Enlarging tongue mass
4
J Oral Maxillofac Surg 56224-227, 1998 Enlarging Tongue Mass William Nelson, DDS, * Thomas Chuprevich, DO, f and David A. Galbraith, DMD$ Case Presentation A 37-year-old white man was referred for evaluation of a right-sided tongue mass that had been present for over 10 years. Significant enlargement had been noticed during the 12 weeks before presentation. He denied pain, dysgeusia, dysphagia, or neurosensory disturbance. The patient was in good health; he was taking no medications and denied any allergies. Oral examination showed a 3.0 X 3.0 X 3.0 cm mass in the anterior right tongue (Fig 1). With the exception of lateral leukoplakic change, the tongue mucosa was intact and normal in color. The mass was very firm, circumscribed, and nonpainful to palpation. It encompassed the dorsal, lateral, and ventral surfaces of the tongue without involve- ment of the floor of the mouth. There were no neuromuscu- lar or neurosensory deficits noted. The remainder of the physical examination and review of systems was unremark- able and the social history was noncontributory. The neck was without lymphadenopathy. An incisional biopsy was performed under local anesthe- sia. Differential Diagnosis David M. Galbraith, DMD In this case, a lateral tongue masshas been present for over 10 years with significant enlargement over the preceding 12 weeks. The overlying mucosa ap- pears to be intact, which may indicate this lesion is related to deeper structures. The superficial leukopla- kit changes are probably related to trauma from the adjacent teeth. When one considers masses that have been present for long periods, benign soft tissue neoplasmsand reactive lesions need to be considered. The significant enlargement of this mass over the past 3 months could indicate a more aggressive lesion; *Private practice, Green Bay, WI. ‘ichief, Department of Pathology, St Vincent Hospital, Green Bay, WI. *Private practice, Farmington, CT. Address correspondence and reprint requests to Dr Nelson: 704 S Webster Ave, Green Bay, WI 54301. o 1998 American Association of Oral and Maxillofacial Surgeons 0278.2391/98/56021)020$3.00/O however, this is unlikely because of a lack of neurosen- sory or mucosal changes. When one considers benign masses in the tongue, one must consider tumors of neural origin high in the differential diagnosis. Neurolemoma or schwannoma, a benign neoplasm of Schwann cell origin, is a slow-growing encapsulated mass that is typically asymptomatic. The most common location is the tongue; however, it can be found anywhere in the oral cavity. Typically these lesions are more common in adults, but they can be seen throughout a wide age range. Schwannomas can range in size from a few millimeters to several centimeters, and a sudden increase in size can be seen in these lesions, which is believed to be due to intralesional hemorrhage. The lesion in this case fits the description of a neurole- moma. Neurofibroma is a peripheral nerve neoplasm that arises from a mixture of cell types, including Schwann cells and perineural fibroblasts. A solitary neurofi- broma can present at any age as a slow-growing, soft, painless submucosal mass. The tongue, buccal mu- cosa, and vestibule are the more common locations, and the lesion can range in size from a small nodule to a large mass. The granular cell tumor is an uncommon benign neoplasm that shows a predilection for the oral cavity. Originally this lesion was thought to be derived from skeletal muscle and was called granular cell myoblas- toma. Now, more recent investigations point to the origin from the Schwann cell or an undifferentiated mesenchymal cell. Half of the reported cases occur on the tongue, and they most often involve the dorsal surface. These lesions typically are found in adults but can be seen at any age. They usually occur as an asymptomatic, sessilenodule that has been present for many months or years. For a massalong the lateral border of the tongue, an irritation fibroma should be included in the differential diagnosis. These are typically firm, sessile masses,and are found in areas of repeated trauma. The labial mucosa, tongue, and gingiva are common sites. The lesions can range in size from several millimeters to several centimeters. In some cases, the surface may appear white as a result of hyperkera- 224
-
Upload
william-nelson -
Category
Documents
-
view
219 -
download
0
Transcript of Enlarging tongue mass

J Oral Maxillofac Surg 56224-227, 1998
Enlarging Tongue Mass
William Nelson, DDS, * Thomas Chuprevich, DO, f
and David A. Galbraith, DMD$
Case Presentation
A 37-year-old white man was referred for evaluation of a right-sided tongue mass that had been present for over 10 years. Significant enlargement had been noticed during the 12 weeks before presentation. He denied pain, dysgeusia, dysphagia, or neurosensory disturbance. The patient was in good health; he was taking no medications and denied any allergies.
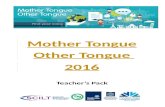
Oral examination showed a 3.0 X 3.0 X 3.0 cm mass in the anterior right tongue (Fig 1). With the exception of lateral leukoplakic change, the tongue mucosa was intact and normal in color. The mass was very firm, circumscribed, and nonpainful to palpation. It encompassed the dorsal, lateral, and ventral surfaces of the tongue without involve- ment of the floor of the mouth. There were no neuromuscu- lar or neurosensory deficits noted. The remainder of the physical examination and review of systems was unremark- able and the social history was noncontributory. The neck was without lymphadenopathy.
An incisional biopsy was performed under local anesthe- sia.
Differential Diagnosis
David M. Galbraith, DMD In this case, a lateral tongue mass has been present
for over 10 years with significant enlargement over the preceding 12 weeks. The overlying mucosa ap- pears to be intact, which may indicate this lesion is related to deeper structures. The superficial leukopla- kit changes are probably related to trauma from the adjacent teeth. When one considers masses that have been present for long periods, benign soft tissue neoplasms and reactive lesions need to be considered. The significant enlargement of this mass over the past 3 months could indicate a more aggressive lesion;
*Private practice, Green Bay, WI.
‘ichief, Department of Pathology, St Vincent Hospital, Green Bay,
WI.
*Private practice, Farmington, CT.
Address correspondence and reprint requests to Dr Nelson: 704 S
Webster Ave, Green Bay, WI 54301.
o 1998 American Association of Oral and Maxillofacial Surgeons
0278.2391/98/56021)020$3.00/O
however, this is unlikely because of a lack of neurosen- sory or mucosal changes.
When one considers benign masses in the tongue, one must consider tumors of neural origin high in the differential diagnosis. Neurolemoma or schwannoma, a benign neoplasm of Schwann cell origin, is a slow-growing encapsulated mass that is typically asymptomatic. The most common location is the tongue; however, it can be found anywhere in the oral cavity. Typically these lesions are more common in adults, but they can be seen throughout a wide age range. Schwannomas can range in size from a few millimeters to several centimeters, and a sudden increase in size can be seen in these lesions, which is believed to be due to intralesional hemorrhage. The lesion in this case fits the description of a neurole- moma.
Neurofibroma is a peripheral nerve neoplasm that arises from a mixture of cell types, including Schwann cells and perineural fibroblasts. A solitary neurofi- broma can present at any age as a slow-growing, soft, painless submucosal mass. The tongue, buccal mu- cosa, and vestibule are the more common locations, and the lesion can range in size from a small nodule to a large mass.
The granular cell tumor is an uncommon benign neoplasm that shows a predilection for the oral cavity. Originally this lesion was thought to be derived from skeletal muscle and was called granular cell myoblas- toma. Now, more recent investigations point to the origin from the Schwann cell or an undifferentiated mesenchymal cell. Half of the reported cases occur on the tongue, and they most often involve the dorsal surface. These lesions typically are found in adults but can be seen at any age. They usually occur as an asymptomatic, sessile nodule that has been present for many months or years.
For a mass along the lateral border of the tongue, an irritation fibroma should be included in the differential diagnosis. These are typically firm, sessile masses, and are found in areas of repeated trauma. The labial mucosa, tongue, and gingiva are common sites. The lesions can range in size from several millimeters to several centimeters. In some cases, the surface may appear white as a result of hyperkera-
224

NELSON, CHUPREVICH, AND GALBRAITH 225
In summary, the following list of differential diag- noses, in order of consideration, should be considered in this patient:
1. Schwannoma or neurolemoma 2. Neurofibroma 3. Granular cell tumor 4. Irritation fibroma 5. Hemangioma or lymphangioma
FIGURE 1. View of the right tongue mass
tosis from continued irritation. Irritation fibromas are most common in the fourth to sixth decades of life.
Soft tissue tumors of muscle origin should also be included. Leiomyornas are rare in the oral cavity. They are thought to be of vascular smooth muscle origin and present as a slow-growing, firm nodule. Solid leiomyomas are usually normal in color, and can be found in the tongue, palate, lips, and cheek. Rhabdomyomas are benign neoplasms of skeletal muscle, which are extremely rare in the tongue, even though it has a large skeletal muscle component. Adult rhabdomyomas are most commonly found in the base of tongue and usually appear as an ill-defined mass.
A differential of tongue lesions would not be com- plete without at least mentioning hemangiomas and lymphangiomas. These lesions can present as a pain- less mass in the tongue, although more often they appear as a superficial lesion with a pebbly surface. However, deeper tumors of this kind present as a soft, ill-defined mass. They can range in color from lighter than the surrounding tissue to a red-blue hue. The tongue is a common site for the lymphangioma, which occurs typically in the anterior two thirds. These tumors most often develop early in life, before the age of 20.
The Zipoma is a benign soft tissue tumor of fat. Although rare in the oral cavity and unlikely in this case, it can present as a smooth-surfaced, nodular mass. The buccal mucosa is the most common loca- tion, but it can also occur in the floor of mouth and tongue. Most cases occur in patients of 40 years old or younger.
k$!ammatory/reactive lesions, such as the pyo- genie granuloma, can occur along the lateral tongue as a result of trauma. However, these lesions are usually smaller, more inflamed, and painful. Malignant neo- plasms have not been included in the differential diagnosis, considering the likelihood that they would present with a shorter history and a more aggressive behavior.
SUBSEQUENT CLINICAL COURSE
Grossly, the biopsy specimen showed firm, glisten- ing, yellowish-white tissue with apparent pseudoen- capsulation. Microscopically, the specimen consisted of adipose tissue exhibiting significant morphologic variation in the lipocytes (Fig 2). Bizzare nuclear and multinucleated varieties were observed, and occa- sional lipoblasts were encountered. Mitotic activity was not seen. Areas of collagenous infiltration were noted (Fig 3). The S-100 protein stain was negative. DNA analysis showed the presence of an aneuploid cell line.
A diagnosis of well-differentiated liposarcoma was made. Because of the rare occurrence of this type of tumor in the oral cavity, consultation was sought for confirmation from several authorities. The consultants disagreed as to whether this represented a malig- nancy; some favored a diagnosis of atypical lipoma, others a well-differentiated liposarcoma.
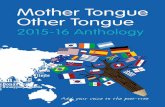
Magnetic resonance imaging was performed to assist in delineating the extent of the tumor. The mass was ovoid and homogenous, and involvement of the right anterior tongue musculature was clearly demar- cated. The tumor gave bright signal on Tl-weighted images (Fig 4) with progressively decreasing signal on the T2-weighted study (Fig 5). Fat-suppression images showed signal dropout within the mass (Fig 6).
Admission laboratory studies and chest radiographs were within normal limits and unremarkable. Because of the uncertain classification of the tumor and recent rapid growth, excision with a 2.0”cm surgical margin was performed under general anesthesia. The speci- men measured 5.0 X 5.0 X 5.0 cm, and all margins were tumor free. A rotational flap from uninvolved tongue tissue was used to reconstruct the surgically created defect. Multiple histologic sections were re- viewed, and the controversy continued regarding the precise diagnosis of this tumor.
The postoperative course was uneventful, without evidence of recurrence in the following 18 months. Mobility of the tongue was satisfactory, and minor speech alterations were resolving. Hyperesthesia of

226 ENLARGING TONGUE MASS
FIGURE 2. Photomicrograph showing the lipomatous compo-
nent with pseudoencapsulation (H&E stain, original magnifica- tion X401.
the right anterior tongue was present, but the patient stated that this was decreasing; taste was not notice- ably affected.
locations as “atypical lipoma” and those in deeper tissues as “well-differentiated liposarcoma” has been proposed.lOJ1
This case shows the excellent delineation of this
Discussion
Liposarcoma involving the oral cavity is rare. l-4 The difficulty in clinical and histologic differentiation of lipomatous oral masses has been recognized by sev- eral authors.5-9 Recently, a classification scheme that histologically categorizes similar lesions in superficial
tongue tumor by magnetic resonance imaging. The value of this modality as an adjunct in planning the extent of surgical intervention is apparent.
Complete surgical excision with a wide margin is the primary treatment of liposarcoma.*,12 Use of radia- tion therapy remains controversial, and an effective chemotherapeutic protocol has yet to be estab-
FIGURE 3. Photon showing pleomorphic pyknoti: nuclei, and c’ infiltration [H&E stair
licrograph lipoblasts,
ollagenous 1, original
magnificati& X 100).

NELSON, CHUPREVICH, AND GALBRAITH 227
FIGURE 4. Tl-weighted sagittal MR image showing the homog-
enous, hyperintense tongue mass.
lished.*Js-‘5 Regional lymph node metastases are rare and routine regional lymph node disection is not recommended.16
The resolution of the dilemma created by differing opinions regarding microscopic diagnosis, classilica- tion, and behavior of lipomatous tumors ultimately rests with the surgeon. In this case, primarily because of the sudden onset of rapid growth of this long-
FIGURE 5. T2-weighted axial MR image clearly demarcating the tongue mass and showing the decreased signal intensity.
FIGURE 6. Fat-suppressed T2-weighted sagittal MR image with signal dropout.
standing tumor, aggressive surgical management was required.
References
1. Eidinger G, Katsikeris N, Gullane P: Liposarcoma: Report of a case and review of the literature. J Oral Maxillofac Surg 48:984, 1990
2. Guest PG: Liposarcoma of the tongue: A case report and review of the literature. Br J Oral Maxillofac Surg 30:268, 1992
3. Dahl EC, Hammond HL, Sequeira E: Liposarcomas of the head and neck. J Oral Maxillofac Surg 40:674, 1982
4. McCulloch TM, Makielski KH, McNutt MA: Head & neck liposarcoma: A histopathologic reevaluation of reported cases. Arch Otolargngol Head Neck Surg 118:1045,1992
5. Guillou L, Dehon A, Charlin B, et al: Pleomorphic lipoma of the tongue: Case report and literature review. J Otolaryngol15:313, 1986
6. Westcott W, Correll R: Multiple recurrences of a lesion at the base of the tongue. JADA 108:231, 1984
7. Minic A: Welldifferentiated liposarcoma mimicking a pleomorpbic lipoma: Acase report. J Craniomaxillofac Surg 21:124,1993
8. Azumi N, Curtis J, Kempson RL, et al: Atypical and malignant neoplasms showing lipomatous diierentiation: A study of 111 cases.AmJSurgPatholll:l61, 1987
9. Hajdu SI: Pathology of Soft Tissue Tumors. Philadelphia, PA, Lea & Febiger, 1979, pp 255-259
10. Evans HL, Soule EH, Winkelmarrn RK: Atypical lipoma, atypical intramuscular Lipoma and well-differentiated retroperitoneal liposarcoma: A reappraisal of 30 cases formerly classified as well-differentiated lyposarcoma. Cancer 43:574, 1979
11. Stewart M, Schwartz M, AIford B: Atypical and malignant lipomatous lesions of the head and neck. Arch Otolaryngol Head Neck Surg 120:1151, 1994
12. Suzuki H, Nagayama M, Kaneda T, et al: Liposarcoma of the cheek in an infant. J Oral Maxillofac Surg 42:180, 1984
13. Charnock D, Jett T, Heise G, et al: Liposarcoma arising in the cheek: Report of a case and review of the literature. J Oral Maxillofac Surg 49:298, 1991
14. Zheng J, Wang Y: Liposarcoma in the oral and maxillofacial region: An analysis of 10 consecutive patients. J Oral Maxillofac Surg 52:595, 1994
15. Glenn J, Kinsella T, Gladstein E: A randominzed prospective trial of adjuvant chemotherapy in adults with soft tissue sarcomas of the head and neck, breast and trunk. Cancer 55:1206, 1985
16. Enzinger FM, Weiss SW Soft Tissue Tumors. St Louis, MO, Mosby-Year Book, 1988, pp 346-382