
Ethical Controversies in Clinical Anesthesia: Exploring ...
113
Ethical Controversies in Clinical Anesthesia: Exploring the Issues D. John Doyle MD PhD Professor of Anesthesiology Cleveland Clinic 2014
Transcript of Ethical Controversies in Clinical Anesthesia: Exploring ...

Ethical Controversies in Clinical Anesthesia: Exploring the Issues
D. John Doyle MD PhDProfessor of Anesthesiology
Cleveland Clinic2014




A woman is unconscious as a result of hypovolemic shock following a motor vehicle accident. The patient has a signed (but undated and unwitnessed) wallet card indicating that sheis a Jehovah's Witness and does not want to receive blood transfusions under any circumstances. However, without blood she will almost certainly die. Given that the wallet card is incompletely filled out, what should be done?
Malette v. Shulman.



Hippocrates

"To consider dear to me as my parents him who taught me this art; to live in common with him and if necessary to share my goods with him; to look upon his children as my own brothers, to teach them this art if they so desire without fee or written promise; to impart to my sons and the sons of the master who taught me and the disciples who have enrolled themselves and have agreed to the rules of the profession, but to these alone the precepts and the instruction. I will prescribe regimens for the good of my patients according to my ability and my judgment and never do harm to anyone. To please no one will I prescribe a deadly drug nor give advice which may cause his death. Nor will I give a woman a pessary to procure abortion. But I will preserve the purity of my life and my art. I will not cut for stone, even for patients in whom the disease is manifest; I will leave this operation to be performed by practitioners, specialists in this art. In every house where I come I will enter only for the good of my patients, keeping myself far from all intentional ill-doing and all seduction and especially from the pleasures of love with women or with men, be they free or slaves. All that may come to my knowledge in the exercise of my profession or in daily commerce with men, which ought not to be spread abroad, I will keep secret and will never reveal. If I keep this oath faithfully, may I enjoy my life and practice my art, respected by all men and in all times; but if I swerve from it or violate it, may the reverse be my lot."
HIPPOCRATIC OATH
I swear by Apollo the physician, by Æsculapius, Hygeia, and Panacea, and I take to witness all the gods, all the goddesses, to keep according to my ability and my judgment, the following Oath.

… to impart to my sons and the sons of the master who taught me and the disciples who have enrolled themselves and have agreed to the rules of the profession, but to these alone the precepts and the instruction.
HIPPOCRATIC OATH
I swear by Apollo the physician, by Æsculapius, Hygeia, and Panacea, and I take to witness all the gods, all the goddesses, to keep according to my ability and my judgment, the following Oath.

To please no one will I prescribe a deadly drug nor give advice which may cause his death. Nor will I give a woman a pessary to procure abortion.
HIPPOCRATIC OATH
I swear by Apollo the physician, by Æsculapius, Hygeia, and Panacea, and I take to witness all the gods, all the goddesses, to keep according to my ability and my judgment, the following Oath.

I will not cut for stone, even for patients in whom the disease is manifest; I will leave this operation to be performed by practitioners, specialists in this art.
HIPPOCRATIC OATH
I swear by Apollo the physician, by Æsculapius, Hygeia, and Panacea, and I take to witness all the gods, all the goddesses, to keep according to my ability and my judgment, the following Oath.

In every house where I come I will enter only for the good of my patients, keeping myself far from all intentional ill-doing and all seduction and especially from the pleasures of love with women or with men, be they free or slaves.
HIPPOCRATIC OATH
I swear by Apollo the physician, by Æsculapius, Hygeia, and Panacea, and I take to witness all the gods, all the goddesses, to keep according to my ability and my judgment, the following Oath.

There are many versions of the Hippocratic oath. The following representative example appears in the Columbia Encyclopedia:
You do solemnly swear, each man by whatever he holds most sacred, that you will be loyal to the profession of medicine and just and generous to its members; that you will lead your lives and practice your art in uprightness and honor; that into whatsoever house you shall enter, it shall be for the good of the sick to the utmost of your power, you holding yourself far aloof from wrong, from corruption, from the tempting of others to vice; that you will exercise your art solely for the cure of your patients and will give no drug, perform no operation, for a criminal purpose, even if solicited, far less suggest it; that whatsoever you shall see or hear of the lives of men which is not fitting to be spoken, you will keep inviolably secret. These things do you swear. Let each man bow the head in sign of acquiescence. And now, if you will be true to this, your oath, may prosperity and good repute be yours; the opposite, if you shall prove yourselves forsworn.
http://media.hoover.org/images/digest20042_alper.jpg




Some Ethical Issues in Medicine• Conflicts of interest• Referral to laboratories• Vendor relationships• Treatment of family members• Inappropriate relationships with patients• Futile care issues• Cultural concerns• Truth-telling and disclosure• Lying for the patient’s benefit• What risks should health care
workers be willing to countenance? • Working while impaired• Research ethics

Some Ethical Issues in Anesthesiology
• Research ethics• Conflicts of interest • Vendor relationships• Gifts• Futile care• Resource allocation• DNR orders in the OR• Cultural concerns• Truth-telling and
disclosure• Working while impaired
• Dating residents• Teaching invasive
procedures• Abortions• Patient refusal of clinically
appropriate / necessary procedures
• Ethical conflicts with surgeons
• Brain death / organ harvesting
• Participation in judicial executions

Some Ethical Issues in Anesthesiology
• Research ethics• Conflicts of interest • Vendor relationships• Gifts• Futile care• Resource allocation• DNR orders in the OR• Cultural concerns• Truth-telling and
disclosure• Working while impaired
• Dating residents• Teaching invasive
procedures• Abortions• Patient refusal of clinically
appropriate / necessary procedures
• Ethical conflicts with surgeons
• Brain death / organ harvesting
• Participation in judicial executions


Some Ethical Issues in Anesthesiology
• Research ethics• Conflicts of interest • Vendor relationships• Gifts• Futile care• Resource allocation• DNR orders in the OR• Cultural concerns• Truth-telling and
disclosure• Working while impaired
• Dating residents• Teaching invasive
procedures• Abortions• Patient refusal of clinically
appropriate / necessary procedures
• Ethical conflicts with surgeons
• Brain death / organ harvesting
• Participation in judicial executions

Samkoff JS, Jacques CH. A review of studies concerning effects of sleep deprivation and fatigue on residents' performance. Acad Med. 1991 Nov;66(11):687-93.
Possible effects of sleep deprivation and fatigue on the performance and well-being of residents have received little scientific examination until recently. This article is a review of the studies on this topic published since 1970. All those studies that dealt with residents' moods and attitudes demonstrated deleterious effects of sleep deprivation and fatigue. The implications of this finding for patient care deserve exploration. Residents' acuity on performance tests requiring prolonged vigilance tended to deteriorate with acute sleep loss, while their performances on most brief psychomotor tests measuring manual dexterity, reaction times, and short-term recall were not adversely affected. The data presently available suggest that sleep-deprived or fatigued house officers can compensate for sleep loss in crises or other novel situations. However, sleep-deprived residents may be more prone to errors on routine, repetitive tasks and tasks that require sustained vigilance, which form a substantial portion of residents' workload. The authors concur with the recommendation of the Executive Council of the Association of American Medical Colleges that the total working hours for residents should not exceed 80 hours per week averaged over four weeks.

Seven Principles That Apply to Medical Ethics
• Beneficence - a practitioner should act in the best interest of the patient.
• Nonmaleficence - "first, do no harm“. • Autonomy - the patient has the right to refuse or
choose their treatment. • Justice - concerns the fair distribution of scarce
health-care resources. • Dignity - the patient (and the person treating the
patient) have the right to dignity. • Truthfulness and honesty• Informed consent
Advance Directive
• An advance directive (“living will”) is a declaration by a competent adult on how he wishes to be treated should he become incompetent and unable to make valid choices.
• An advance directive cannot request treatment that is not in the interests of the patient.
• Advance directives are legally binding.

Durable Power of Attorney for Healthcare
A Durable Power of Attorney for Healthcareis a document that designates who should make medical decisions on your behalf if you are unable to do so. It is sometimes part of an Advance Directive.
In a DPOA you (the “principal”) give someone you trust ( your “agent” or “attorney-in-fact”) the legal authority to act on your behalf when you are unable to make decisions.

What should we do with DNR orders in the OR?
• In 1992, the ASA produced “Guidelines for the Ethical Care of Patients with Do Not Resuscitate Orders”
• It requires a discussion with the patient to determine medical procedures under anesthesia to which the patient would consent.
• Patients do not lose their right to self-determination under anesthesia, and policies that automatically suspend DNR orders in the OR are ethically unsound.
• Rediscussion of the DNR order should occur, where possible, prior to surgery and anesthesia.
http://www.asahq.org/publicationsAndServices/standards/09.pdf



http://i1280.photobucket.com/albums/a485/ComfortGroom/420-medical-tattoosimgcacherev1338995949961_zps9a8b706d.jpg
http://blog.passare.com/wp-content/uploads/2013/10/ Passare-DNR-1.jpeg
http://www.whatwhenwhy.net/wp-content/uploads/2012/05/medical-tattoo-3.jpg
http://media.winnipegfreepress.com/images/cpt607031122_high.jpg

http://www.kaiserhealthnews.org/~/media/Images/KHN%20Features/2011/August/29%202/DNR512.jpg

http://i.dailymail.co.uk/i/pix/2011/09/07/article-2034647-0DC0856A00000578-114_233x423.jpg
http://www.cambstimes.co.uk/polopoly_fs/photo4_1_1_1017632!image/971057381.jpg_gen/derivatives/landscape_630/971057381.jpg
Pathologist Dr. Ed Friedlander of Kansas City, Mo. displays his tattoo with a medical directive to not use CPR. http://i.i.cbsi.com/cnwk.1d/i/tim/2012/02/27/AP110929079090_1_620x350.jpg

http://blog.passare.com/wp-content/uploads/2013/10/Passare-DNR-1.jpg

http://farm3.static.flickr.com/2791/4279010949_ab13c6a2bd.jpg

http://www.hollyzood.com/wp-content/uploads/2011/05/cryonics-tattoo.jpghttp://kriorus.ru/sites/default/files/styles/alcor-dewar2.jpg

http://0.tqn.com/d/create/1/0/O/x/1/-/cropped-tattoo.jpg

http://4.bp.blogspot.com/-ZxVfRPi8bO4/UDHCOqwSdBI/AAAAAAAACFg/rvmxvVXVI14/s1600/DNR+DNI.JPG

Seven Principles That Apply to Medical Ethics
• Beneficence - a practitioner should act in the best interest of the patient.
• Nonmaleficence - "first, do no harm“. • Autonomy - the patient has the right to refuse or
choose their treatment. • Justice - concerns the fair distribution of scarce
health-care resources. • Dignity - the patient (and the person treating the
patient) have the right to dignity. • Truthfulness and honesty• Informed consent

Principalism
• Beneficence - a practitioner should act in the best interest of the patient.
• Nonmaleficence - "first, do no harm“. • Autonomy - the patient has the right to
refuse or choose their treatment. • Justice - concerns the fair distribution of
scarce health-care resources.

Autonomy
Autonomy - the patient has the right to refuse or choose their treatment.
Autonomy usually trumps the other principles when dealing with competent adult Western patients.

http://www.trinity.edu/cbrown/intro/ethicsOverview.gif
Ethical Theories

Virtue Ethics
Virtue ethics describes the character of a moral agent as a driving force for ethical behavior, rather than rules (deontology) or consequentialism, which derives rightness or wrongness from the outcome of the act itself rather than character.

ConsequentialismConsequentialism refers to those moral theories which hold that the consequences of one's conduct are the true basis for any judgment about the morality of that conduct. Thus, from a consequentialist standpoint, a morally right act (or omission) is one that will produce a good outcome, or consequence. This view is often expressed as the aphorism "The ends justify the means".

UtilitarianismUtilitarianism is the idea that the moral worth of an action is determined solely by its usefulness in maximizing utility and minimizing negative utility (utility can be defined as pleasure minus pain, preference satisfaction, knowledge or other things) as summed among all sentient beings. It is thus a form of consequentialism, meaning that the moral worth of an action is determined by its outcome. The most influential contributors to this theory are considered to be Jeremy Bentham and John Stuart Mill.

http://www.papermasters.com/images/utilitariaism.jpg

UtilitarianismUtilitarianism was described by Bentham as "the greatest happiness or greatest felicity principle". Utility, the good to be maximized, has been defined by various thinkers as happiness or pleasure (versus suffering or pain), although preference utilitarians define it as the satisfaction of preferences. It may be described as a life stance, with happiness or pleasure being of ultimate importance.

http://www.phil.cmu.edu/Cavalier/80130/part1/sect4/images/Bentham.gif

Deontological EthicsDeontological ethics or deontology (from Greek δέον, deon, "obligation, duty"; and -λογία, -logia) is an approach to ethics that judges the morality of an action based on the action's adherence to a rule or rules (e.g., Kant’s Categorical Imperitive). Deontologists look at rules and duties.

Example: LyingA consequentialist may argue that lying is wrong because of the negative consequences produced by lying — though a consequentialist may allow that certain foreseeable consequences might make lying acceptable.
A deontologist might argue that lying is always wrong, regardless of any potential "good" that might come from lying.
A virtue ethicist would focus less on lying in any particular instance and instead consider what a decision to tell a lie or not tell a lie said about one's character and moral behavior. As such, lying would be made in a case-by-case basis that would be based on factors such as personal benefit, group benefit, and intentions (as to whether they are benevolent or malevolent).
Example 1 – Nazis looking for Jews (Anne Frank Story)
Example 2 – “Dr. Jones is an excellent surgeon, isn’t he?”

http://socrates.berkeley.edu/~kihlstrm/images/MoralJudgment2011/09TrolleyProb.JPG
The Trolley Problem


http://socrates.berkeley.edu/~kihlstrm/images/MoralJudgment2011/10ProbDat.JPG


http://keithburgess-jackson.com/wp-content/uploads/2007/10/ethics-flowchart.JPG

Case One

Case OneMr. S is a 73-year-old man, with a history of severe coronary artery disease, peripheral vascular disease, and stroke. He suffers from right hemiplegia and mild expressive aphasia. He is awake and alert, and presents for right below the knee amputation (BKA) for vascular insufficiency. His chart carries a DNR order. In the holding area prior to surgery, the anesthesiologist discusses the DNR order with Mr. S, who appears depressed.
http://depts.washington.edu/bioethx/topics/dnrauc1.html

Case OneMr. S states unequivocally, that he does not wish CPR in the OR, regardless of its cause or positive prognosis. He tells his anesthesiologist that he is willing to go "so far, and no more." The patient agrees to subarachnoid anesthesia (spinal block) and sedation. He is not intubated. After about 20 minutes, the patient complains of weakness in his arms, and difficulty breathing. Within 3 minutes, his blood pressure and heart rate fall, and he abruptly arrests. Should the patient be intubated? Should CPR be commenced?http://depts.washington.edu/bioethx/topics/dnrauc1.html
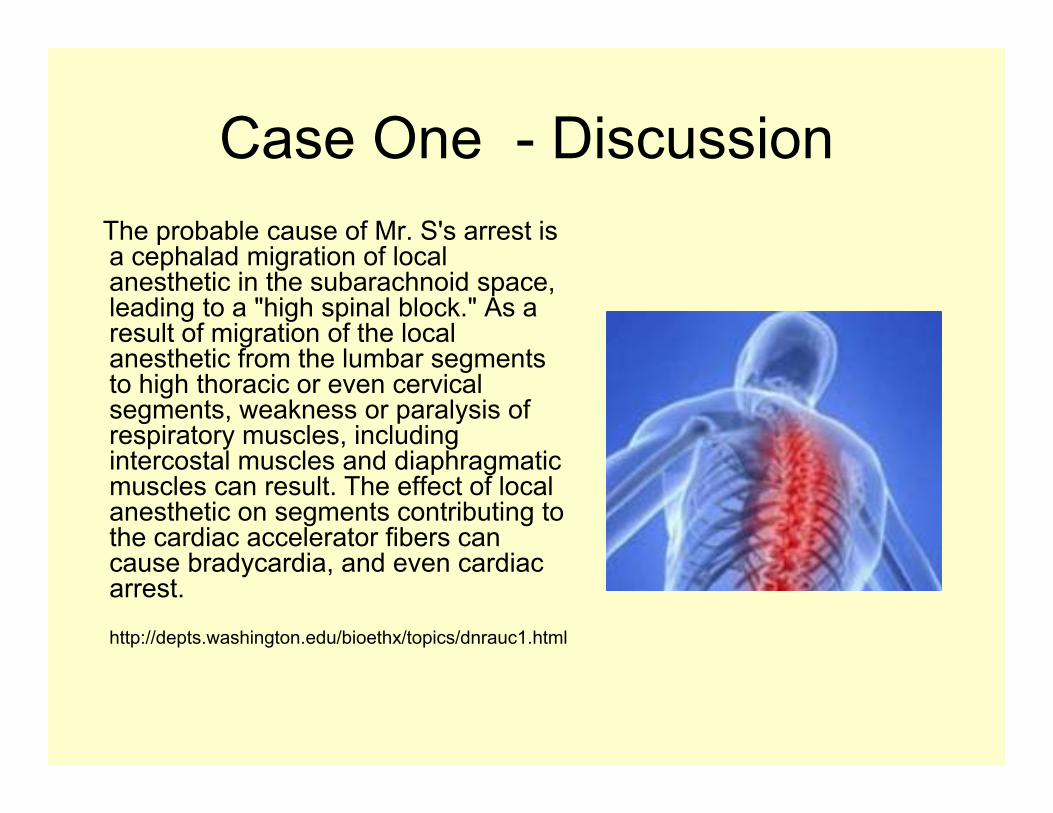
Case One - DiscussionThe probable cause of Mr. S's arrest is a cephalad migration of local anesthetic in the subarachnoid space, leading to a "high spinal block." As a result of migration of the local anesthetic from the lumbar segments to high thoracic or even cervical segments, weakness or paralysis of respiratory muscles, including intercostal muscles and diaphragmatic muscles can result. The effect of local anesthetic on segments contributing to the cardiac accelerator fibers can cause bradycardia, and even cardiac arrest.
http://depts.washington.edu/bioethx/topics/dnrauc1.html

Case One - DiscussionWith cardiopulmonary support, prognosis for total recovery from this event is excellent, with only rare cases of central nervous system damage or death reported. CPR would not be futile from a medical standpoint. Intubation and institution of mechanical ventilation will not alone restore Mr. S's circulation, and these measures alone will be useless. Medications to treat blood pressure and bradycardia will require at least temporary artificial circulation. From the standpoint of medical futility, intubation and mechanical ventilation would be senseless unless accompanied by full CPR, if even briefly.
http://depts.washington.edu/bioethx/topics/dnrauc1.html

Case One - DiscussionIt is hard to argue ethically for the institution of CPR in this patient, who while neurologically impaired, appeared to have full capacity to understand and make decisions regarding his own medical care. Despite preoperative discussion which included information about the good prognosis from CPR in the OR, the patient stated clearly his wishes to not be resuscitated if an arrest occurs. Instituting CPR in this patient because the cause of arrest is anesthetic-related, would be like justifying transfusion in a Jehovah's Witness against their will because the surgery was the cause of life-threatening hemorrhage, yet adhering to their wishes if hemorrhage was due to non-surgical injuries.
http://depts.washington.edu/bioethx/topics/dnrauc1.html

Case Two

The Case of Dr DeBakey
At 98, DeBakey is the oldest survivor of his own operation (Feb 2006).


The Case of Dr DeBakey
• Oldest person ever to have open surgery for ascending aortic tear.
• Anesthesiology team faced an dilemmas regarding consent and advance directive issues.

The Case of Dr DeBakey
“DeBakey himself did not want the operation. He did not check into the hospital for nearly a month. After he did, he had a DNR order on his chart and a progress note that indicated he did not want surgery for the dissecting aortic aneurysm. How, then, did he get the surgery (and the continuous resuscitation that went along with the surgery), apparently against his wishes?”
http://healthlawblog.blogspot.com/2006/12/debakeys-surgery.html

Heroic Measures Extend Life of Surgical Pioneer and Stir Debate
By Neil Osterweil, Senior Associate Editor, MedPage Today January 05, 2007…..
For example, although he had a "do not resuscitate" order (which he later could not recall having made) and a note in his chart stating that he did not want surgery, and although anesthesiologists at the Methodist Hospital refused initially to put him under because of those directives, the demands of his family and the judgment of his physicians overrode Dr. DeBakey's wishes.
From http://www.medpagetoday.com/Surgery/GeneralSurgery/tb/4808

Heroic Measures Extend Life of Surgical Pioneer and Stir Debate
By Neil Osterweil, Senior Associate Editor, MedPage Today January 05, 2007…..
Then there are the questions about the patient's age --just three years shy of the century mark when he was wheeled into the operating suite -- and the wisdom of expending so many medical resources to buy so little extra time.
In a letter to the Times, a Rhode Island physician suggested that Dr. DeBakey's medical team put their reverence and affection for the patient and the wishes of his family ahead of the express wishes of Dr. DeBakey himself.
From http://www.medpagetoday.com/Surgery/GeneralSurgery/tb/4808

Referring to a Jehovah’s Witness case
"Such a stay must easily have cost a six figure sum. Here in Uganda for £250.000 we can treat 25 000 outpatients and 7000 inpatients, conduct over 1000 deliveries, and perform 1500 operations. We run a community health programme for 500 000 people. The costs incurred by this one patient might run our unit for a whole year. Will the time come when a religious group will be charged the costs of keeping its members alive? Ethically one may feel that one should do everything, whatever the cost; at the end of the financial year, however, elective surgery that could be life improving has to be cancelled. The choice is easy here in Uganda. When a child who has severe anaemia from malaria with hookworm infestation and undernutrition comes in the choice is simple: he or she has a transfusion or dies."
Wooding N. Costs incurred by one severely ill Jehovah's Witness could run one unit in Africa for one year. BMJ 1999; 318:873

Case Three

The Jehovah’s Witness Patient

Jehovah’s Witnesses• There are about six million Jehovah’s Witnesses world-
wide, with approximately one million in the USA. • Traditionally, orthodox Jehovah’s Witnesses will not
accept homologous or autologous whole blood, packed red blood cells, plasma, platelets and white blood cells, even when “clinically necessary”.
• This can result in a challenging dilemma for physicians because a routine, safe, and potentially life-saving medical intervention is unacceptable to the patient.

Jehovah’s Witnesses
• Witnesses view Jehovah as the ultimate moral authority and do not salute flags, join service organizations, enlist in the military, vote in public elections, or take an interest in civil government.
• In sharp contrast to most other Christian religions they also do not believe in the concept of the trinity or the usual Christian concept of heaven and hell.
• Jehovah's Witnesses base their religious beliefs on a strict literal interpretation of the Bible and hold that eternal life may be forfeited if they do not exactly follow biblical commands.

Jehovah’s Witnesses
Jehovah’s Witnesses believe that Jesus did not die on a cross but on an upright pole.

• cannot salute the flag, stand for the national anthem, or own a flag
• cannot vote in any political campaign• cannot buy Girl Scout cookies• cannot be a cheerleader• cannot celebrate any holidays (Christmas,
Easter, etc.)• cannot own or wear a cross• cannot accept Christmas gifts• cannot speak to former members who are
shunned (disfellowshipped)
Jehovah’s Witnesses ...


Blood Transfusions• Jehovah's Witnesses believe that the biblical
injunctions concerning blood include both animal and human blood, and that the transfusion of blood is tantamount to "eating" blood.
• Even the use of autologous blood predonated in preparation for surgery is prohibited, as are transfusion of any of the “primary” blood components (red cells, white cells, platelets and plasma), regardless of their source.

Blood TransfusionsThe determination that blood transfusions were a violation of God's law was made in 1945 and is primarily based on the following three biblical passages:
• "Every moving animal that is alive may serve as food for you. As in the case of green vegetation, I do give it all to you. Only flesh with its soul -- its blood -- you must not eat." (Genesis 9:3, 4)
• "As for any man of the house of Israel or some alien resident who is residing as an alien in their midst who eats any sort of blood, I shall certainly set my face against the soul that is eating the blood and I shall indeed cut him off from his people." (Leviticus 17:10-16)
• "The Holy Spirit and we ourselves have favored adding no further burden to you, except these necessary things, to keep abstaining from things sacrificed to idols and from blood and from things strangled and from fornication. If you keep yourselves from these things you will prosper." (Acts 15:28,29)

"The blood in any person is in reality the person himself. ... poisons due to personal living, eating and drinking habits ... The poisons that produce the impulse to commit suicide, murder, or steal are in the blood.”
--Watchtower, September 1, 1961, Page 564

"Moral insanity, sexual perversions, repression, inferiority complexes, petty crimes...often follow in the wake of blood transfusion."
--Watchtower, September 1, 1961, Page 564

Blood Transfusions• Note that despite their refusal to accept transfusions,
contemporary Jehovah’s Witnesses are not against modern medical care. (This was not always true – at various times vaccinations and organ transplants have been outlawed by the church).
• For the most part, Jehovah’s Witnesses are informed health care consumers whose only “anomaly” in their care plan is their refusal to receive blood or blood products. As such, they seek out competent health care providers who will zealously respect their wishes.

Blood Components and Procedures Usually Accepted and Usually Refusedby Jehovah's Witness Patients
Modified from Kaaron Benson, MDManagement of the Jehovah's Witness Oncology Patient: Perspective of the Transfusion ServiceCancer Control: Journal of the Moffitt Cancer Center 1995;6:552-556.http://www.moffitt.usf.edu/pubs/ccj/v2n6/article13.html
Usually Refused Whole bloodErythrocytesPlateletsFresh frozen plasmaCryoprecipitateGranulocytesPredeposited autologous blood
Usually Accepted Normovolemic hemodilution*Intraoperative red blood cell salvage*Erythropoietin**Hemodialysis***Cardiopulmonary bypass***Veno-veno bypass***
IndividualDecision
(“ConscienceItem”)
AlbuminImmune globulinsFactor concentratesOrgan and tissue transplants
* Usually accepted if patient remains continuously in contact with blood.** Synthetic hormone frequently suspended in albumin.*** Provided that a non-blood prime is used.


Awake, May 1994
Front cover illustration of dead children who refused blood

Legal Issues
• Legal issues concerning the medical care of Jehovah's Witnesses often center on patient consent.
• In Canada and the USA, a patient's legal right to refuse or consent to treatment is based on common law and, as such, is in a state of continuous evolution as new cases are decided.

Malette v. ShulmanIn Canada, the landmark legal case regarding the clinical care of Jehovah's Witness patients was the case of Malette v. Shulman.
This case centered on the matter of patient autonomy. The courts established that clinicians should not administer emergency treatment without consent if they have reason to believe that the patient would refuse such treatment if he or she were capable.
In this 1979 case, Dr. Shulman administered a blood transfusion to a patient who was unconscious as a result of hypovolemic shock. The patient carried a signed (but undated and unwitnessed) wallet card indicating that she was a Jehovah's Witness and did not want to receive blood transfusions under any circumstances.
Despite this, blood was transfused out of clinical necessity. Although the transfusions were almost certainly responsible for saving the patient's life, the court found the clinician liable for battery. The judge stated: “To transfuse a Jehovah's Witness in the face of her explicit instructions to the contrary would, in my opinion, violate her right to control her own body and show disrespect for the religious values by which she has chosen to live her life.”
Legal IssuesA particularly unusual case occurred in Pomona, California where a drunken driver rammed his truck into a stationary car, injuring a 55 year old Jehovah’s Witness standing by the side of the road.
She refused a clinically necessary blood transfusion and died.

Legal IssuesProsecutors said the driver was responsible for the death because he caused the injuries and he was convicted of manslaughter. His lawyers argued that the immediate cause of the woman’s death was her refusal of a blood transfusion, since she very likely would have lived had a blood transfusion been carried out.
(Driver got 10 years.)

Blood Management Policies for Jehovah’s Witnesses
Summarized from: Richard K. Spence MD FACS, Surgical Red Blood Cell TransfusionPolicies. The American Journal of Surgery Dec 1995 Vol 170, No. 6A (Suppl)(Results of a Clinical Consensus Conference)
1. Accept the limitation that allogeneic blood cannot be used.
2. Use alternatives to allogeneic blood whenever possible andappropriate.
3. Discuss consequences with the patient, including the potentialfor life-threatening hemorrhage and possible death if nottransfused.
4. If unable or unwilling to treat a Jehovah’s Witness patient,stabilize and transfer the patient to a sympathetic institution, suchas a Center for Bloodless Surgery.

Blood Management Policies for Jehovah’s WitnessesSummarized from: Richard K. Spence MD FACS, Surgical Red Blood Cell Transfusion Policies. The AmericanJournal of Surgery Dec 1995 Vol 170, No. 6A (Suppl) (Results of a Clinical Consensus Conference)
5. Contact the local Jehovah’s Witness liaison committee forinformation and help.
6. In an emergency or if a patient is unconscious, look for an advancedirective.
7. Seek legal assistance when dealing with an unconscious orincompetent adult.

Case Four

Physician Participation in Judicial Executions



"We have enormous protections, the best by far, but we're never going to have a system that will never execute an innocent person."
Statement of Chairperson of the US House of Representatives Judiciary Committee made while supporting the death penalty in 1997.


Physicians and Capital Punishment
Physicians have traditionally shied away from any involvement with capital punishment, seeing themselves as healers and comforters rather than as assassins.
In particular, some physician codes of ethics explicitly forbid any physician involvement in capital punishment.

Physicians and Capital Punishment
The philosophical basis for this position is that physicians are entrusted by society to work for the benefit of their patients and for the benefit of society at large, and that this trust is destroyed when medical expertise is used to facilitate judicial executions.

On 6 November 2001, 45 year old prison inmate Jose High was led into a room at the Georgia Diagnostics and Classification Center in Jackson, Georgia, United States. The room would have looked familiar to a surgeon (or any doctor who performs procedures under sedation): it contained a trolley; cardiac monitor and defibrillator; medical equipment cabinets (including one for storing drugs); equipment stand; and the standard catheters, tubing, and sterile saline bags used to start intravenous lines. High lay down on the trolley, and a nurse tried to start a peripheral intravenous line.
From J. I Groner. Lethal injection: a stain on the face of medicine. BMJ, November 2, 2002; 325(7371): 1026 - 1028

For more than 30 minutes, the nurse made several attempts to start the line at various locations, including High's right hand, right arm, right leg, and right foot. Finally, a doctor who worked under contract with the Georgia Diagnostics and Classification Center stepped in to help. He inserted a 7 French gauge, triple lumen, 20 cm long, central venous catheter into High's right subclavian vein. After the prison warden gave a signal, technicians injected thiopental sodium 6 g, pancuronium bromide 150 mg, and potassium chloride 360 mEq into High; this ended his life.
From J. I. Groner. Lethal injection: a stain on the face of medicine. BMJ, November 2, 2002; 325(7371): 1026 - 1028

Dr Guillotin was among the first doctors to advocate the use of technology to achieve more "humane" executions. Of interest, Guillotin was opposed to the death penalty, and saw his proposal as a step in the path towards the abolition of capital punishment. While a member of the Constituent Assembly Dr. Guillotin proposed that the French develop a uniform method of execution that would replace less humane methods in use at the time, such as hanging, burning, mutilation, and drowning.

In 1871 hangman William Marwood introduced the "long drop" method of hanging which it is thought had been invented by doctors in Ireland. It removed most of the prisoner's physical suffering and made the whole process far less traumatic for the officials who now had to witness it in the confines of the execution cell instead of in the open air. The long drop method was designed to break the prisoners' neck by allowing them to fall a pre-determined distance and then be brought up with a sharp jerk by the rope. [http://www.geocities.com/Hollywood/Studio/3015/ldrop.htm]

Drop distance is based on prisoner's weight and is critical for clean neck snap and instant death. Botched hangings were instrumental in developing more "humane" alternative methods of execution.
The problem with hanging is that the drop length, hence the rope length, is critical. The desired result requires 1260 ft.-lb. of force to snap the neck. If the drop is too short, the victim strangles–a horrific episode that can last up to 15 minutes. Too long a drop risks decapitation–an equally unappetizing event.
To calculate the correct drop length (in feet), the equation is 1260 divided by the victim's weight.

Left: The gas chamber once used at San Quentin State Prison in California has been converted to use for lethal injection. Image credit: http://upload.wikimedia.org/wikipedia/en/2/2e/Gaschamber.jpg
Right: Electric Chair at Sing Sing Prison in Ossining, New York.Image credit: http://www.geh.org/taschen/m197400560386.jpg



American Medical Association Council on Ethical and Judicial Affairs
“A physician, as a member of a profession dedicated to preserving life when there is hope of doing so, should not be a participant in a legally authorized execution. Physician participation in execution is defined generally as actions which would fall into one or more of the following categories:
(1) an action which would directly cause the death of the condemned;
(2) an action which would assist, supervise, or contribute to the ability of another individual to directly cause the death of the condemned;
(3) an action which could automatically cause an execution to be carried out on a condemned prisoner.”

American Medical Association Council on Ethical and Judicial Affairs
“Physician participation in an execution includes, but is not limited to, the following actions: prescribing or administering tranquilizers and other psychotropic agents and medications that are part of the execution procedure; monitoring vital signs on site or remotely (including monitoring electrocardiograms); attending or observing an execution as a physician; and rendering of technical advice regarding execution.”

American Medical Association Council on Ethical and Judicial Affairs
“In the case where the method of execution is lethal injection, the following actions by the physician would also constitute physician participation in execution: selecting injection sites; starting intravenous lines as a port for a lethal injection device; prescribing, preparing, administering, or supervising injection drugs or their doses or types; inspecting, testing, or maintaining lethal injection devices; and consulting with or supervising lethal injection personnel.”

CounterpointLet me make it clear: I am opposed to the death penalty. But the fact remains that the death penalty does still exist in this country. I understand that certain physicians want nothing to do with the executions that result from this policy. But, on the other hand, one of the duties, and desires, of a physician is to provide comfort and relieve pain and suffering. While capital punishment is legal, capital torture is not. I feel that we have a duty, once someone has been ordered executed, to ensure that the execution takes place in as "humane" a fashion as possible. The records are ripe with stories of botched executions. Once we have made the ignominious decision to end a convict's life, we have a huge responsibility to bring this event about in as "efficient" a manner as possible, and that is where the role of the physician comes in.
Enthusiasm for that role is not required, but I just do not see how physicians can walk away from what is, albeit unfortunately, a dirty job that somebody has to do.
[Jack F. Hildebrand, California, USA 95624]http://bmj.bmjjournals.com/cgi/eletters/325/7371/1026#27584

A more practical and humane method of execution might be to use a hood such as that illustrated here, and deliver pure nitrous oxide to the hood via the hose at the lower right. Nitrous oxide delivered in this concentration will lead to painless unconsciousness in a few minutes, but since no oxygen is being administered it will also lead to profound hypoxia and cardiac arrest in a short period following the onset of unconsciousness. Such an approach avoids the need to establish intravenous access needed for the lethal injection process, adding considerable simplicity and reliability to the execution process. In addition, only one pharmacologic agent need be administered in this setting, as opposed to the three intravenous agents used in the traditional lethal injection process.

Time for Discussion


















