Estimation of the Burden of Cancer in Great Britain due to ... · 1 Dept. of Epidemiology and...
32
Estimation of the Burden of Cancer in Great Britain due to Occupation L Rushton 1 , T. Brown 2 , R Bevan 3 , J Cherrie 4 , L Fortunato 1 , S Bagga 3 , P Holmes 3 , S Hutchings 1 , R Slack 3 , M Van Tongeren 4 , C Young 2 1 Dept. of Epidemiology and Public Health, Imperial College London; 2 Health and Safety Laboratory, Buxton, Derbyshire 3 Institute of Environment and Health, Cranfield University 4 Institute of Occupational Medicine This study was funded by the Health and Safety Executive
Transcript of Estimation of the Burden of Cancer in Great Britain due to ... · 1 Dept. of Epidemiology and...

Estimation of the Burden of Cancer in Great Britain due to Occupation
L Rushton1, T. Brown2, R Bevan3, J Cherrie4, L Fortunato1, S Bagga3, P Holmes3, S Hutchings1, R Slack3, M Van Tongeren4, C Young2
1 Dept. of Epidemiology and Public Health, Imperial College London; 2 Health and Safety Laboratory, Buxton, Derbyshire3 Institute of Environment and Health, Cranfield University4 Institute of Occupational Medicine
This study was funded by the Health and Safety Executive

Aims of the study
• Aims of the study:– to develop and apply methodology to estimate current
attributable risk, cancer numbers and DALYs caused by work– to identify important cancer sites– to identify industries and occupations for targeting for reduction
measures– To estimate the future occupational cancer burden in GB under
different scenarios of changing exposure
• Selection of carcinogens and occupations for estimation: – classified by IARC as group 1 (established) and 2A (probable)
carcinogens– with strong or suggestive evidence of carcinogenicity in humans– 24 cancer sites; 42 carcinogenic agents or occupations; over
100 industry sectors

Measure of Burden• Measure of burden used is the AF - proportion of cases
attributable to exposure; needs– risk of disease associated with the exposure of concern (e.g.
relative risk (RR))– proportion exposed in the population
• RR from published literature: meta-analyses, pooled studies, narrative reviews where available
• Selected studies with comparable exposures to GB:– Large sample size– Clear case definition– Appropriate comparison population– Controlled for confounders where possible– Adequate exposure assessment
• Risk estimates obtained for overall ‘higher’ level of exposure and lower/background exposure

Estimating the Proportion Exposed• To take into account latency (length of time before
disease risk increases) we defined the risk exposure period (REP) for:– Solid tumours: 10-50 years; 1956-95– Leukaemia: up to 20 years; 1986-2005
• Proportion exposed over the REP is:number ever exposed/number ever worked
• Estimated using national data sources (CAREX, LFS, CoE)
• Adjusted for turnover, change in numbers employed over REP

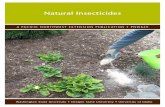
Trends in employment structure in Great Britain, based on Labour Force
Survey data from 1975 to 2007 and projected to 2025, men
0
4,000
8,000
12,000
16,000
20,000
1975
1980
1985
1990
1995
2000
2005
2010
2015
2020
2025
Year
Empl
oym
ent (
'000
)
Agriculture, Hunting and Forestry, FishingMining, Manufacturing, Electricity, gas and water supplyConstructionService sectorTotal

Attributable Numbers and DALYs
• Apply AFs to total nos. of site-specific cancer deaths and registrations to give attributable nos. of deaths and registrations for each carcinogen (ANs)
• AFs and ANs give no idea of the relative ‘costs’ to an individual or society of an occupationally caused cancer
• Apply AFs to measures of:a. Years of life lost (YLL)b. Years lived with a disability (YLD)
• Combine to give DALY• DALYs are a measure of something lost – future years
of life and future years lived without severe mental or physical disability

Cancer Site AF (%) Deaths (2005) Registrations (2004)
M F Total M F Total M F Total
Mesothelioma 97.0 82.5 95.0 1699 238 1937 1699 238 1937
Sinonasal 46.0 20.1 34.4 29 10 39 101 32 133
Lung 21.1 5.3 14.5 4024 726 4749 4632 816 5477
Nasopharynx 11.0 2.5 8.2 7 1 8 14 2 16
Bladder 7.1 1.9 5.3 215 30 245 496 54 550
Breast 4.6 4.6 555 555 1969 1969NMSC 7.1 1.1 4.6 21 2 23 2576 352 2928
Larynx 2.9 1.6 2.6 17 3 20 50 6 56
Oesophagus 3.3 1.1 2.5 156 28 184 159 29 188
STS 3.4 1.1 2.4 11 3 13 22 4 27Stomach 3.0 0.3 2.0 102 6 108 149 9 158
NHL 2.1 1.1 1.7 43 14 57 102 39 140Melanoma (eye)
2.9 0.4 1.6 1 0 1 6 1 6
Total 8.2 2.3 5.3 (4.6, 6.6)
6362 1657 8019 (6891, 9983)
10063 3616 13679 (9310, 20235)

Carcinogen or Occupation Total Registrations Cancer Sites
Asbestos 4216 Larynx, Lung, Mesothelioma, Stomach
Shift work (+ Flight Personnel) 1957 Breast
Mineral oils 1730 Bladder, Lung, NMSC, Sinonasal
Solar radiation 1541 NMSC
Silica 907 Lung
Diesel engine exhaust 801 Bladder, Lung
PAHs - Coal tars and pitches 545 NMSC
Painters 359 Bladder, Lung, Stomach
Dioxins 316 Lung, NHL, STS
Environmental Tobacco Smoke (non-smokers) 284 Lung
Radon 209 Lung
Welders 175 Lung, Melanoma (eye)
Tetrachloroethylene 164 Cervix, NHL, Oesophagus
Arsenic 129 Lung
Strong inorganic-acid mists 122 Larynx, Lung
Chromium 89 Lung, Sinonasal
Non-arsenical insecticides 73 Brain, Leukaemia, Multiple myeloma, NHL

Steel foundry workers
Tin miners Mineral oils Welders
Radon
Haematitemining
Hairdressers & Barbers
Ionisingradiation
ETS
Nickel
ChromiumArsenicArt glass
Cadmium
Dioxin
Nonarsenical insecticides
Acid mists
Painters
Silica
Diesel
PAHs *
BCCM CMME
Isopropyl alc.
Epichlorohydrin
αCT & BC
Construction
Stainless steel
Smelting/RefiningAlloys/Plating
Batteries Pesticide Sprayers
Drivers
Asbestos
Personal &Household Services
Metal machinists
ConstructionQuarriesPottery
Beryllium
MetalsMetals
Talc containing asbestiform fibres
Paper
Paints
Coal‐tar and pitchesAlluminium production
Coal gasificationCoke production
Soot
Foundries/ Steel mills
Cobalt
Lead
Mining
Rubber Industry
Shipbuilding
Dyes/pigments

Arsenic
Asbestos
Beryllium
Cadmium
Chromium IV
Cobalt
Diesel engine exhaust
ETS
Inorganic lead
Ionising radiation
Mineral oils
Nickel
PAHs
Painters
Radon
Silica
Steel foundry workers
Strong inorganic‐acid mistsContaining sulphuric acid
TCCD
Tin miners
Welders
Lung cancer AF by carcinogen/occupation

Industry Sector Attributable RegistrationsMale Female
Exposures
Construction 4752 64 14
Painter + decorators 331 3 1
Roadmen + roofers 538 3 1
Total construction 5621 71 16
Shift work (including flight personnel) 0 1970 1
Metal workers 1081 169 1
Personal + household services 274 530 17
Land Transport 436 43 9
Mining 285 17 10
Printing, publishing and allied trades 225 34 10
Public administration and defence 239 34 6
Wholesale + retail trades 110 159 11
Farming 180 39 5
Welders 165 16 2
Manufacture of instruments, etc 204 16 6
Manufacture of transport equipment 170 18 16
Non-ferrous metal basic industries 125 34 18

Cancer Registrations Attributable to Work in the Construction Industry ‐Men
0 500 1000 1500 2000 2500 3000 3500 4000
ArsenicAsbestosChromium
CobaltDieselETS
FormaldehydeLead
PaintersPAH
PAH ‐ coal tarsand pitches
RadonSilica
Solar RadiationTetrachloroethylene
Wood dust
Carcinogen
Number of Registrations
Construction, inc painters anddecorators; road surfacers,roadmen, roofers & glazers, paviours
Other Sectors

500 1000 1500 2000 2500
Registrations
Bladder
Larynx
Lung
Mesothelioma
Nasopharynx
NMSC
Oesophagus
Sinonasal
Stomach
Attributable Registrations by Cancer Site forWork in the Construction Industry: Men

YLLs and YLDs for cancer due to occupation, men, excluding lung cancer + mesothelioma
0 500 1,000 1,500 2,000 2,500 3,000
BladderBoneBrain
BreastCervixKidneyLarynx
LeukaemiaLiverLH
Melanoma_eyeMultiple Myeloma
NasalNasopharynx
NHLOesophagus
OvaryPancreas
NMSCSTS
StomachThyroid
Years
YLLs
YLDs ‐uncured
YLDs ‐cured

YLLs and YLDs for cancer due to occupation, women, excluding breast and lung cancer and mesothelioma
0 50 100 150 200 250 300 350 400 450
BladderBoneBrainCervixKidneyLarynx
Leukaemia (all) Liver
LymphohaematopoieticMelanoma_eye
Multiple MyelomaNasal
NasopharynxNHL
OesophagusOvary
PancreasNMSC
Soft Tissue SarcomaStomachThyroid
Years
YLLsYLDs –non‐survivors
YLDs ‐survivors

Cancer Site YLL (years)
Deaths (2005) Average YLL (years)
DALY (years)
Bladder 2543 245 10.4 3110Brain 222 11 20.2 232Breast 9600 555 17.3 13797Cervix 156 7 22.3 195Larynx 290 20 14.5 414Leukaemia 407 24 17.0 442Lung 62913 4749 13.2 66080Mesothelioma 26942 1937 13.9 27738
Nasopharynx 158 8 19.8 183
NHL 964 57 16.9 1029
NMSC 208 23 9.0 277
Oesophagus 2528 184 13.7 2691
Ovary 383 23 16.7 418
Sinonasal 652 39 16.7 2691
STS 296 13 22.8 336
Stomach 1331 108 12.3 1460
Total 109810 8019 13.7 119491

Predicting Future Burden
• AFs estimated for forecast years, e.g. 2010, 2020 … 2060
• Define the risk exposure period (REP) for each year e.g. for 2030, 1971 – 2020
• Assume latencies are distributed lognormally across the REPs
• Some past and some future exposure.
• Workers at the beginning assumed to be of all working ages
• Workers recruited through employment turnover are assumed to be only aged 15-24
• Methods being applied to ‘important’ carcinogens/occupations identified from current burden results

20602020
1971‐80 2001‐101981‐90 1991‐00
Risk Exposure Periods Forecast Target Years20502030 2040
2021‐302011‐20 2031‐40 2041‐50
2010
1961‐70
10 year estimation intervals
‘Known’ exposure Forecast exposure
Forecast Risk Exposure Periods – 10‐50 year latency

Possible change scenarios• No change in exposure levels or patterns (baseline)• Linear employment and exposure level trends assumed to 2021‐
30, constant thereafter• Test time of introduction of a reduced or new limit (silica,
tetrachloroethylene, TCDD, arsenic)• Test ‘dynamic exposure standard’ that reduces as forecast levels
are expected to fall and previous intervention standards take effect
• Test compliance by workplace size• Test effect of introducing lower exposure standards versus
compliance rate • Test effect of closing industries, reducing exposed numbers
(asbestos, radon), transferring high/medium exposed workers to low exposed (solar radiation), and lowering RR (painters, welders)

Example Intervention Scenarios for Silica
• Reduce exposure limit from 0.1 to 0.05 mg/m3 in all workplaces, in 2010, with the same proportion exposed above the new limit as above the old
• Reduce exposure limit again to 0.025 mg/m3
• Improve compliance from 33% to 90% in all workplaces
• Try doing both for all workplaces• Successively enforce the new limit and improve
compliance in workplaces of different sizes

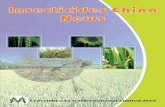
Forecast lung cancer registrations, age 25+, based on population projections and 2004/5 cancer rates by age
0
10,000
20,000
30,000
40,000
50,000
2010 2020 2030 2040 2050 2060
Year
Can
cer r
egis
tratio
ns
0
10,000,000
20,000,000
30,000,000
40,000,000
50,000,000
Proj
ecte
dpo
pula
tion
GB total registrations - men
GB total registrations - women
GB projected population age 25+ - menGB projected population age 25+ - women

Testing reduction of exposure standard and changes in complianceForecast lung cancers for 2060 for Respirable Crystalline Silica
2010Attributable
FractionAttributable registrations
Avoided registrations
3.3 803
2060
Base-line: exposure limit 0.1mg/m3, compliance 33%
1.08 794
Exposure limit 0.05mg/m3, compliance 33% 0.80 592 202
Exposure limit 0.025mg/m3, compliance 33% 0.56 409 385
Exposure limit 0.1mg/m3, compliance 90% 0.14 102 693
Exposure limit 0.05mg/m3, compliance 90% 0.07 49 745
Exposure limit 0.025mg/m3, compliance 90% 0.03 21 773

0100200300400500600700800900
1,000
2010 2020 2030 2040 2050 2060 2070 2080
Att
ribu
tabl
e re
gist
ratio
ns
Forecast year
Forecast Attributable Numbers for Lung cancer and exposure to RCS, Men + Women
Base-line: exposure limit 0.1mg/m3, compliance 33%
Exposure limit 0.05mg/m3, compliance 33%
Exposure limit 0.025mg/m3, compliance 33%
Exposure limit 0.1mg/m3, compliance 90%
Exposure limit 0.05mg/m3, compliance 90%
Exposure limit 0.025mg/m3, compliance 90%

Testing improvement in compliance by workplace sizeForecast lung cancers for 2060 for Respirable Crystalline Silica
2010Attributable Fraction %
Attributable registrations
Avoided registrations
3.3 803
2060
Base-line: exposure limit 0.1mg/m3, compliance 33%
1.08 794
Exposure limit 0.05mg/m3, compliance 33% 0.80 592 202
Exposure limit 0.05mg/m3, % compliance changes by employed workplace size and self employed33% < 250, self employed; 90% 250+ 0.68 499 295
33% < 50, self employed; 90% 50+ 0.61 451 344
33% self employed; 90% all sizes employed 0.35 261 533
90% all workplaces 0.07 49 745

0100200300400500600700800900
1,000
2010 2020 2030 2040 2050 2060 2070 2080
Att
ribu
tabl
e re
gist
ratio
ns
Forecast year
Forecast Attributable Numbers for Lung cancer and exposure to RCS, Men + Women
Base-line: exposure limit 0.1mg/m3, compliance 33%
Exposure limit 0.05mg/m3, compliance 33%
Exposure limit 0.05mg/m3, compliance 33% < 250, self employed; 90% 250+
Exposure limit 0.05mg/m3, compliance 33% < 50, self employed; 90% 50+
Exposure limit 0.05mg/m3, compliance 33% self employed; 90% all sizes employed
Exposure limit 0.05mg/m3, compliance 90% all workplaces

Shift work• Breast cancer due to shift
work likely to increase due to expected increase in service sector employment
• Intervention scenarios: limit proportions exposed for durations of 15+ and 5+ years
• Benefits increase with increased restrictions on years spent on shift work.
• Cancers eliminated by 2060 if exposure for 5+ years eliminated by 2010 (excess risk zero for <5 years exposure)
• Cancers reduced by 94% by 2060 if 90% rather than the current 30% are restricted to <5 years on night shifts.
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
4,500
2010 2020 2030 2040 2050 2060
Attri
buta
ble r
egis
tratio
ns
Forecast year
Shift work: breast cancer, women
(1) Current employment levels maintained, 30% <5, 40% 5-14, 30% 15+ years night shift work
(2) Linear employment trends to 2021-30(3) 50%<5, 30% 5-14, 20% 15+ years night shift work(4) 70%<5, 20% 5-14, 10% 15+(5) 90%<5, 10% 5-14, 0% 15+(6) 100% <5 years

Strong Inorganic Acid Mists
• IARC Group 1 for lung and laryngeal cancers• Risk estimates higher for laryngeal cancers:
H L BLarynx 4.28(2.13, 8.88) 1.91(0.97, 3.78) 1Lung 1.36(0.97,1.94) 1.00• Current burden estimates (total burden)
AF% Deaths RegistrationsLarynx 2.13 (2.61) 16 (20) 46 (2112)Lung 0.20 (14.5) 67 (4748) 76 (4877)• Currently 96% compliance to current WEL 0.3mg/m3

Reduction of exposure standard for Strong Inorganic Acid Mists
2010
Larynx cancer Lung cancerAF% Attributable
registrationsAvoided
registrationsAF% Attributable
registrationsAvoided
registrations
1.9 44 0.19 78
2060
Base-line: 2005 exposure levels maintained 0.1 5 0.003 2
8% linear decline in exposure until 2021-30, constant after 0.5 17 0.029 21
Exposure limit 0.06mg/m3, compliance 90% 0.3 12 6 0.010 7 14
Exposure limit 0.03mg/m3, compliance 90% 0.3 10 7 0.002 2 20
Exposure limit 0.015mg/m3, compliance 90% 0.2 9 8 0.001 0 21
Exposure limit 0.06mg/m3, compliance 99% 0.2 9 8 0.003 2 19

0102030405060708090
100
2010 2020 2030 2040 2050 2060Attr
ibut
able
regi
stra
tions
Forecast year
Strong inorganic acid mists : larynx cancer
0102030405060708090
100
2010 2020 2030 2040 2050 2060Attr
ibut
able
regi
stra
tions
Forecast year
Strong inorganic acid mists: lung cancer

Monitoring success
• Monitor exposure levels
• No reduction in cancer levels until 2030 at earliest (solid tumours)
• After 2030– Use achieved exposed numbers/proportions exposed
at new exposure levels in same (target setting) forecast model to get achieved AF
– Apply achieved AF to same (2005 based) cancer projections to get achieved attributable numbers

Uncertainties and the impact on the burden estimation
Source of Uncertainty Potential impact on burden estimateExclusion of IARC group 2B and unknown carcinogens e.g. for electrical workers and leukaemia
↓
Inappropriate choice of source study for risk estimate
↑↓
Imprecision in source risk estimate ↑↓
Source risk estimate from study of highly exposed workers applied to lower exposed target population
↑
Risk estimate biased down by healthy worker effect, exposure misclassification in both study and reference population
↓
Inaccurate latency/risk exposure period, e.g. most recent 20 years used for leukaemia, up to 50 years solid tumours
↓
Effect of unmeasured confounders ↑↓
Unknown proportion exposed at different levels ↑↓

Summary• Robust methodological approach developed for estimation of burden
for all IARC 1, 2A occupational carcinogens
• Adapted for WHO Global Burden update; Used to inform socio-economic impact analysis of effect of introducing limits for certain carcinogens for DG Employment; HSE costs of workplace illness will include cancer for the first time.
• On-going work: Evaluation of impact of source of bias and uncertainty
• Outputs: – Preliminary work on 6 cancer sites: OEM 2008, 65, 789-800; – Results from all sites: BJC 2010, 102: 1428-1437– Supplement in preparation on current burden detailed results in BJC,
2011 + approx. 24 technical reports + database– Methodology paper on future burden methodology AJE in press– Future burden results in preparation