
onUK
Tissue
Bankingin
theNHSk
•Donors
‘‘needto
be
inform
edparticularlyif
theresearchwillbe
commercial,andgiven
theopportunityto
con-
sentordeclineto
donate
when
inpossessionof
thefullfacts.’’Thefi-
nancesofUK
tissue
banksshould
besubject
tosomeform
ofexter-
nalaudit.
•Data
should
beanon-
ymized,butshould
re-
main
linked
because
unexpectedresearch
findingsmight
benefitfrom
further
detailsaboutthe
donor.
•Theuse
ofadoctorasa
‘‘medicalinterm
ediary’’
isrecommended
topro-
tect
thedonor’srightto
privacy
andconfidenti-
ality.
•Donors
‘‘needto
bein-
form
edparticularlyifthe
researchwillbecommer-
cial,andgiven
theoppor-
tunityto
consentordecline
todonate
when
inposses-
sionofthefullfacts.’’
Speciallydesigned
form
sthatem
ployachecklist
should
beuse
with
donors.
•Written
consentshould
be
obtained.
•Inform
ationpacket
should
beprovided
todonors.
Inform
ationaboutthesto-
rageanddisposaloftissue/
organsshould
begiven
todonors.
•‘‘Controlsoftheusers
ofmaterialsupplied
by
tissuebanksare
more
limited.However,safe-
guardscanbeintro-
ducedbylegalcontract
andinsistingthatdetails
ofproposedusesoftis-
sues
are
madeavailable
priorto
supply.’’
•In
casesofcadaveric
tissue
retrievals,thesesamein-
form
edconsentguidelines
apply
torelatives
ofde-
ceased.
ETHICAL ISSUES IN TISSUE BANKING 125
TABLE
I(C
ontinued)
Commercialization
Confidentiality
Inform
edConsent
Quality
Assurance
NationalBioethicsAd-
visory
Commissionl
N/A
•In
light
of
(Common
Rule45CFR46),NBAC
provides
differentrecom-
mendationsonthehand-
ling
oftissue
samples/
organ
sdepending
on
whether
they
comefrom
living
donors
and
are
being
used
inresearch,
‘‘…federal
legislation
concerning
medical
re-
cord
privacy
should
in-
clude
provisions
for
legitim
ate
accessby
re-
searcherswhohavemet
allapplicablereviewan
dconsentrequirem
ents.’’
•Recommendsmany
levels
ofconsentabout:(1)refu-
sal,(2)whether
biological
materials
willbe
identifi-
able
orcoded,(3)thetype
ofstudiesin
whichmateri-
als
willbe
used,and
(4)
risks.
•In
light
of
(Common
Rule45CFR46),NBAC
recommendsthatbefore
coded
and/oridentified
samplesare
released,a
repository
shouldrequire
investigators
requesting
samples
toeither:
(a)
provide
documentation
forrequester’sIR
Bthat
research
willfollow
ex-
istingfederal
guidelines;
or(b)explain
whytheir
research
isexem
ptfrom
those
regulations.
aAmericanAssociationofTissueBanks,McL
ean,Virginia,USA,URL:http://w
ww.aatb.org/guidelines.htm
(accessed2002Feb
22).
bAmericanMedicalAssociation,Chicago,IL
,USA,URL:http://w
ww.ama-assn.org/ama/pub/article/4301–4409.htm
l(accessed2002Feb
22).
cBritish
AssociationofTissueBanks,London,UK,URL:http://w
ww.batb.org.uk/eneral1.htm
(accessed2002Feb
22).
dB.Indech,‘‘TheInternationalHarm
onizationofHumanTissueRegulation:Regulatory
ControlOver
HumanTissueUse
andTissue
Bankingin
SelectCountriesandtheCurrentState
ofInternationalHarm
onizationEfforts,’’FoodandDrugLawJournal2000[55]:343.
eTheEuropeanGrouponEthicsin
Science
andNew
Technologies.
EthicalAspects
ofHumanTissueBanking,199821July,No.11,
URL:http://europa.eu.int/comm/european_group_ethics/docs/avis11_en.pdf(accessed2002Feb
22).
f DepartmentofHealthandHumanServices.Humancells,tissues,andcellularandtissue-basedproducts;establishmentregistrationand
listing.Washington,DC,FederalRegister200119Jan(66)13,URL:http://w
ww.fda.gov/cber/rules/frtisreg011901.pdf(accessed2002
Feb
22).
KEITH BAUER ET AL.126

gLaw
No.94-654.France
1994
July
29,URL:http://translate.google.com/translate?hl=
en&sl=
fr&u=
http://w
ww.m
ultim
ania.corn/
aedb/legislat/france/lois/l-94654.htm
&prev=
/search%
3Fq%
3D94-654%
2BFrance%
26hl%
3Den
(accessed2002Feb
22).
hDepartmentofHealthandHumanServices,Office
oftheInspectorGeneral.Inform
edconsentin
tissuedonation:expectationsand
realities.Washington,DC.2001Jan.OEI-01-00-00440.URL:http://w
ww.fda.gov/cber/tissue/infrmcnsnt.pdf(accessed2002Feb
22).
i MedicalResearch
Council.
UK
Human
tissue
and
biologicalsamplesforuse
inresearch.1999.URL:http://w
ww.m
rc.ac.uk/
pdf_tissue_guide_fin.pdf(accessed2002Feb
22).
j F.F.Sanchez,Emerging
ethicalissues
inbrain
banking.European
Commission,URL:http://w
ww.iprs.it/brainelsa/BACKUP_cd/
banks1-1ter.htm
(accessed2002Feb
22).
kC.Womack
andN.Gray,‘‘HumanResearchTissueBanksin
theUK
NationalHealthService:Laws,Ethics,ControlsandConstraints.’’
British
JournalofBiomedicalScience.2000March(57)1:250–253.
l NationalBioethicsAdvisory
Commission.Washington,DC,Draftreport
ontheuse
ofhumanbiologicalmaterials,1999May7,URL:
http://bioethics.georgetown.edu/nbac/briefings/may99/hbm_ch4.pdf(accessed2002Feb
22).
ETHICAL ISSUES IN TISSUE BANKING 127

research and support the training of researchers. Perhaps the mostimportant benefit associated with the commercialization of humantissue comes from the successful interchange between the two spheres,toward a more efficient transmission of knowledge from academic-based tissue banks to industry, facilitating the development anddelivery of medical products to the public.7
There is, however, a potential downside to the commercializationof human tissues. Specifically, the growth of for-profit tissue banksand augmented academic-industry partnerships increase the likeli-hood of conflicts of interests. For example, financial incentives toacademic researchers (e.g., stock options and royalties) couldundermine scientific standards of integrity by promoting secrecy, datahoarding, and even the manipulation of research outcomes. If thisoccurs, the commercialization of human tissues could have theunintended consequence of compromising human tissue research andsubordinating the health of the public to profit maximization.
Beyond concerns regarding conflicts of interests, the commercial-ization of human tissues also raises a host of broader social, cultural,religious, and psychological issues on the meanings we assign to thehuman body and, in particular, on how we treat it during life andafter death.8 Many people conceptualize the transfer of human or-gans and tissues during life or after death as a gift motivated byaltruistic feelings, not economic incentives. They believe that thebuying and selling of human biological samples debases the value ofhuman life, is antithetical to the gift paradigm of tissue transfer, canlead to further oppression of the disenfranchised and the poor, and isan affront to the dignity of donors and their families. Others, how-ever, point out that the commodification of human tissues is not new9
(e.g., blood and sperm), and that ‘‘it is virtually impossible to imaginehow human biological materials would be distributed if commerce insuch materials were prohibited.’’10 In fact, although U.S. federal lawprohibits the buying and selling of human organs, it does allow feesfor the recovering, processing and transporting of human tissue.11
The exportation of blood from the U.S. alone is a multi-billion dollarindustry;12 other human tissues such as hair and corneas play animportant role in commerce. Although the commodification of hu-man tissue is not completely novel, the potential for much greatercommercialization of human tissue does exist.
As illustrated in Table 1, the British Association of Tissue Bank-ing (BATB),13 Belgium,14 and Spain15 have adopted policies and lawsthat simply ban all commercial dealings in human tissues. The BATB,
KEITH BAUER ET AL.128

for example, states ‘‘there shall be no commercial dealing in humantissue,’’ the Spanish government holds that ‘‘the human body and itsparts shall not, as such, give rise to financial gain’’ and, as specified inThe Crown Order of June 13, 1986, the government of Belgiumsimply forbids the sale of body/body parts and profit from donation.The problem with this kind of approach is that it fails to specify whatcounts as a commercial activity and ignores or refuses to value thepotential benefits of such activity. The American Association ofTissue Banks (AATB)16 provides even less guidance, as it has noexplicit statement, general or specific, about the commercial aspectsof tissue banking.
Unlike the BATB and the AATB, two reports from the Health andHuman Services/Food and Drug Administration/Office of InspectorGeneral (HHS/FDA/OIG) provide guidelines that address some ofthe commercial aspects of tissue banking.17 As illustrated in Table 1,these agencies hold the view that ‘‘the tissue banking industry shouldwork with groups representing donor families to explore public dis-closure of tissue banks’ finances.’’ Although these reports do not goas far as endorsing commercialization, they do recommend that do-nors/families be informed in a general way of the commercial uses ofdonated tissues and that tissue banks disclose their financing, as wellas the industries with which they have financial arrangements.
Even if we grant that commercial academic-industry relationshipsare beneficial for spurring innovative research and providinghealthcare services and products to the public, there remains theunresolved issue of whether donors and families should be financiallycompensated for donated tissues and for any profits that are gener-ated by the research. The two HHS/FDA/OIG reports do not addressthis issue, but the policies developed by the European Commission(EC), the Medical Research Council (MRC),19 and France20 are ex-plicit in their rejection of financial compensation and profit sharingwith donors/families. There are two reasons why profit sharing withdonors/families is rejected. One reason, according to the MRC, isthat a donated body part or tissue sample is a ‘‘gift’’ and not acommodity for exchange in the marketplace. A second reason held bythe EC, the MRC, and France is that the introduction of financialincentives could lead to the exploitation of donors/families. Overall,however, the EC, MRC, and France do allow for limited partnershipswith industry. The MRC, for example, recommends that commercialcompanies receiving human tissues be allowed exclusive access todata for a period of time to secure patent protection and competitive
ETHICAL ISSUES IN TISSUE BANKING 129

advantage, whereas France recognizes that industry might at timeshave more resources to carry out highly technical human tissue re-search that will eventually benefit public health.
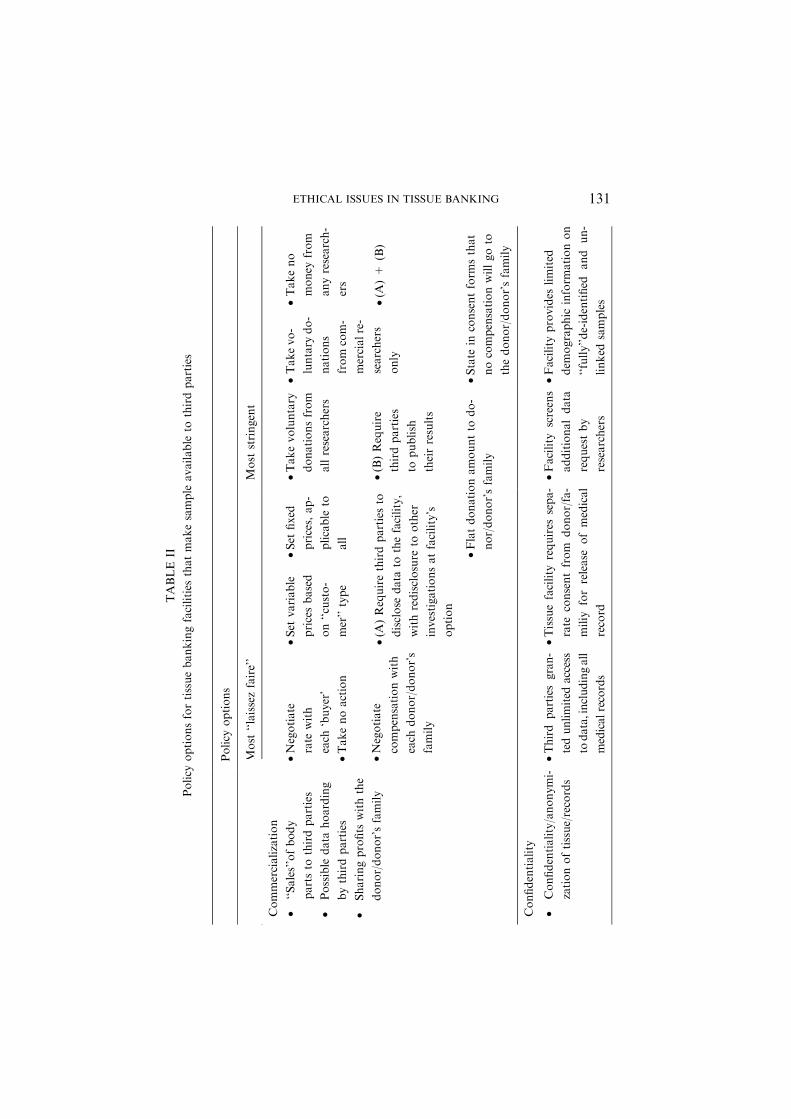
Still, all the policies but that of the AATB reflect an understandingof the most likely abuses associated with the commercialization ofhuman tissue. The spectrum of positions on the commercialization ofhuman tissues is represented in Table 2.
CONFIDENTIALITY
Confidentiality, which refers to the promise not to disclose infor-mation that the donor does not want disclosed, is treated by all theorganizations and countries that were surveyed as an important valueto be protected. Different levels exist among methods to curtailbreaches of confidentiality. Commentators have outlined a usefultaxonomy of:
• Identified: The tissue source is known and the individual’s identityis tied to the sample.
• Identifiable: The tissue source is tied to the specimen through theuse of a link (e.g., a code number), but the identity of the source isnot directly known without tracing the link.
• Anonymized: The tissue source’s identity is irrevocably unlinkedfrom the specimen, so that the individual’s identity cannot bediscerned (i.e., the tissue is not identifiable).
• Anonymous: The tissue source’s identity is never known, since thespecimen is collected with no identifiers at all (i.e., the sample isunidentified).21
Anonymity is achieved when tissue made available for research willnot have any personally identifiable links. This is one of the mosteffective ways to maintain confidentiality. However absolute confi-dentiality is nearly impossible to achieve in practice; nor is it alwayssought. Indeed, once tissue samples are anonymized, their potentialuses in research are diminished – findings associated with tissuesamples cannot be linked back to information regarding the samples’source of origin. On the other hand, linked specimens trigger the needfor IRB review to make certain human subjects are adequately pro-tected.22
The issue of whether tissues are stored as anonymized or identifiedspecimens requires attention. If the tissue is identified, the question
KEITH BAUER ET AL.130
TABLE
II
Policy
optionsfortissuebankingfacilities
thatmakesample
available
tothirdparties
Policy
options
Most
‘‘laissezfaire’’
Most
stringent
Commercialization
•‘‘Sales’’ofbody
partsto
thirdparties
•Possible
data
hoarding
bythirdparties
•Sharingprofits
withthe
donor/donor’sfamily
•Negotiate
rate
with
each
‘buyer’
•Takenoaction
•Set
variable
pricesbased
on‘‘custo-
mer’’type
•Set
fixed
prices,ap-
plicable
to
all
•Takevoluntary
donationsfrom
allresearchers
•Takevo-
luntary
do-
nations
from
com-
mercialre-
searchers
only
•Takeno
money
from
anyresearch-
ers
•(A
)Requirethirdpartiesto
disclose
data
tothefacility,
withredisclosure
toother
investigationsatfacility’s
option
•(B)Require
thirdparties
topublish
theirresults
•(A
)+
(B)
•Negotiate
compensationwith
each
donor/donor’s
family
•Flatdonationamountto
do-
nor/donor’sfamily
•State
inconsentform
sthat
nocompensationwillgoto
thedonor/donor’sfamily
Confidentiality
•Confidentiality/anonymi-
zationoftissue/records
•Third
parties
gran-
tedunlimited
access
todata,includingall
medicalrecords
•Tissuefacility
requires
sepa-
rate
consentfrom
donor/fa-
miliy
forrelease
ofmedical
record
•Facility
screens
additionaldata
requestby
researchers
•Facility
provides
limited
dem
ographic
inform
ationon
‘‘fully’’de-identified
and
un-
linked
samples
ETHICAL ISSUES IN TISSUE BANKING 131

TABLE
II(C
ontinued)
Policy
options
Most
‘‘laissezfaire’’
Most
stringent
Inform
edConsent
•Inform
edConsentof
Donor/Family
Opt-out/opt-in
provi-
sionsforcertain
usesof
material
•Minim
aland
blanket
consent
•Donors
cannotre-
strict
use
ofdona-
tions
•Donors
may
state
non-
bindingpre-
ference
foruse
oftissues
•Manylevals
ofspecifi-
city
•Comprehensive,
blanket
consent
(B)Donars
(A)Donors
canrestrict
use
oftissue
toresearch
onspecific
diseases
canrestrict
use
oftissue
tospecify
research
organization
•(A
)+
(B)
Quality
Assurance
•Ensuringquality
ofre-
searchthatissupported
•Handlingfinancial
conflicts
ofinterest
•Facility
gives
un-
limited
accessof
materialto
allwho
requestit
•Nodisclosure
or
avoidence
provi-
sions
•Facility
uses
aninternal
committeeto
review
con-
troversial
proposals
•Facility
usesanin-
ternalcom-
mitteeto
review
all
proposals
•Facility
usesan
externalcom-
mitteeto
review
controversial
proposal
•Facility
usesanin-
dependent,
external
committee
toreviewall
proposals
•Disclosure
financial
arrangments
topublic/do-
nors/family
•Lim
itfinancialinteractions
(Lim
ited
reim
bursem
ent,no
stock
options,etc…
)
•Nocompensation
orgifts
from
researchersor
organizations
KEITH BAUER ET AL.132

arises of whether researchers may access the donor’s medical records.If this will be permitted, safeguards must be put into place to protectthe donor’s (or donor’s family’s) confidentiality, even prior to theinformed consent process.
The BATB and the EC require coding systems that preserve bothtraceability and confidentiality. Within these policies, tissues are ei-ther identified or identifiable so that limited follow-up by authorizedparties remains possible (if, for instance, a donor wanted to knowabout the possibility of commercial profitability). Unlike the BATBand EC, Spain has specific language that states, ‘‘the identity of thedonor is not relevant to research purposes and is protected by theright to confidence.’’ Other organizations, including the UK’s MRCand the Report on UK Tissue Banking on NHS, use language such as‘‘should’’ rather than ‘‘must’’ in requiring anonymization.23 Some USorganizations have recently developed new policies that addressadequate safeguards for maintaining confidentiality at the level ofinformed consent and beyond. For instance, the AMA’s Code ofMedical Ethics recommends that the level of privacy be disclosed toresearch subjects (i.e., whether the biological material will be coded orcompletely de-identified).24 Finally, the FDA has recently promul-gated rules to regulate the tissue banking industry. All organizationsthat manufacture human cells, tissues, and cellular or tissue-basedproducts will have to register and list their products with the FDA.Moreover, the new Health Insurance Portability and AccountabilityAct of 1996 (HIPAA) regulations in the US prohibit disclosures of‘‘any protected health information related’’ to an individual’s tissuesamples.25 These new requirements will create the first comprehensivedatabase of tissues banked in the US. The resulting database is likelyto appeal to private and public entities for its research potential aswell as commercial opportunities, as well as to raise future privacyconcerns.
INFORMED CONSENT
Informed consent serves as a safeguard for individuals’ rights andwelfare, by providing them the opportunity to understand an inter-vention, its scope, and its implications, before they decide whether toagree to it. In the context of this discussion, the intervention is thecollection of tissue samples by a tissue storage facility for the purposeof research.
ETHICAL ISSUES IN TISSUE BANKING 133

What should the informed consent process for the collection oftissue samples include? This question pertains to tissue samples thathave yet to be collected. It needs to be distinguished from a relatedbut separate matter: What should be done with collected tissuesamples that were obtained with informed consent that would notmeet current standards? The latter question is not directly addressedin this paper, which concerns itself with the collection of tissue, exceptto say that the more rigorous alternative of going back to donors ordonors’ families to obtain consent for unanticipated uses is the goldstandard: it provides assurance that the donor’s wishes will be re-spected. Unless donors (or their families) understand the specificnature of a research protocol in which they are enrolling, they neithercan assess adequately whether participation in the overall investiga-tion is consistent with their values, nor freely and deliberately refuseparticipation in certain aspects of a study.
For the reasons described above, minimal blanket consent, as re-flected at one end of the spectrum in Table 2, is believed to be aninappropriate option for informed consent.26 A comprehensiveblanket consent, which tries to anticipate in detail every possible use,present and future, of a tissue sample, may be overly burdensome andstill may prove insufficient. The intermediary option offers a consentprocess that is tailored to the needs of the individual donor (or donorfamily) and to specific circumstances. The merit of the third optionis that it is more flexible than the other two. However, all threepolicy alternatives for informed consent address the items discussedbelow.
Collecting Tissue Samples: The Intervention
Standards of informed consent require that the donor (or donor’sfamily) have an adequate understanding of the procedure to retrievetissue, including its risks and benefits. How the tissue will be re-moved, how much of it will be removed, and how the procedure willmodify the appearance of the donor’s body are among the questionsthat should be addressed, as well as any physical risks associated withthe intervention in the case of a living donor.
Collected Tissue Samples: Anticipated Uses
Tissue storage facilities receive donations and make samples availableto investigators for research purposes. The donor (or donor’s family)may want to know whether the facility has ties with commercial, as
KEITH BAUER ET AL.134

well as non-commercial, companies. Does it stand to benefit finan-cially? What criteria does the facility use to determine to whom toprovide tissue samples? The party making the donation may be ableto limit or suggest to what sort of company the samples should beprovided. Along similar lines, the donor (or donor’s family) mighthave the opportunity to specify or recommend toward what type ofresearch the tissue may be used. The risk is that people with insuffi-cient scientific grounding will participate in complex research deci-sions and that they may request limits that are difficult, unfeasible, orimpossible to implement.
Findings from Research on Tissue Samples
It seems best to discuss at the time consent is sought what will laterbecome of information derived from tissue samples. Two majorquestions arise with regard to findings. Should they be communicatedto the donor (or donor’s family)? It may be feasible for the facility tocontact the donor (or donor’s family) with findings that pertain tothem, where the samples were identified. For this reason, it isimportant for potential donors to contemplate whether this isinformation they would welcome – and in what detail. Knowledgeregarding the risks and benefits associated with learning this sort ofinformation – and what it means that it is familial in nature – canhelp inform this decision. Where tissue samples are anonymized,general findings are the only kind of information the donor (or thedonor’s family) can consent to receive.
The other question that arises from the findings is whether thedonor (or donor’s family) can share in any profits from products,tests, or discoveries that result from the research. While it seemseasiest to preclude this sort of sharing, some organizations allow it.Details of how the donor (or the donor’s family) will benefit areworked out during the consent process. In these latter cases, it ishelpful to determine conditions as part of the informed consentprocess.
While the organizational policies that were reviewed all include adiscussion of consent, they reflect a broad range of standards. Severalof the European policies rely on notions of presumed consent fororgan and tissue retrieval from deceased individuals (Belgium,European Commission, France, and Spain), while British andAmerican policies stress informed consent with different levels ofspecificity.
ETHICAL ISSUES IN TISSUE BANKING 135

QUALITY OF RESEARCH
Tissue donors might well assume that their tissues will be used only tofurther research that is of the highest possible quality. But tissues arefrequently in greater demand than banks can supply, so allocationdecisions must be made. In this process, the presumption that onlythe highest quality research projects will receive tissues may be sub-verted by both organizational and personal conflicts of interest.Financial conflicts of interest pose immediate concerns. For example,if providing tissues to commercial researchers promises greaterfinancial rewards for the tissue bank, or its staff, there may be atemptation to provide tissue to these researchers even at the expenseof other, higher quality, research proposals from non-commercialsites. But not all potentially conflicting interests are financial. Re-
TABLE III
Definitions of key terms
Key terms Definitions
Human tissue Includes everything from organs and parts of organs, cells and
tissues to subcellular structures and cell products, blood,
gametes, embryos and fetal tissue, and waste. Also referred to
as ‘‘human biological material.’’
Renewable tissue Renewable tissue refers to tissue that the body produces and
replenishes on a regular basis. Such tissue includes hair, nails,
gametes and skin.
Non-renewable
tissue
Non-renewable tissue refers to tissue and organs that the body
does not replenish. Such tissues and organs include internal
organs such as liver and kidneys as well as corneas.
Tissue banking Tissue banking is the storage of tissue. Tissue is stored for
diagnostic procedures, surgical treatment, as well as educa-
tional and research purposes.
Tissue storage Tissue is stored in military facilities, forensic DNA banks,
government laboratories, diagnostic pathology and cytology
laboratories, university- and hospital-based research labora-
tories, commercial enterprises, and nonprofit organizations.
aC. Naser and S. Alpert, ‘‘Genetic Information, Ethics, Ethical Issues in TissueBanking and Human Subject Research in Stored Tissues,’’ in Encyclopedia of
Ethical; Legal; and Policy Issues in Biotechnology, eds. T.H. Murray and M.J.Mehlman (New York: Jon Wiley & Sons, 2000), pp. 363–369.
KEITH BAUER ET AL.136

search that is of particular interest to the bankers may receive specialconsideration, which may or may not be appropriate. A bankestablished to promote research in Alzheimer’s disease will rightfullygive priority to projects that directly address this condition, butwould it be appropriate for the director of the bank to refuse toprovide tissues to researchers in areas that compete with his or herown research?
To avoid the perception, or reality, of poorer quality researchtaking precedence over higher quality research for financial or otherinappropriate reasons, tissue banks can attend to issues such as whomakes allocation decisions, using what criteria, and under whatchecks and balances, with greater transparency. Unfortunately, theseissues were directly addressed in only five of the documents weexamined (AATB, BATB, HHS/OIG, Womack and Gray). Eventhese policies tended towards broad statements about preventingdiscrimination, maximizing research benefits, avoiding financialconflicts of interest, and ensuring that recipient scientists are trainedin the proper handling and use of donated tissues.
DISCUSSION
In light of our examination of representative tissue banking policies,we believe that tissue banks systematically should consider the fol-lowing requirements:
First, each tissue bank should have a mission statement, againstwhich it can assess the merits of proposed uses of donated tissue.Developing such a document will serve to provide a definition ofwhat constitutes high quality research in the eyes of the particularbank.
Second, financial conflicts of interest can be addressed, in part, byensuring that those making tissue allocation decisions do not havepersonal financial stakes in potential recipient organizations, or bysharply circumscribing such relationships. Table 1 lists a few of theways in which organizations have proposed limiting financial inter-actions between tissue banks, their officers and staff, and commercialor non-commercial enterprises. Except in the smallest of organiza-tions or where no shortage of tissues exists, no single person shouldhave control over allocation decisions. At minimum, there should bewritten criteria for evaluating proposed research projects; at best,there will be a clearly defined process for reviewing and approving the
ETHICAL ISSUES IN TISSUE BANKING 137

use of donated tissues, which will fall along the continuum outlined inTable 2.
Third, tissue banks should be explicit about their standards of‘‘confidentiality:’’ Are tissues identified, identifiable, anonymized, oranonymous? They should develop adequate methods to limit brea-ches of confidentiality, which are made known. Tissue bankingguidelines and policies need be specific about the conditions underwhich donated tissues will be deemed confidential. By doing so, tissuebanking guidelines will be more effective in minimizing potentialharms to donors, donor families, as well as to future tissue researchand product development.
Fourth, tissue banking guidelines and policies should specify whatinformation to address as part of the informed consent process. Todo this, tissue banks will already need to be clear about their mission,financial arrangements, and level of confidentiality protections theyintend to use. It is only after receiving the required information thatthe donor (or donor’s family) can arrive at an informed decisionabout whether to provide tissue samples to the facility. Toward thisgoal, the information to be addressed should be presented in clearand understandable language.
These four main requirements are meant to offer general guidanceregarding ethical considerations that deserve to be examined. Theyare neither exhaustive, nor absolute. Rather, they relate to the fourfactors (commercialization, confidentiality, informed consent, andquality of research) that emerged from the authors’ review. Institu-tional Review Boards, or corresponding bodies, the purview of whichis to ensure the protection of research participants, must be involvedto aid tissue banks by providing appropriate oversight and moni-toring of their activities that relate to research, as well as assistancewith specific ethical issues as they arise.
CONCLUSION
Some organizational policies do not address commercialization, whileothers fail to consider confidentiality and quality of research. How-ever, even in those instances where one of the four factors is recog-nized by all policies (commercialization, confidentiality, informedconsent, and quality of research), there is often a lack of uniformity inits meaning, scope, and ethical significance. Until uniform ethicalguidelines regulating the storage, distribution, and use of human
KEITH BAUER ET AL.138

tissues for research are established, the international transfer of hu-man tissues and multinational research involving industry will notonly remain cumbersome but, in many instances, ethically problem-atic. We propose that governments, non-governmental organizations,and other institutions further collaborate and harmonize policiesregarding human tissue, keeping in mind the four factors we outlinehere.
ACKNOWLEDGEMENTS
We thank Matthew Wynia, MD, MPH for suggesting the idea behindthis article and for providing some conceptual foundations during itsearly development. We also thank Elisa Gordon, PhD, Erin Egan,MD, JD, and Robert Mittendorf, MD, DrPh, for their commentsand suggestions.
NOTES
1 Deborah Josefson, ‘‘Human Tissue for Sale: What Are the Costs?’’ WesternJournal of Medicine 5 (2000): 302–303.2 Ted T. Ashburn, Sharon K. Wilson, Barry I. Eisenstein, ‘‘Human Tissue Researchin the Genomic Era of Medicine: Balancing Individual and Societal Interests,’’ Ar-chives of Internal Medicine 160 (2000): 3377–3384. See also, generally, Robert F.Weir, ed., Stored Tissue Samples: Ethical, Legal, and Public Policy Implications (Iowa
City: University of Iowa Press, 1998).3 See Table 3 for a list of definitions regarding human tissue. For the purposes ofthis paper, we generally exclude organs from the definition of tissue. Moreover,
‘‘donor’’ in this paper means both living and deceased individuals.4 Joseph B. Martin, Dennis L. Kasper, ‘‘In Whose Best Interest? Breaching theAcademic-Industrial Wall,’’ New England Journal of Medicine 343 (2000): 1646–
1649.5 Deborah Josefson, ‘‘US Hospitals to Ask Patients for Right to Sell their Tissue,’’British Medical Journal 321 (2000): 653.6 The authors identified these four factors in the early stages of their research, whenconsidering whether and under what conditions non-profit academic brain tissuerepositories should provide for-profit private companies with brain tissue samples ofdeceased individuals.7 John P. Swan, Academic Scientist and the Pharmaceutical Industry (Baltimore: TheJohn Hopkins University Press, 1988).8 Dorothy Nelkin, Lori Andrews, ‘‘Homo Economicus: Commercialization of Body
Tissue in the Age of Biotechnology,’’ Hastings Center Report 28 (1998): 30–39.9 Linda F. Hogle, Recovering the Nation’s Body: Cultural Memory;Medicine; and thePolitics of Redemption (New Brunswick, NJ: Rutgers University Press, 1999): 24.
ETHICAL ISSUES IN TISSUE BANKING 139

10 Julia D. Mahoney, ‘‘The Market for Human Tissue,’’ Virginia Law Review March,
86 (2000): 163–223.11 National Organ Transplant Act, 1984. Pub L. No. 98–507, 3 USC *301.12 Danielle M. Wagner, ‘‘Property Rights in the Human Body: The Commerciali-
zation of Organ Transplantation and Biotechnology,’’ Duquesne Law Review, 33(1995): 931–958.13 British Association of Tissue Banking, ‘‘General Standards for Tissue Banking,’’
(Sept 29, 1999). Available at: http://www.batb.org.uk/general1.htm.14 Barbara Indech, ‘‘The International Harmonization of Human Tissue Regulation:Regulatory Control over Human Tissue Use and Tissue Banking in Select Countries
and the Current State of International Harmonization Efforts,’’ Food and LawJournal, 55 (2000): 343–372.15 F.F. Cruz-Sanchez, ‘‘Emerging Ethical Issues in Brain Banking,’’ EuropeanCommission financed Ethical, Legal, and Social Aspects of Brain Research (1997).
Available at: http://www.iprs.it/brainelsa/BACKUP_cd/banks1-1ter.htm.16 American Association of Tissue Banks, ‘‘Ethical Guidelines for CommercialActivities and Advertising,’’ (Sept. 11, 1996). Available at: http://www.aatb.org/
guidelines.htm.17 Department of Health and Human Services, ‘‘Human Cells, Tissues, and Cellularand Tissue-Based Products; Establishment Registration and Listing,’’ Federal Reg-
ister 66 (Jan. 19, 2001): Rules and Regulations. Available at: http://www.fda.gov/cber/rules/frtisreg011901.pdf.18 European Group on Ethics in Science and New Technologies to the European
Commission, ‘‘Ethical Aspects of Human Tissue Banking,’’ 11 (July 21, 1998).Available at: http://europa.eu.int/comm/european_group_ethics/docs/avis11_en.pdf.19Medical Research Council Working Group to Develop Operational and Ethical
Guidelines, ‘‘Human Tissue and Biological Samples for Use in Research,’’ (April2001). Available at: http://www.mrc.ac.uk/pdf-tissue_guide_fin.pdf.20 See note 15, above.21 Curtis Naser and Sheri Alpert, ‘‘Genetic Information, Ethics, Ethical Issues inTissue Banking and Human Subject Research in Stored Tissues,’’ in: Encyclopedia ofEthical; Legal; and Policy Issues in Biotechnology, eds. T.H. Murray and M.J. Me-
hlman (New York: John Wiley & Sons, 2000), p. 365.22 Naser, Alpert cited in n. 21, above, p. 367.23 Christopher Womack, Neil Gray, ‘‘Human Research Tissue Banks in the UKNational Health Service: Law, Ethics, Controls and Constraints,’’ British Journal of
Biomedical Science 55 (2000): 250–253.24 ‘‘Opinion 2.079: Safeguards in the Use of DNA Databanks in Genomic Re-search,’’ in Council on Ethical and Judicial Affairs, American Medical Association,
Code of Medical Ethics: Current Opinions with Annotations (Chicago, IL: AMAPress, 2002).25 Department of Health and Human Services, Office of the Secretary, ‘‘Standards
for Privacy of Individually Identifiable Health Information,’’ 45 CFR Parts 160through 164. See http://www.cms.hhs.gov/hipaa/hipaa2/regulations/privacy/final-rule/PvcTxt01.asp.
KEITH BAUER ET AL.140

26 Henry T. Greely, ‘‘Breaking the Stalemate: A Regulating Framework for
Unforeseen Research Uses of Human Tissue Samples and Health Information,’’Wake Forest Law Review, 34 (1999): 737–766.
REFERENCES
American Association of Tissue Banks. ‘‘Ethical Guidelines for Commercial Activ-ities and Advertising.’’ (September 11, 1996). Available at: http://www.aatb.org/
guidelines.htm.Ashburn, T.T., S.K. Wilson, and B.I. Eisenstein. ‘‘Human Tissue Research in the
Genomic Era of Medicine: Balancing Individual and Societal Interests.’’ Ar-chives of Internal Medicine 160 (2000): 3377–3384.
British Association of Tissue Banking. ‘‘General Standards for Tissue Banking.’’(September 29, 1999). Available at: http://www.batb.org.uk/general1.htm.
Council on Ethical and Judicial Affairs, American Medical Association. Code of
Medical Ethics: Current Opinions with Annotations. Chicago, IL: AMA Press,2002.
Cruz-Sanchez, F.F. ‘‘Emerging Ethical Issues in Brain Banking.’’ European Com-
mission financed Ethical; Legal; and Social Aspects of Brain Research, 1997.Available at: http://www.iprs.it/brainelsa/BACKUP_cd/banks1–1ter.htm.
Department of Health and Human Services, Office of the Secretary. ‘‘Standards for
Privacy of Individually Identifiable Health Information.’’ 45 CFR Parts 160through 164. Available at: http://www.cms.hhs.gov/hipaa/hipaa2/regulations/privacy/finalrule/PvcTxt01.asp.
Department of Health and Human Services. ‘‘Human Cells, Tissues, and Cellular
and Tissue-Based Products; Establishment Registration and Listing.’’ FederalRegister 66 (January 19, 2001): Rules and Regulations. Available at: http://www.fda.gov/cber/rules/frtisreg011901.pdf.
European Group on Ethics in Science and New Technologies to the EuropeanCommission. ‘‘Ethical Aspects of Human Tissue Banking.’’ 11 (July 21, 1998).Available at: http://europa.eu.int/comm/european_group_ethics/docs/avi-
s11_en.pdf.Greely, H.T. ‘‘Breaking the Stalemate: A Regulating Framework for Unforeseen
Research Uses of Human Tissue Samples and Health Information.’’ Wake
Forest Law Review 34 (1999): 737–766.Hogle, L.F. Recovering the Nation’s Body: Cultural Memory; Medicine; and the
Politics of Redemption. New Brunswick, NJ: Rutgers University Press, 1999.Indech, B. ‘‘The International Harmonization of Human Tissue Regulation: Regu-
latory Control over Human Tissue Use and Tissue Banking in Select Countriesand the Current State of International Harmonization Efforts.’’ Food and LawJournal 55 (2000): 343–372.
Josefson, D. ‘‘Human Tissue for Sale: What Are the Costs?’’ Western Journal ofMedicine 5 (2000): 302–303.
Josefson, D. ‘‘US Hospitals to Ask Patients for Right to Sell Their Tissue.’’ British
Medical Journal 321 (2000): 653.Mahoney, J.D. ‘‘The Market for Human Tissue.’’ Virginia Law Review 86 (2000):
163–223.
ETHICAL ISSUES IN TISSUE BANKING 141

Martin, J.B., and D.L. Kasper. ‘‘In Whose Best Interest? Breaching the Academic-
Industrial Wall.’’ New England Journal of Medicine 343 (2000): 1646–1649.Medical Research Council Working Group to Develop Operational and Ethical
Guidelines. ‘‘Human Tissue and Biological Samples for Use in Research.’’ (April
2001). Available at: http://www.mrc.ac.uk/pdf-tissue_guide_fin.pdf.Murray, T.H., and M.J. Mehlman, eds. Encyclopedia of Ethical; Legal; and Policy
Issues in Biotechnology. New York: John Wiley and Sons, 2000.
National Organ Transplant Act, 1984. Pub L. No. 98–507, 3 USC *301.Nelkin, D., and L. Andrews. ‘‘Homo Economicus: Commercialization of Body
Tissue in the Age of Biotechnology.’’ Hastings Center Report 28 (1998): 30–39.
Swan, J.P. Academic Scientist and the Pharmaceutical Industry. Baltimore: The JohnHopkins University Press, 1988.
Wagner, D. ‘‘Property Rights in the Human Body: The Commercialization of OrganTransplantation and Biotechnology.’’ Duquesne Law Review 33 (1995): 931–958.
Weir, R.F., ed. Stored Tissue Samples: Ethical; Legal; and Public Policy Implications.Iowa City: University of Iowa Press, 1998.
Womack, C., and N. Gray. ‘‘Human Research Tissue Banks in the UK National
Health Service: Law, Ethics, Controls and Constraints.’’ British Journal ofBiomedical Science 55 (2000): 250–253.
KEITH BAUERDepartment of PhilosophyMarquette UniversityU.S.A
SARA TAUBEthics Standards GroupAmerican Medical AssociationChicago, ILU.S.AE-mail: [email protected]
KAYHAN PARSINeiswanger Institute for Bioethics and Health PolicyStritch School of MedicineLoyola University ChicagoU.S.A
KEITH BAUER ET AL.142