ENT Update for General Practice - Parkside Hospital Tweedie... · Paediatric ENT Update for General...
48
Paediatric ENT Update for General Practice PPG Mr Daniel Tweedie MA FRCS(ORL-NHS) DCH Consultant Paediatric ENT, Head and Neck Surgeon Evelina London Children’s Hospital
Transcript of ENT Update for General Practice - Parkside Hospital Tweedie... · Paediatric ENT Update for General...

Paediatric ENT Update for General Practice PPG
Mr Daniel Tweedie MA FRCS(ORL-NHS) DCH
Consultant Paediatric ENT, Head and Neck Surgeon
Evelina London Children’s Hospital

Evelina London Children’s Hospital
• Dedicated tertiary paediatric hospital in central London
(St Thomas’ site)
• Completed in 2004
• Built around children’s requirements
• State of the art facilities
• Innovative management
Paediatric ENT Service
• Five consultants
• Among the largest specialist children’s ENT units in the UK
• All aspects of paediatric ENT
• Very large airway practice
• Excellent links with adult ENT and other specialities
My practice
• Trained in SW Thames, fellowship training at Great Ormond Street Hospital
• All aspects of paediatric ENT- including airway, otology and head and neck surgery
• Training programme director for South London
• Council member of BAPO and Children’s Surgical Forum at the Royal College of Surgeons
• Individualised patient care
• Latest evidence-based management and techniques
Today’s objectives
• Clinical scenarios in paediatric ENT
• Common problems
• Diagnosis and management
• Interactive
• Question and answer opportunities

Scenario 1

Obstructive sleep apnoea in children
• Very common
• 12-15% snore
• 2% have OSA
• ≡ 15000 cases/year in UK
• Major public health problem
• Greatly under-recognised
• Treatment delays common

Causes of OSA in children
• Large tonsils and adenoids
• Adenoids more so in infants
• Other factors: ethnicity, C-F geometry, obesity, syndromes, poor tone
• Also consider rarer cases of central apnoeas- in some syndromes, +/- neurological or developmental delay
Clinical effects of OSA in children
• Not necessarily as for adults: more variable
• Tiredness and lethargy or may be hyperactive • Neurocognitive impairment/ ↓ IQ • Poor concentration • Poor appetite, poor weight gain • Cardiopulmonary effects
• Many of these are reversible with prompt
treatment
Diagnosis (1)
• Not always easy
• May be obvious from history- but may not be • Snoring, apnoeas despite respiratory effort • Head-extended position, mouth open • Restlessness, frequent waking, bed wetting etc • Daytime effects
• But parental history not always reliable- anecdotally low
negative predictive value • Size of tonsils and adenoids not always predictive

Diagnosis (2)
• History and clinical examination- accepting limitations
• Sleep study- recorded domiciliary SaO2*
• Very fast turnaround at Evelina sleep centre
• One stop pick up; posted back; results in 5 days
• Polysomnography: gold standard, selected cases only
Treatment of childhood OSA
• Adenoidectomy
• Tonsillectomy
• Generally curative, some have residual or recurrent symptoms
• Other options including CPAP, and tracheostomy (rarely)
Scenario 2

Tonsillitis
• Very common
• Often viral
• Sometimes bacterial
• Glandular fever
• Management options

Tonsillitis: viral or bacterial? • Centor criteria- score out of 5 • Likelihood of group A Streptococcal pharyngitis
1. Fever 2. Tonsil exudates 3. Anterior cervical lymphadenopathy 4. Absence of cough 5. Age <16 add 1 point; age >44 subtract 1 point
All 4: PPV 40-60% for Group A Strep None: NPV 80% Original study in adults- ? applicability to children

Tonsillitis: management
• Management according to the SIGN guidelines 2010
• Severe attacks: emergency referral
• No routine throat swabs
• Simple analgesia
• Antibiotics according to clinical picture (Centor)
• Penicillin V QDS for 10 days
Recurrent tonsillitis
• SIGN recommendations
• Empirical treatment of each episode
• No great evidence for prophylactic antibiotics*
• Tonsillectomy if severe
• 7 attacks/ 1year; 5 attacks per year for 2 years; 3 attacks per year for 3 years
• Additional clinical judgement

Tonsillectomy
• Ancient procedure • Numerous methods • Traditionally extracapsular • Cauterisation → thermal injury • Muscle exposed → painful • Vessels exposed → risk of bleeding
• High rates of delayed discharge, readmission and
post-operative haemorrhage (3-5%) • Mortality risk
Coblation® intracapsular tonsillectomy
• An alternative approach
• Cold radiofrequency ablation 40-50°C
• Dissection within the tonsil capsule
• Underlying muscle and vessels not exposed

Coblation® intracapsular tonsillectomy

Experience at Evelina • Largest prospective series in the
UK • >430 cases since Spring 2013 • All children: OSA and/or tonsillitis
• Very rapid recovery: 5-6 days • Minimal analgesia • No phone calls from parents • No readmissions with pain • 2 cases of bleeding (0.47%) • Symptomatic improvement • Excellent feedback: > 99% of
parents would recommend
Scenario 3

Acute otitis media
• Commonest reason for under-5s to see their GP (70% affected by 2 years)
• Similar risk factors to glue ear- age, winter, male sex, family history, reflux
Plus: low birth weight, poor immunity (incl. PCV), dummy use, bottle feeding

AOM: pathophysiology
• Viral URTIs- 15-20/year in young children • Generalised mucosal inflammation • Impaired mucociliary clearance • Short, horizontal Eustachian tubes- may allow
bacterial ingress • Limited immunity
• Bacterial supra-infection is common following
initial viral infection • Pneumococcus, Haemophilus, Moraxella
AOM: diagnosis
• Not always easy
• Variable history, especially in younger children (may not be febrile or in pain, may or may not have discharge)
• “Softer” symptoms, eg reduced appetite and play, restlessness at night etc
• Difficult otoscopic view +/- crying-induced vasodilatation of tympanic vessels

AOM: management
• 2013 AAP guidelines • Single episodes • Recurrent AOM • Antibiotics • Grommets • Other measures
• Some differences vs equivalent Cochrane
recommendations • NICE CKS available (2009) but not formal guidelines-
similar to AAP

Single episodes of AOM
• Supportive measures: fluids, rest, regular analgesia (ibuprofen > paracetamol)
• Low threshold for admission of very young or toxic children
• Immediate or delayed antibiotic prescribing policy (see again at 24-48 hours)
• Consider early antibiotics for certain cases: 3 months or younger, symptoms >4 days, bilateral infection in under 2s, perforation and discharge, comorbidities

Benefits of antibiotics
• Reduced mean duration of symptoms by a small amount
• Reduced risk of complications eg mastoiditis, meningitis etc

Which antibiotic?
• Both AAP and NICE recommend amoxilicillin as first line (clarithromycin or erythromycin if allergic)
• No consensus regarding duration (?5-10 days)
• Consider co-amoxiclav or cefuroxime in resistant cases- expect improvement by 48-72 hours

What dose of amoxicillin?
• NICE: 40mg/kg/day in divided doses for 5 days (ie 13mg/kg TDS)
• But evidence from US CDC supports 80-90mg/kg/day, given high prevalence of resistant organisms
• Consider doubling the dose

Recurrent AOM
• AAP- 3 or more episodes in six months, or four in a year, with at least one in the past six months
• Particular risk factors:
First infection < 3 months of age
Persistent previous AOM > 10 days
Winter months
Male gender
Passive smoking

Recurrent AOM- management
• Manage each episode
• Wait for resolution with time
• Address reversible risk factors (incl.PCV)
• Prophylactic measures
Recurrent AOM- prophylaxis
• Antibiotics- limited evidence to support low dose prophylaxis. Cochrane review mildly supportive, AAP does not recommend
• Options include trimethoprim (1-2mg/kg nocte), amoxicillin or azithromycin (10mg/kg M,Tu,W then off for 11 days)
• Grommets- more evidence to support these, but risks of persistent discharge and permanent perforation
• No evidence to support adenoidectomy

Complications of AOM
• Outer ear- otitis externa • Middle ear- perforation, ossicular
erosion, tympanosclerosis, adhesions, facial palsy
• Inner ear- toxicity to cochlea and labyrinth
• Intratemporal- mastoiditis • Press on the cymba conchae • Intracranial- meningitis, abscess,
venous sinus thrombosis

Scenario 4
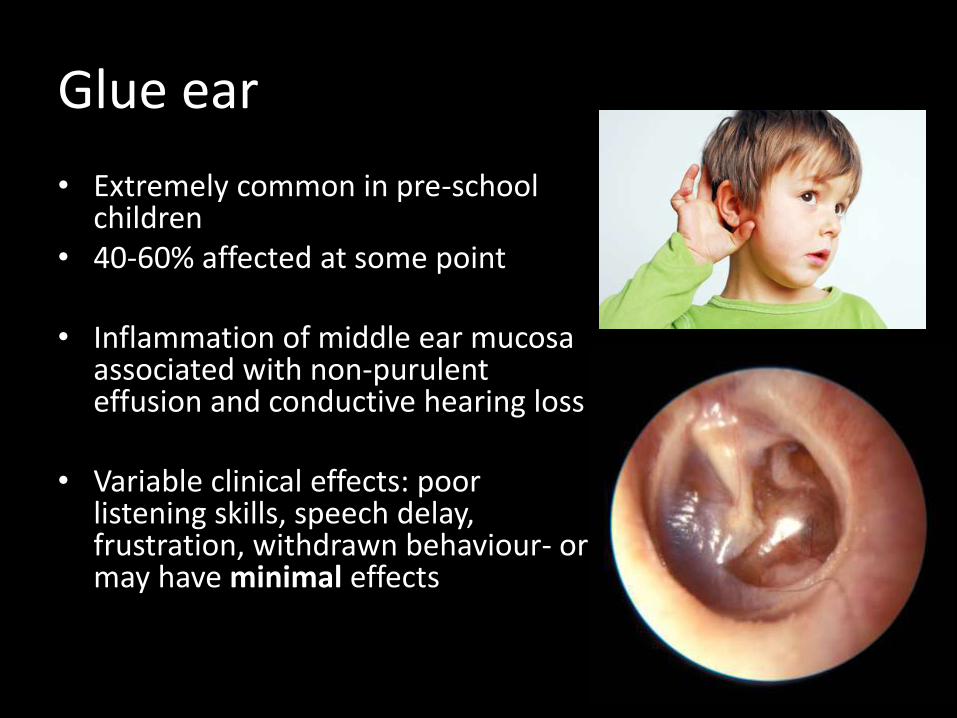
Glue ear
• Extremely common in pre-school children
• 40-60% affected at some point
• Inflammation of middle ear mucosa associated with non-purulent effusion and conductive hearing loss
• Variable clinical effects: poor listening skills, speech delay, frustration, withdrawn behaviour- or may have minimal effects

Glue ear- risk factors
• Individual
• Age- peaks at 2 and 5
• Male sex
• Family history
• Nasal allergy/ adenoiditis
• Reflux
• Environmental
• Winter months
• Passive smoking
• Daycare with >4 children
Glue ear- management framework
• Nice guidelines 2008
• Generally evidence based
• Some limitations

Glue ear-diagnosis
• Clinical suspicion
• Otoscopic examination
• Tympanometry
• Audiometry

Free field audiometry

Hearing tests for children
Visual reinforcement Toy test Conditioned play

Glue ear- general steps
• Maximise listening opportunities
• School or nursery should be aware
• Care with crossing road etc
• Parental advice and reassurance
• Benign condition
• Active monitoring in the first instance- 3 months
• Short/medium term sequelae, less likely to produce long term problems

Glue ear- autoinflation
• Either self-valsalva or using Otovent® balloon
• Not easy for younger children
• Some evidence to support use in parallel with active monitoring (Cochrane)
• Can be prescribed, or available online for about £6-8

Glue ear- after 3 months
• Options include further active monitoring • Particularly if parents are happy and child is doing
well
• Hearing aids- no complications, effective increase in volume with normal underlying sensorineural hearing (especially those with cleft palate or Down’s syndrome)
• Surgery- grommets +/- adenoidectomy • Other measures eg steroids, antibiotics,
osteopathy etc- not recommended by NICE

Grommets
• Reasonable option for hearing loss 25-30dB in the better hearing ear for 3 months
• Remain in situ for 6-18 months before extruding
• Consider adenoidectomy: prolongs benefits of grommets

Grommets- problems
• Limited duration of benefit ≈ 6-8 months on average
• Adenoidectomy at the same time is known to prolong the beneficial effects of grommets
• Difficult to demonstrate long-term benefits of surgical intervention for glue ear
• Risks of recurrence, discharge (5-10%) and persistent perforation (1-2%)

Grommets FAQs/ answers
• OK to swim after 6 weeks- no proven benefit of keeping the ears dry
• Avoid immersion in bath water + avoid diving deep under water
• Treat discharge with water precautions +/- topical medication
• OK to use antibiotic drops if the ear is infected- I tend to use ciprofloxacin eye drops: 3 drops BD for 10 days

Thank you
• ENT patient information and resources for doctors at danieltweedie.com