
Erythropoiesis-Stimulating Agent Drug Class Revie Table 2. Summary of Colony Stimulating Factors 1,...
23
Erythropoiesis-Stimulating Agents 20:16 Hematopoietic Agents Darbepoetin Alfa (Aranesp®) Epoetin Alfa (Epogen®; Procrit®) Final Report September 2013 Review prepared by: Melissa Archer, PharmD, Clinical Pharmacist Carin Steinvoort, PharmD, Clinical Pharmacist Gary Oderda, PharmD, MPH, Professor University of Utah College of Pharmacy Copyright © 2013 by University of Utah College of Pharmacy Salt Lake City, Utah. All rights reserved
Transcript of Erythropoiesis-Stimulating Agent Drug Class Revie Table 2. Summary of Colony Stimulating Factors 1,...
Erythropoiesis-Stimulating Agents 20:16 Hematopoietic Agents
Darbepoetin Alfa (Aranesp®)
Epoetin Alfa (Epogen®; Procrit®)
Final Report
September 2013
Review prepared by:
Melissa Archer, PharmD, Clinical Pharmacist
Carin Steinvoort, PharmD, Clinical Pharmacist
Gary Oderda, PharmD, MPH, Professor
University of Utah College of Pharmacy
Copyright © 2013 by University of Utah College of Pharmacy
Salt Lake City, Utah. All rights reserved
2
Table of Contents
Executive Summary ....................................................................................................................................................... 3
Introduction ................................................................................................................................................................... 5
Table 1. Comparison of the Erythropoiesis-Stimulating Agents .......................................................................... 5
Table 2. Summary of Colony Stimulating Factors ............................................................................................... 6
Disease Overview ...................................................................................................................................................... 9
Figure 1. Classification of Anemia ....................................................................................................................... 9
Table 3. Dosing of the Erythropoiesis-Stimulating Agents ................................................................................ 10
Table 4. Dosing Conversion Recommendations ................................................................................................. 11
Pharmacology/Pharmacokinetics ................................................................................................................................. 12
Table 5. Pharmacokinetics of the Erythropoiesis-Stimulating Agents................................................................ 12
Methods ....................................................................................................................................................................... 13
Clinical Efficacy .......................................................................................................................................................... 13
Special Populations ................................................................................................................................................. 14
Adverse Drug Reactions .............................................................................................................................................. 15
Table 6. Warnings and Adverse Events Reported with the Erythropoietin-Stimulating Agents ........................ 15
Summary...................................................................................................................................................................... 17
References ................................................................................................................................................................... 18
Evidence Table. Clinical Trials Evaluating the Erythropoietin-Stimulating Agents ................................................... 21

3
Executive Summary
Introduction: Several myeloid growth factor therapies are currently available for use in
the United States. This review focuses on the erythropoiesis-stimulating agents (ESAs).
Two erythropoiesis-stimulating agents are currently available for use: darbepoetin alfa
and epoetin alfa. Both agents are indicated in the treatment of anemia due to
myelosuppressive chemotherapy and chronic kidney disease. Epoetin alfa is also
indicated in the treatment of anemia due to human immunodeficiency virus (HIV)
therapy and in the reduction of transfusion in elective surgery. The agents can be used
intravenously or subcutaneously and dosing is titrated to effect.
Anemia affects nearly one third of the world's population and is associated with
an increased rate of mortality and decreased physical functioning and quality of life.
Treatment of anemia depends on the underlying problem and may include an
erythropoiesis-stimulating agent. The erythropoiesis-stimulating agents stimulate
erythroid proliferation and differentiation, improve hematocrit and hemoglobin levels,
and reduce the need for transfusions. Adequate iron supplies are required for sustained
erythropoiesis and supplemental iron is often recommended with ESA therapy.
Guidelines for use of ESA in anemia associated with chronic kidney disease or cancer
chemotherapy recommend the lowest possible dose should be used to gradually increase
the hemoglobin concentrations to a level sufficient to avoid the need for red blood cell
transfusion.
Clinical Efficacy: The efficacy of the erythropoiesis-stimulating agents was directly
compared in five randomized controlled trials and two observational trials. Two trials
examined ESA use in anemia associated with chronic kidney disease and 5 trials
examined ESA use in anemia associated with cancer chemotherapy. No comparative
clinical evidence is available for ESA use in anemia associated with noncardiac surgery
or HIV therapy. Based on the available evidence, darbepoetin and epoetin are effective in
achieving and maintaining hemoglobin levels sufficient to avoid red blood cell
transfusions in patients with anemia associated with chronic kidney disease or cancer
chemotherapy. The agents appear to have comparable safety and efficacy in these patient
populations. Limited data are available evaluating ESA use in special populations.
Careful monitoring of hemoglobin levels, blood pressure, and adverse events are required
in pediatric and geriatric patients receiving ESA therapy.
Adverse Drug Reactions: The most common adverse effects associated with ESA
therapy are hypertension and thromboembolic complications. The US Food and Drug
Administration has issued a warning for increased risk of thrombotic and cardiovascular
events in patients receiving an ESA with hemoglobin levels > 11 g/dL. Hypertension
occurs in about 20-30% of patients receiving ESA therapy, usually as a result of a rapid
increase in hematocrit and ESA use is contraindicated in patients with preexisting
uncontrolled hypertension. Headache, tachycardia, edema, shortness of breath, nausea,
vomiting, diarrhea, injection site reaction, and flu-like symptoms have also been reported

4
in patients receiving ESA therapy. The ESAs may only be prescribed under the risk
evaluation and mitigation strategy program.
Summary: Darbepoetin alfa and epoetin alfa are effective in achieving and maintaining
hemoglobin levels sufficient to avoid red blood cell transfusions in patients with anemia
associated with chronic kidney disease or cancer chemotherapy. In general, therapy with
an ESA should be individualized to achieve and maintain hemoglobin levels within the
range of 10 to 12 g/dL in order to avoid a transfusion while limiting risk of adverse
events.
5
Introduction
Several myeloid growth factor therapies are currently available for use in the
United States: granulocyte-macrophage colony-stimulating factor (GM-CSF),
granulocyte colony-stimulating factor (G-CSF), IL-3, macrophage colony-stimulating
factor (M-CSF or CSF-1), and stem cell factor (SCF).1, 2
Table 2 provides a summary of
the myeloid growth factor therapies. This review will focus on the erythropoiesis-
stimulating agents (ESAs). Two erythropoiesis-stimulating agents are currently available
for use in the United States: darbepoetin alfa and epoetin alfa.3-7
A third ESA,
peginesatide (Omontys®), was recently recalled (February 2013) as a result of
postmarketing reports of serious hypersensitivity reactions, including life-threatening
anaphylaxis.6, 7
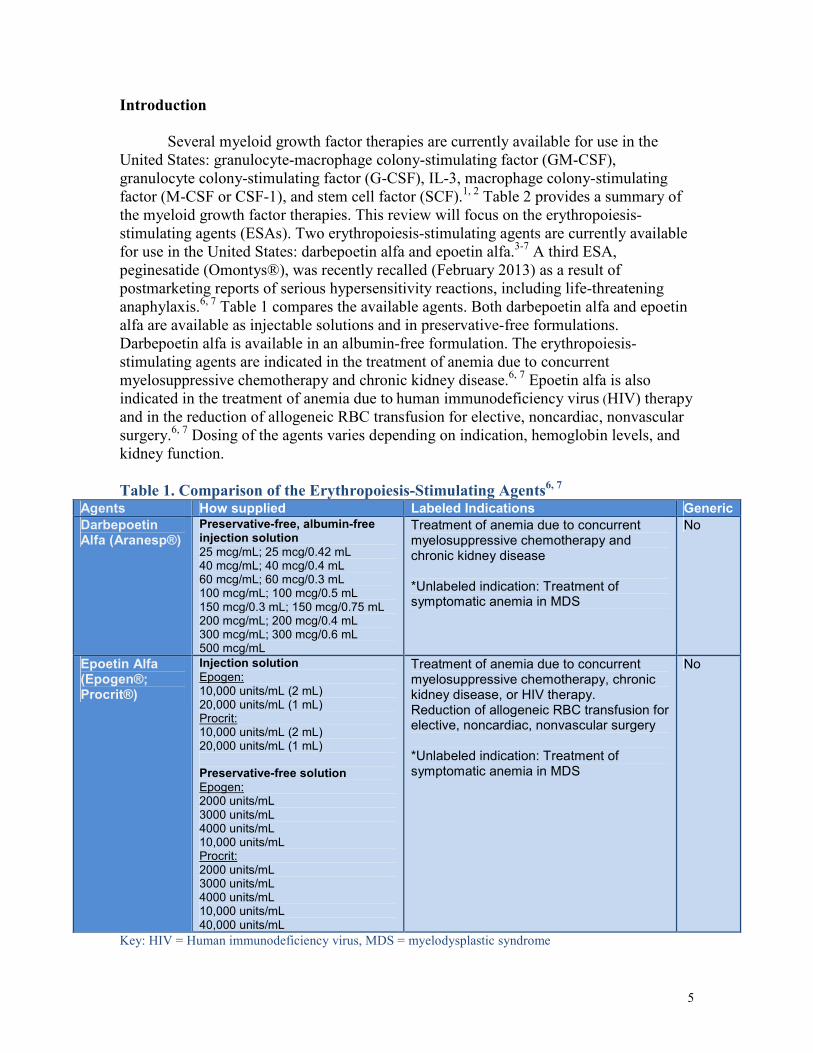
Table 1 compares the available agents. Both darbepoetin alfa and epoetin
alfa are available as injectable solutions and in preservative-free formulations.
Darbepoetin alfa is available in an albumin-free formulation. The erythropoiesis-
stimulating agents are indicated in the treatment of anemia due to concurrent
myelosuppressive chemotherapy and chronic kidney disease.6, 7
Epoetin alfa is also
indicated in the treatment of anemia due to human immunodeficiency virus (HIV) therapy
and in the reduction of allogeneic RBC transfusion for elective, noncardiac, nonvascular
surgery.6, 7
Dosing of the agents varies depending on indication, hemoglobin levels, and
kidney function.
Table 1. Comparison of the Erythropoiesis-Stimulating Agents6, 7
Agents How supplied Labeled Indications Generic
Darbepoetin Alfa (Aranesp®)
Preservative-free, albumin-free injection solution 25 mcg/mL; 25 mcg/0.42 mL 40 mcg/mL; 40 mcg/0.4 mL 60 mcg/mL; 60 mcg/0.3 mL 100 mcg/mL; 100 mcg/0.5 mL 150 mcg/0.3 mL; 150 mcg/0.75 mL 200 mcg/mL; 200 mcg/0.4 mL 300 mcg/mL; 300 mcg/0.6 mL 500 mcg/mL
Treatment of anemia due to concurrent myelosuppressive chemotherapy and chronic kidney disease *Unlabeled indication: Treatment of symptomatic anemia in MDS
No
Epoetin Alfa (Epogen®; Procrit®)
Injection solution Epogen: 10,000 units/mL (2 mL) 20,000 units/mL (1 mL) Procrit: 10,000 units/mL (2 mL) 20,000 units/mL (1 mL) Preservative-free solution Epogen: 2000 units/mL 3000 units/mL 4000 units/mL 10,000 units/mL Procrit: 2000 units/mL 3000 units/mL 4000 units/mL 10,000 units/mL 40,000 units/mL
Treatment of anemia due to concurrent myelosuppressive chemotherapy, chronic kidney disease, or HIV therapy. Reduction of allogeneic RBC transfusion for elective, noncardiac, nonvascular surgery *Unlabeled indication: Treatment of symptomatic anemia in MDS
No
Key: HIV = Human immunodeficiency virus, MDS = myelodysplastic syndrome

6
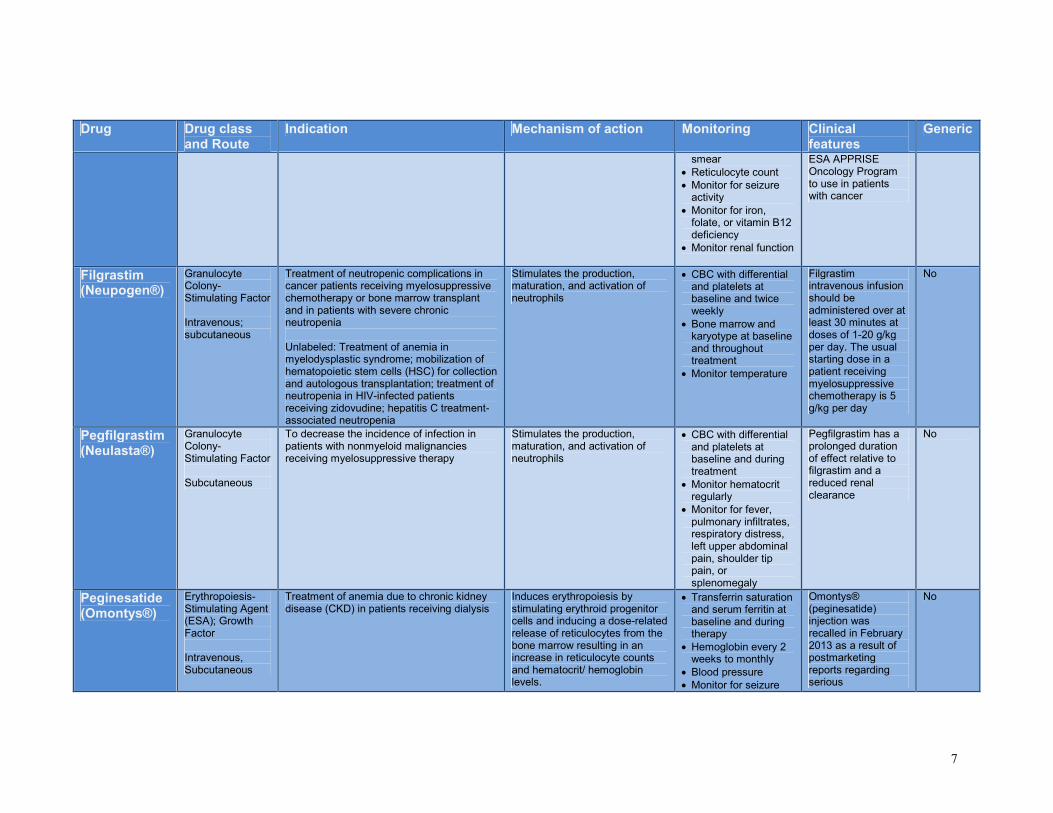
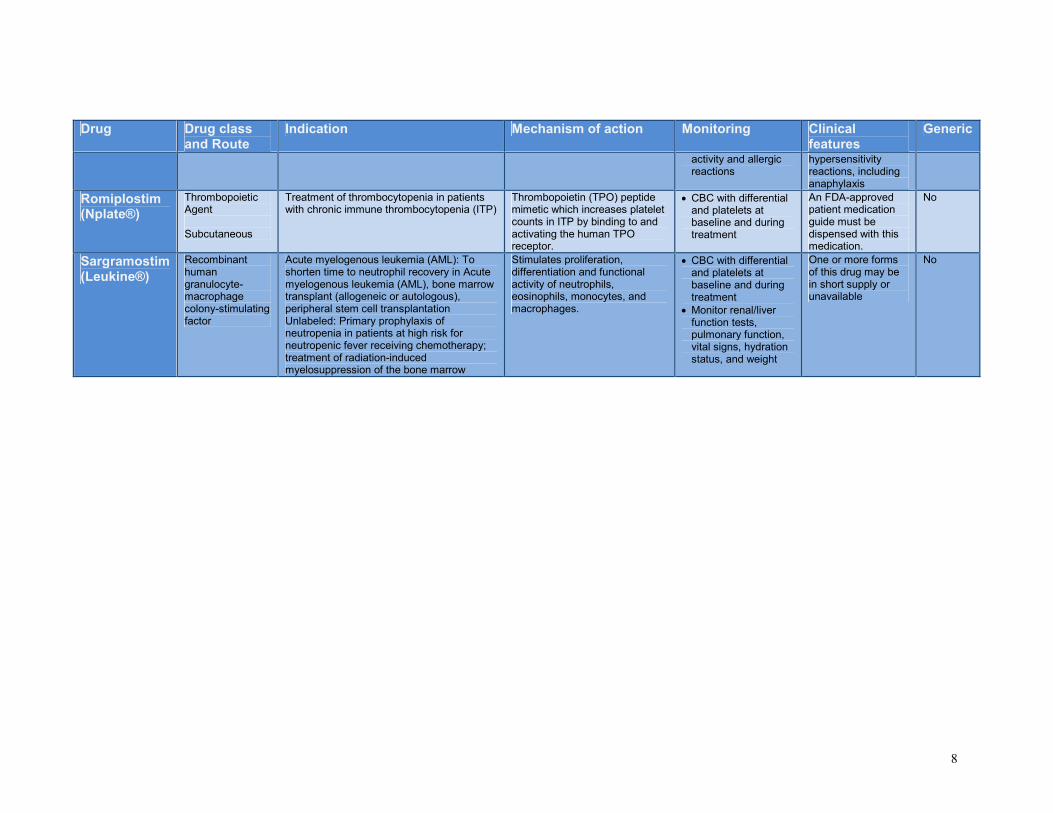
Table 2. Summary of Colony Stimulating Factors1, 2, 6, 7
Drug Drug class
and Route Indication Mechanism of action Monitoring Clinical
features Generic
Darbepoetin Alfa (Aranesp®)
Erythropoiesis-Stimulating Agent (ESA); Growth Factor; Recombinant Human Erythropoietin Intravenous; subcutaneous
Treatment of anemia due to concurrent myelosuppressive chemotherapy in patients with cancer; treatment of anemia due to chronic kidney disease (darbepoetin is not indicated in patients receiving myelosuppressive chemotherapy when the expected outcome is curative Unlabeled: Treatment of symptomatic anemia in myelodysplastic syndrome (MDS)
Induces erythropoiesis by stimulating erythroid progenitor cells and inducing a dose-related release of reticulocytes from the bone marrow resulting in an increase in reticulocyte counts and hematocrit/ hemoglobin levels.
• Hemoglobin weekly to monthly
• Iron stores (transferrin saturation and ferritin) prior to and during therapy
• Serum chemistry
• Blood pressure
• Fluid balance
• Monitor for seizure activity
Supplemental iron intake may be required in patients with low iron stores Access to this medication is restricted. Healthcare providers and hospitals must be enrolled in the ESA APPRISE Oncology Program to use in patients with cancer
No
Eltrombopag (Promacta®)
Thrombopoietic Agent; Thrombopoietin (TPO) nonpeptide agonist Oral
Treatment of thrombocytopenia in patients with chronic immune thrombocytopenia (ITP) or in patients with chronic hepatitis C in order to allow and maintain interferon-based therapy
Binds to and activates human thrombopoietin (TPO) receptor resulting in increased platelet counts. *Does not induce platelet aggregation or activation.
• Liver function tests every 2-4 weeks
• Bilirubin fractionation
• CBC with differential and platelet count weekly to monthly
• Peripheral blood smear at baseline and monthly
• Ophthalmic exam at baseline and during treatment
Take on an empty stomach (food, especially calcium-rich foods and multivitamins with minerals, may decrease the absorption of eltrombopag)
No
Epoetin Alfa (Epogen®; Procrit®)
Erythropoiesis-Stimulating Agent (ESA); Growth Factor; Recombinant Human Erythropoietin Intravenous; subcutaneous
Treatment of anemia due to concurrent myelosuppressive chemotherapy in patients with cancer; treatment of anemia due to chronic kidney disease; treatment of anemia associated with HIV therapy; reduction of allogeneic RBC transfusion for elective, noncardiac, nonvascular surgery (epoetin alfa is not indicated in patients receiving myelosuppressive chemotherapy when the expected outcome is curative Unlabeled: Treatment of symptomatic anemia in myelodysplastic syndrome (MDS)
Induces erythropoiesis by stimulating erythroid progenitor cells and inducing a dose-related release of reticulocytes from the bone marrow resulting in an increase in reticulocyte counts and hematocrit/ hemoglobin levels.
• Transferrin saturation and serum ferritin at baseline and during treatment
• Iron and total iron-binding capacity at baseline and during treatment
• Hemoglobin weekly to monthly
• Blood pressure
• Peripheral blood
Subcutaneous is the preferred route of administration except in patients with CKD on hemodialysis Access to this medication is restricted. Healthcare providers and hospitals must be enrolled in the
No
7
Drug Drug class and Route
Indication Mechanism of action Monitoring Clinical features
Generic
smear
• Reticulocyte count
• Monitor for seizure activity
• Monitor for iron, folate, or vitamin B12 deficiency
• Monitor renal function
ESA APPRISE Oncology Program to use in patients with cancer
Filgrastim (Neupogen®)
Granulocyte Colony-Stimulating Factor Intravenous; subcutaneous
Treatment of neutropenic complications in cancer patients receiving myelosuppressive chemotherapy or bone marrow transplant and in patients with severe chronic neutropenia Unlabeled: Treatment of anemia in myelodysplastic syndrome; mobilization of hematopoietic stem cells (HSC) for collection and autologous transplantation; treatment of neutropenia in HIV-infected patients receiving zidovudine; hepatitis C treatment-associated neutropenia
Stimulates the production, maturation, and activation of neutrophils
• CBC with differential and platelets at baseline and twice weekly
• Bone marrow and karyotype at baseline and throughout treatment
• Monitor temperature
Filgrastim intravenous infusion should be administered over at least 30 minutes at doses of 1-20 g/kg per day. The usual starting dose in a patient receiving myelosuppressive chemotherapy is 5 g/kg per day
No
Pegfilgrastim (Neulasta®)
Granulocyte Colony-Stimulating Factor Subcutaneous
To decrease the incidence of infection in patients with nonmyeloid malignancies receiving myelosuppressive therapy
Stimulates the production, maturation, and activation of neutrophils
• CBC with differential and platelets at baseline and during treatment
• Monitor hematocrit regularly
• Monitor for fever, pulmonary infiltrates, respiratory distress, left upper abdominal pain, shoulder tip pain, or splenomegaly
Pegfilgrastim has a prolonged duration of effect relative to filgrastim and a reduced renal clearance
No
Peginesatide (Omontys®)
Erythropoiesis-Stimulating Agent (ESA); Growth Factor Intravenous, Subcutaneous
Treatment of anemia due to chronic kidney disease (CKD) in patients receiving dialysis
Induces erythropoiesis by stimulating erythroid progenitor cells and inducing a dose-related release of reticulocytes from the bone marrow resulting in an increase in reticulocyte counts and hematocrit/ hemoglobin levels.
• Transferrin saturation and serum ferritin at baseline and during therapy
• Hemoglobin every 2 weeks to monthly
• Blood pressure
• Monitor for seizure
Omontys® (peginesatide) injection was recalled in February 2013 as a result of postmarketing reports regarding serious
No
8
Drug Drug class and Route
Indication Mechanism of action Monitoring Clinical features
Generic
activity and allergic reactions
hypersensitivity reactions, including anaphylaxis
Romiplostim (Nplate®)
Thrombopoietic Agent Subcutaneous
Treatment of thrombocytopenia in patients with chronic immune thrombocytopenia (ITP)
Thrombopoietin (TPO) peptide mimetic which increases platelet counts in ITP by binding to and activating the human TPO receptor.
• CBC with differential and platelets at baseline and during treatment
An FDA-approved patient medication guide must be dispensed with this medication.
No
Sargramostim (Leukine®)
Recombinant human granulocyte-macrophage colony-stimulating factor
Acute myelogenous leukemia (AML): To shorten time to neutrophil recovery in Acute myelogenous leukemia (AML), bone marrow transplant (allogeneic or autologous), peripheral stem cell transplantation Unlabeled: Primary prophylaxis of neutropenia in patients at high risk for neutropenic fever receiving chemotherapy; treatment of radiation-induced myelosuppression of the bone marrow
Stimulates proliferation, differentiation and functional activity of neutrophils, eosinophils, monocytes, and macrophages.
• CBC with differential and platelets at baseline and during treatment
• Monitor renal/liver function tests, pulmonary function, vital signs, hydration status, and weight
One or more forms of this drug may be in short supply or unavailable
No
9
Disease Overview
Anemia affects nearly one third of the world's population.1, 2
Causes of anemia include iron
deficiency, folate deficiencies and other hemoglobinopathies. In the United States, the most common
causes of anemia are iron deficiency, thalassemia, and anemia of chronic disease. Chronic diseases most
frequently associated with anemia in the US are chronic kidney disease (CKD), human
immunodeficiency virus (HIV), rheumatoid arthritis (RA), inflammatory bowel disease (IBD),
congestive heart failure (CHF), and cancer. Anemia is often a sign of an underlying disease process and
is associated with an increased rate of mortality and decreased quality of life.1, 2, 8, 9
Anemia is defined as a reduced concentration of red blood cells (RBCs) reflected by low serum
hemoglobin (Hb).1, 2
The normal range of Hb can vary among different populations (menstruating
women, men, postmenopausal women, etc.) and Hb levels are altered by a number of patient
characteristics, including age, other comorbidities, race, and altitude. The most important function of a
RBC is to transport oxygen. Erythropoiesis is the production of RBCs and occurs continuously within
the body in an attempt to meet the body's demand for oxygen. The average life span of a RBC is 120
days and any process which reduces production, increases destruction, or causes a loss of RBCs will
result in anemia.1, 2
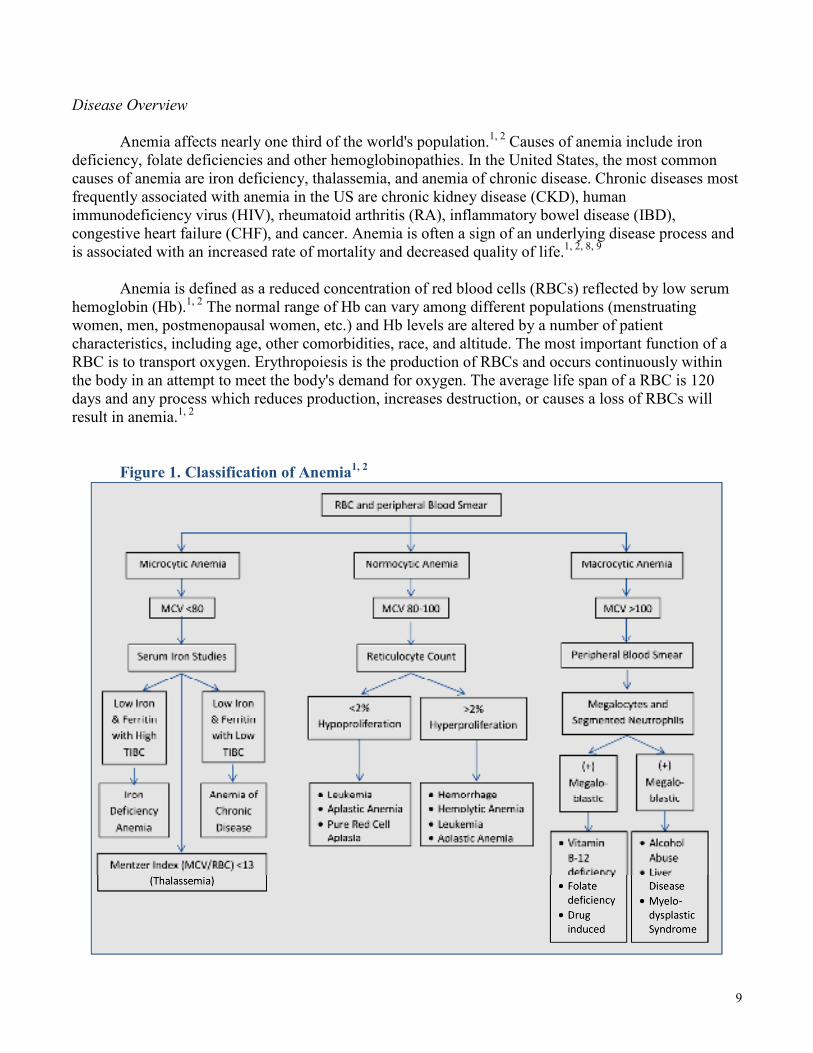
Figure 1. Classification of Anemia1, 2
10
Anemia can be divided into two categories: relative or absolute.1, 2
Relative anemia occurs when
a disturbance in plasma volume regulation occurs with normal total red cell mass. Absolute anemia
occurs when decreased RBC production or increased RBC destruction is accompanied by decreased red
cell mass. Anemia can also be classified by morphologic categories: microcytic anemia, macrocytic
anemia, and normocytic anemia. Figure 1 provides a summary of the morphologic classifications of
anemia. Microcytic anemias are defined by a mean corpuscular volume (MCV) below 80 fL and are
usually a result of iron deficiency, chronic inflammation, or thalassemia. Macrocytic anemias are
defined by a MCV above 100 fL and can be megaloblastic (often seen with vitamin B12 deficiency and
folic acid deficiency) or nonmegaloblastic (often seen with alcoholism, hypothyroidism, and chronic
liver disease). Normocytic anemias are defined by a MCV between 80 and 100 fL and can be hemolytic
(usually resulting from hereditary abnormalities or immune processes) or nonhemolytic (often seen with
renal insufficiency or bone marrow infiltration).1, 2
Treatment of anemia depends on the underlying problem, the symptoms present and the clinical
status of the patient. In addition to treatment of the underlying problem, other treatment options may
include: iron, vitamin B12, folic acid, blood transfusions and hematopoietic growth factors. The
hematopoietic growth factors are hormones which regulate the production and differentiation of
hematopoietic progenitor cells in the bone marrow.1, 2
Erythropoiesis-stimulating agents, darbepoetin
alfa and epoetin alfa, are hematopoietic growth factors which stimulate erythroid proliferation and
differentiation, improve hematocrit and hemoglobin levels, and reduce the need for transfusions. The
erythropoiesis-stimulating agents are used most frequently in the treatment of anemia due to concurrent
myelosuppressive chemotherapy and chronic kidney disease. They may also be used in the treatment of
anemia due to human immunodeficiency virus (HIV) therapy, surgery, prematurity and in the treatment
of symptomatic anemia in myelodysplastic syndrome (MDS). Dosing of the agents varies depending on
indication. Table 3 provides a dosing summary for the ESAs and Table 4 provides dosing conversion
recommendations for epoetin alfa to darbepoetin alfa. During erythropoietin therapy with either agent,
iron deficiency may develop and most patients require iron supplementation and some require folate
supplementation for successful erythropoiesis.1, 2
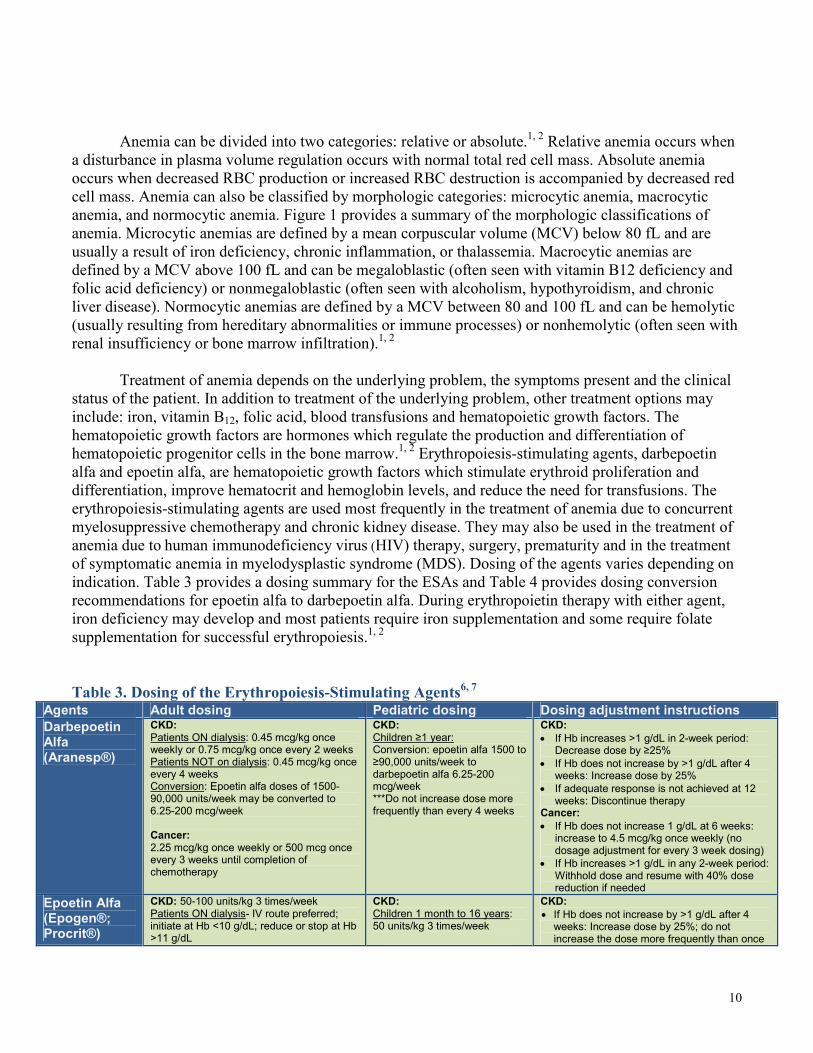
Table 3. Dosing of the Erythropoiesis-Stimulating Agents6, 7
Agents Adult dosing Pediatric dosing Dosing adjustment instructions
Darbepoetin Alfa (Aranesp®)
CKD: Patients ON dialysis: 0.45 mcg/kg once weekly or 0.75 mcg/kg once every 2 weeks Patients NOT on dialysis: 0.45 mcg/kg once every 4 weeks Conversion: Epoetin alfa doses of 1500-90,000 units/week may be converted to 6.25-200 mcg/week Cancer: 2.25 mcg/kg once weekly or 500 mcg once every 3 weeks until completion of chemotherapy
CKD: Children ≥1 year: Conversion: epoetin alfa 1500 to ≥90,000 units/week to darbepoetin alfa 6.25-200 mcg/week ***Do not increase dose more frequently than every 4 weeks
CKD:
• If Hb increases >1 g/dL in 2-week period: Decrease dose by ≥25%
• If Hb does not increase by >1 g/dL after 4 weeks: Increase dose by 25%
• If adequate response is not achieved at 12 weeks: Discontinue therapy
Cancer:
• If Hb does not increase 1 g/dL at 6 weeks: increase to 4.5 mcg/kg once weekly (no dosage adjustment for every 3 week dosing)
• If Hb increases >1 g/dL in any 2-week period: Withhold dose and resume with 40% dose reduction if needed
Epoetin Alfa (Epogen®; Procrit®)
CKD: 50-100 units/kg 3 times/week Patients ON dialysis- IV route preferred; initiate at Hb <10 g/dL; reduce or stop at Hb >11 g/dL
CKD: Children 1 month to 16 years: 50 units/kg 3 times/week
CKD:
• If Hb does not increase by >1 g/dL after 4 weeks: Increase dose by 25%; do not increase the dose more frequently than once

11
Agents Adult dosing Pediatric dosing Dosing adjustment instructions Patients NOT on dialysis- use only if benefits out weight risks, initiate at Hb <10 g/dL and reduce/stop at Hb >10 g/dL Cancer: 150 units/kg 3 times/week or 40,000 units once weekly until completion of chemotherapy ***Initiate only if Hb <10 g/dL and expected duration of myelosuppressive chemotherapy ≥2 months HIV: 100 units/kg 3 times/week Surgery: 300 units/kg per day beginning 10 days before surgery, on the day of surgery, and for 4 days after surgery or 600 units/kg once weekly for 4 doses, given 21- , 14-, and 7 days before surgery, and on the day of surgery ***Perioperative hemoglobin should be 10-13 g/dL; DVT prophylactic anticoagulation is recommended
Cancer: Children ≥5 years: 600 units/kg once weekly until completion of chemotherapy (maximum dose: 60,000 units) HIV: Children 8 months to 17 years: 50-400 units/kg 2-3 times/week (based on limited data)
every 4 weeks
• If Hb increases >1 g/dL in 2-week period: Reduce dose by ≥25%
• Inadequate or lack of response over a 12-week escalation period: Discontinue therapy
Cancer:
• If Hb does not increase by >1 g/dL after 4 weeks: Increase to 300 units/kg 3 times/week or 60,000 units weekly
• If Hb increases >1 g/dL in 2-week period or exceeds target: Withhold dose and resume with 25% dose reduction if needed
• Inadequate response at 8 weeks: Discontinue HIV:
• Hb should not exceed 12 g/dL
• If Hb does not increase after 8 weeks: increase dose by ~50-100 units/kg at 4-8 week intervals; maximum dose: 300 units/kg
• If Hb > 12 g/dL: withhold dose and resume treatment with a 25% dose reduction once hemoglobin <11 g/dL
• If Hb increase is not achieved with 300 units/kg at 8 weeks: Discontinue therapy
Key: Hb = hemoglobin
Table 4. Dosing Conversion Recommendations6, 7
Epoetin alfa dose (units/week)
Darbepoetin alfa dose (mcg/week)*
Adults Children
<1500 6.25 Not established
1500-2499 12.5 6.25
2500-4999 25 10
5000-10,999 40 20
11,000-17,999 60 40
18,000-33,999 100 60
34,000-89,999 200 100
≥90,000 6.25 200
5000-10,999 12.5 Not established
*Epoetin alfa 2-3 times per week = darbepoetin alfa once weekly; Epoetin alfa once
weekly = darbepoetin alfa once every 2 weeks; Darbepoetin dose every 2 weeks is
derived by adding together 2 weekly epoetin alfa doses and then converting to the
appropriate darbepoetin dose
The National Kidney Foundation has published detailed guidelines for use of erythropoietin
stimulating agents in patients with anemia associated with chronic renal diseases. National Kidney
Foundation’s Kidney Disease Outcomes Quality Initiative (KDOQI) updated 2007 guidelines state that
each of the ESAs are effective in achieving and maintaining target Hb levels in patients with chronic
kidney disease (CKD).10
KDOQI recommends the decision to initiate ESA therapy should include
careful consideration of potential benefits (improving quality of life, prevent transfusion, etc.) and
potential harms (life threatening cardiovascular and thrombotic adverse events). According to the
guidelines, target hemoglobin range in dialysis and nondialysis patients with CKD receiving ESA
therapy, should be 11-12 g/dL and should not exceed 13.0 g/dL.

12
Erythropoiesis-stimulating agent therapy in the treatment of anemia due to concurrent
myelosuppressive chemotherapy may be associated with an increased risk of thrombosis, decreased
survival, and shortened time to tumor. The most recent National Comprehensive Cancer Network
(NCCN, 2013) guidelines recommend ESA use is limited to the lowest possible dose and duration to
avoid adverse effects while maintaining hemoglobin levels sufficient to avoid a blood transfusion.11
ESA therapy is not recommended in patients receiving myelosuppressive chemotherapy with curative
intent. The current American Society of Clinical Oncology (ASCO) and the American Society of
Hematology (ASH) joint clinical practice guidelines for the use of erythropoiesis stimulating agents
(ESAs) in patients with cancer (2010) recommend ESA use is guided by clinical judgment, risks and
benefits of ESA therapy, and patient preference.12
Both darbepoetin alfa and epoetin alfa are
recommended as effective treatment options when ESA therapy is indicated. In general, ESA therapy in
patients with chemotherapy-associated anemia should be initiated when Hb levels are 10-12 g/dL.
Erythropoietin stimulating agents may also be used to offset anemia associated with
myelodysplastic syndrome, rheumatoid arthritis, chronic heart failure, prematurity, non-cardiac/non-
vascular surgery and HIV therapy (specifically zidovudine treatment).13, 14
Conservative hemoglobin
targets (<12 g/dL), reduced doses of ESAs and more frequent monitoring should be considered when
administering ESA therapy in these patient populations. Epoetin alfa is the only agent with labeled
indications for use in anemia associated with non-cardiac/non-vascular surgery and HIV therapy.
Pharmacology/Pharmacokinetics1-7
Erythropoietin (EPO) is a hormone produced by the kidneys which interacts with erythropoietin
receptors on hematopoietic progenitor cells and stimulates RBC production and differentiation.
Recombinant human erythropoietin (epoetin alfa) is nearly identical to the endogenous hormone and
results in the same effects. Darbepoetin alfa is a modified version of erythropoietin with additional
carbohydrate side chains used to prolong the action of the drug. When administered intravenously,
epoetin alfa has a serum half-life of 4-12 hours and darbepoetin alfa has a serum half-life 2-3 times
longer. In general, epoetin alfa is administered three times a week and darbepoetin is administered once
weekly. Both agents may also be administered subcutaneously with similar outcomes. Adequate iron
supplies are required for sustained erythropoiesis and most patients receive supplemental iron when
receiving ESA therapy. Recombinant human erythropoietin is banned by the International Olympic
Committee because use by athletes will increase oxygen delivery to muscles and may improve
performance.
Table 5. Pharmacokinetics of the Erythropoiesis-Stimulating Agents3-5
Agents Absorption Distribution Bioavailability Half-life Time-to-peak
Darbepoetin Alfa (Aranesp®)
SubQ: Slow Vd: 0.06 L/kg
SubQ: Adults: 30-50% Children: 32-70%
IV: 21 hrs SubQ: Nondialysis patients: 24-144 hrs Dialysis patients: 12-89 hrs
CKD: Adults: 12-72 hrs Children: 10-58 hrs Cancer: Adults: 28-123 hrs Children: 21-143 hrs

13
Epoetin Alfa (Epogen®; Procrit®)
Several days
Vd: 9 L/kg SubQ: ~21-31% SubQ: Cancer: 16-67 hrs IV: CKD: 4-13 hrs
CKD: SubQ: 5-24 hrs Peak effect on Hb level: 2-6 weeks
Key: SubQ = subcutaneous; IV = intravenous; hrs = hours; CKD = chronic kidney disease; Hb = hemoglobin
Methods
A literature search was conducted to identify comparative clinical trials, searching the
MEDLINE database (1950 – 2013), the Cochrane Library, and reference lists of review articles. For the
clinical efficacy section, only clinical trials published in English and indexed on MEDLINE prior to
8/2013, evaluating efficacy of the erythropoiesis-stimulating agents are included. Trials evaluating the
erythropoiesis-stimulating agents as monotherapy or combination therapy where adjunctive medications
remained constant throughout the trial are included. Trials comparing monotherapy with combination
regimens are excluded. The following reports were excluded (note: some were excluded for more than 1
reason):
• Clinical trials which evaluated pharmacokinetic studies15
, secondary outcomes16-19
, or cost
analyses20-24
• Individual trials involving indirect comparison analyses17, 19, 20, 23-32
• Trials involving dose-finding studies20-23, 28, 31, 33-35
• Individual clinical trials evaluating formulations not currently available in the US33, 34
Clinical Efficacy
The efficacy of the erythropoiesis-stimulating agents was directly compared in five clinical
trials.22, 36-41
An evidence table outlining the comparative trials is included in the appendix. Overall,
achievement of target hemoglobin (Hb) level, incidence of red blood cell (RBC) transfusion and rate of
adverse events were similar between the two erythropoiesis-stimulating agents, darbepoetin and epoetin.
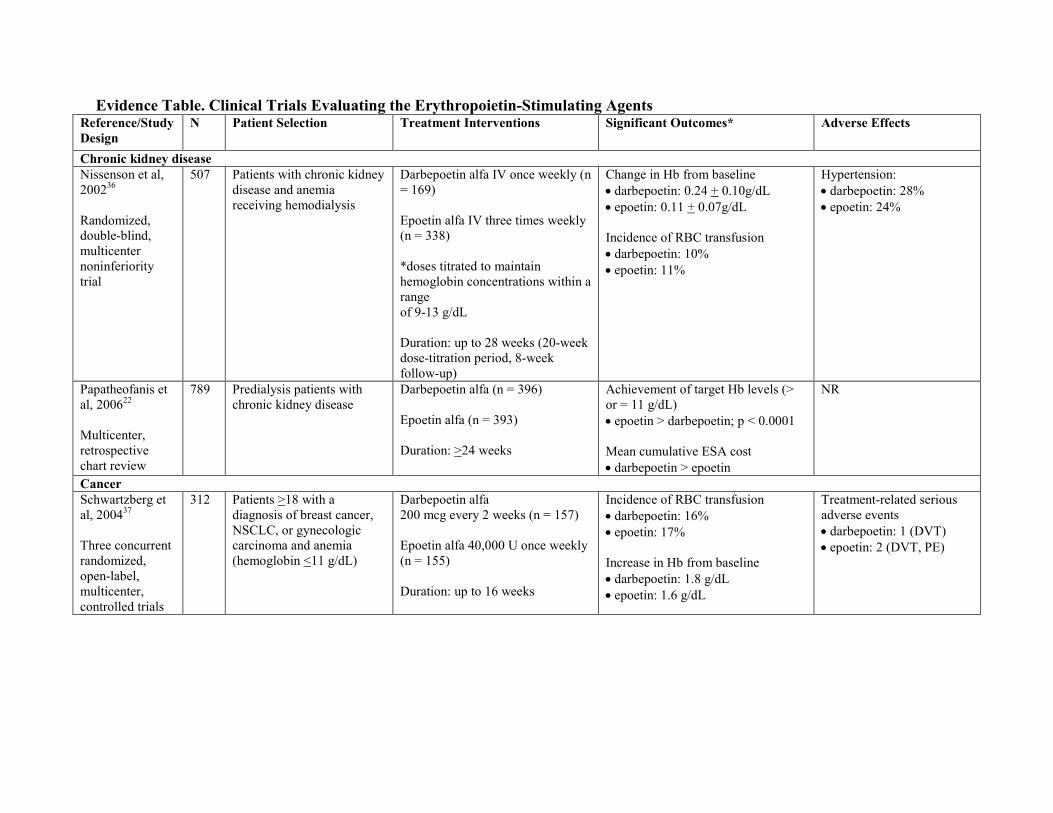
Chronic Kidney Disease
One randomized, controlled trial and one observational trial are available for evaluation of the
ESAs in patients with chronic kidney disease and anemia with a hemoglobin level <11 g/dL. Nissenson
et al36
conducted a randomized, double-blind, noninferiority study evaluating 507 hemodialysis patients
randomized to receive intravenous (IV) epoetin three times weekly or IV darbepoetin once weekly.
Doses of the agents were titrated over a 21 week period to maintain Hb concentrations within -1 to +1.5
g/dL of baseline and within a range of 9 to 13 g/dL. Mean changes in Hb levels from baseline were
clinically insignificant (0.11-0.24) and similar between the agents. No differences in safety were
reported between treatment groups. Papatheofanis et al22
completed a retrospective chart review of 789
predialysis patients with anemia. According to the observational review, epoetin treatment was
associated with a statistically significant increase in achievement of target Hb (>11 g/dL) at weeks 4, 8,
and 12. All patients in both treatment groups achieved target Hb levels by the end of the study period
(24 weeks). Transfusion frequency and adverse event rates were not reported.
14
Cancer chemotherapy
Four randomized, controlled trials and one observational trial are available for evaluation of the
ESAs in patients receiving chemotherapy who have anemia with a hemoglobin level <11 g/dL.
Darbepoetin 200 mcg every 2 weeks was compared to epoetin 40,000 units once weekly in each of the 4
randomized controlled trials. Schwartzberg et al37
conducted three concurrent, randomized open-label
trials evaluating 312 patients with cancer who were randomized to receive darbepoetin or epoetin for up
to 16 weeks. Both agents demonstrated efficacy in increasing Hb levels from baseline (mean change in
hb 1.4-1.5). No differences in incidence of RBC transfusion or rate of adverse events were reported
between treatment groups. Senecal et al38
evaluated the efficacy of the ESAs in 141 patients with breast
cancer and anemia over a 16 week period. According to the data, incidence of RBC transfusions, mean
changes in Hb, and hematopoietic responses were improved and similar between treatment groups.
Waltzman et al39
evaluated 358 patients receiving chemotherapy and either darbepoetin or epoetin over
9 weeks. Increase in Hb level of 1-2 g/dL occurred more frequently in the epoetin treatment group (~47-
57%) compared to the darbepoetin treatment group (~32-41%; p < 0.008); however, no differences in
transfusion rates were reported between treatment groups. Glaspy et al40
conducted a large randomized,
controlled, non-inferiority trial of 1220 patients with nonmyeloid malignancy and Hb < 11g/dL. Patients
were randomized to receive darbepoetin or epoetin for up to 16 weeks. No differences in incidence of
RBC transfusion or achievement of target Hb level were reported between treatment groups. A single
observational study evaluating 540 patients with chemotherapy-induced anemia found an increased rate
of RBC transfusion with darbepoetin treatment (22.5%) compared to epoetin treatment (13.9%; p =
0.026).41
Thromboembolic events and other adverse events were similar across treatment groups in all of
the above comparative studies.
Summary
The erythropoietin-stimulating agents are effective in achieving and maintaining Hb levels
sufficient to avoid RBC transfusions in patients with anemia associated with CKD or cancer
chemotherapy. Based on the available comparative clinical evidence, darbepoetin and epoetin appear to
have comparable safety and efficacy in these patient populations. To reduce risk of adverse events, the
lowest possible dose to gradually increase the hemoglobin concentrations to a level sufficient to avoid
the need for RBC transfusion should be used. In general, therapy with an ESA should be individualized
to achieve and maintain hemoglobin levels within the range of 10 to 12 g/dL.
Special Populations
Pediatrics6, 7
Limited data is available for ESA use in pediatric patients. Epoetin multidose vials are
contraindicated in neonates and infants due to the presence of benzyl alcohol in multidose vials.
Pharmacokinetic profiles of epoetin are similar in both adults and children and epoetin is labeled for the
treatment of anemia in pediatric patients with CKD who are 1 month or older and in pediatric patients
with cancer who are 5 years or older. Limited data are available to support the use of epoetin in patients
eight months or older who are treated with zidovudine for HIV infection. Safety and efficacy of
darbepoetin have not been established in the initial treatment of pediatric patients with CKD or
chemotherapy-induced anemia. A study of the conversion of epoetin to darbepoetin in pediatric patients
with CKD over one year of age showed similar rates of safety and efficacy as found in adult conversion
studies. Darbepoetin pharmacokinetic studies suggest higher bioavailablity and lower doses of
darbepoetin are required in pediatric patients.
15
Geriatrics6, 7
Limited data are available evaluating patients age 65 or older in clinical studies of epoetin or
darbepoetin in the treatment of anemia associated with CKD, cancer chemotherapy, and zidovudine-
treatment of HIV infection. Careful monitoring of Hb levels, blood pressure, and adverse events are
required in geriatric patients.
Adverse Drug Reactions
The most common adverse effects associated with ESA therapy are hypertension and
thromboembolic complications.6, 7
The Food and Drug Administration (FDA) has issued a warning for
increased risk of a thrombotic event in patients with CKD or cancer whose Hb is greater than 12 g/dL
(2007).42-44
In 2011, the FDA published an additional safety alert warning on all ESAs of increased risk
of death, cardiovascular events, and stroke in CKD patients with Hb levels > 11 g/dL. Patients receiving
hemodialysis and epoetin alfa or darbepoetin may require increased anticoagulation. Hypertension
occurs in about 20-30% of patients receiving ESA therapy and usually occurs as a result of a rapid
increase in hematocrit. Blood pressure may be controlled by ultrafiltration in dialysis patients, by
reducing the ESA dose or by increasing antihypertensive therapy. ESAs should not be used in patients
with preexisting uncontrolled hypertension.
Headache, tachycardia, edema, shortness of breath, nausea, vomiting, diarrhea, injection site
reaction, and flu-like symptoms (e.g., arthralgias and myalgias) have also been reported in patients
receiving ESA therapy.6, 7
Allergic reactions to ESAs have been infrequent. Darbepoetin is
contraindicated in patients with hypersensitivity to albumin or mammalian cell-derived products. There
have been a small number of cases of pure red cell aplasia (PRCA) accompanied by neutralizing
antibodies to erythropoietin. ESAs should be used at the lowest dose to avoid transfusions and not to
exceed a hemoglobin level of 12g/dL. The ESAs may only be prescribed under a risk evaluation and
mitigation strategy (REMS) program when used in patients with cancer which requires a medication
guide outlining the risks provided to each patient receiving an ESA and a written acknowledgement of
the risks by both the patient and the provider.
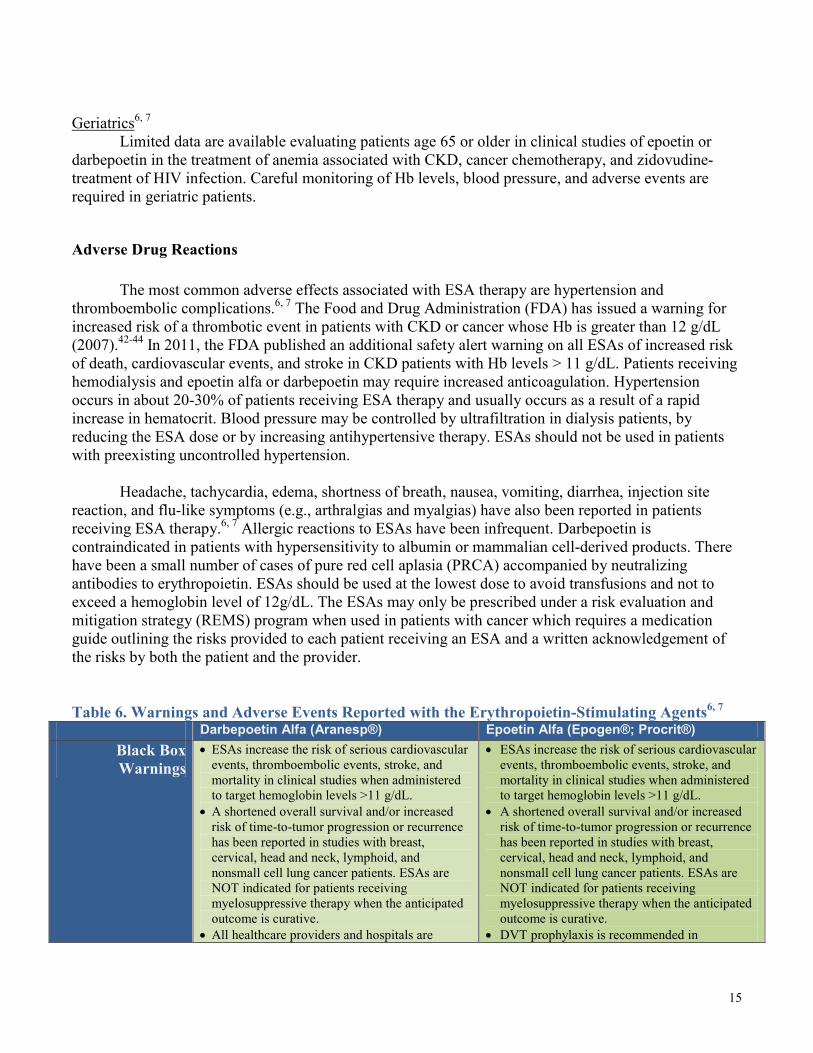
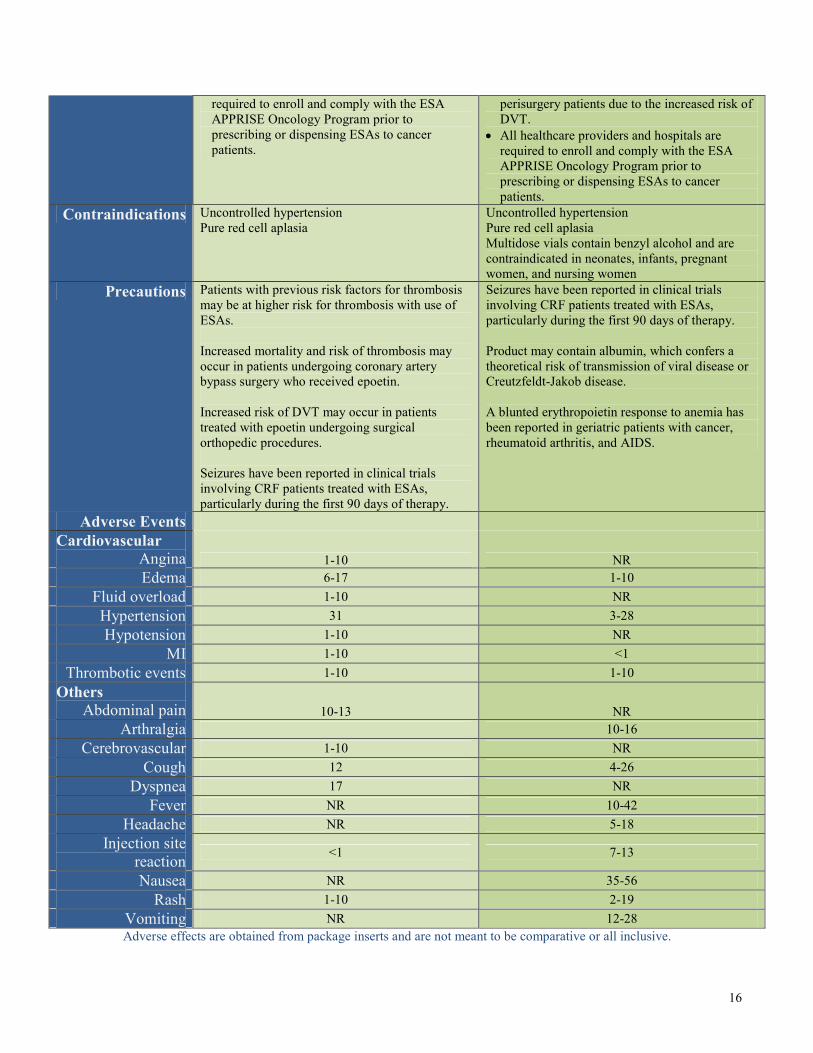
Table 6. Warnings and Adverse Events Reported with the Erythropoietin-Stimulating Agents6, 7
Darbepoetin Alfa (Aranesp®) Epoetin Alfa (Epogen®; Procrit®)
Black Box
Warnings
• ESAs increase the risk of serious cardiovascular
events, thromboembolic events, stroke, and
mortality in clinical studies when administered
to target hemoglobin levels >11 g/dL.
• A shortened overall survival and/or increased
risk of time-to-tumor progression or recurrence
has been reported in studies with breast,
cervical, head and neck, lymphoid, and
nonsmall cell lung cancer patients. ESAs are
NOT indicated for patients receiving
myelosuppressive therapy when the anticipated
outcome is curative.
• All healthcare providers and hospitals are
• ESAs increase the risk of serious cardiovascular
events, thromboembolic events, stroke, and
mortality in clinical studies when administered
to target hemoglobin levels >11 g/dL.
• A shortened overall survival and/or increased
risk of time-to-tumor progression or recurrence
has been reported in studies with breast,
cervical, head and neck, lymphoid, and
nonsmall cell lung cancer patients. ESAs are
NOT indicated for patients receiving
myelosuppressive therapy when the anticipated
outcome is curative.
• DVT prophylaxis is recommended in
16
required to enroll and comply with the ESA
APPRISE Oncology Program prior to
prescribing or dispensing ESAs to cancer
patients.
perisurgery patients due to the increased risk of
DVT.
• All healthcare providers and hospitals are
required to enroll and comply with the ESA
APPRISE Oncology Program prior to
prescribing or dispensing ESAs to cancer
patients.
Contraindications Uncontrolled hypertension
Pure red cell aplasia
Uncontrolled hypertension
Pure red cell aplasia
Multidose vials contain benzyl alcohol and are
contraindicated in neonates, infants, pregnant
women, and nursing women
Precautions Patients with previous risk factors for thrombosis
may be at higher risk for thrombosis with use of
ESAs.
Increased mortality and risk of thrombosis may
occur in patients undergoing coronary artery
bypass surgery who received epoetin.
Increased risk of DVT may occur in patients
treated with epoetin undergoing surgical
orthopedic procedures.
Seizures have been reported in clinical trials
involving CRF patients treated with ESAs,
particularly during the first 90 days of therapy.
Seizures have been reported in clinical trials
involving CRF patients treated with ESAs,
particularly during the first 90 days of therapy.
Product may contain albumin, which confers a
theoretical risk of transmission of viral disease or
Creutzfeldt-Jakob disease.
A blunted erythropoietin response to anemia has
been reported in geriatric patients with cancer,
rheumatoid arthritis, and AIDS.
Adverse Events
Cardiovascular
Angina 1-10 NR
Edema 6-17 1-10
Fluid overload 1-10 NR
Hypertension 31 3-28
Hypotension 1-10 NR
MI 1-10 <1
Thrombotic events 1-10 1-10
Others
Abdominal pain 10-13 NR
Arthralgia 10-16
Cerebrovascular 1-10 NR
Cough 12 4-26
Dyspnea 17 NR
Fever NR 10-42
Headache NR 5-18
Injection site
reaction <1 7-13
Nausea NR 35-56
Rash 1-10 2-19
Vomiting NR 12-28
Adverse effects are obtained from package inserts and are not meant to be comparative or all inclusive.

17
NR = not reported
Summary
Anemia affects nearly one third of the world's population and is associated with an increased rate
of mortality and decreased physical functioning and quality of life. Treatment of anemia depends on the
underlying problem and may include an erythropoiesis-stimulating agent. Two erythropoiesis-
stimulating agents are currently available for use in the United States: darbepoetin alfa and epoetin alfa.
The erythropoiesis-stimulating agents stimulate erythroid proliferation and differentiation, improve
hematocrit and hemoglobin levels, and reduce the need for transfusions. Both agents are indicated in the
treatment of anemia due to myelosuppressive chemotherapy and chronic kidney disease. Epoetin alfa is
also indicated in the treatment of anemia due to human immunodeficiency virus therapy and in the
reduction of transfusion in elective surgery. Adequate iron supplies are required for sustained
erythropoiesis and supplemental iron is often recommended with ESA therapy. Guidelines for use of
ESA in anemia associated with chronic kidney disease or cancer chemotherapy, recommend the lowest
possible dose should be used to gradually increase the hemoglobin concentrations to a level sufficient to
avoid the need for RBC transfusion.
The efficacy of the erythropoiesis-stimulating agents was directly compared in five randomized
controlled trials and two observational trials. Two trials examined ESA use in anemia associated with
chronic kidney disease and 5 trials examined ESA use in anemia associated with cancer chemotherapy.
No comparative clinical evidence is available for ESA use in anemia associated with noncardiac surgery
or HIV therapy. Based on the available evidence, darbepoetin and epoetin are effective in achieving and
maintaining Hb levels sufficient to avoid RBC transfusions in patients with anemia associated with CKD
or cancer chemotherapy. The agents appear to have comparable safety and efficacy in these patient
populations. Limited data are available evaluating ESA use in special populations. Careful monitoring of
Hb levels, blood pressure, and adverse events are required in pediatric and geriatric patients receiving
ESA therapy.
The most common adverse effects associated with ESA therapy are hypertension and
thromboembolic complications. The FDA has issued a warning for increased risk of thrombotic and
cardiovascular events in patients receiving an ESA with Hb levels > 11 g/dL. Hypertension occurs in
about 20-30% of patients receiving ESA therapy, usually occurs as a result of a rapid increase in
hematocrit and ESA use is contraindicated in patients with preexisting uncontrolled hypertension.
Headache, tachycardia, edema, shortness of breath, nausea, vomiting, diarrhea, injection site reaction,
and flu-like symptoms have also been reported in patients receiving ESA therapy. The ESAs may only
be prescribed under the REMS program. In general, therapy with an ESA should be individualized to
achieve and maintain hemoglobin levels within the range of 10 to 12 g/dL in order to avoid a RBC
transfusion while limiting risk of adverse events.
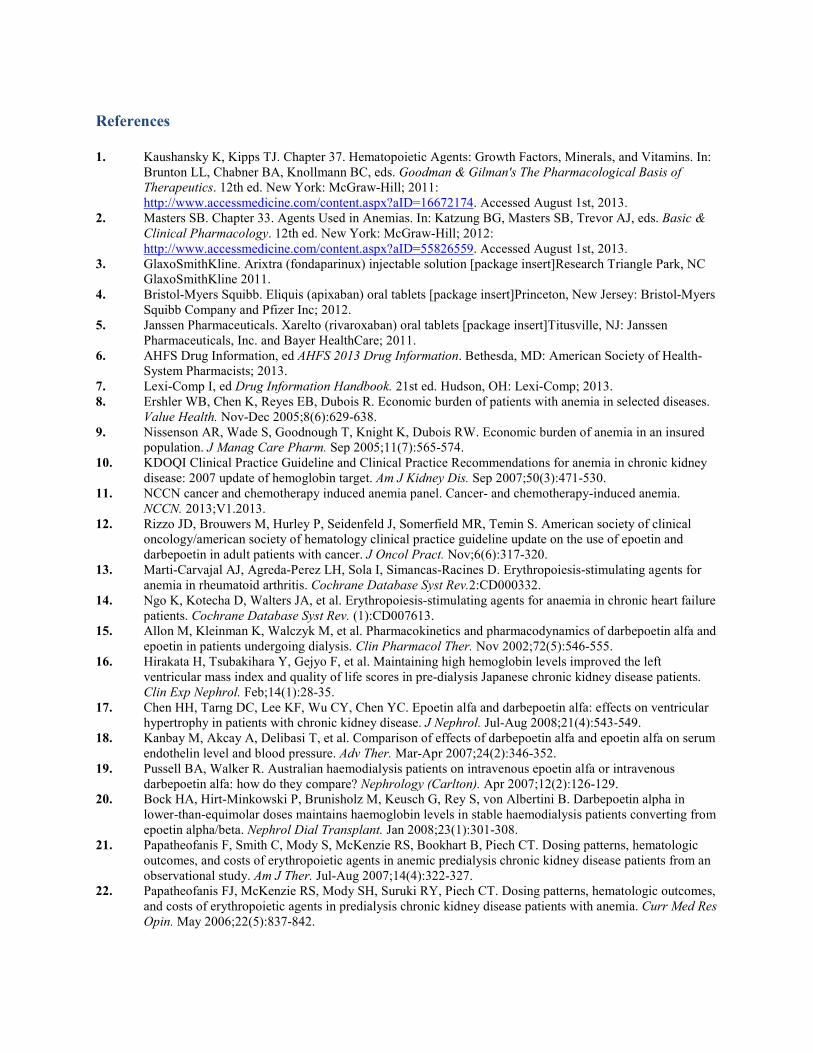
References
1. Kaushansky K, Kipps TJ. Chapter 37. Hematopoietic Agents: Growth Factors, Minerals, and Vitamins. In:
Brunton LL, Chabner BA, Knollmann BC, eds. Goodman & Gilman's The Pharmacological Basis of
Therapeutics. 12th ed. New York: McGraw-Hill; 2011:
http://www.accessmedicine.com/content.aspx?aID=16672174. Accessed August 1st, 2013.
2. Masters SB. Chapter 33. Agents Used in Anemias. In: Katzung BG, Masters SB, Trevor AJ, eds. Basic &
Clinical Pharmacology. 12th ed. New York: McGraw-Hill; 2012:
http://www.accessmedicine.com/content.aspx?aID=55826559. Accessed August 1st, 2013.
3. GlaxoSmithKline. Arixtra (fondaparinux) injectable solution [package insert]Research Triangle Park, NC
GlaxoSmithKline 2011.
4. Bristol-Myers Squibb. Eliquis (apixaban) oral tablets [package insert]Princeton, New Jersey: Bristol-Myers
Squibb Company and Pfizer Inc; 2012.
5. Janssen Pharmaceuticals. Xarelto (rivaroxaban) oral tablets [package insert]Titusville, NJ: Janssen
Pharmaceuticals, Inc. and Bayer HealthCare; 2011.
6. AHFS Drug Information, ed AHFS 2013 Drug Information. Bethesda, MD: American Society of Health-
System Pharmacists; 2013.
7. Lexi-Comp I, ed Drug Information Handbook. 21st ed. Hudson, OH: Lexi-Comp; 2013.
8. Ershler WB, Chen K, Reyes EB, Dubois R. Economic burden of patients with anemia in selected diseases.
Value Health. Nov-Dec 2005;8(6):629-638.
9. Nissenson AR, Wade S, Goodnough T, Knight K, Dubois RW. Economic burden of anemia in an insured
population. J Manag Care Pharm. Sep 2005;11(7):565-574.
10. KDOQI Clinical Practice Guideline and Clinical Practice Recommendations for anemia in chronic kidney
disease: 2007 update of hemoglobin target. Am J Kidney Dis. Sep 2007;50(3):471-530.
11. NCCN cancer and chemotherapy induced anemia panel. Cancer- and chemotherapy-induced anemia.
NCCN. 2013;V1.2013.
12. Rizzo JD, Brouwers M, Hurley P, Seidenfeld J, Somerfield MR, Temin S. American society of clinical
oncology/american society of hematology clinical practice guideline update on the use of epoetin and
darbepoetin in adult patients with cancer. J Oncol Pract. Nov;6(6):317-320.
13. Marti-Carvajal AJ, Agreda-Perez LH, Sola I, Simancas-Racines D. Erythropoiesis-stimulating agents for
anemia in rheumatoid arthritis. Cochrane Database Syst Rev.2:CD000332.
14. Ngo K, Kotecha D, Walters JA, et al. Erythropoiesis-stimulating agents for anaemia in chronic heart failure
patients. Cochrane Database Syst Rev. (1):CD007613.
15. Allon M, Kleinman K, Walczyk M, et al. Pharmacokinetics and pharmacodynamics of darbepoetin alfa and
epoetin in patients undergoing dialysis. Clin Pharmacol Ther. Nov 2002;72(5):546-555.
16. Hirakata H, Tsubakihara Y, Gejyo F, et al. Maintaining high hemoglobin levels improved the left
ventricular mass index and quality of life scores in pre-dialysis Japanese chronic kidney disease patients.
Clin Exp Nephrol. Feb;14(1):28-35.
17. Chen HH, Tarng DC, Lee KF, Wu CY, Chen YC. Epoetin alfa and darbepoetin alfa: effects on ventricular
hypertrophy in patients with chronic kidney disease. J Nephrol. Jul-Aug 2008;21(4):543-549.
18. Kanbay M, Akcay A, Delibasi T, et al. Comparison of effects of darbepoetin alfa and epoetin alfa on serum
endothelin level and blood pressure. Adv Ther. Mar-Apr 2007;24(2):346-352.
19. Pussell BA, Walker R. Australian haemodialysis patients on intravenous epoetin alfa or intravenous
darbepoetin alfa: how do they compare? Nephrology (Carlton). Apr 2007;12(2):126-129.
20. Bock HA, Hirt-Minkowski P, Brunisholz M, Keusch G, Rey S, von Albertini B. Darbepoetin alpha in
lower-than-equimolar doses maintains haemoglobin levels in stable haemodialysis patients converting from
epoetin alpha/beta. Nephrol Dial Transplant. Jan 2008;23(1):301-308.
21. Papatheofanis F, Smith C, Mody S, McKenzie RS, Bookhart B, Piech CT. Dosing patterns, hematologic
outcomes, and costs of erythropoietic agents in anemic predialysis chronic kidney disease patients from an
observational study. Am J Ther. Jul-Aug 2007;14(4):322-327.
22. Papatheofanis FJ, McKenzie RS, Mody SH, Suruki RY, Piech CT. Dosing patterns, hematologic outcomes,
and costs of erythropoietic agents in predialysis chronic kidney disease patients with anemia. Curr Med Res
Opin. May 2006;22(5):837-842.
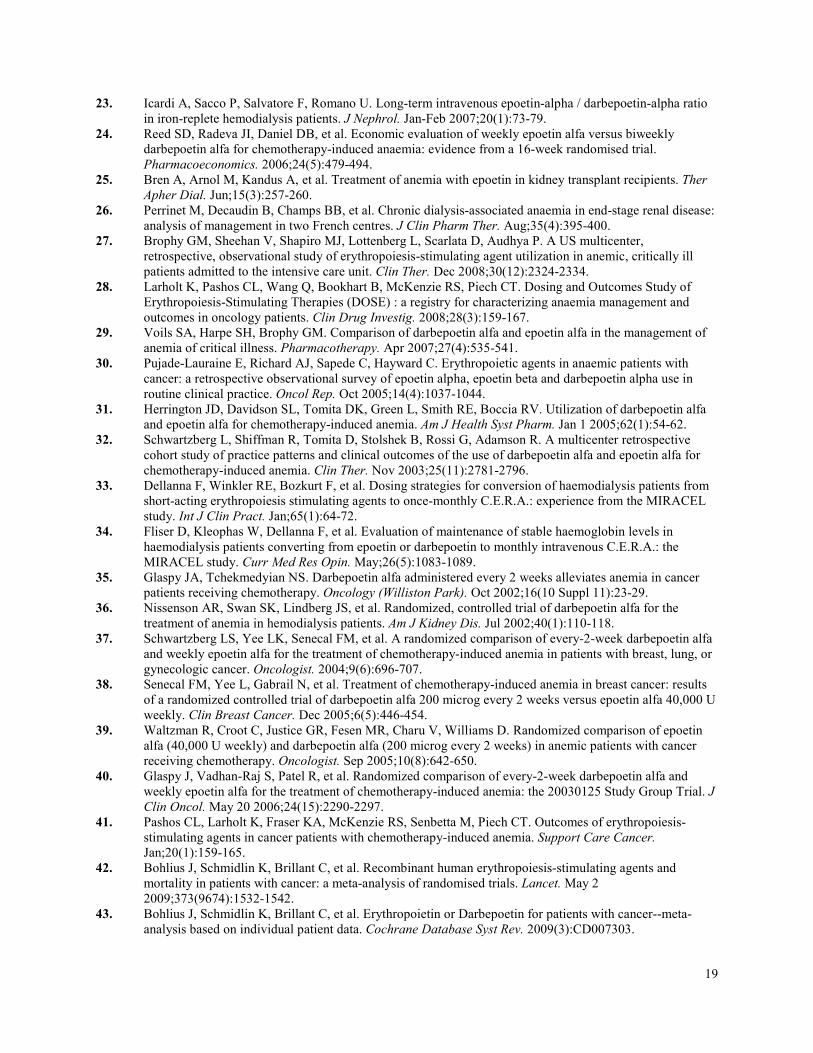
19
23. Icardi A, Sacco P, Salvatore F, Romano U. Long-term intravenous epoetin-alpha / darbepoetin-alpha ratio
in iron-replete hemodialysis patients. J Nephrol. Jan-Feb 2007;20(1):73-79.
24. Reed SD, Radeva JI, Daniel DB, et al. Economic evaluation of weekly epoetin alfa versus biweekly
darbepoetin alfa for chemotherapy-induced anaemia: evidence from a 16-week randomised trial.
Pharmacoeconomics. 2006;24(5):479-494.
25. Bren A, Arnol M, Kandus A, et al. Treatment of anemia with epoetin in kidney transplant recipients. Ther
Apher Dial. Jun;15(3):257-260.
26. Perrinet M, Decaudin B, Champs BB, et al. Chronic dialysis-associated anaemia in end-stage renal disease:
analysis of management in two French centres. J Clin Pharm Ther. Aug;35(4):395-400.
27. Brophy GM, Sheehan V, Shapiro MJ, Lottenberg L, Scarlata D, Audhya P. A US multicenter,
retrospective, observational study of erythropoiesis-stimulating agent utilization in anemic, critically ill
patients admitted to the intensive care unit. Clin Ther. Dec 2008;30(12):2324-2334.
28. Larholt K, Pashos CL, Wang Q, Bookhart B, McKenzie RS, Piech CT. Dosing and Outcomes Study of
Erythropoiesis-Stimulating Therapies (DOSE) : a registry for characterizing anaemia management and
outcomes in oncology patients. Clin Drug Investig. 2008;28(3):159-167.
29. Voils SA, Harpe SH, Brophy GM. Comparison of darbepoetin alfa and epoetin alfa in the management of
anemia of critical illness. Pharmacotherapy. Apr 2007;27(4):535-541.
30. Pujade-Lauraine E, Richard AJ, Sapede C, Hayward C. Erythropoietic agents in anaemic patients with
cancer: a retrospective observational survey of epoetin alpha, epoetin beta and darbepoetin alpha use in
routine clinical practice. Oncol Rep. Oct 2005;14(4):1037-1044.
31. Herrington JD, Davidson SL, Tomita DK, Green L, Smith RE, Boccia RV. Utilization of darbepoetin alfa
and epoetin alfa for chemotherapy-induced anemia. Am J Health Syst Pharm. Jan 1 2005;62(1):54-62.
32. Schwartzberg L, Shiffman R, Tomita D, Stolshek B, Rossi G, Adamson R. A multicenter retrospective
cohort study of practice patterns and clinical outcomes of the use of darbepoetin alfa and epoetin alfa for
chemotherapy-induced anemia. Clin Ther. Nov 2003;25(11):2781-2796.
33. Dellanna F, Winkler RE, Bozkurt F, et al. Dosing strategies for conversion of haemodialysis patients from
short-acting erythropoiesis stimulating agents to once-monthly C.E.R.A.: experience from the MIRACEL
study. Int J Clin Pract. Jan;65(1):64-72.
34. Fliser D, Kleophas W, Dellanna F, et al. Evaluation of maintenance of stable haemoglobin levels in
haemodialysis patients converting from epoetin or darbepoetin to monthly intravenous C.E.R.A.: the
MIRACEL study. Curr Med Res Opin. May;26(5):1083-1089.
35. Glaspy JA, Tchekmedyian NS. Darbepoetin alfa administered every 2 weeks alleviates anemia in cancer
patients receiving chemotherapy. Oncology (Williston Park). Oct 2002;16(10 Suppl 11):23-29.
36. Nissenson AR, Swan SK, Lindberg JS, et al. Randomized, controlled trial of darbepoetin alfa for the
treatment of anemia in hemodialysis patients. Am J Kidney Dis. Jul 2002;40(1):110-118.
37. Schwartzberg LS, Yee LK, Senecal FM, et al. A randomized comparison of every-2-week darbepoetin alfa
and weekly epoetin alfa for the treatment of chemotherapy-induced anemia in patients with breast, lung, or
gynecologic cancer. Oncologist. 2004;9(6):696-707.
38. Senecal FM, Yee L, Gabrail N, et al. Treatment of chemotherapy-induced anemia in breast cancer: results
of a randomized controlled trial of darbepoetin alfa 200 microg every 2 weeks versus epoetin alfa 40,000 U
weekly. Clin Breast Cancer. Dec 2005;6(5):446-454.
39. Waltzman R, Croot C, Justice GR, Fesen MR, Charu V, Williams D. Randomized comparison of epoetin
alfa (40,000 U weekly) and darbepoetin alfa (200 microg every 2 weeks) in anemic patients with cancer
receiving chemotherapy. Oncologist. Sep 2005;10(8):642-650.
40. Glaspy J, Vadhan-Raj S, Patel R, et al. Randomized comparison of every-2-week darbepoetin alfa and
weekly epoetin alfa for the treatment of chemotherapy-induced anemia: the 20030125 Study Group Trial. J
Clin Oncol. May 20 2006;24(15):2290-2297.
41. Pashos CL, Larholt K, Fraser KA, McKenzie RS, Senbetta M, Piech CT. Outcomes of erythropoiesis-
stimulating agents in cancer patients with chemotherapy-induced anemia. Support Care Cancer.
Jan;20(1):159-165.
42. Bohlius J, Schmidlin K, Brillant C, et al. Recombinant human erythropoiesis-stimulating agents and
mortality in patients with cancer: a meta-analysis of randomised trials. Lancet. May 2
2009;373(9674):1532-1542.
43. Bohlius J, Schmidlin K, Brillant C, et al. Erythropoietin or Darbepoetin for patients with cancer--meta-
analysis based on individual patient data. Cochrane Database Syst Rev. 2009(3):CD007303.

20
44. Tonia T, Mettler A, Robert N, et al. Erythropoietin or darbepoetin for patients with cancer. Cochrane
Database Syst Rev.12:CD003407.
Evidence Table. Clinical Trials Evaluating the Erythropoietin-Stimulating Agents Reference/Study
Design
N Patient Selection Treatment Interventions Significant Outcomes* Adverse Effects
Chronic kidney disease
Nissenson et al,
200236
Randomized,
double-blind,
multicenter
noninferiority
trial
507 Patients with chronic kidney
disease and anemia
receiving hemodialysis
Darbepoetin alfa IV once weekly (n
= 169)
Epoetin alfa IV three times weekly
(n = 338)
*doses titrated to maintain
hemoglobin concentrations within a
range
of 9-13 g/dL
Duration: up to 28 weeks (20-week
dose-titration period, 8-week
follow-up)
Change in Hb from baseline
• darbepoetin: 0.24 + 0.10g/dL
• epoetin: 0.11 + 0.07g/dL
Incidence of RBC transfusion
• darbepoetin: 10%
• epoetin: 11%
Hypertension:
• darbepoetin: 28%
• epoetin: 24%
Papatheofanis et
al, 200622
Multicenter,
retrospective
chart review
789 Predialysis patients with
chronic kidney disease
Darbepoetin alfa (n = 396)
Epoetin alfa (n = 393)
Duration: >24 weeks
Achievement of target Hb levels (>
or = 11 g/dL)
• epoetin > darbepoetin; p < 0.0001
Mean cumulative ESA cost
• darbepoetin > epoetin
NR
Cancer
Schwartzberg et
al, 200437
Three concurrent
randomized,
open-label,
multicenter,
controlled trials
312 Patients >18 with a
diagnosis of breast cancer,
NSCLC, or gynecologic
carcinoma and anemia
(hemoglobin <11 g/dL)
Darbepoetin alfa
200 mcg every 2 weeks (n = 157)
Epoetin alfa 40,000 U once weekly
(n = 155)
Duration: up to 16 weeks
Incidence of RBC transfusion
• darbepoetin: 16%
• epoetin: 17%
Increase in Hb from baseline
• darbepoetin: 1.8 g/dL
• epoetin: 1.6 g/dL
Treatment-related serious
adverse events
• darbepoetin: 1 (DVT)
• epoetin: 2 (DVT, PE)

22
Senecal et al,
200538
Randomized,
multicenter,
open-label phase
II trial
141 Patients >18 with a
diagnosis of breast cancer
and anemia
Darbepoetin alfa 200 mcg every 2
weeks (n = 72)
Epoetin alfa 40,000 U
weekly (n = 69)
Duration: >16 weeks
Incidence of RBC transfusion
• darbepoetin: 6%
• epoetin: 16%
Mean change in hemoglobin from
baseline
• darbepoetin: 1.9 g/dL
• epoetin: 1.7 g/dL
Hematopoietic responses
(>2 g/dL increase or Hb >12 g/dL)
• darbepoetin: 88%
• epoetin: 81%
Safety
• darbepoetin = epoetin
Waltzman et al,
200539
Randomized,
open-label,
multicenter trial
358 Patients >18 receiving
cancer chemotherapy who
have anemia (hemoglobin
<11 g/dL)
Darbepoetin alfa
200 mcg every 2 weeks (n = 180)
Epoetin alfa 40,000 U once weekly
(n = 178)
Duration: 9 weeks
Incidence of RBC transfusion
• darbepoetin: 17.8%
• epoetin: 12.9%
Achievement of increase ≥1 g/dl at 5
weeks
• darbepoetin: 32.5%
• epoetin: 47%; p = 0.0078
Achievement of increase ≥2 g/dl at 9
weeks
• darbepoetin: 41.8%
• epoetin: 57.7%; p = 0.004
Thromboembolic events:
• darbepoetin: 9%
• epoetin: 11%
Neutropenia
• darbepoetin: 26%
• epoetin: 17%
Nausea
• darbepoetin: 27%
• epoetin: 33%
Diarrhea
• darbepoetin: 20%
• epoetin: 26%

23
Glaspy et al,
200640
Randomized,
controlled phase
III non-inferiority
trial
1220 Patients >18 with a
diagnosis of nonmyeloid
malignancy and anemia
(hemoglobin <11 g/dL)
Darbepoetin alfa 200mcg every
two weeks (n = 613)
Epoetin alfa 40,000 units every
week (n = 607)
Duration: up to 16 weeks
Incidence of RBC transfusion
(Kaplan-Meier estimate)
• darbepoetin: 21%
• epoetin: 16%
Achievement of target hemoglobin
• darbepoetin: 80%
• epoetin: 86%
Hemoglobin concentrations
Baseline:
• darbepoetin: 10.18
• epoetin: 10.21
Week 9:
• darbepoetin: 11.44
• epoetin: 11.76
Week 17:
• darbepoetin: 11.75
• epoetin: 11.85
Cardiovascular/
thromboembolic events:
• darbepoetin: 6%
• epoetin: 7%
Rates of death
• darbepoetin: 11%
• epoetin: 14%
Pashos et al,
201041
Multicenter (US),
prospective,
observational
study
540 Patients with chemotherapy-
induced anemia
Darbepoetin alfa 500 mcg (n =
120)
Epoetin alfa 40,000 U (n = 420)
Duration: January 1, 2006 and May
8, 2009
RBC transfusion required
• darbepoetin: 22.5%
• epoetin: 13.9%; p = 0.026
Change in Hb from baseline
• darbepoetin: 0.1 g/dL
• epoetin: 0.6 g/dL; p = 0.032
Mean cumulative ESA cost
• darbepoetin: 8,643
• epoetin: 4,261; p < 0.0001
NR
*p value is not significant, unless otherwise noted


















