Environmental Medical Hazards
38
1 DYPMC Medicine Department Electrical Injuries
-
Upload
dpu-dypmc -
Category
Health & Medicine
-
view
76 -
download
0
description
electricity and heat related
Transcript of Environmental Medical Hazards

1
DYPMCMedicine Department
Electrical InjuriesElectrical Injuries

2
To identify the important complications of electrical injuries.
To expose the pitfalls in diagnosis.To explore the management.
Electrical Injuries Goals

3
Define the population at risk.Determine the factors predicting the severity of
injury.Differentiate between high-voltage and low-
voltage injuries.Recognize which patients require admission or
referral.Decide which patients need cardiac monitoring.
Electrical InjuriesObjectives
Electrical InjuriesObjectives

4
Extent of injury determined by type, amount ,duration and pathway of electric current
Clinical findings alone are unreliable, hence resuscitation MUST be attempted without presuming death
Skin findings are misleading and are not indicative of deeper injury
Essentials of Electrical Injury

5
• Electrical Injuries Are Uncommon
Top 10 Myths of Electrical InjuryMyth #1

6
5X additional patients requiring emergency treatment
3-5% of all burn centre admissions
Bimodal distributionToddlers, Electricians
Electrical InjuriesEpidemiology
Electrical InjuriesEpidemiology

7
• Voltage Is the Most Important Determinant of Injury
Top 10 Myths of Electrical InjuryMyth #2

8
1. V = voltage
2. i = current
3. R = resistance
Electrical InjuriesFactors Determining Severity
Electrical InjuriesFactors Determining Severity
OHM’S LAW: i = V / R

9
Electrical InjuriesFactors Determining Severity
Electrical InjuriesFactors Determining Severity
JOULE’S LAW:
Power (watts) = Energy (Joules) time= V x i= i2 x R

10
Skin Resistivity - Ohms/cm2
100300 - 10 000
1 200 - 1 5002 500
10 000 - 40 000100 000 - 200 000
1 000 000 - 2 000 000
Mucous membranesVascular areas
• volar arm, inner thighWet skin
• Sweat• Bathtub
Other skinSole of footHeavily calloused palm
Electrical Injuries Factors Determining Severity
Electrical Injuries Factors Determining Severity

11
• High Voltage Is More Likely to Kill Than Low Voltage
Top 10 Myths of Electrical InjuryMyth #3

12
A momentary dose of high voltage electricity is not necessarily fatal.
Low voltage is just as likely to kill as high voltage.
Electrical InjuryFactors Determining Severity

13
The Extent of the Surface Burn Determines the Severity of Injury
Top 10 Myths of Electrical InjuryMyth #4

14
• Direct contact– Direct tissue heating
– Contact burns (entry and exit)
– Thermal burns
Electrical InjuriesPatterns of Injury
Electrical InjuriesPatterns of Injury

15
The Pathway the Electrical Current Takes Through the Victim Predicts the Pattern of Injuries
Top 10 Myths of Electrical InjuryMyth #5

16
Skin Resistivity
Least Nerves
Blood
Mucous membranes
Muscle
Intermediate Dry skin
Tendon
Fat
Most Bone
Electrical InjuriesPatterns of Injury
Electrical InjuriesPatterns of Injury

17
1 mAmp Threshold of perception5 mA Maximum harmless current6 mA Ground fault interrupter opens10 mA “Let-go” current20 mA Possible tetany of resp muscles100 mA VF threshold6 A Defibrillation20 A Household circuit breaker
opens
Electrical InjuriesEffects of 60 Hz Current
Electrical InjuriesEffects of 60 Hz Current

18
Electricity Kills by Causing Myocardial Damage
CK and/or Troponin Are Good Markers for Myocardial Damage in Electrical Injury
Top 10 Myths of Electrical InjuryMyth #6

19
All Patients With Electrical Injury Require 24 Hours of Cardiac Monitoring
Top 10 Myths of Electrical InjuryMyth #7

20
• Cardiac monitoring is not justified in ASYMPTOMATIC patients,
• Or, in patients with only CUTANEOUS burns,
• Who had a normal ECG after a 120 v or 240 v injury.
Electrical InjuriesCardiac Monitoring

21
ALL Patients Who Are Asymptomatic and Who Have a Normal ECG After a 120V or 240V Injury Can Be Safely Discharged From the ED
Top 10 Myths of Electrical InjuryMyth #8

22
PregnancyFetal monitoring is
mandatory for pregnant patients
Oral commisure burns Cataracts Delayed neuro-
psychological sequelae
Electrical InjuriesPatterns of Injury
Electrical InjuriesPatterns of Injury

23
Electrical injuries involve multiple body systems.Entry and exit wounds fail to reflect the true
extent of underlying tissue damage.Electrical current may cause injuries distant from
its apparent pathway through the victim.Controversies exist regarding indications for
admission and cardiac monitoring following low voltage injuries.
Electrical InjuriesSummary - The Challenges
Electrical InjuriesSummary - The Challenges

24
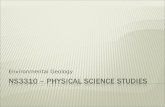
Electric Shock: What Should You Do?
Electric Shock: What Should You Do?The victim:
Felt the currentpass throughhis/her body
The currentpassed through
the heart
Was held by thesource of the
electric current
Lostconsciousness
YesNo
No
No1 secondor more
Yes
No
Yes
Cardiac Monitoring24 hours
Touched a voltagesource of morethan 1 000 volts
Yes
No
Yes

Electric Shock: What Should You Do?
Page 2.
Electric Shock: What Should You Do?
Page 2.Touched a voltage
source of morethan 1 000 volts
Cardiac Monitoring24 hours
Has burn markson his/her
skin
The currentpassed through
the heart
Yes
No
Yes
Yes
Evaluate and treat burns (surgical evaluation,
look for myogolbinuria, etc.)
No
Was thrown fromthe source
Evaluate trauma
No
Is pregnantEvaluate fetal
activity
No
Yes
YesNo
BENIGN SHOCKReassure and discharge
25

26
Hyperthermia results from body’s inability to maintain normal temperature through heat loss
Heat Disorders

27
An unchanged setting of the hypothalamic set point in conjunction with an uncontrolled increase in body temperature that exceeds the body’s ability to lose heat
Hyperthermia

28
An elevation of normal body temperature in conjunction with an increase in the hypothalamic set point
Heat Disorders-Fever

29
Spectrum of diseases- Heat syncope /collapse Heat cramps Heat exhaustion Heat Stroke
Essentials of Heat disorders

30
Heat strokeThermoregulatory failure in association with a warm environment Malignant hyperthermiaHyperthermic and systemic response to halothane and other inhalational anesthetics in patients with genetic abnormality Neuroleptic malignant syndrome
Essentials of Heat disorders

31
Syndrome of hyperthermia, autonomic dysregulation, and extra pyramidal side effects caused by neuroleptic agents (e.g., haloperidol)
Hyperpyrexia-Temperature >41.5°C (>106.7°F)Can occur with severe infections, but more commonly occurs with central nervous system (CNS) haemorrhages or hyperthermia
Heat stroke

32
Salt tablets are not recommended without medical supervision Whole Body cooling methods to be instituted early for rapid
cooling Avoid shivering during cooling---too much cold Know different methods of cooling and their judicious use
according to severity of heat disorder.
Essentials of Heat disorders

33
Clinical Findings Laboratory Findings Treatment Prevention
Heat disorders

34
GeneralAbdomen, CVS, CNSKidney, Liver, MOF
Heat disorders
Clinical symptoms/signs

35
All patients irrespective of severity of manifestations for monitoring/observations
Vitals, Cardiac rhythm, ARDS, infectionKidney parameters, LFT, hypoglycemia, seizures
When to admit to hospital

36
Multi organ failure- CK> 1000 Metabolic acidosis High liver enzymes
Prognosis
Mortality high

37
a core temperature >40.0°Ca core temperature >41.5°Can uncontrolled increase in body temperature de- spite a normal hypothalamic temperature settingan elevated temperature that normalizes with anti- pyretic therapytemperature >40.0°C, rigidity, and autonomic dys- regulation
Q1---Hyperthermia is defined as

38
Immediate therapy should include
intravenous dantrolene sodiumacetaminophenexternal cooling devicesA and CA, B, and C
Q-2 A patient in the intensive care unit develops a temper- ature of 40.8°C, profoundly rigid tone, and hemody- namic shock 2 min after a succinylcholine infusion is started.