Epidemiology and prevention of HCV in IDUs
25
Epidemiology and prevention of HCV in IDUs Viktor Mravcik MD PhD
description
Epidemiology and prevention of HCV in IDUs. Viktor Mravcik MD PhD. HCV. enveloped RNA virus, genus Hepacivirus within the Flaviviridae family reservoir is human, but transmission to chimpanzees possible highly mutable – can escape host detection and elimination - PowerPoint PPT Presentation
Transcript of Epidemiology and prevention of HCV in IDUs

Epidemiology and prevention of HCV in IDUs
Viktor Mravcik MD PhD

HCV enveloped RNA virus, genus Hepacivirus within the
Flaviviridae family reservoir is human, but transmission to chimpanzees
possible highly mutable – can escape host detection and
elimination highly heterogeneous – 11 genotypes (1-4 the most
prevalent) and more than 80 subtypes– In Europe historically genotypes 1-3, but recent
transmission of genotype 4 among IDUs

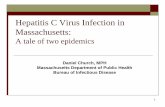
Global distribution of HCV genotypes

Routes of transmissionIDU the highest risk of infection, the most-at-risk
subgroup in developed countries
Iatrogenic exposure such as unsafe invasive procedures, infected blood products (in developing countries)
Mother to child transmission risk 4–8% among mothers without and 17-25% with HIV co-infection
Sexual transmission low or no risk of sexual HCV transmission, increased with HIV co-infection
Intranasal drug use increased risk
Tattoo and piercing increased risk (OR=2.2)
Undocumented route of transmission 20-25% of HCV infections

Natural history of HCV infection Incubation period: 2 weeks – 6 months Acute infection: typically asymptomatic or
unspecific symptoms Spontaneous clearance: 20–60 % (Loomba et al. 2011)
– IDUs 1/3 (van den Berg et al. 2011)
Cirrhosis in 8–45 % of chronic carriers in 20 years– 15 % in IDUs (John-Baptiste et al. 2010)
Liver decompensation and/or HCC peaks in 30 years after infection (Davis et al. 2010)

Natural history of HCV infection
Source: WHO (2014) Guidelines for the screening, care and treatment of persons with hepatitis C infection

Factors contributing to progression of liver diseases in HCV infection
Podle Virová hepatitida C, Urbánek 2010 a Chronické virové hepatitidy, Galský a Plíšek, 2010
Virologic factors External factorsHigh viral load Alcohol
Genotype 1SmokingEnvironmental contaminants
Host factorsHigher age ComorbidityMale gender liver fibrosis, cirrhosisRace (Afro-American) hemochromatosisCo-infections: non-alcoholic steatohepatitis
HBV weak immune responseHIV diabetes mellitus
Genetic factors obesityHLA class II Expression of diseasegenetic polymorphism in IL28B normal ALT

Prevalence of HCV Prevalence of anti-HCV globally 2.8 % (95% CI:
2,6–3,1%) = central estimate of 185 million people living with HCV infection (Mohd Hanafiah et al. 2012)
– in Europe prevalence of HCV typically 1.5–3.5 %– in the Czech Republic: 0.2% (Němeček, 2003)
350 000 deaths annually (1/4 cirrhosis and HCC attributable to HCV) (Perz et al. 2006)


Anti-HCV seroprevalence in general population in Europe
Source: ECDC, 2009

Reported HCV cases per 100 th. population in 2007

HCV in IDUs Global prevalence of anti-HCV in IDUs: 60–80% (Nelson et al.
2011)
– the highest (over 90%) in Russia, China, Poland, Spain Prevalence of anti-HCV in IDUs in EU: 12–85%, mostly over
40% (EMCDDA, 2012) IDUs represent 75–100% all newly diagnosed cases of HCV in
most European countries (Wiessing et al. 2008)
Incidence rate in IDUs: up to 40, typically 10–20 per 100 person-years (Roy et al. 2002; Roy et al. 2007; Stein et al. 2009; Holtzman et al. 2009)
Re-infection in IDUs quite rare (3–5%) even in active drug users (Dalgard et al. 2002; Grebely et al. 2011)

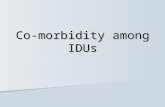
Ant-HCV prevalence in IDUs in 2010– 2011C
zech
Rep
ublic
Hun
gary
Slo
veni
a
Mal
ta
Slo
vaki
a
Aus
tria
Uni
ted
Kin
gdom
Tur
key
Cyp
rus
Sw
eden
Por
tuga
l
Net
herla
nds
Italy
Latv
ia
Bel
gium
Ger
man
y
Nor
way
Gre
ece
Bul
garia
Est
onia
%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Source: EMCDDA, 2013

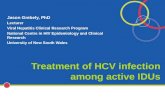
Notified cases of HCV – proportion of IDUs
199219931994199519961997199819992000200120022003200420052006200720082009201020110
10
20
30
40
50
60
70
80
90
100
Czech Republic (AC)Denmark (C)Germany (AC)Estonia (A)Ireland (AC)Italy (A)Luxembourg (AC)Slovakia (A)Slovakia (C)Finland (AC)Sweden (AC)United Kingdom (AC)Turkey (AC)Norway (AC)
%
Source: EMCDDA, 2013

ECDC AND EMCDDA GUIDLINES 2011: Prevention and control of infectious diseases among people who inject drugs
http://www.emcdda.europa.eu/publications/ecdc-emcdda-guidance

16
Seven recommended key interventions 1. Access to injection equipment (NSPs)2. Vaccination
– not in HCV3. Drug dependence treatment
– including OST4. Testing (early detection)
– including on-the-spot rapid testing5. Infectious disease treatment
– antiviral treatment in HCV6. Health promotion
– safer inj. behaviour, condom use, disease prevention, testing, treatment7. Targeted delivery of services
– organised, combined, referrals, multidisciplinary (one-stop-shop)
Combination of these key interventions enhances prevention synergy and effectiveness!

OST coverage in EU in 2011
Latvi
a
Slova
kia
Lithuania
Cypru
s
Hungary
Greece
Croatia
Ireland
Germany
Malta
Austria
Czech
Republic
The Neth
erlands
Italy
England
Luxe
mbourg
Norway
0
10
20
30
40
50
60
70
80
90
100
Opi
oid
mai
nten
ance
trea
tmen
t clie
nts (
%)

Syringes distributed through NSPs per estimated IDUs in 2011

NSPs and OST in HCV prevention NSPs less effective in prevention of HCV than in HIV
(Mehta et al. 2011) Simultaneous participation in NSP and OST enhances
the effect (Hagan, 2011; van den Berg et al. 2007; Turner et al. 2011) However NSP and OST have limited effect in
substantial reduction of HCV prevalence – unless the intervention coverage is scaled-up to 60% for 40% baseline HCV prevalence (Vickerman et al., 2012a, Vickerman et al., 2012b)
Strong preventive potential of HCV treatment!

HCV treatment in IDUs Standard: PEG-IFN and RBV for 48 (genotypes 1 and 4) or 24
(genotypes 2 and 3) weeks – SVR approx. 50% in genotype 1 and 65-82% in genotype 2 and 3
SVR in IDUs comparable to non-IDUs:– central estimates 54-56% (Hellard et al. 2009, Dimova et al. 2012)– 56% (95%CI: 50-61%), 37% for GT 1/4, 67% for GT 2/3 (Aspinall et al. 2013)
DAAs:– higher SVR: median 90%, range 80–100% (Martin et al. 2013)– shorter regimens (12 weeks)
However HCV treatment uptake in IDUs is generally low– fear of low adherence leading to low SVR– range of specific factors related to uptake and adherence in IDUs
More in following presentations!

HCV treatment as a (primary) prevention Risk of HCV transmission decreases with lower HCV prevalence Even for low treatment rates, a large reduction of HCV at the
population level can be achieved (Zeiler et al. 2010; Martin et al. 2011) Effect is larger in populations with a lower baseline HCV
prevalence (Vickerman et al. 2010) HCV treatment of active injecting drug users is the most cost-
effective policy option when the chronic HCV prevalence among PWID is below 60% and even for lower suggested SVR in IDUs (Martin et al. 2012)
In low-prevalent countries (anti-HCV below 30 %), treatment of active IDUs is more efficient (AnnekeS de Vos et al. 2013)

Source: Martin NK, Vickerman P, Foster GR, Hutchinson SJ, Goldberg DJ, and Hickman M. J Hep 2011; 54:1137-44
22
Preventive effect of HCV treatment in IDUs

Preventive effect of HCV treatment in IDUs
Source: Can Hepatitis C virus treatment be used as a prevention strategy? Additional model projections for Australia and elsewhere, Vickerman et al., 2010

Combination of NSP, OST and HCV treatment in reducing HCV prevalence Source: Martin et al. 2013