Epidemiology of Dengue
13
Official reprint from UpToDate www.uptodate.com ©2015 UpToDate Author Alan L Rothman, MD Section Editor Martin S Hirsch, MD Deputy Editor Elinor L Baron, MD, DTMH Epidemiology of dengue virus infections All topics are updated as new evidence becomes available and our peer review process is complete. Literature review current through: Jul 2015. | This topic last updated: Dec 11, 2014. INTRODUCTION — The viral etiology of dengue was established in the 1940s, and records of dengue-like illness date back more than 200 years [ 1]. Major changes in the epidemiology of dengue virus infections began after World War II and have continued to date. Given estimates of 390 million infections worldwide each year and over 2.5 billion individuals at risk for infection [ 2], the dengue viruses are arguably the most important arthropod-borne viruses from a medical and public health perspective. The cardinal features of the dengue virus transmission cycle, the characteristics of the mosquito vectors, and the factors that contribute to dengue virus transmission in the major affected regions will be reviewed here. The pathogenesis, clinical manifestations, diagnosis, treatment, and prevention of dengue virus infection are discussed separately. (See "Pathogenesis of dengue virus infection" and "Clinical manifestations and diagnosis of dengue virus infection" and "Prevention and treatment of dengue virus infection".) CLASSIFICATION — Dengue viruses are members of the family Flaviviridae, genus Flavivirus [ 3,4]. The dengue virus complex comprises at least four antigenically related but distinct viruses, designated dengue virus serotypes 1 through 4. All dengue viruses are mosquito-borne human pathogens that exclusively cause acute infection. TRANSMISSION CYCLE — Both epidemic and endemic transmission of dengue viruses are maintained through a human-mosquito-human cycle involving mosquitoes of the genus Aedes (Stegomyia) [ 5]. Transmission of dengue viruses between mosquitoes and nonhuman primates has been demonstrated in Asia and Africa, but there is no evidence that such transmission is an important reservoir for transmission to humans [ 5,6]. Susceptible humans become infected after being bitten by an infected female Aedes mosquito. Viremia in humans begins toward the end of a four- to six-day incubation period and persists until fever abates, which is typically three to seven days [ 7,8]. An uninfected Aedes mosquito may acquire the virus after feeding during this viremic period. The mosquito has an incubation period of 8 to 12 days before it is capable of transmitting the virus to susceptible individuals. Once infected, mosquitoes carry the virus for their lifespan and remain infective for humans. MOSQUITO VECTORS — Aedes (Stegomyia) aegypti mosquitoes, the principal vector for the transmission of dengue virus, have many characteristics that make them ideal for dissemination of the virus [ 5,9]. A. aegypti typically breed in or close to houses, laying eggs in both man-made and natural water containers. The typical flight distance is relatively short [ 10]. A. aegypti are daytime feeders that prefer to bite humans and are frequently unnoticed. They are easily interrupted in their feeding and move on to another host, frequently taking multiple blood meals in a single breeding cycle [ 11]. Thus, an infected A. aegypti mosquito may transmit dengue virus to several individuals in a small area. For these reasons, family members who are at home during the daytime, typically women and young children, are at particularly high risk for infection. A. aegypti are widely distributed in tropical and subtropical areas from latitude 45º North to 35º South. Yellow fever is also principally transmitted by A. aegypti; efforts to control urban yellow fevers in the Americas in the 1970s greatly restricted the distribution of the mosquitoes in the Western hemisphere, but the mosquitoes have since reinfested nearly all of their former habitats [ 7]. A. albopictus mosquitoes are also a competent vector for the transmission of dengue virus under both experimental and natural conditions [ 5,12]; they are more tolerant of the cold and have a wider geographic distribution than A. aegypti [ 12,13]. However, they are less likely to transmit since they do not bite humans as frequently as A. aegypti ® ® Epidemiology of dengue virus infections http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiolog... 1 de 13 11/08/2015 09:57 p.m.
-
Upload
said-plazola-mercado -
Category
Documents
-
view
6 -
download
0
description
Epidemiology of Dengueepidemiología del Dengue distribucion geográfica
Transcript of Epidemiology of Dengue

Official reprint from UpToDate
www.uptodate.com ©2015 UpToDate
AuthorAlan L Rothman, MD
Section EditorMartin S Hirsch, MD
Deputy EditorElinor L Baron, MD, DTMH
Epidemiology of dengue virus infections
All topics are updated as new evidence becomes available and our peer review process is complete.
Literature review current through: Jul 2015. | This topic last updated: Dec 11, 2014.
INTRODUCTION — The viral etiology of dengue was established in the 1940s, and records of dengue-like illness
date back more than 200 years [1]. Major changes in the epidemiology of dengue virus infections began after World
War II and have continued to date. Given estimates of 390 million infections worldwide each year and over 2.5 billion
individuals at risk for infection [2], the dengue viruses are arguably the most important arthropod-borne viruses from
a medical and public health perspective.
The cardinal features of the dengue virus transmission cycle, the characteristics of the mosquito vectors, and the
factors that contribute to dengue virus transmission in the major affected regions will be reviewed here. The
pathogenesis, clinical manifestations, diagnosis, treatment, and prevention of dengue virus infection are discussed
separately. (See "Pathogenesis of dengue virus infection" and "Clinical manifestations and diagnosis of dengue virus
infection" and "Prevention and treatment of dengue virus infection".)
CLASSIFICATION — Dengue viruses are members of the family Flaviviridae, genus Flavivirus [3,4]. The dengue
virus complex comprises at least four antigenically related but distinct viruses, designated dengue virus serotypes 1
through 4. All dengue viruses are mosquito-borne human pathogens that exclusively cause acute infection.
TRANSMISSION CYCLE — Both epidemic and endemic transmission of dengue viruses are maintained through a
human-mosquito-human cycle involving mosquitoes of the genus Aedes (Stegomyia) [5]. Transmission of dengue
viruses between mosquitoes and nonhuman primates has been demonstrated in Asia and Africa, but there is no
evidence that such transmission is an important reservoir for transmission to humans [5,6].
Susceptible humans become infected after being bitten by an infected female Aedes mosquito. Viremia in humans
begins toward the end of a four- to six-day incubation period and persists until fever abates, which is typically three
to seven days [7,8]. An uninfected Aedes mosquito may acquire the virus after feeding during this viremic period.
The mosquito has an incubation period of 8 to 12 days before it is capable of transmitting the virus to susceptible
individuals. Once infected, mosquitoes carry the virus for their lifespan and remain infective for humans.
MOSQUITO VECTORS — Aedes (Stegomyia) aegypti mosquitoes, the principal vector for the transmission of
dengue virus, have many characteristics that make them ideal for dissemination of the virus [5,9]. A. aegypti typically
breed in or close to houses, laying eggs in both man-made and natural water containers. The typical flight distance
is relatively short [10]. A. aegypti are daytime feeders that prefer to bite humans and are frequently unnoticed. They
are easily interrupted in their feeding and move on to another host, frequently taking multiple blood meals in a single
breeding cycle [11]. Thus, an infected A. aegypti mosquito may transmit dengue virus to several individuals in a
small area. For these reasons, family members who are at home during the daytime, typically women and young
children, are at particularly high risk for infection.
A. aegypti are widely distributed in tropical and subtropical areas from latitude 45º North to 35º South. Yellow fever is
also principally transmitted by A. aegypti; efforts to control urban yellow fevers in the Americas in the 1970s greatly
restricted the distribution of the mosquitoes in the Western hemisphere, but the mosquitoes have since reinfested
nearly all of their former habitats [7].
A. albopictus mosquitoes are also a competent vector for the transmission of dengue virus under both experimental
and natural conditions [5,12]; they are more tolerant of the cold and have a wider geographic distribution than A.
aegypti [12,13]. However, they are less likely to transmit since they do not bite humans as frequently as A. aegypti
®
®
Epidemiology of dengue virus infections http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiolog...
1 de 13 11/08/2015 09:57 p.m.

and appear to be less efficient natural vectors for dengue virus. Endemic transmission or large outbreaks in regions
that have A. albopictus but not A. aegypti mosquitoes are both rare. Both A. albopictus and A. aegypti are also
competent vectors for transmission of chikungunya virus, which has led to simultaneous outbreaks of both diseases
in some areas [14]. (See "Chikungunya fever".)
Other Aedes mosquitoes have been suspected of dengue virus transmission in isolated outbreaks in the Pacific
islands [15]. However, these species appear to play an insignificant role in the global transmission of dengue virus.
DISTRIBUTION OF A. AEGYPTI MOSQUITOES — A. aegypti and dengue viruses are endemic in many countries
(figure 1) [4,16], although epidemic dengue hemorrhagic fever (DHF) occurs predominantly in certain parts of Asia
and South America. The risk for exposure to A. aegypti is often higher in urban areas. Many tourist facilities present
a lower risk than local residential areas because of air conditioning, groundskeeping, elevation, or combinations of
these factors.
The number of cases of dengue fever (DF) and DHF reported globally varies considerably from year to year,
although the overall trend is one of increasing incidence. Global epidemics of disease have occurred at intervals of
several years [17-19].
The reported dengue activity in specific regions is described further below. Most available information is gathered
through passive surveillance activities and must be interpreted cautiously in light of underreporting of cases [20] and
lack of laboratory confirmation (table 1).
Asia and Pacific
Southeast Asia — A. aegypti mosquitoes are present throughout the region, extending to southern China and
the south of the island of Taiwan, and all countries in the region are affected by dengue virus infection.
Hyperendemic transmission of all four dengue serotypes (with cases of DHF) has occurred in Thailand, Vietnam,
and Indonesia for over 40 years. Epidemic dengue reemerged in China during the 1980s and the 1990s after an
absence of several decades and was associated with the first occurrence of DHF in that country [21]. Nepal had the
first cases detected in 2004.
Over 140 locally acquired cases of dengue were detected in Japan in 2014, representing the first occurrence of
transmission in that nation since World War II [22]. More than 80 percent of cases have been associated with visiting
a single location in Tokyo, and A. albopictus is the apparent vector in this outbreak.
Dengue virus transmission occurs year round but typically reaches a seasonal peak that varies in timing between
countries (for example, between June and November in Thailand, between January and February in Indonesia).
More than 200,000 cases of DHF were reported from the region each year from 2012 with the exception of 2011
(177,500 cases); Indonesia and Thailand accounted for the majority of cases in each of these years [23].
South Asia — A. aegypti are widely distributed in India, Pakistan, and Sri Lanka. Dengue virus transmission,
particularly in India and Sri Lanka, increased substantially during the 1980s and 1990s. Hyperendemic circulation of
all four dengue serotypes appears to be established, and outbreaks of DHF have become more frequent. Over
50,000 cases were reported from India in 2012, more than twice the average over the previous decade. Pakistan
has reported several outbreaks since 2011.
Western Pacific islands — A. aegypti mosquitoes are present in most of the region. Hyperendemic transmission
of all four dengue serotypes is present in Malaysia and the Philippines. Other islands experience frequent dengue
outbreaks; high incidence rates were reported from 14 island nations for 2009, including American Samoa, Cook
Islands, French Polynesia, New Caledonia, and Tonga [24]. (See "Potential health hazards in travelers to Australia,
New Zealand, and the southwestern Pacific (Oceania)".)
Australia — A. aegypti mosquitoes are present in the northeastern corner of Australia. Dengue viruses are not
endemic to the continent, but periodic introduction of dengue viruses from neighboring islands has led to epidemics
in urban areas of north Queensland [25,26]. (See "Potential health hazards in travelers to Australia, New Zealand,
and the southwestern Pacific (Oceania)".)
Epidemiology of dengue virus infections http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiolog...
2 de 13 11/08/2015 09:57 p.m.

Africa and Eastern Mediterranean — A. aegypti mosquitoes are present in much of sub-Saharan Africa and the
Middle East. Data are scant on dengue virus transmission. However, documented infections in visitors to the area
indicate that there is ongoing dengue virus transmission [27,28]. Several outbreaks were reported from Central
Africa, East Africa, and the Middle East during the 1990s and 2000s [14,16].
Europe — A. albopictus is present across much of southern Europe [29]. Most dengue cases reported from the
region have been acquired during travel to endemic countries. However, local transmission of dengue virus was
documented in both southern France and Croatia in 2010 [30]. In 2012, an outbreak of dengue was reported on
Madeira Island (Portugal), associated with the presence of A. aegypti [30].
Americas
North America — A. aegypti mosquitoes are present in most areas of Mexico and in the southeastern United
States. A. albopictus is also present in these areas, but its range extends further north, nearly to the Great Lakes.
Hyperendemic transmission of all four dengue virus serotypes is present throughout the range of A. aegypti in
Mexico. Dengue virus transmission is seasonal, with peak activity in late summer and fall. In 2013, over 230,000
cases of dengue infection were reported from Mexico, including more than 18,000 cases of severe dengue and 104
deaths [19].
Most dengue virus infections identified in the continental United States and all cases identified in Canada were
acquired during travel abroad or to Puerto Rico or the United States Virgin Islands [31-34]. Limited transmission of
dengue virus within southern Texas has been described since the 1980s [35], and an outbreak involving over 120
cases of locally acquired dengue infection occurred in Hawaii in 2001 [36]. In 2007, the Centers for Disease Control
and Prevention reported a case of DHF in a resident native to Texas who lived in a bordering area with Mexico [37];
this prompted a serosurvey of 346 households in the immediate neighborhood, which demonstrated that 38 percent
of the residents had IgG antibodies to dengue. In 2010, dengue fever was reported in 28 residents of Key West,
Florida, who had not traveled abroad [38], and a serosurvey of 240 participants living in Key West found that 5
percent had evidence of recent dengue infection. Local transmission of dengue virus continues to occur in south
Florida but thus far appears to be very limited in scope. Of 543 cases reported across the United States in 2013, 24
were locally acquired [19].
Central America — A. aegypti mosquitoes and hyperendemic transmission of all four dengue virus serotypes
are present throughout the region. The region experienced a major outbreak in 2013; Nicaragua and Costa Rica
reported among the highest numbers of cases of dengue (77,000 and 49,000, respectively) and incidence rates
(over 1000 cases per 100,000 population) that year [19]. However, all of these countries have had one or more years
of heavy dengue activity during the past five years.
Caribbean — A. aegypti mosquitoes are present throughout the region. Hyperendemic circulation of dengue
virus serotypes 1, 2, and 4 has been present on the larger islands (other than Cuba) for several decades and
dengue virus serotype 3 has been present since 1998. In Puerto Rico, peak dengue virus transmission usually
occurs between October and December; over 21,000 cases of dengue virus infection were reported there in 2010,
representing the largest outbreak ever recorded. The Dominican Republic (16,000 cases), French Guiana (16,000
cases), Guadeloupe (12,000 cases), Martinique (7,000 cases), and St. Martin (3,000 cases) all reported major
outbreaks in 2013 [19]. Other islands have experienced periodic dengue epidemics.
South America — A. aegypti mosquitoes are present in every South American country except Chile [16].
Hyperendemic circulation of all four dengue virus serotypes has been present in the north of the continent since the
reintroduction of dengue virus serotype 3 was detected in Brazil and Venezuela during 2000. Brazil, Venezuela, and
Colombia have reported the largest number of dengue cases. Low-level, year-round transmission has been
observed, but most cases follow an epidemic pattern; in Brazil, peak dengue transmission occurs between February
and May [39].
Brazil experienced a major outbreak in 2013, with nearly 1.5 million cases nationwide, including almost 7,000 cases
of severe dengue [19]. Colombia (127,000 cases) and Paraguay (144,000 cases) also reported major dengue
Epidemiology of dengue virus infections http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiolog...
3 de 13 11/08/2015 09:57 p.m.

outbreaks in 2013.
PATTERNS OF TRANSMISSION — Dengue virus transmission follows two general (but not mutually exclusive)
patterns, with different implications for disease risk in both the local population and travelers.
Epidemic dengue — Epidemic dengue transmission occurs when the introduction of dengue virus into a region is
an isolated event involving a single virus strain. If sufficiently large populations of susceptible hosts and mosquitoes
are present, transmission of dengue is explosive, leading to a recognizable epidemic. The incidence of infection
among susceptible individuals often reaches 25 to 50 percent [40] and can be considerably higher. Herd immunity,
changes in weather, and mosquito control efforts can all contribute to the termination of the epidemic [5].
Prior to World War II, transmission of dengue viruses almost exclusively followed this pattern [41]. Seaports
frequently were the point of initial introduction of dengue viruses, and these port cities then acted as distribution
points to nearby inland areas.
In smaller island nations, certain areas of South America and Africa, and in the areas of Asia where dengue virus
transmission has reemerged, epidemic activity is the predominant pattern of dengue virus transmission. The
incidence of dengue virus infections in these locations varies considerably from year to year. Intervals of several
years or more usually pass between epidemics, allowing the number of susceptible individuals to accumulate so that
the next epidemic can be perpetuated.
In the setting of epidemic transmission, adults and children in the local population are affected. Among travelers, the
risk for acquisition of dengue virus is high during an epidemic but low at other times. The frequency of dengue
hemorrhagic fever (DHF) is usually low, with some exceptions [42]. The viral serotype and strain and the interval
since the previous epidemic seem to influence the risk for DHF. (See "Pathogenesis of dengue virus infection".)
Hyperendemic dengue — "Hyperendemic" transmission refers to the continuous circulation of multiple dengue
virus serotypes in the same area. This requires the year-round presence of competent vector mosquitoes and either
a large population or steady movement of individuals into the area to maintain a pool of susceptible individuals.
Hyperendemic circulation involves the occurrence of multiple epidemics in a smaller geographic scale (eg, village or
school) [43].
Seasonal variation in virus transmission is common. The incidence of infection also varies from year to year, with
increased dengue transmission at intervals of three to four years, but this variation is not as dramatic as in areas
where transmission predominantly follows the epidemic pattern. A mathematical analysis of data from Thailand
suggested that these surges in dengue transmission originate in waves from major urban centers [44].
Areas with hyperendemic dengue virus transmission contribute to the majority of cases of dengue virus infection
globally. In some regions, 5 to 10 percent of the susceptible population experiences dengue virus infection annually
[45-47]. Urban areas are particularly affected.
In the setting of hyperendemic transmission, the prevalence of antibody against dengue virus rises with age.
Children are more likely than adults to experience disease, and most adults in the local population are immune to
infection. Among travelers, the risk for acquisition is higher than in areas that experience epidemic transmission, but
the seasonal variation in risk is somewhat predictable. Hyperendemicity is a major factor contributing to the
occurrence of DHF.
FACTORS INFLUENCING TRANSMISSION — The worldwide incidence of dengue and DHF has been increasing
in the past several decades, and the geographic distribution of these diseases has expanded. The emergence of
DHF as a public health problem has largely been a result of human behaviors including population growth, poor
urban planning with overcrowding and poor sanitation, modern transportation which allows increased movement of
humans, mosquitoes and viruses, and lack of effective mosquito control [7].
The potential effects of global climate change are a major source of concern for the future. Increased dengue virus
transmission has been associated with El Nino/Southern Oscillation events [48,49]. Mathematical models predict
that increased global temperatures will further expand the range of A. aegypti and dengue virus [50,51].
Epidemiology of dengue virus infections http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiolog...
4 de 13 11/08/2015 09:57 p.m.

The transmission cycle for dengue viruses is dependent upon the interaction between infective mosquitoes and
susceptible humans and between susceptible mosquitoes and viremic humans. Dengue virus transmission is
enhanced by the following factors [5]:
OTHER ROUTES OF TRANSMISSION — Given the high titers of infectious dengue virus found in blood and tissues
during acute infection, the potential exists for virus transmission by routes other than mosquito vectors.
Nosocomial transmission — At least four well-documented cases of transmission of dengue virus in the healthcare
setting via needlestick and one case of transmission by nonpercutaneous exposure have been reported [56]. Some
blood donors, although asymptomatic, have levels of viremia sufficient to transmit infection to recipients of their
blood components [57]. Cases of nosocomial transmission in dengue-endemic regions (also likely to encompass the
majority of exposures) would usually be overlooked due to the inability to distinguish nosocomial transmission from
mosquito transmission.
Vertical transmission — Vertical transmission of dengue has been reported in a few small case series [58]; based
on these cases and the known pattern of viremia, this possibility should be considered in cases where illness in the
mother occurs within the 10 days before delivery (including onset on the day of delivery). Illness presented in these
newborns up to 11 days (median 4 days) after birth.
Pregnancy does not appear to increase the incidence or severity of dengue [59]. In a prospective study conducted in
Kuala Lumpur of 2958 parturients, 2531 paired maternal-umbilical cord blood samples were tested for dengue-
specific IgM to determine the prevalence of infection and the vertical transmission rate [60]. Sixty-three women (2.5
percent) had a positive IgM serology. Only one (1.6 percent, 95% CI 0-9.5%) of the paired umbilical cord samples
was seropositive for dengue. None of the maternal and fetal blood samples had evidence of viral RNA by
polymerase chain reaction.
Breastfeeding has also been proposed as a route of vertical transmission of dengue virus [61].
SUMMARY
Increased vector density – One study of naturally infected humans estimated that viremia levels of
approximately 6 to 8 log10 RNA copies/mL led to infection of half of A. aegypti mosquitoes that took a blood
meal under laboratory conditions [52]. In many tropical countries, seasonal increases in rainfall contribute to an
increased density of mosquitoes. One factor that can be modified is the presence of open water storage
containers in or near the home.
●
Shorter mosquito incubation – The length of the incubation time in the mosquito (known as the extrinsic
incubation period) is inversely associated with the ambient temperature. Warmer temperatures increase the
length of time that a mosquito remains infective.
●
Increased movement of mosquito vectors and viruses – Air, land, and water transportation of mosquitoes or
viremic humans facilitate the dissemination of dengue viruses.
●
Increased density of susceptible hosts – Crowded conditions probably increase the potential for virus
transmission. However, as the prevalence of prior infection increases, the fraction of the population that
remains susceptible is reduced.
●
Increased duration and magnitude of viremia in humans – Attenuated virus strains produced in the laboratory
have been shown to produce low titers of virus in the blood, which are not efficiently transmitted to mosquitoes
[53,54]. It is unclear whether natural strains of dengue virus differ in the viremia titers they produce [55].
●
Dengue viruses are members of the family Flaviviridae, genus Flavivirus. The dengue virus complex comprises
four antigenically related but distinct viruses, which are mosquito-borne human pathogens. (See 'Classification'
above.)
●
Susceptible humans become infected after being bitten by an infected female Aedes mosquito. Viremia in
humans begins toward the end of a four- to six-day incubation period and persists until fever abates. An
●
Epidemiology of dengue virus infections http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiolog...
5 de 13 11/08/2015 09:57 p.m.

Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
Rush AB. An account of the bilious remitting fever, as it appeared in Philadelphia in the summer and autumn ofthe year 1780. In: Medical Inquiries and Observations, Richard & Hall, Philadelphia p.104.
1.
Bhatt S, Gething PW, Brady OJ, et al. The global distribution and burden of dengue. Nature 2013; 496:504.2.
Henchal EA, Putnak JR. The dengue viruses. Clin Microbiol Rev 1990; 3:376.3.
Wilder-Smith A, Schwartz E. Dengue in travelers. N Engl J Med 2005; 353:924.4.
Kuno G. Review of the factors modulating dengue transmission. Epidemiol Rev 1995; 17:321.5.
Wang E, Ni H, Xu R, et al. Evolutionary relationships of endemic/epidemic and sylvatic dengue viruses. J Virol2000; 74:3227.
6.
Gubler DJ. Epidemic dengue and dengue hemorrhagic fever: a global public health problem in the 21stcentury. In: Emerging Infections I, Scheld WM, Armstrong D, Hughes JM (Eds), ASM Press, Washington, DC1998. p.1.
7.
Vaughn DW, Green S, Kalayanarooj S, et al. Dengue in the early febrile phase: viremia and antibodyresponses. J Infect Dis 1997; 176:322.
8.
Halstead SB. Selective primary health care: strategies for control of disease in the developing world. XI.Dengue. Rev Infect Dis 1984; 6:251.
9.
Harrington LC, Scott TW, Lerdthusnee K, et al. Dispersal of the dengue vector Aedes aegypti within andbetween rural communities. Am J Trop Med Hyg 2005; 72:209.
10.
Scott TW, Amerasinghe PH, Morrison AC, et al. Longitudinal studies of Aedes aegypti (Diptera: Culicidae) inThailand and Puerto Rico: blood feeding frequency. J Med Entomol 2000; 37:89.
11.
Gratz NG. Critical review of the vector status of Aedes albopictus. Med Vet Entomol 2004; 18:215.12.
uninfected Aedes mosquito may acquire the virus after feeding on an infected individual during this viremic
period. Once infected, mosquitoes carry the virus for their lifespan and remain infective for humans. (See
'Transmission cycle' above.)
Aedes aegypti mosquitoes are daytime feeders that prefer to bite humans and are frequently unnoticed. They
are easily interrupted in their feeding and move on to another host, frequently taking multiple blood meals in a
single breeding cycle. Thus, an infected A. aegypti mosquito may transmit dengue virus to several individuals
within a small geographic area. (See 'Mosquito vectors' above.)
●
Epidemic dengue transmission occurs when the introduction of dengue virus into a region is an isolated event
involving a single virus strain. If sufficiently large populations of susceptible hosts and mosquitoes are present,
transmission of dengue is explosive, leading to a recognizable epidemic. Herd immunity, changes in weather,
and mosquito control efforts can all contribute to the termination of the epidemic. (See 'Epidemic dengue'
above.)
●
"Hyperendemic" transmission refers to the continuous circulation of multiple dengue virus serotypes in the
same area. This requires the year-round presence of competent vector mosquitoes and an ongoing presence
of susceptible individuals. (See 'Hyperendemic dengue' above.)
●
Dengue virus transmission is enhanced by multiple factors, including higher vector density, greater movement
of mosquito vectors, and increased density of susceptible humans. (See 'Factors influencing transmission'
above.)
●
Aedes aegypti and dengue viruses are endemic in every continent except Europe and Antarctica, although
epidemic dengue hemorrhagic fever occurs predominantly in Asia and the Americas. (See 'Distribution of A.
Aegypti mosquitoes' above.)
●
Epidemiology of dengue virus infections http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiolog...
6 de 13 11/08/2015 09:57 p.m.

Centers for Disease Control (CDC). Update: Aedes albopictus infestation--United States, Mexico. MMWRMorb Mortal Wkly Rep 1989; 38:440, 445.
13.
Caron M, Paupy C, Grard G, et al. Recent introduction and rapid dissemination of Chikungunya virus andDengue virus serotype 2 associated with human and mosquito coinfections in Gabon, central Africa. Clin InfectDis 2012; 55:e45.
14.
Savage HM, Fritz CL, Rutstein D, et al. Epidemic of dengue-4 virus in Yap State, Federated States ofMicronesia, and implication of Aedes hensilli as an epidemic vector. Am J Trop Med Hyg 1998; 58:519.
15.
Pinheiro FP, Corber SJ. Global situation of dengue and dengue haemorrhagic fever, and its emergence in theAmericas. World Health Stat Q 1997; 50:161.
16.
WHO Report on Global Surveillance of Epidemic-Prone Infectious Diseases. www.who.int/csr/resources/publications/dengue/CSR_ISR_2000_1/en (Accessed on October 08, 2014).
17.
DengueNet www.who.int/denguenet (Accessed on October 08, 2014).18.
PanAmerican Health Organization. Dengue. http://new.paho.org/hq/index.php?option=com_content&task=view&id=264&Itemid=363&lang=en (Accessed on October 08, 2014).
19.
Undurraga EA, Halasa YA, Shepard DS. Use of expansion factors to estimate the burden of dengue inSoutheast Asia: a systematic analysis. PLoS Negl Trop Dis 2013; 7:e2056.
20.
Qiu FX, Gubler DJ, Liu JC, Chen QQ. Dengue in China: a clinical review. Bull World Health Organ 1993;71:349.
21.
Kutsuna S, Kato Y, Moi ML, et al. Autochthonous dengue fever, Tokyo, Japan, 2014. Emerg Infect Dis 2015;
21:517.
22.
World Health Organization Regional Office of South-East Asia. Dengue fact sheet. http://www.searo.who.int/entity/vector_borne_tropical_diseases/data/data_factsheet/en/ (Accessed on October 09, 2014).
23.
World Health Organization Western Pacific Region. Dengue in the Western Pacific Region.http://www.wpro.who.int/emerging_diseases/Dengue/en/ (Accessed on October 09, 2014).
24.
Dengue in the WHO Western Pacific Region. Wkly Epidemiol Rec 1998; 73:273.25.
Mackenzie JS, Broom AK, Hall RA, et al. Arboviruses in the Australian region, 1990 to 1998. Commun DisIntell 1998; 22:93.
26.
Eisenhut M, Schwarz TF, Hegenscheid B. Seroprevalence of dengue, chikungunya and Sindbis virus infections
in German aid workers. Infection 1999; 27:82.
27.
Sharp TW, Wallace MR, Hayes CG, et al. Dengue fever in U.S. troops during Operation Restore Hope,Somalia, 1992-1993. Am J Trop Med Hyg 1995; 53:89.
28.
Schaffner F, Medlock JM, Van Bortel W. Public health significance of invasive mosquitoes in Europe. ClinMicrobiol Infect 2013; 19:685.
29.
Tomasello D, Schlagenhauf P. Chikungunya and dengue autochthonous cases in Europe, 2007-2012. TravelMed Infect Dis 2013; 11:274.
30.
Centers for Disease Control and Prevention (CDC). Imported dengue--United States, 1997 and 1998. MMWRMorb Mortal Wkly Rep 2000; 49:248.
31.
Rigau-Pérez JG, Gubler DJ, Vorndam AV, Clark GG. Dengue surveillance--United States, 1986-1992. MMWRCDC Surveill Summ 1994; 43:7.
32.
Centers for Disease Control and Prevention (CDC). Travel-associated dengue infections--United States,2001-2004. MMWR Morb Mortal Wkly Rep 2005; 54:556.
33.
Centers for Disease Control and Prevention (CDC). Notes from the field: School reporting of a dengueoutbreak--St. Croix, U.S. Virgin Islands, 2012. MMWR Morb Mortal Wkly Rep 2013; 62:172.
34.
Centers for Disease Control and Prevention (CDC). Imported dengue--United States, 1996. MMWR MorbMortal Wkly Rep 1998; 47:544.
35.
Effler PV, Pang L, Kitsutani P, et al. Dengue fever, Hawaii, 2001-2002. Emerg Infect Dis 2005; 11:742.36.
Centers for Disease Control and Prevention (CDC). Dengue hemorrhagic fever--U.S.-Mexico border, 2005.MMWR Morb Mortal Wkly Rep 2007; 56:785.
37.
Epidemiology of dengue virus infections http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiolog...
7 de 13 11/08/2015 09:57 p.m.

Centers for Disease Control and Prevention (CDC). Locally acquired Dengue--Key West, Florida, 2009-2010.MMWR Morb Mortal Wkly Rep 2010; 59:577.
38.
Siqueira JB Jr, Martelli CM, Coelho GE, et al. Dengue and dengue hemorrhagic fever, Brazil, 1981-2002.Emerg Infect Dis 2005; 11:48.
39.
McBride WJ, Mullner H, LaBrooy JT, Wronski I. The 1993 dengue 2 epidemic in North Queensland: aserosurvey and comparison of hemagglutination inhibition with an ELISA. Am J Trop Med Hyg 1998; 59:457.
40.
Gubler DJ. Dengue and dengue hemorrhagic fever: its history and resurgence as a global public health
problem. In: Dengue and Dengue Hemorrhagic Fever, Gubler DJ, Kuno G (Eds), CAB International,Wallingford 1997. p.1.
41.
Kouri GP, Guzmán MG, Bravo JR, Triana C. Dengue haemorrhagic fever/dengue shock syndrome: lessonsfrom the Cuban epidemic, 1981. Bull World Health Organ 1989; 67:375.
42.
Endy TP, Nisalak A, Chunsuttiwat S, et al. Spatial and temporal circulation of dengue virus serotypes: aprospective study of primary school children in Kamphaeng Phet, Thailand. Am J Epidemiol 2002; 156:52.
43.
Cummings DA, Irizarry RA, Huang NE, et al. Travelling waves in the occurrence of dengue haemorrhagic feverin Thailand. Nature 2004; 427:344.
44.
Burke DS, Nisalak A, Johnson DE, Scott RM. A prospective study of dengue infections in Bangkok. Am J TropMed Hyg 1988; 38:172.
45.
Porter KR, Beckett CG, Kosasih H, et al. Epidemiology of dengue and dengue hemorrhagic fever in a cohort ofadults living in Bandung, West Java, Indonesia. Am J Trop Med Hyg 2005; 72:60.
46.
Endy TP, Chunsuttiwat S, Nisalak A, et al. Epidemiology of inapparent and symptomatic acute dengue virusinfection: a prospective study of primary school children in Kamphaeng Phet, Thailand. Am J Epidemiol 2002;156:40.
47.
Hales S, Weinstein P, Woodward A. Dengue fever epidemics in the South Pacific: driven by El Niño SouthernOscillation? Lancet 1996; 348:1664.
48.
Dengue. Wkly Epidemiol Rec 1998; 73:185.49.
Jetten TH, Focks DA. Potential changes in the distribution of dengue transmission under climate warming. AmJ Trop Med Hyg 1997; 57:285.
50.
Hales S, de Wet N, Maindonald J, Woodward A. Potential effect of population and climate changes on globaldistribution of dengue fever: an empirical model. Lancet 2002; 360:830.
51.
Nguyet MN, Duong TH, Trung VT, et al. Host and viral features of human dengue cases shape the populationof infected and infectious Aedes aegypti mosquitoes. Proc Natl Acad Sci U S A 2013; 110:9072.
52.
Bhamarapravati N, Yoksan S, Chayaniyayothin T, et al. Immunization with a live attenuated dengue-2-viruscandidate vaccine (16681-PDK 53): clinical, immunological and biological responses in adult volunteers. BullWorld Health Organ 1987; 65:189.
53.
Schoepp RJ, Beaty BJ, Eckels KH. Infection of Aedes albopictus and Aedes aegypti mosquitoes with dengueparent and progeny candidate vaccine viruses: a possible marker of human attenuation. Am J Trop Med Hyg1991; 45:202.
54.
Gubler DJ, Suharyono W, Lubis I, et al. Epidemic dengue 3 in central Java, associated with low viremia inman. Am J Trop Med Hyg 1981; 30:1094.
55.
Chen LH, Wilson ME. Transmission of dengue virus without a mosquito vector: nosocomial mucocutaneoustransmission and other routes of transmission. Clin Infect Dis 2004; 39:e56.
56.
Stramer SL, Linnen JM, Carrick JM, et al. Dengue viremia in blood donors identified by RNA and detection ofdengue transfusion transmission during the 2007 dengue outbreak in Puerto Rico. Transfusion 2012; 52:1657.
57.
Sirinavin S, Nuntnarumit P, Supapannachart S, et al. Vertical dengue infection: case reports and review.Pediatr Infect Dis J 2004; 23:1042.
58.
Carroll ID, Toovey S, Van Gompel A. Dengue fever and pregnancy - a review and comment. Travel Med InfectDis 2007; 5:183.
59.
Tan PC, Rajasingam G, Devi S, Omar SZ. Dengue infection in pregnancy: prevalence, vertical transmission,and pregnancy outcome. Obstet Gynecol 2008; 111:1111.
60.
Epidemiology of dengue virus infections http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiolog...
8 de 13 11/08/2015 09:57 p.m.

Barthel A, Gourinat AC, Cazorla C, et al. Breast milk as a possible route of vertical transmission of denguevirus? Clin Infect Dis 2013; 57:415.
61.
Topic 3028 Version 15.0
Epidemiology of dengue virus infections http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiolog...
9 de 13 11/08/2015 09:57 p.m.

GRAPHICS
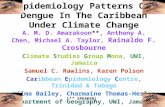
Map of global dengue burden
Reproduced from: Guzman MG, Harris E. Dengue. Lancet 2014. Illustration used with the permission of Elsevier Inc. All rights reserve
Graphic 60722 Version 2.0
Epidemiology of dengue virus infections http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiolog...
10 de 13 11/08/2015 09:57 p.m.

Alphabetical listing of countries and territories with reported dengue
transmission since 2000
Anguilla
Antigua and Barbuda
Argentina
Aruba
Australia
Bahamas
Bangladesh
Barbados
Belize
Bhutan
Bolivia
Brazil
Brunei Darussalam
Cambodia
Cameroon
Cape Verde
Chile (Easter Island)
China
Colombia
Cook Islands
Costa Rica
Côte d'Ivoire
Croatia
Cuba
Dominica
Dominican Republic
Ecuador
El Salvador
Fiji
France
French Guiana
French Polynesia
Gabon
Grenada
Malaysia
Maldives
Martinique
Mauritius
Mexico
Micronesia
Montserrat
Myanmar
Nepal
New Caledonia
New Zealand
Nicaragua
Northern Mariana Islands
Pakistan
Palau
Panama
Papua New Guinea
Paraguay
Peru
Philippines
Portugal (Madeira)
Puerto Rico
Rarotonga
Samoa
Saudi Arabia
Senegal
Singapore
Solomon Islands
Sri Lanka
St. Kitts & Nevis
St. Lucia
St. Vincent & the Grenadines
Suriname
Tahiti
Epidemiology of dengue virus infections http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiolog...
11 de 13 11/08/2015 09:57 p.m.

Guadeloupe
Guatemala
Guyana
Haiti
Honduras
India
Indonesia
Jamaica
Japan
Kiribati
Lao People's Democratic Republic
Madagascar
Taiwan
Thailand
Timor-Leste
Tonga
Trinidad & Tobago
United States of America
Vanuatu
Venezuela
Viet Nam
Virgin Islands (UK)
Virgin Islands (US)
Yemen
Courtesy of Alan L Rothman, MD.
Graphic 70287 Version 3.0
Epidemiology of dengue virus infections http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiolog...
12 de 13 11/08/2015 09:57 p.m.

Disclosures: Alan L Rothman, MD Consultant/Advisory Boards: Sanofi Pasteur [Prevention and treatment of dengue virus infections(Tetravalent live-attenuated dengue vaccine Chimerivax-DEN)]. Martin S Hirsch, MD Nothing to disclose. Elinor L Baron, MD, DTMHNothing to disclose.
Contributor disclosures are reviewed for conflicts of interest by the editorial group. When found, these are addressed by vetting through amulti-level review process, and through requirements for references to be provided to support the content. Appropriately referenced content isrequired of all authors and must conform to UpToDate standards of evidence.
Conflict of interest policy
Disclosures
Epidemiology of dengue virus infections http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiolog...
13 de 13 11/08/2015 09:57 p.m.