Essential newborn care: It’s about time!...Essential newborn care: It’s about time! Susan...
26
Essential newborn care: It’s about time! Susan Niermeyer, MD, MPH, FAAP University of Colorado School of Medicine and Colorado School of Public Health Aurora, Colorado, USA
Transcript of Essential newborn care: It’s about time!...Essential newborn care: It’s about time! Susan...

Essential newborn care: It’s about time!
Susan Niermeyer, MD, MPH, FAAPUniversity of Colorado School of Medicine and Colorado School of Public Health
Aurora, Colorado, USA

• No relevant financial relationships with any commercial interests.
• Editor, Helping Babies Breathe, American Academy of Pediatrics and technical advisor to World Health Organization for development of educational materials
• Content expert, ILCOR Neonatal Life Support – cord management
• Senior Medical Advisor for Newborn Health, USAID The views and opinions expressed in this presentation are those of the author and not necessarily the views and opinions of the United States Agency for International Development
COI - Susan Niermeyer

Learning objectives
• Review recent evidence supporting livesavingactions in essential newborn care• Thorough drying and immediate skin-to-skin
care, delayed umbilical cord clamping, early initiation of breastfeeding
• Basic resuscitation• Kangaroo mother and father care, family-
integrated care• Discuss initiatives to strengthen systems of care to
improve global neonatal outcomes• Appreciate the relevance of essential newborn care
to both resource-limited and resource-rich settings
Essential newborn care: increasing survival, improving outcome, eliminating disparities

Causes of neonatal mortality—The Big Three
SevereInfections
Intrapartum-related complications
Complications from preterm birth
Liu L et al. Lancet 2012

Evidence-based interventions3 major causes of neonatal mortality
Maternal tetanus immunizationDx/rx bacteruriaHygieneImmediate skin-to-skinExclusive breastfeedingRecognition of Danger Signs- coordinated postnatal care
Improved fetal monitoringAccess to C-sectionNeonatal resuscitationDelayed umbilical cord
clamping
Dx/rx pre-eclampsiaAntenatal steroids and tocolyticsAntibiotics for PROMKangaroo mother careFamily-centered care
http://www.who.int/pmnch/knowledge/publications/201112_essential_interventions/en/

Preterm birth
• Antenatal corticosteroids, preterm labor management
• Care including essential newborn care + Kangaroo mother care
Birth complications
(and intrapartum stillbirths)
• Prevention by skilled attendance and obstetrics
• Care including essential newborn care + resuscitation
Neonatal infections
• Prevention, essential newborn care especially breastfeeding, chlorhexidine where appropriate
• Case management of neonatal sepsis with antibiotics
1
2
* Prioritised by the UN Commission on Life Saving Commodities for Women and Children
71% of newborn deaths preventable
actionable now without intensive care
3
Three main causes of newborn deaths all have effective and feasible interventions = 3 by 2
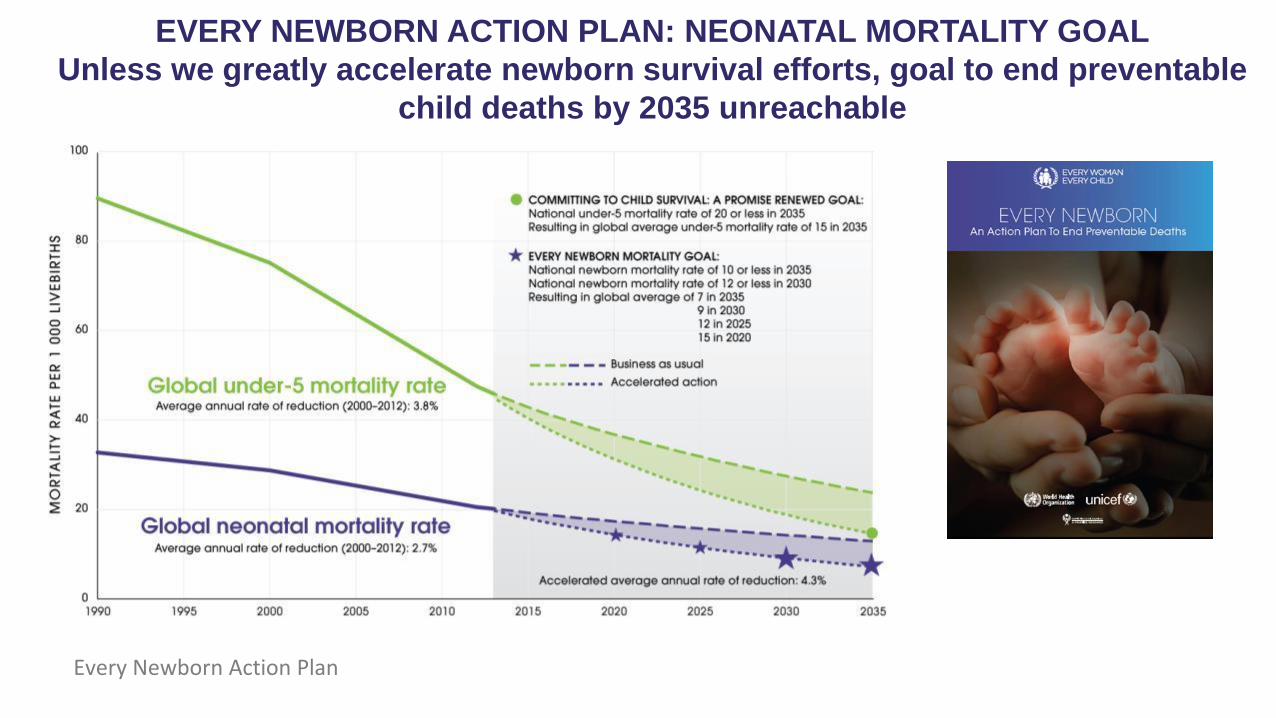
EVERY NEWBORN ACTION PLAN: NEONATAL MORTALITY GOAL
Unless we greatly accelerate newborn survival efforts, goal to end preventable
child deaths by 2035 unreachable
Every Newborn Action Plan

Implementation of best practices
patient survival is the product of three important factors
Søreide E et al. Resuscitation 2013;84:1487-93
Medical
Science
Educational
Efficiency
Local
ImplementationSurvival
The Formula for Survival

Implementation of best practices: basic stabilization and resuscitation
Drying to provide stimulation of breathing
and prevent hypothermia
Immediate skin-to-skin contact to promote early
breastfeeding and prevent hypothermia
Delayed umbilical cord clamping to promote
cardiovascular stability
Early initiation of breastfeeding to avoid
hypoglycemia
Clearing the airway only if necessary
Specific stimulation to breathe
Ventilation within one minute after birth, The Golden Minute
Improved ventilation

Implementation of best practices: drying and immediate skin-to-skin contact
Advantages of immediate skin-to-skin contact
• Promotes physiological stability of infant – stimulates breathing, maintains temperature and decreases stress
• Improves breastfeeding outcomes to 6 months
• Facilitates maternal-infant attachment
o Preparation of mothero Presence of companiono Adjustment of workflow
www.Cochrane.org/CD003519, 2016

Skin-to-skin contact and importance of normal temperaturehypothermia is common – especially in small or preterm infants
N=8782 infants < 1500 grams
Miller S et al. J Perinatology 2011; 31:S49

Skin-to-skin contact and importance of normal temperature
• Temperature < 36⁰C at birth is an independent risk factor for death in premature infants• Evidence from 36 observational studies
• Low quality evidence upgraded to moderate due to effect size, dose-effect relationship, single direction of evidence
• Hypothermia is associated with morbidities• Respiratory distress
• Metabolic derangements - hypoglycemia
• Intraventricular hemorrhage
• Late-onset sepsis
hypothermia is associated with mortality and morbidity in premature infants
Mullany LC et al. Arch Pediatr Adolesc Med 2010;164:650Laptook AR et al Pediatrics 2007119:e643

Skin-to-skin contact and importance of normal temperature
Lyu Y et al. JAMA Pediatrics 2015; 169(4)
hypothermia and hyperthermia are associated with mortality and morbidity in premature infants
N = 9833 infants < 33 weeks

Implementation of best practices: physiological umbilical cord clamping
Advantages of delayed umbilical cord clamping• Smoother cardiopulmonary
transition at birth• Improved placental
transfusion – reduction of anemia, higher BP and temperature
• Feasibility at vaginal or C-section birth
• Resuscitation with cord intact (option)
o Physical space for infanto Communication among providerso Preparation of mother
Ersdal H et al. Pediatrics 2014; DOI: 10.1542/peds.2014-0467

Physiologic umbilical cord clamping reduces in-hospital mortality < 37 weeks
Fogarty M et al. AJOG 2017

Implementation of best practices: early initiation of breastfeeding (1st hour)
Advantages of early initiation of breastfeeding
• Reduced hypoglycemia
• Improved success with latch/suckling in first days
• Timely switch from colostrum to milk production
• Improved milk volume at 4 days, 4 weeks, 4 months
• Lower mortality
o Preparation of mothero Skin-to-skin contacto Undisturbed first houro Adjustment of workflow
www.who.int/elena/titles/early_breastfeeding/en/

Implementation of best practices: basic resuscitation (Helping Babies Breathe)
Dol J. JBI Database of Sys Rev and Impl Rep 2018
Fresh stillbirth
First-day mortality
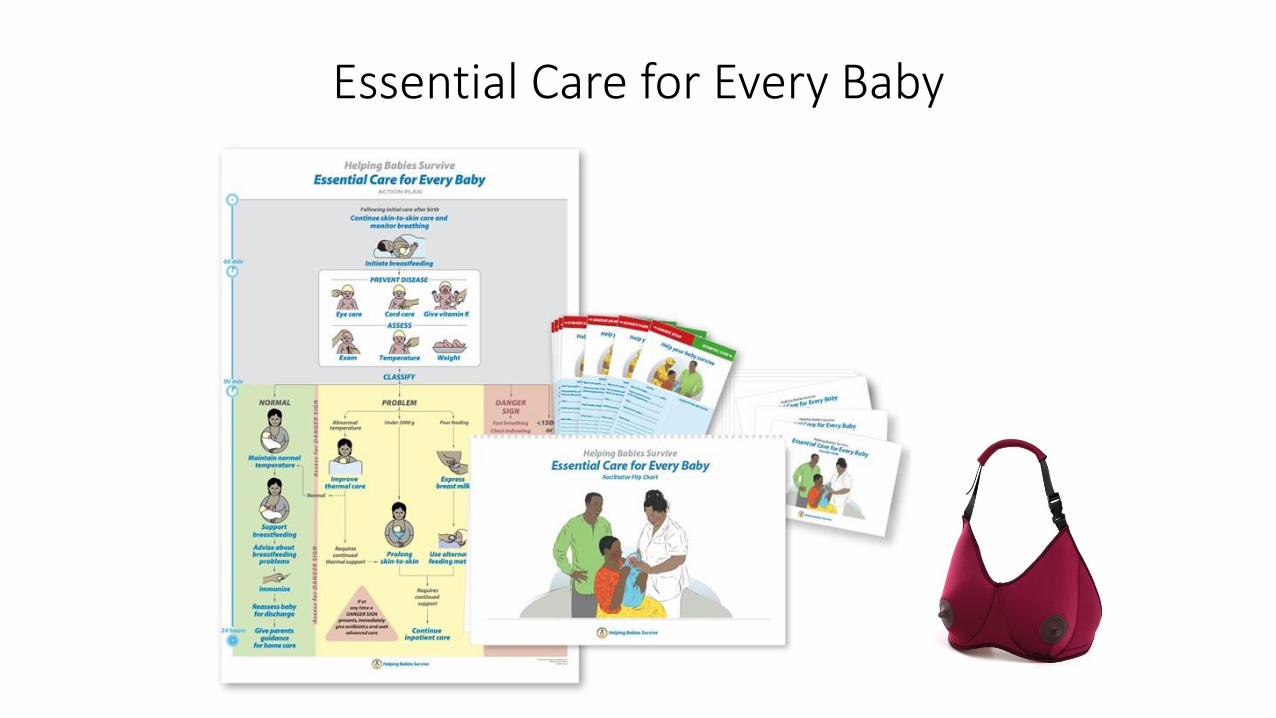
Essential Care for Every Baby
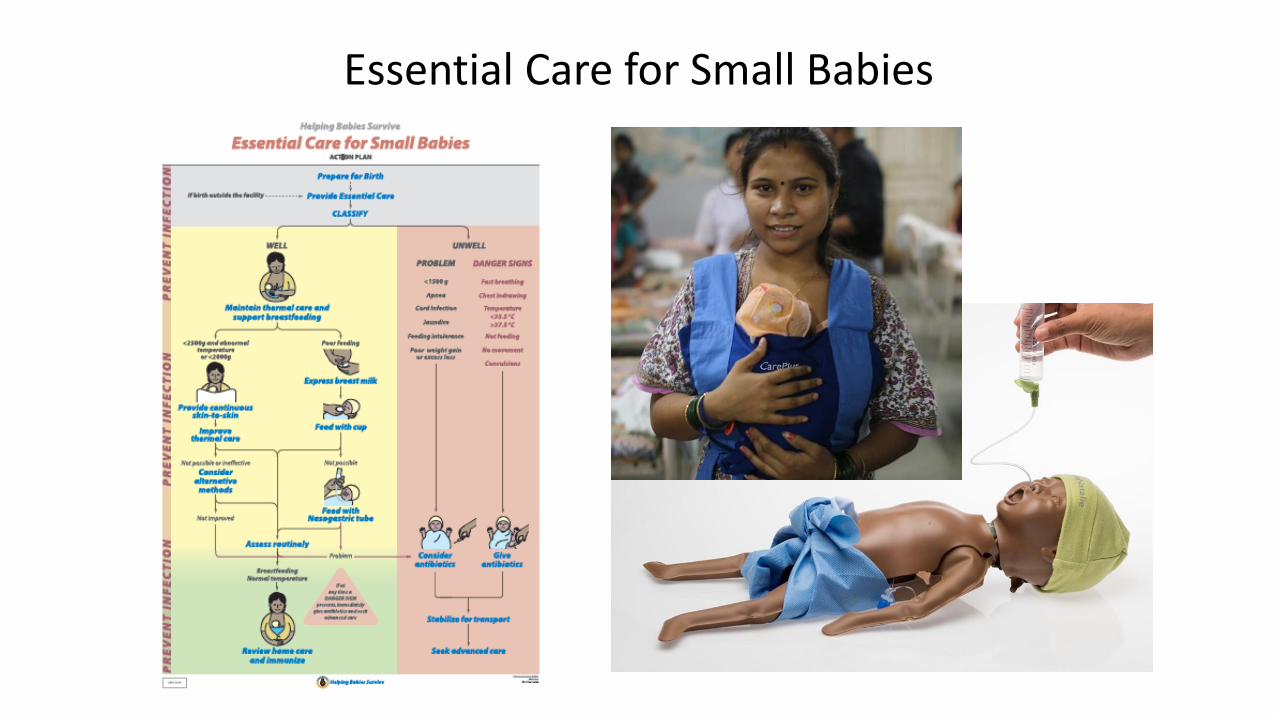
Essential Care for Small Babies

Implementation of best practices: family-integrated care
Advantages of family-integrated care
• Capacity-building of caregivers• Hygiene – handwashing, equipment• Bathing/cleaning the baby• Breastfeeding/expression and feeding of breastmilk• Skin-to-skin care• Developmentally supportive care• Recognition of Danger Signs and seeking medical help
• Improved infant and parent outcomes• Improved weight gain, exclusive breastfeeding• Reduced parental stress and anxiety
• Improved patient-staff interactiono Change in policies and staff roleso Continuous support and
supervisiono Physical facilities and services O’Brien K et al. Lancet Child Adolesc Health 2018
Verma A, et al. Indian Pediatrics 2017; 54:455

Implementation of best practices: Kangaroo mother (and father) care
Advantages of kangaroo care
• Improved survival of LBW in resource-limited settings
• Support of breastfeeding/ breast milk feeding
• Improved growth
• Infection prevention
• Thermal stability
• Shorter facility stay
o Preparation of mother/familyo Flexible use of available bedspaceo Facilities/services for families –
sleeping space, toilet, water and food
https://www.healthynewbornnetwork.org/hnn-content/uploads/ PA-KMC-Joint-Statement_final_2017.pdf

Implementation of best practices: developmentally supportive care
Optimizing nutritionProtecting skin
Safeguarding sleep
Minimizing stress and pain
Positioning and interacting
PARENTS/FAMILY
CARE PROVIDERS
Altimier L, Phillips R. Newborn & Infant Nsg Rev 2016; 16:230

10 steps for Helping Babies and Mothers Survive 1. Secure Ministry of Health buy-in
2. Form a working group for planning, training and monitoring
3. Develop national roll-out plan for pre-service and in-service
training, in both public and private sector
4. Provide learning materials & equipment at time of training
5. Identify and support local leaders and champions
6. Establish Low-Dose High-Frequency refresher training
7. Establish facility level quality improvement teams
8. Monitor performance
9. Establish a system for reporting and feedback
10.Engage health providers, families and the broadercommunity
http://journals.plos.org/plosone/article?id=10.1371/journal.pone.10178073
Implementation of best practices: strengthening systems

WHOEssential Newborn Care educational materials
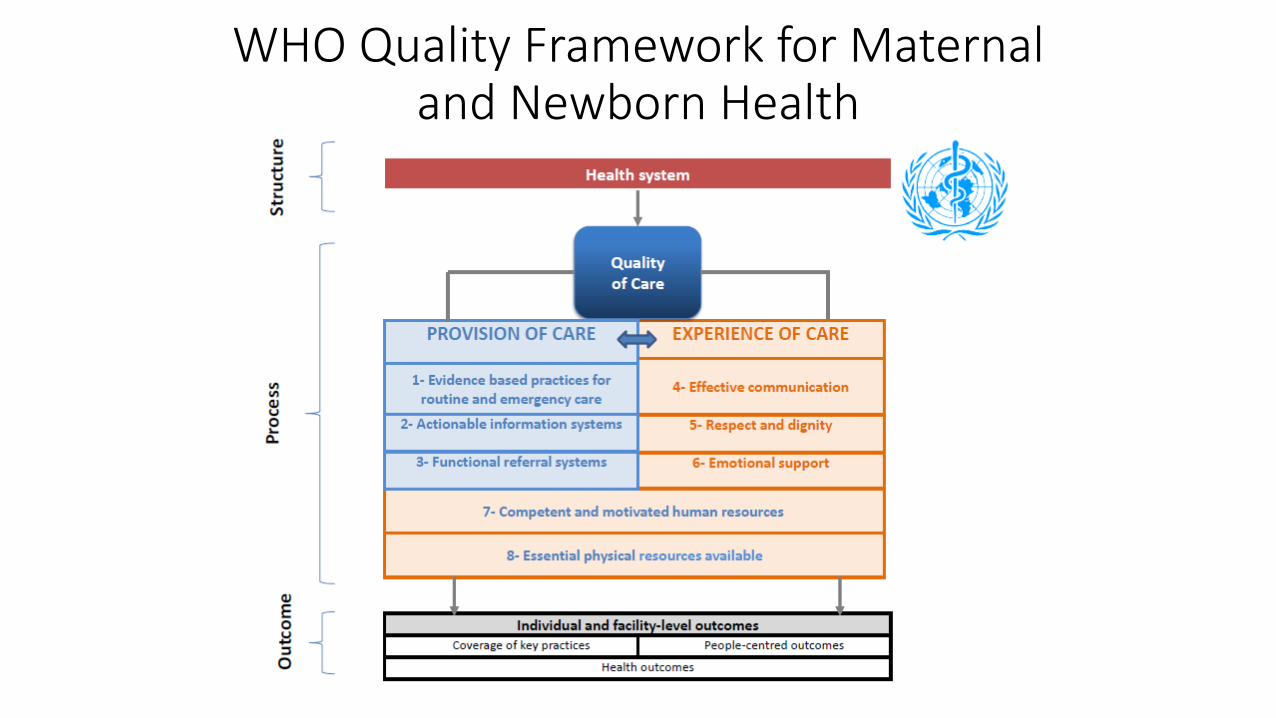
WHO Quality Framework for Maternal and Newborn Health

Essential newborn care – lifesaving in every setting
WHO Western Pacific Region, Early Essential Newborn Care