Epistaxis new
37
EPISTAXIS DR. M. FAROOQ S/R ENT DEPTT. SZH RYK
-
Upload
mfarooq184 -
Category
Health & Medicine
-
view
259 -
download
0
description
Epistaxis
Transcript of Epistaxis new

EPISTAXIS
DR. M. FAROOQS/R ENT DEPTT. SZH RYK

CONTENTSDEFINITIONSURGICAL ANATOMYBLOOD SUPPLYEPIDEMIOLOGYCLASSIFICATIONMANAGEMENT

EPISTAXISDefinition
Bleeding from noseGreek word- Epistazo ( Epi + Stazo) Epi - Over / above Stazo- To drip (from nostrils)

ANATOMY OF NOSE

ANATOMY OF NOSE

ANATOMY OF NOSE

BLOOD SUPPLYArterial supply
Ext. Carotid A Int. Carotid A
Venous Drainage Facial V Pterygoid Plexus Ant. & Post. Ethmoidal Veins

External Carotid Artery
-Sphenopalatine artery
-Greater palatine artery
-Ascending pharyngeal artery
-Posterior nasal artery
-Superior Labial artery
Internal Carotid Artery
-Anterior Ethmoid artery
-Posterior Ethmoid artery

BLOOD SUPPLY

BLOOD SUPPLY

BLOOD SUPPLY

BLOOD SUPPLY

EPIDEMIOLOGY30% of ENT AdmissionAgeSexSeasonArea / Region

CLASSIFICATIONOn the basis of
Etiology - Primary /Secondary Age - Children / Adult Site - Ant. / Post.

Anterior vs. PosteriorMaxillary sinus ostiumAnterior: younger, usually septal vs. anterior ethmoid, most common (>90%), typically less severePosterior: older population, usually from Woodruff’s plexus, more serious.

CAUSES OF EPISTAXISLocal Causes
General / systemic Causes
Idiopathic Causes

LOCAL CAUSESNose
Trauma Infections Foreign bodies Neoplasm Atmospheric changes DNS

LOCAL CAUSESNasopharynx
Infection Neoplasm

GENERAL CAUSESCardiovascular System
HTN, Mitral stenosis, Pregnancy.Disorders of Blood & blood Vessels
Aplastic Anaemia, Leukaemia, Thrombocytopaenias, Vascular Purpura, Haemophilia, Scurvy, Vit K Defficiency.

GENERAL CAUSESLiver Disease - CirrhosisKidney Disease- Ch. NephritisDrugs- NSAIDS, Anticoagulants (Warfarin)Mediastinal CompressionAccute General infections-
Measles, Chicken pox.

MANAGEMENTAims of Management
To stop blood loss To replace blood loss To find out the cause and treat it

MANAGEMENTMANAGEMENT – Diagnosis+TreatmentDiagnosis
History Examination Investigations CBC Bleeding & clotting profiles Radiology - Angiography

MANAGEMENTTreatment -Hierarchy of treatment
General Measures Direct Therapy - Primary Epistaxis Indirect Therapy - Secondary Epistaxis Surgical Options - Sec. Epistaxis

MANAGEMENT PLAN

Initial ManagementABC’sMedical history/MedicationsVital signs—need IV?Physical exam
Anterior rhinoscopyEndoscopic rhinoscopy
Laboratory examRadiologic studies

Non-surgical treatments Control of hypertension Correction of coagulopathies/thrombocytopenia
FFP or whole blood/reversal of anticoagulant/platelets
Pressure/Expulsion of clotsTopical decongestants/vasocontrictorsCautery (AgNo3 , Bipolar)Nasal packing (effective 80-90% of time)

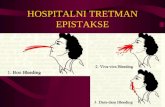
Nasal packsAnterior nasal packs
TraditionalRecent modifications
Posterior nasal packsTraditional Recent modifications
Ant/Post nasal packing

TSS—Nugauze vs. Merocel
Electron microscopy

Posterior Packs – Admission Elderly and those with other chronic diseases may need to be admitted to the ICUContinuous cardiopulmonary monitoringAntibioticsOxygen supplementation may be neededMild sedation/analgesiaIVF

Indications for surgery/embolizationContinued bleeding despite nasal packingPt requires transfusion/admit hct of <38% (barlow)Nasal anomaly precluding packingPatient refusal/intolerance of packingPosterior bleed vs. failed medical mgmt after >72hrs (wang vs. schaitkin)

Selective Angiography/embolizationHelps identify location of bleedingEmbolization most effective in patients who
Still bleeding after surgical arterial ligationBleeding site difficult to reach surgicallyComorbidities prohibit general anesthetic
Effective only when bleeding is >.5 ml/min90+% success rate, complication rate of 0.1%Only able to embolize external carotid & branchesComplications: minor (18-45%)/major (0-2%)Contraindicated in bad atherosclerosis, Ethmoid bleed

Surgical treatment
Transmaxillary IMA ligationIntraoral IMA ligationAnterior/Posterior Ethmoidal ligationTransnasal Sphenopalatine ligationExternal carotid artery ligation
Septodermoplasty/Laser ablation

Transmaxillary IMA ligationWaters view Caldwell-LucElectrocautery of posterior wall before removalMicroscopic dissection and ligation of IMA --descending palatine & sphenopalantine most importantRecurrence rate (failure rate) of 10-15%Complication rate of 25-30% (oa fistula,dental, n)

Intraoral IMA ligationPosterior gingivobuccal incision beginning at second molarTemporalis mm split and partially dissectedIMAX visualized, clipped and dividedAdvantages: children/facial fracturesDisadvantages: more proximal ligationComplications: trismus, damage to infraorbital n

Ant./Post. Ethmoidal ligationPatients s/p IMAX ligation still bleeding, superior nasal cavity epistaxis, or in conjunction when source unclearLynch incisionFronto-ethmoid
suture line12-24-6
(14-18, 8-10, 4-6)

Transnasal Endoscopic Sphenopalatine Artery ligation
Follow Middle Turbinate to posteriormost aspectVertical mucoperiosteal incision 7-8mm anterior to post middle turb (between mid. and inf. turbs)Elevation of flap—ID neurovascular bundle at foramenLigation with titanium clipReapproximate flapComplications –few, Failures—0-13%

THANK………….
YOU……………….