Eric Niederhoffer, Ph.D. SIU-SOM Biochemical basis of acidosis and alkalosis: evaluating acid base...
29
Eric Niederhoffer, Ph.D. SIU-SOM Biochemical basis of acidosis and alkalosis: evaluating acid base disorders
-
Upload
lydia-robertson -
Category
Documents
-
view
225 -
download
1
Transcript of Eric Niederhoffer, Ph.D. SIU-SOM Biochemical basis of acidosis and alkalosis: evaluating acid base...

Eric Niederhoffer, Ph.D.
SIU-SOM
Biochemical basis of acidosis and alkalosis: evaluating acid base disorders

Outline• Approach
historyphysical examinationdifferentialsclinical and laboratory studiescompensation
• Respiratoryacidosisalkalosis
• Metabolicacidosisalkalosis
• Special casespregnancychildren
Approach
• History - subjective information concerning events,
environment, trauma, medications, poisons, toxins• Physical examination - objective information
assessing organ system status and function• Differentials - potential reasons for presentation• Clinical and laboratory studies - degree of changes
from normal• Compensation - assessment of response to initial
problem
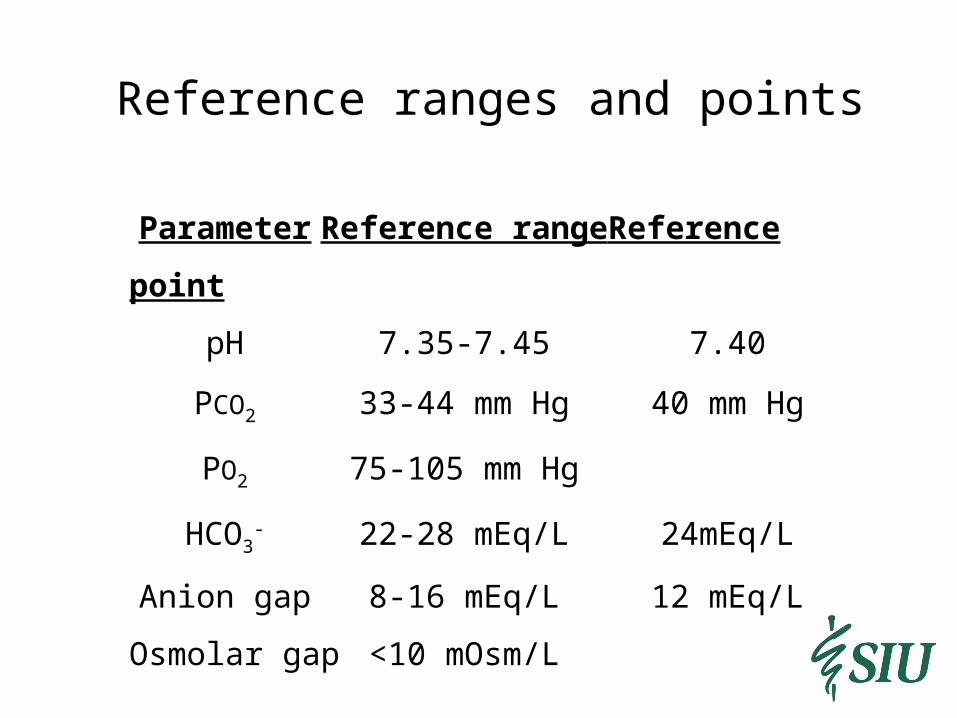
Reference ranges and points
Parameter Reference range Reference point
pH 7.35-7.45 7.40
PCO2 33-44 mm Hg 40 mm Hg
PO2 75-105 mm Hg
HCO3- 22-28 mEq/L 24mEq/L
Anion gap 8-16 mEq/L 12 mEq/L
Osmolar gap <10 mOsm/L
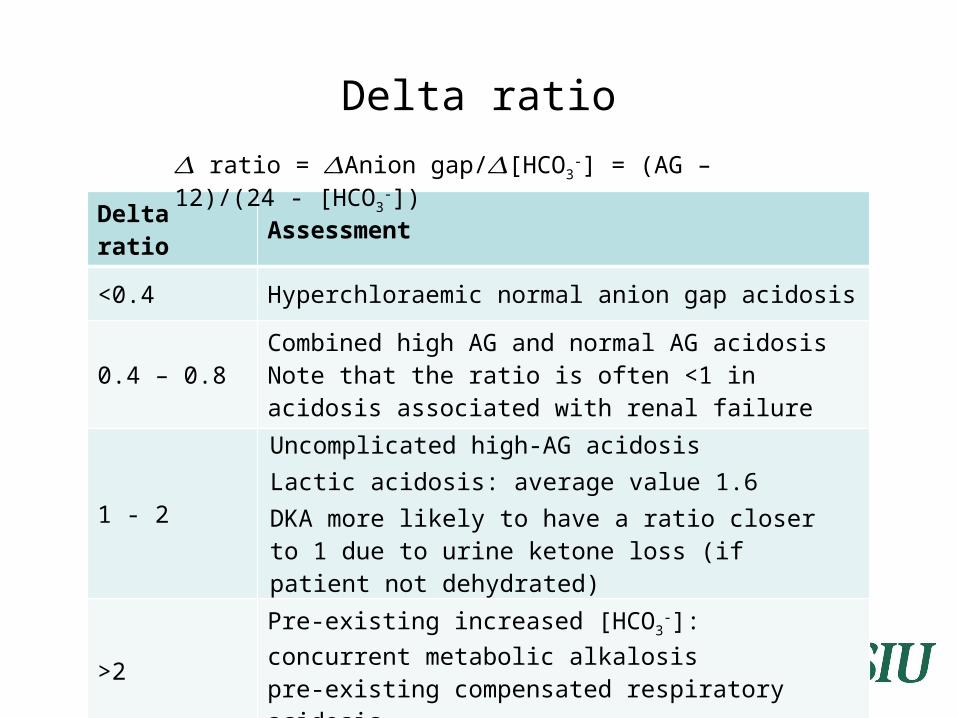
Delta ratio
Delta ratio Assessment
<0.4 Hyperchloraemic normal anion gap acidosis
0.4 – 0.8 Combined high AG and normal AG acidosisNote that the ratio is often <1 in acidosis associated with renal failure
1 - 2
Uncomplicated high-AG acidosisLactic acidosis: average value 1.6 DKA more likely to have a ratio closer to 1 due to urine ketone loss (if patient not dehydrated)
>2 Pre-existing increased [HCO3
-]:concurrent metabolic alkalosispre-existing compensated respiratory acidosis
𝛥 ratio = Anion gap/ [HCO𝛥 𝛥 3-] = (AG – 12)/(24 -
[HCO3-])

CompensationPrimary
DisturbancepH HCO3
- PCO2 Compensation
Respiratory acidosis <7.35 Compensatory increase
Primary increase
Acute: 1-2 mEq/L increase in HCO3
- for every 10 mm Hg increase
in PCO2
Chronic: 3-4 mEq/L increase in HCO3
- for every 10 mm Hg increase
in PCO2
Respiratory alkalosis >7.45 Compensatory decrease
Primary decrease
Acute: 1-2 mEq/L decrease in HCO3
- for every 10 mm Hg decrease in PCO2
Chronic: 4-5 mEq/L decrease in HCO3
- for every 10 mm Hg decrease in PCO2
Metabolic acidosis <7.35 Primary decrease
Compensatory decrease
1.2 mm Hg decrease in PCO2 for every 1 mEq/L decrease in HCO3
-
Metabolic alkalosis >7.45 Primary increase
Compensatory increase
0.6-0.75 mm Hg increase in PCO2 for every 1 mEq/L increase in HCO3
-
, PCO2 should not rise above 55 mm Hg in compensation
Respiratory acidosis
PCO2 greater than expectedAcute or chronicCauses
excess CO2 in inspired air(rebreathing of CO2-containing expired air, addition of CO2 to inspired air, insufflation of CO2 into body cavity)
decreased alveolar ventilation(central respiratory depression & other CNS problems, nerve or muscle disorders, lung or chest wall defects, airway disorders, external factors)
increased production of CO2
(hypercatabolic disorders)
Racid acute
A 65-year-old man with a history of emphysema comes to the physician with a 3-hour history of shortness of breath.
pH 7.18
PO2 61 mm Hg
PCO2 58 mm Hg
HCO3- 26 mEq/L
History suggests hypoventilation, supported by increased PCO2 and lower than anticipated PO2.
Respiratory acidosis (acute) due to no renal compensation.

Description
pH 7.18
PO2 61 mm Hg
PCO2 58 mm Hg
HCO3- 26 mEq/L
1-2 mEq/L increase in HCO3- for every 10 mm Hg increase
in PCO2.
PCO2 increase = 58-40 = 18 mm Hg.
HCO3- increase predicted = (1-2) x (18/10) = 2-4 mEq/L
add to 24 mEq/L (reference point) = 26-28 mEq/L
Racid chronic
A 56-year-old woman with COPD is brought to the physician with a 3-hour history of severe epigastric pain.
pH 7.39
PO2 62 mm Hg
PCO2 52 mm Hg
HCO3- 29 mEq/L
History suggests hypoventilation, supported by increased PCO2.
Respiratory acidosis (chronic) with renal compensation.
Description
pH 7.39
PO2 62 mm Hg
PCO2 52 mm Hg
HCO3- 29 mEq/L
3-4 mEq/L increase in HCO3- for every 10 mm Hg increase
in PCO2.
PCO2 increase = 52-40 = 12 mm Hg.
HCO3- increase predicted = (3-4) x (12/10) = 4-5 mEq/L
add to 24 mEq/L (reference point) = 28-29 mEq/L

Respiratory alkalosis
PCO2 less than expected
Acute or chronic
Causes increased alveolar ventilation
(central causes, direct action via respiratory center; hypoxaemia, act via peripheral chemoreceptors; pulmonary causes, act via intrapulmonary receptors; iatrogenic, act directly on ventilation)
Ralk acute
A 17-year-old woman is brought to the physician with a 3-hour history of epigastric pain and nausea. She admits taking a large dose of aspirin. Her respirations are full and rapid.
pH 7.57
PO2 104 mm Hg
PCO2 25 mm Hg
HCO3- 23 mEq/L
History suggests hyperventilation, supported by decreased PCO2.
Respiratory alkalosis (acute) due to no renal compensation.

DescriptionpH 7.57
PO2 104 mm Hg
PCO2 25 mm Hg
HCO3- 23 mEq/L
1-2 mEq/L decrease in HCO3- for every 10 mm Hg decrease
in PCO2.
PCO2 decrease = 40-25 = 15 mm Hg.
HCO3- decrease predicted = (1-2) x (15/10) = 2-3 mEq/L
subtract from 24 mEq/L (reference point) = 21-22 mEq/L
Ralk chronic
A 81-year-old woman with a history of anxiety is brought to the physician with a 2-hour history of shortness of breath. She has been living at 9,000 ft elevation for the past 1 month. Her respirations are full at 20/min.
pH 7.44
PO2 69 mm Hg
PCO2 24 mm Hg
HCO3- 16 mEq/L
History suggests hyperventilation, supported by decreased PCO2.
Respiratory alkalosis (chronic) with renal compensation.
DescriptionpH 7.44
PO2 69 mm Hg
PCO2 24 mm Hg
HCO3- 16 mEq/L
4-5 mEq/L decrease in HCO3- for every 10 mm Hg decrease
in PCO2.
PCO2 decrease = 40-24 = 16 mm Hg.
HCO3- decrease predicted = (4-5) x (16/10) = 6-8 mEq/L
subtract from 24 mEq/L (reference point) = 16-18 mEq/L

Metabolic acidosis
Plasma HCO3- less than expected
Gain of strong acid or loss of base
Alternatively, high anion gap or normal anion gap metabolic acidosis
Causes high anion-gap acidosis (normochloremic)
(ketoacidosis, lactic acidosis, renal failure, toxins) normal anion-gap acidosis (hyperchloremic)
(renal, gastrointestinal tract, other)
Macid high AGA 20-year-old man with a history of diabetes is brought to the emergency department with a 3-day history of feeling ill. He is non-adherent with his insulin. Urine ketones are 2+ and glucose is 4+.
pH 7.26 Na+ 136 mEq/LPO2 110 mm Hg K+ 4.8 mEq/LPCO2 19 mm Hg Cl- 101 mEq/LHCO3
- 8 mEq/L CO2, total 10 mEq/LGlucose 343 mg/dL Urea 49 mg/dL
Creatinine 1 mg/dLHistory suggests diabetic ketoacidosis.Metabolic acidosis with appropriate respiratory compensation.
DescriptionpH 7.26 Na+ 136 mEq/LPO2 110 mm Hg K+ 4.8 mEq/LPCO2 19 mm Hg Cl- 101 mEq/LHCO3
- 8 mEq/L Glucose 343 mg/dLUrea 49 mg/dL
AG = 136-101-8=27 mEq/L Creatinine 1 mg/dL
1.2 mm Hg decrease in PCO2 for every 1 mEq/L decrease in HCO3
-.
HCO3- decrease = 24-8 = 16 mEq/L
PCO2 decrease predicted = 1.2 x 16 = 19 mm Hg.
subtract from 40 mm Hg (reference point) = 21 mm Hg

Macid normal AG
A 43-year-old man comes to the physician with a 3-day history of diarrhea. He has decreased skin turgor.
pH 7.31 Na+ 134 mEq/LPO2 -- mm Hg K+ 2.9 mEq/LPCO2 31 mm Hg Cl- 113 mEq/LHCO3
- 16 mEq/L Urea 74 mgl/dLCreatinine 3.4 mmol/L
History is limited.
Metabolic acidosis with respiratory compensation.
DescriptionpH 7.31 Na+ 134 mEq/LPO2 -- mm Hg K+ 2.9 mEq/LPCO2 31 mm Hg Cl- 113 mEq/LHCO3
- 16 mEq/L Urea 74 mg/dLCreatinine 3.4 mg/dL
AG = 134-113-16=5 mEq/L
1.2 mm Hg decrease in PCO2 for every 1 mEq/L decrease in HCO3
-.
HCO3- decrease = 24-16 = 8 mEq/L
PCO2 decrease predicted = 1.2 x 8 = 10 mm Hg.
subtract from 40 mm Hg (reference point) = 30 mm Hg
Metabolic alkalosis
Plasma HCO3- greater than expected
Loss of strong acid or gain of base
Causes (2 ways to organize) loss of H+ from ECF via kidneys (diuretics) or gut (vomiting) gain of alkali in ECF from exogenous source (IV NaHCO3
infusion) or endogenous source (metabolism of ketoanions)or addition of base to ECF (milk-alkali syndrome) Cl- depletion (loss of acid gastric juice) K+ depletion (primary/secondary hyperaldosteronism) Other disorders (laxative abuse, severe hypoalbuminaemia)
Urinary Chloride
Spot urine Cl- less than 10 mEq/L often associated with volume depletion respond to saline infusion common causes - previous thiazide diuretic therapy,
vomiting (90% of cases)
Spot urine Cl- greater than 20 mEq/L often associated with volume expansion and hypokalemia resistant to therapy with saline infusion causes: excess aldosterone, severe K+ deficiency, current
diuretic therapy, Bartter syndrome

Malk high Urine Cl-
An 83-year-old woman is brought to the physician with a 1-week history of weakness and poor appetite.
pH 7.58 Na+ 145 mEq/LPO2 60 mm Hg K+ 1.9 mEq/LPCO2 56 mm Hg Cl- 86 mEq/LHCO3
- 52 mEq/L Urine Cl- 74 mEq/L
History is limited.
Metabolic alkalosis with respiratory compensation.
The cause is unknown, most likely excess adrenocortical activity, current diuretic therapy, or idiopathic.

DescriptionpH 7.58 Na+ 145 mEq/LPO2 60 mm Hg K+ 1.9 mEq/LPCO2 56 mm Hg Cl- 86 mEq/LHCO3
- 52 mEq/L Urine Cl- 74 mEq/L
0.6-0.75 mm Hg increase in PCO2 for every 1 mEq/L increase in HCO3
-.
HCO3- increase = 52-24 = 28 mEq/L
PCO2 increase predicted = 0.6-0.75 x 28 = 17-21 mm Hg.
add to 40 mm Hg (reference point) = 57-61 mm Hg

Malk low Urine Cl-
An 24-year-old woman is brought to the physician with a 3-month history of weakness and fatigue. Blood pressure is 90/60 mm Hg.
pH 7.52 Na+ 137 mEq/LPO2 78 mm Hg K+ 2.6 mEq/LPCO2 49 mm Hg Cl- 90 mEq/LHCO3
- 39 mEq/L Urine Cl- 5 mEq/L
History and physical examination suggests bulimia.
Metabolic alkalosis with respiratory compensation.
The cause is most likely bulimia.
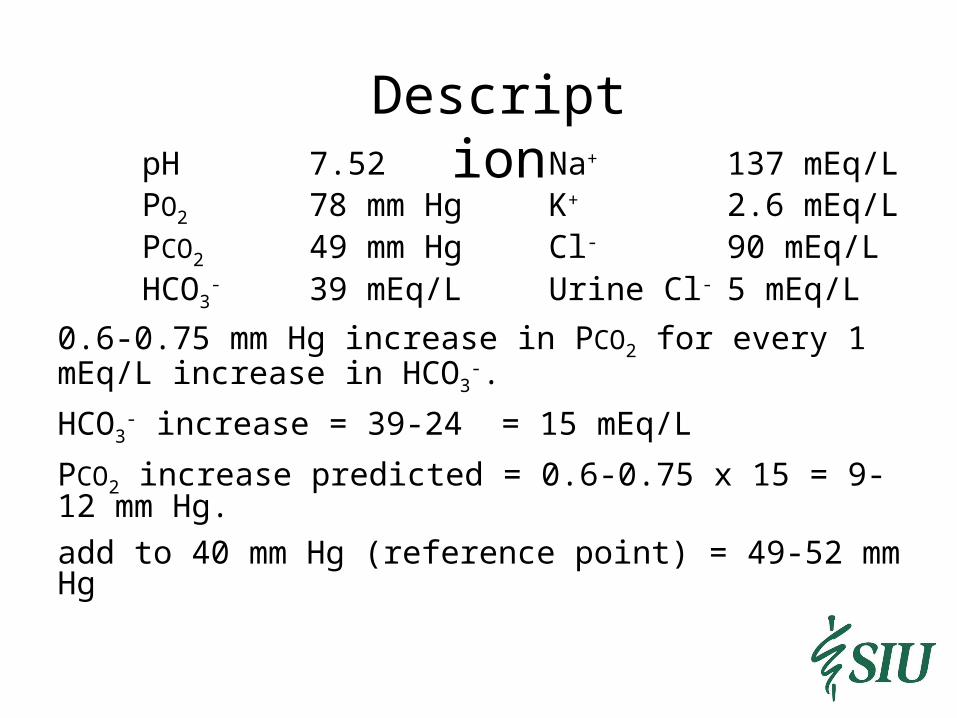
DescriptionpH 7.52 Na+ 137 mEq/LPO2 78 mm Hg K+ 2.6 mEq/LPCO2 49 mm Hg Cl- 90 mEq/LHCO3
- 39 mEq/L Urine Cl- 5 mEq/L
0.6-0.75 mm Hg increase in PCO2 for every 1 mEq/L increase in HCO3
-.
HCO3- increase = 39-24 = 15 mEq/L
PCO2 increase predicted = 0.6-0.75 x 15 = 9-12 mm Hg.
add to 40 mm Hg (reference point) = 49-52 mm Hg
Special Cases
• Pregnancy – hyperventilation (respiratory alkalosis),
hyperemesis (metabolic alkalosis or acidosis), maternal
ketosis (metabolic acidosis)• Children – low bicarbonate reserve (N=12-16 mEq/L),
low acid excretion reserve, inborn errors in metabolism,
diabetes, and poisoning (all metabolic acidosis)
Review Questions
• What is an effective approach to acid base problems?
• What are the normal ranges and reference points?
• What are the anion and osmolar gap?
• What is compensation?
• What are the characteristics of respiratory acidosis and
alkalosis?
• What are the characteristics of metabolic acidosis and
alkalosis?
• What is the utility of spot urine Cl-?
• What kinds of acid base conditions present during pregnancy
and infancy?