EPIDEMIOLOGY OF COMMUNITY ACQUIRED PNEUMONIA … · quantitative polymerase chain reaction for...
22
EPIDEMIOLOGY OF COMMUNITY EPIDEMIOLOGY OF COMMUNITY ACQUIRED PNEUMONIA IN THE ICU ACQUIRED PNEUMONIA IN THE ICU APRIL 17, 2013 RABEA ALZUBAIDY Directeur de mémoire : Dr Denis GAROT Service de Réanimation Médicale Polyvalente, CHRU de Tours Mémoire DESC de Réanimation Inter-région Ouest Université François Rabelais Faculté de médecine de Tours 2012-2013
Transcript of EPIDEMIOLOGY OF COMMUNITY ACQUIRED PNEUMONIA … · quantitative polymerase chain reaction for...

EPIDEMIOLOGY OF COMMUNITY EPIDEMIOLOGY OF COMMUNITY ACQUIRED PNEUMONIA IN THE ICUACQUIRED PNEUMONIA IN THE ICU
APRIL 17, 2013 RABEA ALZUBAIDY
Directeur de mémoire : Dr Denis GAROT Service de Réanimation Médicale Polyvalente, CHRU de Tours
MémoireDESC de Réanimation Inter-région Ouest
Université François Rabelais Faculté de médecine de Tours 2012-2013

Community Acquired PneumoniaCommunity Acquired Pneumonia• Epidemiology of CAP and their pathogen
o The etiology remains unknown in approximately one-half of the cases
o Establishing a microbial diagnosis is challenging.
o The role of viruses ??
• The new PCRo Still developing since 1983, recently implemented in clinical practice for bacterial and viral
pathogens
o The multiplex PCR RespiFinder SMART 22®: 21 microorganisms
Jokinen C, Heiskanen L, Juvonen H, et al. Microbial etiology of community-acquired pneumonia in the adult population of 4 municipalities in eastern Finland. Clin Infect Dis 2001; 32(8):1141–1154.
Bartlett, J. M. S.; Stirling, D. (2003). "A Short History of the Polymerase Chain Reaction". PCR Protocols 226. pp. 3–6. doi:10.1385/1-59259-384-4:3. ISBN 1-59259-384-4.
Targets of The RespiFinder®SMART 22
Bacteria• Mycoplasma pneumoniae
• Legionella pneumophila• Chlamydophila pneumoniae
• Bordetella pertussis
DNA Viruses• Adenovirus
• Bocavirus
RNA Viruses• Influenza A
• Influenza A/H1N1• Influenza B
• Coronavirus 229E• Coronavirus HKU1
• Coronavirus NL63• Coronavirus OC43
• Human Metapneumovirus• Parainfluenza Type 1
• Parainfluenza Type 2
• Parainfluenza Type 3• Parainfluenza Type 4
• Respiratory Syncytial Virus A• Respiratory Syncytial Virus B
• Rhinovirus/Enterovirus

Materials and Methods Materials and Methods • Retrospective cohort Study, 37-beds medical ICU (Bretonneau Hospital, University
hospital of Tours, France).• The winter-spring months (from the 1st of November 2011 till the 2nd of May 2012).• All patients with primary diagnosis of CAP:
o Review of the ICU database for CAP diagnosis.o Review of the PCR laboratory database
All discharge summary were reviewed to check for diagnostic criteria of CAP • Data extraction :
o Demographics, outcomeo Microbiological samples :
o Cultures: Blood, endotracheal aspirate or bronchoalveolar lavage.o Urine samples for Streptococcus pneumoniaeand Legionella pneumophilaantigen detection.o Serology for Mycoplasma pneumoniae, Chlamydophila pneumoniae, Legionella pneumophilaand
Coxiella burnetti. o PCR: Nasopharyngeal secretion or bronchoalveolar lavage.

ResultsResultsbaseline characteristics and comorbidities baseline characteristics and comorbidities
• During 6 months, 98 patients with CAP were included.
• A microbial etiology could be identified for 64% (n= 63).Baseline characteristics and risk factors
Characteristics No. of patients (n= 98)Male / Female 61 (62%) / 37 (38%)
Age (years) 63±16.6
Simplified acute physiology score II 37±19
Mechanical ventilation 47 (48%)
Chronic obstructive pulmonary disease 20 (20%)
Other chronic respiratory disease 19 (19%)
Chronic renal failure 10 (10%)
Chronic heart failure 13 (13%)
Hypertension 40 (41%)
Diabetes 22 (22%)
Obesity 10 (10%)
Immunocompromised patient 3 (3%)
Data are presented as count (percentage) and mean±SD

ResultsResultsSpecimensSpecimens

Results Results Overall DistributionsOverall Distributions
Bacteria
n= 40
Viruses
n= 40
Co
-infectio
n
n= 17
Isolated
Bacteria
n= 23
58%
Isolated
Viruses
n= 22
55% Total patients n= 98
Patients with at least one pathogen n= 63

ResultsResultsBacterial InfectionsBacterial Infections
Bacterial pathogens
Pathogen No. of patients (%)
Streptococcus pneumoniae 26 (65%)
Mycoplasma pneumoniae 7 (18%)
Staphylococcus aureus 3 (7.5%)
Legionella pneumophila 1 (2.5%)
Haemophilus influenzae 1 (2.5%)
Neisseria 1 (2.5%)
Acinetobacter baumannii 1 (2.5%)
No bacterial-bacterial co-infection
• 40 patients (63% of the patients with an identified etiology)

ResultsResultsBacterial Infections: Bacterial Infections: Streptococcus PneumoniaeStreptococcus Pneumoniae
• The most frequent pathogen n= 26 patients (41% of the patients with an identified etiology).
• Detection methodso Urine Antigen for 20 patients (78%).o Blood Cultures for 8 patients (31%).o Endotracheal Aspirate for 5 patients (19%).
• 8 cases (31% of streptococcalcases) with viral co-infections (Myxovirus influenzae A and Adenovirus).

ResultsResultsBacterial Infections: Bacterial Infections: Mycoplasma PneumoniaeMycoplasma Pneumoniae
• 7 patients diagnosed by The new PCR (11% of patients with an identified etiology).
• The serologic diagnosis was either negative (n=3) or not contributive in 4 patients
Mycoplasma pneumoniae (PCR versus serology)
No. patients (n=7) PCR 1st serolog 2nd serology
2 Positive Negative Not repeated
2 Positive Not specific Not repeated
3 Positive Negative Negative• Overall serology test was
challengingo 1st serology (n= 44) 45%
o 2nd serology (n= 13) 13%

ResultsResultsViral InfectionsViral Infections
• Virus identifications:
58% Positive Viral
infections (n=40)

ResultsResultsViral InfectionsViral Infections
• 40 patients (63% of the patients with an identified etiology)
• Viral pathogens:
Viruses identifies through PCR
Pathogen Positive patients (n= 40 out of 69 tested patients)
Myxovirus influenzae A 15 (38%)
Bocavirus 11 (28%)
Adenovirus 8 (20%)
Rhinovirus 8 (20%)
Coronavirus 5 (12%)
Human Metapneumovirus 5 (12%)
Parainfluenza Type 3 1 (2%)
Respiratory Syncytial Virus B 1 (2%)
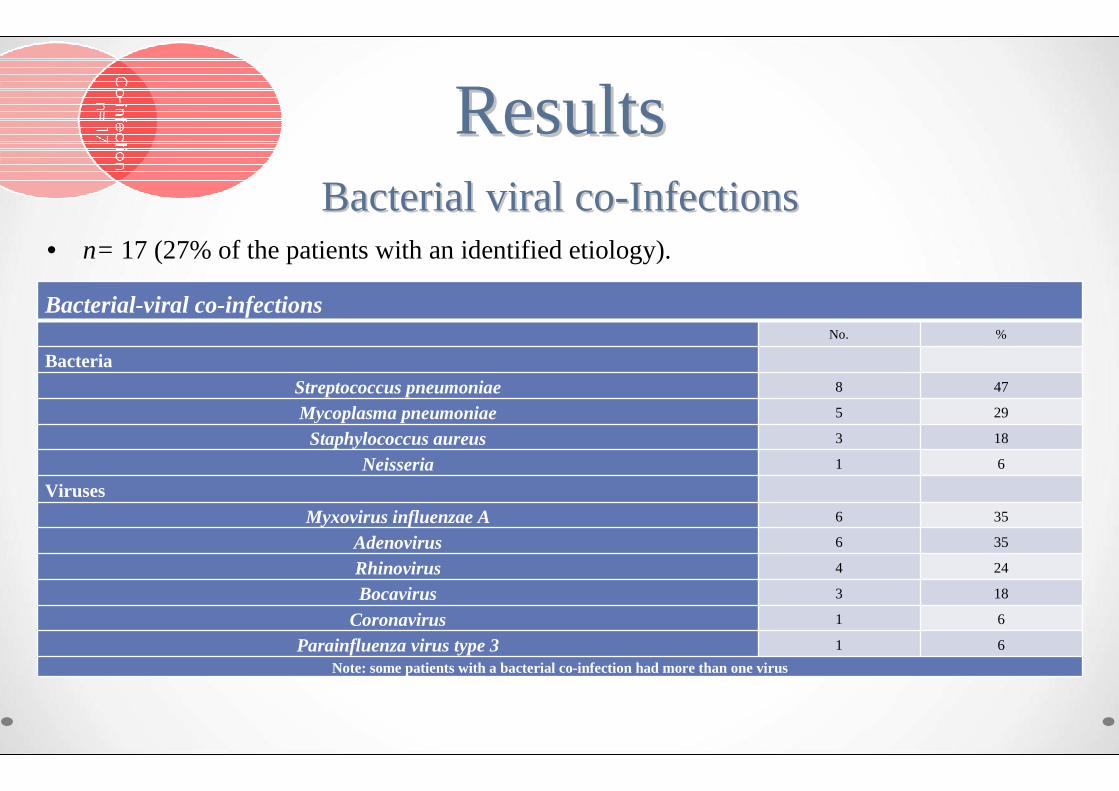
ResultsResultsBacterial viral coBacterial viral co--InfectionsInfections
• n= 17 (27% of the patients with an identified etiology).
Bacterial-viral co-infectionsNo. %
BacteriaStreptococcus pneumoniae 8 47
Mycoplasma pneumoniae 5 29
Staphylococcus aureus 3 18
Neisseria 1 6
VirusesMyxovirus influenzae A 6 35
Adenovirus 6 35
Rhinovirus 4 24
Bocavirus 3 18
Coronavirus 1 6
Parainfluenza virus type 3 1 6
Note: some patients with a bacterial co-infection had more than one virus

ResultsResultsMortalityMortality
• The overall ICU mortality was 15% (n= 15).

DiscussionDiscussion
• The main results of this retrospective study :
o Among two-thirds of patients in whom a pathogen could be identified, Streptococcus pneumoniae, was the most frequently identified pathogen.
o Identification of pathogens with the multiplex PCR tool was frequent. This was particularly important for viruses, observed in more than half of the samples analyzed, and to a lesser extend for Mycoplasma pneumoniae.

• Adults with CAP admitted to hospital were studied prospectively during a 12-month period.
• Microbiological testing methods: same samples collection but different PCR technique (real-time quantitative PCR).
• Results:o n=184
o A microbial etiology could be identified for 67% (n=124).
o The most frequently detected pathogen was S. pneumoniae 56% (n=70).
o Respiratory virus 43% (n=53).
o Co-infections (n=43) 35% (most commonly S. pneumoniae).
Niclas Johansson, Mats Kalin, et al. Etiology of community-acquired pneumonia: increased microbiological yield with new diagnostic methods. Clinical Infectious Diseases 2010; 50:202–9

• A prospective cohort study for CAP and HCAP (in a 28-bed medical ICU); for one year.
• Microbiological testing methods: same samples collection but different PCR technique (real-time quantitative PCR).
• Results for CAP:o n= 198, (CAP n= 64; HCAP n= 134).o A microbial etiology could be identified for 67% (n= 133)o S. pneumoniae: n=23 (17%). o Respiratory virus 54% (n= 72).o Co-infections 14% (n= 18).
Choi SH, Hong SB, Ko GB, et al. Viral infection in patients with severe pneumonia requiring intensive care unit admission. Am J Respir Crit Care Med. 2012;186 (4):325-332

LimitationsLimitations• Uncompleted patients’ information and clinical data.
• Lack of adjustment for confounders of outcomes including severity of disease, comorbidities and complications.
• The interdependence between diagnostic toolso The sample collection was not completed for all patients (only 40% had complete sampling n= 39)o Some samples may not be taken if previous results are known to the physician.
• The exact time of sampling in relation with antibiotics delivery was unknown.
• No firm gold standard diagnostic used for: viruses, Mycoplasma

ConclusionConclusion• The most common pathogen in severe forms of CAP was Streptococcus
pneumoniae… PCR technique soon to come into clinical practice…
• Multiplex PCR was frequently positive in our patients : viruses,Mycoplasma
• Viruses were frequently found and may cause severe forms of pneumonia (either alone or in association with bacteria).
• Co-infections were observed in 1/3 of the patients
• To overcome the limits of this retrospective study we initiated a prospective data collection which started in the winter 2012-2013.

ReferencesReferences1. File TM. Community-acquired pneumonia. Lancet 2003; 362(9400): 1991–2001.
2. Ruiz M, Ewig S, Marcos MA, et al. Etiology of community-acquired pneumonia: impact of age, comorbidity, and severity. Am J Respir Crit Care Med 1999; 160(2):397–405.
3. Jokinen C, Heiskanen L, Juvonen H, et al. Microbial etiology of community-acquired pneumonia in the adult population of 4 municipalities in eastern Finland. Clin Infect Dis 2001; 32(8):1141–1154.
4. Niclas Johansson, Mats Kalin, et al. Etiology of community-acquired pneumonia: increased microbiological yield with new diagnostic methods. Clinical Infectious Diseases 2010; 50:202–9
5. Welti M, Jaton K, Altwegg M, Sahli R, Wenger A, Bille J. Development of a multiplex real-time quantitative PCR assay to detect Chlamydia pneumoniae, Legionella pneumophila and Mycoplasma pneumoniae in respiratory tract secretions. Diagn Microbiol Infect Dis 2003; 45(2): 85–95.
6. Kais M, Spindler C, Kalin M, Ortqvist A, Giske CG. Quantitative detection of Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis in lower respiratory tract samples by real-time PCR. Diagn Microbiol Infect Dis 2006; 55(3):169–178.
7. Johansson N, Kalin M, Giske CG, Hedlund J. Quantitative detection of Streptococcus pneumonia from sputum samples with real-time quantitative polymerase chain reaction for etiologic diagnosis of community-acquired pneumonia. Diagn Microbiol Infect Dis 2008; 60(3): 255–261.
8. World Health Organization (WHO), manual for the laboratory diagnosis and virological surveillance of influenza 2011.
9. Choi SH, Hong SB, Ko GB, et al. Viral infection in patients with severe pneumonia requiring intensive care unit admission. Am J Respir Crit Care Med. 2012;186 (4):325-332.
10. Harper SA, Bradley JS, et al. Seasonal influenza in adults and children--diagnosis, treatment, chemoprophylaxis, and institutional outbreak management: clinical practice guidelines of the Infectious Diseases Society of America. Clin Infect Dis. 2009 15;48 (8):1003-32.

ReferencesReferences11. Papadopoulos NG, Bates PJ, Bardin PG, et al. Rhinoviruses infect the lower airways. J Infect Dis 2000; 181(6):1875–1884.
12. Samransamruajkit R, Hiranrat T, Chieochansin T, et al. Prevalence, clinical presentations and complications among hospitalized children with influenza pneumonia. Jpn J Infect Dis 2008; 61(6):446–449.
13. Angeles Marcos M, Camps M, Pumarola T, et al. The role of viruses in the aetiology of community-acquired pneumonia in adults. Antivir Ther 2006; 11(3):351–359.
14. Jennings LC, Anderson TP, Beynon KA, et al. Incidence and characteristics of viral community-acquired pneumonia in adults. Thorax 2008; 63(1):42–48. 18
15. Tiveljung-Lindell A, Rotzen-Ostlund M, Gupta S, et al. Development and implementation of a molecular diagnostic platform for daily rapid detection of 15 respiratory viruses. J Med Virol 2009; 81(1):167–175.
16. Johnstone J, Majumdar SR, Fox JD, Marrie TJ. Viral infection in adults hospitalized with community-acquired pneumonia: prevalence, pathogens, and presentation. Chest 2008; 134:1141–1148.
17. Charles PG, Whitby M, Fuller AJ, Stirling R, Wright AA, Korman TM, Holmes PW, Christiansen KJ, Waterer GW, Pierce RJ, et al.The etiology of community-acquired pneumonia in Australia: why penicillin plus doxycycline or a macrolide is the most appropriate therapy. Clin Infect Dis 2008; 46:1513–1521.
18. Cillo´ niz C, Ewig S, Ferrer M, Polverino E, Gabarrus A, Puig de la Bellacasa J, Mensa J, Torres A. Community-acquired polymicrobial pneumonia in the intensive care unit: aetiology and prognosis. Crit Care 2011; 15:R209.
19. American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med 2005; 171:388–416.
20. Palacios G, Hornig M, Cisterna D, Savji N, Bussetti AV, Kapoor V, Hui J, Tokarz R, Briese T, Baumeister E, et al. Streptococcus pneumonia coinfection is correlated with the severity of H1N1 pandemic influenza. PLoS ONE 2009; 4:e8540.

ReferencesReferences21. Carratala J, Mykietiuk A, Fernandez-Sabe N, Suarez C, Dorca J, Verdaguer R, Manresa F, Gudiol F. Health care-associated pneumonia requiring hospital admission: epidemiology, antibiotic therapy, and clinical outcomes. Arch Intern Med 2007; 167:1393-1399.
22. de Roux A, Marcos MA, Garcia E, et al. Viral community-acquired pneumonia in non immunocompromised adults. Chest 2004; 125(4):1343–1351.
23. Kalin M, Lindberg AA. Diagnosis of pneumococcal pneumonia: a comparison between microscopicexamination of expectorate, antigen detection and cultural procedures. Scand J Infect Dis 1983; 15(3):247–255.
24. Bartlett JG, Dowell SF, Mandell LA, File TM Jr, Musher DM, Fine MJ. Practice guidelines for the management of community-acquired pneumonia in adults. Clin Infect Dis 2000; 31(2):347–382.
25. Hedlund J, Ortqvist A, Kalin M. Nasopharyngeal culture in the pneumonia diagnosis. Infection 1990; 18(5):283–285.
26. Kalin M. Bacteremic pneumococcal pneumonia: value of culture of nasopharyngeal specimens and examination of washed sputum specimens. Eur J ClinMicrobiol 1982; 1(6):394–396.
27. Bartlett JG, Finegold SM. Bacteriology of expectorated sputum with quantitative culture and wash technique compared to transtracheal aspirates. Am Rev Respir Dis 1978; 117(6):1019–1027.
28. Howard LS, Sillis M, Pasteur MC, Kamath AV, Harrison BD. Microbiological profile of community-acquired pneumonia in adults over the last 20 years. J Infect 2005; 50 (2):10713. 19
29. Genné D, Sommer R, Kaiser L, Saaïdia A, Pasche A, Unger PF. Analysis of factors that contribute to treatment failure in patients with community-acquired pneumonia. Eur J Clin Microbiol Infect Dis 2006;25(3):159-66.
30. Noreddin AM, Elkhatib WF. Levofloxacin in the treatment of community-acquired pneumonia. Expert Rev Anti Infect Ther= 2010;8(5):505-14.

ReferencesReferences31. Chokshi R, Restrepo MI, Weeratunge N, Frei CR, Anzueto A, Mortensen EM. Monotherapy versus combination antibiotic therapy for patients with bacteremic Streptococcus pneumoniae community-acquired pneumonia. Eur J Clin Microbiol Infect Dis 2007;26(7):447-51.
32. CDC. Interim Guidance on Antiviral Recommendations for Patients with Confirmed or Suspected Swine Influenza A (H1N1) Virus Infection and Close Contacts. Centers for Disease Control and Prevention. Available at http://www.cdc.gov/swineflu/recommendations.htm[Accessed April 28, 2012].
33. WHO guidelines for pharmacological management of pandemic (H1N1) 2009 influenza and other influenza viruses. World Health Organization. Available at http://www.who.int/csr/resources/publications/swineflu/h1n1_use_antivirals_20090820/en/index.html. [Accessed August 20, 2012].
34. Lim WS, Macfarlane JT, Boswell TC, et al. Study of community acquired pneumonia aetiology (SCAPA) in adults admitted to hospital: implications for management guidelines. Thorax 2001; 56(4):296–301.
35. Oosterheert JJ, van Loon AM, Schuurman R, et al. Impact of rapid detection of viral and atypical bacterial pathogens by real-time polymerase chain reaction for patients with lower respiratory tract infection. Clin Infect Dis 2005; 41(10):1438–1444.