Erna Hoch, Contents of Depressive Ideas in Indian Patients. Indian J Psychiatry, Jan 1961

of 9
-
Upload
amitranjan-basu -
Category
Documents
-
view
216 -
download
0
Transcript of Erna Hoch, Contents of Depressive Ideas in Indian Patients. Indian J Psychiatry, Jan 1961
-
7/27/2019 Erna Hoch, Contents of Depressive Ideas in Indian Patients. Indian J Psychiatry, Jan 1961
1/9
[ aQrticleD r. E R N A H O C H , M.D., D.P.M.,Nur Manzi l , Psychiat r ic Centre ,Lai Bagh , Lucknow.
To a foreign psychiatrist workingamongst patients of a different culture, thedifferences and similarities in the symptomatology of mental i l lness naturally presen t a fascinating field for studies. Bytrying to evaluate, how cultural influencesare changing a pattern of illness in a particular diagnostic group, one might , moreeasily than if one only sees patients of one'sown country, learn to dist inguish, what isaccidental and what is essential in a part icular type of mental or emotional disturb an ce .
After my coming to India in April 1956,i t did not take me long to notice that ,while in Indian patients schizophrenicmanifestations often differ considerablyfrom those we are used to in Europe, onecan hardly ever go wr ong in recogn izingcases of ma nic-de pressive illness. I foundhere the same familiar complaints, thesame predominance of pyknic body- types ,the same reaction to an at t i tude of sympathet ic unders tanding and pat ien t reassurance as I had been used to meet in mypatie nts in Sw itzerland . This confirmedmy conviction, which I still keep up inspite of others who refuse to make a distinction between various forms of depression, that manic-depressive illness is a definite morbid entity, presumably with somebiological foundation. A s such it is to bedistinguished from reactive depression,neurotic depression, depressive syndromesoccurring in the course of other psychoses,involutional depression and a part icular
Contents of DepressiveIdeas in Indian Patients
type of depression which is best characterized as exhaustive depression. (See alsoKielholz (1) ). This classification doesnot exclude the possibility that occasionally we may be in doubt , into which category to place a part icula r case. In youngpatients, e.g., it is often very difficult to distinguish in the first phase of illness,whether a manic or depressive episode ismore of cyclic or of schizophrenic character , while in the elderly patient one mayhesitate, whether to diagnose a genuineendogenous mania or depression or to callit an involutional depression or senilemania. Family-history, body -type, pre morbid personali ty and ult imate course ofthe illness often help to make the distinct ion, where symptomatology alone doesnot point clearly enough towards a defin i te d iagnost ic group. Fur therm ore, onemay of course have to differentiate etiological or precipitating factors, which in anindividual case may suggest more a constitutional bias, in some other case a morepsychogenic origin. Phenom enologically ,however, I f ind that the patients withmanic-depressive illness form a quite characterist ic group, which is absolutely comparable to patients of the same category inE urope. (See also H och (2) ) .
Having been tempted for quite sometime to investigate this similarity of manic-depressive patients in Europe and Indiamore closely, I was finally stimulated intoundertaking the present study of the con-
[Downloaded free from http://www.indianjpsychiatry.org on F riday, November 19, 2010, IP: 14.96.220.85]
-
7/27/2019 Erna Hoch, Contents of Depressive Ideas in Indian Patients. Indian J Psychiatry, Jan 1961
2/9
January 1961 ] Contents of Depressive Ideas in Indian PatientsHoch 29tents of depressive ideas by a letter froman Aust r ian co l league, which reached melast sum me r. Dr. H . Lenz , ret ired lecturer in psychiatry, of Lenz, wrote to me,as follows : (3).
"For some t ime past I have been busyinvestigating the changes to be noted inthe psychopathology of the major psychoses du rin g the last 50 years. I have justterminated a study on 376 depressions, inwhich I found mainly that the tendenciestowards guil t and suicide are decreasing."
Dr. Lenz then makes some remarks onthe change in contents of ideas in schizophrenic patients and goes on to discuss hisfindings :
"As far as I can see, this change in psychopathology is due to a great extent to ach an ge in the spirit of the age. This insight again is important for a biologicallyoriented psychiatry, which ought to consider symptoms that are, as far as possible,independent of variat ions due to the atmosphere of an age or to psychologicals i tuat ions ."
" In connect ion wi th these problems, Ishould be very much interested to know,which , nowadays are the main symptomsin melancholia or endogenous depressionand paranoid schizophrenia in India, acountry or cultural unit which is so different from the W estern cultural sphere . Ican imagine that in India, correspondingto the different a t t i tude of man to wa rdsmaterial possessions, religion etc., a quitedifferent spirit might still reign the epoch,and that this might have i ts consequencesalso for the psychopathological manifestat ions of depressions."
To this I answered in November 1959,promising to compile some figures aboutthe contents of depressive and paranoidideas . ' 'M eanw hi le , howeve r ," I wrote , " Ican already tel l you now that any material
gained in this way may not necessarilygive a valid answe r to your questions. W eshall only know, what the contents of theideas of those patients who are already"civil ized" enough to come to a psychiatricclinic. . . . O ur patients, w ho come main lyfrom Lucknow, but also from the wholeProvince of Uttar Pradesh and beyond,from all over India, are a selection of peop le who al ready have somewhat more enl ightened ideas about mental i l lness. Apartfrom this, it is often a mere matter ofchance that they have heard about our cl inic. So one could easily im agin e tha t thevery patients, whose ideas still have got astrongly magic, animistic content, first ofall would not know about a clinic of thiskind, and, even if they knew, would be farmore l ikely to take treatment from somemag ician, fakir or qua ck. A part fromthis, if one really wanted to be exact, onewould have to divide up the observed patients acc ording to religion and caste. Itseems a fair assumption to me, that a member of the caste of merchants may ratherhave ideas of improvement, while a Brahmin may more easily produce idas of sinfulness and religious doubt."
"Theoretically speaking, or perhaps evenwhen taking certain practical experiencesinto account , i t seems quite plausible to methat the contents of ideas should changewith the spirit of the time. If one assum esthat, fundamentally, illness usually is insome form an excuse for one's refusing toaccept life as it is or to accept oneself asone might be, the "excuse" naturally hasto be valid, not only for the patient himself, but also for his surrounding s. A phe-nomen of this kino".has been observed inthe change of symptoms in war-neuroses.As soon as some "hiding-place" has beenexposed as such by science or public opinion, new, and more valid excuses andescapes have to be found."
[Downloaded free from http://www.indianjpsychiatry.org on Friday, Novemb er 19, 2010, IP: 14.96.220.85]
-
7/27/2019 Erna Hoch, Contents of Depressive Ideas in Indian Patients. Indian J Psychiatry, Jan 1961
3/9
30 Indian Journal of Psychiatry [ Vol. Ill No. 1A short while ago he sent me a r ep r i n tof a p ap er of his, enti t led : "In t roduct ionto the problems of Diagnosis and Treat m e n t of Depressions" , publ ished in the
"Wiener klinische Wochenschrift ' ' (4).In this paper, Lenz enters into the q u e s t ion of the lead ing symptoms of endogenous depressions and their variat ions in thecourse of t i m e and in different areas. Hestates that by older authors guilt-feelingswer e n am ed as the essential symptoms ofendogenous depression. More recently ,e.g. in a p a p e r by Von Orell i , (5) p u b lished in 1954 in Switzer land , it has b eenshown that during the p as t 75 years guilt-feelings have become less predominant.In his own mater ial , Lenz (4) only foundthem present in 50% of the cases, while inprevious investigations this figure wasab o u t 75%. He comments on this :"One would have to conclude from thisthat guilt-feelings have no immediate connection with the essence of depression, butonly indirec tly. Gu ilt-feelings possibly
a r e far more due to the concept which thepat ien t has m a d e for himself or taken overfrom others about God and the world . Insome, as yet unpubl ished , papers I h av etried to show up, how the increasing appreciat ion of our "ego" takes a more orless parallel course with a diminution ofinterest in and a t t ach m en t to Chris t ian religion. This wou ld also explain the decrease of guil t-feelings."Lenz then makes a s tatement , forwhich he mentions Prof. Ur b an of I n n s bruck (who has been in India several timesand has studied Buddhism at N a l a n d aUnivers i ty) , Prof. M. Boss and myselfas witnesses and sources. I cannotqui te imagine, how, from my s tatementswhich I t ranslated to you, he could havegot the following ideas, which certainlymisrepresent matters. He writes :
"In endogenous depress ions of H i n d u s , and endogenous depression occurs inIndia just as m u ch as h er e , no guilt-feelings are known, a fact which can easilybe explained from the philosophical andreligious point of view of H i n d u i s m .W h en , h o wev er , a H i n d u who is converted to the Christian faith, falls into endogenous depression, he too will suffer fromguil t-feelings According to L e h m a n n(6) non-Christ ian, primitive Africans alsomanifest no guilt-feelings or self-accusat ions durin g endoge nous depression. A nother author, Volkel (7), recently seriouslyquest ioned the value of guilt-feelings forestablishing the diagnosis of an endogenousdepression. ' '
Lenz then turns to the question of suicide, which by some authors also has beenconsidered as a central phenomen in thepsychopathology of depression. Onenotes, however, that in cer tain Europeanregions (the author names Hol land andSachsen, a province of G e r m a n y ) , the freq u en cy of endogenous depressions is equal ,b u t the frequency of suicide committedduring endogenous depression is q u i t e different , in accordance wi th the rate of suicide in the total population of the twocountries. It seems that the r a t e of suicide varies in different epoc hs. Fro m themater ial of the Central Statistical Office ofAustr ia one has to conclude that dur ingthe last 20 years the figure for suicides hassignificantly decreased. Quite independently of this figure, about which he only-heard later , the author also stated a decrease of suicidal tendencies during thelast 20 years in the 367 depressive patientsinvestigated by him. Lenz assumes thatsimilar variations, due to cultural surroundings and the "spirit of the age",might also be proved wi th regard to otherideas, such as the illusion of impoverishm en t and hypochondriac symptoms.
[Downloaded free from http://www.indianjpsychiatry.org on Friday, Novem ber 19, 2010, IP: 14.96.220.85]
-
7/27/2019 Erna Hoch, Contents of Depressive Ideas in Indian Patients. Indian J Psychiatry, Jan 1961
4/9
January 1 9 6 1 ] Contents of Depre ssive Ideas in Indian Patients Hoch 31N o t i c i n g a l l t h e s e v a r i a t i o n s i n s y m p t o m s
t h a t w e r e o n c e s u p p o s e d t o b e c e n t r a l a n de sse n t i a l , Le n z a sk s , w h a t , a f t e r a l l t h i s ,s h o u l d b e c o n s i d e r e d a s " t h e f u n d a m e n t a ls y n d r o m e o f e n d o g e n o u s d e p r e s s i o n , o n et h a t is p r e s e n t i n e v e r y d e p r e s s i o n w i t h o u tr e g a r d t o p e r s o n a n d l i f e - s i t u a t io n , t h e i m m e d i a t e a n d t a n g i b l e e x p r e s s i o n o f t h a tv i t a l s a d n e s s , w h i c h K . S c h n e i d e r ( 8 ) c o n s i d e r s a s t h e u l t i m a t e , i r r e d u c i b l e b a s i s o fa l l d e p r e s s i o n s , a n d w h i c h W y r s c h ( 9 )n a m e s " m o t i v e - l e s s , v i t a l m e l a n c h o l i a " .
L e n z c a l l s t h e b a s i c s y n d r o m e , w h i c h h ef o u n d i n 9 0 % o f h i s c a se s a l l t h r o u g h t h e5 0 y e a r s of o b s e r v a t i o n , t h a t of " c o m p l a i n i n g o f b e i n g w i t h o u t " o r " b e i n g d e p r i v e do f" . H e e x p l a i n s i t a s " a c o m p l e x sy n d r o m e , t h e e x p r e ss i o n o f a l o ss o f a l l f u n c t i o n s a n d r e l a t i o n sh i p s o f m a n i n t h i s w o r l da n d b e y o n d i t. L o s s i s t h e e s s e n t i a l c o n t e n t of a l l d e p r e s s i o n . N e w e r a u t h o r s( v o n G e b s a t t e l ( 1 0 ) a n d E . S t r a u s s ( 1 1 ) ) ,i l l u m i n a t i n g t h e p h e n o m e n o n o f d e p r e s s io nf ro m a n o t h e r s i d e , h a v e c h a r a c t e r i z e d i t a sa s t o p p i n g o f t i m e a n d t h e p o ss i b i l i t i e s f o rd e v e l o p m e n t g i v e n b y t i m e . " L e n z t h e nd e s c r i b e s , h o w t h i s s y n d r o m e o f " b e i n gw i t h o u t " c a n s t a r t w i t h t h e v e g e t a t i v e f u n c t ions , i .e . loss of appet i te , loss of s leep;then comes loss of joy , loss of in terest , losso f p o w e r o f d e c i s i o n , l o ss o f j u d g m e n t , l o ssof act iv i ty , loss of p lanning, loss of a im,loss of values , loss of meaning, loss of conso l a t i o n , l o ss o f c o u r a g e , l o ss o f h o p e , l o sso f p e a c e a n d l o ss o f f a i t h . T h o u g h su c hs y m p t o m s a l s o o c c u r i n o t h e r t y p e s o f d e p r e s s i o n , t h e c h a r a c t e r i s t i c f e a t u r e o f e n d o g e n o u s d e p r e s s i o n i s s e e n b y L e n z i n t h ei n t e n s i t y a n d u n i v e r s a l e x t e n t o f t h e s e c o m p l a i n t s o f " b e i n g w i t h o u t " , a l s o b y t h e f a c tt h a r o u t w a r d c i r c u m s t a n c e s p l a y h a r d l ya n y r o l e i n p r o d u c i n g t h e m . H e p o i n tso u t t h a t , i n m a n i a , t h i s s y n d r o m e o f " b e i n gw i t h o u t " is c h a n g e d i n t o i t s o p p o s i t e : t h em a n i c p a t i e n t h a s e v e r y t h i n g , c o m m a n d s
e v e r y t h i n g , i s in c o n t a c t w i t h e v e r y t h i n g ,n o t o n l y a t p r e s e n t , b u t e v e n i n f u t u r e .L e n z t h e n a d d s , a n d i n t h i s h e is q u i t ec o r r e c t , t h a t t h i s s y n d r o m e o f " b e i n g w i t h o u t ' ' i s a l so f o u n d i n t h e d e p r e ss i o n s o fH i n d u p a t i e n t s .
I t w o u l d o f c o u r s e b e b e g g i n g t h e q u e s t i o n t o a sk , w h e t h e r i n m y c a se - m a t e r i a l ,w h i c h , w i t h o n l y 5 3 c a s e s of e n d o g e n o u sd e p r e ss i o n i s p e r h a p s r a t h e r t o o sm a l l , t h i sv i t a l s y n d r o m e o f " b e i n g w i t h o u t " a l s o i sp r e s e n t . I n m o r e o r l e ss t h e f o rm d e sc r i b e d b y L e n z , I a c t u a l l y m a d e it t h e c r i t e r i o n f o r c l a ss i fy i n g a d e p r e ss i o n a s e n d o g e n o u s , t a k i n g i n t o c o n s i d e r a t i o n , o fc o u r se , su c h fa c t o r s a s f a m i l y - h i s t o r y ,b o d y - t y p e , p r e v i o u s m a n i c o r d e p r e s s i v ep h a se s , u l t i m a t e c o u r se o f t h e i l l n e ss a n dr e s p o n s e t o t r e a t m e n t . S o , w h a t I w o u l dc a l l t h e " v i t a l sy n d r o m e ' ' , w a s p r e se n t i na ll t h e c a se s . A s I m e n t i o n e d in t h e b e g i n n i n g , i t is a m a z i n g t o f in d , h o w s i m i l a rt h e c o m p l a i n t s o f I n d i a n p a t i e n t s a r e t othos e on e i s use d to f ind in the W es t : th esa m e d e c l i n e o f a l l v i t a l f u n c t i o n s , t h e sa m el a c k o f f a i t h , h o p e , c o n f i d e n c e , t h e sa m ee x p e r i e n c e o f a c l o se d w o r l d , o f a d a r k c u r t a i n t h a t h a s f a l l e n d o w n o v e r e v e r y t h i n go r o f t i m e h a v i n g c o m e to a s t o p . I tm i g h t b e in t e r e s t i n g t o i n v e s t i g a t e t h e v e r b a l f o r m s of e x p r e ss i o n u se d t o d e s i g n a t et h i s e x p e r i e n c e . O u r r e c o r d s d o n o t a l l o win a l l cases to ex am ine th is . Bu t 1 sho uldl i k e t o p o i n t t o t h e d i f f e r e n c e i n a g e n e r a lw a y o f f o r m u l a t i n g d e p r e s s i v e e x p e r i e n c e :T h e t e r m " d e p r e s s i o n " i n d i c a t e s t h a t t h es u b j e c t f e e ls w e i g h e d , p r e s s e d d o w n . I nG e r m a n w e t a lk a b o u t . " S c h w e r m u t " ,w h i c h p e r h a p s c o u l d b e s t b e t r a n s l a t e d a s" h e a v y m o o d " . I n H i n d u s t a n i w e h e a r t h ep a t i e n t s a y : " T a b i a t g i r t i " . W h i l e " d e p r e s s i o n " i n d i c a t e s a p a s s i v e e x p e r i e n c e o fb e i n g p r e s s e d b y s o m e w e i g h t fr o m o u t s i d e o r p o s s i b l y o n e 's o w n w e i g h t , " g i r n a "s e e m s t o b e s o m e t h i n g m o r e s p o n t a n e o u s .
[Downloaded free from http://www.indianjpsychiatry.org on Friday, Novemb er 19, 2010, IP: 14.96.220.85]
-
7/27/2019 Erna Hoch, Contents of Depressive Ideas in Indian Patients. Indian J Psychiatry, Jan 1961
5/9
32It might therefore be considered as something more active. O n the other h and,however, an object will fall, if it does notresist the forces that draw it down, while"depression ' ' may indicate that the pressure from above has to be exercised againstresistance. To conclude from this, thatIndian patients, who, according to usage oflanguage "let themselves fal l" , might bemore prone to fall into depression than theWestern patient , who has to be presseddown against resistance, would however bewrong . W hen last year, in a lectu re givenat the University Clinic of Psychiatry atBasel (12), I reported about some stat ist ical figures of our Center, I was told thatthe distribution of cases amongst the various diagnostic categories was remarkablysimilar to that registered in Swiss clinics.As to Indian figures, I could not find anymaterial up to now, which would have allowed valid comparison with our particularcase -ma terial. (I found some figures forR anehi M ental H ospital : For 194S''49 thefigure for manic-depressive psychosis is4.4 % . for 1 949 /50 it is 6.3', , , for 1950 /51it is 7 .8 ' . ) (1 3) 1 would be interested ingetting figures from other clinics with in-and out -pateints. It goes witho ut saying,that our figures can in no way be utilizedto gain some idea about the incidence ofmanic-depressive illness in the total population.
Our own figures are taken from 1190 patients examined between April 19.56 andJun e 1960. Of these patie nts, 6.2 % , i.e.74, were diagnosed as suffering from eithera manic or a depressive phase of cyclicpsychosis, while, just to give one figure forcomparison, 27.6 '
-
7/27/2019 Erna Hoch, Contents of Depressive Ideas in Indian Patients. Indian J Psychiatry, Jan 1961
6/9
Janury \?6l \ Contents of Depressive Ideas in Indian Patients Hoch 53
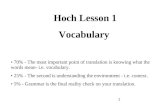
BODYPAMIEYWORKSUICIDEGUILTMINDRELIGIONPARANOIDPOSSESSIONS
CONTENTS OF DEPRESSIVE IDEASAll Patients (50)
1I
/
50jj
All Men (20) All Women (30}BODYF AMI L YWORKSUICIDE.GUILTMINDR E L I G I O NP A R A N O I DP O S S E S S I O N SJ
50*