Enhancing retention in care for HIV-positive mothers and ... · strengthen the SOP through the...
66
30 September 2016 This publication was produced for the United States Agency for International Development. It was prepared by Godfrey Woelk,Yashin Lin, Brady Zieman, Rhoderick Machekano, Addmore Chadambuka, Cephas Muchuchuti, Auxilia Muchedzi, and Agnes Mahomva. ENHANCING RETENTION IN CARE FOR HIV-POSITIVE MOTHERS AND THEIR INFANTS BY IMPROVING FACILITY TRACKING AND COMMUNITY HEALTH WORKER TRACING IN ZIMBABWE THE TRACTOR STUDY REPORT
Transcript of Enhancing retention in care for HIV-positive mothers and ... · strengthen the SOP through the...
30 September 2016
This publication was produced for the United States Agency for International Development. It was prepared by Godfrey Woelk, Yashin Lin,
Brady Zieman, Rhoderick Machekano, Addmore Chadambuka, Cephas Muchuchuti, Auxilia Muchedzi, and Agnes Mahomva.
ENHANCING RETENTION IN CARE FOR HIV-POSITIVE MOTHERS AND THEIR INFANTS BY IMPROVING FACILITY TRACKING AND COMMUNITY HEALTH WORKER TRACING IN ZIMBABWE THE TRACTOR STUDY REPORT


ENHANCING RETENTION IN CARE FOR HIV-POSITIVE MOTHERS AND THEIR INFANTS BY IMPROVING FACILITY TRACKING AND COMMUNITY HEALTH WORKER TRACING IN ZIMBABWE THE TRACTOR (TRACKING AND TRACING OPERATIONS RESEARCH) STUDY REPORT
GODFREY WOELK, YASHIN LIN, BRADY ZIEMAN, RHODERICK MACHEKANO, ADDMORE CHADAMBUKA, CEPHAS MUCHUCHUTI, AUXILIA MUCHEDZI, AND AGNES MAHOMVA

This report was made possible through support provided by the President’s Emergency Plan for AIDS Relief and the U.S. Agency for International Development (USAID) via HIVCore, a Task Order funded by USAID under the Project SEARCH indefinite quantity contract (Contract No. AID-OAA-TO-11-00060).
HIVCore improves the efficiency, effectiveness, scale, and quality of HIV treatment, care, and support, and prevention of mother-to-child transmission (PMTCT) programs. The Task Order is led by the Population Council in partnership with Elizabeth Glaser Pediatric AIDS Foundation, Palladium, and the University of Washington. www.hivcore.org
Published in September 2016. ©2016. The Population Council Inc.
Cover photo: Provided courtesy of the Elizabeth Glaser Pediatric AIDS Foundation.
Suggested citation: Woelk, Godfrey, Yashin Lin, Brady Zieman, Rhoderick Machekano, Addmore Chadambuka, Cephas Muchuchuti, Auxilia Muchedzi, Agnes Mahomva. 2016. “Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and community health worker tracing in Zimbabwe,” HIVCore Final Report. Washington, DC: USAID | Project Search: HIVCore.
ACKNOWLEDGEMENTS
We would like to thank the health care and community health workers of the participating clinics for their cooperation in this study. We would especially like to thank the research assistants, Mongiwa Zondo, Francis Simmonds, Fortunate Mukandambi, and Shingi Chigwada, for their diligent and conscientious work on the study. We also very much appreciate students Everson Molande, who helped with data collection, and Tori Rivera and Sarah Money for their assistance with the data collation and analysis.

The TracTOR Study Report ■ i
TABLE OF CONTENTS
ACRONYMS ............................................................................................................... II
EXECUTIVE SUMMARY ...........................................................................................1
INTRODUCTION ......................................................................................................4
METHODOLOGY ......................................................................................................7
Study objectives and research questions ................................................................................................... 7Study design ..................................................................................................................................................... 7Study population ............................................................................................................................................. 7Sampling, sample size, and randomization ................................................................................................. 8The intervention ............................................................................................................................................. 9Research activities ........................................................................................................................................ 11Data collection and management .............................................................................................................. 12Data analysis .................................................................................................................................................. 13
KEY FINDINGS .........................................................................................................14
Baseline facility audit .................................................................................................................................... 14Focus group discussions .............................................................................................................................. 15Evaluation findings ...................................................................................................................................... 17High- versus low-performing intervention sites ...................................................................................24Factors influencing intervention implementation ..................................................................................25Process evaluation ....................................................................................................................................... 26
LIMITATIONS ...........................................................................................................27
DISCUSSION ...........................................................................................................28
REFERENCES ............................................................................................................30
APPENDICES ............................................................................................................31
Appendix 1 High and low performing sites by ANC visits, nurses, and facility rooms ................31Appendix 2 Tractor intervention guide .................................................................................................32Appendix 3 SOP for patient tracing in health facilities in Zimbabwe .............................................42Appendix 4 Periodicity of ART drug pick up per study site .............................................................58
ii ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
ACRONYMS
3TC LamivudineANC Antenatal careARV AntiretroviralART Antiretroviral therapyAZT ZidovudineCD4 Cluster of differentiation 4, refers to T-helper cells, a measure of immune statusCHW Community health workerCWC Child welfare clinicDNA Deoxynucleic acidDP Defaulting patientEGPAF Elizabeth Glaser Pediatric AIDS FoundationEID Early infant diagnosisFGD Focus group discussionHCW Health care workersHEI HIV-exposed infantHTC HIV testing and counselingL&D Labor and deliveryLTFU Lost to follow-upMBP Mother-baby pairMCH Maternal and child healthMTCT Maternal to child transmission (of HIV)MOHCC Ministry of Health and Child CareNVP NevirapinePCR Polymerase chain reaction PMTCT Prevention of mother to child transmission (of HIV)PNC Postnatal careRA Research assistantSOP Standard operating procedureVHW Village health workerWHO World Health Organization

The TracTOR Study Report ■ 1
EXECUTIVE SUMMARY
There is a high loss to follow-up rate in prevention of mother-to-child transmission of HIV (PMTCT) programs. A 2012 survey of mothers and infants who enrolled in Option-A1 PMTCT services in Zimbabwe in 2012 found a sharp decline in retention of HIV-positive pregnant women in HIV care between the second (83 percent retention) and fourth (45 percent retention) antenatal care (ANC) visit (EGPAF and Ministry of Health and Child Care 2013). Delays in drug pick-up also indicated poor retention in care and poor drug adherence among HIV-exposed infants (HEIs). Nevirapine (NVP) collection dropped from 44 percent to 12 percent between the second to the 10th antiretroviral (ARV) pick-up. Since Zimbabwe adopted the Option B+2 PMTCT schedule in 2013, the importance of ensuring that mother-baby pairs (MBPs) are retained in HIV care services has only increased. HIV-positive women who are not retained in HIV care are at increased risk of vertical transmission of HIV to their infants, and their infants are at increased risk of morbidity and mortality. Tracking and tracing HIV-positive women who miss their PMTCT clinic appointments allows health facility staff to adopt an active approach to helping women adhere to HIV care. In 2014, the Zimbabwe Ministry of Health and Child Care (MOHCC) implemented the Tracking and Tracing Standard Operating Procedure (SOP) to improve PMTCT retention. The SOP describes a systematic process to first identify MBPs that have failed to attend their scheduled clinical appointments (described as “defaulters” in the SOP), and subsequently utilize existing cadres of lay-health workers to trace these MBPs in their communities and facilitate their return to care.
Under the United States Agency for International Development-funded HIVCore project, led by the Population Council, the Elizabeth Glaser Pediatric AIDS Foundation designed an intervention to strengthen the SOP through the development of tools and procedures to support the appointment-making process, and identify and trace defaulters. The objective of this study was to determine whether the strategies proposed to enhance support for the implementation of Zimbabwe’s patient-tracing SOP affect rates of mother-baby pair retention in PMTCT programs, and infant HIV testing.
METHODS
Study designA two-arm cluster-randomized study where HIV-positive mothers and their HEIs that met study criteria were included in a cohort study in the study facilities and their outcomes were followed over a period of six months.
1Antepartum: AZT starting as early as 14 weeks gestation; Intrapartum: at onset of labor, single-dose NVP and first dose of AZT/3TC; Postpartum: daily AZT/3TC through 7 days postpartum; Infant daily NVP from birth until 1 week after cessation of all breastfeeding; or, if not breastfeeding or if mother is on treatment, through age 4–6 weeks (WHO 2012).2Maternal: triple ARVs starting as soon as diagnosed, continued for life; Infant: daily NVP or AZT from birth through age 4–6 weeks regardless of infant feeding method (WHO 2012).
2 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
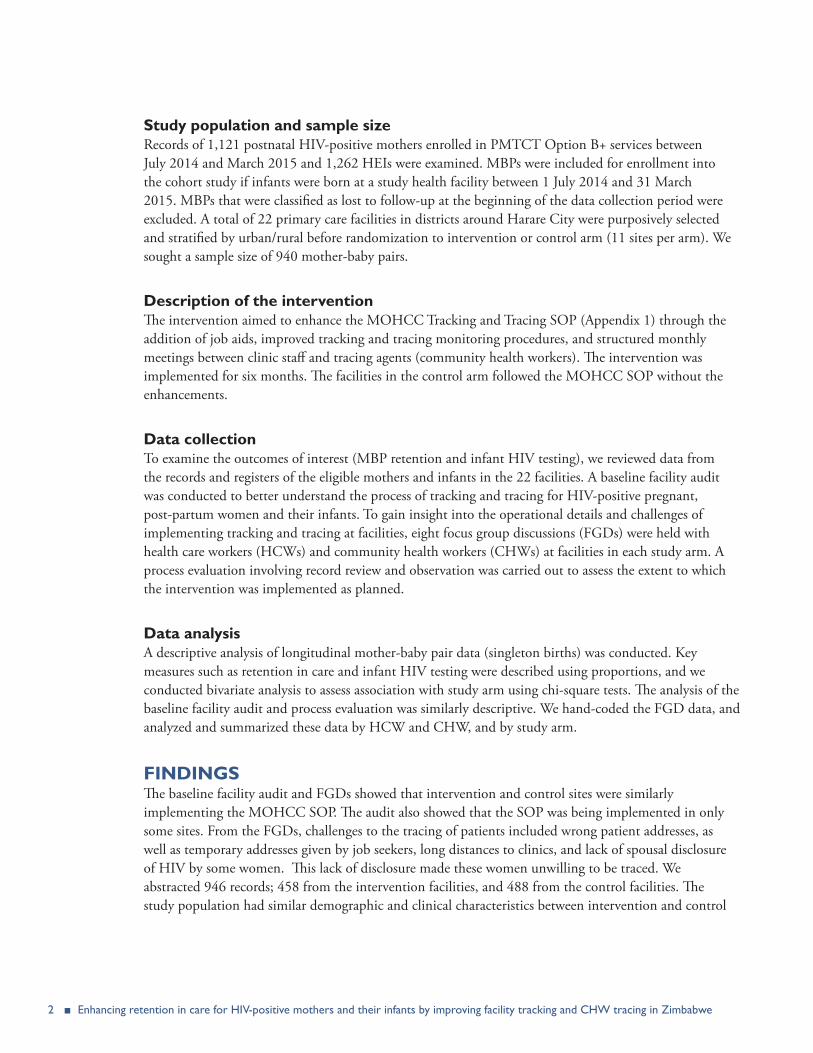
Study population and sample sizeRecords of 1,121 postnatal HIV-positive mothers enrolled in PMTCT Option B+ services between July 2014 and March 2015 and 1,262 HEIs were examined. MBPs were included for enrollment into the cohort study if infants were born at a study health facility between 1 July 2014 and 31 March 2015. MBPs that were classified as lost to follow-up at the beginning of the data collection period were excluded. A total of 22 primary care facilities in districts around Harare City were purposively selected and stratified by urban/rural before randomization to intervention or control arm (11 sites per arm). We sought a sample size of 940 mother-baby pairs.
Description of the interventionThe intervention aimed to enhance the MOHCC Tracking and Tracing SOP (Appendix 1) through the addition of job aids, improved tracking and tracing monitoring procedures, and structured monthly meetings between clinic staff and tracing agents (community health workers). The intervention was implemented for six months. The facilities in the control arm followed the MOHCC SOP without the enhancements.
Data collectionTo examine the outcomes of interest (MBP retention and infant HIV testing), we reviewed data from the records and registers of the eligible mothers and infants in the 22 facilities. A baseline facility audit was conducted to better understand the process of tracking and tracing for HIV-positive pregnant, post-partum women and their infants. To gain insight into the operational details and challenges of implementing tracking and tracing at facilities, eight focus group discussions (FGDs) were held with health care workers (HCWs) and community health workers (CHWs) at facilities in each study arm. A process evaluation involving record review and observation was carried out to assess the extent to which the intervention was implemented as planned.
Data analysisA descriptive analysis of longitudinal mother-baby pair data (singleton births) was conducted. Key measures such as retention in care and infant HIV testing were described using proportions, and we conducted bivariate analysis to assess association with study arm using chi-square tests. The analysis of the baseline facility audit and process evaluation was similarly descriptive. We hand-coded the FGD data, and analyzed and summarized these data by HCW and CHW, and by study arm.
FINDINGSThe baseline facility audit and FGDs showed that intervention and control sites were similarly implementing the MOHCC SOP. The audit also showed that the SOP was being implemented in only some sites. From the FGDs, challenges to the tracing of patients included wrong patient addresses, as well as temporary addresses given by job seekers, long distances to clinics, and lack of spousal disclosure of HIV by some women. This lack of disclosure made these women unwilling to be traced. We abstracted 946 records; 458 from the intervention facilities, and 488 from the control facilities. The study population had similar demographic and clinical characteristics between intervention and control
The TracTOR Study Report ■ 3
facilities. Maternal appointment-making significantly increased in the intervention sites compared to the control sites (51 percent versus 36 percent, p = 0.027), as did infant appointment-making (41 percent versus 5 percent, p < 0.001). There was overall no difference in the proportion of missed appointments, though there were significantly fewer missed maternal appointments in rural facilities vs. urban facilities (86 percent versus 95 percent, p = 0.042). A higher proportion of mothers in the intervention arm returned to care within three months of a missing appointment (11 percent versus 4 percent in SOC arm, p = 0.023), and this was significant for urban (10 percent versus 3 percent, p = 0.001), but not rural facilities. Similarly, a higher proportion of maternal and infant defaulting appointments were traced in the intervention arm compared to the control arm, though the actual proportions were small (3 percent versus 0 percent, p = 0.004, and 5 percent versus 0 percent, p < 0.001, respectively) The small numbers returning to care, however, limit comparisons between the two study groups. Default rates based on drug pickup data showed no difference between intervention and control sites. However, more women in the intervention arm returned to care after a tracing visit than those in the control arm (41 percent compared to 29 percent) though this difference was not statistically significant. There was no difference in the HIV testing rates between HEIs in the intervention and control facilities (14 percent versus 11 percent, p = 0.145). The assessment of the outcomes was affected by inadequate documentation, particularly of tracing data.
CONCLUSIONThe intervention of the enhanced MOHCC Tracking and Tracing SOP had some effect in improving appointment making, returning women to care within three months of a missed appointment (especially in urban areas), and in tracing defaulting women. However, inadequate tracing documentation limited the assessment of this effect. There was some evidence of improvement in tracing using drug defaulting data. Implementing an enhanced tracking and tracing procedure for HIV-positive pregnant and post-partum women may be effective, but consideration will need to be given to improving documentation, especially for CHWs, and designating a focal person to ensure the intervention overall is fully implemented and sustained. Consideration needs to be given also to issues improving capture of addresses, and spouse disclosure, as these may be important barriers to effective tracing by CHWs.

4 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
INTRODUCTION
Retention in HIV care is critical for preventing HIV transmission from HIV-positive mothers to their HIV-exposed infants (HEIs) and improving clinical outcomes of positive mothers and infants (Sibanda 2013). In 2012, Elizabeth Glaser Pediatric AIDS Foundation (EGPAF) and the Zimbabwe Ministry of Health and Child Care (MOHCC) implemented a survey examining retention-in-care and ART adherence of mothers and infants who enrolled in Option-A3 prevention of mother-to-child transmission (PMTCT) services. The survey found a sharp decline in retention of HIV-positive pregnant women in HIV care between the second and fourth antenatal care (ANC) visit—from 83 to 45 percent retention. Similarly, Nevirapine (NVP) collection for infants dropped from 44 to 12 percent between the second to the 10th antiretroviral (ARV) pick-up (EGPAF and Ministry of Health and Child Care 2013). Lack of retention in care of HEIs carries the additional risk of delaying HIV testing and early treatment.
In seeking to address the challenge of retention in PMTCT care in the context of health worker shortages, we drew evidence from Zambia (Putta et al. 2011; Mulenga et al. 2011), Nigeria (Adedeji et al. 2011) and Ethiopia (Mclaughlin et al. 2010; Greyling, Long, and Kean 2013). The evidence suggests that employing community-based and peer-led strategies can improve the overall performance of PMTCT programs, as well as the retention of PMTCT-enrolled mothers and their infants (Marcos, Phelps, and Bachman 2012; Kim, et al. 2012). WHO supports this approach, which recommends strengthening CHW capacity to enable this cadre to assist in the delivery of PMTCT services (WHO 2010).
In 2014, the Zimbabwe MOHCC proposed standard operating procedures (SOP) to improve PMTCT retention through a community based approach, including contact tracing and tracking of mothers who failed to attend the scheduled appointments (see Appendix 1). Through the United States Agency for International Development-funded HIVCore project, led by the Population Council, researchers from the Elizabeth Glaser Pediatric AIDS Foundation and the Popuulation Council conducted a learning visit in March 2015 to design the intervention. Discussions with EGPAF staff in Zimbabwe and observations in the health facilities indicated key gaps that could potentially hinder the success of the client tracing activities laid out by the SOP, including insufficient training and guidance on implementing new tools, and poor monitoring and supervision. Thus, the current study was conceived as an opportunity to develop an intervention to address such gaps and assess its effect on retention.
Tracking and Tracing SOP The SOP describes how health care workers (HCWs) should identify mother-baby pairs (MBPs) that have failed to attend their scheduled clinical appointments, how community health workers (CHWs) should trace these MBPs in their communities and facilitate their return to care, and how HCWs and CHWs should coordinate and communicate on tracking and tracing.
3Antepartum: AZT starting as early as 14 weeks gestation; Intrapartum: at onset of labor, single-dose NVP and first dose of AZT/3TC; Postpartum: daily AZT/3TC through 7 days postpartum; Infant daily NVP from birth until 1week after cessation of all breastfeeding; or, if not breastfeeding or if mother is on treatment, through age 4–6 weeks (WHO 2012).

The TracTOR Study Report ■ 5
To thoroughly understand the activities described in the SOP, and how the proposed intervention complemented its implementation, it is important to first define several terms:
Default: An MBP is considered to have defaulted on care if they have missed a scheduled appointment by more than five days. Once an MBP crosses this five-day threshold, they are targeted for active tracing efforts through home-based follow-up visits from community health workers. Tracing is carried out to obtain information about the outcome of the MBP—i.e., whether they may have transferred, stopped treatment, or died. Tracing is also done to help or persuade those who have stopped treatment to resume.
Lost to follow-up: Once an MBP has been in default for a period of at least 90 days, the MBP is considered lost to follow-up (LTFU) and will be removed from client tracing reports.
Tracking: Tracking refers to the process of identifying MBPs who have missed scheduled appointments, and monitoring their status (i.e., results from tracing efforts, return to the clinic).
Tracing: Tracing is the process by which CHWs will attempt to re-establish contact with defaulting MBP in their homes or communities. Once a CHW has located a defaulting MBP, they will conduct a follow-up visit to encourage the pair to return to clinical care and help reschedule missed visits.
Implementation of the MOHCC tracking and tracing SOP took place in July 2014 with training workshops for tracing defaulting patients in the community and with training for tracking defaulting patients in May 2015.
Description of the intervention We designed the Tracking and Tracing Operations Research (TracTOR) study intervention with information from a learning visit conducted in March 2015. The learning visit focused on whether and how the tracking and tracing system was being implemented at seven clinics, including representation from rural and urban sites, as well as Harare City council-run and MOHCC-run facilities. The following is a summary of the learning visit findings and how the intervention design proposed to address the identified gaps.
Support for appointment making. The learning visit indicated that the appointment diary had been distributed at most sites. In some sites it was not actively used, and at sites in which it was used, it was sometimes used for other purposes (e.g., notebook) or was not being used correctly (i.e., without collecting the correct information for each patient). Thus, the study intervention consisted of a plan for regular spot checking of the appointment-making process, which could be conducted by clinic staff as part of a quality improvement cycle, or it could be conducted by study staff with spot check results fed back to clinic staff. In addition, a job aid was devised consisting of a ruler with column headings pasted to its back so that staff could complete the diary with the appropriate information for tracing a defaulting patient in the community (Figure 2).
Support for identification of defaulters. The learning visit indicated that facility staff seemed to have a system in place for identifying patients that miss their appointments and following up with them in the community. However, there was no documentation regarding whether such patients were visited by community health workers (CHWs), or the outcome of a CHW follow-up. To address this, the study intervention included a defaulter’s box and notebook. The box was to be a location where patient medical

6 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
records (“green books”) of patients that did not attend their clinic visits were to be stored at the end of each day. In order to document tracing efforts, the intervention also included a defaulter’s notebook that was to be used for tracking MBPs that missed their appointments. An accompanying ruler job aid with defaulter notebook column headings in the back would provide guidance on the appropriate information to document in the notebook, much like the equivalent job aid for the diary (Figure 2).
Support for tracing defaulters. The learning visit also indicated that clinic staff provided lists of defaulting patients at monthly meetings with CHWs. In addition, clinic staff distributed forms that CHWs were to complete and CHWs received their stipends at these meetings. But the manner in which meetings were structured was not clear. Thus, the study intervention consisted of a plan to structure meetings systematically for sharing tracing results for each defaulting patient (described in the monthly section of the SOP for clinic staff), in order to track and trace defaulters in the TracTOR intervention description. As envisioned, the structure of the meeting would allow clinic staff to document the updated status of each defaulting patient in the defaulter’s notebook, based on tracing reports from CHWs.
The intervention was pre-tested in two health facilities, one urban and one rural, in mid-July 2015, and then implemented between late July and late August 2015. Some of the findings from the pre-test included the following:
1. The appointment diary was in use, but was not being consistently completed;
2. The facilities had developed their own individual processes for tracking and tracing the mothers (e.g., having a notebook for defaulters they called the “Follow-up register,” and drawing up a list of defaulters with name, address, reason, and outcome/comments, which is then given to the CHW to follow-up); and
3. The defaulter notebook and defaulter box tools were welcomed.
The TracTOR Study Report ■ 7
METHODOLOGY
STUDY OBJECTIVES AND RESEARCH QUESTIONSThe study objectives were to:
y Determine whether the strategies proposed to enhance support for the implementation of Zimbabwe’s patient tracing SOP improve rates of MBP retention in PMTCT programs, and infant HIV testing.
y Document the implementation of MBP tracking and tracing activities and assess their fidelity to the SOP.
Primary research questions y What is the effect of the intervention on the proportion of MBPs seen in the clinic within two weeks,
one month, and three months of a missed clinic appointment?
y What is the effect of the intervention on the proportion of women successfully traced4 by a CHW?
y What is the effect of the intervention on the proportion of all eligible HEIs who received at least one HIV test during the study period?
y How does the real-world implementation client tracking and tracing SOP deviate from the SOP?
Secondary research questions y What is the effect of the intervention on the proportion of MBPs who default on their scheduled HIV
related clinic visits, including ARV pickups?
y What is the effect of the intervention on the proportion of women who return and remain in care for at least three consecutive follow-up visits after missing a clinic appointment?
y What is the effect of the intervention on the proportion of HIV-infected infants initiated on ART?
y What is the effect of the intervention on the average time between initial service default and return to care among defaulters who are not lost to follow-up?
STUDY DESIGNWe undertook a two-arm cluster-randomized study where all records of HIV-positive mothers and their HIV-exposed infants that met study criteria were enrolled in a cohort in the study facilities and their outcomes followed over time.
STUDY POPULATIONThe study population consisted of the records of 1,121 postnatal HIV-positive mothers enrolled in PMTCT Option B+ services and 1,262 HIV-exposed infants. Mother-baby pairs (MBPs) were included
4A woman is considered “traced” if a CHW completed a home-visit with the targeted client or otherwise provides justification for her removal from future follow-up. Outcomes of CHW tracing activities include: home visit completed, documented transfer to another facility, refused further care, client deceased.

8 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
if infants were born at a study health facility between 1 July 2014 and 31 March 2015. Mother-baby pairs that were classified as lost to follow-up at the beginning of data collection period (1 July 2015) were excluded.
Figure 1 Timeline of study activities, relative to infant date of birth range defining study cohort
SAMPLING, SAMPLE SIZE, AND RANDOMIZATIONA total of 22 primary care health facilities (11 in each arm) were purposively selected as study sites based on road access, presence of a cadre of community health workers, and proximity to Harare city. Study sites in Harare (urban sites) were purposively selected among high volume, non-referral health facilities concentrated in one geographic location and offering maternity services. For the sites in the rural and semi-rural districts, EGPAF selected all public health facilities in selected districts with relatively high patient volume and that were not participating in other studies. The health facilities were located in seven out of the 62 health districts in Zimbabwe.
Sites were classified as urban, semi-urban, and rural before they were randomly assigned to a study arm within each stratum. To randomly assign sites, we gave each facility the value of a random six-digit decimal between 0 and 1, using the Excel RAND() function. The last digit of this number was used to assign sites to study arms: odd numbers were assigned to the control arm.
We based our sample size on the difference in proportions in intervention and control conditions of HEI receiving HIV testing after nine months of age. Based on 2013 client service records supplied by EGPAF-supported facilities in Zimbabwe, we estimated that only 35–40 percent of HEIs will receive HIV testing after nine months of age. We designed the study to detect a 15-percentage point difference in infant HIV testing rates between intervention and comparison facilities, with a 95 percent confidence level, and 80 percent power. Using the estimated infant HIV testing rates and a design effect of 2.0 to account for intra-cluster correlation, we calculated a sample size of a minimum of 470 records of HIV-positive PMTCT-enrolled, post-partum MBPs in each study arm consisting of 11 facilities, for a total sample size of 940 MBPs.
2014 Oct Jan 2015 Apr Jul Oct Jan 2016
Infant date of birth
MOHCC Tracking and Tracing TOT
Study observation period
Intervention launch

The TracTOR Study Report ■ 9
THE INTERVENTIONThe intervention aimed to enhance the MOHCC SOP. The central elements of the SOP were:
y Appointment-making process captured in appointment books (tracking MPBs).
y Use of CHWs for tracing of defaulting mothers, and documentation of tracing in the registers.
y Referral slips given by CHWs to the mothers who have been traced, for them to give to the clinic on their return to care.
y Inclusion of tracking and tracing activities in the standard monthly meetings of the clinic staff and the CHWs.
The intervention included pretested job aids, improved tracking and tracing procedures, and structured monthly meetings, in addition to the SOP. Figure 2 presents a diagram of the intervention (intervention guide is presented in Appendix 3).

10 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
Figure 2 The interventionControl condition
(The MOHCC SOP)
Intervention condition
(developed from preliminary study assessment and discussion with HCWs)
Appointment books Appointment booksCHWs CHWs
CHW registers CHW registersReferral slips Referral slips
Monthly meeting Monthly meeting
PlusJob aids (defaulter box, defaulter’s log, rulers with column headings for diary and log)
Defaulter box
Rulers with column headings for (1) appointment diary and (2) defaulter’s notebook to assure correct
information is captured
RULER FRONT
RULER BACK, APPOINTMENT DIARY would include a sticker with column headings that should be included in the appointment diary (2–5)
RULER BACK, DEFAULTER’S NOTEBOOK would include a sticker with column headings that should be included in the defaulter’s notebook (1–10)
(2) Mother’s Full Name (3) ART number (4) Phone (5) Address

The TracTOR Study Report ■ 11
Improved tracking and tracing monitoring procedures (appointment monitoring and defaulter identification and monitoring, including “run” charts)
Structured monthly meetings
The job aids (which were pre-tested) included the defaulter’s box, to store medical records of defaulting patients; the defaulter’s log, to document tracing outcomes of defaulting patients; rulers with column headings for the appointment diary; and the defaulter’s notebook to assure correct information is captured.
The improved monitoring procedures included periodic spot-checking of appointment-making for clinic visits and infant testing through the adequacy of ART numbers in pharmacy register, and a “run” chart tool to graph results, with the results provided as feedback to staff daily. In addition, weekly procedures for identifying and monitoring defaulters included detailed procedures documenting tracing efforts of MBPs that miss appointments, and instructions on using job aids.
The structured monthly meeting involved procedures for monthly meetings between clinic staff and CHWs, including pre-meeting verification of whether defaulting clients re-appeared at clinic, progress indicators shared by each CHW, and feedback to CHWs on which clients returned to clinic.
RESEARCH ACTIVITIESThe study involved the following activities:
Baseline facility audit: The study included a baseline facility audit, conducted between August and September 2015 for most sites. The purpose of the facility audit was to better understand the process of tracking and tracing for HIV-positive pregnant, post-partum women and their infants.
12 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
Focus group discussions: We conducted focus group discussions (FGDs) with HCWs and CHWs to gain insight into the operational details and challenges of implementing tracking and tracing at facilities in each arm.
Process evaluation: As part of study monitoring, we undertook a process evaluation to assess the extent to which the intervention was implemented as planned.
Construction and observation of the cohort of mother-baby pairs: The observation of the cohort from the patient records and registers enabled the evaluation of the intervention.
DATA COLLECTION AND MANAGEMENTThe data collection for the main study consisted of clinic register and medical record abstraction, conducted in two parts. The first phase comprised the identification of eligible study participants and baseline data collection from registers (delivery register, postnatal care register) and maternal and infant medical records (i.e., OI/ART Care booklet and Exposed Infant Register). Maternal and infant register and record data were systematically entered in Microsoft Access data entry forms, which also applied study inclusion and exclusion criteria. Working in teams, four research assistants (RAs) collected longitudinal data across registers.
The second part consisted of abstraction of follow-up data in the sources above as well as 10 additional registers, ultimately including the appointment diary as well as community health worker registers. Mother-baby pairs were linked in the study database using randomly-generated unique study identification numbers.
Data quality was assessed by the study coordinator and data manager at 12 sites in three rounds. Sites were randomly selected using proportional sampling within urban/rural strata (nine rural and three urban). Ten percent of MBPs at each site were identified using systematic sampling, and key variables in MBP identification were abstracted and compared with research-assistant collected data. Systematic discrepancies were fed back to the RA team.
The baseline audit consisted of an interview with the nurse-in-charge in the MCH unit and included information from facility records consulted during the interview. The audit gathered descriptive data on facility-level health service characteristics and clinic operations.
For the FGDs, trained research assistants facilitated eight focus group discussions (FGDs), with five to eight participants each. In each study arm, two FGDs were held with facility HCWs and two were held with CHWs who participated in client tracing activities.
There were several sources of information for assessing the extent to which intervention components were implemented. RAs conducted visual assessments of the status of selected intervention components, as well as spot checks of the adequacy in the use of ART numbers and appointment making. Visual assessments of intervention components, such as the use of the defaulter’s box and notebook, were documented in checklists. In the case of spot checks, RAs selected a random sample of 10 medical records of patients documented to have appointments in the current month, and searched for corresponding appointments documented in the appropriate appointment diary. The adequacy of the use of ART numbers in key registers was spot-checked using a similar method. The findings of the spot-checking resulted in a percentage “score” of records with ART documentation (i.e., out of 10 charts reviewed), and this was

The TracTOR Study Report ■ 13
entered in a run chart to monitor potential improvement. During the study observation period, each facility should have ended up with five scores, though logistically, RAs were not able to complete all spot-checking at all sites every month. RAs completed checklists and run charts about once a month at each intervention site, during biweekly assessments conducted during data collection site visits, and provided feedback to staff on findings.
A third information source consisted of the FGDs (described above), which were conducted among HCWs and CHWs, and took place in the middle of the study observation period.5
Finally, the team of RAs constituted a fourth source of information for the process evaluation. Because the team developed a relationship with facility staff in the course of introducing and reinforcing intervention components at health facilities, as well as data collection activities, they brought valuable insights into understanding potential reasons intervention components were or were not implemented.
DATA ANALYSISWe undertook a descriptive analysis of longitudinal MBP data (singleton births). Key measures such as retention in care and HIV testing were described using proportions, and bivariate analysis was conducted to assess association with study arm, using chi-square tests. The analysis of the baseline facility audit and process evaluation was similarly descriptive.
FGD data were recorded digitally and simultaneously transcribed and translated into English. To assure data quality, the project coordinator reviewed transcripts and their translations. The data were coded by hand, and inter-coder reliability was assured, as the analysis was conducted by a single researcher. Data were then analyzed and summarized by HCW and CHW responses in the intervention and control arms.
5For intervention sites, the HCW FGDs took place on 28 October and 3 December 2015, while the CHW FGDs took place on 27 October and 5 November 2015.

14 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
KEY FINDINGS
We present findings from the facility audit, the FGDs, the evaluation findings by study objective, and the process evaluation findings.
BASELINE FACILITY AUDIT
Facility audit—Linking client appointments, care, and tracingTable 1 presents the facility audit findings on the appointment-making process. As described in the methods section, research assistants randomly selected two patients from the ART register and attempted to find their details in the appointment diary or other documentation. The research assistants also found documentation that these patients were being followed by CHWs.
In four of the ten intervention facilities and five of 11 control facilities, at least one patient from the register was found in the appointment diary and the patients appeared to be followed up by the CHWs in the same proportion of facilities.
Table 1 Facility audit; Linking client appointments, care, and tracingRandomly select 2 patients from the ART register of women who delivered in 2014:
Intervention (N = 10)
Control (N = 11)
Can find at least one patient in the diary from the register 4 5
Can produce follow-up documentation on patients who were not found in ART register
0 0
Document which patients currently being followed by CHW 4 5
The audit also examined communication between the clinic and the CHWs, with particular reference to the tracking and tracing SOP, but bearing in mind that CHWs have broader duties. Overall, there appeared to be frequent communication between CHWs and clinic staff, with staff from 7 intervention clinics and an equal number of control clinics reporting calling the CHWs 17 times on the phone for the intervention sites and 19 for the control sites in the past month. Clinic staff in 7/9 intervention sites and 6/6 control sites reported that they had met monthly with the CHWs as a group to discuss tracking and tracing activities in the past three months. However, CHWs did not appear to get their stipends on time, as staff in 6/8 intervention facilities and 5/7 control facilities indicated that the CHWs had not been given their stipends on time in the past three months, though they eventually did receive their stipends.
Overall, these findings suggest that at baseline, intervention and control sites were similar in their implementation of the MoHCC SOP.
The TracTOR Study Report ■ 15
FOCUS GROUP DISCUSSIONSThe findings from the FGDs indicated that there were similar operating practices between intervention and control sites in appointment making.
Making appointmentsHCWs at both control and intervention sites indicated that future appointments are set when the client comes into the clinic for a scheduled visit (control sites indicated that it is when the patient comes in to collect medication) and the patient’s information is written in the appointment diary. Control sites also write it down on a card to present to the patient and the intervention sites write it down in the “client book.” However, where the appointment diary was kept, it varied for both control and intervention sites.
Identifying defaulting patientsControl sites explained that the HCWs use the PMTCT diary to identify defaulting patients (DPs). Review dates for patients are written in this diary and HCWs will comment or “tick” in the PMTCT diary when the patient attends on that date. Any patient that is not “ticked” in the PMTCT diary is considered a defaulting patient. Intervention sites instead use the referral slips and appointment diary to identify those patients that successfully attended an appointment.
Reasons mothers give for defaultingCHWs gave reasons for defaulting, including distance and lack of transport, job seeking mobility, patients’ health status (i.e., inability to travel to the clinic due to poor health), employment (patient not given permission to take off work or patient cannot financially afford to miss a day of work), and long wait at the clinic as potential reasons for defaulting. Sometimes a lack of disclosure of their status to husbands and family members was a factor. Additionally, some mothers discontinued the child’s medication because they did not have enough food to give the child and the medication had negative side effects when taken without food.
Tracing methodsAt both control and intervention sites, HCWs call the DP if there is a number listed in the file to encourage the patient to come into the clinic. Control site HCWs also visit the DP at home if the patient lives close to the clinic. If the DP cannot be contacted by phone, the CHW is asked to trace and visit the person at the addresses listed and leave a letter or a message for them. CHWs in intervention sites also tended to use the phone more, and to intimate to the patients that phoning rather than visiting helped to protect confidentiality.
Tracing challengesThe CHWs in both control and intervention sites cited wrong addresses as a major challenge in tracing. Distance is also a barrier to tracing in both control and intervention sites. Additionally, the mobility of these populations due to job-seeking behaviors makes tracing difficult in both control and intervention sites. In control sites, this meant that patients were providing the local address where they stay but not their permanent address. In intervention sites, tracing people on farms becomes difficult because patients are working all day and farm managers do not give the patients time off to attend the clinic. Both control

16 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
and intervention sites indicated that women who have yet to disclose their status to their husbands presented a tracing challenge, as the presence of the CHW may reveal their status.
Confidentiality between CHWs and defaulting patientsDisclosure was a prominent issue at some intervention sites, despite clinic staff doing their best to treat ART patients in the same manner as every other patient that comes to the clinic. Intervention site CHWs have communicated with HCWs that it is difficult to maintain confidentiality, especially if they are to leave a message with someone other than the patient themselves, which often happens if the CHW is unable to return to the home multiple times due to distance of the home.
HCW-CHW communication HCWs at both control and intervention sites speak with CHWs every week in person when CHWs are in the clinic. HCWs at control sites rarely use cell phones unless the matter is urgent, while HCWs at intervention sites use cell phones.
Monthly meetingsBoth control and intervention sites conduct meetings on a weekly basis (four per month) in order to update CHWs on current trends or information on health issues, as well as receive feedback from CHWs about health issues in the community and discuss best approaches and solutions to overcoming them. However, CHWs from the control sites mentioned challenges such as the long duration of meetings leading to apathy and hunger, lack of materials such as stationery and notebooks, transportation to the clinic, and staff turnover in the clinic head position.
Referral slipThe HCWs and CHWs explained that the referral slip helps to indicate that a patient attended the clinic and communicate this between CHWs, HCWs, and patients. Control sites also indicated that the slip motivates CHWs to ensure patients attend the clinic (makes them feel accountable), ensures that reasons for the visit are confidential (referral slips are given to all patients no matter the visit reason), and shows patients they have a support system with the clinic that cares about their health. Intervention sites indicated that the slip also helps to determine the number of DPs, as well as the delay between when the CHW traced the patient and when the patient arrives at the clinic. However, some control sites explained that referral slips are either nonexistent in their area or patients do not bring them to visits.
CHW registerHCWs in the intervention sites indicated that often they do not look at the CHWs register because of workload. Challenges for both control and intervention sites include the heavy weight of the register; as a result, CHWs move around the community with a separate notebook and transfer the details into the CHW register when they return home. Additional challenges for the intervention sites included a better understanding/more training required to complete it accurately. Some CHWs are having trouble completing the forms because they are older and cannot write properly.
The TracTOR Study Report ■ 17
Recommendations for tracking and tracing of MBPsBoth control and intervention sites suggested that airtime and cell phones to trace patients, transport for both CHWs and MBPs, and the welfare of the CHWs (providing them with sunhats, umbrellas, etc.) would be helpful. Control sites also suggested subsidizing the USD 25 registration fee for mothers, improving information sharing within the community to help mothers understand the importance of registering their pregnancies, and working with clinics to transfer the medication to local communities where travel is difficult and long. Intervention sites suggested additional trainings for staff and peer groups for mothers to increase the effectiveness of tracing MBPs.
EVALUATION FINDINGS
Objective 1: To determine whether the strategies proposed to enhance support for the implementation of Zimbabwe’s patient tracing SOP affect rates of MBP retention in PMTCT programs, and infant HIV testing.We extracted records for 946 mother/baby pairs, 458 (48 percent) in the intervention arm, and 488 (52 percent) in the control arm. We first present a description of the study population to assess the extent to which these characteristics are balanced by study arm, as this may have implications for the analysis.
Table 1 presents the demographic and clinical characteristics of the study cohort by intervention and control study arms. Overall, the demographic and clinical characteristics were similar between the two arms. About 37 percent of the mothers were under the age of 30 years, about 72 percent were married, and about 20 percent had a CD4 count < 350 mmHg3, though these data were missing for 55 percent of the women. About 9 percent of women in the intervention sites had been classified as WHO stage III at ART initiation, compared to 4 percent in the control sites, though this did not reach statistical significance, (p = 0.057). These data were missing for about 30 percent of all the mothers. Forty percent of mothers in the intervention arm and 44 percent of mothers in the control arm had secondary or higher education, though again, these data were missing for about 57 percent of all the women. Similar proportions (78 percent) had documented addresses, and about 60 percent of the women in both study arms had documented phone numbers. The proportion of infants more than 12 months of age compared with those 12 months or less was significantly higher in the control arm compared to the intervention (i.e., infants were older in the control group) (p = 0.007). Similarly, significantly more infants in the control arm had had infant PCR testing prior to the study observation period (p < 0.001).
Making and documenting appointments is an essential first step to assess whether the women returned on time, subsequently triggering tracing activities if they have not returned in a timely manner. Table 2 presents the appointments made and the missed appointments by study arm and by urban/rural facilities.

18 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
Table 2 Demographic and clinical characteristics of the study population by study arm Intervention
n (%)Control
n (%)P value
Number of MBPs 458 (48.4) 488 (51.6)Received care at urban facility 303 (66.2) 295 (60.4) 0.069
Mother’s age 0.526< 25 69 (15.1 ) 78 (16.0 )25– < 35 215 (46.9 ) 200 (41.0 )≥ 35 94 (20.5 ) 113 (23.1 )Missing 80 (17.5) 97 (19.9)
Marital status 0.829Married 341 (74.4 ) 349 (71.5)Single/divorced/widowed 31 (6.8 ) 25 (5.1)Missing 86 (18.8) 114 (23.4)
Mother’s CD4 count at initiation 0.137<350 109 (23.8 ) 96 (19.7 )350+ 95 (20.7 ) 107 (21.9 )Missing 254 (55.5) 285 (58.4)
Mother’s WHO stage at initiation (include missing)
0.061
Stage I/II 288 (62.9) 297 (60.9)Stage III 40 (8.7) 20 (4.1)Missing 130 (28.4) 171 (35.0)
Education 0.057Primary or less 40 (8.7) 63 (12.9)Secondary or more 184 (40.2) 219 (44.9)Missing 234 (51.1) 206 (42.2)
Have documented address 358 (78.2) 389 (79.7) 0.560Missing 100 (21.8) 99 (20.3)
Have documented phone 260 (56.8) 298 (61.1) 0.179Missing 198 (43.2) 190 (38.9)
Infant age at beginning of observation period
<6 m 123 (26.9) 120 (24.6) 0.0586–<9 m 158 (34.5) 169 (34.6)9–<12 m 153 (33.4) 151 (30.9)≥ 12 m 24 (5.2) 48 (9.8)
Infant had PCR testing completed before study observation period†
226 (49.3) 315 (64.6) <0.001
†Due to study timeline, all infants should have completed PCR testing before study observation period
The TracTOR Study Report ■ 19
Table 3 Appointment making by study arm and by urban/rural facilities, mothers and infants
Intervention n (%)
Control n (%)
P-value n (%)
Total mother-baby pairs 458 488Women with at least one appointment 233 (50.9) 175 (35.9)
Urban facilities 165 (54.5) 134 (45.4) 0.027
Rural facilities 68 (43.9) 41 (21.2) <0.001
Total maternal appointments at: 539 363 <0.001Urban facilities 366 (67.9) 285 (78.5)Rural facilities 173 (32.1) 78 (21.5)
Missed appointments† 437 (81.1) 291 (80.1)
Urban facilities 288 (78.7) 217 (76.1) 0.439
Rural facilities 149 (86.1) 74 (95.2) 0.042Infants with at least one appointment 190 (41.5) 22 (4.5) <0.001
Urban facilities 124 (40.9) 0 <0.001
Rural facilities 66 (42.6) 22 (11.4) <0.001Total infant appointments: 617 56
Urban facilities 442 (71.6) 0 (0)Rural facilities 175 (28.4) 51 (100.0)
Missed infant appointments 504 (81.7) 51 (91.1) 0.077Urban facilities 361 (82.4) 0Rural facilities 143 (79.9) 51 (91.1) 0.054
†Missed appointments are appointments which are missed by 5 days or more
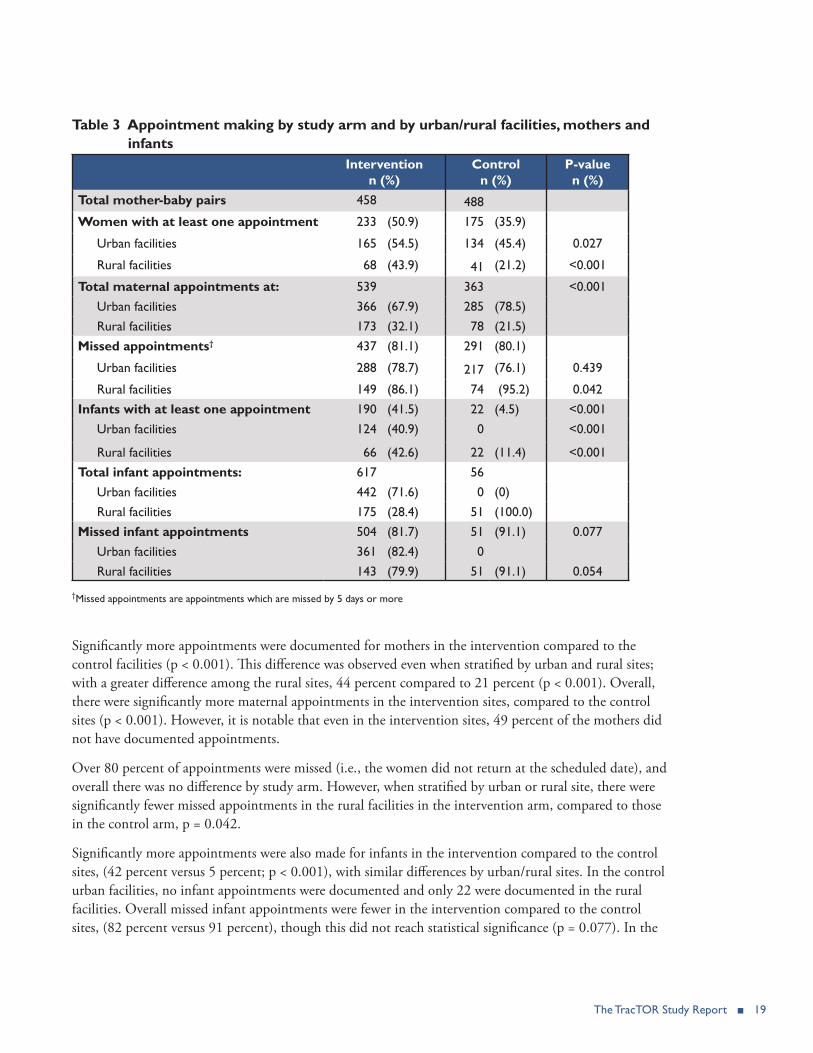
Significantly more appointments were documented for mothers in the intervention compared to the control facilities (p < 0.001). This difference was observed even when stratified by urban and rural sites; with a greater difference among the rural sites, 44 percent compared to 21 percent (p < 0.001). Overall, there were significantly more maternal appointments in the intervention sites, compared to the control sites (p < 0.001). However, it is notable that even in the intervention sites, 49 percent of the mothers did not have documented appointments.
Over 80 percent of appointments were missed (i.e., the women did not return at the scheduled date), and overall there was no difference by study arm. However, when stratified by urban or rural site, there were significantly fewer missed appointments in the rural facilities in the intervention arm, compared to those in the control arm, p = 0.042.
Significantly more appointments were also made for infants in the intervention compared to the control sites, (42 percent versus 5 percent; p < 0.001), with similar differences by urban/rural sites. In the control urban facilities, no infant appointments were documented and only 22 were documented in the rural facilities. Overall missed infant appointments were fewer in the intervention compared to the control sites, (82 percent versus 91 percent), though this did not reach statistical significance (p = 0.077). In the
20 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
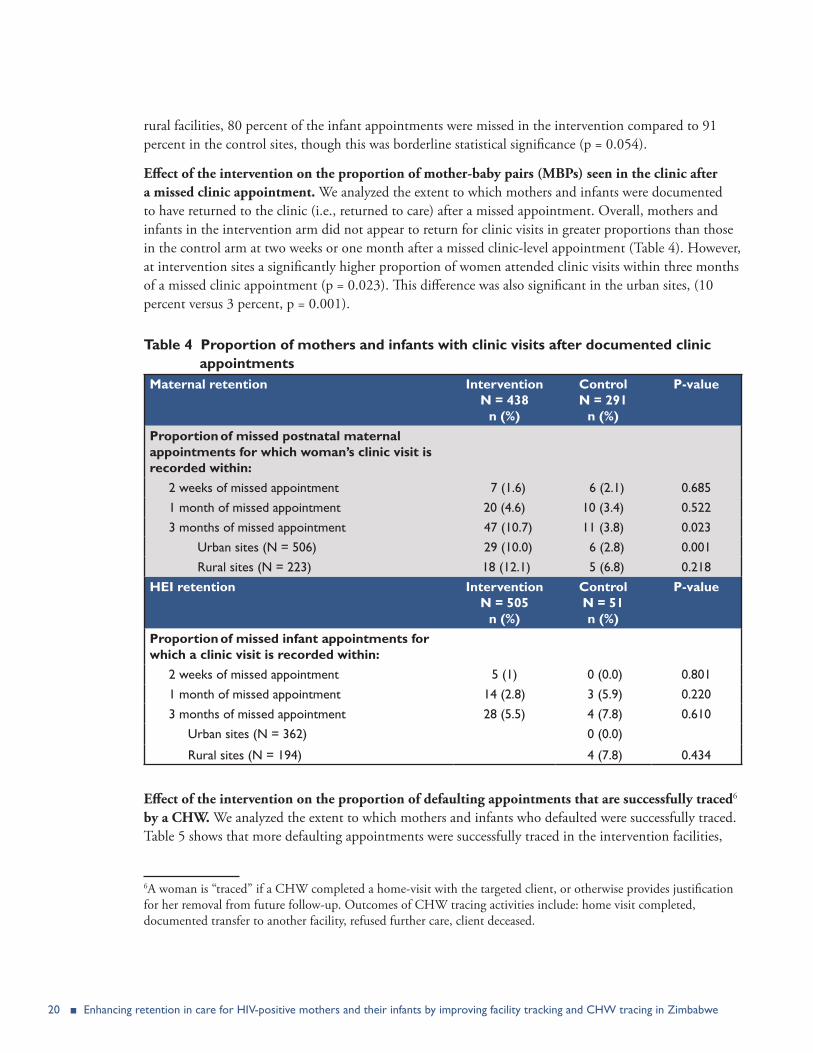
rural facilities, 80 percent of the infant appointments were missed in the intervention compared to 91 percent in the control sites, though this was borderline statistical significance (p = 0.054).
Effect of the intervention on the proportion of mother-baby pairs (MBPs) seen in the clinic after a missed clinic appointment. We analyzed the extent to which mothers and infants were documented to have returned to the clinic (i.e., returned to care) after a missed appointment. Overall, mothers and infants in the intervention arm did not appear to return for clinic visits in greater proportions than those in the control arm at two weeks or one month after a missed clinic-level appointment (Table 4). However, at intervention sites a significantly higher proportion of women attended clinic visits within three months of a missed clinic appointment (p = 0.023). This difference was also significant in the urban sites, (10 percent versus 3 percent, p = 0.001).
Table 4 Proportion of mothers and infants with clinic visits after documented clinic appointmentsMaternal retention Intervention
N = 438 n (%)
Control N = 291
n (%)
P-value
Proportion of missed postnatal maternal appointments for which woman’s clinic visit is recorded within:
2 weeks of missed appointment 7 (1.6) 6 (2.1) 0.6851 month of missed appointment 20 (4.6) 10 (3.4) 0.5223 months of missed appointment 47 (10.7) 11 (3.8) 0.023
Urban sites (N = 506) 29 (10.0) 6 (2.8) 0.001 Rural sites (N = 223) 18 (12.1) 5 (6.8) 0.218
HEI retention Intervention N = 505
n (%)
Control N = 51 n (%)
P-value
Proportion of missed infant appointments for which a clinic visit is recorded within:
2 weeks of missed appointment 5 (1) 0 (0.0) 0.8011 month of missed appointment 14 (2.8) 3 (5.9) 0.2203 months of missed appointment 28 (5.5) 4 (7.8) 0.610
Urban sites (N = 362) 0 (0.0)
Rural sites (N = 194) 4 (7.8) 0.434
Effect of the intervention on the proportion of defaulting appointments that are successfully traced6 by a CHW. We analyzed the extent to which mothers and infants who defaulted were successfully traced. Table 5 shows that more defaulting appointments were successfully traced in the intervention facilities,
6A woman is “traced” if a CHW completed a home-visit with the targeted client, or otherwise provides justification for her removal from future follow-up. Outcomes of CHW tracing activities include: home visit completed, documented transfer to another facility, refused further care, client deceased.

The TracTOR Study Report ■ 21
for both mothers and infants. However, the documented community-level tracing efforts were low overall, with 0 in the control sites, and 3 percent and 5 percent for the mothers and infants in the intervention sites.
Table 5 Proportion of defaulting appointments for which there is documentation of tracing done by a CHW
Intervention N = 437
n (%)
Control N = 291
n (%)Among maternal appointments for which patient defaulted, proportion that were traced
12 (2.7) 0 (0.0)
N = 504 n (%)
N = 51 n (%)
Among infant appointments for which patient defaulted, proportion that were traced
25 (5.0) 0 (0.0)
Effect of intervention on proportion of women who return and remain in care for at least three consecutive clinic visits. Defaulting women who return to care may not remain in care. We thus used a measure of three consecutive follow up visits as a way of assessing retention over a longer period. The assumption was based on the understanding that patients returned to the clinic every month to pick up a monthly supply of ARVs.
During the course of this study, we learned that each health facility set very different intervals between clinic visits and appointment dates; the most common interval was 60 days. Appendix 4 presents a complete list of study facilities and corresponding intervals, varying between 30 and 180 days for adults. In order to assess the proportion of women returning to care for at least three consecutive visits, we would have needed data on three consecutive follow up visits after a missed clinic visit, representing six months (i.e., three 60-day intervals) and five days (i.e., a missed visit is declared five days after a missed appointment). Since the entirety of our observation period was six months, it was too short to answer this research question.
Effect of intervention on infant HIV testing and ARV initiation. The Zimbabwe MOHCC 2013 guidelines recommend that asymptomatic HEIs are tested for HIV; (1) at six weeks (virological test) and, if the child has ever breastfed, (2) at nine months (antibody test), and (3) at six or more weeks after cessation of breastfeeding (MOHCC 2013). HEIs testing HIV-positive are given a confirmatory test at 18 months of age. Because there is generally less known about HIV testing after the 6–8 week PCR testing, the study design targeted the nine-month antibody testing. During the six-month observation period, the youngest HEI was between four and 10.1 months, while the oldest was 13 to 19 months.
Only 12 percent of HEIs were documented to have had any HIV testing at study facilities during this time, with no difference observed between study arms (Table 6). A slightly higher proportion of HEIs in the intervention arm were tested (Table 6: 14 percent vs 11 percent), but the difference was not significant (p = 0.145). However, the HEIs in the intervention arm that were tested appeared to do so at a significantly younger age than HEIs in the control arm—a difference of 40 days, though there were significant differences in the age distribution of infants between the two study arms at the outset. When

22 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
adjusted for age, there was no significant difference in the proportion of HEI tested by intervention and control arms (p = 0.121).
No HEIs were initiated on ART in either study arm during the study observation period. Prior to the study observation period, more HIV-infected infants initiated ART in the intervention arm compared to the control arm, 7/18 (39 percent) versus 2/9 (22 percent), though this was not statistically significant (p = 0.667).
Table 6 Infant HIV testing and ART initiationIntervention
N = 458Control N = 488
P-value
HIV-exposed infants with any HIV testing during study observation period
63 (13.8%) 52 (10.7%) 0.145
Average age in days at 1st HIV test during study observation period†
316.08 days~10.4 months
355.75~11.7 months
<0.001
HIV-exposed infants testing HIV-positive 18 9HIV-infected infants initiating ART (before study observation period)
7 (38.9%) 2 (22.2%) 0.667
†Infants were 4 to 13 months at the beginning of the 6 month observation period
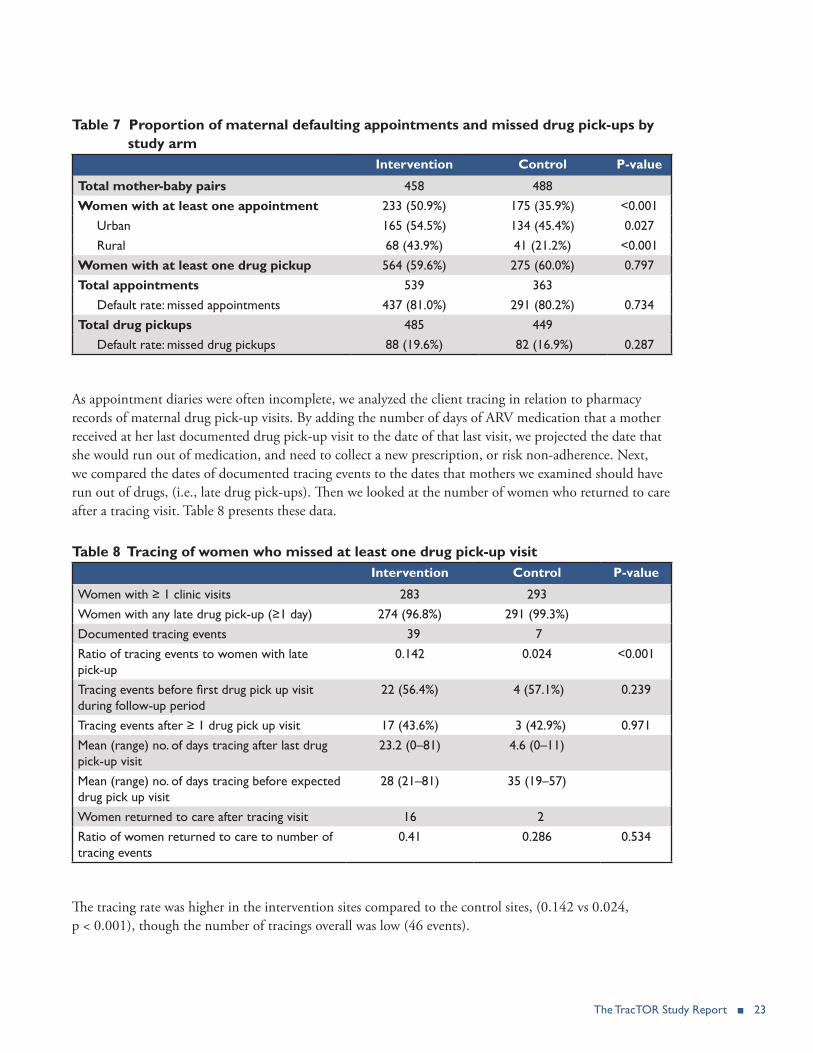
Effect of the intervention on the proportion of MBPs who default on their scheduled HIV-related clinic visits, including ARV pickups. Among maternal appointments in each study arm, approximately the same proportion were appointments that were missed by over seven days7 (81 percent and 80 percent in the intervention and control groups respectively). While the study intervention sought to address missed appointments, ultimately, we were interested in retention as an estimate of potential drug adherence. We thus also sought to estimate defaulting based on drug quantities documented in pharmacy registers. Table 7 presents this analysis. To assess patient default rates based on drug data, we calculated the next expected ARV pick up date for each participant, based on the number of days of drug supply that was retrieved at the pharmacy. The expected pick up date was compared to the next actual drug pick up date, and a default was defined as a difference of over five days. The missed drug pick-up default rate was similar for the intervention and controls sites (20 percent in the intervention sites vs. 17 percent in the control sites, p = 0.287).
7While the MOHCC SOP defines a defaulter as a patient who misses her appointment by five days, we allowed for “defaulting” to be seven days, as it is likely that clinic staff would actually begin to act after a week (seven days).
The TracTOR Study Report ■ 23
Table 7 Proportion of maternal defaulting appointments and missed drug pick-ups by study arm
Intervention Control P-value
Total mother-baby pairs 458 488Women with at least one appointment 233 (50.9%) 175 (35.9%) <0.001
Urban 165 (54.5%) 134 (45.4%) 0.027Rural 68 (43.9%) 41 (21.2%) <0.001
Women with at least one drug pickup 564 (59.6%) 275 (60.0%) 0.797Total appointments 539 363
Default rate: missed appointments 437 (81.0%) 291 (80.2%) 0.734Total drug pickups 485 449
Default rate: missed drug pickups 88 (19.6%) 82 (16.9%) 0.287
As appointment diaries were often incomplete, we analyzed the client tracing in relation to pharmacy records of maternal drug pick-up visits. By adding the number of days of ARV medication that a mother received at her last documented drug pick-up visit to the date of that last visit, we projected the date that she would run out of medication, and need to collect a new prescription, or risk non-adherence. Next, we compared the dates of documented tracing events to the dates that mothers we examined should have run out of drugs, (i.e., late drug pick-ups). Then we looked at the number of women who returned to care after a tracing visit. Table 8 presents these data.
Table 8 Tracing of women who missed at least one drug pick-up visitIntervention Control P-value
Women with ≥ 1 clinic visits 283 293Women with any late drug pick-up (≥1 day) 274 (96.8%) 291 (99.3%)Documented tracing events 39 7Ratio of tracing events to women with late pick-up
0.142 0.024 <0.001
Tracing events before first drug pick up visit during follow-up period
22 (56.4%) 4 (57.1%) 0.239
Tracing events after ≥ 1 drug pick up visit 17 (43.6%) 3 (42.9%) 0.971Mean (range) no. of days tracing after last drug pick-up visit
23.2 (0–81) 4.6 (0–11)
Mean (range) no. of days tracing before expected drug pick up visit
28 (21–81) 35 (19–57)
Women returned to care after tracing visit 16 2Ratio of women returned to care to number of tracing events
0.41 0.286 0.534
The tracing rate was higher in the intervention sites compared to the control sites, (0.142 vs 0.024, p < 0.001), though the number of tracings overall was low (46 events).
24 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
Of note is that 26 of the 46 documented tracing events occurred after the start of the data collection period, but before the clients’ first visit to the clinic. Of the 20 tracing events after completing at least one drug pickup visit, 17 tracings were recorded in the intervention group, compared to 3 in the control sites (p = 0.971). Of the women traced, 16 returned to care in the intervention sites, compared to 2 in the control sites. Thus the ratio of women returned to care to number of tracing events was 0.41 in the intervention compared to 0.286 in the control ( p = 0.534). This difference was not statistically significant because of the small numbers, particularly in the control sites.
Objective 2: Documentation of implementation of MBP tracking and tracing activities and fidelity to the MOHCC tracking and tracing SOPThe MOHCC tracking and tracing SOP can be divided into three parts: appointment making, tracking of defaulters, and tracing of defaulters.
From the facility audits at baseline, linking client appointments, care, and tracing, in only nine of the 21 sites evaluated (43 percent) was there evidence that at least one patient from the diary could be found in the ART register. In the same proportion of sites, 9/21, there was evidence that patients were currently being followed by CHWs. The data from the FGDs suggest that appointment books were being used to document appointments. However, the proportion of women with at least one appointment was only 36 percent in the control sites, and even in the intervention facilities, this was only 51 percent. In the rural control facilities, the proportion of women with at least one appointment was only 21 percent. The proportion of infants with at least one appointment was only 5 percent, with none recorded in the urban facilities.
The examination of the proportion of defaulting appointments for which there was evidence of tracing showed that there were none in the control sites, and only 3 percent of these appointments were traced in the intervention facilities (Table 5). When we analyzed the proportion of women traced who missed at least one drug pick-up visit, there were only seven tracing events in the control sites and 46 overall (Table 8). Only two women in the control sites were documented to have returned to care after being traced.
HIGH- VERSUS LOW-PERFORMING INTERVENTION SITES In order to understand better how the multi-component study intervention may have been implemented, we compared high-performing sites against low-performing sites among the 11 intervention sites. We defined high and low performance by the proportion of women with at least one appointment, since appointment-making triggers the chain of health clinic actions that would potentially bring a woman who misses a clinic visit back into care. Using the current paper-based health facility information system, missed appointments are the method by which providers are supposed to systematically identify women who miss clinic appointments. If a health facility does not recognize that a clinic visit has been missed, under the existing information system (i.e., no electronic medical record), there is no active effort to retain the patient.
Two urban (one in a small town) and one rural facility had the highest proportions of women at the facilities receiving at least one appointment (average 75 percent). In analyzing common factors in the intervention implementation experience of these three facilities, we also included another rural facility that had 71 percent of women with at least one appointment. There were three facilities, one urban and
The TracTOR Study Report ■ 25
two rural, with lowest proportions of women with at least one appointment. An average of 16 percent of women at these facilities received at least one appointment.
Implementation of the interventionGiven that high- and low-performing sites were defined according to appointment-making, we compared details in the intervention implementation process in an attempt to garner insight as to the underpinning reasons for the differences. The process of spot-checking the quality of appointment-making was done by conducting a monthly check of 10 non-consecutive records of mothers who should have had appointments in the previous month, and calculating an appointment making score by adding up the number of appointments that were written in the appointment diary. The score for this exercise was then presented to an MCH nurse as part of the coaching part of the intervention. High-performing sites scored higher in appointment making scores from the inception.
We examined a proxy measure for workload of ANC visits per nurse per month and the number of rooms used for PMTCT activities as a crude indicator of crowding. We present these data in Appendix 2. This comparison showed little difference in either of these indicators, suggesting that other factors may be relevant in explaining the difference. However, the average number of nurses in a facility does not adequately account for staff being away on training or nights off, so that in fact there may be less staff available at any one time than indicated by the average proxy. Study staff suggested that through their observations, clinic organization and flow may have been important also in the extent to which the intervention was implemented. We were however unable to adequately assess this as a factor.
FACTORS INFLUENCING INTERVENTION IMPLEMENTATIONIn order to understand the factors affecting the study intervention implementation, we conducted a guided discussion with the study team members that introduced, monitored, and reinforced the study intervention at intervention sites (research coordinator and research assistants). Over the six-month observation period, this team developed a relationship with health facility staff and considerable knowledge of the clinic organization, including its information system. The guided discussion called for team members to first rate the degree to which each of a list of potential factors were important influences in the quality of implementation of each intervention component (improvement of diary use, defaulter’s box, defaulter’s notebook, structured CHW meetings, CHW reporting). The potential facility-level factors included the value of the intervention component, motivational factors, nurse-in-charge support for the intervention, district support for the intervention, nurse-in-charge ability to enforce new procedures among staff, staff workload and staff turnover. Research assistants (RAs) were also asked to assess the relative importance of factors related to their own support on implementation; these factors included the initial introduction to intervention activities, ongoing coaching and support, routine monitoring of intervention activities, and RA ability to influence facility staff to implement intervention.
RAs perceived that the facility factors that most influenced the implementation of the intervention at high performing sites were the nurse-in-charge’s support for the intervention and his or her ability to enforce new procedures. Additional factors noted included the quality of the intervention component, district support for the intervention, and staff workload. Study staff also felt that their monitoring and coaching strongly influenced appointment-making at high-performing sites. At low-performing sites, the study team felt the most important factor influencing the implementation of the intervention was the nurse-in-charge’s ability to enforce new procedures. More details that emerged from the facilitated discussion with

26 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
RAs and that have been shared throughout the study are included below to better illustrate each point.
Leadership and staff. In one urban facility in a small town, the nurse-in-charge demonstrated a high level of interest, motivation, and problem-solving ability in addressing defaulters before the study team started to interact with them. Study staff described “[the] MCH nurse is in charge of everything. She is just more knowledgeable.” First, the site already had an improvised register for tracking defaulters (Follow Up Register), so after the study initiated, the nurse-in-charge just had to decide on whether the site should continue using this register or the Defaulter’s Notebook. In addition, the monthly CHW meetings were already structured to systematically document updated information for defaulting patients: the nurse would call out the name of each patient, and the corresponding CHW would share the outcome of the tracing activity and patient status. During the course of the study, the nurse realized that it was more efficient for each CHW to directly update the defaulter’s notebook for the patients she was assigned as the CHW arrived at the clinic for the meeting.
At the other urban site (large city), the facility staff were described as very supportive and appreciative during the piloting of the intervention. Staff were amenable to operational adjustments proposed to implement the intervention. The nurse-in-charge at one of the rural sites was described as enthusiastic about the intervention and her attitude may have contributed to the use of the defaulter’s notebook and box. Facility staff were also noted to have been cooperative.
Intervention monitoring and reinforcementDue to budgetary constraints, the RAs also had to monitor the implementation of the intervention in addition to collecting data. This may have limited the time available for intervention monitoring activities.
PROCESS EVALUATION As stated earlier in the methods section, we attempted to assess the extent to which the intervention elements were implemented as planned. We examined documentation of ART numbers, as this permits long-term mother-baby pair follow-up across registers. In 10 of the 11 intervention sites, we found that ART numbers had been consistently documented in the appointment diary as compared to the ART numbers in the ART pharmacy register. We found consistent documentation of ART numbers for infants in 7/11 sites. For appointments scheduled in the diary, we found this available in 7/11 sites for mothers and 5/11 sites for infants.
We also assessed the use of the intervention tools over two periods; September 2015 through January 2016 and again in March 2016. In 5/11 sites, the defaulter’s box was spontaneously mentioned by the HCW FGDs over the period September 2015 to January 2016. The defaulter’s log was also spontaneously mentioned in 4/11 sites in this time. In March 2016, 4/11 sites had evidence of use of the defaulter’s box, and 2/11 sites, the defaulter’s log. The process evaluation suggests that after initial uptake of some of the intervention tools, there was decay in the behavior toward the end of the six-month intervention period.
Concerning the structured monthly meetings, we were not able to follow up to verify if the monthly meetings had been restructured due to intensive data collection needs.

LIMITATIONS
There are several limitations to this study. Our analysis would not have been able to account for self-transfers from health facilities, which could have been interpreted as defaulting. We also could not account for documentation about appointments that might have been on the patients’ cards, which they carry with them.
The FGD facilitators also introduced and monitored the intervention, so that another limitation is the possibility of skewed responses positively on related questions (social desirability bias) in the FGDs, even though the researchers did work to decrease these biases by encouraging participants to report as accurately as possible, despite what they may believe to be the anticipated or desired outcome. Another limitation is that as we randomized at the facility level, we could not engage district-level health staff in supporting and facilitating the intervention. An additional limitation is that the six-month intervention period was too short to evaluate adequately the intervention, particularly as many women were given drug supplies for three months. Also this time period was too short to adequately evaluate the effect on HEI testing and treatment if HIV infected.

28 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
DISCUSSION
Overall, the intervention significantly increased appointment-making for both mothers and infants in both urban and rural sites. The intervention increased maternal retention by returning to care women with missed appointments within three months, overall and in the urban sites, but not in the rural sites. The intervention also increased the amount of tracing among defaulting appointments, again among both the mothers and infants. However, even among the interventions sites, the number of documented tracing events was very low.
Though the proportion of mothers returning after missed appointments remained low, the finding that mothers returned to care within three months of missed appointments, rather than earlier, suggests that the intervention needs to have a “maturation period” before showing an effect.
While the intervention improved appointment-making and may have improved retention within three months, there was less effect on tracing activities. This finding may have been because of poor documentation. The CHWs may not have been adequately documenting their efforts in their registers. In addition, the provision of wrong addresses and population mobility, particularly in urban areas, could have contributed to poor tracing. It may be also that these data are written on the patient cards, rather than in the clinic records.
The deficiencies in documentation may have affected our ability to evaluate the intervention effect on infant HIV testing, resulting in a smaller number of HEI than envisaged and assessed to have been tested.
The improved appointment-making did not appear to result in lower default rates. This may have been related to how defaulting was defined. But even when drug availability was used to assess defaulting rates, there was no apparent effect. Part of this may be because of the lack of visibility in terms of who is defaulting. Even with the additional tools, this may not be easily visible without significant additional work. Not adequately knowing who is coming and who is not means that clinic staff may not know that they have a problem, and so they may not be motivated to track and trace the patients.
The analysis of the high- versus low-performing sites and the assessment of factors affecting the implementation of the intervention suggests that a key factor in implementing the intervention is leadership at the site level. If the nurse-in-charge is interested and committed, she can usually implement change effectively. It would be important to identify and engage champions to facilitate the intervention.
An important finding was that only nine of 27 HIV-infected infants had been initiated on ART according to the clinic records, showing a clear need for improvements in infant treatment.
Lessons learned include the following:
1. The importance of documentation. Tools should be designed with input from the intended users so that they can be optimally used. The source of tracing information is the CHW register. This register is not easy to carry around, so the CHWs use notebooks and other tools to capture these data, with the potential for error in transcribing the information into the register.

The TracTOR Study Report ■ 29
2. The intervention package was effective in improving some aspects of the tracking and tracing process. There clearly is a need for job aids and better monitoring procedures in the tracking and tracing process. The intervention may have been more effective if there had been a dedicated intervention coordinator for a limited time until the intervention elements had been integrated into the systems of all the intervention facilities. The implication for programming is that there needs to be a focal person who will be responsible for the implementation, especially since there was evidence that the intervention was beginning to decay over time, with some of the tools no longer being used. However, given resource constraints, consideration should be given to how staff from relatively high-performing sites can share their enthusiasm and interest with other staff, and how champions can be engaged in the process.
3. Disclosure and confidentiality are important barriers to effective tracing as mentioned by the CHWs in the FGDs. This has implications for the type of cadre used to trace the HIV-positive women as to whether to use another HIV-positive woman such as from mothers-to-mothers, or a general purpose cadre, such as a CHW.
30 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
REFERENCES
Adedeji, O. et al. 2011. “Role of community resource persons (CORPs) in increasing utilization of ANC, HCT, and PMTCT services in Nigeria.” Poster presented at 6th IAS Conference on HIV Pathogenesis and Treatment, Rome, Italy, 17–20 July.
EGPAF & Ministry of Health and Child Care. 2013. “Survey on adherence to ARV pick up for prophylaxis/ART and retention of mothers and infants in the PMTCT program in Zimbabwe.”
Greyling, C., S. Long, and S. Kean. 2013. “Best practices for establishing mother support groups to reduce HIV vertical transmission: a review of programmes in Africa.” Poster presented at 19th International AIDS Conference, Washington, DC, 22–27 July.
Kim, M. H. et al. 2012. “The Tingathe programme: a pilot intervention using community health workers to create a continuum of care in the prevention of mother to child transmission of HIV (PMTCT) cascade of services in Malawi,” Journal of the International AIDS Society 15(Suppl 2): 17389. doi:10.7448/IAS.15.4.17389.
Marcos, Y., B. R. Phelps, and G. Bachman. 2012. “Community strategies that improve care and retention along the prevention of mother-to-child transmission of HIV cascade: a review,” Journal of the International AIDS Society 15(Suppl 2): 17394. doi:10.7448/IAS.15.4.17394
Mclaughlin, P. et al. 2010. “Effective community health worker approaches in Ethiopian PMTCT.” Presented at 18th International AIDS Conference, Vienna, Austria, 18–23 July.
Ministry of Health and Child Care (2013). Guidelines for Antiretroviral Therapy for the Prevention and Treatment of HIV in Zimbabwe.
Mulenga, P. et al. 2011. “Scaling up of prevention of mother to child transmission (PMTCT) services, through community involvement, in a resource constrained rural setting, Chilonga Zambia.” Poster presented at 6th IAS Conference on HIV Pathogenesis and Treatment, Rome, Italy, 17–20 July.
Putta, N. et al. 2011. “Lay counselors improve PMTCT (prevention of mother to child transmission) care in Mongu district, Zambia.” Presented at 6th IAS Conference on HIV Pathogenesis and Treatment, Rome, Italy, 17–20 July.
Sibanda, E. L. et al. 2013. “The magnitude of loss to follow-up of HIV-exposed infants along the prevention of mother-to-child HIV transmission continuum of care: a systematic review and meta-analysis,” AIDS 27(17): 2787–2797.
WHO. 2010. “PMTCT strategic vision 2010–2015 : preventing mother-to-child transmission of HIV to reach the UNGASS and Millennium Development Goals.” Geneva: World Health Organization.
WHO. 2012. “Programmatic update: use of antiretroviral drugs fro treating pregnant women and preventing HIV infection in infants, executive summary.” Geneva: WHO.
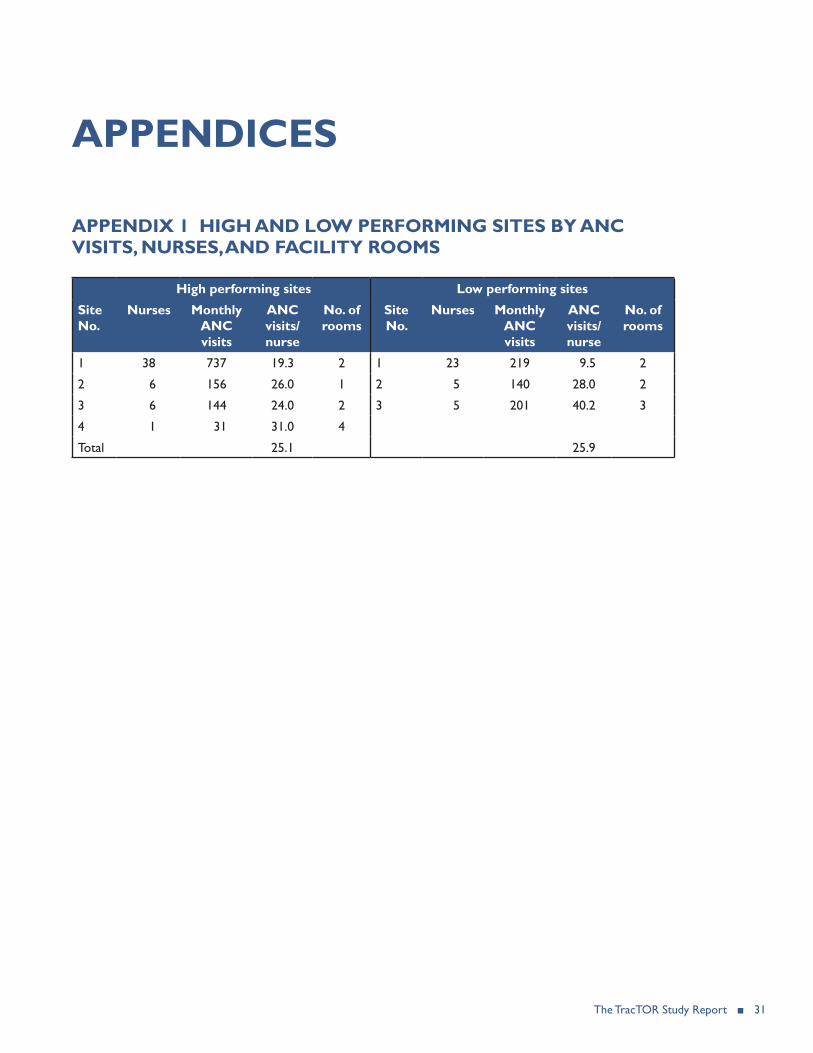
The TracTOR Study Report ■ 31
APPENDICES
APPENDIX 1 HIGH AND LOW PERFORMING SITES BY ANC VISITS, NURSES, AND FACILITY ROOMS
High performing sites Low performing sites
Site No.
Nurses Monthly ANC visits
ANC visits/nurse
No. of rooms
Site No.
Nurses Monthly ANC visits
ANC visits/nurse
No. of rooms
1 38 737 19.3 2 1 23 219 9.5 2
2 6 156 26.0 1 2 5 140 28.0 2
3 6 144 24.0 2 3 5 201 40.2 3
4 1 31 31.0 4
Total 25.1 25.9

32 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
AP
PE
ND
IX 2
TR
AC
TO
R IN
TE
RVE
NT
ION
GU
IDE
Th
e Tra
CTO
R in
terv
entio
n fo
cuse
s on
impr
ovin
g th
ree
mai
n pr
oces
ses:
the
appo
intm
ent-m
akin
g pr
oces
s, th
e pr
oces
s for
trac
king
, tra
cing
an
d do
cum
entin
g de
faul
ters
, and
syste
mat
ic d
ocum
enta
tion
of C
HW
wor
k. Th
e co
mpo
nent
s are
des
crib
ed in
mor
e de
tail
in th
e ta
ble
belo
w.
The
curr
ent T
raC
TOR
inte
rven
tion
guid
e al
so in
clud
es th
e fo
llow
ing
tool
s: a
CH
W lo
g to
trac
k C
HW
wor
k (A
-1),
a D
efau
lter N
oteb
ook
Rule
r (A-
2), a
Def
aulte
r Not
eboo
k pr
otot
ype
(A-3
), an
d SO
P th
at d
escr
ibe
the
daily
, wee
kly,
and
mon
thly
pro
cess
es n
eede
d to
impl
emen
t the
in
terv
entio
n (A
-4).
1Ap
poin
tmen
t mak
ing
proc
ess
Goa
lIn
terv
enti
on a
ctiv
ity
Det
aile
d id
eas
(ple
ase
com
men
t/ex
pand
)C
omm
ents
1aA
ssur
e th
at A
#s
are
docu
men
ted
in e
ntri
es in
key
re
gist
ers
and
Impr
ove
syst
emat
ic
docu
men
tatio
n of
rou
tine
clin
ical
vi
sits
in g
reen
boo
ks
and
Expo
sed
Infa
nt
Reg
iste
rs
IC1 c
oach
es f
acili
ty s
taff
to le
ad
mon
thly
Pla
n-D
o-St
udy-
Act
cyc
les2 :
1. E
very
mon
th, I
C a
nd in
-cha
rge
toge
ther
mea
sure
the
ext
ent
of
the
prob
lem
usi
ng t
he in
dica
tor
deta
iled
to t
he r
ight
2. I
n-ch
arge
dis
cuss
es w
ith s
taff
why
thi
s is
a p
robl
em
3. I
n-ch
arge
lead
s fa
cilit
ated
di
scus
sion
to
iden
tify
the
root
of
or r
easo
ns fo
r th
e pr
oble
m
4. S
taff
brai
nsto
rm w
ays
of
addr
essi
ng p
robl
em
5. I
C a
nd in
-cha
rge
cont
inue
to
trac
k in
dica
tor
each
mon
th
to m
easu
re a
nd d
iscu
ss
impr
ovem
ent
as a
gro
up u
ntil
indi
cato
r m
easu
res
at 9
0% fo
r 3
cons
ecut
ive
mon
ths.
Inte
rven
tion
coor
dina
tor
asse
sses
the
be
low
indi
cato
r at
reg
iste
rs a
t th
e si
te t
o de
term
ine
mag
nitu
de o
f pro
blem
:1.
In
dica
tor
to c
heck
on
leve
l of
docu
men
tatio
n of
A#s
for
HIV
-pos
itive
w
omen
in P
MT
CT
[# o
f pts
(of
tho
se in
the
den
omin
ator
) fo
und
in A
RT p
harm
acy
regi
ster
3 usi
ng
A#s
][“
Ran
dom
” s
elec
tion
of 1
0 gr
een
book
s of
PM
TC
T c
lient
s w
ith A
#s fo
r w
hich
the
re a
re e
ntri
es in
the
pre
viou
s re
port
ing
mon
th]
2.
Indi
cato
r to
che
ck o
n le
vel o
f do
cum
enta
tion
of A
#s fo
r H
EIs
[# o
f HEI
s (o
f tho
se in
the
den
omin
ator
) w
ho a
re fo
und
in t
he In
fant
Dis
pens
ing
Reg
iste
r us
ing
mot
her’s
P#
or fi
rst/
last
na
me
chea
t she
et]
[Ran
dom
sel
ectio
n of
10
HEI
s fo
r w
hich
th
ere
are
entr
ies
in t
he p
revi
ous
mon
th
in t
he E
xpos
ed In
fant
Reg
iste
r]
Peri
odic
ity:
Mon
thly
unt
il le
vel o
f qu
ality
is s
usta
ined
PDSA
act
ivity
wou
ld in
itial
ly b
e co
nduc
ted
toge
ther
with
IC s
uppo
rt
as a
cap
acity
bui
ldin
g ex
erci
se.
Ove
r tim
e, w
e ho
pe t
his
wou
ld b
e co
nduc
ted
by t
he in
-cha
rge
duri
ng
regu
lar
staf
f mee
tings
.
Late
r, si
mila
r ef
fort
s co
uld
focu
s on
qu
ality
of d
ata
in D
NA
/PC
R R
egis
ters
an
d/or
Infa
nt D
iagn
osis
Reg
iste
r
1 Inte
rven
tion
coor
dina
tor
2 For
bac
kgro
und
on P
DSA
cyc
le: h
ttp:
//ww
w.in
stitu
te.n
hs.u
k/qu
ality
_and
_ser
vice
_im
prov
emen
t_to
ols/
qual
ity_a
nd_s
ervi
ce_i
mpr
ovem
ent_
tool
s/pl
an_d
o_st
udy_
act.h
tml
3 Mos
t pl
aces
do
not
have
ART
pha
rmac
y on
ly fo
r PM
TC
T m
othe
rs.
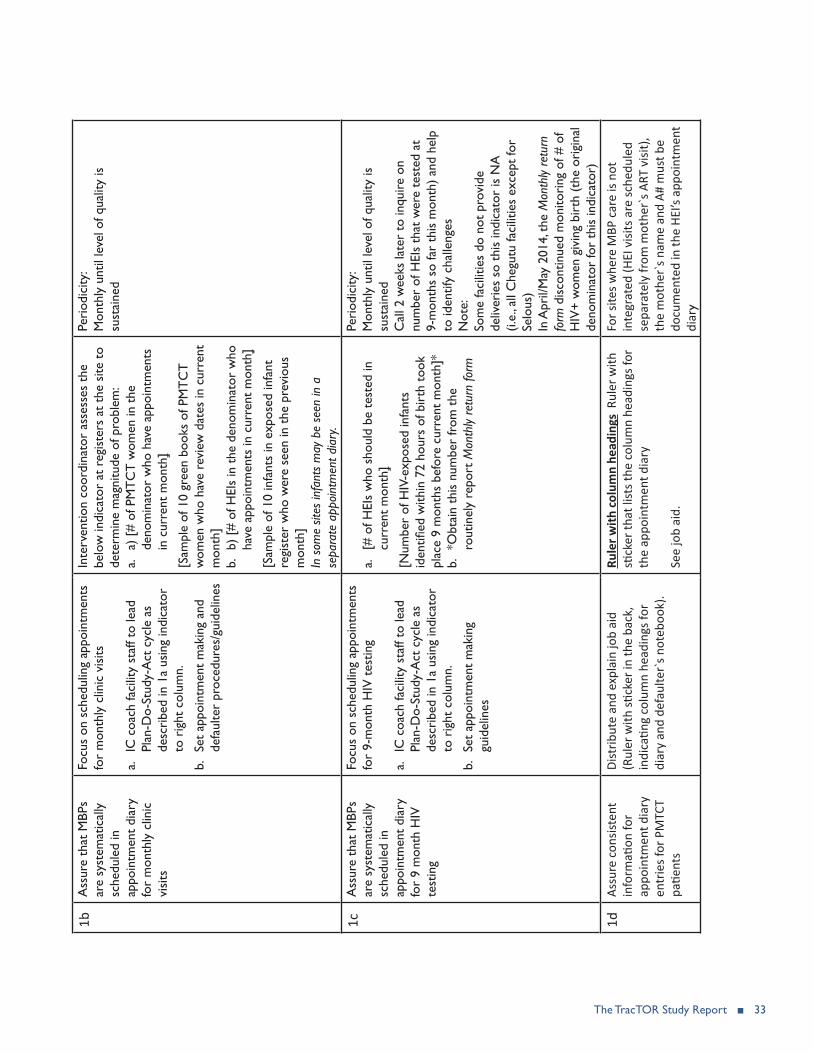
The TracTOR Study Report ■ 33
1bA
ssur
e th
at M
BPs
are
syst
emat
ical
ly
sche
dule
d in
ap
poin
tmen
t di
ary
fo
r m
onth
ly c
linic
vi
sits
Focu
s on
sch
edul
ing
appo
intm
ents
fo
r m
onth
ly c
linic
vis
its
a. IC
coa
ch fa
cilit
y st
aff t
o le
ad
Plan
-Do-
Stud
y-A
ct c
ycle
as
desc
ribe
d in
1a
usin
g in
dica
tor
to r
ight
col
umn.
b.
Set
appo
intm
ent
mak
ing
and
defa
ulte
r pr
oced
ures
/gui
delin
es
Inte
rven
tion
coor
dina
tor
asse
sses
the
be
low
indi
cato
r at
reg
iste
rs a
t th
e si
te t
o de
term
ine
mag
nitu
de o
f pro
blem
:a.
a) [
# of
PM
TC
T w
omen
in t
he
deno
min
ator
who
hav
e ap
poin
tmen
ts
in c
urre
nt m
onth
]
[Sam
ple
of 1
0 gr
een
book
s of
PM
TC
T
wom
en w
ho h
ave
revi
ew d
ates
in c
urre
nt
mon
th]
b.
b) [
# of
HEI
s in
the
den
omin
ator
who
ha
ve a
ppoi
ntm
ents
in c
urre
nt m
onth
]
[Sam
ple
of 1
0 in
fant
s in
exp
osed
infa
nt
regi
ster
who
wer
e se
en in
the
pre
viou
s m
onth
]In
som
e sit
es in
fant
s m
ay b
e se
en in
a
sepa
rate
app
oint
men
t dia
ry.
Peri
odic
ity:
Mon
thly
unt
il le
vel o
f qua
lity
is
sust
aine
d
1cA
ssur
e th
at M
BPs
are
syst
emat
ical
ly
sche
dule
d in
ap
poin
tmen
t di
ary
for
9 m
onth
HIV
te
stin
g
Focu
s on
sch
edul
ing
appo
intm
ents
fo
r 9-
mon
th H
IV t
estin
g
a. IC
coa
ch fa
cilit
y st
aff t
o le
ad
Plan
-Do-
Stud
y-A
ct c
ycle
as
desc
ribe
d in
1a
usin
g in
dica
tor
to r
ight
col
umn.
b.
Set
appo
intm
ent
mak
ing
guid
elin
es
a. [#
of H
EIs
who
sho
uld
be t
este
d in
cu
rren
t m
onth
]
[Num
ber
of H
IV-e
xpos
ed in
fant
s id
entifi
ed w
ithin
72
hour
s of
bir
th t
ook
plac
e 9
mon
ths
befo
re c
urre
nt m
onth
]*b.
*O
btai
n th
is n
umbe
r fr
om t
he
rout
inel
y re
port
Mon
thly
retu
rn fo
rm
Peri
odic
ity:
Mon
thly
unt
il le
vel o
f qua
lity
is
sust
aine
dC
all 2
wee
ks la
ter
to in
quire
on
num
ber
of H
EIs
that
wer
e te
sted
at
9-m
onth
s so
far
this
mon
th)
and
help
to
iden
tify
chal
leng
esN
ote:
Som
e fa
cilit
ies
do n
ot p
rovi
de
deliv
erie
s so
thi
s in
dica
tor
is N
A
(i.e.
, all
Che
gutu
faci
litie
s ex
cept
for
Selo
us)
In A
pril/
May
201
4, t
he M
onth
ly re
turn
fo
rm d
isco
ntin
ued
mon
itori
ng o
f # o
f H
IV+
wom
en g
ivin
g bi
rth
(the
ori
gina
l de
nom
inat
or fo
r th
is in
dica
tor)
1dAs
sure
con
siste
nt
info
rmati
on fo
r ap
poin
tmen
t dia
ry
entr
ies f
or P
MTC
T pa
tient
s
Dist
ribut
e an
d ex
plai
n jo
b ai
d (R
uler
with
stick
er in
the
back
, in
dica
ting
colu
mn
head
ings
for
diar
y an
d de
faul
ter`
s not
eboo
k).
Rule
r with
col
umn
head
ings
Rul
er w
ith
stick
er th
at li
sts t
he c
olum
n he
adin
gs fo
r th
e ap
poin
tmen
t dia
ry
See
job
aid.
For s
ites w
here
MBP
car
e is
not
inte
grat
ed (H
EI v
isits
are
sche
dule
d se
para
tely
from
mot
her`
s ART
visi
t),
the
mot
her`
s nam
e an
d A#
mus
t be
docu
men
ted
in th
e HE
I’s a
ppoi
ntm
ent
diar
y

34 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
2Pr
oces
s for
trac
king
, tra
cing
and
doc
umen
ting
defa
ulte
rs
Goa
lIn
terv
enti
on a
ctiv
ity
Det
aile
d id
eas
(ple
ase
com
men
t/ex
pand
)C
omm
ents
2aA
ssur
e th
at P
MT
CT
pa
tient
s w
ho m
iss
appo
intm
ents
by
>5
days
are
sy
stem
atic
ally
sen
t to
C
HW
s
Impl
emen
t th
e fo
llow
ing
at
inte
rven
tion
site
s:
Def
aulte
r bo
x S
tore
gre
en
book
s fo
r w
omen
who
mis
s ap
poin
tmen
ts in
a D
efau
lter
Box
Box
dim
ensi
ons
(~2
boxe
s pe
r si
te):
Wid
th: 1
1.5
to 1
2 in
Hei
ght:
8 in
ches
(yo
u ca
n cu
t th
is
to s
ize)
Dep
th: a
nyD
efau
lter
note
book
Tra
ck (
i.e.,
docu
men
t) w
omen
who
mis
s ap
poin
tmen
ts u
sing
a n
oteb
ook
atta
ched
to
box,
follo
win
g co
lum
n he
adin
gs o
n th
e sa
me
rule
r as
the
ap
poin
tmen
t di
ary.
1. D
efau
lter
box
We
wou
ld li
ke t
he g
reen
boo
ks in
the
def
aulte
r bo
x to
be
filed
in o
rder
of M
issed
Rev
iew
Dat
e , a
nd in
suc
h a
way
tha
t th
e A
# is
eas
ily
visi
ble.
To
faci
litat
e id
entif
ying
gre
en b
ooks
of c
lient
s w
ho d
efau
lt in
car
e (i.
e.,
mis
s th
eir
appo
intm
ents
by
> 5
days
) w
e su
gges
t us
ing
a la
rge
book
mar
k th
at
can
be m
oved
to
mar
k th
ose
gree
n bo
oks
of c
lient
s th
at h
ave
mis
sed
thei
r re
view
dat
es—
such
clie
nts
wou
ld t
hen
be w
ritt
en in
to t
he D
efau
lter
note
book
.
2. D
efau
lter
not
eboo
k T
his
note
book
wou
ld li
st e
ach
MBP
tha
t m
isse
d ap
poin
tmen
ts b
y >5
day
s (i.
e., d
efau
lter)
and
who
are
cur
rent
ly b
eing
follo
wed
up
by
all C
HW
s at
tha
t si
te.
Plea
se r
efer
to
the
prot
otyp
e of
the
def
aulte
r no
tebo
ok.
Faci
lity
staf
f wou
ld fi
ll ou
t…:
Fiel
ds (
i.e.,
colu
mns
) 1-
5 in
the
def
aulte
r no
tebo
ok d
aily
at t
he e
nd o
f eac
h da
y, w
hen
clin
ic s
taff
iden
tify
the
MBP
s th
at m
isse
d th
eir
appo
intm
ents
for
the
day.
Fiel
ds 6
-7 w
ould
be
fille
d ou
t w
eekl
y by
the
FFP
as
defa
ulte
rs a
re id
entifi
edFi
elds
8-9
wou
ld b
e fil
led
out
mon
thly
duri
ng t
he C
HW
mee
ting
as e
ach
CH
W
repo
rts
on t
he r
esul
ts o
f the
ir t
raci
ng e
ffort
sFi
elds
10
may
be
fille
d ou
t da
ily a
s ap
prop
riat
e, w
hen
a re
turn
ed d
efau
lter
MBP
sh
ows
up fo
r an
app
oint
men
t. If
clin
ic s
taff
dete
rmin
es t
he M
BP is
a c
lient
who
pr
evio
usly
mis
sed
a re
view
dat
e, s
taff
retr
ieve
s th
e cl
ient
’s gr
een
book
in t
he
defa
ulte
r bo
x, a
nd u
pdat
es d
efau
lter
note
book
by
ente
ring
RT
C. M
onth
ly, t
his
field
m
ay b
e up
date
d du
ring
the
CH
W m
eetin
g as
app
ropr
iate
, if a
CH
W r
epor
ts t
hat
a cl
ient
is fi
nally
iden
tified
as
Dec
ease
d or
LT
FU.
2bD
ocum
ent
outc
ome
of t
raci
ng e
ffort
s by
pa
tient
at
the
clin
ic
leve
l (se
e 3b
)
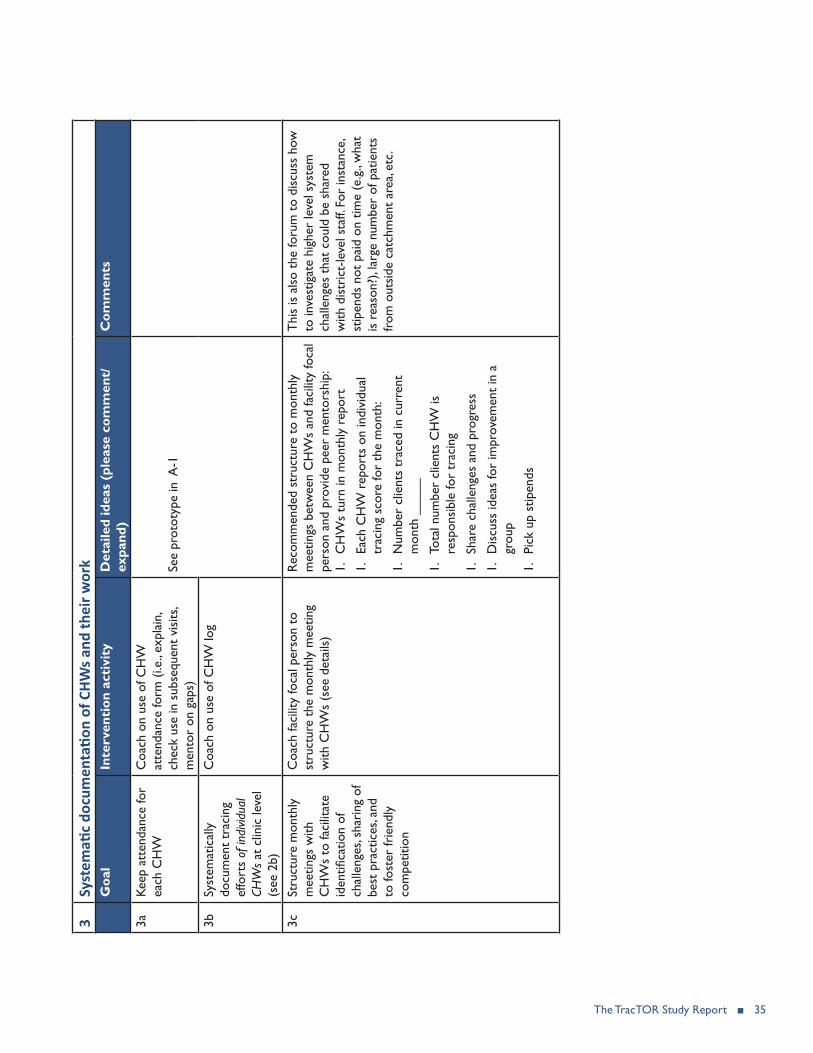
The TracTOR Study Report ■ 35
3Sy
stem
atic
docu
men
tatio
n of
CHW
s and
thei
r wor
kG
oal
Inte
rven
tion
act
ivit
yD
etai
led
idea
s (p
leas
e co
mm
ent/
expa
nd)
Com
men
ts
3aKe
ep a
tten
danc
e fo
r ea
ch C
HW
Coa
ch o
n us
e of
CH
W
atte
ndan
ce fo
rm (
i.e.,
expl
ain,
ch
eck
use
in s
ubse
quen
t vi
sits
, m
ento
r on
gap
s)Se
e pr
otot
ype
in A
-1
3bSy
stem
atic
ally
do
cum
ent
trac
ing
effo
rts
of in
divid
ual
CHW
s at
clin
ic le
vel
(see
2b)
Coa
ch o
n us
e of
CH
W lo
g
3cSt
ruct
ure
mon
thly
m
eetin
gs w
ith
CH
Ws
to fa
cilit
ate
iden
tifica
tion
of
chal
leng
es, s
hari
ng o
f be
st p
ract
ices
, and
to
fost
er fr
iend
ly
com
petit
ion
Coa
ch fa
cilit
y fo
cal p
erso
n to
st
ruct
ure
the
mon
thly
mee
ting
with
CH
Ws
(see
det
ails
)
Rec
omm
ende
d st
ruct
ure
to m
onth
ly
mee
tings
bet
wee
n C
HW
s an
d fa
cilit
y fo
cal
pers
on a
nd p
rovi
de p
eer
men
tors
hip:
1.
CH
Ws
turn
in m
onth
ly r
epor
t
1.
Each
CH
W r
epor
ts o
n in
divi
dual
tr
acin
g sc
ore
for
the
mon
th:
1.
Num
ber
clie
nts
trac
ed in
cur
rent
m
onth
___
__
1.
Tota
l num
ber
clie
nts
CH
W is
re
spon
sibl
e fo
r tr
acin
g
1.
Shar
e ch
alle
nges
and
pro
gres
s
1.
Dis
cuss
idea
s fo
r im
prov
emen
t in
a
grou
p
1.
Pick
up
stip
ends
Thi
s is
als
o th
e fo
rum
to
disc
uss
how
to
inve
stig
ate
high
er le
vel s
yste
m
chal
leng
es t
hat
coul
d be
sha
red
with
dis
tric
t-le
vel s
taff.
For
inst
ance
, st
ipen
ds n
ot p
aid
on t
ime
(e.g
., w
hat
is r
easo
n?),
larg
e nu
mbe
r of
pat
ient
s fr
om o
utsi
de c
atch
men
t ar
ea, e
tc.
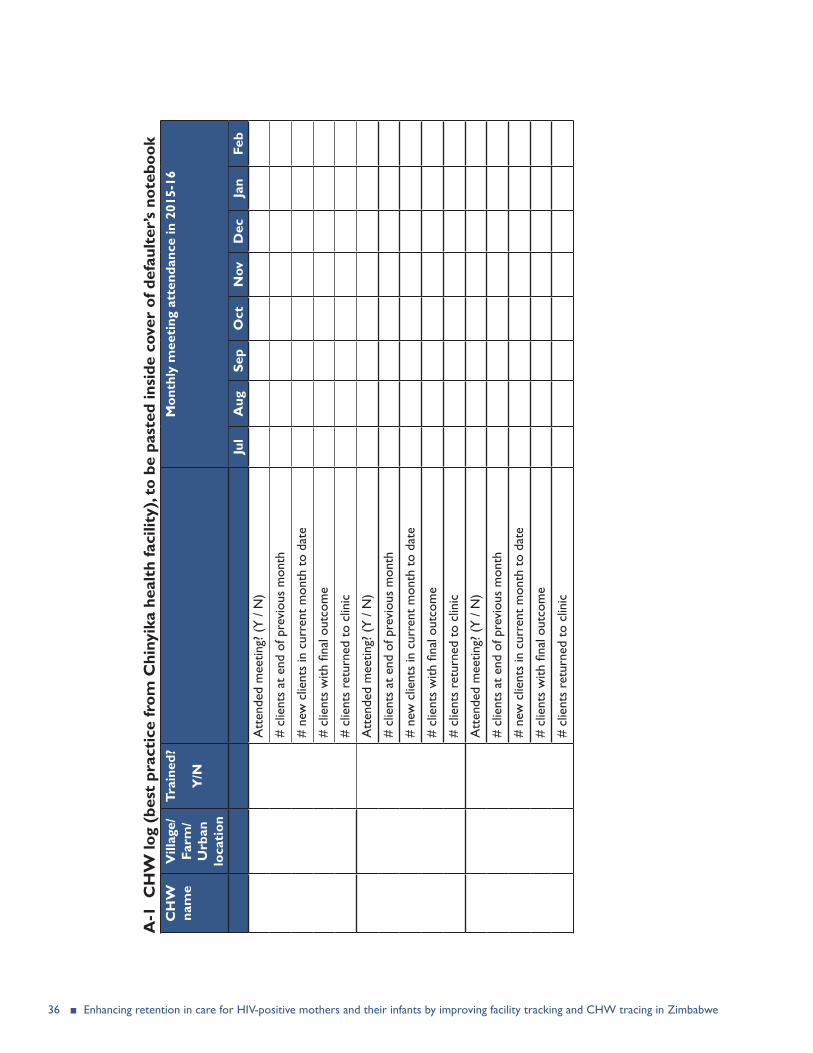
36 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
A-1
CH
W lo
g (b
est
prac
tice
from
Chi
nyik
a he
alth
faci
lity)
, to
be p
aste
d in
side
cov
er o
f def
ault
er’s
note
book
CH
W
nam
eV
illag
e/Fa
rm/
Urb
an
loca
tion
Trai
ned?
Y/N
Mon
thly
mee
ting
att
enda
nce
in 2
015-
16
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Att
ende
d m
eetin
g? (
Y /
N)
# cl
ient
s at
end
of p
revi
ous
mon
th
# ne
w c
lient
s in
cur
rent
mon
th t
o da
te
# cl
ient
s w
ith fi
nal o
utco
me
# cl
ient
s re
turn
ed t
o cl
inic
Att
ende
d m
eetin
g? (
Y /
N)
# cl
ient
s at
end
of p
revi
ous
mon
th
# ne
w c
lient
s in
cur
rent
mon
th t
o da
te
# cl
ient
s w
ith fi
nal o
utco
me
# cl
ient
s re
turn
ed t
o cl
inic
Att
ende
d m
eetin
g? (
Y /
N)
# cl
ient
s at
end
of p
revi
ous
mon
th
# ne
w c
lient
s in
cur
rent
mon
th t
o da
te
# cl
ient
s w
ith fi
nal o
utco
me
# cl
ient
s re
turn
ed t
o cl
inic

The TracTOR Study Report ■ 37
A-2 Visual representation of Appointment Diary Ruler and Defaulter Notebook Ruler, with sticker indicating column headings
RULER FRONT
RULER BACK, APPOINTMENT DIARY would include a sticker with column headings that should be included in the appointment diary (2–5)
(2) Mother’s full name (3) ART number (4) Phone (5) Address
RULER BACK, DEFAULTER’S NOTEBOOK would include a sticker with column headings that should be included in the defaulter’s notebook (1–10)
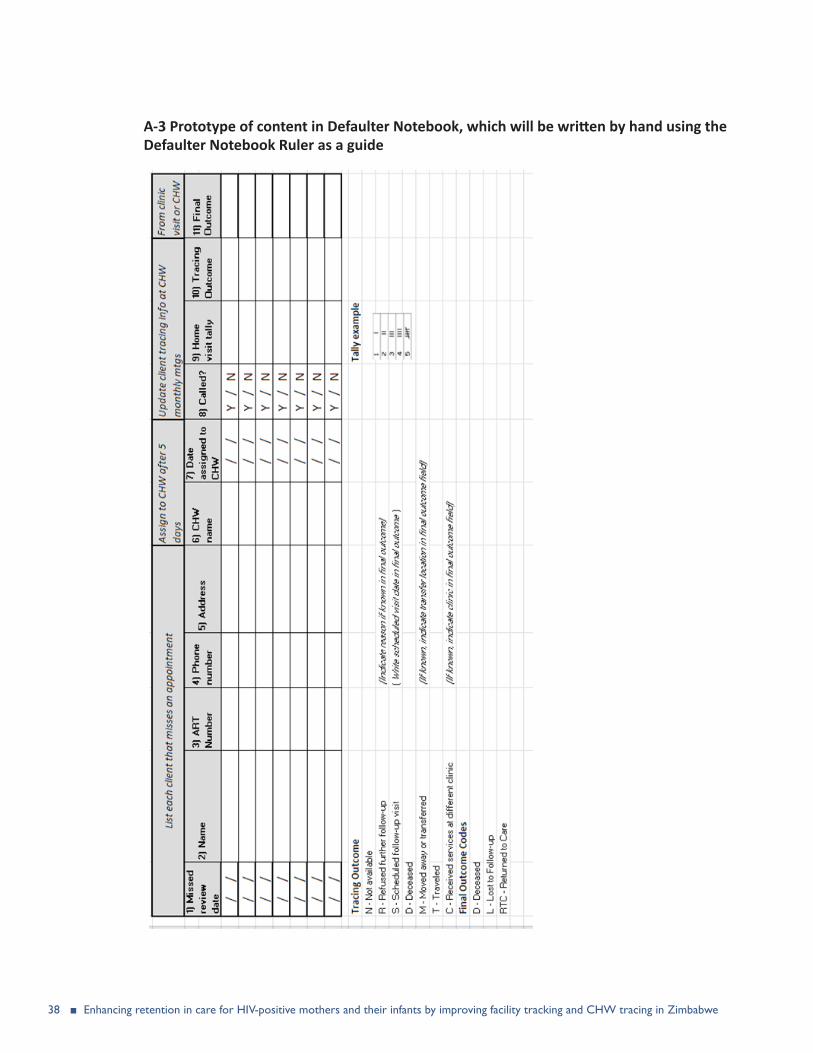
38 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
A-3 Prototype of content in Defaulter Notebook, which will be written by hand using the Defaulter Notebook Ruler as a guide

The TracTOR Study Report ■ 39
A-4 SOP for clinic staff to track and trace defaulters
Materials: y Defaulter box (ideally: handles for easy carrying; 11-12” or 23-24” width x 9-10” height x 20-30” depth)
Defaulter notebook (A-3), which will be set up by hand using the Defaulter notebook rulerDefaulter notebook ruler (A-2) y Large bookmark (thick cardboard or plastic card, 9” x 11”)
1. Daily: Prepare appointment diary for use Take the Defaulter Notebook Ruler (A-2) as a straight edge to mark columns (2) to (5) as indicated in the ruler sticker. Copy the column headings on to the notebook—do this for several pages. a) Set appointments at the end of each day For all clients that attended the clinic on the current date,
transfer their next review date in their green book to the appointment diary under the appropriate review date
b) File clients who missed appointments in Defaulter box For each patient who missed their review date on the current date: i) Call patient and provide reminder that appointment was missedii) Collect mothers’ green books and file in defaulter box in order of date of missed review date
(1) This box will be the location to search for green books of patients who show up at the clinic and are not listed in the appointment diary on that date
iii) Write the following column headings for that patient in notebook attached to defaulter box:(1) Missed review date (2) Mother’s full name(3) A#(4) Phone number (5) Address (6) CHW name(7) Date name provided to CHW(8) Home visit tally(9) Tracing outcome (N = Not available | R = Refused further follow-up (Indicate reason) |S =
Scheduled follow-up visit | D = Deceased | M = Moved away or transferred (If known, indicate transfer location) | T = Traveled |C = Received services from a different clinic (indicate clinic))
(10) Final outcome (D = Deceased| L = Lost To Follow Up | RTC = Returned to Care | Additional comments)
c) Prepare for next dayi) Identify PMTCT clients (mothers and infants) that have appointments the next day, and pull out
their green books so that they are easily accessible the next day
1) Daily: When clients arrive at the clinic for their appointments…a) Ask for the client’s name and HIV card, and locate her in the appointment diary under the page for
the current dateb) If you can locate the client listed under to-day`s date

40 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
i) Add a checkmark next to the client`s entry in the diary to indicate she attended the clinic ii) Locate the client`s green book among the regular green book files
c) If the client’s name is not listed under to-day’s date, i) Find out on patient booklet or by asking the patient when she was supposed to be at the clinic,
and search for her in the diary and the Defaulter`s Box ii) Update the client`s information in the defaulter`s notebook (i.e., write RTC under (10) Final
outcome)iii) After client is seen, update green book and/or infant exposed register accordingly
2) Weekly:a) Send list of defaulters to the corresponding CHW
i) Move the bookmark to identify patients who missed review date by 5 days ii) If resources allow, call defaulting patients to provide a reminder to attend cliniciii) If not reached by phone:
(1) Write lists of defaulters to provide to each CHWs, based on the CHW’s coverage area (i.e., village/farm/etc.)
(2) Communicate with the CHW to provide him/her the list of defaulters to follow up on using whichever method the facility is already using (e.g., SMS, provide paper list in person directly to CHW etc.). One strategy would be to provide a weekly list to CHWs by phone text, and confirm the list during the monthly CHW meeting.
(3) Document CHW assignment in defaulter’s notebook
3) Monthly:a) Intervention coordinator (IC) meets with facility focal person (FFP) at each of the 11
intervention facilities for coaching:i) Activities to improve use of appointment diary
(1) Prior to meeting with FFP, IC measures indicators 1a, 1b, 1c (a) Prior to the very first meeting, IC should measure baseline levels the indicators. In other
words: (i) 1a: would be measured as defined earlier (i.e., no adjustment necessary)(ii) 1b: baseline indicator would be measured as such:
[# of PMTCT women in the denominator who had appointments in previous month] [Sample of 10 green books of PMTCT women who had review dates in the previous month]
(iii) 1c: baseline indicator would be measured as such:
[# of HEIs who should be tested in current month][Number of HIV-exposed infants identified within 72 hours of birth took
place 9 months before current month]
(b) To “randomly” identify 10 green books for 1a and 1b:(i) At each site, keep a written list of numbers from 1 to 30 in the back of the
Defaulter’s Notebook.
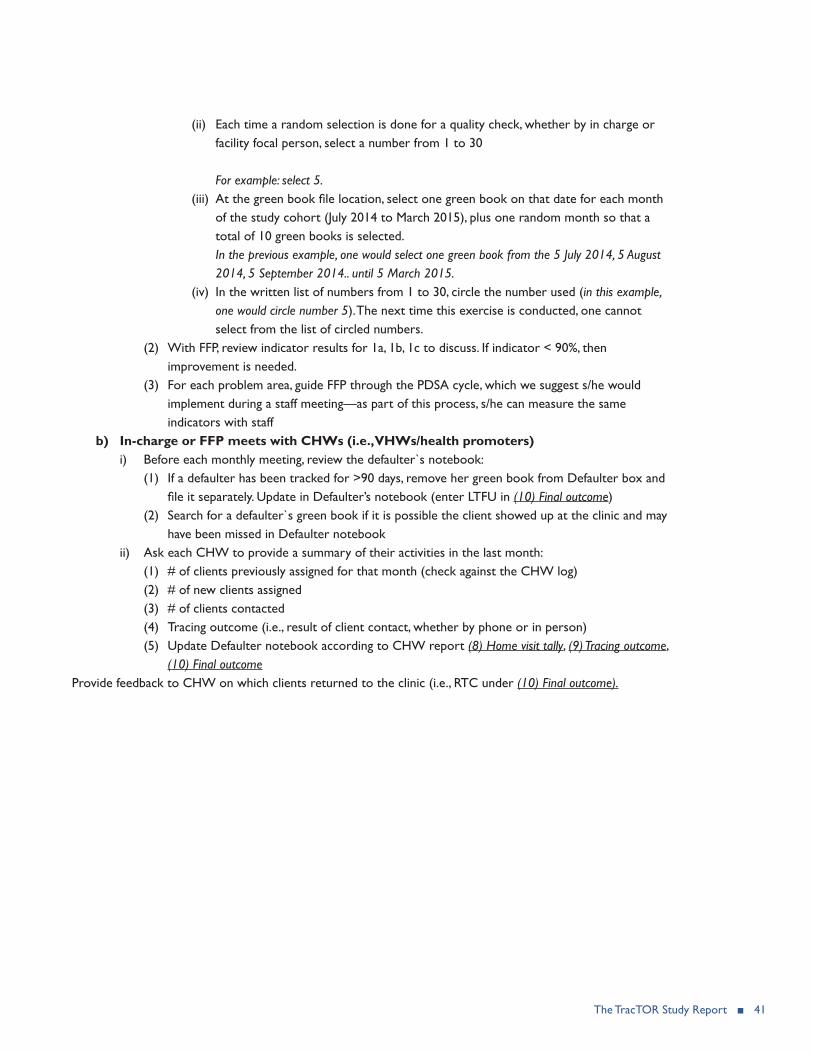
The TracTOR Study Report ■ 41
(ii) Each time a random selection is done for a quality check, whether by in charge or facility focal person, select a number from 1 to 30
For example: select 5.(iii) At the green book file location, select one green book on that date for each month
of the study cohort (July 2014 to March 2015), plus one random month so that a total of 10 green books is selected. In the previous example, one would select one green book from the 5 July 2014, 5 August 2014, 5 September 2014.. until 5 March 2015.
(iv) In the written list of numbers from 1 to 30, circle the number used (in this example, one would circle number 5). The next time this exercise is conducted, one cannot select from the list of circled numbers.
(2) With FFP, review indicator results for 1a, 1b, 1c to discuss. If indicator < 90%, then improvement is needed.
(3) For each problem area, guide FFP through the PDSA cycle, which we suggest s/he would implement during a staff meeting—as part of this process, s/he can measure the same indicators with staff
b) In-charge or FFP meets with CHWs (i.e., VHWs/health promoters)i) Before each monthly meeting, review the defaulter`s notebook:
(1) If a defaulter has been tracked for >90 days, remove her green book from Defaulter box and file it separately. Update in Defaulter’s notebook (enter LTFU in (10) Final outcome)
(2) Search for a defaulter`s green book if it is possible the client showed up at the clinic and may have been missed in Defaulter notebook
ii) Ask each CHW to provide a summary of their activities in the last month:(1) # of clients previously assigned for that month (check against the CHW log) (2) # of new clients assigned(3) # of clients contacted (4) Tracing outcome (i.e., result of client contact, whether by phone or in person)(5) Update Defaulter notebook according to CHW report (8) Home visit tally, (9) Tracing outcome,
(10) Final outcomeProvide feedback to CHW on which clients returned to the clinic (i.e., RTC under (10) Final outcome).

42 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
APPENDIX 3 SOP FOR PATIENT TRACING IN HEALTH FACILITIES IN ZIMBABWE
Ministry of Health and Child Care
Standard Operating Procedures for Patient Tracing in Health Facilities in Zimbabwe

The TracTOR Study Report ■ 43
1. Introduction
1.1. Background
Zimbabwe’s Ministry of Health and Child Care (MOHCC) has been implementing the prevention of mother-to-child transmission (PMTCT) of HIV program since 2000 when single-dose Nevirapine (sd-NVP) was the recommended PMTCT regimen for mother-baby pairs. In 2010, Zimbabwe adopted Option A of the World Health Organization (WHO) 2010 Guidelines for PMTCT, which were rolled out countrywide in 2011. Following the launch of the Global Plan for Elimination of New HIV Infections in Children and Keeping Mothers Alive8 in June 2011 in New York, Zimbabwe developed its own national elimination of mother-to-child transmission (eMTCT) strategic plan for the period 2012-2015. The goal of the strategic plan is the elimination of new HIV infections among children by 2015 and improving the survival of mothers and children in the context of HIV. The new strategy seeks to scale up all four pillars of PMTCT including: primary prevention of HIV infection for reproductive women; prevention of unintended pregnancies; provision of antiretrovirals (ARVs) for prophylaxis; and antiretroviral therapy (ART) to all pregnant and lactating women who need it for their own health including provision of ARVs for prophylaxis to all HIV-exposed infants, as well as providing comprehensive family centered HIV care and treatment9.
By the end of 2012, more than 1,380 health facilities in Zimbabwe were offering PMTCT services according to Option A of the 2010 WHO guidelines. To attain virtual elimination of pediatric HIV and achieve the best possible outcomes for mothers and their infants, women will need to be tested for HIV, and to start ART as early as 14 weeks gestational age. They will also need to return repeatedly for antenatal care (ANC) visits, deliver their babies at health facilities, and continue to adhere to the prevention/treatment recommendations throughout ANC and the breastfeeding period. Yet globally, PMTCT programs are hampered by high loss to follow up rates even with simple ARV regimens. Figure 1 below shows a typical PMTCT cascade, which highlights loss to follow up (missed opportunities) at every stage.
8Global Plan Towards The Elimination Of New HIV Infections Among Children By 2015 And Keeping Their Mothers Alive, Joint United Nations Programme on HIV/AIDS (UNAIDS), June 20119Zimbabwe National Strategic Plan for Eliminating New Paediatric HIV Infections in Children and Keeping Mothers and Families Alive: 2011-2015

44 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
Figure 1: Typical PMTCT Cascade with Missed Opportunities
Most women in Zimbabwe who attend ANC are tested for HIV and receive their results on the day of testing. Of the women identified as HIV positive during pregnancy, not all receive ARV prophylaxis and fewer go on to be assessed for ART eligibility by CD4 testing. Of those that do receive ARVs, it is not known how many of these women are adherent to the regimen. Furthermore, a significant number of their infants do not receive ARV prophylaxis at birth nor are they initiated on Cotrimoxazole (CTX) prophylaxis at 6 weeks and even fewer of those infants go on to access early infant diagnosis (EID) and therefore have no access to lifesaving ART. The adaptation of the 2010 WHO PMTCT guidelines calls for early ANC booking, an extended period of maternal and infant ARV prophylaxis, good adherence and retention of clients in care and treatment, as well as more stringent longitudinal follow up and retention in care for both mothers and babies in order to achieve elimination of new HIV infections by 2015 in children and for keeping their mothers alive. Effective patient tracing systems and strategies therefore need to be developed so as to be able to identify mother-baby pairs that are not attending scheduled clinic visits and trace them back into care.
The MOHCC, with support from the Elizabeth Glaser Pediatric AIDS Foundation (EGPAF), is piloting an electronic database (EDB) that captures client-level information in 36 health facilities across five districts. The EDB helps in the identification of patients who would have missed their clinic appointments and therefore require tracing in the community; however it is currently difficult for health workers to identify defaulting clients in health facilities without the EDB.
One of the key strategies for improving retention of patients within care and treatment is having a functional patient tracing mechanism at all health facilities offering PMTCT services. The patient tracing mechanism should be integrated with the health system in which community health workers, particularly Village Health Workers (VHWs) play a critical role. Currently there are no documented Standard Operating Procedures (SOPs) for patient tracing within Zimbabwe’s national PMTCT program. It is against this background that systems for patient tracking need to be put in place to identify mother-baby pairs that have not kept their clinic appointments and then to actively trace these pairs to limit drop outs from HIV care and treatment. It is envisaged that SOPs for patient tracing will help health workers to identify mother-baby pairs lost to

The TracTOR Study Report ■ 45
follow up and trace them back into care and treatment.
1.2. Overview of Village Health Work in Zimbabwe
The MOHCC established a village health worker program in the early 1980s. The main purpose of the village health worker program is to form a linkage between the formal health delivery system and communities, thereby ensuring community participation and ownership in health issues. In addition to VHWs, the MOHCC also works with community-based health workers who include community based distributors (CBDs) of family planning commodities, peer facilitators, male champions, home-based care providers and behavior change facilitators among others. The core activities undertaken by VHWs include raising community awareness and education on health-related issues; growth monitoring for children under five years of age; management, control and reporting of communicable disease outbreaks to health facilities. Other VHW activities include distribution of commodities such as mosquito bed nets and family planning commodities; treatment of minor ailments; reinforcing adherence to treatment for clients on chronic care; tracing of clients defaulting treatment, as well as referral of clients identified in the community to nearby health facilities.
Within the formal health system, community-based health workers are coordinated by the VHW who is supported by the Community Health Nurses; however, various other professional cadres interact directly and provide technical guidance to village health workers. These other cadres include health workers at primary-level facilities and Environmental Health Technicians (EHTs) at rural health centers. The Community Health Nurses work in collaboration with EHTs and health promotion officers.
VHWs are found in all districts of the country and are primarily supported by the MOHCC. Other community-based health workers (e.g. male champions and home-based care providers) are often supported by Non-Governmental Organizations and development partners and therefore not available in every district. Village health workers meet monthly with facility-level health workers (in most cases, every month end). The purpose of these meetings is to submit basic reports and discuss activities of the VHWs, health challenges being faced in the communities, success stories, sharing experiences and lessons learned.
The MOHCC developed draft tools (registers and reporting forms) for use by village health workers; however, these have neither been printed nor distributed. Some districts receive additional support for village health workers from various partners who often introduce reporting tools that emphasize the partners’ particular area of interest. Where there is no partner support, village health workers use the MOHCC tools to document and report their community health activities; therefore, there is presently no standardized reporting by these cadres.
1.3. Purpose of SOPs for Patient Tracing
The purpose of these SOPs is to provide facility-level health workers and village health workers with guidelines on procedures for patient tracing of clients in the community to improve retention of mother-baby pairs within HIV care and treatment. The procedures for patient tracing include the following;
• Identification of active community-based health workers in the area served by a health facility;• Identification of clients who need follow up; • Communication between facility-level health workers and community-based health workers;

46 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
• Patient tracing in the community; and• Feedback from community-based health workers.
These SOPs also outline roles and responsibilities of facility-level and village health workers in patient tracing, the monitoring and evaluation (M&E) tools required for tracing, as well as serve as a guide for capacity building of facility-level health workers and village health workers in patient tracing.
1.4. Users of the SOPs
These standard operating procedures can be used by programs in which patient tracing is required. These SOPs are intended for use by:
• Village health workers• Facility-level health workers
2. Patient Tracing
2.1. Identification of Village Health Workers
Facility-level health workers should identify the active village health workers serving their catchment areas. An inventory of all village health workers should be kept at the health facility and efforts should be made to periodically assess functionality of these cadres. This inventory should include capacity building needs of village health workers in line with current national guidelines for the various programs that facilities will be implementing.
2.2 Patient Identification at Health Facilities
Facility-level health workers traditionally use the standard registers for identification of patients who require follow up in the community; however, the use of these registers is limited because some are not longitudinal (i.e. the same client is recorded on different pages for every visit and therefore the health workers need to flip through pages to identify when clients came for their scheduled clinic appointments). In addition, clients may not be given specific days to return to the health facility.
Facility-level health workers should ensure that:
• Upon registration, every client who receives services at the health facility is recorded in the relevant national register(s).
• Each client is assigned a unique, program-specific identifier such as a pregnancy number for women booking for ANC.
• All relevant fields in the register(s) are completed each time a client comes for follow-up visits.• Each client is given a review date and this date is documented in the relevant field of the register(s).• Each client is documented in an appointment diary:
o Clients should be documented against the date when they are due for review; ando Client’s full name, physical address and phone number should be documented.

The TracTOR Study Report ■ 47
• They make use of the appointment diary on every clinic day:o Clients who came to the facility on their appointment dates should be marked to
differentiate them from those who failed to turn up.• At the end of the week, a list of all clients who failed to turn up on their appointment date and within
five days of this date should be prepared:o The list should have clients’ physical address, telephone number where applicable and the
name of village health worker for the respective address.• At the end of every month, a complete list of all defaulting clients identified that month should be shared
with village health workers during the monthly meetings.
2.3. Communication between Facility and Village Health Workers
On the last day of every week, facility-level health workers should communicate with village health workers. Facility-level health workers should:
• Make use of any means of communication available (e.g. cell phones) to communicate with village health workers.
• For village health workers with cell phones, facility-level health workers should send a call me back message to the village health worker
o Upon receiving the message and conditions permitting, the village health worker should immediately report to the health facility.
• For village health workers without cell phones, health workers can make use of school children, clients, or any person to convey the message.
• Upon arrival at the health facility, the village health worker should be given a complete list of clients in their catchment area that missed their clinic appointments.
• Communication between facility health workers and village health workers should be continuous throughout the month to ensure timely and continuous tracking of clients.
2.4. Patient Tracing in the Community
Village health workers should conduct physical follow-up of all clients who have missed their clinic appointments. Village health workers should ensure that:
• All clients that were followed up are documented in the village health worker register• All followed up clients have been issued a referral slip to take to the health facility• The referral slip includes the reasons for referral
o Upon arrival at the health facility, the referred client should hand over the referral slip to the nurse, who in turn should give the tear off section to the client to take back to the village health worker;
o Clinic nurses should update all relevant registers and clearly indicate in the appointment register that the client has reported to the health facility including date seen
48 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
• All followed up clients are provided with health education and counseling on the importance of adherence to treatment
• All referred clients are advised to submit the tear off section of the referral slip to the village health worker after visiting the health facility as evidence of completion of referral
• Tracing of clients should continue for 90 days from the scheduled clinic appointment date before a patient is declared lost to follow up
2.5. Feedback from Community-Based Health Workers
Facility-level health workers should ensure that monthly meetings are held with VHWs. During these monthly meetings village health workers should:
• Share reports of follow-up outcomes with facility-level health workers. • Share a list of clients they failed to reach or locate.• Share their success stories and challenges with regards to client tracing.
During the monthly meeting, facility-level health workers should:
• Share with village health workers a list of clients who reported to health facility and those who failed to do so.
• Collect the list of clients who the village health workers failed to reach or locate and share this list with Environmental Health Technicians (EHTs)
o EHTs should assist with follow-up of these hard to reach clients using motorbikes.
3. M&E Tools for Patient Tracing
3.1. Health Facility Appointment Diary
The health facility appointment diary is an A4 diary with a calendar used by health workers to record clinic appointments for patients. Facility-level health workers should:
• Ensure that the appointment diary is available at all service delivery points.• All clients with review dates are documented in the appointment diary; clients should be documented
against their scheduled clinic appointment dateo Client identification information to be documented include: full name, physical address,
unique identification number, phone number where applicable and name of village health worker in their localities.
• Document all clients who report on scheduled appointment visits.• Regularly review the appointment diary to identify clients who require tracing in the community and
generate follow up lists for the village health workers.

The TracTOR Study Report ■ 49
3.2. Village Health Worker Register
Health facility nurses should provide all village health workers with registers for capturing all clients followed up or identified in the community. The register should capture demographic information, type of client, purpose of visit and action taken by village health worker. The register should have instructions on how it should be used and should be translated into vernacular language for ease of use by village health workers. The village health worker register helps to keep track of the clients visited, the purpose of visit, actions taken by village health workers and outcome(s) of these actions. All defaulting clients visited by the village health workers should be captured in this register; this helps to monitor behavior of these clients with regards to keeping clinic appointments and taking their prescribed medicines. See Annexure 3 for a copy of the register.
3.3. Village Health Worker Referral Slip
Health facility nurses should provide all village health workers with referral slips for use when they follow up and refer clients to health facilities. The referral slip should have a tear off section, which the referred clients should take back to village health workers after visiting a health facility. The referral slip should capture patient identification information, referral date and reasons for referral. The referral slip should be handed over by the village health worker to the referred client to take to the health facility. At the health facility, the nurse should deposit the slip into a box and give the tear off slip to the client to take back to the village health worker. The use of the referral slip ensures that there is linkage between village health workers and nurses with regards to client tracing in the community; it serves as evidence that patient tracing is occurring. See Annexure 4 for a copy of the referral slip.
3.4. Reporting Patient Tracing Activities
All village health workers should report their monthly activities to their respective health facilities. Health facility nurses should provide village health workers with a standard monthly progress report form (Annexure 1) to summarize their community-based activities including client tracing. The monthly report can be used to assess the extent to which village health workers are tracing clients in the community, thereby contributing to retention of clients within care and treatment. Facility-level health workers should summarize activities of all village health workers and submit a monthly summary report (Annexure 2) to the DNO together with other facility summary reports. See Annexures 3 and 4 for copies of the report forms.
4. Roles and Responsibilities of Facility and Village Health Workers in Patient Tracing
4.1. Responsibility of the Community Health Nurse
Community Health Nurses are the overall managers of the village health worker program and some of their responsibilities include:
• Organizing and facilitating trainings of village health workers;• Ensuring that monthly meetings are conducted at every health facility and minutes of the meetings are
submitted to the DNO’s office on time;
50 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
• Ensuring availability of M&E tools for use by village health workers; and • Ensuring timely submission and consolidation of monthly progress reports.
4.2. Responsibilities of Facility-Level Health Workers
Facility-level health workers are responsible for:
• Documenting all relevant client-level information in M&E tools, ensuring that all fields are completed and the clients’ physical address and telephone numbers are captured;
• Identification of clients who require follow up in the community;• Generating weekly list of defaulting clients who require follow up in the community; • Notification of village health workers with regards to clients who require follow up; client identification
information including physical address and contact number should be given to the village health workers; and
• Compiling monthly reports on client tracing activities undertaken by village health workers and submitting the report to the DNO.
4.3. Responsibilities of Village Health Workers
The village health workers are responsible for:
• Identification and referral of clients in the community who have not sought service from the health center, e.g. pregnant women;
• Active follow up of all defaulting clients; • Documentation of relevant patient-level information in the village health worker register;• Referral of followed up clients to health facilities using the referral slip;• Advising clients to report back after they have visited the health facility; and• Completing and submitting monthly summary reports to the local health facility.
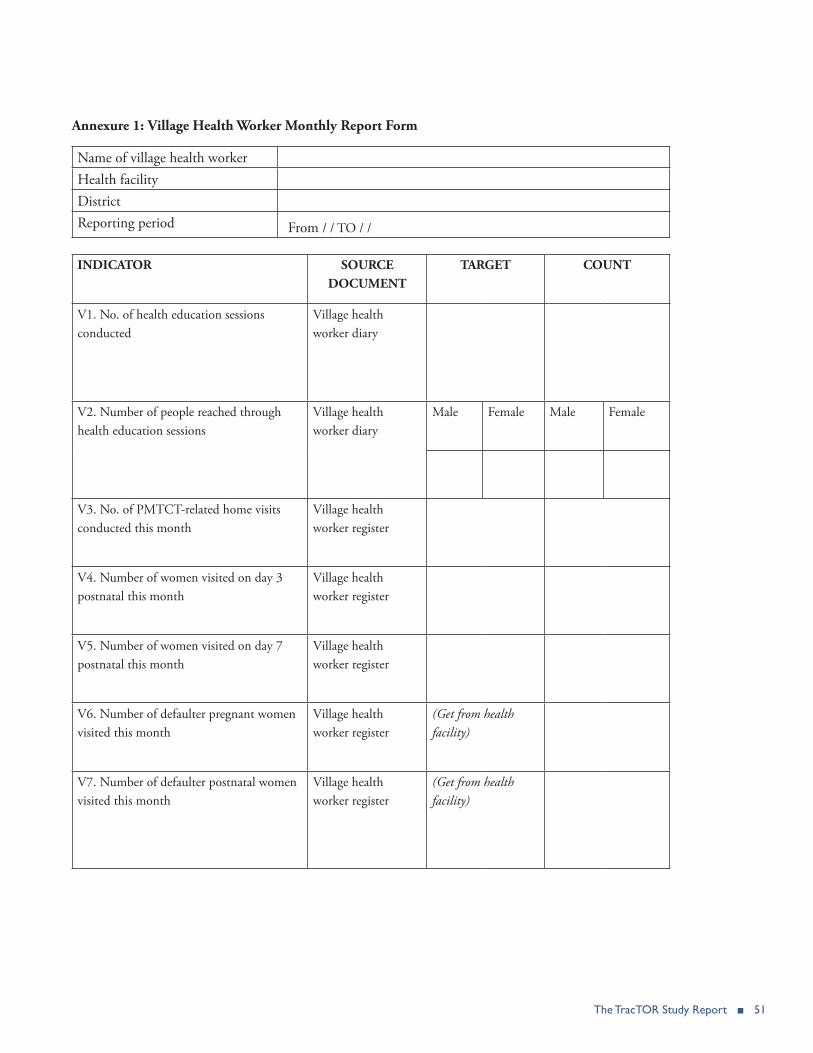
The TracTOR Study Report ■ 51
Annexure 1: Village Health Worker Monthly Report Form
Name of village health workerHealth facility DistrictReporting period From / / TO / /
INDICATOR SOURCE DOCUMENT
TARGET COUNT
V1. No. of health education sessions conducted
Village health worker diary
V2. Number of people reached through health education sessions
Village health worker diary
Male Female Male Female
V3. No. of PMTCT-related home visits conducted this month
Village health worker register
V4. Number of women visited on day 3 postnatal this month
Village health worker register
V5. Number of women visited on day 7 postnatal this month
Village health worker register
V6. Number of defaulter pregnant women visited this month
Village health worker register
(Get from health facility)
V7. Number of defaulter postnatal women visited this month
Village health worker register
(Get from health facility)
52 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
V8. Number of defaulter HIV exposed infants visited this month
Village health worker register
(Get from health facility)
V9. Number of routine follow up visits conducted this month
Village health worker register
V10. Number of home deliveries reported this month
Village health worker register
(Expected monthly home deliveries in area served by community based health worker)
V11. Number of clients referred to health facility this month
Village health worker register
V12. Number of clients counselled this month
Village health worker register

The TracTOR Study Report ■ 53
Annexure 2: Health Worker Monthly Report Form
Name of health facilityDistrictReporting period / / to / /Number of active village health workers Number of reporting village health workers
INDICATOR TARGET COUNT
V1. No. of health education sessions conducted by village health workers this month (Source: Community based health worker report)V2. Number of people reached through health education sessions
V3. No. of PMTCT-related home visits conducted by village health workers this month (Source: Community based health worker report)V4. No. of pregnant women referred for ANC booking at 14 weeks this month (Source: Referral slip) V5. No. of pregnant women referred for ANC booking after 14 weeks this month (Source: Referral slip)V6. No. of mothers visited by VHWs on day 3 postnatal this month (Source: Community based health worker report)V7. No. of mothers visited by VHWs on day 7 postnatal this month (Source: Community based health worker report)V8. No. of defaulting pregnant women followed up this month (Source: Referral slip)V9. No. of defaulting pregnant women
V10. No. of defaulting postnatal women followed up this month (Source: Referral slip)V11. No. of defaulting postnatal women
V12 No. of home deliveries referred to health facility this month (Source: Referral slip)
V13. No. of infants defaulting after 6 weeks post-delivery followed up this month (Source: Referral slip)

54 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
V14. No. of infants defaulting after 6 week post-delivery
V15. Average gestational age at booking (Source: ANC register)
V16. Number of routine follow up visits conducted by VHWs this month (Source: Community based health worker report)
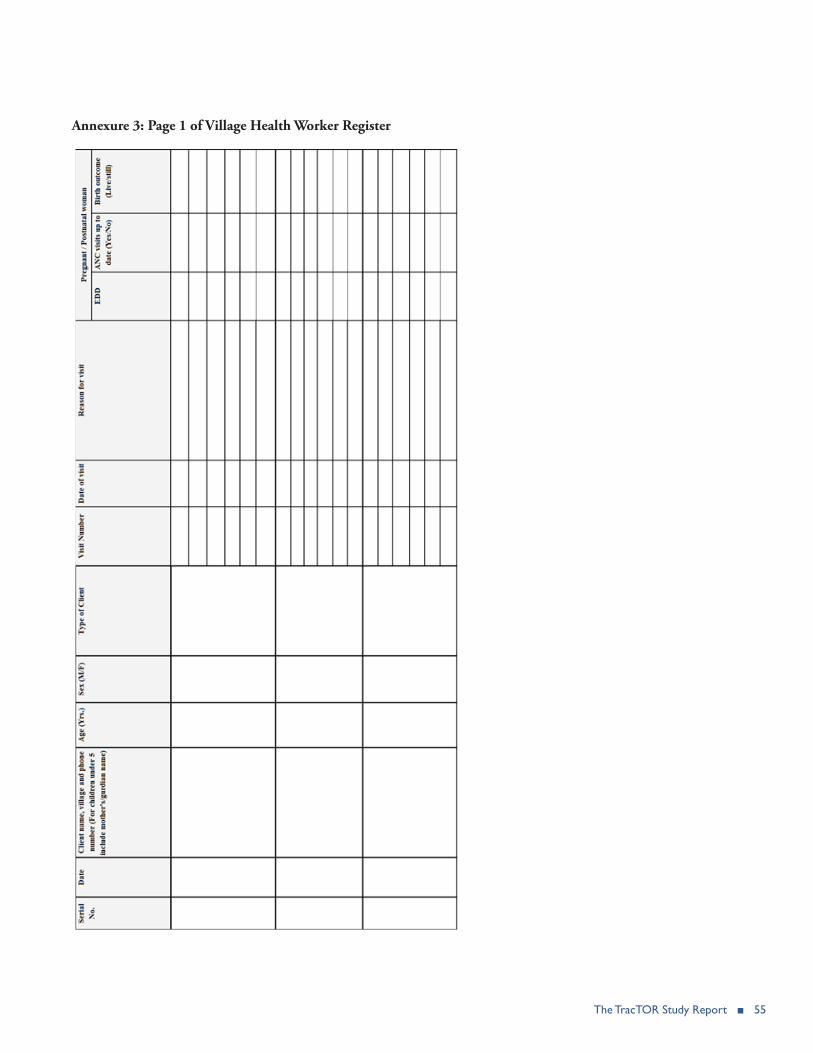
The TracTOR Study Report ■ 55
Annexure 3: Page 1 of Village Health Worker Register

56 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
Annexure 3: Page 2 of the Village Health Worker Register

The TracTOR Study Report ■ 57
Annexure 4: Village Health Worker Referral Slip
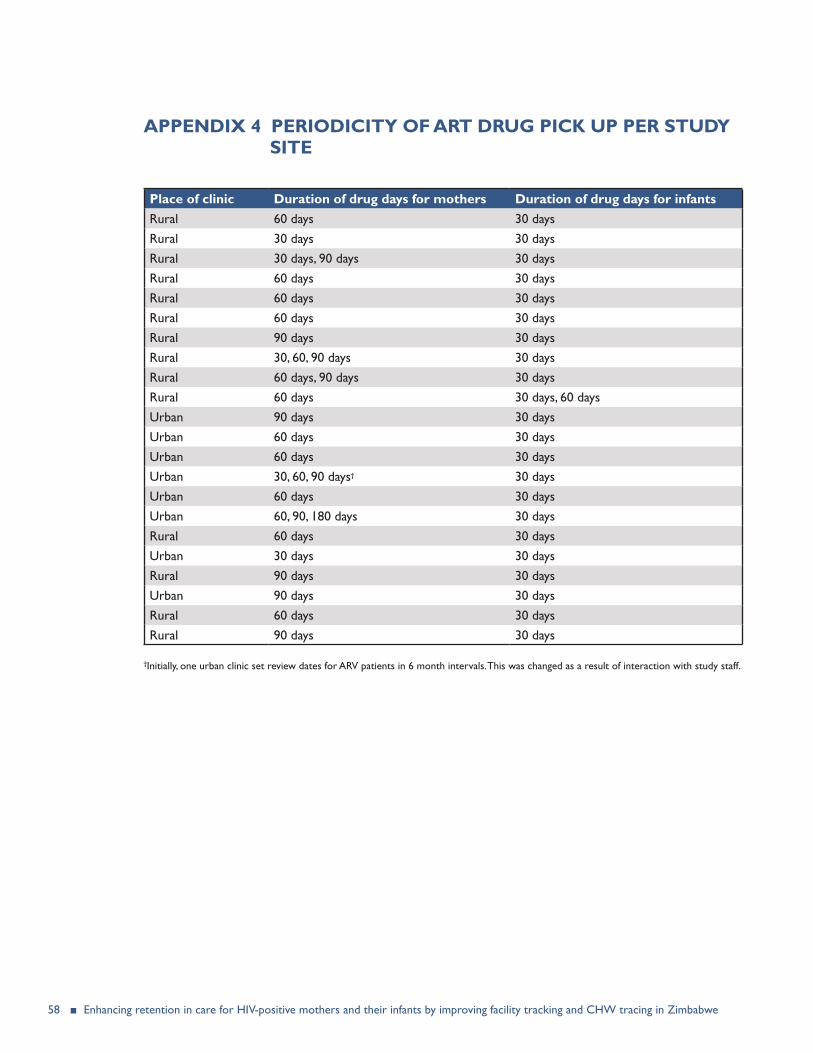
58 ■ Enhancing retention in care for HIV-positive mothers and their infants by improving facility tracking and CHW tracing in Zimbabwe
APPENDIX 4 PERIODICITY OF ART DRUG PICK UP PER STUDY SITE
Place of clinic Duration of drug days for mothers Duration of drug days for infantsRural 60 days 30 daysRural 30 days 30 daysRural 30 days, 90 days 30 daysRural 60 days 30 daysRural 60 days 30 daysRural 60 days 30 daysRural 90 days 30 daysRural 30, 60, 90 days 30 daysRural 60 days, 90 days 30 daysRural 60 days 30 days, 60 daysUrban 90 days 30 daysUrban 60 days 30 daysUrban 60 days 30 daysUrban 30, 60, 90 days† 30 daysUrban 60 days 30 daysUrban 60, 90, 180 days 30 daysRural 60 days 30 daysUrban 30 days 30 daysRural 90 days 30 daysUrban 90 days 30 daysRural 60 days 30 daysRural 90 days 30 days
†Initially, one urban clinic set review dates for ARV patients in 6 month intervals. This was changed as a result of interaction with study staff.


U.S. Agency for International Development1300 Pennsylvania Avenue, NW
Washington, DC 20523Tel: (202) 712-0000Fax: (202) 216-3524
www.usaid.gov