
ESMO SUMMIT MIDDLE EAST 2018...ESMO SUMMIT MIDDLE EAST 2018 Breast Clinical Cases Presentation...
89
ESMO SUMMIT MIDDLE EAST 2018 Breast Clinical Cases Presentation Hampig Raphael Kourie , MD , MSc , MBioethics Faculty of Medicine , Saint Joseph University of Beirut, Lebanon 6-7 April 2018, Dubai, UAE
Transcript of ESMO SUMMIT MIDDLE EAST 2018...ESMO SUMMIT MIDDLE EAST 2018 Breast Clinical Cases Presentation...

ESMO SUMMIT MIDDLE EAST 2018Breast Clinical Cases Presentation
Hampig Raphael Kourie , MD , MSc , MBioethics
Faculty of Medicine , Saint Joseph University of Beirut, Lebanon
6-7 April 2018, Dubai, UAE

CONFLICT OF INTEREST DISCLOSURE
No conflict of interest

CASE 1: Treatment-naïve ER+ metastatic breast cancer in premenopausal woman
CASE 2 : Adjuvant treatment in TNBC
CASE 3 : Heavily pretreated HER2+ metastatic breast cancer
CASE 4 : Heavily pretreated ER+ metastatic breast cancer
CASE 5: Hereditary breast cancer
CASE 6 : Metastatic breast cancer in man

CASE 1 : ER+ METASTATIC BREAST CANCER IN PRE-
MENOPAUSAL WOMAN

CASE 1 : ER+ METASTATIC BREAST CANCER IN PRE-
MENOPAUSAL WOMAN
HISTORY AND SYMPTOMS
40 years old woman (born in 1978) without relevant past medical history
Familial History : Mother diagnosed with a breast cancer at the age of 60 and a
maternal cousin with breast cancer at the age of 50
She felt a right breast nodule, 4 years ago, (2014) during her pregnancy , without
doing any further investigation
She presented a dorsal pain since November 2017

CASE 1 : ER+ METASTATIC BREAST CANCER IN PRE-
MENOPAUSAL WOMAN
WORK-UP
In the end of January 2018 , she visited an orthopedic surgeon for investigation
Persistant dorsal and lumbar pain despite the antalgic treatment
Dorso-lombar MRI : secondary lesions at D12 and L2

Mammogram : 4 cm lesion in the right breast with supra-centimetric axillary lymph
nodes
TAP CT Scan : no other secondary lesion
Ca 15-3 : 20.54 (N)
CASE 1 : ER+ METASTATIC BREAST CANCER IN PRE-
MENOPAUSAL WOMAN
WORK-UP

CASE 1 : ER+ METASTATIC BREAST CANCER IN PRE-
MENOPAUSAL WOMAN
WORK-UP
Biopsy of the right breast nodule (2/2/2018) :
Invasive ductal carcinoma moderately differentiated
ER : positive (80%)
PR : negative
HER2 2+ FISH negative
Ki67 : 25%
Grade 2

Persistant dorsal pain without any response to antalgic treatment in ER+ metastatic
breast cancer
What to do next ?

POSSIBLE THERAPEUTIC OPTIONS ?
1)Chemotherapy followed by hormonal therapy
2)Radiation therapy followed by hormonal therapy
3)Hormonal therapy
4)Breast Surgery followed by hormonal therapy

REMOVAL OF THE PRIMARY IN METASTATIC BREAST
CANCER

Radiation therapy on D12 and L2 vertebral secondary lesions (10 sessions) +
Zoledronic acid
What to do next ?

POSSIBLE THERAPEUTIC OPTIONS ?
1)LHRH agonists + AI
2)LHRH agonists + AI+ anti-CDK4/6
3)Bilateral oophorectomy + AI
4)Bilateral oophorectomy + AI + anti-CDK4/6
5)Tamoxifene
6)LHRH agonists + tamoxifene
7)LHRH agonists + tamoxifene + anti-CDK4/6

OVARIAN ABLATION VERSUS SUPPRESSION

eUpdate – ESMO Advanced Breast Cancer Algorithms , 2017

MONALEESA-7: Phase III placebo-controlled study of ribociclib
and tamoxifen/NSAI + goserelin
• Tumor assessments were performed every 8 weeks for 18 months, then every 12 weeks thereafter
• Primary analysis planned after ~329 PFS events
– 95% power to detect a 33% risk reduction (hazard ratio 0.67) with one-sided α=2.5%, corresponding to an increase in
median PFS to 13.4 months (median PFS of 9 months for the placebo arm1,2), and a sample size of 660 patients
NSAI, non-steroidal aromatase inhibitor; RECIST, Response Evaluation Criteria in Solid Tumors. *Tamoxifen = 20 mg/day; NSAI: anastrozole = 1 mg/day or letrozole = 2.5 mg/day; goserelin = 3.6 mg every 28 days;
‡PFS by Blinded Independent Review Committee conducted to support the primary endpoint.1. Klijn JG, et al. J Clin Oncol 2001;19:343–353; 2. Mourisden H, et al. J Clin Oncol 2001;19:2596–2606.
Stratified by:
• Presence/absence of liver/lung metastases
• Prior chemotherapy for advanced disease
• Endocrine therapy partner (tamoxifen vs
NSAI)
Primary endpoint
• PFS (locally assessed per
RECIST v1.1)‡
Secondary endpoints
• Overall survival (key)
• Overall response rate
• Clinical benefit rate
• Safety
• Patient-reported outcomes
• Pre/perimenopausal women
with HR+, HER2– ABC
• No prior endocrine therapy for
advanced disease
• ≤1 line of chemotherapy for
advanced disease
• N=672
Randomization (1:1)
Ribociclib(600 mg/day; 3-weeks-on/1-week-
off)
+ tamoxifen/NSAI + goserelin*
n=335
Placebo+ tamoxifen/NSAI + goserelin*
n=337
Tripathy et al , SABCS 2017

PRIMARY ENDPOINT: PFS (INVESTIGATOR-ASSESSED)
CI, confidence interval; NR, not reached.
Goserelin included in all combinations.
Pro
bab
ility
of
PF
S (
%)
Time (months)No. at risk
Ribociclib + tamoxifen/NSAI 335 301 284 264 245 235 219 178 136 90 54 40 20 3 1 0
Placebo + tamoxifen/NSAI 337 273 248 230 207 183 165 124 94 62 31 24 13 3 1 0
PFS (investigator assessment)
Ribociclib + tamoxifen/NSAI n=335
Placebo + tamoxifen/NSAI n=337
Number of events, n (%) 131 (39.1) 187 (55.5)
Median PFS, months (95% CI)
23.8(19.2–NR)
13.0(11.0–16.4)
Hazard ratio (95% CI) 0.553 (0.441–0.694)
One-sided p value 0.0000000983
1086420
100
80
60
40
20
0
30282624222018161412
10
30
50
70
90
Tripathy et al , SABCS 2017

TREATMENT
16/3/2018 : bilateral oophorectomy
19/3/2018 : Started letrozole + palbociclib + zoledronic acid

UNMET NEED IN PREMENOPAUSAL PATIENTS WITH
HR+, HER2– ABC
Estimates suggest that in 2017 in the US, ~19% of invasive breast cancers will be diagnosed in women
aged ≤49 years
The proportion of patients aged <50 years may be up to 40% to 50% in the Middle East (Najjar et
al)
The last randomized trial focusing solely on premenopausal women with ABC was published in 2000
Young women with ABC have a distinct tumor biology, experience more aggressive disease, and are
more likely to die from their cancer than older women

TAKE HOME MESSAGES FROM CASE ONE
Premenopausal breast cancer patients represent an important public health issue in
the Middle East
More studies should be done in this specific population , mainly in developing
countries
Anti-CDK4/6 agents will certainly have their place in the algorithm of the treatment
of pre-menopausal ER+ metastatic breast cancer

CASE 2 : ADJUVANT TREATMENT IN TNBC

HISTORY AND WORK-UP
A 37 years old woman (born in 1981) without relevant past medical history
Ultrasound of the left breast (24/1/2018) : an inferior-intern nodule of 1.8 cm
(ACR4a)
Breast MRI (8/2/2018) : an inferior-intern nodule of 2 cm ACR6 at left (ACR6)
A biopsy was done (9/2/2018) :ductal carcinoma of unknown specificity (aspects of
metaplastic carcinoma); ki67 : 70% , triple negative , grade 3

TUMORECTOMY
19/2/2018 : Tumorectomy
Invasive ductal carcinoma , metaplastic with a squamous cell component and a
ductal carcinoma NOS , grade 3 , T=2.4 cm
Negative margins
0/10 positive lymph nodes
Absence of vascular and lymphatic invasion

WORK-UP
PET/CTScan : negative
Cardiac US : EF=70%
Genetic testing : ongoing

HISTOLOGIC SUBTYPES : INFILTRATIVE CARCINOMA

METAPLASTIC CARCINOMA
RARE
POOR PROGNOSIS
CHEMORESISTANT ?

IN FRONT OF TNBC WITH METAPLASTIC
COMPONENT?
1)SURVEILLANCE
2)ADJUVANT CHEMOTHERAPY
3)RADICAL MASTECTOMY

It was decided to start a chemotherapy.
Dose Dense versus every 3 weeks adjuvant chemotherapy ?

San Antonio 2017


Is there any role for carboplatine in the adjuvant setting if there is a BRCA mutation
?

CARBOPLATIN BASED REGIMEN IN THE NEO-
ADJUVANT SETTING
Castrellon et al , 2017

TWO NEGATIVE TRIALS IN THE ADJUVANT SETTING
ASCO 2017

TAKE HOME MESSAGES FROM CASE 2
TNBC is divided in different histologic and molecular subtypes ; each one having
specific characteristics
Dose-dense chemotherapy could be considered in the adjuvant setting , namely in
TNBC 5% decrease in recurrence rate at 10 years
No evidence on the use of carboplatine in the adjuvant setting in BRCA mutated
triple negative breast cancer

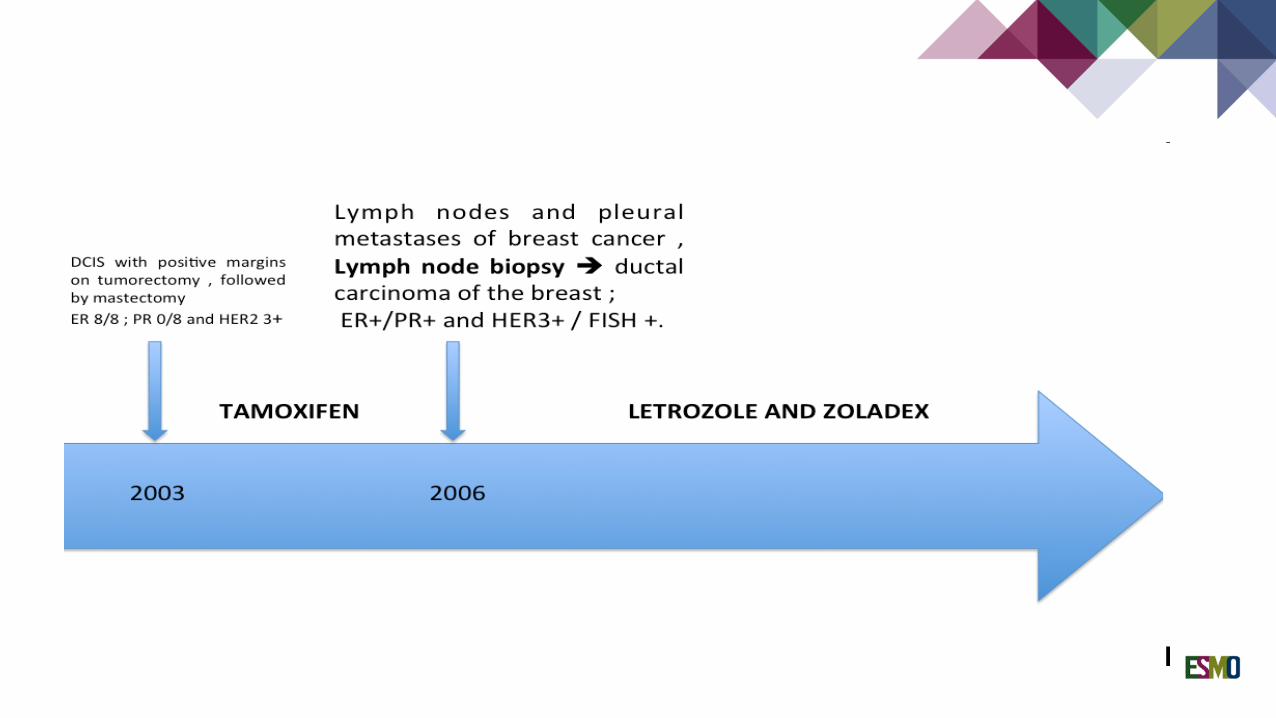
CASE 3 : HEAVILY TREATED HER2+ MBC
55 years old women, without past medical history or comorbidities , diagnosed in
2003 with right breast cancer.
Tumorectomy ; pathology : DCIS of 3.5 cm with positive margins , ER 8/8 , PR
0/8 and HER2 3+
Right mastectomy

HISTORY
55 years old women, without past medical history or comorbidities , diagnosed in
2003 with right breast cancer.
Tumorectomy ; pathology : DCIS of 3.5 cm with positive margins , ER 8/8 , PR
0/8 and HER2 3+
Right mastectomy





\

OTHER POSSIBLE TREATMENT OPTIONS
Eribuline role ? with trastuzumab ?
Platinum-based agents?
A place for pertuzumab in heavily pre-treated HER2+ patients ?


HER2 + BC WITH BRAIN METASTASES

SUPPRESSION OF ANTI-HER2 PATHWAY

CASE 4 : HEAVILY TREATED PREMENOPAUSAL HR+ MBC

HISTORY AND DIAGNOSIS
45 years old woman, without past medical history, diagnosed in 1999 at the age of 28 with
right breast cancer
Tumorectomy + lymph node dissection : 22 mm invasive ductal carcinoma with positive
hormonal receptors and negative HER2
Familial history : Absence of other cancers in the family
Genetic screening : Absence of BRCA1 or BRCA2 mutation

ADJUVANT TREATMENT
Followed by adjuvant chemotherapy 4 adriamycine and 3 MF , radiation therapy
and tamoxifen (stopped in 2001 , after 1 year for pregnancy and restarted after that)
3MF instead of CMF : cyclophosphamide was omitted in order to decrease the risk
of toxicity to the ovaries

PREMENOPAUSAL LUMINAL BREAST
CANCER-PREGNANCY
Fertility concerns influence treatment decision in an important number of patients
Many patients still fear that a future pregnancy will increase their risk of recurrence
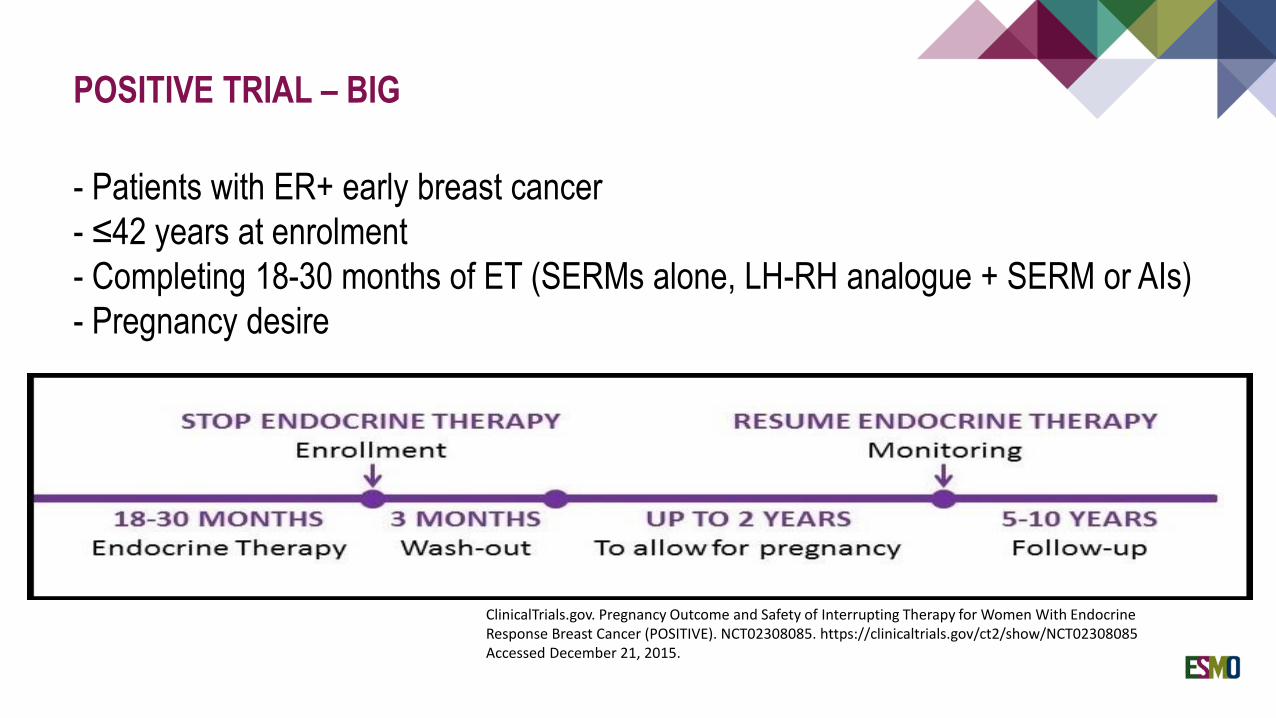
POSITIVE TRIAL – BIG
- Patients with ER+ early breast cancer
- ≤42 years at enrolment
- Completing 18-30 months of ET (SERMs alone, LH-RH analogue + SERM or AIs)
- Pregnancy desire
ClinicalTrials.gov. Pregnancy Outcome and Safety of Interrupting Therapy for Women With Endocrine Response Breast Cancer (POSITIVE). NCT02308085. https://clinicaltrials.gov/ct2/show/NCT02308085 Accessed December 21, 2015.




The patient presented a new bone marrow progression .
Suggestions ?
New agents
Experimental therapy (phase 1 ?)
Other?

Treatment by aromatase inhibitor (started 6/1/2016) and palbociclib (22/1/2016)
Schedule of Palbociclib was adapted according to hematogical count during
therapy

Good performance status during the evolution of the disease and willing to be
“actively” treated.
In addition to standard of care , access to 3 new therapies that become available
during the course of the disease (eribuline , afinitor and palbociclib) and 1
experimental agent (XRP).
Long ambulatory course treatment of 17 years (Her child become an adolescent of
16 years at her death) Hospitalized only for 2 times
One episode of febrile neutropenia (March 2016)
Death due to hepatic PD (April 2016 )

CASE 5 : HEREDITARY CANCERS

HISTORY
Mrs R is a single woman, without a relevant past medical history, diagnosed at the
age of 40 from a breast cancer.

PEDIGREE
? 4
Lena, Melanoma at 60
Eugénie, Lung?
Elias
2 3 4
Najib
Suzanne, breast cancer at the age of 50
2
Fouad
Tony,prostatecancer at 64
3
Michel
Rabiha, CUP at 27 years old
5
Wadih, 1939 ,died in 2011
Souad1950
2 3
Jean, melanoma at the age 64 died at the age of 68
Maroun 1968 Joseph 1969
Simon 1972
Rania 1973
1996 1993 1999 1995 2008 2010

DIAGNOSIS
Pathology report (2014) :
Triple negative invasive ductal carcinoma , grade 3.
T=1.8cm without lymph node invasion.

TREATMENT
Treated with neo-adjuvant chemotherapy (4AC-4T) followed by partial mastectomy
and radiation therapy.
She relapsed in 2016 and presented a single pulmonary nodule of 1.2 cm , treated
by surgery.
Now she is under surveillance.

Is there any indication for genetic testing ?
Which genes should be tested ?


WHEN WE SHOULD SUSPECT A HEREDITARY BREAST
CANCER IN A PATIENT WITH BREAST CANCER?
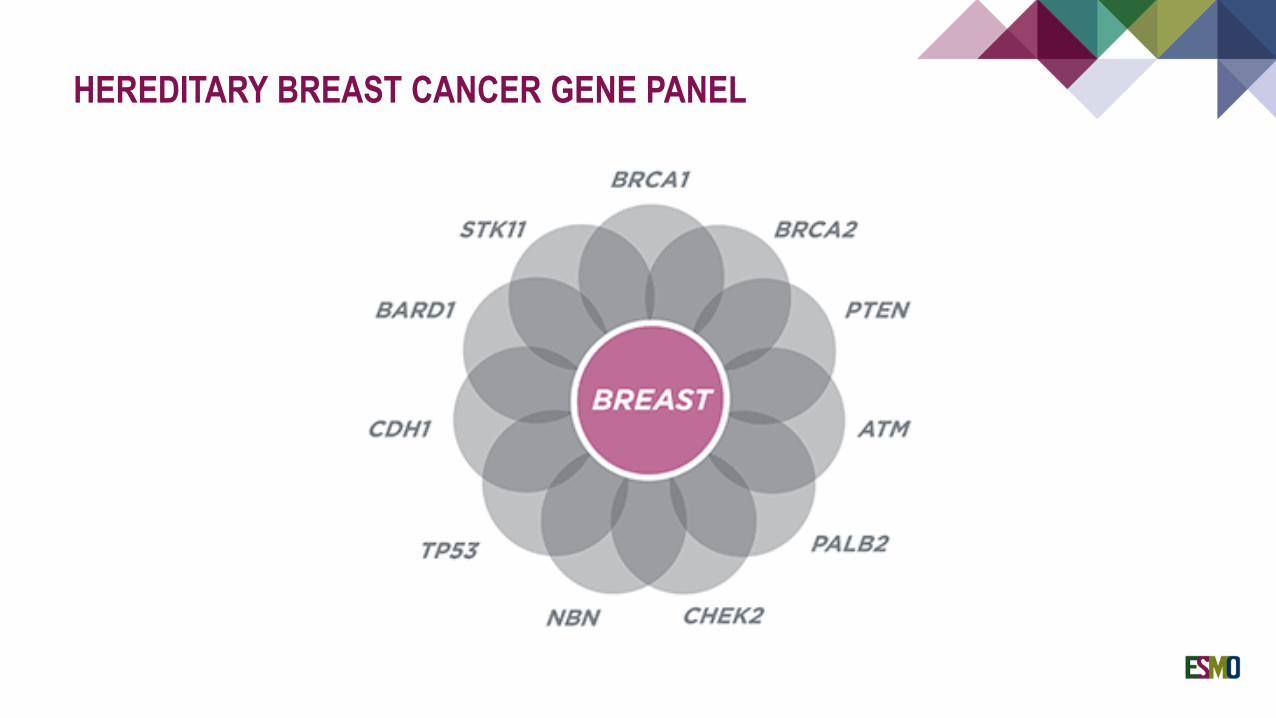
HEREDITARY BREAST CANCER GENE PANEL

RESULTS OF GENETIC TESTING
Panel of 19 genes for breast ovarian hereditary cancer panel
Presence of pathogenic BRCA1 mutation

CONSEQUENCES ON THE PATIENT AND HIS FAMILY
Prophylactic bilateral mastectomy and salpingo-oophorectomy
Targeted genetic testing in the children and brotherhood

PREVENTION AND SCREENING IN BRCA MUTATION
CARRIERS AND OTHER BREAST/OVARIAN
HEREDITARY CANCER SYNDROMES: ESMO CLINICAL
PRACTICE GUIDELINES
Paluch-Shimon et al , Annals of Oncology 2016

PREVENTION AND SCREENING IN BRCA MUTATION CARRIERS
AND OTHER BREAST/OVARIAN HEREDITARY CANCER
SYNDROMES: ESMO CLINICAL PRACTICE GUIDELINES
Paluch-Shimon et al , Annals of Oncology 2016
Breast cancer risk reduction – screening

PREVENTION AND SCREENING IN BRCA MUTATION CARRIERS
AND OTHER BREAST/OVARIAN HEREDITARY CANCER
SYNDROMES: ESMO CLINICAL PRACTICE GUIDELINES
Paluch-Shimon et al , Annals of Oncology 2016
Breast cancer risk reduction – surgery

OTHER BRCA-ASSOCIATED CANCER
Paluch-Shimon et al , Annals of Oncology 2016

PREVENTION AND SCREENING STRATEGIES FOR
SPECIFIC MUTATIONS
Paluch-Shimon et al , Annals of Oncology 2016

TAKE HOME MESSAGES FOR CASE 5
Genetic counseling is necessary in :
-patients with familial history of breast and ovarian cancer ,
-young patients with breast cancers
-patient with more than one cancer from the spectrum of HBOC .
Panel of genes for HBOC syndrome by NGS
Prophylactic screening modalities and surgey are indicated in the presence of
deleterious mutations leading to HBOC syndrome

CASE 6 : METASTATIC BREAST CANCER IN MALE

HISTORY
A 43 years old patient (born in 1975) without relevant past medical history
No familial history of cancer

DIAGNOSIS
October 2016 : palpation of a lump in the right breast
Total body MRI done showed a 4.4 cm nodule in the with axillary lymph nodes , 2
costal secondary lesions and diffuse small pulmonary nodules (<5 mm)

PATHOLOGY REPORT
Invasive ductal carcinoma
ER : 75%
PR : 10%
HER2 :-
Grade 2

TREATMENT
November 2016: He was treated with letrozole and palbociclib
February 2017: Partial response ; breast lesion decreased to 2.8 cm instead of 4.4
cm ; disapparance of costal lesions , decrease and disappearance of lung lesions

In april 2018, after 18 months of treatment by letrozole and palbociclib, he
presented a progression in the axillary lymph nodes (+20%) and appearance of a
new bone lesion and progression of the costal lesions
The patient tolerated very well the treatment without remarkable side effects


FEW CASES REPORTED IN THE LITERATURE
ASCO 2017

What is the treatment option after progression?

eUpdate – ESMO Advanced Breast Cancer Algorithms , 2017

What is the treatment option after progression?

TAKE HOME MESSAGES
A genetic counseling is necessary in every man with breast cancer
Second line hormonal-based treatment is indicated after progression on 1st
line ER+ metastatic breast cancer in the absence of visceral crisis
Extrapolation of the treatment of breast cancer in men from women

THANK YOU


















