ENTC 4350 Ventilators. Sometimes the outcome of the pulmonary function tests may dictate a need for...
102
ENTC 4350 Ventilators
-
Upload
gabriel-knight -
Category
Documents
-
view
215 -
download
1
Transcript of ENTC 4350 Ventilators. Sometimes the outcome of the pulmonary function tests may dictate a need for...

ENTC 4350
Ventilators

Sometimes the outcome of the pulmonary function tests may dictate a need for assisted breathing, which is provided by the use of ventilatory assist devices or respirators. • The most critical test in determining whether a
patient requires respirator therapy is the blood gas situation, particularly regarding oxygen.

Excessive or inadequate CO2 can be compensated by drugs but there is no substitute or compensation for low oxygen levels.

In extreme cases, when the usual methods of oxygen enrichment and ventilatory assistance are inadequate or cannot be used, artificial blood oxygenation may be required.

The techniques of anesthesiology are related to those of ventilatory assistance; • In fact, ventilatory assistance may be required
as the anesthesiologist maintains the surgical patient on that razor’s edge between life and death.

ASSISTED BREATHING
Under normal conditions, breathing is pretty much of an automatic thing. • The rib cage moves outward, the lungs
expand, and air enters the newly opened lung spaces. • Oxygen diffuses through the alveoli into the
blood, and carbon dioxide diffuses out.
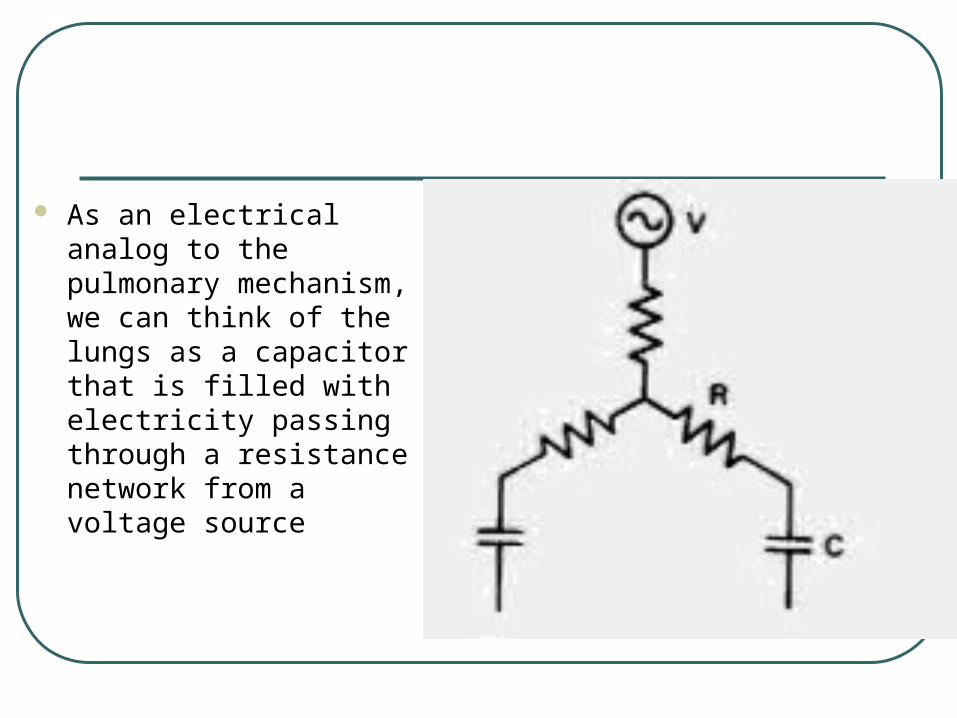
As an electrical analog to the pulmonary mechanism, we can think of the lungs as a capacitor that is filled with electricity passing through a resistance network from a voltage source

The pressure of the atmosphere is analogous to the voltage source or battery, and the nose. mouth, trachea, bronchi, and so on provide the resistances.
• If every thing is normal, the atmosphere provides plenty of pressure, the tracheobronchial tree does not induce significant resistance, and the resuIting system is a low-impedance source that delivers adequate air to the lungs.

If we climb a mountain, the atmospheric pressure drops. • This, in effect, is like weakening the battery or
raising its output impedance. and we feel altitude sickness.

The same thing can occur if the air passages are blocked: the body yells about a shortage of oxygen. • Once again, a system which normally has low
output impedance has been converted to a high-impedance system.

SOURCES OF RESPIRATORY DIFFICULTY Some of the more common problems
include the following:1.Deterioration of lung tissue may interfere with the
gas-exchange processes in the lung.
2. Infection or mucus can obstruct the trachea or bronchial tubes and reduce the air flow through these passages.
3.Neural or muscular control of the nh cage may be impaired.
4.Lung diseases—e.g.. pulmonary fibrosis or pneumonia—may reduce the lung elasticity and produce stiff lung.”

The term compliance is often used in cases of stiff lung, and the thing to remember is that compliance is the opposite of stiffness. • A normal lung has good elasticity, it is
compliant.

A stiff lung is just the opposite. • That is why compliance measurements are an
important guide to patient health.

All these problems are to some extent related to aging, and, as our population grows older, we can expect to see more widespread use of breathing-assist devices.• Problems 1 and 2 are examples of what
happens when the resistance in the circuit goes up; less current flows.

Problems 3and 4 are of a different nature. • In these, the input impedance of the system,
i.e., the lung, increases because the lung cannot expand to the proper volume.

With a transducer or a recorder, high input impedance was what we wanted, but in this case, we must get a maximum quantity of air into the lung to provide for O2 diffusion and CO2 removal.
• The lung as a capacitor has become smaller, and that is bad news. • In terms of our example, pulmonary compliance is
analogous to increased electrical capacitance.

MECHANICAL VENTILATORY ASSIST DEVICES
The objective here is to force air, oxygen or a controlled mixture of the two into the patient’s lungs. • Too little air, or oxygen. will cause lung
deterioration; too much will be just as bad.

The earliest mechanical breathing system was the famous (or infamous) iron lung.* • This boiler-shaped device applied a negative
pressure to the outside of the chest to induce rib cage expansion: it then reversed and applied a positive pressure to compress the lungs and force air out.

A simple (simple to discuss, that is) system of this type can simulate normal breathing for an indefinite period of time.

The older, boiler-type systems had to be provided with glove ports so that the nurses could perform necessary patient services. • They were clumsy, and bedsores were a
continual problem.

The more modern systems are mounted on the chest wall, and in some cases, the patients can sit up or even walk for limited periods of time. • One major problem with many breathing-
assist systems is their need for electrical power. • Any loss of power or other breakdown is
immediately life-threatening.

Some systems have provisions for emergency operation, and it is well to find and practice using them before they are needed. • Frayed and damaged electrical wires or a
smell of hot insulation is a sign that something is definitely wrong.

If you can reach the drive motor on the machine, make it a practice to touch it now and then to get a feeling for its normal temperature.• If the motor seems warmer than usual, it is
time to call the maintenance department.

If your unit has no emergency power supply, you will have to be prepared to ventilate patients by hand (or mouth) in case of power outage. • It is also vital that you know just what alarms
the machine provides for various problems.

The more common breathing-assist units use a mask that fits over the patient’s nose and mouth. • There are two types of machines: the
constant-pressure and the constant-volume units.

The constant-volume or volume-regulated respirator delivers a given volume of air;• The constant-pressure or pressure-regulated
respirator delivers air until a predetermined pressure is reached.
• Both units should allow a measurement of the actual volume delivered and the proper gauges to measure the pressure applied to the lungs.

Both of these systems are triggered by the patient upon inhalation. • Patient inspiration pulls a small vacuum on
one side of a diaphragm;
• The diaphragm then moves and closes a switch to the machine.
• On some units, the switch can be set to trigger on every breath, on every third or fourth breath, or on any breath in which the patient does not inspire a sufficient quantity of air.

If natural breathing stops, the machine will operate continuously at some fixed rate. • For patients who have no normal breathing
reflex, the machine is set to cycle at some 12 to 15 breaths per minute.
Constant-Pressure Machines
The constant-pressure respirator delivers air (or air plus oxygen) to the patient until the pressure reaches some preset level, at which time the pressure is released. • The volume delivered by a constant-pressure
machine will vary with the patient’s position.
Any sputum or other plug in the airway system can stop the machine before it delivers a significant volume of air. • This problem is particularly serious when the
patient resents the machine; the patient can effectively prevent the delivery of air by blocking the flow with his tongue.
In fact, some patients will actually eject the mouthpiece. • An air flow sensor to detect this loss of
contact should be available, and if you have one, test it.
Most sensors are of the heated thermistor type; • If air flow stops they overheat and sound an
alarm.

Another problem with the constant-pressure units is poor control of the oxygen-to-air ratio.
• If the O2 level goes too high, it will result in patient distress.

In most cases, the constant-pressure machines are used for intermittent assistance only. • Regular checking of the oxygen-to-air ratio is
important.
The fact that many constant-pressure machines operate on a purely pneumatic basis from gas bottles and do not need electrical power makes them suitable for use during patient transfer or in situations when the electrical power is uncertain.

Constant-Volume Machines
The constant-volume machine is designed to deliver a preset quantity of air by means of a piston and cylinder. • The machine will, within limits, raise the
pressure as high as is necessary to deliver the proper quantity of air.

Constant-volume systems have the advantage of delivering a known amount of gas regardless of the patient’s position.• Airway obstructions and patient resistance
can be overridden by the constant-volume system, but good drainage must be provided to insure that sputum is not forced down into the lung passages.

Constant-volume systems are more complex than constant-pressure systems, but they allow better control over gas delivery and they are, in general, more suitable for long-term applications.

Most constant-volume units provide a spirometer to allow the nurse to see how much air the patient is taking in on an unassisted breath. • The volume delivered by the machine can
then be adjusted to provide more ventilation if necessary.

Many constant-volume machines have alarms for a variety of emergencies, such as loss of power, mucus blockage, breakage or kinks in the tubing, and so on.
• If you turn off the alarms while aspirating the patient, be sure to turn them on again when the machine is reactivated. • Failure to do this has resulted in some nasty accidents.
0ther Features of Breathing-Assistance Systems
There are other breathing-assistance systems that provide positive pressure during the patient’s normal inspiration. • In many cases, the added air or oxygen can
serve as a carrier for water vapor or for drugs dispersed by means of a nebulizer.

Some dispute exists about the value of intermittent positive-pressure breathing (IPPB) systems and their use should be controlled by the policy of the hospital. • Some patients use positive-pressure units for
home therapy, and again, the rationale for this is the physician’s decision.

Another factor in the employment of breathing-assistance systems is the use of differential inspiration-expiration periods. • Usually, the time allowed for expiration is
twice that allowed for inspiration.

This additional time is needed for the patient’s muscular system to exhale the air that the constant-volume or constant-pressure machine has forced into the lungs.
A feature of these systems is the application of periodic, extra large breaths. • This procedure is called “sighing the patient.”

Sighing is thought to be necessary to prevent deterioration of the lung tissue, which may lead to atelectasis. • The exact mechanism of atelectasis is not yet
under- stood, and there are various opinions about the need for sighing.

We suggest you consult a local pulmonary specialist if the question arises.

A. Power source
B. Electric blower
C. Inspiratory flow rate control
D. Delivery tube from blower to plastic cylinder
E. Inlet valve to plastic cylinder
F. Outlet valve from plastic cylinder
G. Sensitivity control
H. Inspiratory signal lamp
J. Inlet valve to bellows
K. Outlet valve from bellows
M. Rubber bellows
N. Plastic cylinder
P. Humidifier chamber
R. Foam of bubbles
S. Heater with thermoswltch
T. Non-rebreathing valve
W. Patient connection

Some breathing-assistance machines maintain a small positive pressure on the patient’s respiratory system at all times. • This is called positive-expiratory pressure
(PEP), and it seems to be an important factor in weaning the patient off the respiratory-assist system.
The proper pressure level (about 25 mm Hg) should not be exceeded; • Too great a pressure would excessively
increase the work of exhalation.
Oxygen Enrichment Methods and Problems
Many machines provide facilities for oxygen enrichment and humidification as necessary.
• If significant quantities of O2 are used, humidification is always necessary.

Humidity plays an important role in loosening sputum.

When O2 is used with assisted breathing, the apparatus for controlling the mixture of O2 and air should be carefully checked. • Just because the mixer worked last year does
not mean it will work tomorrow.
• Some systems use an O2 sensor, whereas others mix predetermined volumes of O2 and air.

Excessive O2 can be dangerous, especially to the newborn. • It is worth emphasizing the hazard of
excessive O2 :
• Experiments with normal individuals indicate that an O2 level of 35% to 55% can be tolerated indefinitely, but with 100% O2 severe pain and respiratory disturbances occur after 6 to 30 hours of exposure.

If your breathing-assistance machine is driven by compressed O2 with a venturi for air mixture, there is no way of knowing exactly what the O2-to-air ratio is.
• In many cases where compressed O2 was used to drive the machine, the gas inhaled by the patient was found to be over 40% O2 .

This suggests that compressed air should be used to drive the machine and the O2 be added as necessary.
• Periodic checks with an O2 analyzer might well be in order.

Weaning the Patient from the Machine
This becomes a problem whenever the patient gets ‘lazy” and does not put out enough effort to breathe without the machine. • In this case, you have to be kind but firm and
adjust the machine so that it only triggers on every third or fourth breath.

Some machines can be set to trigger only if the patient fails to inspire enough air. • In many cases, the machine is simply
disconnected and the patient is encouraged, or forced, to walk about.

Humidity Control
As ambient air enters the nasal passages, it is humidified to avoid drying the trachea and lung tissue. • Under normal circumstances, the nasal
passages produce an adequate amount of moisture to handle the driest of air.

This may not be the case when assisted breathing is employed, because commercial bottled air or O2 is sold in “bone dry” condition to avoid condensation and rusting of the tanks. • If a patient is to breathe bottled gas for any
period of time, it should be humidified with a bubbler to avoid excessive drying of nasal tissue.

Role of Carbon Dioxide
Carbon dioxide displays an interesting aspect of lung physiology in that the air entering the lungs must have a low level of CO2 (below 1%) in order for the CO2 to diffuse out of the blood.
• If the CO2 level rises above 2%, or about 10 mm Hg, there will be changes in the patient’s behavior.

At the 3% level, the disturbance is severe, and stupor and death ensue at the 6% CO2 level.
• This dramatic effect of CO2 is due to the direct influence of this gas on respiration and heart rate.

An increase in the CO2 level in the lungs is a signal to the body that a more rapid metabolic rate is required.
• This allows CO2 to be used as a respiratory stimulant, but only up to a point.

If the CO2 level goes above about 4%, there will be patient distress, regardless of how much O2 is available.

The CO2 level is one reason why medical gases are handled differently than the gases used for welding.
• If a tank of welding oxygen is 3% CO2, the buyer might get a lower price, and the gas would be quite suitable for welding.
In hospital use, however, this could be a tragedy. • Other impurities that are kept out of
‘breathing-grade’ gases are oil vapor (because it causes lung problems) and carbon monoxide.
• The effects of carbon-monoxide poisoning are so serious and so well known that no discussion is necessary.
The fact that CO2 normally stimulates the respiratory process is the basis for the tendency to use CO2 whenever there is depression of the respiratory process. • The danger here is that such patients are
already suffering from excess CO2 or hypercapnia, and the respiratory control center has become immune to this stimulus.

At this point, the lack of O2, or hypoxia, is the only thing that maintains the breathing process.
• Administration of CO2 will not be of any help, because the response center is already saturated, and the sudden admission of high concentrations of O2 is equally dangerous, because it will remove the only stimulus for breathing (hypoxia) and respiration will cease.

Patients with hypercapnia, or, as it is sometimes called, carbon-dioxide narcosis, must be brought out very carefully.
• Excessive loss of CO2, or hypocapnia, may be due to a variety of factors associated with hyperventilation.
In this case, CO2 is administered in spite of the fact that it is usually considered a respiratory stimulus.
The patient’s blood level of CO2 must be raised to the proper level, and this is usually best done by CO2 administration.

The point is that the effects of CO2 are not necessarily simple, and when dealing with problems of ventilation, both thought and knowledge are needed.

BLOOD OXYGENATION SYSTEMS
We know that oxygen is carried by the blood to various parts of the body.
• The carrier system for O2 involves the formation of a chemical compound, oxyhemoglobin, which serves as the actual transport medium in the blood.

When there is severe impairment or failure of the blood-gas exchange that normally occurs in the lungs, a blood oxygenation machine can be used.
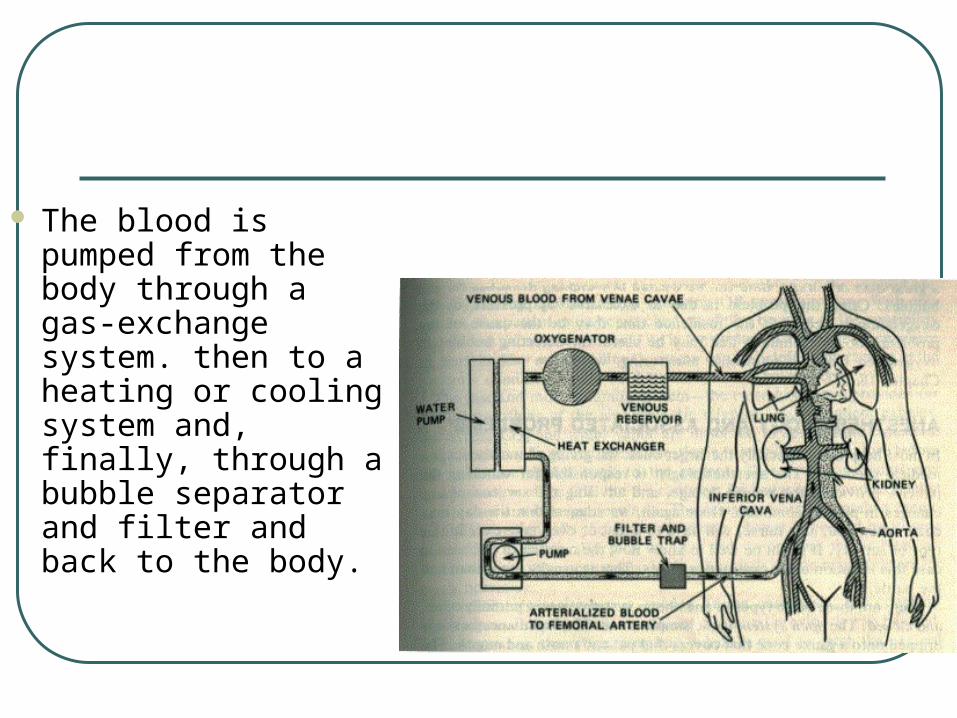
The blood is pumped from the body through a gas-exchange system. then to a heating or cooling system and, finally, through a bubble separator and filter and back to the body.

The gas-exchange system provides for diffusion of O2 into the blood to produce oxyhemoglobin.
• It must also encourage CO2 (carbon dioxide) and CO to diffuse out of the blood.

These processes can be accomplished by bubbling air—or more commonly, oxygen—through the blood while at the same time rotating a series of discs in the blood to increase the contact area between the gas and the blood. • In some systems, a complex of narrow
passages is produced by a membrane system.

The membrane (a special plastic) permits O2 to diffuse into the blood while allowing CO and CO2 to diffuse out.
The Bubble Problem
The main problem with blood oxygenation systems is that O2 can enter the blood as a solution of a gas in a liquid. • The danger of this gas-in-solution business is
that the gas can come back out of solution and appear as bubbles.
If the gas bubbles at the wrong time (e.g., after the blood has returned to the patient), there will be dire consequences.

The physics of the bubble problem depends upon two effects:1. Frothing of the blood in the gas-exchange
system. • This produces large bubbles that are easily
removed by the usual bubble separation system.
2. True solution problems based on the effects of Henry’s law. This is by far the most serious problem.

Henry’s law states that the quantity of gas that dissolves in a fluid goes up as a function of the gas pressure in the system. • In the older blood oxygenation systems, the
O2 pressure was held at a value that was high enough to insure the rapid diffusion of O2, but this meant that there was some dissolution of O2 in the blood.

If the pressure was reduced even slightly, O2 could come back out as bubbles, like removing the cap from a bottle of soda. • This problem could be compounded if the
blood is cooled before it enters the oxygenation system, as, say, in hypothermic therapy.

Gases are more soluble in cooled blood, but they tend to come out of solution when the blood warms up. • Boiled water tastes ‘flat” because it has no air
dissolved in it.

The blood oxygenation system always includes a bubble and froth remover, but it might not always get all the dissolved gas out. • If this unit is inadequate, • If the blood is too cold, • If the residence time (i.e., the time the blood
spends in the oxygenator) is too short, or • If the O2 pressure in the oxygenator is too high,
The bubbles will then reappear after the blood has entered the connecting tubes or, worse yet, the patient’s body.

This has led to be a severe problem with many blood oxygenation systems.• A useful technique for detecting bubbles in
oxygenated blood is ultrasonic monitoring.
ANESTHESIOLOGY AND ASSOCIATED PROBLEMS
In most hospitals, the giving of anesthetics is a medical specialty. • The anesthesiologist is responsible for
watching the patient, providing the proper dosage, and advising the surgeon of any changes in patient condition.

There are three basic types of anesthesia systems: • open,
• partially open, and
• closed.
The open system is the simplest one. • The liquid anesthetic is dripped onto a gauze
cone that covers that patient’s nose and mouth.
• The anesthetic vaporizes and is mixed with the air that enters the patients lungs.
One advantage of this system is its insensitivity to excessive use of anesthetic; • It is almost impossible to give the patient too
much.
The disadvantages are • The need for excessive quantities of
anesthetic,
• Contamination of the operating room, and
• Possible fire or explosion hazards if ether is used.
The partially open system is really a generic term for several kinds of apparatus. • In most units, the anesthetic gases are
provided in a bag reservoir so that they do not mix with air.
As the patient breathes, he or she receives a controlled mixture of air and anesthetic.
• In some cases, the air will be enriched with O2 or c to assist the patient’s respiration processes.
• If bottled gases are used, appropriate humidification is necessary to avoid patient injury.

This system makes it convenient to use gases that are not liquids at room temperature.• You would have great difficulty in dosing a
patient with a gas like halothane via a nose cone.
The partially open systems allow the gas mixture that leaves the patient’s lung to exhaust into the operating room. • This provides for good control of the patients
CO2 level, but there is some contamination of the OR.

Some machines provide for partial rebreathing of the expired air, thereby saving anesthetic and reducing OR contamination. • With this system, the patient must be watched
carefully, because of the possibility that excess anesthetic will build up in the system.
This is one place where an ear Oximeter or indwelling O2 sensor can be helpful;
• Any change in the patient’s condition would be detected almost immediately.

The last and most common system—the closed system—provides for 100% rebreathing of the air-anesthetic mixture.
• As the patient exhales, the excess CO2 and water vapor are absorbed in appropriate canisters.
Any necessary O2 or additional anesthetic is added to the mixture before the gases are cycled back to the patient. • This system prevents any contamination of
the OR, but the canisters for water vapor and CO2 must be watched and changed regularly.

The canisters usually contain a chemical indicator that tells the operator when a change is needed by turning color.
• The canisters also pick up CO2 and water from the ambient air whenever they have been opened.
• Most hospitals put on new canisters for every operation.

If ventilatory assistance is needed during anesthesia, the constant-volume or constant-pressure machines discussed previously can be used. • In emergencies, the rebreathing bag, which is
used to catch the expired gas, can be used to ventilate the patient;
• The operator periodically squeezes and then lets go of the bag.
This activates the absorption and supply system, and it allows patient maintenance in case of machine failure.

Improper gas mixtures must be watched for, because many anesthesia systems do not have integral gas analyzers. • You just have to adjust the appropriate
flowmeters and observe the patient’s condition.