Enhancing Management of Circulatory Instability in ... - SAP · Enhancing Management of Circulatory...
73
Patrick McNamara Associate Professor of Pediatrics Associate Scientist Enhancing Management of Circulatory Instability in Neonates
-
Upload
phungkhuong -
Category
Documents
-
view
213 -
download
0
Transcript of Enhancing Management of Circulatory Instability in ... - SAP · Enhancing Management of Circulatory...

Patrick McNamara
Associate Professor of Pediatrics
Associate Scientist
Enhancing Management of Circulatory Instability in Neonates

The Vulnerable Neonate
How will you ensure cardiovascular stability?

Myths
&
Magical numbers
&
Cook books

Metabolic Homeostasis
Cellular Metabolism
Oxygen Delivery
HemoglobinAnemia
Hemorrhage
Oxygen SaturationLung disease
Shunts
Cardiac OutputHeart Ratearrhythmia
PreloadVolume status
Diastolic functionPericardial effusion
ContractilityCatecholamines, sepsis
Cardiomyopathy, acidosis
AfterloadSVR, pericardial “P”
BP
SVR
Oxygen Consumption
Basal MetabolismPain, sedation, anxiety
thermogenesis
WorkBreathing, growth, trauma
catabolism, fever

Cost-effectiveness
Optimal Outcome
The Changing NICU

What is Targeted Neonatal Echocardiography?
• Extension of the clinical examination - not confined to organs (Assessment phase)– Hemodynamics, Organs, Catheters– Ductal evaluation, Pulmonary hemodynamics, LV performance
• Relate physiologic and hemodynamic data to the clinical problem (Integration phase)
• Focused clinical decision making
• Response to intervention (Response)

Scenario I
• 19 day old male, born at 24 weeks gestation (650 gms), with a large HSDA (3.2 mm) referred for surgical ligation (failed 2 courses of indomethacin)
• E Coli sepsis, bilateral IVH
• Lung disease: HFOV 9 cm H20, FiO2 0.4
• Uneventful procedure (52 mins duration)

Blood Pressure
Time [hrs]
0 5 10 15 20 25 30
BP [m
mHg
]
10
20
30
40
50
60
70
Dobut.
5 mcg/kg/minDobut. 10
Dobut.20
0 1 4 8 10 20 26Heart rate 163 159 150 155 160 159 151
FiO2 0.25 0.3 0.25 0.31 0.3 0.35 0.35
MAP 7.6 8.1 6.7 7 7.6 8 9.8
pH 7.37 7.36 7.26 7.14 7.21
LAC 1.0 1.7 2.6 5.4 3.6

IssuesProblem: Systemic hypotension & low output
state secondary to LV dysfunction and mechanical compression effects of extra-cardiac effusion
Issue: :• Reason for clinical deterioration different
from presumed physiology• Potential for cardiorespiratory arrest high
without timely and appropriate intervention

Scenario II• 40 week male, 3.3 kg with antenatal diagnosis of
CDH & suspected aortic arch hypoplasia
• Severe oxygenation failure from birth
• Prostaglandin infusion (0.05) commenced
• No response to inhaled Nitric Oxide
• Postnatal echo equivocal

PGE1 iNO Dopamine Epinephrine Milrinone, wean PGE1/pressors
0.01 20ppm 15 µg/kg/min 0.03 mg/kg/mi 0.66 mg/kg/min
BP 31/23 (26) 43/30 (35) 39/30 (34) 43/32 (35) 56/32 (46)
HR 182 194 186 193 161
Lactate 2.8 5.5 7.2 7.9 1.3
U.O. (mls/kg/hr) 0.75 4.2
4hrs 12hrs 24 hrs 36hrs

Issues:Problem: Low systemic blood flow 2° to hyperinotropy and
excessive L-R transductal shunting
Danger: Complication of therapy• Cardiotropic agents (e.g. dopamine, epinephrine) which
increase myocardial contractility → impair diastolic performance and low cardiac output state.
• Pressor agents further exacerbate the transductal shunt → low cardiac output state
Impact: Functional USS may help identify to origin of the low output state (e.g. myocardial dysfunction, transductalshunting) facilitating the choice of cardiotropic agent(pressor vs vasodilator)

Merits of TnECHO
• Provides timely hemodynamic information to confirm or question the presumed pathophysiology
• Earlier identification of “neonatal disease” e.g. HSDA, pericardial effusion, CHD
• Delineates “need” for treatment and assists with selection of “desirable therapy” e.g. iNO or cardiotrope, vasodilator or vasopressor
• Facilitates monitoring the response to therapySeghal & McNamara 2008

Emergence of Point of Care USS
•1950-60s: 1st ultrasound equipment, restricted use: not portable
• 1970s: Cranial USS performed by neonatologists in Europe, Australasia
Levene 1982 Arch Dis Child
• Echo performed by radiology until late 1970s (TURF War I)
•Point of Care ultrasound used by adult intensivists, OBG nurses (hemorrhage, fetal well-being), ER physician (abominal aneurysm) & surgeons (acute abdomen, scrotum)
Australasian Society for Ultrasound Certificate in Clinician performed USS

Evans 2000 – Survey of neonatal fECHO practice in ANZAC
Ward 2001 – Errors in neonatal echo in ANZAC
2009 PAS, AAP workshops in fECHO
2010 Canadian fECHO Network40% centers with trained neonatologist
2007 CCPU, Australasia
2003 Toronto – fECHO in clinical care
Pre-2000 – Ad-hoc fECHO practice in ANZAC, UK & Europe
2005 Toronto – fECHO training program
2005 RCPCH, UK fECHO manadatedfor tertiary level neonatologists
ECHO in the NICU, ASE writing group
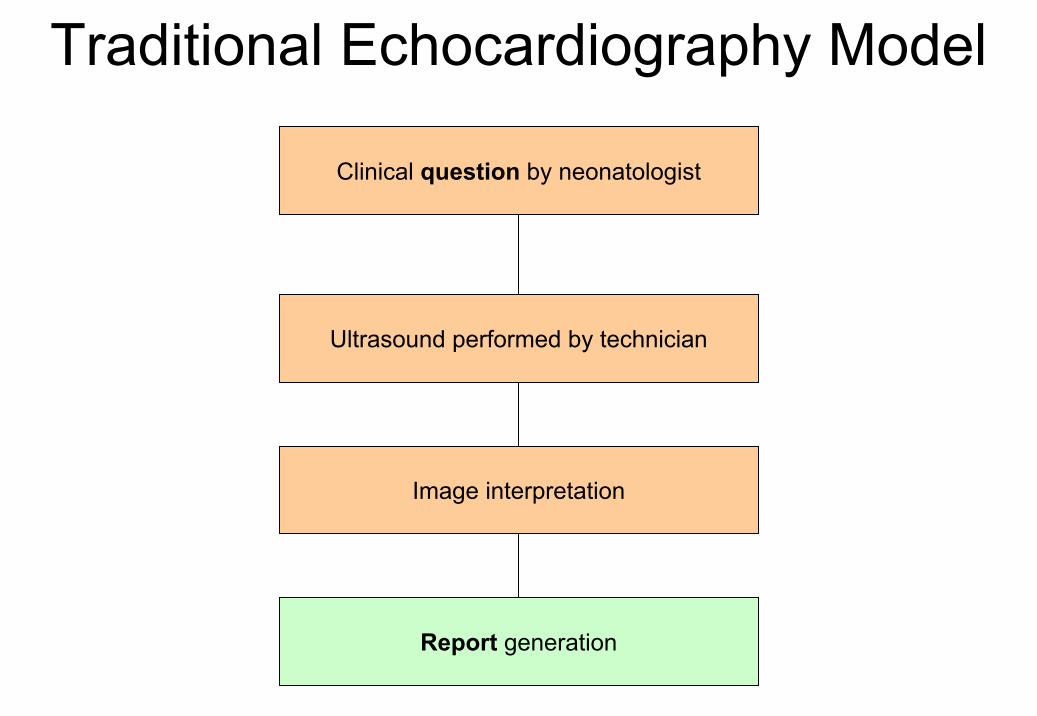
Clinical question by neonatologist
Ultrasound performed by technician
Image interpretation
Report generation
Traditional Echocardiography Model

Issues• Disconnect between clinical question and study
interpretation
• Information missing with need for repeat of study
• Temporal delay in acquisition of information
• Limited ability to perform sequential studies
• Out-of-hours studies limited to cases where likelihood of CHD high

Refining Therapeutic Decision-Making

Clinical Problem
Functional Evaluation
Hemodynamic Problem Anatomic Problem
Medical decision Cardiology
Consultation

TnECHO - Indications• Is their a hemodynamically significant ductus
arteriosus?– Size of the shunt, effect on myocardial performance and end-organ
perfusion
• Evaluation of pulmonary hemodynamics– Degree of pulmonary hypertension vs. impact on myocardial
performance– Presence or absence of shunt
• Troubleshooting systemic hypoperfusion or hypotension– Systolic vs. diastolic performance (afterload effect?)– Low SVC flow, low cardiac output
• Miscellaneous– Confirmation of line placement (assist insertion)– Presence or effusions or thrombi

Defining the Nature of the Problem
Preload MyocardialFunction
Afterload Heart Problem
Rhythm problem
Hypovolaemia Prematurity < 48 hours of life HSDA SVT
Overinflation Sepsis / NEC PDA Ligation Coarctation Complete heart block
Adrenal suppression
Adrenal suppression
Pulmonary hypertension
HLHS
IDM Aortic stenosis

Is the neonatologist reliable?
Does TnECHO improve outcomes?

Challenges• Validity of some measurements• Collaboration with Pediatric Cardiologists
– Income streams– Misdiagnosis & Maltreatment– Terms/Level of Engagement
• Standards for training• Access to equipment (Ownership)• Data storage


Ward 2001 J Pediatr Child HealthDiagnostic Errors 47/110 (44%)

Samson 2004 Card Young
Neonatologist & CHD

626, 781 live births
4295 cases of CHD
451 major cardiac defects
238 (52.8%) cases detected antenatally
Drawing Parallels: Antenatal Diagnosis of CHD
Chew 2007 Ultrasound Obs Gyn

Target group Duration Assessment AccuracyFocused Assessment with Sonography for Trauma
15 scans:
50 scans:
Trauma assessment
sensitivity 90%, accuracy 99% sensitivity 96%, accuracy 100%
McCarter 2000Ann Surg
Limited Echo Assessment Project (LEAP): Residents
20 hours LV function & pericardial effusion
High Alexander 2001 Circulation
Medical students
20 hours LV function & pericardial effusion
Complete echo: 97%Accuracy: 80%
Alexander 2001 Circulation
Non-cardiologist 10 hours LV assessment
Accuracy 87% Manasia 2004 J CardiovascAnesth
Non-cardiologist 4 hours LV function Sensitivity 77%Specificity 94%
Melamed 2004 Chest
Residents 20 hours Complete assessment
Accuracy 93% Croft 2006 Echo
EVIDENCE FROM ADULT TRAINING
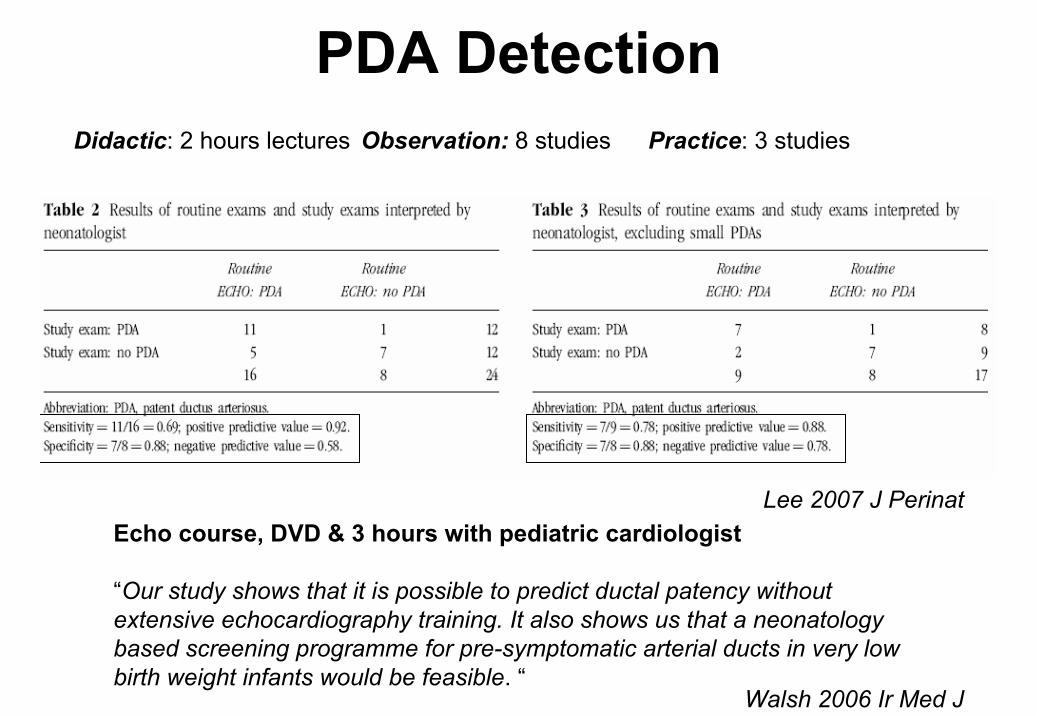
PDA Detection
Lee 2007 J PerinatEcho course, DVD & 3 hours with pediatric cardiologist
“Our study shows that it is possible to predict ductal patency without extensive echocardiography training. It also shows us that a neonatology based screening programme for pre-symptomatic arterial ducts in very low birth weight infants would be feasible. “
Walsh 2006 Ir Med J
Didactic: 2 hours lectures Observation: 8 studies Practice: 3 studies

Is the neonatologist reliable?
Does TnECHO improve outcomes?

Efficacy of GDFI in adult care
• Changes in clinical care in 53% of patient Gorcsan 2001 JAMSE
• ↑ diagnostic accuracy (50%) in RCT of goal directed echo for hypotensive patients in ER
Jones 2005 Crit Care Med
Manasia 2004 J Cardiovasc Anesth
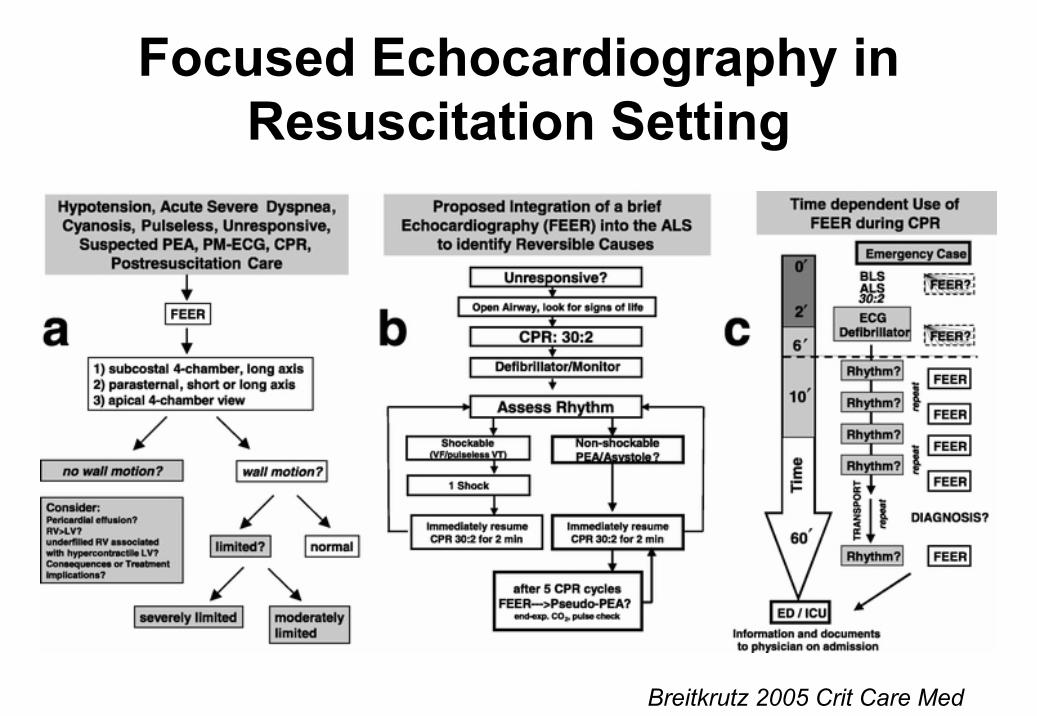
Focused Echocardiography in Resuscitation Setting
Breitkrutz 2005 Crit Care Med

PDA Echocardiography research
Time period
1970-79 1980-89 1990-99 2000-present
Num
ber o
f pub
licat
ions
0
5
10
15
20
25
30
Neonatology Cardiology

Intraventricular Hemorrhage
Era
Before After%
0
10
20
30
40
50
60
IVH Gd III/IV
Era I Era II
Gestation [weeks]
26.1[24.5-29.5] 26.6 [23.8-28.1]
PDA diagnosis [days]
4 [2-13] 3 [3-4] *
PDA treatment I [days]
5 [3-25] 3 [3-7] *
PDA treatment II [days]
12 [9-14] 8 [7-9] *
Ventilation [days]
13 [0-66] 9 [1-66] *
Early Detection & Outcome
O’Rouke 2008 Acta Paed

Duration of Indomethacin Treatment of the Preterm PDA as Directed by Echocardiography
Carmo J Pediatr 2009
Premature infants with HSDA
fECHO guided intervention Conventional group

Duration of Indomethacin Treatment of the Preterm PDA as Directed by Echocardiography
• Reduction in indomethacin administration from a median of 3 doses (1-12) to 1 dose (1-15) using fECHO directed therapy
• No increased in need for subsequent indomethacin or PDA ligation
Carmo J Pediatr 2009

Toronto Crisis
• Waiting time for PDA ligation 2-3 weeks
• Delayed time of intervention
• Inconsistent referral pattern
• Post-ligation Cardiac Syndrome (PLCS) common
Enhancing PDA Care• Creation of PDA ligation team
• Comprehensive TnECHO before intervention
• Categorisation system for PDA
• Early postoperative TnECHO to guide neonatal care

PDA Ligation [Toronto]
Year
2004 2005 2006 2007 2008 2009
Rat
e
0
20
40
60
80
100 Triaging system
TnECHO
TnECHO - postop

Dealing with Education and Accreditation


First symposium on First symposium on fECHOfECHO Oct 08 M. Oct 08 M. KluckowKluckow

Recent Initiatives
• Establishment of np-fECHO working group for Canadian Neonatologists (Calgary 2010)
• American Society of Echocardiography Writing group 2010– Guidelines for ECHO in the NICU– Cardiologists, Neonatologists

Use of npFE - Guiding Principles
• Echocardiography information dependant on quality of images and reliability of interpretation (Competence)
• Hemodynamic information should only be used in the context of the clinical scenario (Logic and Reason)

np-fECHO evaluations must be performed by personnel who have completed a
recognised training program, met basic criteria for image acquisition and
interpretation.

Established Standby Interest
Calgary Winnipeg Montreal
Toronto (n=3) Hamilton London
Vancouver Halifax Edmonton
Quebec city

Neonatal Cardiology Specialist
Imaging Equipment
Training Program
Archiving & Reporting
Neonatal Cardiology Consult Model
Clinical Practice Guidelines
Toronto TnECHO Model of Care

CLINICAL RESEARCH EDUCATIONNeonatal cardiovascular consult model of care- Guidelines &Referral process- 3 trained fellows
Prospective observational human studies• PDA Ligation physiology experiments• Milrinone pharmacokinetics• Surfactant hemodynamics• Furosemide and blood transfusion
Translational Sciences• Asphyxial cardiac arrest and vasopressin - piglet• Pulmonary Hypertension collaborations – neonatal rodents
Echocardiography training- Phase I (3 months)- Phase II (3-6 months)Completed by 16 fellowsIn progress – 4 fellows
Neonatal Cardiology Fellowship (TBA) – 1 year
Resources: Publications, WINFOCUS, Evans DVDs
Elective opportunities Elective opportunities- 4 neonatologists (2 4/52)- 1 sabbatical- 6 fellows, next 12 months
Portable laptop systems– HSC / SunybrookRoving machine – 1 siteStandardized image acquisition and protocols
Electronic reporting
Ancillary Resources- Online npfECHO teaching module- Competency evaluation & OSCE development (Finan)
Archiving - ECHOPAC Archiving - ECHOPAC Archiving - ECHOPAC
↓ Ligation rates & PLCSECMO-medical rare
Developmental Hemodynamics group
Global Workshops – PAS, India, Saudi Arabia, AAP

Year
2006 2007 2008 2009 2010
TnEC
HO
0
100
200
300
400
500
Year
2005 2006 2007 2008 2009 2010 2011
Sono
grap
hers
0
1
2
3
4
5
6
7
TnECHO Sonographers

TnECHO training modulePhase I:• Didactic sessions
• Hands-on supervised sessions (12 weeks)– Equipment– Landmarks & standard views– Goal directed assessments
• Ongoing scanning (12 weeks ) : LogbookPhase II:• Independent scanning: Neocardiac rotations /formal
review
• Formal evaluation

Training Modules
1. Physics of Ultrasound 2. 2D, M-mode and Doppler imaging3. Orientation and image acquisition for basic
transthoracic cardiac views 4. Evaluation of left ventricular systolic and
diastolic performance 5. Evaluation of pulmonary hemodynamics6. Evaluation of the ductus arteriosus7. Evaluation of systemic hemodynamics8. Evaluation of indwelling catheters, brain
parenchyma, effusions and bladder.
Maintain logbook - completed a minimum of 50 complete echocardiograms of which 25 are ductusarteriosus evaluations.

Challenges• Learning curve for functional
echocardiography
• Standardized echocardiography approach
• Quality assurance for imaging
• Therapeutic protocol – consistent approach

Scenario III• Term 40 wks gestation; Bwt 5.060 Kg • Severe uncontrolled maternal IDDM• SVD Resp distress intubated & surfactant good
response ventilated on AC on 22/6 in 25% oxygen
• Severe hypoglycemia D20W @ 120ml/kg/day• Insulin level 571• UVC high slightly high on Xray adjusted
• Murmur ECHO; severe septal hypertrophy with mid cavity gradient
• To treat as HOCM if symptomatic

Case Progression• Day 3 extubated in LF• Sugars stable D20W at 120 + glucagon
Day 5 • Glucose 6 at 0600 hrs• Inc to 10 (0900), 14 (1200) 18 (1400)• Lactate 6 8• Poor perfusion, reduced urine output• Increasing resp distress CXR rpt • Inc cardiomegaly + UVC migrated deep in RA• TnECHO performed
Echo clip #1Echo clip #2

• Effusion (TPN) drained under Echo guidance
• Echo next day showed thin rim of effusion and well filled heart
• Extubated to low flow oxygen• Off glucagon over the next 3 days• Transferred to L2 for establishing feeds

Take Home Messages • Targeted Neonatal Echo should be used in combination
with clinical acumen and not as replacement
• The focus is to provide longitudinal hemodynamicinformation in critically ill neonates
• This information either compliments what is clinically suspected or provides novel physiologic insights
• Catalyst for prospective physiology based research
• Issues related to training, accreditation and standards need to be addressed locally and in collaboration with our cardiology colleagues

“Information Age ”Reinvigoration of the physical assessment
“The role of goal directed ultrasound is not to replace or detract from a complete echocardiogramperformed by the pediatric cardiologist but to enhance the physical examination by providing additional real-time physiologic information”

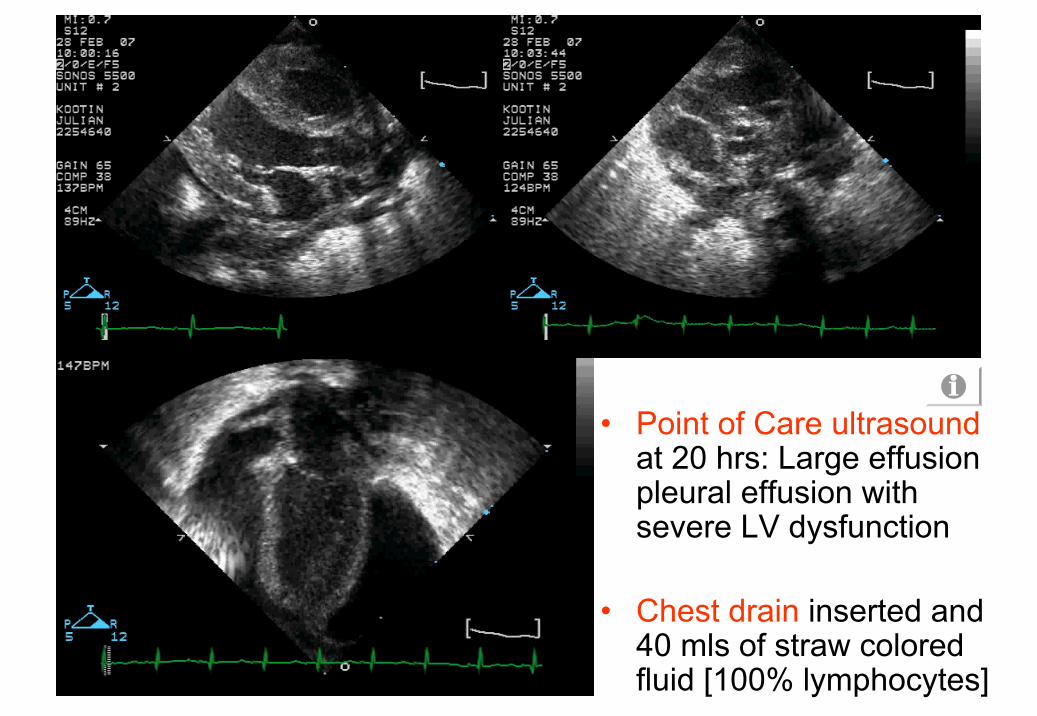
• Point of Care ultrasoundat 20 hrs: Large effusion pleural effusion with severe LV dysfunction
• Chest drain inserted and 40 mls of straw colored fluid [100% lymphocytes]

• Point of Care ultrasoundHypercontractilemyocardium with unrestrictive L-R transductal flow
• PGE1 & pressorsweaned
LV
RV
AO
LA
PDA
PA

Zhang 1999 Arch Dis Child
Dopamine and Afterload
Group 1 Dopamine 8 µg/kg/min
Group 2 Dopamine 6 µg/kg/min

Ultrasound as a research tool Ultrasound as a clinical tool
Clinical Dilemmae.g. hypotension, ductus arteriosus
? Improved Clinical Care

Pillars of Training• Credentialing committees for each country.
• Development and maintenance of standards for both trainees and trainers.
• Ongoing support for trainees (experienced mentor).
• OSCE a useful method for assessment of skills
• Regular re-accreditation of trainees.
• Quality control including a requirement for log books supported by comparison with gold standards.

Sick Neonate
Brain assessment? Hemorrhage MCA Doppler
Abdominal assessment? Ascites Bladder
Renal, mesenteric, celiac Doppler
? Organs present
Heart & lung assessmentPreload Contractility
HSDA CHD
Effusion
Cyanosis (SpO2 65%)? Ebsteins
Brain assessmentVein of Galen malformation
Abdominal assessment
Normal
Heart & lung assessment
PPHN
Dilated SVC with turbulent flow

TnECHO in Canada 2008• fECHO is used less often in
Canada. (79% vs. 91%, p=0.01)
• 86% of respondents reported
that average time to obtain echo
was close to 6hrs
• Most common indications were– Exclude PPHN
– Confirm PPHN
– Assess response to treatment
– Others (serial functional assessment, target therapy, aid weaning)
Comparison of professionals performing FECHO
0
10
20
30
40
50
60
70
80
90
Neonatologist Cardiologist Others
Professional
Prop
ortio
n of
resp
onde
nts
(%)
Canada(n=89)Aus-NZ(n=98)
#
# p<0.05 significant
#
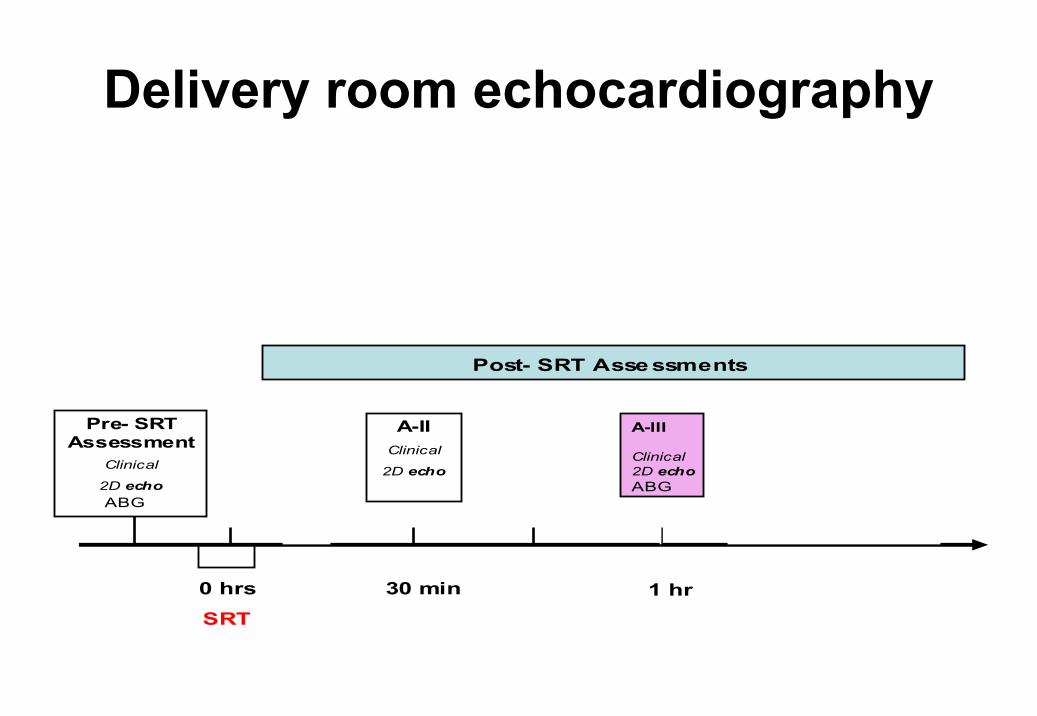
Pre- SRT Assessment
Clinical
2D echo
0 hrs
SRT
30 min 1 hr
A-IIIClinical
2D echo
Post- SRT Assessments
A-IIClinical
2D echo
ABGABG
1 hr
A-III
Clinical2D echoABG
Delivery room echocardiography

Left Ventricle
Ao
PDA Ao SVR+++++
PVR+++
+++
Surfactant
Hyperoxia
Hypocapnia / Alkalosis
Placenta elimination
Hyperoxia
Hypothermia
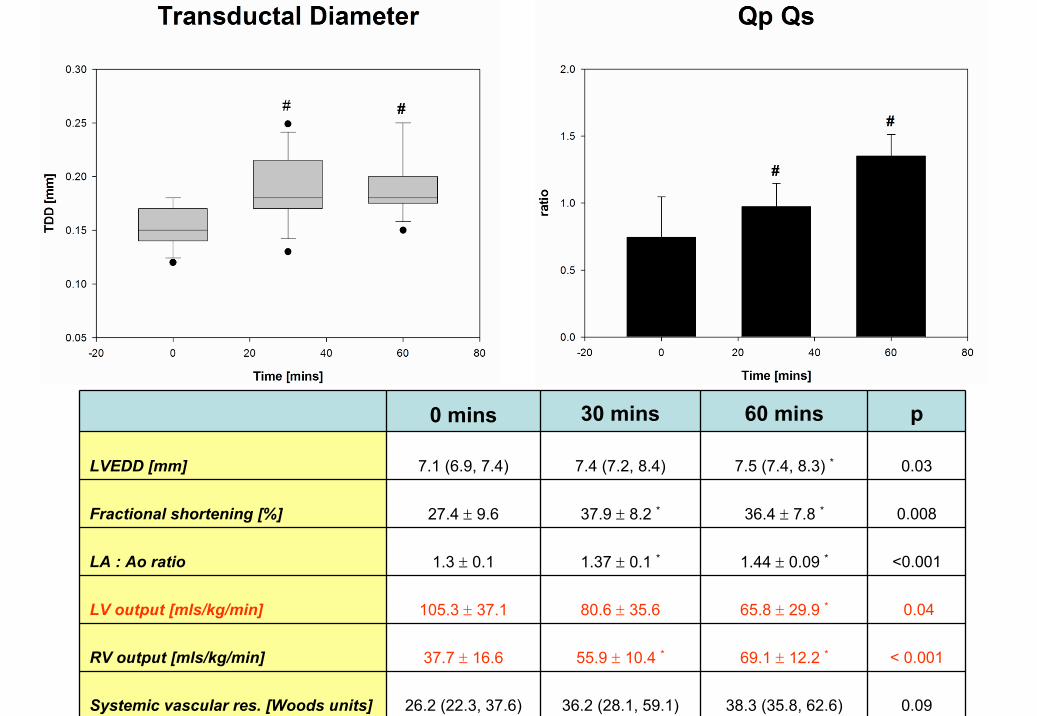
0 mins 30 mins 60 mins p
LVEDD [mm] 7.1 (6.9, 7.4) 7.4 (7.2, 8.4) 7.5 (7.4, 8.3) * 0.03
Fractional shortening [%] 27.4 ± 9.6 37.9 ± 8.2 * 36.4 ± 7.8 * 0.008
LA : Ao ratio 1.3 ± 0.1 1.37 ± 0.1 * 1.44 ± 0.09 * <0.001
LV output [mls/kg/min] 105.3 ± 37.1 80.6 ± 35.6 65.8 ± 29.9 * 0.04
RV output [mls/kg/min] 37.7 ± 16.6 55.9 ± 10.4 * 69.1 ± 12.2 * < 0.001
Systemic vascular res. [Woods units] 26.2 (22.3, 37.6) 36.2 (28.1, 59.1) 38.3 (35.8, 62.6) 0.09
Surfactant administration is followed by………
• Increased systolic but decreased diastolic BP.
• Increased ductal size and exclusive left-to-right transductal flow within the first hour of life.
• Extremely low pulmonary and systemic blood flow in first hour of life
• Redistribution of the amount of pulmonary and systemic blood flow resulting in increased Qp:Qs
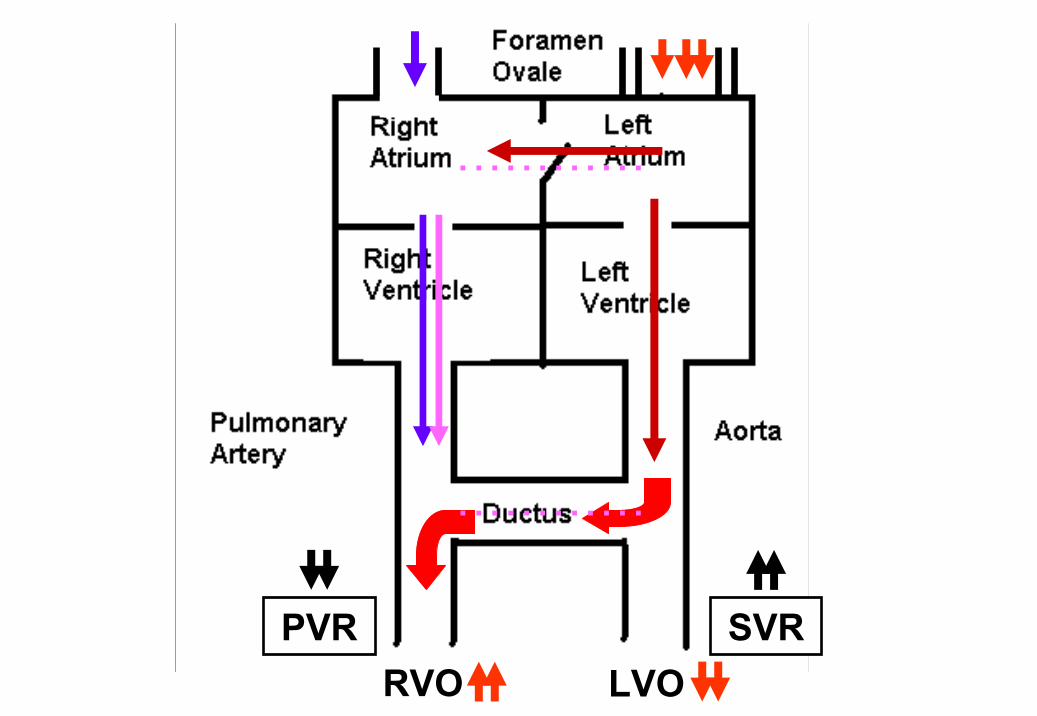
RVO LVOSVRPVR
…………
…………

Japanese Experience• TnECHO
– Delivery room and 8 hourly until 96 hours
– Day 7 & 10– Weekly evaluation x 6
weeks, & discharge– Strict Protocols with
management approach

Merits Challenges
All doctors trained
24/7 coverage
Dedicated up-to-date equipment
Standardized image acquisition and protocols
Brief study (10-15 mins)
Electronic reporting and archiving system
Lack of scientific validation for many hemodynamicmarkers (e.g. IVC diameter, ESWS)
Ad-hoc Echocardiography training