Envisioning the Integration of Behavioral Health in a Women’s Care Clinic: A tour of the process a...
21
Envisioning the Integration of Behavioral Health in a Women’s Care Clinic: A tour of the process a year in K.C. Lomonaco, Psy.D., Psychologist, Denver Health Medical Center Alison Lieberman, Psy.D., Psychologist, Denver Health Medical Center Collaborative Family Healthcare Association 17 th Annual Conference October 15-17, 2015 Portland, Oregon U.S.A. Session # C2b October 16, 2015
-
Upload
samson-page -
Category
Documents
-
view
215 -
download
0
Transcript of Envisioning the Integration of Behavioral Health in a Women’s Care Clinic: A tour of the process a...
Envisioning the Integration of Behavioral Health in a Women’s Care Clinic: A tour of the
process a year in
K.C. Lomonaco, Psy.D., Psychologist, Denver Health Medical CenterAlison Lieberman, Psy.D., Psychologist, Denver Health Medical Center
Collaborative Family Healthcare Association 17th Annual ConferenceOctober 15-17, 2015 Portland, Oregon U.S.A.
Session # C2bOctober 16, 2015
Faculty Disclosure
The presenters of this session:
Have NOT had any relevant financial relationships during the past 12 months.
Learning Assessment
• A learning assessment is required for CE credit.
• A question and answer period will be conducted at the end of this presentation.
Learning Objectives
At the conclusion of this session, the participant will be able to:
• Define the steps necessary for implementing integrated behavioral health in women’s care.
• Describe the role of integrated behavioral health in women’s care clinics.
• Discuss why integrated behavioral health is a perfect fit for women’s care clinics.
References• World Health Organization (2001). World Health Report, 2001. Mental Health: New
Understanding, New Hope.
• Poleshuck, E.L. & Woods, J. (2014). Psychologists Partnering with Obstetricians and Gynecologists: Meeting the Need for Patient-Centered Models of Women’s Health Care Delivery. American Psychologist, Vol. 69, No. 4: 344-354. DOI: 10.1037/aoo36044
• Freed, R.D., Chan, P.T., Dingman Boger, K, & Tompson, M.C. (2012). Enhancing Meternal Depression Recognition in Health Care Settings: A Review of Strategies to Improve Detection, Reduce Barrieres, and Reach Mothers in Need. Families, Systems, & Health, Vol. 30, No. 1: 1-18.
• Baker-Ericzén, M.J., et.al. (2012). A Collaborative Care Telemedicine Intervention
to Overcome Treatment Barriers for Latina Women with Depression During the Perinatal Period. Families, Systems, & Health, Vol 30, No.1, 224-240.
• Chin, J.L., Yee, B.W.K., Banks, M.E. (2014). Women’s Health and Behavioral
Health Issues in Health Care Reform. Journal of Social Work in Disability and Rehabilitation, 13:122-138.
References: •Katon, W.J., et.al. (2010). Collaborative Care for Patients with Depression and Chronic Illness. The New England Journal of Medicine; 363:2611-20.
•Funderbunk, J.S. et.al. (2010). The Description and Evaluation of the Implementation of an Integrated Healthcare Model. Families, Systems, and Health; Vol 28, No.2: 146-160.
•Jarrett, E.M., Yee, B.W.K., & Banks, M.E. (2007). Benefits of Comprehensive Health Care for Improving Health Outcomes in Women. Professional Psychology: Research and Practice; Col 38, No.3; 305-13.
•Baker-Ericzén,M.J., Mueggenborg, M.G., Hartigan, P., Howard, N., Wilke, T. (2008). Partnership for Women’s Health: A New-Age Collaborative Program for Addressing Maternal Depression in the Postpartum Period. Families, Systems, and Health: Vol. 26, No 1., 30-43.
•Adams, Susan M. On The Scene: Integration of Mental Health Services within Ob/Gyn Private Practice: A Collaborative Model. Nursing
•Selix, N.W. and Goyal D., (2015). Postpartum Depression Among Working Women: A Call for Practice and Policy Change. The Journal of Nurse Practioners, Vol 11 (9), 897-902.
Integrated Care at Denver Health
• Population of Denver Health• Growth and change of the
program• Women’s Care Clinic at Denver
Health
Why is integrated care needed in women’s care?
• Referrals to specialty mental health• Limitations of specialty care • Women’s Care IS primary care for many women. The WHO recommended
(2001) that mental health care be moved in to primary care/into the community
• Allows for early screening and treatment for pregnancy related mood/anxiety disorders
• 3300 deliveries per year-about 16% of women with previously diagnosed comorbid mental health disorders
• 1:7 women have chronic pelvic pain during reproductive years• Aging population growing with increase in urogynecological problems
(admittedly more local competition in this area)• Women are the healthcare decision-makers for their households
Barriers to specialty behavioral health
• Why women’s care patients are reluctant to seek behavioral health treatment
• Demystifying the role of behavioral health in integrated care
• Keys to the successful warm handoff in establishing therapeutic alliance
• Improving access, reducing stigma and decreasing barriers to care
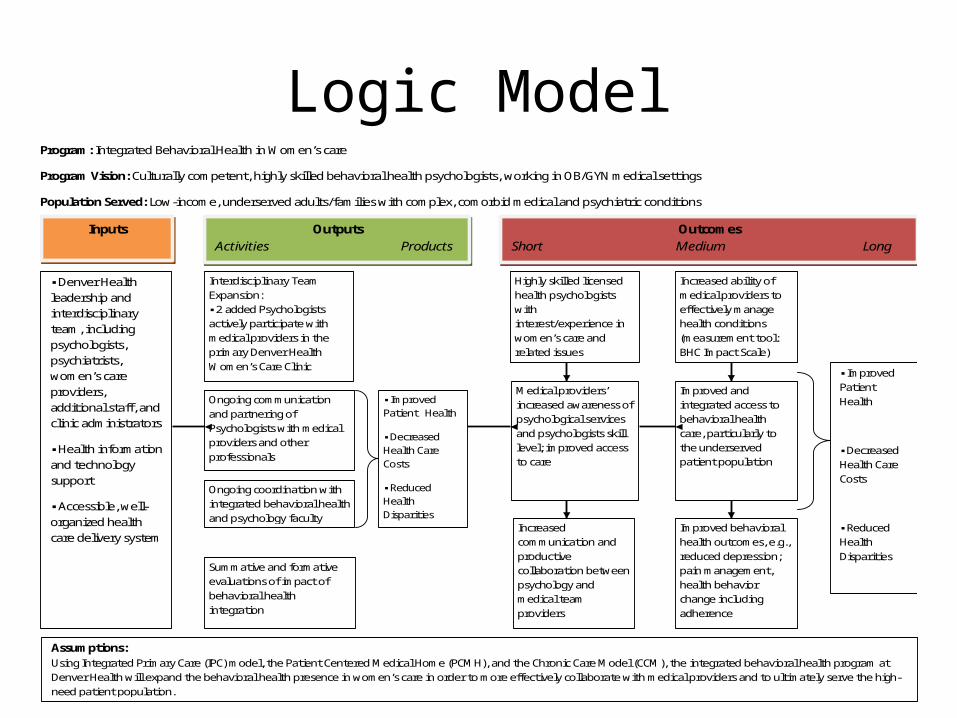
Logic ModelProgram: Integrated Behavioral Health in Women’s care
Program Vision: Culturally competent, highly skilled behavioral health psychologists, working in OB/GYN medical settings
Population Served: Low-income, underserved adults/families with complex, comorbid medical and psychiatric conditions
Inputs
▪ Denver Health leadership and interdisciplinary team, including psychologists, psychiatrists, women’s care providers, additional staff, and clinic administrators
▪ Health information and technology support
▪ Accessible, well-organized health care delivery system
Outputs Activities Products
Interdisciplinary Team Expansion: ▪ 2 added Psychologists actively participate with medical providers in the primary Denver Health Women’s Care Clinic
Ongoing coordination with integrated behavioral health and psychology faculty
Ongoing communication and partnering of Psychologists with medical providers and other professionals
Summative and formative evaluations of impact of behavioral health integration
▪ Improved Patient Health
▪ Decreased Health Care Costs
▪ Reduced Health Disparities
Outcomes
Short Medium Long
Highly skilled licensed health psychologists with interest/experience in women’s care and related issues
Improved behavioral health outcomes, e.g., reduced depression; pain management, health behavior change including adherence
Increased communication and productive collaboration between psychology and medical team providers
Medical providers’ increased awareness of psychological services and psychologists skill level; improved access to care
Improved and integrated access to behavioral health care, particularly to the underserved patient population
Increased ability of medical providers to effectively manage health conditions (measurement tool: BHC Impact Scale)
▪ Improved Patient Health
▪ Decreased Health Care Costs
▪ Reduced Health Disparities
Assumptions: Using Integrated Primary Care (IPC) model, the Patient Centered Medical Home (PCMH), and the Chronic Care Model (CCM), the integrated behavioral health program at Denver Health will expand the behavioral health presence in women’s care in order to more effectively collaborate with medical providers and to ultimately serve the high-need patient population.
Starting from Scratch
• Seeking out institutional support• “Shark tank” – WIPHC at Denver Health• Budget expansion/Grant funding• Have a clinic champion• Allocation of time, space, and resources • Clinician training and focus – OB vs. Gyn
Respect for Cultural Diversity
• Maternal depression can have various meanings across communities
• May affect how women (and fathers) perceive and report symptoms
• Varying opinions about the meanings and cause of sadness across cultures
• Traditional healing practices are often part of the intervention
• Religious communities can support or increase shame and guilt (Dennis & Chung-Lee, 2006).
Screening
•While it is feasible to conduct perinatal depression screenings in primary care settings and OB/GYN clinics, only a small percentage of women are estimated to be screened for depression during pregnancy or in their first year postpartum. ACOG recommendations.
•Marcus et al. found that 20% of pregnant women in obstetric clinics had elevated depressive symptom scores, but only 13.8% of these received any formal treatment for depression.
• Screening for mood/anxiety/trauma in women with chronic health conditions
Benefits of integration
• Improved access to comprehensive care • Unique interactions from multiple disciplines
and providers elicit different perspectives• Mutual support around challenging patients and
team approach to care, reduces provider burnout
• Collaboration/communication to improve patient outcomes
• Improved screening protocols
Implementation
• Four days per week in the women’s care clinic • Divide and conquer-taking all comers • Utilizing areas of expertise/interest• Provide in-service, training for staff • Marketing
AdvertisePsychology available for:
*weight management *smoking cessation*treatment adherence *diagnostic clarification/treatment planning/referrals*GynOnc/end-of-life issues *sleep hygiene*substance use/abuse *crisis intervention/psychosis or acute issues*risk assessment *couples and family issues*mood disorders *chronic disease/chronic pain management*anxiety disorders *resources for housing, OP therapies, substance*grief and loss, fetal demise *triage for psychiatric appointments/consults*perinatal mood and anxiety *transitions to parenting or parenting concerns*postpartum issues *chronic pelvic pain*fertility issues *issues of psychosis*suicidality *health behavior change
What we do
• Collaboration takes multiple forms (curbside, integrated visits, behavioral health visits)
• Screenings/Assessment (psychosocial, cognitive, health behaviors, functional)
• Interventions (short term vs. long term, couples/family, cultural sensitivity, evidence based)
• Additional functions (referrals, case management, etc)
Data
• Numbers: 900+ billable visits (Aug 2014 - July 2015)
• Population: Complicated GYN/OB and multiple psychosocial issues/concerns.
• Provider satisfaction: 90+% say the presence of BH in WCC has improved their satisfaction within their own practice
• Provider utilization frequency • Provider rating of BHC assessment and
interventions
Qualitative Data• Availability of resources to mentally ill patients who are in clinic but
not planning to see a psychologist. • The warm hand off and immediate assessment and ability to
provide more extensive counseling than can be done in the MD visit. • On a daily basis, there is a patient in need of BH services. It is a
significant improvement to quality patient care, to be able to offer this to patients, the very same day, while they are already present in the clinic.
• Having a backup when we have a patient that needs more time and expertise on a behavior health related issue
• Being confident that patients actually get adequate attention for mental health needs that I am not able to provide in limited schedules
Lessons learned one year in
• Infinite need-opening the floodgates• Challenges to the short term model• Challenges in management after pregnancy• High no show rates/low availability• Individual provider variables• Culture of Medicine vs. Psychology• Social work and psychiatric support• Expansion to outside clinics
Session Evaluation
Please complete and return theevaluation form to the classroom
monitor before leaving this session.
Thank you!