Eptifibatid u ACS

of 6
-
Upload
sofija-vukadinovic -
Category
Documents
-
view
216 -
download
0
Transcript of Eptifibatid u ACS
-
8/13/2019 Eptifibatid u ACS
1/6
Administration of Eptifibatideto Acute Coronary Syndrome PatientsReceiving Enoxaparin or Unfractionated HeparinEffect on Platelet Function and Thrombus FormationEli I. Lev, MD,* David Hasdai, MD,* Erez Scapa, MD, Ana Tobar, MD, Abid Assali, MD,*
Judith Lahav, PHD, Alexander Battler, MD,* Juan J. Badimon, PHD,Ran Kornowski, MD*
Tel Aviv, Israel; and New York, New York
OBJECTIVES The goal of this study was to compare the antithrombotic effects of enoxaparin versusunfractionated heparin (UFH) when combined with eptifibatide in acute coronary syndrome(ACS) patients.
BACKGROUND An increasing number of high-risk ACS patients are treated with low-molecular-weightheparin and a glycoprotein (GP) IIb/IIIa inhibitor. There is a paucity of data regarding theantithrombotic properties of such a combination as compared with UFH and GP IIb/IIIainhibitors.
METHODS Twenty-six ACS patients scheduled to undergo coronary angiography were treated withsubcutaneous enoxaparin (n 13) or intravenous UFH (n 13). All patients received
eptifibatide just before coronary angiography. Antithrombotic effects were assessed as changesin platelet-thrombus formation using the Badimon ex vivo perfusion chamber. Perfusions
were carried out at a high shear rate (HSR) and a low shear rate (LSR). Patients underwenttwo perfusion studies: at baseline (under enoxaparin or UFH) and 10 min after theeptifibatide bolus. Platelet function was evaluated by ADP-induced platelet aggregation andthe rapid platelet function analyzer.
RESULTS Both therapeutic combinations achieved a marked reduction in platelet aggregation aftereptifibatide (83% to 89.7% reduction in the enoxaparin-eptifibatide group and 77.8% to85.5% reduction in the UFH-eptifibatide group, inter-group differences not significant). Bothgroups also demonstrated marked reductions in thrombus formation, but the reductionsachieved in the enoxaparin-eptifibatide group were significantly higher than those achieved inthe UFH-eptifibatide group (HSR: 75.6% reduction vs. 63.9%, respectively, p 0.01; LSR:79.7% reduction vs. 66.1%, respectively, p 0.0001).
CONCLUSIONS The combination of eptifibatide with enoxaparin appears to have a more potent antithrom-
botic effect than that of eptifibatide and UFH in the doses tested. (J Am Coll Cardiol 2004;43:96671) 2004 by the American College of Cardiology Foundation
Antithrombotic treatment with aspirin and heparin eitherunfracionated (UFH) or low-molecular-weight heparin(LMWH)represents the current standard of care forpatients hospitalized with an acute coronary syndrome(ACS) without ST-elevation(1,2).Low-molecular-weightheparin has several advantages over UFH: it has a morepredictable anticoagulant effect with a higher ratio ofanti-factor Xa to anti-factor IIa activity (3), requires nomonitoring of anticoagulation, is resistant to inhibition by
activated platelets(4),and has a lower incidence of heparin-induced thrombocytopenia (5). In addition, the LMWHenoxaparin has been shown to have a significant clinicaladvantage over UFH in reducing the composite end point of
death, myocardial infarction (MI), or need for urgentrevascularization in ACS patients(6,7).
The development of platelet glycoprotein (GP) IIb/IIIainhibitors has extended the therapeutic options for anti-thrombotic and anti-platelet treatment in the ACS andpercutaneous coronary intervention (PCI) setting. Glyco-protein IIb/IIIa inhibitors given to ACS patients and/orpatients undergoing PCI have been shown to significantlyreduce the rate of ischemic complications (811). There-fore, an increasing number of high-risk ACS patients aretreated with enoxaparin and a GP IIb/IIIa inhibitor, such aseptifibatide.
Recently, the concept of combining LMWH with GPIIb/IIIa inhibitor therapy has gained support(1217).Thesafety of this combination therapy has been demonstratedwhen using abciximab or eptifibatide and intravenous enox-aparin during PCI(1214)and the combination of tirofibanor eptifibatide given with subcutaneous enoxaparin to ACSpatients(1517).Recent data also suggest that the combi-nation of a GP IIb/IIIa inhibitor with enoxaparin has better
clinical efficacy than the combination with UFH. In theAntithrombotic Combination Using Tirofiban and Enox-
From the *Cardiology Department, Rabin Medical Center, Israel (affiliated withthe Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel); Departmentof Medicine H, Rabin Medical Center, Israel (affiliated with the Sackler School ofMedicine, Tel Aviv University, Tel Aviv, Israel); Pathology Department, RabinMedical Center, Israel (affiliated with the Sackler School of Medicine, Tel AvivUniversity, Tel Aviv, Israel); Coagulation Laboratory, Rabin Medical Center, Israel(affiliated with the Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel);and the Cardiovascular Biology Research Laboratory, the Cardiovascular Institute,Mount Sinai Medical Center, New York, New York. Supported, in part, by Aventis
Pharma Ltd. Israel, and by Schering-Plough Israel.Manuscript received August 19, 2003; accepted September 16, 2003.
Journal of the American College of Cardiology Vol. 43, No. 6, 2004 2004 by the American College of Cardiology Foundation ISSN 0735-1097/04/$30.00Published by Elsevier Inc. doi:10.1016/j.jacc.2003.09.060
-
8/13/2019 Eptifibatid u ACS
2/6
aparin (ACUTE) II trial, therapy with tirofiban and enox-aparin was associated with a reduction in refractory ischemiarequiring urgent revascularization, as compared with UFHand tirofiban (16). Similar results were obtained in the
Integrilin and Enoxaparin Randomized Assessment ofAcute Coronary Syndrome Treatment (INTERACT) trial,in which treatment of ACS patients with eptifibatide andenoxaparin was associated with decreased ischemia as de-tected by continuous electrocardiographic monitoring(17).Despite the emerging clinical evidence, there is a paucity ofdata comparing the antithrombotic properties of the twocombination treatments, apart from a trend toward reducedinhibition of platelet aggregation when GP IIb/IIIa inhibitorsare administered with UFH(15,18,19).The aim of the currentstudy, therefore, was to compare the antithrombotic effects ofenoxaparin versus UFH when combined with eptifibatide in
ACS patients intended for coronary angiography.
METHODS
Patients. Twenty-six ACS patients scheduled to undergocoronary angiography within 24 to 48 h of enrollment wereincluded in the study. Acute coronary syndrome was definedas unstable angina or nonST-segment elevation MI, withsymptoms presenting in the 24 h before admission. Exclu-sion criteria were ST-segment elevation acute MI; history ofhemorrhagic diathesis; any major surgery; gastrointestinal orgenitourinary bleeding within six weeks; history of stroke
within two years or a residual neurological deficit; concur-rent administration of oral anticoagulants unless the pro-thrombin time was 1.2 times control; thrombocytopenia(100,000 cells/l); hemoglobin level 14 g/dl; severeuncontrolled hypertension (180/110); known hypersensi-tivity to any component of eptifibatide, enoxaparin, orUFH; renal failure (creatinine level 2.5 mg/dl); or prioruse of a GP IIb/IIIa inhibitor within the previous month.The study was approved by the Institutional Review Boardof the Rabin Medical Center, and informed consent wasobtained from each patient.Study medications. The study was comprised of two groups
of consecutively enrolled patients. Group 1 (n 13), whichwas enrolledfirst, received the combination of enoxaparin and
eptifibatide, and group 2 (n 13) received the combination ofUFH and eptifibatide. In group 1, the patients receivedenoxaparin at a 1 mg/kg dose, administered subcutaneouslyevery 12 h. After at least two enoxaparin injections, and 3 to5 h after the last injection, the patients were taken to thecatheterization laboratory. Just before the angiography, after
obtaining arterial access, eptifibatide was administered as anintravenous bolus of 180 g/kg, followed by 2.0 g/kg/mininfusion over 18 to 24 h. In group 2, the patients received UFHas a bolus of 70 U/kg intravenously and an infusion of 15 U/kg,adjusted every 8 h to achieve 1.5 to 2.5 times the controlactivated partial thromboplastin time (aPTT) value(1),whichis 30 s at the Rabin Medical Center laboratory. Unfractionatedheparin was continued during the patients arrival at thecatheterization laboratory, arterial access gain, and perfor-mance of the second perfusion chamber, as detailed below. Itwas discontinued after the perfusion chamber. Before theangiography, after obtaining the arterial access, eptifibatide was
administered in an identical manner to group 1. In the patientswho underwent PCI in group 2, additional UFH boluses weregiven as necessary during PCI (after the perfusion chamber) tomaintain an activated clotting time (ACT) of 225 to 275 s.
Concomitant medical therapy included oral aspirin 200 mgdaily from admission time, given to all patients. In addition,patients who underwent intracoronary stent deployment re-ceived clopidogrel at a dose of 75 mg daily for four weeks afterPCI.Ex vivo perfusion chamber. All patients underwent twoperfusion chamber studies. This design allows each patient toserve as his own control. Immediately before each perfusion
study, blood was also collected for coagulation and plateletfunction tests. In group 1, the first perfusion chamber wasperformed 3 to 5 h after an enoxaparin injection, whenmaximum anti-Factor Xa and anti-Factor IIa activities occur(4).The second chamber was also performed 3 to 5 h after anenoxaparin injection, and 10 min after the eptifibatide bolus,just before performing the angiography. In group 2, thefirstperfusion chamber was performed at least 1 h after the UFHbolus and beginning of infusion. The second chamber wasperformed, similar to group 1, 10 min after the eptifibatidebolus,when the patient was still receiving UFHand just beforeperforming the angiography.
Antithrombotic effects were assessed as changes in thesurface of the platelet thrombus formed on the Badimonperfusion chamber. The perfusion chamber used in thisstudy has been extensively described elsewhere(20 22). Inbrief, it consists of a cylindrical flow channel (1- or 2-mmdiameter, 2-cm length) that allows the flowing of blood,pumped directly from the patient, over an exposed throm-bogenic surface. Perfusions were performed at rheologicconditions of low (212/s) and high (1,690/s) shear rate.These local flow conditions mimic mild to moderatelystenotic coronary arteries, respectively. Our previous workdemonstrated that these rheologic conditions resulted in
consistent levels of platelet deposition and thrombus forma-tion(22,23).
Abbreviations and Acronyms
ACS acute coronary syndromeACT activated clotting timeaPTT activated partial thromboplastin timeGP glycoproteinHSR high shear rate
LMWH low-molecular-weight heparinLSR low shear rateMI myocardial infarctionPCI percutaneous coronary interventionRPFA rapid platelet function analyzer
TAT thrombin antithrombin complexUFH unfractionated heparin
967JACC Vol. 43, No. 6, 2004 Lev et al.
March 17, 2004:96671 Eptifibatide Combined With Enoxaparin or Heparin
-
8/13/2019 Eptifibatid u ACS
3/6
Thrombogenic substrates and perfusion studies. To trig-ger thrombus formation, porcine aortic tunica media was usedas substrate. The substrates (25 10-mm sections) weresurgically prepared to simulate the degree of severe arterialinjury induced by PCI, as previously described(20,21).Duringeach perfusion study, venous blood was circulated from the
patient directly through three flow chambers connected inseriesone at low shear rate (LSR) and two at high shear rate(HSR). The perfusion chamber system was connected withpolyethylene tubing to the patients intravenous access anddistally to a peristaltic pump (Masterflex model 7013, Cole-Palmer Inc., Vernon Hills, Illinois) calibrated to maintain theselected bloodflow. Perfusion time was 5 min in both studies.All the perfusion studies were performed at 37C by placingthe chambers in a water bath.Evaluation of thrombus formation. After perfusion, spec-imens were removed from the chamber and immediatelyfixed in 4% phosphate-buffered para-formaldehyde. Speci-
mens were then transversely cut into 2- to 4-mm thickpieces and paraffin embedded. Histologic sections (5 m)from each specimen were prepared and stained with twotypes of stain: combined Massons trichrome-elastin, whichstains total thrombus, and a murine monoclonal anti-humanB15 42 antibody, which reacts withfibrin polymer.
Morphometric analyses were conducted at 10-fold mag-nification. Thrombus area was measured on each section bycomputerized planimetry using Image-Pro Plus software(Media Cybernetics, Silver Spring, Maryland). The resultsof six sections were averaged to determine the total throm-bus andfibrin area for each chamber.
Platelet function assessment and coagulation tests.Before each of the perfusion studies, blood was collected invacutainers containing D-Phe-Pro-Arg chloromethyl ke-tone dihydrochloride (PPACK). The samples were evalu-ated for platelet function, as well as coagulation profile(aPTT), complete blood count, anti-factor Xa activity,thrombin antithrombin complex (TAT), and prothrombinfragment 1 2 (F1.2). Anti-factor Xa activity was quanti-fied by the Coamatic Heparin kit (Chromogenix Instru-mentation, Milano, Italy). Thrombin antithrombin complexand F1.2 levels were measured by enzyme immunoassay kits(Enzygnost-Dade Behring, Liederbach, Germany). Platelet
function was assessed by in vitro platelet aggregation andthe rapid platelet function analyzer (RPFA) (AccumetricsInc., San Diego, California). Platelet aggregation was per-formed in platelet-rich plasma in response to 10 and 20 Madenosine 5-diphosphate (ADP), as previously described(24).The extent of aggregation was defined as the maximalamount of light transmission reached within 6 min after theagonist addition. The RPFA is a point-of-care system thatquantitatively measures the ability of platelets to agglutinatefibrinogen-coated beads (25). Results were expressed asplatelet activation units and percentage of baseline.Statistical analysis. Patient demographics, platelet func-
tion data, and coagulation tests are described using mean
SD. Thrombus area is described using mean standard
error of mean (SEM). Intra-group comparisons were per-formed using paired two-tailed Student ttests. Inter-groupcomparisons were performed using unpaired ttests and theMann-Whitney non-parametric tests. Categorical variableswere compared with the chi-square test. Analyses wereperformed using SPSS version 10 statistical software (SPSSInc., Chicago, Illinois), and statistical significance wasconsidered as p 0.05.
RESULTS
The characteristics of the patient populations are outlined inTable 1.There were no significant differences in any of theclinical parameters between the two groups. Table 2presentsthe complete blood count parameters and coagulation tests.Intra-group differences between the baseline and post-eptifibatide samples were observed only in the hemoglobinlevel of group 1 (a decrease from 14.5 2.1 to 13.9 2.0
gm/dl, p
0.01, both within normal range). Inter-groupdifferences were observed in the aPTT and anti-Xa levels. Asexpected, group 2 (treated by UFH) had significantly higheraPTT levels (28.2 4.4 s and 29.8 4.6 s in group 1 vs. 58.9 21.5 s and 52.4 10.4 s in group 2, p 0.001), whereasgroup 1 (treated by enoxaparin) exhibited higher levels ofanti-Xa activity (0.85 0.2 and 0.84 0.2 IU/ml in group 1vs. 0.57 0.1 and 0.55 0.1 IU/ml in group 2, p 0.001).In group 2, at the second time point (on arrival at thecatheterization laboratory and post-eptifibatide), all patientswere within the recommended aPTT range (at least 45 s),except for one patient who had an aPTT level of 42.2 s.
Activated clotting time values at the second time point were128.2 6.2 s in group 1 and 179.7 21.8 s in group 2 (p 0.001).
The results of platelet function tests are outlined inTable3. In both groups, marked reductions in platelet functionwere achieved after eptifibatide (p 0.0001 for baseline vs.post-eptifibatide in all tests). Differences between thegroups in the extent of platelet function reduction were notsignificant.
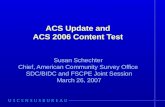
Total thrombus formation is presented inFigure 1.Theadministration of eptifibatide significantly reduced throm-bus formation in both groups. The antithrombotic effect
was observed at both high and low shear rates (p
0.0001for both groups at both shear rates). However, the reduc-
Table 1. Clinical Characteristics
Group 1(n 13)
Group 2(n 13)
Age (yrs) 60.2 11.2 59.4 13.1Males, n (%) 11 (84.6%) 12 (92.3%)Diabetes, n (%) 5 (38.5%) 4 (30.8%)Hyperlipidemia, n (%) 9 (69.2%) 8 (61.5%)Hypertension, n (%) 9 (69.2%) 7 (53.8%)Current smoking, n (%) 4 (30.8%) 3 (23.1%)Unstable angina, n (%) 4 (30.8%) 2 (15.4%)NonST-elevation MI, n (%) 9 (69.2%) 11 (84.6%)Previous MI, n (%) 3 (23.1%) 4 (30.8%)
MI myocardial infarction.
968 Lev et al. JACC Vol. 43, No. 6, 2004Eptifibatide Combined With Enoxaparin or Heparin March 17, 2004:96671
-
8/13/2019 Eptifibatid u ACS
4/6
tions achieved in group 1 were significantly higher thanthose achieved in group 2 (HSR: 75.6% reduction from
10,845 1,279 m2
to 2,647 507 m2
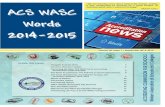
in group 1 vs.63.9% reduction from 12,878 1,258m2 to 4,648 340m2 in group 2, p 0.01; LSR: 79.7% reduction from7,753 542 m2 to 1,576 240 m2 in group 1 vs. 66.1%reduction from 8,098 1,281 m2 to 2,747 273m2 ingroup 2, p 0.0001). There were no significant differencesin the absolute baseline values of thrombus area at HSR orLSR between the two groups. Photomicrographs of totalthrombus formation in a representative patient from group1 are shownFigure 2.
To investigate the contribution of fibrin deposition tothrombus formation, we quantified fibrin area in both
groups. Fibrin deposition at HSR in group 1 decreased from7,276 1,033 m2 at baseline to 3,064 767 m2
post-eptifibatide (57.9% decline, p 0.0001). In group 2,fibrin deposition decreased from 8,081 2,039 m2 atbaseline to 4,093 1,009 m2 after the eptifibatide bolus(49.4% decline, p 0.0001). Although the reduction infibrin deposition achieved in group 1 was higher, thedifference between the groups did not reach statisticalsignificance.
DISCUSSION
The current study compared the antithrombotic efficacy ofeptifibatide administered to ACS patients receiving eitherenoxaparin or UFH. Both therapeutic combinations in-duced marked reductions in platelet aggregation andplatelet-thrombus formation. However, eptifibatide admin-istered with enoxaparin was associated with a significantlyhigher reduction in thrombus formation. This combinationtherapy, therefore, appears to exert a more potent anti-thrombotic effect than eptifibatide administered with UFHin the doses tested.In vitro and ex vivo effects of UFH and LMWH. In vitroand ex vivo studies have demonstrated that UFH causes
enhanced platelet activation (19,26,27). Unfractionatedheparin administrated to coronary patients or ex vivo addi-
tion of UFH to blood from normal volunteers resulted inactivation of GP IIb/IIIa receptors, increased expression of
P-selectin, and enhanced platelet aggregation with lowconcentrations of agonists (19,26 28). The mechanismresponsible for the UFH-induced platelet activation may beits binding to the platelet integrin alphaIIb-beta3 resultingin increased fibrinogen binding to the integrin and, there-fore, enhanced fibrinogen binding to the activated platelet(29). In contrast with UFH, LMWH has been shown tohave a more predictive anticoagulant effect with only minoreffects on platelet activation(26,27).Furthermore, admin-istration of LMWH, but not UFH, prevented repetitiveplatelet-dependent thrombus formation in a stenosed caninecoronary artery model(30).
Platelet effects of other GP IIb/IIIa inhibitors with UFHor LMWH. The reported increased platelet reactivity as-sociated with UFH could be the responsible mechanism forthe relatively reduced antithrombotic activity of eptifibatideadministered with UFH when compared with the combi-nation with enoxaparin in the current study. Other groupshave reported similar observations on the variability andplatelet inhibitory effects of other GP IIb/IIIa inhibitorswhen combined with UFH or LMWH. Administration oftirofiban or abciximab with LMWH resulted in lesservariability and a trend towards greater inhibition of plateletaggregation, as compared with the combination with UFH
(15,18). Furthermore, coadministration of tirofiban or ab-ciximab with UFH attenuated the inhibition offibrinogen-GP IIb/IIIa receptor binding achieved withoutUFH (18). This attenuation was not demonstrated whencombining these GP IIb/IIIa inhibitors with LMWH(18).
Table 2. Results of Complete Blood Count and Coagulation Tests
Group 1 (n 13) Group 2 (n 13)
Baseline Post-Eptifibatide Baseline Post-Eptifibatide
Hg (gm/dl) 14.5 2.1* 13.9 2.0* 13.8 1.5 13.7 1.5Plt (1,000/l) 240.1 57.5 235.9 43.7 223.5 43.6 233.2.1 50.6Fibr (mg/dl) 499.3 133.3 510.6 123.9 538.9 136.0 583.2 183.3
INR 1.0 0.1 1.0 0.1 1.1 0.1 1.0 0.1aPTT (s) 28.2 4.4 29.8 4.6 58.9 20.9 52.4 10.4
Anti-Xa (IU/ml) 0.85 0.2 0.84 0.2 0.57 0.1 0.55 0.1TAT (g/l) 10.0 10.7 11.5 11.6 9.0 9.6 8.2 6.5F1.2 (nmol/l) 1.4 0.4 1.6 0.6 1.8 1.0 1.8 0.8
Data presented as mean SD.*p 0.01, for baseline vs. post-eptifibatide in the specific group;p 0.001, for differences between the two groups in both
baseline and post-eptifibatide values.Anti-Xa anti-factor Xa activity; aPTT activated partial thromboplastin time; Fibr fibrinogen; F1.2 prothrombin
fragment 1 2; Hg hemoglobin; INR international normalized ratio; Plt platelets; TAT thrombin-antithrombincomplex.
Table 3. Results of Platelet Function Tests*
Group 1 (n 13) Group 2 (n 13)
10 M ADP aggregation 89.7% 85.5%20 M ADP aggregation 83.0% 77.9%RPFA 94.7% 92.9%
Differences between the two groups were not significant. *Expressed as percent
inhibition from baseline.ADP adenosine 5-diphosphate; RPFA rapid platelet function analyzer.
969JACC Vol. 43, No. 6, 2004 Lev et al.
March 17, 2004:966 71 Eptifibatide Combined With Enoxaparin or Heparin
-
8/13/2019 Eptifibatid u ACS
5/6
Similarly, UFH induced a reduction in the extent of platelet
inhibition produced by abciximab (19). However, this re-duction was only present at abciximab doses that inducedpartial platelet inhibition, and not when abciximab induced80% platelet aggregation inhibition(19).This observationmay explain the lack of significant differences in plateletaggregation between our two treatment groups. Eptifibatideat a dose of 180 g/kg bolus, followed by 2.0 g/kg/mininfusion, has been consistently shown to induce plateletaggregation inhibition 80%(3133).This marked plateletinhibitory effect may have overshadowed subtle differencesin platelet aggregation between the two combination groupsin our study. Microscopic evaluation of platelet-thrombus
formation under severe arterial injury conditions and atvarious shear rates may represent a more physiologic andsensitive method for assessment of therapeutic antithrom-botic effects.Effect onfibrin deposition. Treatment with abciximab hasbeen shown to reduce both platelet aggregates and thefibrinlayer of the thrombus when using a perfusion flow chambermodel (34). We have also observed, apart from a markedreduction in total thrombus formation, a decline in fibrindeposition after eptifibatide administration in both groups(57.9% reduction when eptifibatide was combined withenoxaparin and 49.4% reduction when combined with
UFH). Platelet aggregates facilitate thrombin generation byproviding a phospholipid surface on which coagulation
reactions occur efficiently (35). The reduction in fibrin
deposition after eptifibatide administration is explained by adecrease in the platelet mass available for thrombin forma-tion as a result of inhibition of platelet aggregation. A directeffect of eptifibatide on thrombin seems unlikely because, aspreviously observed(36),no reduction in thrombin forma-tion (F1.2) or TAT occurred after eptifibatide administra-tion, and furthermore, eptifibatide therapy has been shownnot to prolong ACT(37).Study limitations. Our study is limited by the smallnumber of patients in each group. However, because eachpatients baseline value served as his own control, highlysignificant intra-group differences could be obtained. The
significant differences observed between the two groups intotal thrombus formation are further emphasized given therelatively small patient number. The study was not random-ized, although we enrolled consecutive patients, and thedemographic and clinical characteristics of the two groupswere similar.
The results of the current study support the recentfindings of clinical trials evaluating combination therapywith small molecule GP IIb/IIIa inhibitors and enoxaparinin ACS patients(16,17).Both tirofiban and eptifibatide incombination with enoxaparin have been shown to reduceparameters of ischemia as compared with their combination
with UFH(16,17).The combination of GP IIb/IIIa inhib-itors with enoxaparin has also been shown to be safe(1217).Given the results of the recent clinical efficacy trialsand our findings regarding antithrombotic activity, thecombination of eptifibatide with enoxaparin appears to exerta more potent antithrombotic effect than eptifibatide andUFH in the doses tested. Further studies are needed inorder to determine whether ourfindings can be extrapolatedto other GP IIb/IIIa inhibitors and other LMWHs.
AcknowledgmentsThe authors gratefully acknowledge the critical comments
by Dr. David Varon and Dr. Yochai Birnbaum, which wereessential to the design and analysis of the study.
Figure 1. (A)Total thrombus area (m2) at high shear rate (HSR) and lowshear rate (LSR) in the enoxaparin-eptifibatide group, and (B) the UFH-eptifibatide group. Data presented as mean SEM. In both groups and atboth shear rates, highly significant differences were observed between thebaseline value and the post-eptifibatide value (p 0.0001). However, thereductions achieved in group 1 were significantly higher than those achieved ingroup 2 (p 0.01 for inter-group differences at HSR, p 0.0001 for LSR).Solid bars baseline;open bars post-eptifibatide.
Figure 2. Photomicgrographs of total thrombus formation in a represen-tative patient from group 1. (Upper panel) At baseline under enoxaparintreatment.(Lower panel)Combined treatment by enoxaparin and eptifi-batide (post-eptifibatide bolus). Staining with combined Massonstrichrome-elastin, 10-fold magnification.
970 Lev et al. JACC Vol. 43, No. 6, 2004Eptifibatide Combined With Enoxaparin or Heparin March 17, 2004:96671
-
8/13/2019 Eptifibatid u ACS
6/6
Reprint requests and correspondence: Dr. Ran Kornowski,Cardiology Department, Rabin Medical Center, 39 Jabotinski St.Petah-Tikva, 49100, Israel. E-mail: [email protected].
REFERENCES
1. Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA guidelineupdate for the management of patients with unstable angina andnon-ST-segment elevation myocardial infarction2002: summaryarticle: a report of the American College of Cardiology/AmericanHeart Association Task Force on Practice Guidelines (Committee onthe Management of Patients With Unstable Angina). Circulation2002;106:1893900.
2. Theroux P, Ouimet H, McCans J, et al. Aspirin, heparin or both totreat acute unstable angina. N Engl J Med 1988;319:110511.
3. Samama MM, Bara L, Gerotziafas GT. Mechanisms for the anti-thrombotic activity in man of low molecular weight heparins (LM-
WHs). Haemostasis 1994;24:10517.4. Hirsh J, Levine MN. Low molecular weight heparin. Blood 1992;79:
117.5. Warkentin TE, Levine MN, Hirsh J, et al. Heparin-induced throm-
bocytopenia in patients treated with low-molecular-weight heparin or
unfractionated heparin. N Engl J Med 1995;332:1330 5.6. Cohen M, Demers C, Gurfinkel EP, et al. A comparison of low-molecular weight heparin with UFH for unstable coronary arterydisease: Efficacy and Safety of Subcutaneous Enoxaparin in NonQ-
Wave Coronary Events study group. N Engl J Med 1997;337:44752.7. Antman EM, McCabe CH, Gurfinkel EP, et al. Enoxaparin prevents
death and cardiac ischemic events in unstable angina/nonQ-wavemyocardial infarction: results of the thrombolysis in myocardial infarc-tion (TIMI) 11B trial. Circulation 1999;100:1593601.
8. The PRISM-PLUS Investigators. Inhibition of the platelet glycopro-tein IIb/IIIa receptor with tirofiban in unstable angina and nonQ-
wave myocardial infarction. N Engl J Med 1998;338:148897.9. The PURSUIT Investigators. Inhibition of the platelet glycoprotein-
IIb/IIIa with eptifibatide in patients with acute coronary syndromes.N Engl J Med 1998;339:436 43.
10. The EPISTENT Investigators. Randomised placebo-controlled and bal-
loon angioplasty-controlled trial to assess safety of coronary stenting withuse of platelet glycoprotein IIb/IIIa blockade. Lancet 1998;352:8792.11. OShea JC, Hafley GE, Greenberg S, et al. Platelet glycoprotein
IIb/IIIa integrin blockade with eptifibatide in coronary stent interven-tion: the ESPRIT trial: a randomized controlled trial. JAMA 2001;16:246873.
12. Kereiakes DJ, Grines C, Fry E, et al. Enoxaparin and abciximabadjunctive pharmacotherapy during percutaneous coronary interven-tion. J Invasive Cardiol 2001;13:2728.
13. Galeote G, Hussein M, Sobrino N, Calvo L, Sanchez-Recalde A,Sobrino JA. Use of a combination of enoxaparin or unfractionatedheparin and abciximab during percutaneous coronary interventions: arandomized pilot study. Rev Esp Cardiol 2002;55:1261 6.
14. Khosla S, Kunjummen B, Guerrero M, et al. Safety and efficacy ofcombined use of low molecular weight heparin (enoxaparin, lovenox)and glycoprotein IIb/IIIa receptor antagonist (eptifibatide, integrelin)
during nonemergent coronary and peripheral vascular intervention.Am J Ther 2002;9:48891.15. Cohen M, Theroux P, Weber S, et al. Combination therapy with
tirofiban and enoxaparin in acute coronary syndromes. Int J Cardiol1999;71:27381.
16. Cohen M, Theroux P, Borzak S, et al. Randomized double-blindsafety study of enoxaparin versus unfractionated heparin in patients
with nonST-segment elevation acute coronary syndromes treatedwith tirofiban and aspirin: the ACUTE II study. The AnithromboticCombination Using Tirofiban and Enoxaparin. Am Heart J 2002;144:4707.
17. Goodman SG, Fitchett D, Armstrong PW, Tan M, Langer A.Randomized evaluation of the safety and efficacy of enoxaparin versusunfractionated heparin in high-risk patients with nonST-segmentelevation acute coronary syndromes receiving the glycoprotein IIb/IIIainhibitor eptifibatide. Circulation 2003;107:238 44.
18. Klinkhardt U, Graff J, Westrup D, et al. Pharmcodynamic character-ization of the interaction between abciximab or tirofiban with unfrac-
tionated or low molecular weight heparin in healthy subjects. Br J ClinPharmacol 2001;52:297305.
19. Mascelli MA, Kleiman NS, Marciniak SJ, Jr., Damaraju L, WeismanHF, Jordan RE. Therapeutic heparin concentrations augment plateletreactivity: implications for the pharmacologic assessment of the gly-coprotein IIb/IIIa antagonist abciximab. Am Heart J 2000;139:696 703.
20. Frenandez-Ortiz A, Badimon JJ, Falk E, et al. Characterization of the
relative thrombogenicity of atherosclerotic plaque components: impli-cations for consequences of plaque rupture. J Am Coll Cardiol1994;23:15629.
21. Badimon L, Turitto V, Rosenmark JA, Badimon JJ, Fuster V.Characterization of a tubular flow chamber for studying plateletinteraction with biologic and prosthetic materials: deposition ofindium 111-labeled platelets on collagen, subendothelium, and ex-panded polytetrafluoroethylene. J Lab Clin Med 1987;110:706 18.
22. Mailhac A, Badimon JJ, Fallon JT, et al. Effect of an eccentric severestenosis onfibrin(ogen) deposition on severely damaged vessel wall inarterial thrombosis: relative contribution offibrin(ogen) and platelets.Circulation 1994;90:988 96.
23. Toschi V, Gallo R, Lettino M, et al. Tissue factor modulates thethrombogenicity of atherosclerotic plaques. Circulation 1997;95:5949.
24. Galvez A, Badimon L, Badimon JJ, Fuster V. Electrical aggregometry
in whole blood from human, pig, rabbit. Thromb Haemost 1986;56:12832.25. Smith JW, Steinhubl SR, Lincoff AM, et al. Rapid platelet-function
assay: an automated and quantitative cartridge-based method. Circu-lation 1999;99:6205.
26. Xiao Z, Theroux P. Platelet activation with unfractionated heparin attherapeutic concentrations and comparisons with a low-molecular-
weight heparin and with a direct thrombin inhibitor. Circulation1998;97:2516.
27. Westwick J, Scully MF, Poll C, Kakkar VV. Comparison of lowmolecular weight heparin and unfractionated heparin on activation ofhuman platelets in vitro. Thromb Res 1986;42:43547.
28. Furman MI, Kereiakes DJ, Krueger LA, et al. Leukocyte-plateletaggregation, platelet surface P-selectin, and platelet surface glycopro-tein IIIa after percutaneous coronary intervention: effects of dalteparinor unfractionated heparin in combination with abciximab. Am Heart J
2001;142:790 8.29. Sobel M, Fish WR, Toma N, et al. Heparin modulates integrinfunction in human platelets. J Vasc Surg 2001;33:58794.
30. Leadley RJ, Jr., Kasiewski CJ, Bostwick JS, Bentley R, Dunwiddie CT,Perrone MH. Inhibition of repetitive thrombus formation in thestenosed canine coronary artery by enoxaparin, but not by unfraction-ated heparin. Arterioscler Thromb Vasc Biol 1998;18:908 14.
31. Steinhubl SR, Talley JD, Braden GA, et al. Point-of-care measuredplatelet inhibition correlates with a reduced risk of an adverse cardiacevent after percutaneous coronary intervention: results of the GOLD(AU-Assessing Ultegra) multicenter study. Circulation 2001;103:25728.
32. Batchelor WB, Tolleson TR, Huang Y, et al. Randomized comparisonof platelet inhibition with abciximab, tirofiban and eptifibatide duringpercutaneous coronary interventions in acute coronary syndromes: theCOMPARE trial. Circulation 2002;106:1470 6.
33. Kereiakes DJ, Broderick TM, Roth EM, et al. Time course, magni-tude, and consistency of platelet inhibition by abciximab, tiro fiban, oreptifibatide in patients with unstable angina pectoris undergoingpercutaneous coronary intervention. Am J Cardiol 1999;15:3915.
34. Dangas G, Badimon JJ, Coller BS, et al. Administration of abciximabduring percutaneous coronary intervention reduces both ex vivo plate-let thrombus formation and fibrin deposition. Arterioscler ThrombVasc Biol 1998;18:13429.
35. Swords NA, Mann KG. The assembly of the prothrombinase complexon adherent platelets. Arterioscler Thromb 1993;13:160212.
36. Kleiman NS, Tracy RP, Talley JD, et al. Inhibition of plateletaggregation with a glycoprotein IIb-IIIa antagonist does not preventthrombin generation in patients undergoing thrombolysis for acutemyocardial infarction. J Thromb Thrombolysis 2000;9:512.
37. Dauerman HL, Ball SA, Goldberg RJ, Desourdy MA, Furman MI.Activated clotting times in the setting of eptifibatide use during
percutaneous coronary intervention. J Thromb Thrombolysis 2002;13:12732.
971JACC Vol. 43, No. 6, 2004 Lev et al.
March 17, 2004:966 71 Eptifibatide Combined With Enoxaparin or Heparin