Eric T. Stoopler and Faizan Alawi -...
31
Pigmented Lesions of the Oral Mucosa Eric T. Stoopler and Faizan Alawi Abstract Pigmented lesions of the oral mucosa are encountered on a routine basis in clinical prac- tice. Oral health-care providers must assess several parameters associated with pigmented lesions, such as location, shape, color, and size. Etiology of pigmented lesions may be attrib- uted to a local phenomenon and/or associated with an underlying systemic disorder. Diag- nostic and therapeutic modalities must be care- fully considered as these lesions encompass the spectrum of clinical pathology, ranging from benign to malignant. Clinicians should conduct a thorough medical history and relevant phys- ical examination for patients with pigmented lesions to identify possible adrenal, gastroin- testinal, or genetic disorders that are commonly associated with these types of lesions. If a systemic disorder is suspected, the patient should be promptly referred to the appropriate health-care provider for further evaluation and management. Multidisciplinary care is often necessary to effectively manage patients with these conditions. This chapter provides a contemporary perspective of pigmented lesions of the oral mucosa and is intended to serve as a practical clinical resource for oral health-care providers. Keywords Oral mucosa • Pigmentation • Melanin • Focal • Multifocal • Diffuse • Systemic • Genetic • Exogenous Contents Introduction .......................................... 2 Focal Pigmentation .................................. 2 Freckle/Ephelis ........................................ 2 Oral/Labial Melanotic Macule ........................ 3 Oral Melanoacanthoma ............................... 5 Melanocytic Nevus .................................... 6 Malignant Melanoma ................................. 8 Multifocal/Diffuse Pigmentation .................... 14 Physiologic Pigmentation ............................. 14 Drug-Induced Melanosis .............................. 15 Smoker’ s Melanosis ................................... 16 Post-inflammatory (Inflammatory) Hyperpigmentation ................................ 17 Laugier-Hunziker Pigmentation ...................... 18 Pigmentation Associated with Systemic or Genetic Disorders .......................................... 19 Adrenal Insufficiency (Addison Disease) ............. 19 Cushing Disease ....................................... 21 Human Immunodeficiency Virus (HIV): Associated Pigmentation ....................................... 23 Peutz-Jeghers Syndrome .............................. 24 Exogenous Causes of Clinical Pigmentation ....... 26 Tattoos: Amalgam, Graphite, and Ornamental ....... 26 Metal-induced Discoloration .......................... 28 E.T. Stoopler (*) Department of Oral Medicine, University of Pennsylvania School of Dental Medicine, Philadelphia, PA, USA e-mail: [email protected] F. Alawi Department of Pathology, University of Pennsylvania School of Dental Medicine, Philadelphia, PA, USA e-mail: [email protected] # Springer International Publishing AG 2017 C.S. Farah et al. (eds.), Contemporary Oral Medicine, DOI 10.1007/978-3-319-28100-1_17-1 1
Transcript of Eric T. Stoopler and Faizan Alawi -...

Pigmented Lesions of the Oral Mucosa
Eric T. Stoopler and Faizan Alawi
AbstractPigmented lesions of the oral mucosa areencountered on a routine basis in clinical prac-tice. Oral health-care providers must assessseveral parameters associated with pigmentedlesions, such as location, shape, color, and size.Etiology of pigmented lesions may be attrib-uted to a local phenomenon and/or associatedwith an underlying systemic disorder. Diag-nostic and therapeutic modalities must be care-fully considered as these lesions encompass thespectrum of clinical pathology, ranging frombenign tomalignant. Clinicians should conducta thorough medical history and relevant phys-ical examination for patients with pigmentedlesions to identify possible adrenal, gastroin-testinal, or genetic disorders that are commonlyassociated with these types of lesions. If asystemic disorder is suspected, the patientshould be promptly referred to the appropriatehealth-care provider for further evaluation andmanagement. Multidisciplinary care is oftennecessary to effectively manage patients withthese conditions. This chapter provides a
contemporary perspective of pigmentedlesions of the oral mucosa and is intended toserve as a practical clinical resource for oralhealth-care providers.
KeywordsOral mucosa • Pigmentation •Melanin • Focal •Multifocal • Diffuse • Systemic • Genetic •Exogenous
ContentsIntroduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Focal Pigmentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Freckle/Ephelis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Oral/Labial Melanotic Macule . . . . . . . . . . . . . . . . . . . . . . . . 3Oral Melanoacanthoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Melanocytic Nevus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Malignant Melanoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Multifocal/Diffuse Pigmentation . . . . . . . . . . . . . . . . . . . . 14Physiologic Pigmentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Drug-Induced Melanosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Smoker’s Melanosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Post-inflammatory (Inflammatory)
Hyperpigmentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Laugier-Hunziker Pigmentation . . . . . . . . . . . . . . . . . . . . . . 18
Pigmentation Associated with Systemic or GeneticDisorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Adrenal Insufficiency (Addison Disease) . . . . . . . . . . . . . 19Cushing Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Human Immunodeficiency Virus (HIV): Associated
Pigmentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Peutz-Jeghers Syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Exogenous Causes of Clinical Pigmentation . . . . . . . 26Tattoos: Amalgam, Graphite, and Ornamental . . . . . . . 26Metal-induced Discoloration . . . . . . . . . . . . . . . . . . . . . . . . . . 28
E.T. Stoopler (*)Department of Oral Medicine, University of PennsylvaniaSchool of Dental Medicine, Philadelphia, PA, USAe-mail: [email protected]
F. AlawiDepartment of Pathology, University of PennsylvaniaSchool of Dental Medicine, Philadelphia, PA, USAe-mail: [email protected]
# Springer International Publishing AG 2017C.S. Farah et al. (eds.), Contemporary Oral Medicine,DOI 10.1007/978-3-319-28100-1_17-1
1

Conclusion and Future Directions . . . . . . . . . . . . . . . . . . 28
Cross-References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Introduction
The mucous membranes lining the oral cavity arenot uniformly colored and dependent upon the spe-cific anatomic location; healthy tissue commonlyranges in color fromwhite to red-purple. This is dueto the interaction of various tissues that compose themucosal lining, including presence or absence ofkeratin on the surface epithelium, location and pres-ence of vascular structures in the stroma, existenceof adipocytes, and the lack of melanin pigmentationin the basal cell layer of the epithelium. Pigmentdeposition, whether physiologic or pathologic, orattributed to endogenous or exogenous substances,will impart gray, blue, brown and/or black colorchanges to the oral mucosa. The most commonendogenous sources of pigmentation are melanin,hemoglobin, and hemosiderin, while exogenoussources of pigmentation are usually attributed totraumatic or iatrogenic events that result in deposi-tion of foreign material directly into the mucosaltissues. Several parameters associated withpigmented lesions, such as location, shape, color,and size, must be assessed in order for clinicians toappropriately evaluate andmanage the condition, aspathology of pigmented lesions ranges from benignto malignant. Clinicians should conduct a thoroughmedical, family, and social history, as well as arelevant physical examination for patients withpigmented lesions, to identify possible adrenal, gas-trointestinal, or genetic disorders that are commonlyassociated with these types of lesions. If a systemicdisorder is suspected, the patient should bepromptly referred to the appropriate health-careprovider for further evaluation and management.Multidisciplinary care is often necessary to effec-tively manage patients with these conditions. Thischapter provides a contemporary perspective ofpigmented lesions of the oral mucosa focusing onthose associatedwithmelanin andwill discuss focalpigmentation conditions, multifocal or diffuse pig-mentation conditions, pigmentation associated with
systemic or genetic disorders, and exogenouscauses of clinical pigmentation (Table 1).
Melanocytes are derived from neural crest cellsand are located in the basal epithelial layerof squamous mucous membranes (Meleti et al.2008). The functions of melanocytes are notfully understood, but the melanin producedby these cells absorb ultraviolet light, scavengereactive oxygen species, and determine skin, hair,and eye color (Meleti et al. 2008; Feller et al.2014a, b). Oral melanocytes are regularly inter-spersed between basal keratinocytes, and melaninfrom the melanocytes are transported and trans-mitted to epithelial cells via dendritic migration ofmelanosomes (melanin-containing vesicles). Theratio of melanocytes to keratinocytes in the basalepithelial layer ranges from 1:10 to 1:15 (Felleret al. 2014a, b). Two chemically distinct types ofmelanin exist, eumelanin (brown-black) andpheomelanin (red/yellow), and melanogenesis isconsidered a mixed process between these mela-nin types, with proportions of eumelanin andpheomelanin being genetically determined (Felleret al. 2014a, b). There are no numerical or struc-tural differences in oral melanocytes between
Table 1 Pigmented lesions of the oral mucosa
I. Focal pigmentation conditions
a. Freckle/ephelis
b. Oral/labial melanotic macule
c. Oral melanoacanthoma
d. Melanocytic nevus
e. Malignant melanoma
II. Multifocal/diffuse pigmentation conditions
a. Physiologic pigmentation
b. Drug-induced melanosis
c. Smoker’s melanosis
d. Post-inflammatory (inflammatory) hyperpigmentation
e. Laugier-Hunziker pigmentation
III. Pigmentation associated with systemic or geneticdisorders
a. Adrenal insufficiency (Addison disease)
b. Cushing disease
c. Human immunodeficiency virus (HIV) – associatedpigmentation
d. Peutz-Jeghers syndrome
IV. Exogenous causes of clinical pigmentation
a. Tattoos – amalgam, graphite and ornamental
b. Metal – induced discoloration
2 E.T. Stoopler and F. Alawi

light-skinned and dark-skinned individuals exceptthat in the latter, the melanosomes are larger andmore numerous (Feller et al. 2014a, b). Severalfactors likely determine intraoral mucosal color,including number and melanogenic activity ofmelanocytes, differences in number, size and dis-tribution of melanosomes, difference in the typeof melanin, and the masking effect of heavilykeratinized epithelium (Feller et al. 2014a, b).
Focal Pigmentation
Freckle/Ephelis
EpidemiologyA freckle (ephelis) is a hyperpigmented maculecommonly observed on the facial and perioralskin. They usually develop during the first decadeof life and are more common in light-skinnedindividuals with blonde or red hair (Gaeta et al.2002; Hatch 2005). There is no gender predilec-tion, and the color intensity and frequency offreckles typically decrease after adolescence(Gaeta et al. 2002; Hatch 2005).
EtiologyFreckles are thought to be developmental in origin(Gaeta et al. 2002; Hatch 2005). Genetic poly-morphisms associated with the melanocortin-1receptor (MC1R) gene and chromosome 4q32-q34 have been strongly associated with freckledevelopment (Bastiaens et al. 2001).
PathophysiologyFreckles are due to an increase in melanin produc-tion without an increase in the number of melano-cytes and become more pronounced after sunexposure. They are also associated closely with ahistory of symptomatic childhood sunburns (Blisset al. 1995).
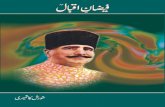
Clinical-Pathologic FeaturesFreckles appear as a uniformly tan- or brown-colored, oval or round macule, between 1 and3 mm in size on sun-exposed cutaneous surfaces(Gaeta et al. 2002; Hatch 2005) (Fig. 1). Theyhave regularly defined borders, are not elevated
above the skin surface, and are asymptomatic(Gaeta et al. 2002; Hatch 2005). They oftenappear on the perioral skin and vermillion borderof the lips with increased frequency on the lowerlip (Hatch 2005). Although many individualshave less than ten lesions, due to the great vari-ability in the number of lesions present, some mayhave hundreds of freckles (Gaeta et al. 2002;Hatch 2005). Histopathologically, freckles exhibitabundant melanin deposition in the basal celllayer of the epidermis without elongation of reteridges (Hatch 2005).
Patient ManagementTreatment is typically not indicated for freckles inchildhood or adolescence (Hatch 2005). Sun-screens may help prevent darkening of existinglesions and prevent the appearance of new lesions(Bliss et al. 1995). Freckles of cosmetic concernmay be treated with chemical peels, laser therapy,and/or cryotherapy. MC1R gene variants havebeen associated with an increased risk for spo-radic cutaneous melanoma (Pasquali et al. 2015).
Oral/Labial Melanotic Macule
EpidemiologyA melanotic macule is a benign pigmented lesionthat may occur on intraoral mucosal surfaces (oralmelanotic macule) or on the lips (labial melanoticmacule) (Tarakji et al. 2014). They are consideredto be the most common oral mucosal lesions ofmelanocytic origin and are also termed focalmelanosis (Alawi 2013; Muller 2010). Oral/labialmelanotic macules are present in up to 3% of thepopulation, are typically observed in patients inthe fourth and fifth decades, and have a 2:1 femalepredilection (Hatch 2005; Meleti et al. 2008;Muller 2010).
EtiologyThe etiology of oral/labial melanotic macules hasnot been definitively determined but may repre-sent a reactive or a physiologic process (Meletiet al. 2008).
Pigmented Lesions of the Oral Mucosa 3
PathophysiologyOral/labial melanotic macules are caused by anincreased production and deposition of melaninwithin the basal cell layer, the lamina propria, orboth (Meleti et al. 2008). The etiology of theselesions is unclear; however, sun exposure does notappear to be a precipitating factor.
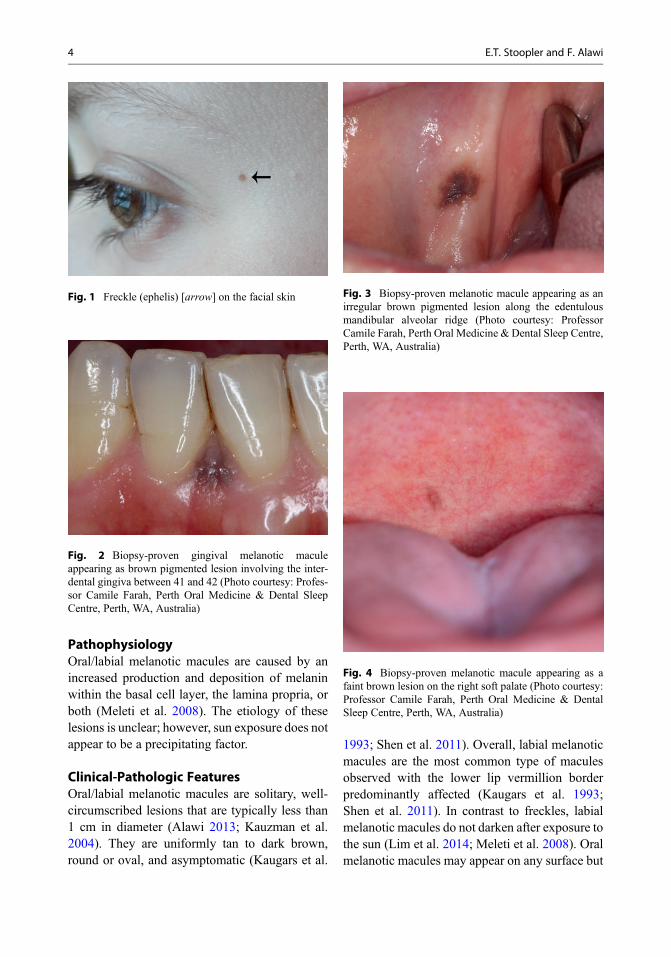
Clinical-Pathologic FeaturesOral/labial melanotic macules are solitary, well-circumscribed lesions that are typically less than1 cm in diameter (Alawi 2013; Kauzman et al.2004). They are uniformly tan to dark brown,round or oval, and asymptomatic (Kaugars et al.
1993; Shen et al. 2011). Overall, labial melanoticmacules are the most common type of maculesobserved with the lower lip vermillion borderpredominantly affected (Kaugars et al. 1993;Shen et al. 2011). In contrast to freckles, labialmelanotic macules do not darken after exposure tothe sun (Lim et al. 2014; Meleti et al. 2008). Oralmelanotic macules may appear on any surface but
Fig. 1 Freckle (ephelis) [arrow] on the facial skin
Fig. 2 Biopsy-proven gingival melanotic maculeappearing as brown pigmented lesion involving the inter-dental gingiva between 41 and 42 (Photo courtesy: Profes-sor Camile Farah, Perth Oral Medicine & Dental SleepCentre, Perth, WA, Australia)
Fig. 3 Biopsy-proven melanotic macule appearing as anirregular brown pigmented lesion along the edentulousmandibular alveolar ridge (Photo courtesy: ProfessorCamile Farah, Perth Oral Medicine & Dental Sleep Centre,Perth, WA, Australia)
Fig. 4 Biopsy-proven melanotic macule appearing as afaint brown lesion on the right soft palate (Photo courtesy:Professor Camile Farah, Perth Oral Medicine & DentalSleep Centre, Perth, WA, Australia)
4 E.T. Stoopler and F. Alawi

are most commonly observed on the buccalmucosa, gingiva, and palate (Kauzman et al.2004) (Figs. 2, 3, 4, and 5a, b). Intraoral lesionsare often larger than those located on the lips(Meleti et al. 2008). Histopathological analysisof melanotic macules reveals an increase in mel-anin in the basal and parabasal layers of normalstratified squamous epithelium without an
increase in number of melanocytes (Kaugarset al. 1993; Shen et al. 2011) (Fig. 6). Melaninmay also be observed within melanophages ormay be free (incontinence) in the subepithelialconnective tissue, and these lesions do not typi-cally demonstrate elongated rete ridges (Alawi2013).
Patient ManagementOral/labial melanotic macules are consideredbenign lesions without malignant potential(Kauzman et al. 2004). Since early malignantmelanoma may have a similar clinical appearanceand exhibits a predilection for the maxillary alve-olar mucosa and palate, it is strongly advisable toperform an excisional biopsy for any suspectedoral/labial melanotic macule for histopathologicanalysis (Kauzman et al. 2004). Labial melanoticmacules may be of cosmetic concern, and removalof these lesions may be accomplished by scalpel,cryosurgery, electrocautery, or laser ablation(Alawi 2013; Lim et al. 2014).
Oral Melanoacanthoma
EpidemiologyOral melanoacanthoma represents a benignmelanocytic lesion that is most commonly
Fig. 5 Biopsy-proven melanotic macule involving thehard palate demonstrating irregular pigmentation and bor-der viewed with white light (a) and with optical fluores-cence imaging VELscope Vx (b) showing loss of
fluorescence limited to lesion with no diascopy (Photocourtesy: Professor Camile Farah, Perth Oral Medicine &Dental Sleep Centre, Perth, WA, Australia)
Fig. 6 Melanotic macule. Melanin pigmentation is notedin the basal epithelial layer (hematoxylin and eosin, 200�)
Pigmented Lesions of the Oral Mucosa 5
observed in dark-complexioned females between30 and 50 years of age (Arava-Parastatidis et al.2011). This condition has been reported in His-panic, Asian, and Caucasian patients and has anoverall female predilection (Arava-Parastatidiset al. 2011).
EtiologyOral melanoacanthoma is of unknown etiology(Gondak et al. 2012; Muller 2010).
PathophysiologyThe pathophysiologic mechanism for oralmelanoacanthoma is most consistently associatedwith acute regional trauma or chronic irritation(Alawi 2013; Arava-Parastatidis et al. 2011).
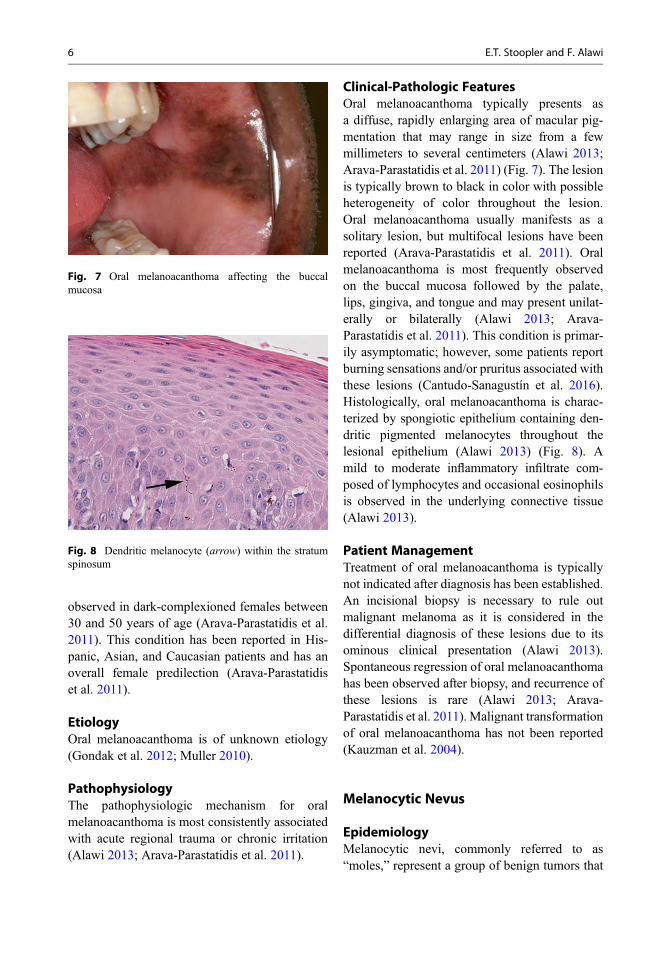
Clinical-Pathologic FeaturesOral melanoacanthoma typically presents asa diffuse, rapidly enlarging area of macular pig-mentation that may range in size from a fewmillimeters to several centimeters (Alawi 2013;Arava-Parastatidis et al. 2011) (Fig. 7). The lesionis typically brown to black in color with possibleheterogeneity of color throughout the lesion.Oral melanoacanthoma usually manifests as asolitary lesion, but multifocal lesions have beenreported (Arava-Parastatidis et al. 2011). Oralmelanoacanthoma is most frequently observedon the buccal mucosa followed by the palate,lips, gingiva, and tongue and may present unilat-erally or bilaterally (Alawi 2013; Arava-Parastatidis et al. 2011). This condition is primar-ily asymptomatic; however, some patients reportburning sensations and/or pruritus associated withthese lesions (Cantudo-Sanagustín et al. 2016).Histologically, oral melanoacanthoma is charac-terized by spongiotic epithelium containing den-dritic pigmented melanocytes throughout thelesional epithelium (Alawi 2013) (Fig. 8). Amild to moderate inflammatory infiltrate com-posed of lymphocytes and occasional eosinophilsis observed in the underlying connective tissue(Alawi 2013).
Patient ManagementTreatment of oral melanoacanthoma is typicallynot indicated after diagnosis has been established.An incisional biopsy is necessary to rule outmalignant melanoma as it is considered in thedifferential diagnosis of these lesions due to itsominous clinical presentation (Alawi 2013).Spontaneous regression of oral melanoacanthomahas been observed after biopsy, and recurrence ofthese lesions is rare (Alawi 2013; Arava-Parastatidis et al. 2011). Malignant transformationof oral melanoacanthoma has not been reported(Kauzman et al. 2004).
Melanocytic Nevus
EpidemiologyMelanocytic nevi, commonly referred to as“moles,” represent a group of benign tumors that
Fig. 7 Oral melanoacanthoma affecting the buccalmucosa
Fig. 8 Dendritic melanocyte (arrow) within the stratumspinosum
6 E.T. Stoopler and F. Alawi

develop due to melanocytic growth and prolifera-tion (Alawi 2013; Hatch 2005). Cutaneous neviare common and typically develop during child-hood with most cutaneous lesions present beforethe age of 35 (Marangon Junior et al. 2015). Inaddition, Caucasians tend to develop cutaneousnevi more frequently than blacks or Asians(Marangon Junior et al. 2015). The intramucosalnevus is the most frequently observed type of oralnevus followed by the blue nevus, compoundnevus, junctional nevus, and combined nevus, indecreasing order of frequency (Alawi 2013). Oralmelanocytic nevi are frequently observed in thethird to fourth decades of life, and while the totalnumber of nevi tends to be higher in males, oralmelanocytic nevi are more common in females(Alawi 2013).
EtiologyIn general, melanocytic nevi are acquired lesionswith both environmental and genetic factorsthought to play a role in the development ofcutaneous lesions (Alawi 2013; Muller 2010).Sun exposure is a well-recognized environmentalfactor for development of cutaneous nevi (Limet al. 2014). Recent studies have demonstratedcutaneous nevi exhibiting somatic, activatingmutations in the BRAF, HRAS, and NRAS proto-oncogenes (Alawi 2013; Meleti et al. 2008). Itremains unclear if similar mutations are impli-cated as the etiology of oral melanocytic nevi(Alawi 2013).
PathophysiologyThe pathogenesis of melanocytic nevi, includingoral melanocytic nevi, is poorly understood(Meleti et al. 2008). Acquired melanocytic nevievolve through several developmental stagesalthough not all nevi pass through each stage(Meleti et al. 2008). It has been postulated thatjunctional nevi evolve into compound nevi andultimately into intramucosal nevi, with differenti-ating clinical and histologic features (Alawi2013). Melanocytic proliferation can be consid-ered in three phases that correspond to each of theaforementioned nevi types: (1) proliferation ofbenign neoplastic melanocytes along theepithelial-mesenchymal junction (i.e., junctional
nevus), (2) migration of these cells into the mes-enchymal compartment (i.e., compound nevus),and (3) loss of the junctional component of thenevus so all remaining cells are located within thesubepithelial compartment (intramucosal nevi)(Meleti et al. 2008). Blue nevi are melanocyticlesions that typically appear slate blue to blueblack and account for up to 35% of all oral nevi(Pinto et al. 2003). They are categorized into thecommon type and the less frequently encounteredcellular type, and while each has specific charac-teristic histopathologic features, both types harbormelanin particles deep to the surface so thatreflected light appears blue to the observer (Pintoet al. 2003). Darkly pigmented blue nevi may beclinically indistinguishable from other types ofmelanocytic nevi.
Clinical-Pathologic FeaturesCutaneous junctional nevi commonly appear as asharply demarcated macule less than 6 mm indiameter with brown or blue coloration (Alawi2013). Compound nevi may bemacular or slightlyelevated, soft with a relatively smooth surface,while intradermal (cutaneous counterpart tointramucosal) nevi exhibits loss of pigmentationand a papillomatous surface with possible centralhair growth (Alawi 2013). Oral melanocytic nevihave no distinguishing clinical characteristics;however, they are usually asymptomatic, solitary,well circumscribed, less than 1 cm, macular ornodular in appearance, and brown or blue incolor (Alawi 2013) (Figs. 9 and 10). It is
Fig. 9 Intramucosal nevus (arrow) located on the palate(Courtesy of Dr. Edward Marcus)
Pigmented Lesions of the Oral Mucosa 7
important to note that up to 15% of oral nevi maynot exhibit any evidence of clinical pigmentation(Alawi 2013; Muller 2010). The most commonlyaffected intraoral surfaces are the hard palate,buccal and labial mucosae, and gingiva, respec-tively (Alawi 2013; Meleti et al. 2008).
Histopathologically, nevus cells confined tothe basal layer at the junction of the epitheliumand connective tissue, especially at the tips of therete ridges are characteristic of junctional nevi(Alawi 2013). As the junctional nevus evolves,clustered melanocytes proliferate down into theconnective tissue, forming nests of various sizes,while some nevus cells are still seen at theepithelial-connective tissue surface, all of whichare characteristic of the compound nevus (Alawi2013). Intramucosal nevi demonstrate nevus cells
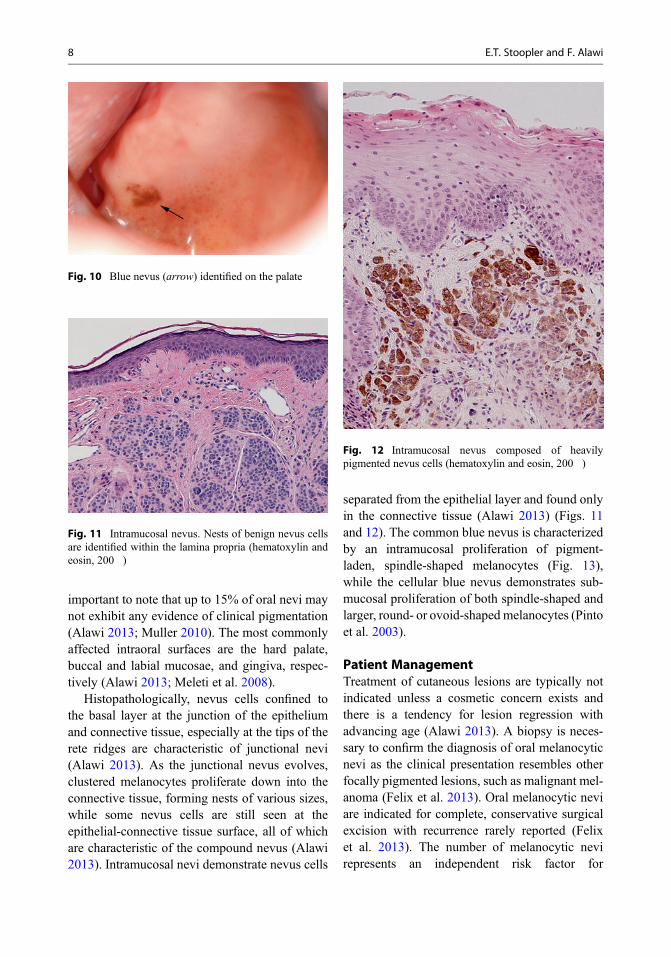
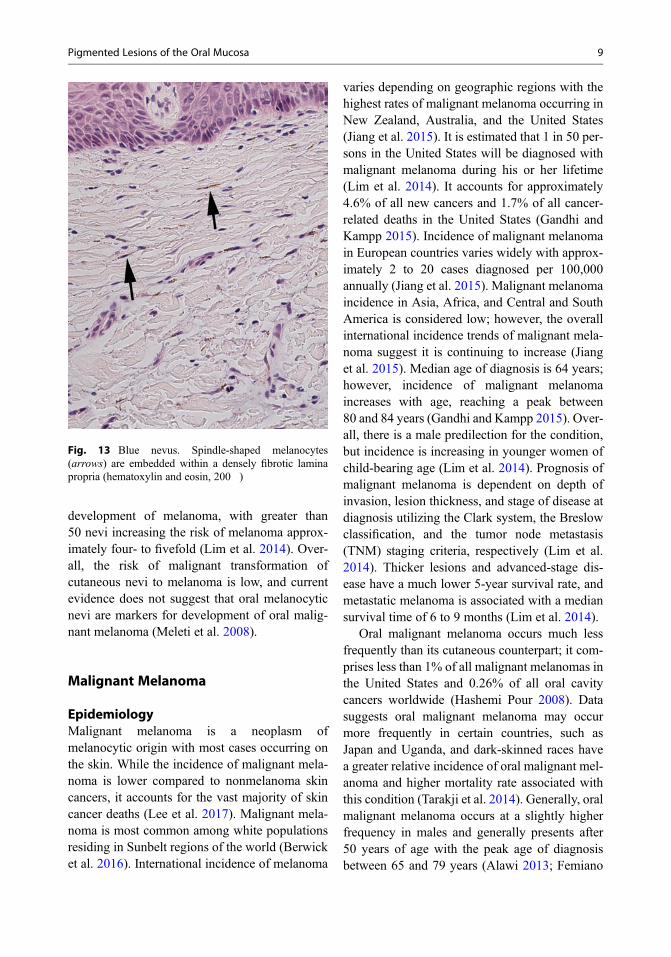
separated from the epithelial layer and found onlyin the connective tissue (Alawi 2013) (Figs. 11and 12). The common blue nevus is characterizedby an intramucosal proliferation of pigment-laden, spindle-shaped melanocytes (Fig. 13),while the cellular blue nevus demonstrates sub-mucosal proliferation of both spindle-shaped andlarger, round- or ovoid-shaped melanocytes (Pintoet al. 2003).
Patient ManagementTreatment of cutaneous lesions are typically notindicated unless a cosmetic concern exists andthere is a tendency for lesion regression withadvancing age (Alawi 2013). A biopsy is neces-sary to confirm the diagnosis of oral melanocyticnevi as the clinical presentation resembles otherfocally pigmented lesions, such as malignant mel-anoma (Felix et al. 2013). Oral melanocytic neviare indicated for complete, conservative surgicalexcision with recurrence rarely reported (Felixet al. 2013). The number of melanocytic nevirepresents an independent risk factor for
Fig. 11 Intramucosal nevus. Nests of benign nevus cellsare identified within the lamina propria (hematoxylin andeosin, 200�)
Fig. 12 Intramucosal nevus composed of heavilypigmented nevus cells (hematoxylin and eosin, 200�)
Fig. 10 Blue nevus (arrow) identified on the palate
8 E.T. Stoopler and F. Alawi
development of melanoma, with greater than50 nevi increasing the risk of melanoma approx-imately four- to fivefold (Lim et al. 2014). Over-all, the risk of malignant transformation ofcutaneous nevi to melanoma is low, and currentevidence does not suggest that oral melanocyticnevi are markers for development of oral malig-nant melanoma (Meleti et al. 2008).
Malignant Melanoma
EpidemiologyMalignant melanoma is a neoplasm ofmelanocytic origin with most cases occurring onthe skin. While the incidence of malignant mela-noma is lower compared to nonmelanoma skincancers, it accounts for the vast majority of skincancer deaths (Lee et al. 2017). Malignant mela-noma is most common among white populationsresiding in Sunbelt regions of the world (Berwicket al. 2016). International incidence of melanoma
varies depending on geographic regions with thehighest rates of malignant melanoma occurring inNew Zealand, Australia, and the United States(Jiang et al. 2015). It is estimated that 1 in 50 per-sons in the United States will be diagnosed withmalignant melanoma during his or her lifetime(Lim et al. 2014). It accounts for approximately4.6% of all new cancers and 1.7% of all cancer-related deaths in the United States (Gandhi andKampp 2015). Incidence of malignant melanomain European countries varies widely with approx-imately 2 to 20 cases diagnosed per 100,000annually (Jiang et al. 2015). Malignant melanomaincidence in Asia, Africa, and Central and SouthAmerica is considered low; however, the overallinternational incidence trends of malignant mela-noma suggest it is continuing to increase (Jianget al. 2015). Median age of diagnosis is 64 years;however, incidence of malignant melanomaincreases with age, reaching a peak between80 and 84 years (Gandhi and Kampp 2015). Over-all, there is a male predilection for the condition,but incidence is increasing in younger women ofchild-bearing age (Lim et al. 2014). Prognosis ofmalignant melanoma is dependent on depth ofinvasion, lesion thickness, and stage of disease atdiagnosis utilizing the Clark system, the Breslowclassification, and the tumor node metastasis(TNM) staging criteria, respectively (Lim et al.2014). Thicker lesions and advanced-stage dis-ease have a much lower 5-year survival rate, andmetastatic melanoma is associated with a mediansurvival time of 6 to 9 months (Lim et al. 2014).
Oral malignant melanoma occurs much lessfrequently than its cutaneous counterpart; it com-prises less than 1% of all malignant melanomas inthe United States and 0.26% of all oral cavitycancers worldwide (Hashemi Pour 2008). Datasuggests oral malignant melanoma may occurmore frequently in certain countries, such asJapan and Uganda, and dark-skinned races havea greater relative incidence of oral malignant mel-anoma and higher mortality rate associated withthis condition (Tarakji et al. 2014). Generally, oralmalignant melanoma occurs at a slightly higherfrequency in males and generally presents after50 years of age with the peak age of diagnosisbetween 65 and 79 years (Alawi 2013; Femiano
Fig. 13 Blue nevus. Spindle-shaped melanocytes(arrows) are embedded within a densely fibrotic laminapropria (hematoxylin and eosin, 200�)
Pigmented Lesions of the Oral Mucosa 9

et al. 2008). Unlike cutaneous malignant mela-noma, histopathologic parameters cannot be reli-ably used to determine prognosis of oralmalignant melanoma (Alawi 2013). Oral malig-nant melanoma is associated with a very poorprognosis; 5-year survival rates range between5% and 50% with a large cluster at 10–25%(Femiano et al. 2008). Less than 10% of patientswith distant metastases survive greater than5 years, and the 10-year survival rate has beenreported to be 0% (Hashemi Pour 2008).
EtiologyWhile the cause of malignant melanoma has notbeen clearly defined, multiple risk factors havebeen associated with onset of the cancer (Limet al. 2014).
Exposure to the sun is the most importantenvironmental cause of cutaneous malignant mel-anoma, with ultraviolet radiation, primarily ultra-violet A type, being most associated withtumorigenesis and development of the disease(Lim et al. 2014). In light-skinned populations,the main nonsolar source of exposure to ultravio-let light are tanning beds, and several recent stud-ies demonstrate that the risk of malignantmelanoma is increased by 20% for those whoever used indoor tanning (Lim et al. 2014).
There is a relationship between a prior personalor family history and malignant melanoma riskwith approximately 10% of malignant melanomasoccurring in familial clusters (Lim et al. 2014).Mutations have been identified in two high-penetrance susceptibility genes, the cyclin-dependent kinase inhibitor 2A (CDKN2A) onchromosome 19p21 and cyclin-dependent kinase4 (CDK4) on chromosome 12q14 (Lim et al.2014). The MC1R gene has been identified as alow penetrance malignant melanoma susceptibil-ity gene, and alterations of the BRAF, HRAS, andNRAS proto-oncogenes, and alteration or loss ofPTEN function, have been associated with malig-nant melanoma development (Lim et al. 2014).
As discussed previously, the number ofmelanocytic nevi represents an independent riskfactor for development of malignant melanoma,with greater than 50 nevi increasing the riskof malignant melanoma approximately four- to
fivefold (Lim et al. 2014). Sun protection atan early age may lower the subsequent risk ofmalignant melanoma (Lim et al. 2014; MacLen-nan et al. 2003).
The etiology of oral malignant melanoma isunknown, and unlike its cutaneous counterpart,risk factors for development have not been clearlydefined (Femiano et al. 2008).
PathophysiologyMalignant melanomas may either develop denovo or from a preexisting benign melanocyticlesion (Chatzistefanou et al. 2016). Melanocytesare neuroectodermal derivatives and normallymigrate to the skin and other ectodermally derivedmucosae (Femiano et al. 2008). Less frequently,melanocytes migrate to endodermally derivedmucosae, such as those found in the head andneck, and melanocytes have been observed inthe deep stroma of oral mucosa (Femiano et al.2008). Due to both extrinsic and intrinsic factorspreviously described, proliferation of malignantmelanocytes gives rise to a variety of melanomatypes.
Clinical-Pathologic FeaturesMalignant melanoma can have a variety of clini-cal appearances, with early lesions typically char-acterized by a macule or plaque with differenthues (brown, black, blue, red, or white) or occa-sionally as an ulceration that does not heal (Limet al. 2014). The ABCDE acronym (asymmetry,border irregularity, color variegation, diametergreater than 6 mm, and evolution or surface ele-vation) is commonly used to initially evaluatepigmented cutaneous lesions, although not allmalignant melanomas present with all of thesefeatures (Lim et al. 2014). The anatomic distribu-tion of malignant melanoma differs by sex andage. In men, lesions are commonly located on thetrunk (55%), especially the back (39%), while inwomen, 42% of malignant melanoma lesions arelocalized to the lower extremities, with 24% onthe lower leg (Lim et al. 2014).
Four major clinical-pathologic subtypes ofnon-oral malignant melanoma have beendescribed: superficial spreading melanoma,lentigo maligna melanoma, acral lentiginous
10 E.T. Stoopler and F. Alawi

melanoma, and nodular melanoma (Lim et al.2014). Superficial spreading melanoma is themost common subtype, accounting for 70% ofall melanoma diagnoses (Lim et al. 2014). Mostlesions of this type occur de novo, and, clinically,
a superficial spreading melanoma appears varie-gated with a sharply marginated, irregular borderand is typically smaller than 3 cm (Lim et al.2014). Multiple hues and shades are often notedwith superficial spreading melanoma, such as tan,brown, gray, black, blue, white, and pink (Limet al. 2014) (Figs. 14 and 15). Nodular melanomarepresents 15% of cutaneous melanomas and ismore common in men (Lim et al. 2014). Typically,they are found on the trunk, and, interestingly,one-third of lesions develop in the head and neck(Lim et al. 2014). Clinically, nodular melanomamay be deeply pigmented (Fig. 16); however, dueto the possibility of melanoma cells being sopoorly differentiated, these cells may stop produc-ing melanin, resulting in a nonpigmentedamelanotic macule. Lentigo maligna melanomaaccounts for 5–10% of melanomas and has apredilection for sun-exposed areas such as thenose, malar region, temple, forehead, neck, andforearms in older adults (Lim et al. 2014). It pre-sents as a slowly enlarging, asymmetric maculewith irregular borders that is variably pigmentedwith tan, brown, black, and possibly white colors(Lim et al. 2014). Acral lentiginous melanoma,the least common subtype, accounts for less than5% of all melanomas but accounts for 70% ofmelanomas seen in African-Americans (Limet al. 2014). Clinically, it affects hairless areaslike subungual, palmar, and plantar regions and
Fig. 14 Superficial spreading melanoma of the scalp(1.2 mm in depth) in an 86-year-old male (Photo courtesy:Dr. Simon Lee, Head of Surgery, The Skin Hospital,Darlinghurst, NSW, Australia)
Fig. 15 Superficial spreading melanoma of the cheek(0.7 mm in depth) in a 71-year-old male (Photo courtesy:Dr. Simon Lee, Head of Surgery, The Skin Hospital,Darlinghurst, NSW, Australia)
Fig. 16 Nodular melanoma on the toe (5.7 mm in depth)in a 67-year-old male (Photo courtesy: Dr. Simon Lee,Head of Surgery, The Skin Hospital, Darlinghurst, NSW,Australia)
Pigmented Lesions of the Oral Mucosa 11

mucous membranes and presents as a variablycolored macule, usually brown or black, whichdevelops irregular borders and increases in sizeover time (Lim et al. 2014).
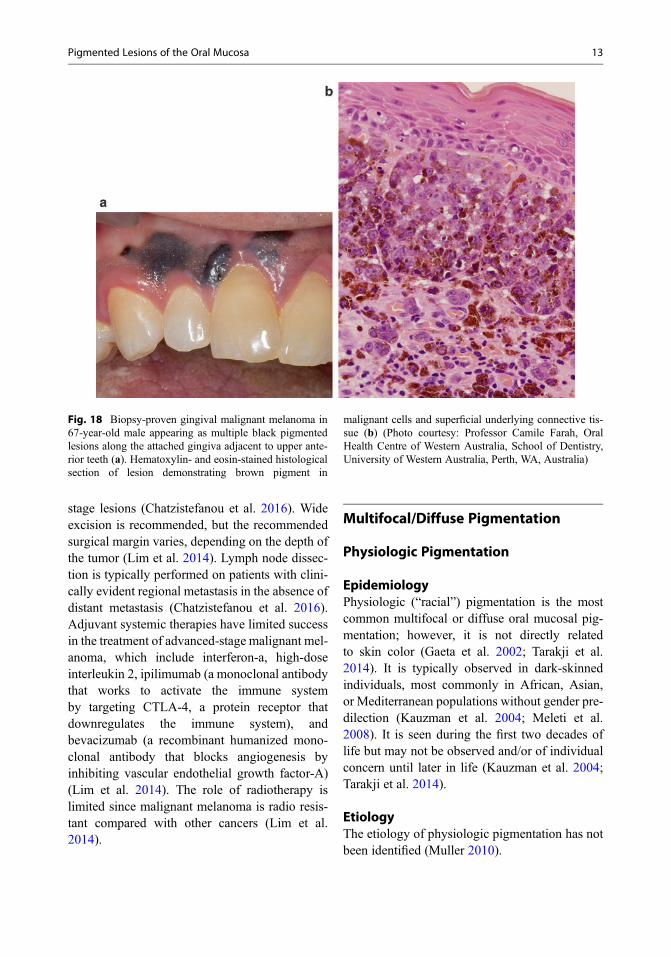
Oral malignant melanoma, however, has nosuch distinctive clinical appearance and is ofteninitially asymptomatic. The lesion typicallybegins as a brown to black macule with irregularborders and may even lack pigment (HashemiPour 2008) (Fig. 17). Lesions are relatively softto palpation and may be accompanied by ery-thema and/or ulceration, which can potentiallycause pain (Mohan et al. 2013). Tooth mobilityor spontaneous exfoliation, root resorption, anes-thesia/paresthesia, and bone loss may be evident(Mohan et al. 2013). Diffuse, contiguous muco-sal pigmentation should be viewed suspiciouslyas possible malignant melanoma compared todiffuse, noncontiguous pigmentation (Alawi2013). While any mucosal site may be affected,the palate is the most common intraoral locationof oral malignant melanoma followed by themaxillary gingiva/alveolar crest (Femiano et al.2008) (Fig. 18a, b). There may be radiographicevidence of “moth-eaten” or irregular bonedestruction associated with these lesions, andcervical lymph nodes may be palpable due tometastasis at initial presentation (Hashemi Pour2008).
Microscopically, superficial spreading mela-noma, lentigo maligna melanoma, and acrallentiginous melanoma demonstrate a lateral andsuperficial spread of melanocytic tumor cells
along the basal layer of the surface epitheliumprior to invasion of the underlying connectivetissue, which is described as radial extension(Lim et al. 2014). Pagetoid and nested epithelioidmelanocytes cells in the intraepidermal portionwith poor circumscription are characteristic ofsuperficial spreading melanoma (Lim et al.2014). In contrast, nodular melanoma is charac-terized by vertical growth of malignant melano-cytes into the connective tissue, which typicallyoccurs early in the disease process. The tumorusually appears as pleomorphic, spindle-shaped,or epithelioid cells arranged in loosely aggregatedsheets and cords.
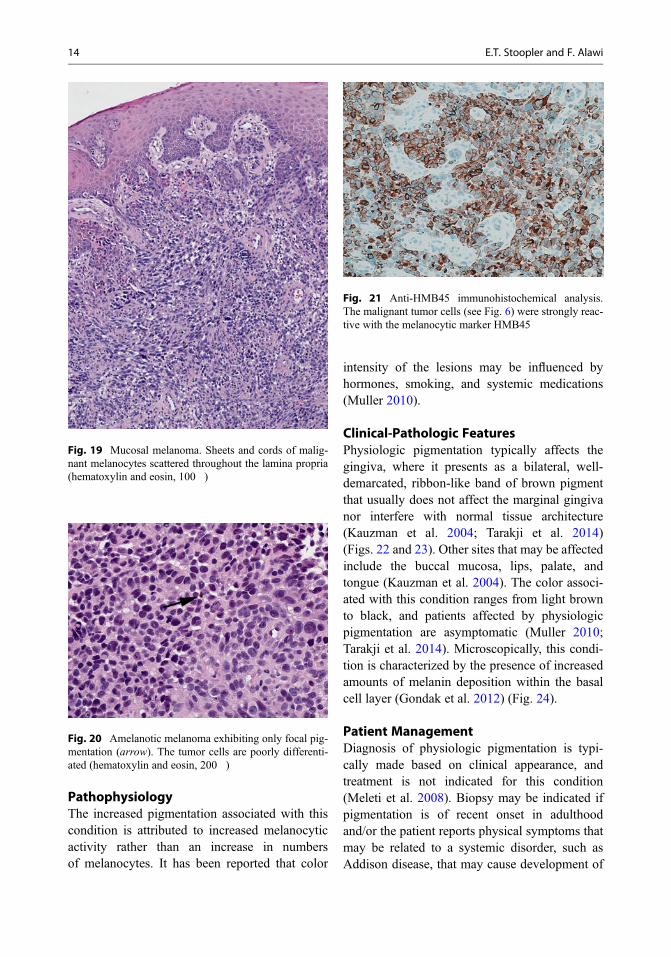
Oral malignant melanomas are usually charac-terized by sheets or islands of malignant melano-cytes within the connective tissue with possiblepagetoid spread (Alawi 2013; Chatzistefanouet al. 2016) (Fig. 19). Poorly differentiated tumorsmay exhibit only minimal pigment or none at all(Fig. 20). Like its cutaneous counterpart, oralmalignant melanomas exhibit an initial radialgrowth phase, typically followed by a verticalpattern of growth with deeper tissue invasion(Chatzistefanou et al. 2016). The presence ofmalignant cells in the lamina propria and a hightumor mitotic rate are characteristic of invadingactivity (Chatzistefanou et al. 2016). Immunohis-tochemistry studies using antibodies directedagainst HMB45, S100, MART1, and/or micro-phthalmia-associated transcription factor (MitF)are necessary for definitive diagnosis of oralmalignant melanoma (Muller 2010) (Fig. 21).
Patient ManagementBiopsy is mandatory for any persistent solitarypigmented lesion, as they can be representativeof a variety of processes, from innocuous lesionsto life-threatening malignant melanoma (Mohanet al. 2013). Once malignant melanoma is diag-nosed, it is important, yet challenging, to deter-mine if the lesion represents a primary malignancyor a metastasis from a distant site, as this informa-tion will dictate tumor staging and direct therapy(Alawi 2013). Surgical excision is the primarytreatment modality for malignant melanoma,which is curative for most patients with early-
Fig. 17 Malignant melanoma present on the lower labialmucosa
12 E.T. Stoopler and F. Alawi
stage lesions (Chatzistefanou et al. 2016). Wideexcision is recommended, but the recommendedsurgical margin varies, depending on the depth ofthe tumor (Lim et al. 2014). Lymph node dissec-tion is typically performed on patients with clini-cally evident regional metastasis in the absence ofdistant metastasis (Chatzistefanou et al. 2016).Adjuvant systemic therapies have limited successin the treatment of advanced-stage malignant mel-anoma, which include interferon-a, high-doseinterleukin 2, ipilimumab (a monoclonal antibodythat works to activate the immune systemby targeting CTLA-4, a protein receptor thatdownregulates the immune system), andbevacizumab (a recombinant humanized mono-clonal antibody that blocks angiogenesis byinhibiting vascular endothelial growth factor-A)(Lim et al. 2014). The role of radiotherapy islimited since malignant melanoma is radio resis-tant compared with other cancers (Lim et al.2014).
Multifocal/Diffuse Pigmentation
Physiologic Pigmentation
EpidemiologyPhysiologic (“racial”) pigmentation is the mostcommon multifocal or diffuse oral mucosal pig-mentation; however, it is not directly relatedto skin color (Gaeta et al. 2002; Tarakji et al.2014). It is typically observed in dark-skinnedindividuals, most commonly in African, Asian,or Mediterranean populations without gender pre-dilection (Kauzman et al. 2004; Meleti et al.2008). It is seen during the first two decades oflife but may not be observed and/or of individualconcern until later in life (Kauzman et al. 2004;Tarakji et al. 2014).
EtiologyThe etiology of physiologic pigmentation has notbeen identified (Muller 2010).
Fig. 18 Biopsy-proven gingival malignant melanoma in67-year-old male appearing as multiple black pigmentedlesions along the attached gingiva adjacent to upper ante-rior teeth (a). Hematoxylin- and eosin-stained histologicalsection of lesion demonstrating brown pigment in
malignant cells and superficial underlying connective tis-sue (b) (Photo courtesy: Professor Camile Farah, OralHealth Centre of Western Australia, School of Dentistry,University of Western Australia, Perth, WA, Australia)
Pigmented Lesions of the Oral Mucosa 13
PathophysiologyThe increased pigmentation associated with thiscondition is attributed to increased melanocyticactivity rather than an increase in numbersof melanocytes. It has been reported that color
intensity of the lesions may be influenced byhormones, smoking, and systemic medications(Muller 2010).
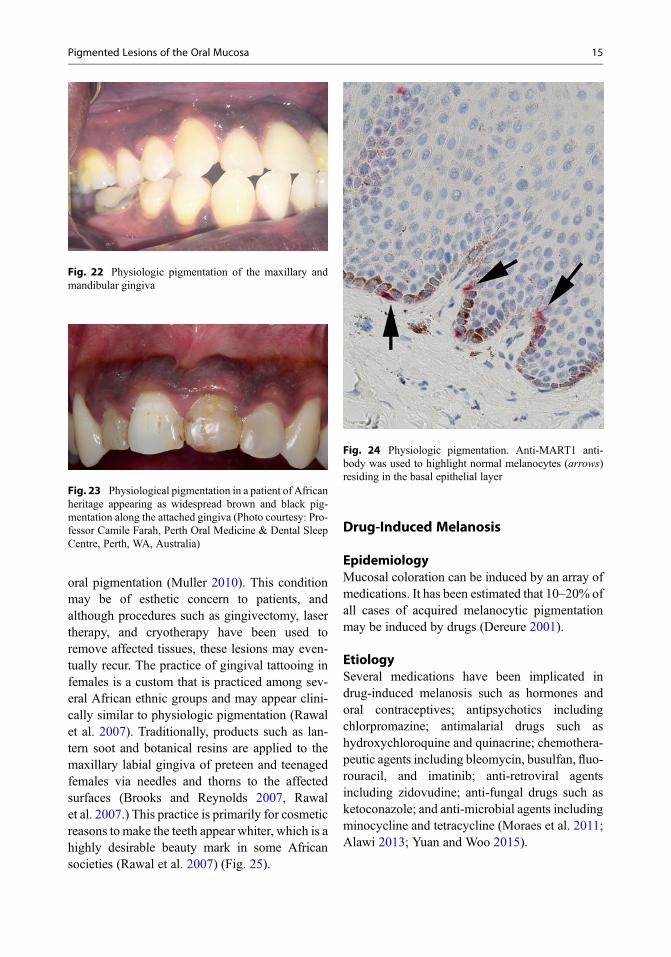
Clinical-Pathologic FeaturesPhysiologic pigmentation typically affects thegingiva, where it presents as a bilateral, well-demarcated, ribbon-like band of brown pigmentthat usually does not affect the marginal gingivanor interfere with normal tissue architecture(Kauzman et al. 2004; Tarakji et al. 2014)(Figs. 22 and 23). Other sites that may be affectedinclude the buccal mucosa, lips, palate, andtongue (Kauzman et al. 2004). The color associ-ated with this condition ranges from light brownto black, and patients affected by physiologicpigmentation are asymptomatic (Muller 2010;Tarakji et al. 2014). Microscopically, this condi-tion is characterized by the presence of increasedamounts of melanin deposition within the basalcell layer (Gondak et al. 2012) (Fig. 24).
Patient ManagementDiagnosis of physiologic pigmentation is typi-cally made based on clinical appearance, andtreatment is not indicated for this condition(Meleti et al. 2008). Biopsy may be indicated ifpigmentation is of recent onset in adulthoodand/or the patient reports physical symptoms thatmay be related to a systemic disorder, such asAddison disease, that may cause development of
Fig. 19 Mucosal melanoma. Sheets and cords of malig-nant melanocytes scattered throughout the lamina propria(hematoxylin and eosin, 100�)
Fig. 20 Amelanotic melanoma exhibiting only focal pig-mentation (arrow). The tumor cells are poorly differenti-ated (hematoxylin and eosin, 200�)
Fig. 21 Anti-HMB45 immunohistochemical analysis.The malignant tumor cells (see Fig. 6) were strongly reac-tive with the melanocytic marker HMB45
14 E.T. Stoopler and F. Alawi
oral pigmentation (Muller 2010). This conditionmay be of esthetic concern to patients, andalthough procedures such as gingivectomy, lasertherapy, and cryotherapy have been used toremove affected tissues, these lesions may even-tually recur. The practice of gingival tattooing infemales is a custom that is practiced among sev-eral African ethnic groups and may appear clini-cally similar to physiologic pigmentation (Rawalet al. 2007). Traditionally, products such as lan-tern soot and botanical resins are applied to themaxillary labial gingiva of preteen and teenagedfemales via needles and thorns to the affectedsurfaces (Brooks and Reynolds 2007, Rawalet al. 2007.) This practice is primarily for cosmeticreasons to make the teeth appear whiter, which is ahighly desirable beauty mark in some Africansocieties (Rawal et al. 2007) (Fig. 25).
Drug-Induced Melanosis
EpidemiologyMucosal coloration can be induced by an array ofmedications. It has been estimated that 10–20% ofall cases of acquired melanocytic pigmentationmay be induced by drugs (Dereure 2001).
EtiologySeveral medications have been implicated indrug-induced melanosis such as hormones andoral contraceptives; antipsychotics includingchlorpromazine; antimalarial drugs such ashydroxychloroquine and quinacrine; chemothera-peutic agents including bleomycin, busulfan, fluo-rouracil, and imatinib; anti-retroviral agentsincluding zidovudine; anti-fungal drugs such asketoconazole; and anti-microbial agents includingminocycline and tetracycline (Moraes et al. 2011;Alawi 2013; Yuan and Woo 2015).
Fig. 22 Physiologic pigmentation of the maxillary andmandibular gingiva
Fig. 23 Physiological pigmentation in a patient of Africanheritage appearing as widespread brown and black pig-mentation along the attached gingiva (Photo courtesy: Pro-fessor Camile Farah, Perth Oral Medicine & Dental SleepCentre, Perth, WA, Australia)
Fig. 24 Physiologic pigmentation. Anti-MART1 anti-body was used to highlight normal melanocytes (arrows)residing in the basal epithelial layer
Pigmented Lesions of the Oral Mucosa 15

PathophysiologyIn some cases, the coloration is true pigmentationresulting from stimulation of melanin synthesis bythe drug and/or its metabolites; the mechanismsmay differ between different drugs. In other cases,drug precipitates deposit within the lamina propriaor submucosa resulting in blue-brown-blackmucosal coloration (Alawi 2013; Yuan and Woo2015).
Clinical-Pathologic FeaturesDrug-induced pigmentation can affect anymucosal site. In general, the gingiva, tongue,and hard palate are most commonly affected(Fig. 26). Some medications, such ashydroxychloroquine, produce characteristic pat-terns of mucosal pigmentation; the palate is usu-ally affected in patients taking this drug (Alawi2013). Minocycline can induce true melanocyticpigmentation and produce precipitates thatdeposit within soft and hard tissues, includingbone, and appear blue gray or even green incolor (Hatch 2005; Kauzman et al. 2004;Bowen and McCalmont 2007; Tarakji et al.2014; Yuan and Woo 2015). Microscopically,basilar hyperpigmentation and melanin inconti-nence without a concomitant increase in number
of melanocytes are characteristics of drug-induced melanotic lesions.
Patient ManagementDiagnosis of drug-induced melanosis can beachieved if a temporal association is madebetween the use of a medication and developmentof pigmentation (Alawi 2013). Biopsy iswarranted if a diagnosis of drug-inducedmelanosis cannot be appropriately rendered(Alawi 2013). Drug-induced melanosis is clini-cally inconsequential beyond potential estheticconcerns. Discontinuation of the medicationmay eventually resolve the pigmentation, whichmay take weeks to months to achieve (Alawi2013). Malignant transformation of drug-inducedmelanotic lesions has not been reported (Tarakjiet al. 2014).
Smoker’s Melanosis
EpidemiologySmoker’s melanosis is the term used to describeoral mucosal pigmentation that develops second-ary to heavy tobacco use. This condition has beenreported to affect nearly 22% of smokers and ismore common in females (Kauzman et al. 2004;Muller 2010). This condition may cause oral pig-mentation to develop in light-skinned individualsand accentuate pigmentation in dark-skinned indi-viduals (Tarakji et al. 2014).
Fig. 25 Extensive gray/black coloration of the maxillarylabial attached gingiva as a result of intraoral cosmetictattooing. Note the presence of diffuse brown pigmentationinvolving the mandibular labial gingiva and the anteriorportions of the maxillary labial gingiva consistent withphysiological pigmentation (Photo courtesy: ProfessorMichael McCullough, Melbourne Dental School, Univer-sity of Melbourne, VIC, Australia)
Fig. 26 Chemotherapy-induced pigmentation affectingthe tongue
16 E.T. Stoopler and F. Alawi
EtiologyPolycyclic amines, such as nicotine and benzopy-rene, are chemical compounds in tobaccosmoke that have demonstrated the ability to stim-ulate melanocytes to produce melanin (Hassonaet al. 2016).
PathophysiologyMelanin pigmentation in the skin is protectiveagainst ultraviolet damage, and melanocytes innon-sun-exposed areas produce melanin thatcan bind to noxious substances (Meleti et al.2008). It has been postulated that melanin produc-tion stimulated by tobacco smoke may have aprotective role against the harmful agents in thesmoke, such as those described previously(Hassona et al. 2016; Muller 2010). Additionally,the heat of the smoke is thought to be a stimulatingfactor for pigment development (Alawi 2013).Since smoker’s melanosis is more prevalent inwomen, it has been suggested that female sexhormones (i.e., estrogen) may have a role indevelopment of this condition (Kauzman et al.2004; Muller 2010).
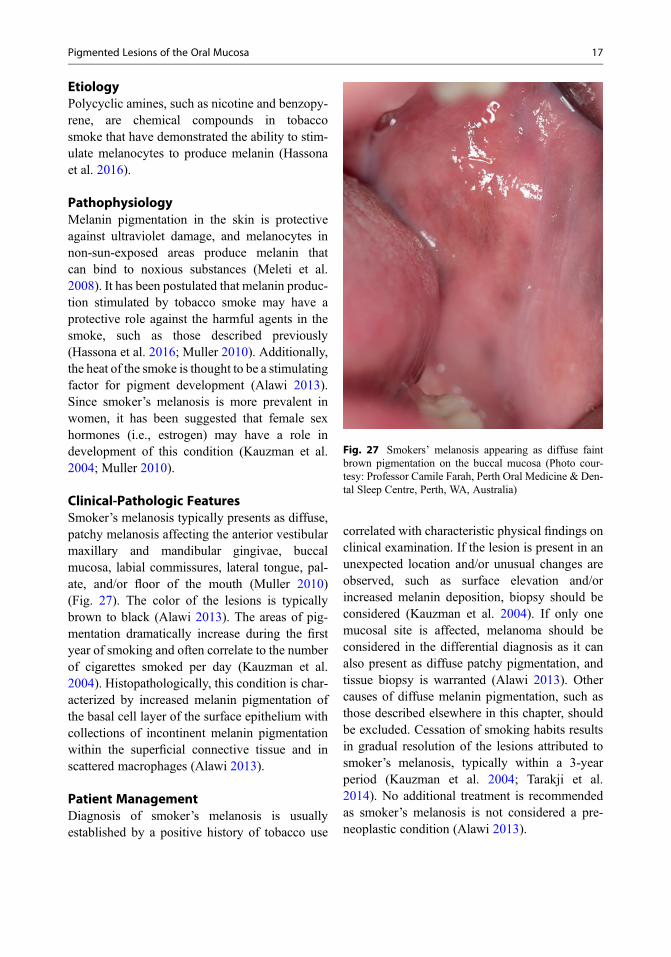
Clinical-Pathologic FeaturesSmoker’s melanosis typically presents as diffuse,patchy melanosis affecting the anterior vestibularmaxillary and mandibular gingivae, buccalmucosa, labial commissures, lateral tongue, pal-ate, and/or floor of the mouth (Muller 2010)(Fig. 27). The color of the lesions is typicallybrown to black (Alawi 2013). The areas of pig-mentation dramatically increase during the firstyear of smoking and often correlate to the numberof cigarettes smoked per day (Kauzman et al.2004). Histopathologically, this condition is char-acterized by increased melanin pigmentation ofthe basal cell layer of the surface epithelium withcollections of incontinent melanin pigmentationwithin the superficial connective tissue and inscattered macrophages (Alawi 2013).
Patient ManagementDiagnosis of smoker’s melanosis is usuallyestablished by a positive history of tobacco use
correlated with characteristic physical findings onclinical examination. If the lesion is present in anunexpected location and/or unusual changes areobserved, such as surface elevation and/orincreased melanin deposition, biopsy should beconsidered (Kauzman et al. 2004). If only onemucosal site is affected, melanoma should beconsidered in the differential diagnosis as it canalso present as diffuse patchy pigmentation, andtissue biopsy is warranted (Alawi 2013). Othercauses of diffuse melanin pigmentation, such asthose described elsewhere in this chapter, shouldbe excluded. Cessation of smoking habits resultsin gradual resolution of the lesions attributed tosmoker’s melanosis, typically within a 3-yearperiod (Kauzman et al. 2004; Tarakji et al.2014). No additional treatment is recommendedas smoker’s melanosis is not considered a pre-neoplastic condition (Alawi 2013).
Fig. 27 Smokers’ melanosis appearing as diffuse faintbrown pigmentation on the buccal mucosa (Photo cour-tesy: Professor Camile Farah, Perth Oral Medicine & Den-tal Sleep Centre, Perth, WA, Australia)
Pigmented Lesions of the Oral Mucosa 17
Post-inflammatory (Inflammatory)Hyperpigmentation
EpidemiologyPost-inflammatory (inflammatory) hyper-pigmentation is a condition characterized by pig-ment deposition in area(s) subjected toinflammation or previous injury that is more com-monly observed in dark-complexioned individ-uals (Alawi 2013).
EtiologyThe etiology of post-inflammatory (inflamma-tory) hyperpigmentation has not been determined(Gondak et al. 2012; Tarakji et al. 2014).
PathophysiologyInflammatory conditions, such as lichen planus,cause perturbation of epithelial melanocytes,resulting in increased melanin deposition inaffected areas (Kauzman et al. 2004).
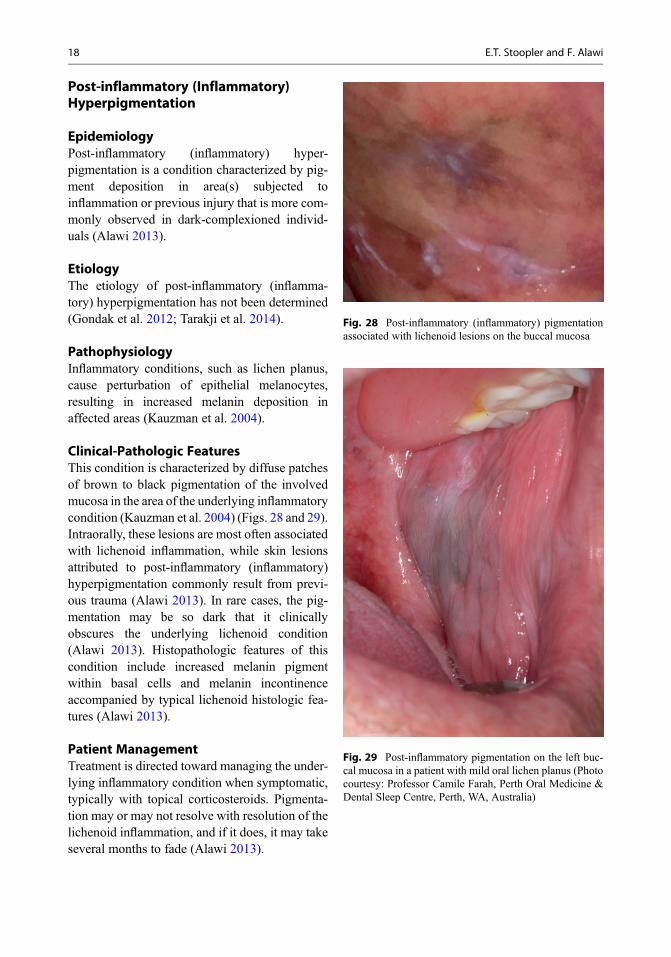
Clinical-Pathologic FeaturesThis condition is characterized by diffuse patchesof brown to black pigmentation of the involvedmucosa in the area of the underlying inflammatorycondition (Kauzman et al. 2004) (Figs. 28 and 29).Intraorally, these lesions are most often associatedwith lichenoid inflammation, while skin lesionsattributed to post-inflammatory (inflammatory)hyperpigmentation commonly result from previ-ous trauma (Alawi 2013). In rare cases, the pig-mentation may be so dark that it clinicallyobscures the underlying lichenoid condition(Alawi 2013). Histopathologic features of thiscondition include increased melanin pigmentwithin basal cells and melanin incontinenceaccompanied by typical lichenoid histologic fea-tures (Alawi 2013).
Patient ManagementTreatment is directed toward managing the under-lying inflammatory condition when symptomatic,typically with topical corticosteroids. Pigmenta-tion may or may not resolve with resolution of thelichenoid inflammation, and if it does, it may takeseveral months to fade (Alawi 2013).
Fig. 28 Post-inflammatory (inflammatory) pigmentationassociated with lichenoid lesions on the buccal mucosa
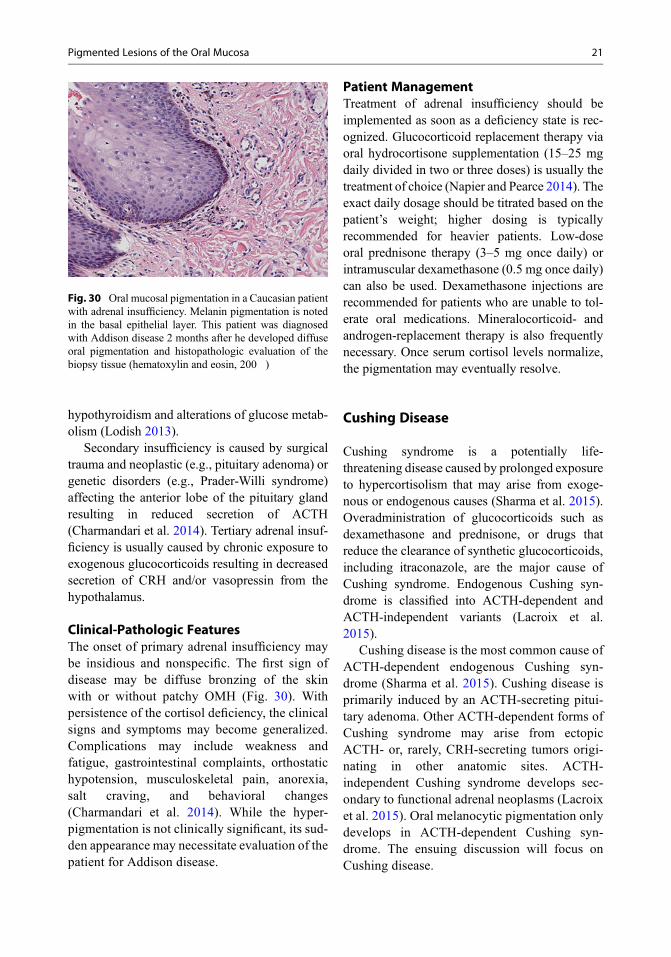
Fig. 29 Post-inflammatory pigmentation on the left buc-cal mucosa in a patient with mild oral lichen planus (Photocourtesy: Professor Camile Farah, Perth Oral Medicine &Dental Sleep Centre, Perth, WA, Australia)
18 E.T. Stoopler and F. Alawi

Laugier-Hunziker Pigmentation
EpidemiologyLaugier-Hunziker pigmentation (Laugier-Hunzikersyndrome, Laugier-Hunziker-Baran syndrome) ischaracterized by acquired melanotic pigmentationof the labial and buccal mucosa (Alawi 2013; Yagoet al. 2008). This is considered a rare condition thatusually begins in the third to fifth decade of lifewith an overall female-male ratio of 2:1 (Nikitakisand Koumaki 2013; Yago et al. 2008). This condi-tion has been reported in individuals in NorthAmerica, Europe, and Asia and has been morecommonly observed in Caucasian or light-skinnedindividuals (Yago et al. 2008).
EtiologyWhile the etiology of Laugier-Hunziker pigmen-tation is unknown, hormonal or genetic roles havenot been associated with this condition (Alawi2013; Fernandes et al. 2015; Nikitakis andKoumaki 2013).
PathophysiologyThe precise pathophysiologic mechanism ofLaugier-Hunziker pigmentation is unclear, but itis considered an acquired pigmentation disorderthat results from increased basal keratinocyte mel-anin without an increase in melanocytes(Nikitakis and Koumaki 2013).
Clinical-Pathologic FeaturesMultifocal, macular hyperpigmentation of the oralmucosa and lips is characteristic of Laugier-Hunziker pigmentation (Alawi 2013; Nikitakisand Koumaki 2013). Lesions may be solitary orconfluent, brown to black to gray in color, andhave been reported in all regions of the oral cavity,including the lips, buccal mucosa, tongue, hardpalate, and gingiva (Nikitakis and Koumaki2013). Melanotic longitudinal streaks in the nailswithout associated nail dystrophy are frequentlyassociated with oral pigmentation (Alawi 2013;Nikitakis and Koumaki 2013; Yago et al. 2008).Up to 60% of affected patients have nail involve-ment with fingernails more commonly affectedthan toenails (Fernandes et al. 2015). Similarlesions may be observed on other cutaneous
surfaces, such as the facial skin and abdomen,and other mucosal surfaces, including the esoph-agus, conjunctiva, and anogenital mucosa (Alawi2013; Nikitakis and Koumaki 2013). Typical his-tologic findings associated with Laugier-Hunzikerpigmentation include increased basal keratinocytemelanin without an increase in number of mela-nocytes, melanin incontinence, and epithelialacanthosis in the absence of rete ridges or inflam-mation (Nikitakis and Koumaki 2013).
Patient ManagementTreatment for this condition is typically not indi-cated unless there is an esthetic and/or psycholog-ical concern (Nikitakis and Koumaki 2013). Lasertherapy and cryotherapy have been used to removepigmentation, but recurrence is possible (Nikitakisand Koumaki 2013). It is important to considersystemic etiologies in the differential diagnosis ofLaugier-Hunziker pigmentation, such as Addisondisease and Peutz-Jeghers syndrome, as these con-ditions are also characterized by multiple oralmucosal macules (Nikitakis and Koumaki 2013).A thorough medical, social, and family history, inaddition to a complete review of systems, areimportant in rendering an accurate diagnosis andappropriate referral to medical specialists, if neces-sary. Biopsy may be considered to confirm theclinical diagnosis and rule out other sources oforal pigmentation. Laugier-Hunziker pigmentationis a diagnosis of exclusion after all other potentialsources for pigmentation have been eliminated asan etiology for the condition (Alawi 2013).Laugier-Hunziker pigmentation is not associatedwith malignant predisposition (Fernandes et al.2015; Rangwala et al. 2010; Yago et al. 2008).
Pigmentation Associatedwith Systemic or Genetic Disorders
Adrenal Insufficiency (AddisonDisease)
EpidemiologyAdrenal insufficiency is a potentially life-threatening endocrinopathy that is characterizedby diminished production of glucocorticoids
Pigmented Lesions of the Oral Mucosa 19

(cortisol) with or without a concomitant defi-ciency in mineralocorticoid and adrenal androgenlevels (Naziat and Grossman 2000). Dysfunctionin the hypothalamus-pituitary-adrenal gland axisgives rise to adrenal insufficiency. Primary, sec-ondary, and tertiary forms of adrenal insufficiencyare dependent upon the anatomic site of originprecipitating the dysfunction.
An estimated 4.4–6 new cases of primary adre-nal insufficiency develop per million people peryear (Charmandari et al. 2014). In contrast, sec-ondary adrenal insufficiency is more commonthan the primary disease with an estimated preva-lence of 150–280 per million people. Overall, theprevalence of Addison disease in Caucasians isestimated to be between 1 in 8000–20,000 in theUnited States and Europe (Naziat and Grossman2000). Primary adrenal insufficiency manifestsmore frequently in females than males and oftenbetween the ages of 30 and 50. Secondary diseaseis also more common in females but is usuallydiagnosed later in life. While the prevalence oforal mucosal hyperpigmentation (OMH) associ-ated with adrenal insufficiency is not known,OMH is observed only in primary disease states.
EtiologyThe hypothalamus-pituitary-adrenal gland axisis tightly coordinated to ensure glucocorticoidhomeostasis (Charmandari et al. 2014). Thehypothalamus produces corticotropin-releasinghormone (CRH) and vasopressin. These hor-mones act synergistically on the pituitary glandto activate pro-opiomelanocortin (POMC) geneexpression (Anderson et al. 2016). Thecorresponding 241 amino acid POMC polypep-tide then undergoes an array of posttranslationalmodifications to yield several biologically distincthormone peptides. These include adrenocortico-tropic hormone (ACTH); α-, β-, andγ-melanotropins (also known as melanocyte stim-ulating hormone), respectively, β- andγ-lipotropins; β-endorphin; and metenkephalin(Anderson et al. 2016). ACTH is secreted intothe circulation and binds to receptors in the adre-nal cortex to stimulate glucocorticoid productionand release. Once serum cortisol levels are stabi-lized, ACTH and CRH synthesis are inhibited
through an intricate negative feedback mecha-nism. When reduced cortisol levels are sensedby the hypothalamus, the CRH-POMC-ACTH-cortisol signaling cascade is reactivated.
OMH is observed only in primary adrenalinsufficiency (Charmandari et al. 2014). The con-stitutively low cortisol levels stimulate persistentPOMC production to yield high levels of ACTH.Since the defective adrenal glands are unable tosufficiently respond to ACTH, the signaling cas-cade remains active. In conjunction with ACTHoverproduction, α-MSH levels are also increasedin parallel. α-MSH is a short peptide encodedwithin the ACTH peptide and generated via post-translational cleavage (Anderson et al. 2016).Since α-MSH is a potent stimulator of melano-genesis, this triggers the mucocutaneous pigmen-tation observed in primary adrenal insufficiency(Anderson et al. 2016; Feller et al. 2014b). ACTHand α-MSH levels are reduced in secondary andtertiary adrenal insufficiency (Charmandari et al.2014). Thus, the pigmentation does not occur inthese forms of the disease.
PathophysiologyPrimary adrenal insufficiency is caused by adre-nocortical disease. While the most common causeis autoimmune adrenalitis, other conditions suchas cancer, infection, and hemorrhagic infarctioncan also directly damage the adrenal glands(Charmandari et al. 2014). Several genetic disor-ders may lead to congenital defects in adrenalgland structure and function. Other genetic dis-eases may affect sensitivity of the glands toACTH, limit glucocorticoid synthesis, or acceler-ate cortisol metabolism. A number of medicationscan also limit glucocorticoid biosynthesis oraccelerate cortisol metabolism (Michels andMichels 2014). Examples include phenobarbitaland phenytoin which activate cytochrome P450enzymes thereby stimulating glucocorticoidmetabolism. The antimycotic fluconazole andketoconazole reduce cortisol synthesis byinhibiting mitochondrial cytochrome P450enzymes. In rare instances, the use of the tyrosinekinase inhibitors imatinib, saracatinib, andsunitinib has been associated with adrenal insuf-ficiency and other endocrinopathies, including
20 E.T. Stoopler and F. Alawi
hypothyroidism and alterations of glucose metab-olism (Lodish 2013).
Secondary insufficiency is caused by surgicaltrauma and neoplastic (e.g., pituitary adenoma) orgenetic disorders (e.g., Prader-Willi syndrome)affecting the anterior lobe of the pituitary glandresulting in reduced secretion of ACTH(Charmandari et al. 2014). Tertiary adrenal insuf-ficiency is usually caused by chronic exposure toexogenous glucocorticoids resulting in decreasedsecretion of CRH and/or vasopressin from thehypothalamus.
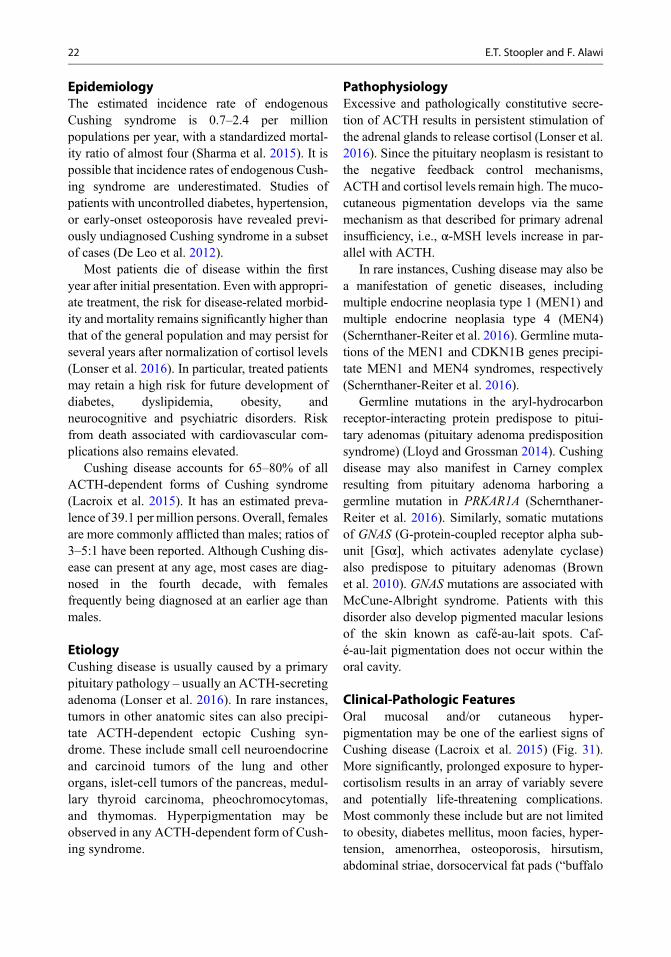
Clinical-Pathologic FeaturesThe onset of primary adrenal insufficiency maybe insidious and nonspecific. The first sign ofdisease may be diffuse bronzing of the skinwith or without patchy OMH (Fig. 30). Withpersistence of the cortisol deficiency, the clinicalsigns and symptoms may become generalized.Complications may include weakness andfatigue, gastrointestinal complaints, orthostatichypotension, musculoskeletal pain, anorexia,salt craving, and behavioral changes(Charmandari et al. 2014). While the hyper-pigmentation is not clinically significant, its sud-den appearance may necessitate evaluation of thepatient for Addison disease.
Patient ManagementTreatment of adrenal insufficiency should beimplemented as soon as a deficiency state is rec-ognized. Glucocorticoid replacement therapy viaoral hydrocortisone supplementation (15–25 mgdaily divided in two or three doses) is usually thetreatment of choice (Napier and Pearce 2014). Theexact daily dosage should be titrated based on thepatient’s weight; higher dosing is typicallyrecommended for heavier patients. Low-doseoral prednisone therapy (3–5 mg once daily) orintramuscular dexamethasone (0.5 mg once daily)can also be used. Dexamethasone injections arerecommended for patients who are unable to tol-erate oral medications. Mineralocorticoid- andandrogen-replacement therapy is also frequentlynecessary. Once serum cortisol levels normalize,the pigmentation may eventually resolve.
Cushing Disease
Cushing syndrome is a potentially life-threatening disease caused by prolonged exposureto hypercortisolism that may arise from exoge-nous or endogenous causes (Sharma et al. 2015).Overadministration of glucocorticoids such asdexamethasone and prednisone, or drugs thatreduce the clearance of synthetic glucocorticoids,including itraconazole, are the major cause ofCushing syndrome. Endogenous Cushing syn-drome is classified into ACTH-dependent andACTH-independent variants (Lacroix et al.2015).
Cushing disease is the most common cause ofACTH-dependent endogenous Cushing syn-drome (Sharma et al. 2015). Cushing disease isprimarily induced by an ACTH-secreting pitui-tary adenoma. Other ACTH-dependent forms ofCushing syndrome may arise from ectopicACTH- or, rarely, CRH-secreting tumors origi-nating in other anatomic sites. ACTH-independent Cushing syndrome develops sec-ondary to functional adrenal neoplasms (Lacroixet al. 2015). Oral melanocytic pigmentation onlydevelops in ACTH-dependent Cushing syn-drome. The ensuing discussion will focus onCushing disease.
Fig. 30 Oral mucosal pigmentation in a Caucasian patientwith adrenal insufficiency. Melanin pigmentation is notedin the basal epithelial layer. This patient was diagnosedwith Addison disease 2 months after he developed diffuseoral pigmentation and histopathologic evaluation of thebiopsy tissue (hematoxylin and eosin, 200�)
Pigmented Lesions of the Oral Mucosa 21
EpidemiologyThe estimated incidence rate of endogenousCushing syndrome is 0.7–2.4 per millionpopulations per year, with a standardized mortal-ity ratio of almost four (Sharma et al. 2015). It ispossible that incidence rates of endogenous Cush-ing syndrome are underestimated. Studies ofpatients with uncontrolled diabetes, hypertension,or early-onset osteoporosis have revealed previ-ously undiagnosed Cushing syndrome in a subsetof cases (De Leo et al. 2012).
Most patients die of disease within the firstyear after initial presentation. Even with appropri-ate treatment, the risk for disease-related morbid-ity and mortality remains significantly higher thanthat of the general population and may persist forseveral years after normalization of cortisol levels(Lonser et al. 2016). In particular, treated patientsmay retain a high risk for future development ofdiabetes, dyslipidemia, obesity, andneurocognitive and psychiatric disorders. Riskfrom death associated with cardiovascular com-plications also remains elevated.
Cushing disease accounts for 65–80% of allACTH-dependent forms of Cushing syndrome(Lacroix et al. 2015). It has an estimated preva-lence of 39.1 per million persons. Overall, femalesare more commonly afflicted than males; ratios of3–5:1 have been reported. Although Cushing dis-ease can present at any age, most cases are diag-nosed in the fourth decade, with femalesfrequently being diagnosed at an earlier age thanmales.
EtiologyCushing disease is usually caused by a primarypituitary pathology – usually an ACTH-secretingadenoma (Lonser et al. 2016). In rare instances,tumors in other anatomic sites can also precipi-tate ACTH-dependent ectopic Cushing syn-drome. These include small cell neuroendocrineand carcinoid tumors of the lung and otherorgans, islet-cell tumors of the pancreas, medul-lary thyroid carcinoma, pheochromocytomas,and thymomas. Hyperpigmentation may beobserved in any ACTH-dependent form of Cush-ing syndrome.
PathophysiologyExcessive and pathologically constitutive secre-tion of ACTH results in persistent stimulation ofthe adrenal glands to release cortisol (Lonser et al.2016). Since the pituitary neoplasm is resistant tothe negative feedback control mechanisms,ACTH and cortisol levels remain high. The muco-cutaneous pigmentation develops via the samemechanism as that described for primary adrenalinsufficiency, i.e., α-MSH levels increase in par-allel with ACTH.
In rare instances, Cushing disease may also bea manifestation of genetic diseases, includingmultiple endocrine neoplasia type 1 (MEN1) andmultiple endocrine neoplasia type 4 (MEN4)(Schernthaner-Reiter et al. 2016). Germline muta-tions of the MEN1 and CDKN1B genes precipi-tate MEN1 and MEN4 syndromes, respectively(Schernthaner-Reiter et al. 2016).
Germline mutations in the aryl-hydrocarbonreceptor-interacting protein predispose to pitui-tary adenomas (pituitary adenoma predispositionsyndrome) (Lloyd and Grossman 2014). Cushingdisease may also manifest in Carney complexresulting from pituitary adenoma harboring agermline mutation in PRKAR1A (Schernthaner-Reiter et al. 2016). Similarly, somatic mutationsof GNAS (G-protein-coupled receptor alpha sub-unit [Gsα], which activates adenylate cyclase)also predispose to pituitary adenomas (Brownet al. 2010). GNAS mutations are associated withMcCune-Albright syndrome. Patients with thisdisorder also develop pigmented macular lesionsof the skin known as café-au-lait spots. Caf-é-au-lait pigmentation does not occur within theoral cavity.
Clinical-Pathologic FeaturesOral mucosal and/or cutaneous hyper-pigmentation may be one of the earliest signs ofCushing disease (Lacroix et al. 2015) (Fig. 31).More significantly, prolonged exposure to hyper-cortisolism results in an array of variably severeand potentially life-threatening complications.Most commonly these include but are not limitedto obesity, diabetes mellitus, moon facies, hyper-tension, amenorrhea, osteoporosis, hirsutism,abdominal striae, dorsocervical fat pads (“buffalo
22 E.T. Stoopler and F. Alawi

hump”), cutaneous purpura, poor wound healing,muscular weakness, psychological, psychiatricand neurocognitive disturbances, immune sup-pression, male impotence, and female infertility(Lacroix et al. 2015).
Patient ManagementThere is no specific treatment for the pigmenta-tion. Treatment of the underlying cause of Cush-ing disease – usually surgical removal of thepituitary tumor – often times has an immediateinhibitory effect on cortisol secretion (Lau et al.2015). In cases where the tumor may be inopera-ble, radiation therapy may be employed, or thehypercortisolism may be treated medicinally.Medical therapies can target the pituitary gland,the adrenal gland, or the peripheral tissues. Pitui-tary targeting is designed to inhibit ACTH syn-thesis and secretion. Cabergoline (dopamine2 receptor agonist) and pasireotide (somatostatin5 receptor agonist) are two drugs that are currentlyavailable for patients who are poor surgical can-didates or who failed surgical therapy (Lau et al.2015). Steroidogenic inhibitors including ketoco-nazole may be used to inhibit cortisol synthesis.Mifepristone is a progesterone receptor antagonistthat also inhibits glucocorticoid receptor activity.Mifepristone reduces the hyperglycemia associ-ated with Cushing disease. Resolution of the bio-chemical defect will result in normalization ofACTH and α-MSH levels. Over time, the pigmen-tation may eventually resolve.
Human Immunodeficiency Virus (HIV):Associated Pigmentation
EpidemiologyOMH is a recognized occurrence in HIV-seropos-itive and AIDS-afflicted individuals. If itdevelops, the pigmentation usually becomesapparent within the first 2 years after initial HIVdiagnosis and usually in patients with CD4+ T-cellcounts of 200 cells/mm3 or less (Feller et al.2014a). A potential relationship between viralload and OMH remains uncertain.
The overall prevalence of OMH is not known.However, there are geographic and ethnic differ-ences that could reflect specific characteristics ofthe HIV infection, access to appropriate treatment,and/or administration of specific drug regimens.In South Africa, Venezuela, and India, 18.5–38%of HIV-seropositive patients were identified withOMH (Bravo et al. 2006; Chandran et al. 2016;Feller et al. 2014a). In contrast, in Greece and ItalyOMH accounts for less than 2% and 7%, respec-tively, of all examined patients. In general, muco-sal pigmentation is usually more prominent indarker-skinned individuals and may be moreprevalent in females than in males (Feller et al.2014a). In at least one study, HIV-associatedOMH was also significantly associated withsmoking (Chandran et al. 2016).
EtiologyThe etiology of HIV/AIDS-associated pigmenta-tion is multifactorial. There is currently no evi-dence HIV can directly infect or activatemelanocytes (Feller et al. 2014a). Instead,HIV-induced cytokine dysregulation may induceOMH. Nonspecific, generalized oral mucosalinflammation could also be contributory.Pro-inflammatory cytokines including interleukin(IL)-1, IL-6, and tumor necrosis factor (TNF)-αare known to regulate melanocytes andmelanogenesis (Feller et al. 2014b). Constitutiveupregulation of these and other pro-inflammatorymediators may stimulate production of α-MSHthereby leading to the pigmentation.HIV-induced cytokine dysregulation typicallyparallels decreasing CD4+ T-cell counts (Felleret al. 2014a).
Fig. 31 Multifocal mucosal pigmentation on the hardpalate (arrows) in a patient who was eventually diagnosedwith Cushing syndrome
Pigmented Lesions of the Oral Mucosa 23

More commonly, OMH may arise in responseto treatment with a number of different medica-tions frequently used to treat HIV/AIDS and itsassociated complications; zidovudine (azidothy-midine [AZT]; nucleoside reverse transcriptaseinhibitor) is just one example (Feller et al.2014a). The pigment frequently appears withinthe first few weeks after initiation of the therapy.When the drug is withdrawn, the pigment usuallydiminishes. OMH is significantly more commonin HIV-seropositive patients treated with antire-troviral therapy (ART) than in ART-naïveindividuals.
Primary or secondary adrenocortical dysfunc-tion may occur in as many as 20% of HIV patients(Hruz 2014). This may be due to HIV-associatedviral or mycobacterial infections of the adrenalgland or by medications used to treat the disease.Ritonavir (protease inhibitor) in combination withexogenous steroids is known to induce adrenalinsufficiency which, in turn, may induce the pig-mentation (Wood et al. 2015).
PathophysiologyThe pathogenesis of HIV-associated pigmentationvaries depending on the etiologic agent. Similar toother forms of OMH, the pigmentation is usuallythe result of increased melanogenesis without achange in melanocyte number. The pigment isconcentrated within the basal layer of the stratifiedsquamous epithelium and accompanied by mela-nin incontinence within the papillary lamina pro-pria (Feller et al. 2014a). The pigment is ofteneasily visualized in biopsy tissue with routinelight microscopy. HIV-induced cytokinedysregulation and AZT and other medicationsmay also induce pigmentation by stimulatingmelanocytic hyperplasia accompanied by anincrease in melanin synthesis.
Clinical-Pathologic FeaturesThe pigmentation may manifest as multiple dis-crete light to dark brown macules or as patchy anddiffuse. The coloration may appear anywherewithin the oral cavity, but the gingiva tends to bethe most commonly affected site. In darker-skinned individuals, differentiatingHIV-associated pigment from physiologic
pigmentation may be difficult. The appearance,extent, and intensity of OMH is also similar tothat observed in other disorders known to inducemucocutaneous pigmentation. The diagnosis ofHIV-associated pigmentation is rendered if thepigment initially appears or becomes exacerbatedafter the diagnosis of HIV infection or followingthe initiation of therapy (Feller et al. 2014a).
Patient ManagementApart from possible esthetic concerns, there doesnot appear any clinical significance attributable toHIV-associated OMH. However, new onset oralpigmentation in an individual deemed potentiallyhigh risk for HIV infection, including intravenousdrug users, should prompt an evaluation for pos-sible infection.
Peutz-Jeghers Syndrome
Peutz-Jeghers syndrome (PJS) is an autosomaldominant disorder associated with oral and peri-oral melanocytic pigmentation, benignhamartomatous polyps of the gastrointestinaltract, and increased risk for developing malignan-cies of the gastrointestinal tract, breast, uterinecervix, ovary, pancreas, and other anatomic sites(Riegert-Johnson et al. 2009). The risk is esti-mated to be 18-fold higher than that of the generalpopulation. The hyperpigmentation often mani-fests early in life and may be the first sign ofdisease in some patients.
EpidemiologySince PJS is a rare disorder, reliable estimates ofincidence and prevalence are lacking. Nonethe-less, PJS has an estimated incidence of 1 in8000–200,000 live births without gender or racialpredilection (Riegert-Johnson et al. 2009). Mor-tality associated with PJS is usually cancerrelated.
EtiologyApproximately 75% of all PJS patients harbor agermline mutation in the SKT11 (LKB1) genelocated on chromosome 19p13.3 (Meserve andNucci 2016). The remaining patients do not have
24 E.T. Stoopler and F. Alawi

known STK11 mutations; the genetic cause ofthese patients’ disease remains undetermined.Mutations in STK11-interacting proteins havenot yet been found in these latter patients. Thus,it has been suggested that these patients may havelarge STK11 gene rearrangements that cannot beidentified by routine molecular testing (Meserveand Nucci 2016).
PathophysiologySTK11 is serine-threonine kinase that directsenergy sensing and nutrient metabolism throughactivation of an array of downstream factors(Shorning and Clarke 2016). Together, STK11and its phosphorylated substrates help to regulatecellular metabolism, proliferation, polarity, anddifferentiation by maintaining and monitoring cel-lular energy homeostasis. STK11 also contributesto genomic stability by participating in DNAdouble-strand break repair.
It is apparent that STK11 plays an importantrole in melanocyte biology since the mucocutane-ous pigmentation is observed in essentially allpatients with PJS (Ponti et al. 2016). Moreover,the hyperpigmentation can be observed inSTK11-deficient murine models (Meserve andNucci 2016). Nonetheless, the mechanisms bywhich loss of STK11 function induces hyper-pigmentation remain unclear.
Clinical-Pathologic FeaturesPJS is commonly associated with multiple mela-notic macules of the lips accompanied by diffuse
freckling of the perioral skin (Ponti et al. 2016)(Fig. 32). The pigmented macules may coalesce toproduce broader areas of pigmentation. Less com-monly, intraoral pigmentation may also beobserved; the tongue and buccal and/or labialmucosae are typically affected. Pigmented spotsare also commonly observed on the fingertips.The pigmentation typically presents duringinfancy, childhood, or adolescence, and is oftenthe first sign of PJS. At least some of the pigmen-tation may spontaneously resolve with age.
A biopsy of a pigmented lesion usually revealsnonspecific histopathology (Ponti et al. 2016).There is increased melanin pigmentation withinthe basal epithelial layer and melanin inconti-nence within the papillary lamina propria. Theremay also be evidence of melanocytic hyperplasia.
Note that while highly characteristic, the pat-tern of labial and perioral pigmentation is notpathognomonic for PJS. Laugier-Hunziker pig-mentation is an acquired and idiopathic form ofpigmentation that frequently mimics PJS andshould be considered in the differential diagnosis(Alawi 2013). However, Laugier-Hunziker pig-mentation typically manifests during adulthoodand may be accompanied by pigmentation of thenails. Patients with Laugier-Hunziker pigmenta-tion do not exhibit STK11 mutations, and they donot manifest with gastrointestinal polyps.
Apart from the gastrointestinal polyps and can-cer, other systemic complications may includeintussusception, rectal bleeding, iron deficiencyanemia, and development of ovarian cysts(Riegert-Johnson et al. 2009).
Patient ManagementThe development of labial and perioral pigmenta-tion early in life should prompt genetic testing forPJS (Meserve and Nucci 2016). In patients with aknown family history or in newly diagnosedpatients, surveillance strategies should bedesigned to ensure continuous and lifelong clini-cal monitoring. Surgical treatment may be neededto remove potentially obstructive gastrointestinalpolyps. Iron supplementation may be necessaryfor a subset of patients who are anemic. Prognosisis primarily related to the occurrence of cancer(Meserve and Nucci 2016). The pigmentation is
Fig. 32 Perioral melanosis associated with Peutz-Jegherssyndrome
Pigmented Lesions of the Oral Mucosa 25

not symptomatic and does not require treatmentunless there is an esthetic concern.
Exogenous Causes of ClinicalPigmentation
Tattoos: Amalgam, Graphite,and Ornamental
The most common nonphysiologic source of oralmucosal coloration is exogenous and not endoge-nous in origin (Alawi 2013). Amalgam tattoos arethe most common cause of oral “pigmentation”(Alawi 2013). They result from the iatrogenicmucosal implantation of amalgam particles usu-ally during the course of a dental procedure.Amalgam tattoos are macular, usually small andfrequently identified in close proximity toamalgam-restored teeth or in areas where suchteeth were previously present (Figs. 33a–c, 34,35, and 36). Amalgam tattoos may be identifiedin any oral location, but the gingiva and alveolarmucosa are most commonly affected.
While an amalgam tattoo may be blue gray toblack in color, and thus the mucosa may appearclinically pigmented, the mucosa is not actuallypigmented (Alawi 2013). The coloration is dueto the visualization of metallic particles embed-ded within the lamina propria and/or submu-cosa. Similarly, graphite tattoos may appearclinically identical to amalgam tattoos(Fig. 37). Graphite tattoos are caused by themucosal implantation of graphite particles typ-ically originating from the tip of a pencil (Alawi2013). These tattoos are usually the result ofaccidental trauma.
Ornamental or intentional oral mucosal tattooshave long been a custom in some parts of theworld, including within specific African tribalcommunities, which has been described previ-ously in this chapter (Gondak et al. 2012). Thetattoo ink is usually plant based and may be com-bined with other carbon-based substances such asburnt wood, plastic, India ink, or even pen ink.Ornamental tattooing is a growing trend in otherparts of the world, including Eastern Europeanand Western countries (Fig. 38).
Fig. 33 Amalgam tattoo appearing clinically as a blackpigmented lesion on the labial gingiva of the tooth 16 (a).Same lesion noted on multislice CT sagittal (b) and axial
(c) views confirming presence of amalgam particles (Photocourtesy: Professor Camile Farah, Perth Oral Medicine &Dental Sleep Centre, Perth, WA, Australia)
26 E.T. Stoopler and F. Alawi

Fig. 36 Amalgam tattoo appearing clinically as blackpigmented lesion in a 65-year-old female presenting onthe buccal mucosa adjacent to a heavily restored molar(Photo courtesy: Professor Camile Farah, Perth Oral Med-icine & Dental Sleep Centre, Perth, WA, Australia)Fig. 34 Amalgam tattoo appearing clinically as black
pigmented lesion on the attached mucosa adjacent toheavily restored molar (Photo courtesy: Professor CamileFarah, Perth Oral Medicine & Dental Sleep Centre, Perth,WA, Australia)
Fig. 37 Biopsy-proven graphite tattoo in a 63-year-oldfemale appearing clinically as a gray pigmented lesion onthe gingiva (Photo courtesy: Professor Camile Farah, PerthOral Medicine & Dental Sleep Centre, Perth, WAAustralia)
Fig. 35 Biopsy-proven amalgam tattoo appearing clini-cally as black pigmented lesion in a 30-year-old female atthe mucogingival junction adjacent to virgin canine andpremolar teeth with braces. Lesion was remnant fromheavily restored primary dentition (Photo courtesy: Profes-sor Camile Farah, Perth Oral Medicine & Dental SleepCentre, Perth, WA, Australia)
Pigmented Lesions of the Oral Mucosa 27
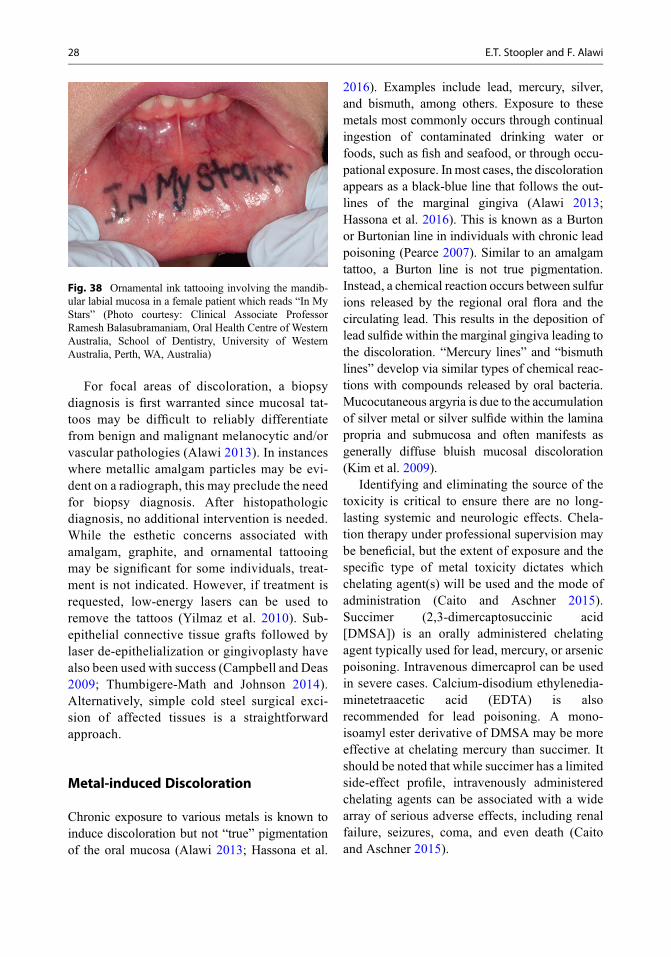
For focal areas of discoloration, a biopsydiagnosis is first warranted since mucosal tat-toos may be difficult to reliably differentiatefrom benign and malignant melanocytic and/orvascular pathologies (Alawi 2013). In instanceswhere metallic amalgam particles may be evi-dent on a radiograph, this may preclude the needfor biopsy diagnosis. After histopathologicdiagnosis, no additional intervention is needed.While the esthetic concerns associated withamalgam, graphite, and ornamental tattooingmay be significant for some individuals, treat-ment is not indicated. However, if treatment isrequested, low-energy lasers can be used toremove the tattoos (Yilmaz et al. 2010). Sub-epithelial connective tissue grafts followed bylaser de-epithelialization or gingivoplasty havealso been used with success (Campbell and Deas2009; Thumbigere-Math and Johnson 2014).Alternatively, simple cold steel surgical exci-sion of affected tissues is a straightforwardapproach.
Metal-induced Discoloration
Chronic exposure to various metals is known toinduce discoloration but not “true” pigmentationof the oral mucosa (Alawi 2013; Hassona et al.
2016). Examples include lead, mercury, silver,and bismuth, among others. Exposure to thesemetals most commonly occurs through continualingestion of contaminated drinking water orfoods, such as fish and seafood, or through occu-pational exposure. In most cases, the discolorationappears as a black-blue line that follows the out-lines of the marginal gingiva (Alawi 2013;Hassona et al. 2016). This is known as a Burtonor Burtonian line in individuals with chronic leadpoisoning (Pearce 2007). Similar to an amalgamtattoo, a Burton line is not true pigmentation.Instead, a chemical reaction occurs between sulfurions released by the regional oral flora and thecirculating lead. This results in the deposition oflead sulfide within the marginal gingiva leading tothe discoloration. “Mercury lines” and “bismuthlines” develop via similar types of chemical reac-tions with compounds released by oral bacteria.Mucocutaneous argyria is due to the accumulationof silver metal or silver sulfide within the laminapropria and submucosa and often manifests asgenerally diffuse bluish mucosal discoloration(Kim et al. 2009).
Identifying and eliminating the source of thetoxicity is critical to ensure there are no long-lasting systemic and neurologic effects. Chela-tion therapy under professional supervision maybe beneficial, but the extent of exposure and thespecific type of metal toxicity dictates whichchelating agent(s) will be used and the mode ofadministration (Caito and Aschner 2015).Succimer (2,3-dimercaptosuccinic acid[DMSA]) is an orally administered chelatingagent typically used for lead, mercury, or arsenicpoisoning. Intravenous dimercaprol can be usedin severe cases. Calcium-disodium ethylenedia-minetetraacetic acid (EDTA) is alsorecommended for lead poisoning. A mono-isoamyl ester derivative of DMSA may be moreeffective at chelating mercury than succimer. Itshould be noted that while succimer has a limitedside-effect profile, intravenously administeredchelating agents can be associated with a widearray of serious adverse effects, including renalfailure, seizures, coma, and even death (Caitoand Aschner 2015).
Fig. 38 Ornamental ink tattooing involving the mandib-ular labial mucosa in a female patient which reads “In MyStars” (Photo courtesy: Clinical Associate ProfessorRamesh Balasubramaniam, Oral Health Centre of WesternAustralia, School of Dentistry, University of WesternAustralia, Perth, WA, Australia)
28 E.T. Stoopler and F. Alawi

Conclusion and Future Directions
Melanin-associated pigmented lesions of the oralmucosa can range from innocuous findings to life-threatening conditions. It is important for oralhealth-care providers to be familiar with therange of clinical phenomena associated withthese types of pigmented lesions that affect boththe oral cavity and cutaneous surfaces. As under-standing of genetics associated with melanogene-sis and human biology are further refined, targetedgene therapy and development of novel immuno-therapeutics will potentially improve detection,treatment, and prognosis of life-threatening mela-nin-associated pigmentation disorders, such asmelanoma.
Cross-References
▶Cutaneous pathology of the Head and NeckRegion
▶Gingival Pathology▶Head and Neck Malignancies▶Oral Lichen Planus▶Oral Manifestations of Systemic Diseases andtheir Treatments
▶Oral Mucosal Malignancies▶ Paediatric Oral Medicine
References
Alawi F. Pigmented lesions of the oral cavity: an update.Dent Clin N Am. 2013;57(4):699–710.
Anderson EJ, Cakir I, Carrington SJ, Cone RD, Ghamari-Langroudi M, Gillyard T, et al. 60 YEARS OF POMC:regulation of feeding and energy homeostasis by alpha-MSH. J Mol Endocrinol. 2016;56(4):T157–74.
Arava-Parastatidis M, Alawi F, Stoopler ET. Multifocalpigmentation of the oral cavity. Oral melanoacanthomaJ Am Dent Assoc. 2011;142(1):53–6.
Bastiaens M, ter Huurne J, Gruis N, Bergman W,Westendorp R, Vermeer BJ, et al. The melanocortin-1-receptor gene is the major freckle gene. Hum MolGenet. 2001;10(16):1701–8.
Berwick M, Buller DB, Cust A, Gallagher R, Lee TK,Meyskens F, et al. Melanoma epidemiology and pre-vention. Cancer Treat Res. 2016;167:17–49.
Bliss JM, Ford D, Swerdlow AJ, Armstrong BK,Cristofolini M, Elwood JM, et al. Risk of cutaneous
melanoma associated with pigmentation characteristicsand freckling: systematic overview of 10 case-controlstudies. Int J Cancer. 1995;62(4):367–72.
Bowen AR, McCalmont TH. The histopathology of sub-cutaneous minocycline pigmentation. J Am AcadDermatol. 2007;57(5):836–9.
Bravo IM, Correnti M, Escalona L, Perrone M, Brito A,Tovar V, et al. Prevalence of oral lesions in HIV patientsrelated to CD4 cell count and viral load in a Venezuelanpopulation. Med Oral Patol Oral Cir Bucal.2006;11(1):E33–9.
Brooks JK, Reynolds MA. Ethnobotanical tattooing of thegingiva: literature review and report of a case. J AmDent Assoc. 2007;138(8):1097–101.
Brown RJ, Kelly MH, Collins MT. Cushing syndrome inthe McCune-Albright syndrome. J Clin EndocrinolMetab. 2010;95(4):1508–15.
Caito S, Aschner M. Neurotoxicity of metals. Handb ClinNeurol. 2015;131:169–89.
Campbell CM, Deas DE. Removal of an amalgam tattoousing a subepithelial connective tissue graft and laserdeepithelialization. J Periodontol. 2009;80(5):860–4.
Cantudo-Sanagustín E, Gutiérrez-Corrales A, Vigo-Martínez M, Serrera-Figallo MÁ, Torres-Lagares D,Gutiérrez-Pérez JL. Pathogenesis and clinicohisto-pathological characteristics of melanoacanthoma:a systematic review. J Clin Exp Dent.2016;8(3):e327–36.
Chandran R, Feller L, Lemmer J, Khammissa RA.HIV-associated oral mucosal melanin hyper-pigmentation: a clinical study in a South African pop-ulation sample. AIDS Res Treat. 2016;2016:8389214.
Charmandari E, Nicolaides NC, Chrousos GP. Adrenalinsufficiency. Lancet. 2014;383(9935):2152–67.
Chatzistefanou I, Kolokythas A, Vahtsevanos K,Antoniades K. Primary mucosal melanoma of the oralcavity: current therapy and future directions. Oral SurgOral Med Oral Pathol Oral Radiol. 2016;122(1):17–27.
De LeoM, Cozzolino A, Colao A, Pivonello R. SubclinicalCushing’s syndrome. Best Pract Res Clin EndocrinolMetab. 2012;26(4):497–505.
Dereure O. Drug-induced skin pigmentation. Epidemiol-ogy, diagnosis and treatment. Am J Clin Dermatol.2001;2(4):253–62.
Felix DH, Luker J, Scully C. Oral medicine: 7. Red andpigmented lesions. Dent Update. 2013;40(3):231–4.236–8.
Feller L, Chandran R, Kramer B, Khammissa RA,Altini M, Lemmer J. Melanocyte biology and functionwith reference to oral melanin hyperpigmentation inHIV-seropositive subjects. AIDS Res Hum Retrovir.2014a;30(9):837–43.
Feller L, Masilana A, Khammissa RA, Altini M, Jadwat Y,Lemmer J. Melanin: the biophysiology of oral melano-cytes and physiological oral pigmentation. Head FaceMed. 2014b;10:8.
Femiano F, Lanza A, Buonaiuto C, Gombos F, Di Spirito F,Cirillo N. Oral malignant melanoma: a review of theliterature. J Oral Pathol Med. 2008;37(7):383–8.
Pigmented Lesions of the Oral Mucosa 29

Fernandes D, Ferrisse TM, Navarro CM, Massucato EM,Onofre MA, Bufalino A. Pigmented lesions on themucosa: a wide range of diagnoses. Oral Surg OralMed Oral Pathol Oral Radiol. 2015;119(4):374–8.
Gaeta GM, Satriano RA, Baroni A. Oral pigmentedlesions. Clin Dermatol. 2002;20(3):286–8.
Gandhi SA, Kampp J. Skin cancer epidemiology, detec-tion, and management. Med Clin NorthAm. 2015;99(6):1323–35.
Gondak RO, da Silva-Jorge R, Jorge J, Lopes MA,Vargas PA. Oral pigmented lesions: clinicopathologicfeatures and review of the literature. Med Oral PatolOral Cir Bucal. 2012;17(6):e919–24.
Hashemi Pour MS. Malignant melanoma of the oral cavity:a review of the literature. Indian J Dent Res.2008;19(1):47–51.
Hassona Y, Sawair F, Al-Karadsheh O, Scully C. Preva-lence and clinical features of pigmented oral lesions. IntJ Dermatol. 2016;55(9):1005–13.
Hatch CL. Pigmented lesions of the oral cavity. Dent ClinN Am. 2005;49(1):185–201. ix–x.
Hruz PW. HIVand endocrine disorders. Endocrinol MetabClin N Am. 2014;43(3):xvii–xviii.
Jiang AJ, Rambhatla PV, Eide MJ. Socioeconomic andlifestyle factors and melanoma: a systematic review.Br J Dermatol. 2015;172(4):885–915.
Kaugars GE, Heise AP, Riley WT, Abbey LM, Svirsky JA.Oral melanotic macules: a review of 353 cases. OralSurg Oral Med Oral Pathol. 1993;76(1):59–61.
Kauzman A, Pavone M, Blanas N, Bradley G. Pigmentedlesions of the oral cavity: review, differential diagnosis,and case presentations. J Can Dent Assoc.2004;70(10):682–3.
Kim Y, Suh HS, Cha HJ, Kim SH, Jeong KS, Kim DH. Acase of generalized argyria after ingestion of colloidalsilver solution. Am J Ind Med. 2009;52(3):246–50.
Lacroix A, Feelders RA, Stratakis CA, Nieman LK.Cushing’s syndrome. Lancet. 2015;386(9996):913–27.
Lau D, Rutledge C, Aghi MK. Cushing’s disease: currentmedical therapies and molecular insights guiding futuretherapies. Neurosurg Focus. 2015;38(2):E11.
Lee CS, Thomas CM, Ng KE. An overview of the chang-ing landscape of treatment for advanced melanoma.Pharmacotherapy. 2017;37(3):319–33.
Lim GF, Cusack CA, Kist JM. Perioral lesions and derma-toses. Dent Clin N Am. 2014;58(2):401–35.
Lloyd C, Grossman A. The AIP (aryl hydrocarbonreceptor-interacting protein) gene and its relation tothe pathogenesis of pituitary adenomas. Endocrine.2014;46(3):387–96.
Lodish MB. Clinical review: kinase inhibitors: adverseeffects related to the endocrine system. J Clin Endo-crinol Metab. 2013;98(4):1333–42.
Lonser RR, Nieman L, Oldfield EH. Cushing’s disease:pathobiology, diagnosis, and management.J Neurosurg. 2016:1–14.
MacLennan R, Kelly JW, Rivers JK, Harrison SL. Theeastern Australian childhood nevus study: site differ-ences in density and size of melanocytic nevi in relation
to latitude and phenotype. J Am Acad Dermatol.2003;48(3):367–75.
Marangon Junior H, Souza PE, Soares RV, de Andrade BA,de Almeida OP, Horta MC. Oral congenitalmelanocytic nevus: a rare case report and review ofthe literature. Head and Neck Pathol. 2015;9(4):481–7.
Meleti M, Vescovi P, Mooi WJ, van der Waal I. Pigmentedlesions of the oral mucosa and perioral tissues: a flow-chart for the diagnosis and some recommendations forthe management. Oral Surg Oral Med Oral Pathol OralRadiol Endod. 2008;105(5):606–16.
Meserve EE, Nucci MR. Peutz-Jeghers syndrome: patho-biology, pathologic manifestations, and suggestions forrecommending genetic testing in pathology reports.Surg Pathol Clin. 2016;9(2):243–68.
Michels A, Michels N. Addison disease: early detectionand treatment principles. Am Fam Physician.2014;89(7):563–8.
Mohan M, Sukhadia VY, Pai D, Bhat S. Oral malignantmelanoma: systematic review of literature and report oftwo cases. Oral Surg Oral Med Oral Pathol Oral Radiol.2013;116(4):e247–54.
Moraes PC, Noce CW, Thomaz LA, Cintra ML,CorreaME. Pigmented lichenoid drug eruption second-ary to chloroquine therapy: an unusual presentation inlower lip. Minerva Stomatol. 2011;60(6):327–32.
Muller S. Melanin-associated pigmented lesions of the oralmucosa: presentation, differential diagnosis, and treat-ment. Dermatol Ther. 2010;23(3):220–9.
Napier C, Pearce SH. Current and emerging therapies forAddison’s disease. Curr Opin Endocrinol DiabetesObes. 2014;21(3):147–53.
Naziat A, GrossmanA. Adrenal Insufficiency. In: De GrootLJ, Chrousos G, Dungan K, et al., editors. Endotext.South Dartmouth (MA): MDText.com, Inc.; 2000-.Available from: https://www.ncbi.nlm.nih.gov/books/NBK279122/
Nikitakis NG, Koumaki D. Laugier-Hunziker syndrome:case report and review of the literature. Oral Surg OralMed Oral Pathol Oral Radiol. 2013;116(1):e52–8.
Pasquali E, Garcia-Borron JC, Fargnoli MC, Gandini S,Maisonneuve P, Bagnardi V, et al. MC1R variantsincreased the risk of sporadic cutaneous melanoma indarker-pigmented Caucasians: a pooled-analysis fromthe M-SKIP project. Int J Cancer. 2015;136(3):618–31.
Pearce JM. Burton’s line in lead poisoning. Eur Neurol.2007;57(2):118–9.
Pinto A, Raghavendra S, Lee R, DeRossi S, Alawi F.Epithelioid blue nevus of the oral mucosa: a rare histo-logic variant. Oral Surg Oral Med Oral Pathol OralRadiol Endod. 2003;96(4):429–36.
Ponti G, Tomasi A,Manfredini M, Pellacani G. Oral muco-sal stigmata in hereditary-cancer syndromes: fromgermline mutations to distinctive clinical phenotypesand tailored therapies. Gene. 2016;582(1):23–32.
Rangwala S, Doherty CB, Katta R. Laugier-Hunziker syn-drome: a case report and review of the literature.Dermatol Online J. 2010;16(12):9.
30 E.T. Stoopler and F. Alawi

Rawal SY, Burrell R, Hamidi CS, Kalmar JR, Tatakis DN.Diffuse pigmentation of maxillary attached gingiva:four cases of the cultural practice of gingival tattoo. JPeriodontol. 2007;78(1):170–6.
Riegert-Johnson D, Gleeson FC, Westra W, Hefferon T,Wong Kee Song LM, Spurck L, et al. Peutz-Jegherssyndrome. In: Riegert-Johnson DL, Boardman LA,Hefferon T, Roberts M, editors. Cancer syndromes.Bethesda: National Center for Biotechnology Informa-tion (US); 2009.
Schernthaner-Reiter MH, Trivellin G, Stratakis CA.MEN1, MEN4, and carney complex: pathology andmolecular genetics. Neuroendocrinology.2016;103(1):18–31.
Sharma ST, Nieman LK, Feelders RA. Cushing’s syn-drome: epidemiology and developments in diseasemanagement. Clin Epidemiol. 2015;7:281–93.
Shen ZY, Liu W, Bao ZX, Zhou ZT, Wang LZ. Oral mel-anotic macule and primary oral malignant melanoma:epidemiology, location involved, and clinical implica-tions. Oral Surg Oral Med Oral Pathol Oral RadiolEndod. 2011;112(1):e21–5.
Shorning BY, Clarke AR. Energy sensing and cancer:LKB1 function and lessons learnt from Peutz-Jegherssyndrome. Semin Cell Dev Biol. 2016;52:21–9.
Tarakji B, Umair A, Prasad D, Alsakran AM. Diagnosis oforal pigmentations and malignant transformations.Singap Dent J. 2014;35C:39–46.
Thumbigere-Math V, Johnson DK. Treatment of amalgamtattoo with a subepithelial connective tissue graft andacellular dermal matrix. J Int Acad Periodontol.2014;16(2):50–4.
Wood BR, Lacy JM, Johnston C, Weigle DS,Dhanireddy S. Adrenal insufficiency as a result ofritonavir and exogenous steroid exposure: report of6 cases and recommendation for management. J IntAssoc Provid AIDS Care. 2015;14(4):300–5.
Yago K, Tanaka Y, Asanami S. Laugier-Hunziker-Baransyndrome. Oral Surg Oral Med Oral Pathol Oral RadiolEndod. 2008;106(2):e20–5.
Yilmaz HG, Bayindir H, Kusakci-Seker B, Tasar S,Kurtulmus-Yilmaz S. Treatment of amalgam tattoowith an Er, Cr:YSGG laser. J Investig Clin Dent.2010;1(1):50–4.
Yuan A, Woo SB. Adverse drug events in the oral cavity.Oral Surg Oral Med Oral Pathol Oral Radiol.2015;119(1):35–47.
Pigmented Lesions of the Oral Mucosa 31