Equine Diagnostic Radiography & Ultrasonography Radiography Distal Limb T… · • Echogenicity...
10
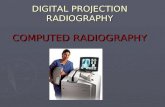
1 Equine Diagnostic Radiography & Ultrasonography Dr. Russell Tucker DACVR Prof Emeritus, WSU 90 ~30 DLPMO ~ projects medial forward lateral backward ~30 PL to DM projection
Transcript of Equine Diagnostic Radiography & Ultrasonography Radiography Distal Limb T… · • Echogenicity...

1
Equine Diagnostic
Radiography & UltrasonographyDr. Russell Tucker DACVR
Prof Emeritus, WSU
90
~30
DLPMO ~ projects
medial forward
lateral backward
~30PL to DM projection

2
DMPLO (PL-DMO)
~ projects
lateral forward
medial backward
EQUINE DISTAL LIMB
TENDONS & LIGAMENTS
Anatomic Abbreviations:
SDF = Superficial Digital Flexor
DDF = Deep Digital Flexor
ICL = Inferior Check Ligament
SL = Suspensory Ligament
AL = Annular Ligament
DAL = Digital Annular Ligament
DDAL = Distal Digital Annular Ligament
SDSL = Straight Distal Sesamoidean Ligament
ODSL = Oblique Distal Sesamoidean Ligament
PL = Plantar Ligament
CL = Collateral Ligament
1. Longitudinal
Scanning Planes
2. Transverse
3. Oblique
2
1
3
Sedated & Placed in Stocks
Clip & Shave Both Legs
or
Clean & Wet Hair (diluted 30% alcohol)
Scan in Direction of Hair
Preparation Standoff Pads
or
Offsets
“sonolucent”
material for
scanning irregular
surfaces
&
superficial structures

3
Extended FOV
proximal distal
5 cm
Elasticity Imaging DDF lesion
Metacarpus
Proximal MCIII longitudinal
4 cm “footprint” 12 MHz linear probe, using ACC bone as reference
- with 5 focal zones activated & uniform gain across FOV
Metacarpus
Mid-Distal MCIII longitudinal
Metacarpus
Distal MCIII & Inter-Sesamoid longitudinal
Suspensory Branch Insertion
transverse longitudinal
Insertion onto abaxial fossa of proximal sesamoid bone

4
Suspensory Branch
Insertion
longitudinal
transverse
TRANSVERSE IMAGES
• Orthogonal to Longitudinal Images
• Zones 1a, 1b --- 3a, 3b on front limbs
• Zones 1a, 1b --- 4a, 4b on rear limbs
• Use cm distal to LANDMARKS
• Distal Accessory Carpal Bone (DACB)
• Tuber Calcaneous Bone or MT4 head
MCIII 4 cm distal to accessory carpal boneTransverse
41A
A
4 cm “footprint” 12 MHz linear probe, using ACC bone as reference
- with 5 focal zones activated & uniform gain across FOV
MCIII 8 cm distal to accessory carpal boneTransverse
MCIII 12 cm distal to accessory carpal bone
Transverse
MCIII 16 cm distal to accessory carpal bone
Transverse

5
MCIII 20 cm distal to accessory carpal bone
Transverse
MCIII 24 cm distal to accessory carpal bone
Transverse
Suspensory branched
~proximal pouch of fetlock joint
MCIII 24 cm distal to accessory carpal bone
Transverse
Suspensory Branch Insertion
may require stand off pad
1 cm
MCIII 24 cm distal to accessory carpal bone
Transverse
Proximal sesamoids axial surfaces
MCIII 24 cm distal to accessory carpal bone
Transverse
Palmar Annular Ligament Thickness
~ requires dynamic imaging to visualize
REAR LIMBS
• Orthogonal to Longitudinal Images
• Zones 1a, 1b --- 3a, 3b on front limbs
• Zones 1a, 1b --- 4a, 4b on rear limbs
• Use cm distal to LANDMARKS
• Distal to 4th Metatarsal Head (MT4)
• Distal to point of Tuber Calcaneus

6
Distal Tarsus -Transverse
DDF exiting tarsal canal
MTIII 4 cm distal to Tarsus
Transverse
* need to image slightly medially for entire DDF
MTIII 8 cm distal to Tarsus
Transverse
MTIII 12 cm distal to Tarsus
Transverse
MTIII 24 cm distal to Tarsus
Transverse
Identical to front legs
~may require stand off pad for PaAL
Tendon & Ligament Pathology
• Compare Sides RT vs LT
• Sequential Scanning Protocol
• Record in at least 2 anatomic planes
– Sagittal (longitudinal)
– Transverse (axial)
– Oblique Planes may be required
*Carefully document & describe lesions

7
Tendon & Ligament Scanning
• Clip or Not ?
• Shave or Not ?
• Fiber pattern important
• Try 30% diluted alcohol
• Image 2 orthogonal planes
– Sagittal (longitudinal)
– Transverse (axial)
– Oblique scan planes
Compare legs
RH norm prox suspensory
LH abnormal proximal suspensory
Compare size & echogenicity & fiber patterns
LF vs RF
ICL size
Compare to other limb
or medial vs lateral
LH medial Susp
LH lateral Susp
Loss of fiber pattern
• Cross-sectional area
• Region of involvement
• Length of lesion
• Echogenicity
• Focal or diffuse
• Fiber pattern
• Change over time
25 mm2
Lesion Characterization & Descriptions
DDF
Cross Sectional Area of Lesions
• Trace the tendon
1 = total tendon
• Trace the lesion
2 = lesion
• Calculate X-sec %
ROI 1 / ROI 2 = 38 %

8
5 yr THB gelding RF lame
~ swelling above fetlock
R
R
R
DMPLO
projects medial
sesamoid caudally
5 yr THB gelding RF lame
~ swelling above fetlock
RF Suspensory med branch
- 5.28 cm outline/ 1.92 cm2
- hypoechoic & fiber loss
RF Suspensory lat branch (norm)
- 4.54 cm outline/1.47 cm2
- uniform fiber pattern
Lat Branch
Med Branch
Echogenicity of Lesions
• Hypoechogenicity
– Acute & Healing Phases
• Hyperechogenicity
– Healing & Chronic Phases
• Calculate Abnormal %
– % change over time
Fiber Integrity of Lesions1. Fiber Loss & Disruption
– Acute & Healing Phases
2. Fiber Replacement
– Healing & Chronic Phases
3. Fiber Restructuring
– % change over time
• Type I replaces Type III collagen
• Longitudinal orientation
• May require 6-12 months to occur
• Forever decreased strength
Focal vs Diffuse
Common digital extensor tendon over medial carpusDLPMO
Focal vs Diffuse lesions

9
Core Lesions
~ contained w/in interior
Peripheral Lesions
~ extend to edgeLesion: Proximal to Distal
10-22 cm DACB
SDF Tear
10cm
12cm
15cm
22cm
SDF
DDF
Acute Inflammatory Stage
~ edema & hemorrhage (hypoechoic)
Initial scan DDF
90 days lay off
Healing 3-6 months
Type I replaces Type III collagen
~ restores fiber orientation
PROGRESSIVE
REHABILITATION
Month 0-2
Stall rest & hand walk
30 min/d Mon 1, 45 min/d Mon 2
Month 2-3
Stall rest & hand walk
25-45 min/d, jog 5 min/d
Month 4-6
Stall rest & hand walk
20-45 min/d, jog 10 min/d
Peri-tendinal effusions
• Amount
• Cellularity
• Fibrin
• Adhesions
• Tendon sheath
• Synovium

10
Fluid & Effusion
Composition10 yr gelding THB - chronic RF fetlock swelling & lameness
R
R R
Lat RF collateral transverse
Dynamic Imaging for Adhesions
• Critical for follow-up exams
• Exact location of lesion
• Size & characteristics
• Compare to other limb
Accurate & Detailed
Lesion DescriptionsQuestions???