Epidemiologic Measure (6)

of 30
-
Upload
estipramestiningtyas -
Category
Documents
-
view
239 -
download
4
Transcript of Epidemiologic Measure (6)
-
7/31/2019 Epidemiologic Measure (6)
1/30
Afifah Machlaurin
-
7/31/2019 Epidemiologic Measure (6)
2/30
-
7/31/2019 Epidemiologic Measure (6)
3/30
The letter from McBride 1961 aboutcongenital
abnormalities
In 1962 FrancesOldham Kelsey (FDA)blocked themarketing of
thalidomide
-
7/31/2019 Epidemiologic Measure (6)
4/30
Antibiotics were administered to the patienteven before an infectious cause of fever wasidentified.
Why????? The potential risk of complications from
delayed antibiotic treatment outweighed thelikelihood of harm from treatmentadministered before the cause of the feverwas determined.
-
7/31/2019 Epidemiologic Measure (6)
5/30
every treatment decision involves acounterbalancing of risks and benefits
how epidemiologic measures can be used toassess outcomes and thereby guide decisionmaking
-
7/31/2019 Epidemiologic Measure (6)
6/30
Risk the likelihood that an individual willcontract a disease
prevalence the amount of disease alreadypresent in a population
incidence rate how fast new occurrencesof disease arise. In addition, these measurescan be used to assess the prognosis andmortality of patients with disease.
-
7/31/2019 Epidemiologic Measure (6)
7/30
risk is the proportion of unaffectedindividuals who, on average, will contract the
disease of interest over a specified period oftime.
-
7/31/2019 Epidemiologic Measure (6)
8/30
This study began in 1995 andconcluded in 2004. Patient A wasenrolled in 1995, was diagnosedwith the disease just prior to 1997,and was followed up until death in2002. Patient B was enrolled in
1997, was followed up until 1999without developing the disease,and then discontinuedparticipation in the study. PatientC was enrolled in 1999, wasdiagnosed with the disease justprior to 2002, and survived
through the end of theobservation period in 2004.Patients D, E, and F entered thestudy in 1997, 2002, and 1998,respectively; each patient wasfollowed through 2004 withoutdeveloping the disease.
-
7/31/2019 Epidemiologic Measure (6)
9/30
The 2-yearrisk of
disease,therefore, isestimated by
-
7/31/2019 Epidemiologic Measure (6)
10/30
to estimate a cancer patient's risk of acquiring aninfection in the hospital (a nosocomial infection), astudy was conducted of 5031 patients admitted to acomprehensive cancer center. The investigatorscarefully defined a nosocomial infection as aninfection that (1) is documented by cultures, (2) wasnot incubating at admission, (3) occurred at least 48hours after admission, and (4) occurred no more than
48 hours following discharge (somewhat longer forsurgical wound infections). Of the 5031 patients, 596developed an infection that met these criteria.
-
7/31/2019 Epidemiologic Measure (6)
11/30
1022 cancer patients with fever andgranulocytopenia were studied according to adefined protocol. Of these patients, 530 had a
clinically or microbiologically documented bacterialinfection. Thus, the risk of infection ingranulocytopenic, febrile cancer patients isestimated to be
This result suggests that patients similar to the one described in the PatientProfile have a very high risk of a bacterial infection, thus supporting the decisionto treat the patient with antibiotics even before an infection is diagnosed.
-
7/31/2019 Epidemiologic Measure (6)
12/30
Prevalence indicates the number of existingcases of the disease of interest in a
population
cases (C), the number of persons
in the population (N)
-
7/31/2019 Epidemiologic Measure (6)
13/30
Prevalence in1995
-
7/31/2019 Epidemiologic Measure (6)
14/30
96 people attending an outpatient clinic forthe first time. Patients with skin infections
were excluded from the study. S aureus wascultured from specimens from 62 patients.The prevalence of colonization with S aureusin this group was
-
7/31/2019 Epidemiologic Measure (6)
15/30
incidence rate measures the rapidity withwhich newly diagnosed cases of the disease
of interest develop
-
7/31/2019 Epidemiologic Measure (6)
16/30
Patient A developedthe disease 2 yearsafter entry into thestudy. Becausesubjects contribute
person-time onlywhile eligible todevelop the disease,the person-time forPatient A was 2 years.Similarly, Patients B,C, D, E, and Fcontributed 2, 3, 7, 2,and 6 years,respectively. PatientsA and C developeddisease
-
7/31/2019 Epidemiologic Measure (6)
17/30
Thus, A (the numberof new cases ofdisease in thepopulation) = 2, the
total PT = 2 + 2 + 3 + 7+ 2 + 6 = 22 person-years,
-
7/31/2019 Epidemiologic Measure (6)
18/30
Returning to the study cited in Example 1, the incidence rateof nosocomial infections can be calculated from additionaldata reported in that investigation. The 5031 patients
remained under observation for a total of 127,859 patient-days (or an average length of stay of 127,859/5031 = 25.4days). Since 596 patients developed an infection that metthe definition for a hospital-acquired infection, the incidencerate can be estimated as
-
7/31/2019 Epidemiologic Measure (6)
19/30
In the United States, the National Cancer Institutemaintains a network of registries that collectinformation on all new occurrences of cancer within
populations residing in specific geographic areas.Collectively, these registries cover about 14% of thepopulation of the United States, and between 1996and 2000, 2957 females were newly diagnosed withacute myelocytic leukemia in these areas. Anestimated 19,185,836 females lived in these combinedareas on average during this 5-year period.
Calculate the IR !
-
7/31/2019 Epidemiologic Measure (6)
20/30
-
7/31/2019 Epidemiologic Measure (6)
21/30
The use of an antibiotic, norfloxacin, was studiedfor prevention of gram-negative bacterialinfections in patients with acute leukemia who
had treatment-related low neutrophil counts. All35 patients who received norfloxacin developedfever. The 35 patients were observed for a totalof 220.5 person-days before first developing
fever; each day, on average, about 28% of thepatients had a fever.
Calculate the R, P, and IR !
-
7/31/2019 Epidemiologic Measure (6)
22/30
Survival is the probability of remaining alivefor a specific length of time.
S = Survival
A = the number of newly diagnosed patientsunder observation D = the number of newly diagnosed patients
under observation
-
7/31/2019 Epidemiologic Measure (6)
23/30
the 2-yearsurvival is
-
7/31/2019 Epidemiologic Measure (6)
24/30
When studying survival and risk, problemsmay arise if the investigator cannot follow
some subjects for the entire risk period Statisticians have developed special
techniques called survival analyses,
-
7/31/2019 Epidemiologic Measure (6)
25/30
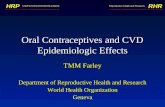
The horizontal axis plotstime in years sincediagnosis (0 = time ofdiagnosis) and the verticalaxis plots the percentageof patients who are alive.
The survival curve begins atthe time of diagnosis,when 100% of patients arealive. During the first yearfollowing diagnosis, 32% ofthe patients die (orequivalently, 100% 32% =68% survive). During thenext year, another 10% ofpatients die (cumulativesurvival = 68% 10% =58%). The process ofattrition to death continueseach year through the endof the 5-year observation
period.
-
7/31/2019 Epidemiologic Measure (6)
26/30
Thepercentage of5 yearssurvivors
(47%) is thenread from thevertical axis
-
7/31/2019 Epidemiologic Measure (6)
27/30
mediansurvival
time = 3
tahun
-
7/31/2019 Epidemiologic Measure (6)
28/30
The propensity of a disease to cause thedeath of affected patients
-
7/31/2019 Epidemiologic Measure (6)
29/30
-
7/31/2019 Epidemiologic Measure (6)
30/30
Penelitian ini dimulai pada tahun 1995 dan menyimpulkanpada tahun 2004. Seorang pasien yang terdaftar padatahun 1995, didiagnosa menderita penyakit ini hanyasebelum 1997, dan diikuti sampai meninggal pada tahun
2002. B Pasien terdaftar pada tahun 1997, dilanjutkanhingga 1999 tanpa penyakit, dan kemudian dihentikanpartisipasi dalam studi. C Pasien terdaftar pada tahun1999, didiagnosa menderita penyakit ini hanya sebelum2002, dan bertahan sampai akhir periode observasi pada
tahun 2004. Pasien D, E, dan F memasuki studi pada tahun1997, 2002, dan 1998, masing-masing; setiap pasiendiikuti sampai 2004 tanpa terserang penyakit itu.