
England 1^' Crg/ MORBIDITYANDMORTALITYWEEKLYREPORT …
12
Transcript of England 1^' Crg/ MORBIDITYANDMORTALITYWEEKLYREPORT …

CENTER FOR DISEASE CONTROL September 1, 1978 / VWll / Nch$5 <*
MORBIDITY AND MORTALITY WEEKLY REPORT
International Notes
England 1^' Crg/Current Trends'f" /,Measles — Unit '
321 Q Fever - New Y
ACIP Recommenda
327 Meningococcal Polysaci
Vaccines
International Notes
Laboratory-Associated Smallpox — England
England has reported a case of laboratory-associated smallpox. This is the first small
pox case reported in the world since October 26, 1977, when a case occurred in Somalia.
The patient is a 40-year-old female medical photographer employed at Birmingham
Medical School; her office is located on the floor above the Department of Virology,
where work on variola viruses is done. She developed fever on August 11 and rash 2 days
later. She was hospitalized on August 24; the same day she was transferred to a small
pox infectious disease hospital.
Electron microscopy (EM) was positive for pox virus on August 25; on August 27,
variola major virus was isolated.
Thirty-nine close and 196 casual contacts of the patient have been identified. Three
f contacts who have become ill have been admitted to isolation as a precautionary measure.
EM results on one such contact, who had rash and fever, showed Herpes virus. As of
August 30, all other contacts are well.
One contact, a 20-year-old British woman, traveled to North Dakota on August 18.
When it was learned that her co-worker had smallpox, state and local health officials
were notified, and CDC dispatched a medical epidemiologist to the farm where she is
staying. She is afebrile and has no symptoms. She had been vaccinated 5 years ago.
Daily surveillance is being maintained by local health authorities.
As of August 30, the patient is still hospitalized but improving. She has a confluent
rash on her face and discrete lesions on her extremeties. The medical school labora
tory has been closed.
Reported by PA Hyzler, MD, National Health Div, Dept of Health and Social Security, London;
K Mosser, State Epidemiologist, North Dakota State Dept of Health; Bur of Smallpox Eradication,
CDC.
Editorial Note: This patient was presumably infected by airborne transmission of vari
ola virus from the smallpox laboratory on the ground floor to the patient's normal
work area on the first floor. The ability of variola virus to transmit from 1 floor to
another via external air currents has been previously documented in a hospital out
break of smallpox in Meschede, Germany (/). Investigation will be required to iden
tify the specific safety breakdown in the Birmingham laboratory.
As smallpox laboratories hold the only known reservoir of smallpox virus, the World
Health Organization (WHO) has urged that storage of the reference virus strains be
restricted to the 5 WHO Pox Virus Reference Centers (2). Since 1975, 62 of 76 labora
tories with known variola virus have destroyed or transferred their virus stocks. The
Birmingham incident emphasizes the continuing risk of laboratory-acquired infection
and the need to ensure maximum security at every facility holding the virus.
U.S. DEPARTMENT OF HEALTH, EDUCATION, AND WELFARE / PUBLIC HEALTH SERVICE

September 1, 1978
Smallpox — Continued
The British contact now in the United States is not believed to be at risk of devel
oping smallpox because her exposure to the case occurred 2-3 days before the patient
had become infectious and 21 days have elapsed since exposure—more than the maxi
mum expected incubation period. U.S. and British vaccination requirements for inter
national travelers remain unchanged {3). However, Malta and Jamaica are now requiring
valid vaccination certificates for anyone who has been in Birmingham in the previous
14 days.
References
1. Wehrle PF, Posch J, Richter KH, Henderson DA: An airborne outbreak of smallpox in a German
hospital and its significance with respect to other recent outbreaks in Europe. Bull WHO 43:669-
679,1970
2. WHO: Laboratories retaining variola virus. Weekly Epidemiological Record 53:221-222, 1978
3. MMWR 27:295, 1978
Current Trends
Measles - United States, 1978
During the first 33 weeks of 1978, 22,546 cases of measles were reported to CDC-
a 57.1% decrease from the same period in 1977 (/). Twenty-six states have reported no
measles for at least a 1-month period. The incidence of measles this year is 15.8% greater
than the equivalent period in 1974, when the fewest number of cases was reported
(Figure 1).
Five states—Maine, Michigan, Virginia, West Virginia, and Wisconsin—have each re
ported a measles incidence rate greater than 100 cases per 100,000 population less than
FIGU14,000-I
3.500-
3000-
2,500-
« 2,000-<
1.500-
1,000-
500-
0
RE1. Reported measles cases, by week.
A
A f \/ V \
United States,
\
1974,1977, 1978
-- I974
- 1977
— I978
345 6 7 8 9 10 II 12 13 14 15 16 17 18 19 2021 22 23 24 25 36 27 28 29 30 31 32 33 34 35 36 37 38 J9 40 41 42 43 44 4546 47 48495051 52

September 1,1978 MMWR 321
Measles — Continued
18 years of age.* These stdtes, which together account for 10.3% of the U.S. population
of this age, have reported 60.9% of the nation's measles cases this year.
Reported by Immunization Div, Bur of State Services, CDC.
Editorial Note: Data collected prior to the introduction of measles vaccine suggest
that only about 10% of measles cases occurring in the United States at that time were
reported to local health officials. Although it is generally felt that reporting efficiency
has improved somewhat since then, it is clear that a significant amount of underreporting
still exists. Since there is variation from area to area in the methodology (and probably
the sensitivity) of the current measles surveillance system, incidence rate data must be
interpreted with some caution. Nonetheless, it is reasonable to assume that prolonged
absence of reported cases in a particular state probably indicates little or no measles
transmission. Preliminary indications from the 5 high-incidence states that a large number
of cases are occurring in junior and senior high school students highlight the need to
assess immunization status of children of all ages and to provide immunization to those
not known to be protected.
Reference
1.MMWR 27:252, 1978
1976 population data
Epidemiologic Notes and Reports
Q Fever — New York
On May 25, 1978, the Suffolk County Department of Health Services was informed
by an infection control nurse at the Brookhaven Memorial Hospital that 2 days earlier
a 27-year-old man had been admitted with a 4-day history of fever to 104 F (40 C),
severe headache, chills, malaise, and vomiting. This patient had visited West Africa in
April and was an employee of an exotic bird and reptile importing company in Deer
Park, New York. Within 1 week, 3 other employees of that company were admitted to
the same hospital with similar symptoms. One had a non-productive cough. All were
treated with oral tetracycline with rapid resolution of their symptoms and complete
recovery.
These 4 persons had all been involved in unpacking and deticking a shipment of
approximately 500 ball pythons (Python regius), which were imported on May 3 from
Accra, Ghana. Examination of the hemolymph of 5 ticks removed from these snakes
indicated that all contained numerous bacteria, both bacillary and coccoid forms, and
that 2 contained rickettsiae which were not further characterized. Three types of ticks
were identified, namely, Amblyomma nuttalli, Aponomma latum, and Aponomma
flavomaculaturn.
Paired serum samples examined by the New York State Department of Health Labora
tory revealed rising titers against the Q fever antigen by complement fixation. Serum
specimens from the 4 hospitalized patients, tested at Rocky Mountain Laboratory,
National Institutes of Health (NIH), by microimmunofluorescence, showed confirma
tory rises in titers to Q fever.
Seven other persons were identified who had been in contact with the pythons, ticks
from the pythons, or excreta of ticks or pythons. Of thpse, 5 had had febrile illnesses
3 0001 00128 1270

322 MMWR September 1, 1978
Q Fever — Continued
with similar, but somewhat milder, symptoms than the hospitalized group. Four of the
5 had been seen by their family physicians and had received oral tetracycline. The fifth
did not see a physician. Serologic tests in 4 of these individuals confirmed a recent Q
fever infection in one and probable Q fever infections in 2 others.
Samples of python blood, spleen and liver, as well as 15 live ticks and 5 frozen ticks
removed from the pythons, were processed for attempted isolation of organisms; all
were negative.
The county health department has been informed that 420 of the pythons have been
sold to retailers all over the United States. The distribution list is unavailable at this time.
Reported by S Kim, MD, Patchogue, New York; S Guirgis, PhD, D Harris, MD, MPH, T Keelan, RN,
MPH, M Mayer, MD, MPH, M Zaki, MD, DrPH, Suffolk County Dept of Health Services; L Steinert,
RN, BS, Brookhaven Memorial Hospital; J Benach, PhD, D White, MS, DO Lyman, MD, State Epi
demiologist, New York State Dept of Health; R Ormsbee, PhD, Rocky Mountain Laboratory, Nation
al Institute of Allergy and Infectious Diseases, NIH; Viral Diseases Div, Bur of Epidemiology, CDC.
Editorial Note: Q fever is an acute, systemic disease caused by Coxiella burneti. Charac
terized by the abrupt onset of headache, myalgia, chills and fever, it is usually a self-
limited illness of 1-3 weeks duration. Pneumonia and hepatitis are frequent manifesta
tions (7), and endocarditis has been reported (2). Patients with Q fever, as opposed to
those with other rickettsial diseases, do not develop Weil-Felix agglutinins and virtually
never have an accompanying rash. The treatment of choice is tetracycline or chloram-
phenicol.
(Continued on page 327)
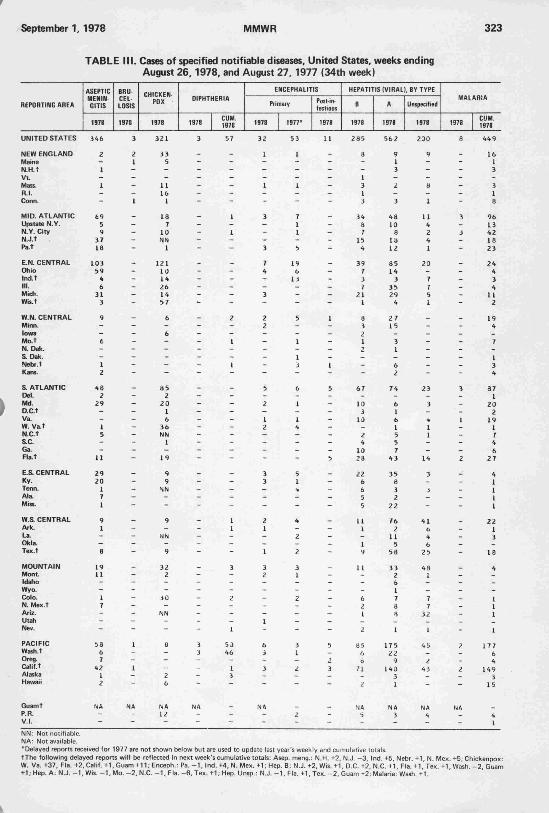
TABLE 1. Summary -- cases of specified notifiable diseases. United States
[Cumulative totals include revised and delayed reports through previous weeks.]
DISEASE
Aseptic meningitis
Brucellosis
Chickenpox
Diphtheria
Encephalitis: Primary (arthropod-borne & unspec.)
Post-infectious
Hepatitis, Viral: Type B
Type A
Type unspecified
Malaria
Measles (rubeola)
Meningococcal infections: Total
Civilian
Military
Mumps
Pertussis
Rubella (German measles)
Tetanus
Tuberculosis
Tularemia
Typhoid fever
Typhus fever, tick borne (Rky. Mt. spotted)
Venereal diseases:
Gonorrhea: Civilian
Military
Syphilis, primary & secondary: Civilian
Military
Rabies in animals
34th WEEK ENDING
August 26, | August 27,1978
346
3
321
3
32
11
285
562
200
8
91
32
32—
106
54
65
3
568
1
10
44
21,662
428
477
5
31
1977*
2 06
14
217
1
53
3
304
612
169
15
103
16
15
1
106
97
49
3
644
4
a
53
2 0,445
602
444
2
54
J tar ni A IUMtUIAN
1973-1977**
131
6
263
1
53
6
273
I 673f
14
103
16
15
-
269
49
3
644
3
6
32
20,750
604
463
2
59
iCUMULATIVE, FIRST 34 WEEKS
August 26,
1978
2,706
100
121,877
57
490
137
9,561
18,535
5,832
449
22,637
1.702
1,682
20
13,015
1,235
14,908
53
19,677
69
284
743
640,068
16,321
13,687
187
2,001
August 27,
1977*
2,491
150
159,902
60
5 54
148
10,765
20,196
5,763
354
52,6 00
1,226
1,217
9
15,730
865
18,428
45
19,779
102
231
884
635,797
17,679
13,455
192
1,992
TABLE II. Notifiable diseases of low frequency. United States
Anthrax (N.Dak. 1)
Botulism
Congenital rubella syndrome (Mich. 1)
Leprosy (Tex. I.Calif. 5)
Leptospirosis
Plague
re used to
CUM. 1978
5 Polion
55
22 Psittac
104 Rabies
39 Trichi
6 Typht
uDdate last vear's w
yelitis: Total
Paraly
osis (La. 1)
in man
losis (NYC 2)
s fever, flea bor
'eklv and cumu
tic
ne (endemic, muri
lative totals.
le)
MEDIAN
1973-1977**
1,835
150
144,519
126
592
196
7,511
1 22,856j
268
23,999
1,022
999
23
43,881
14,654
57
20,574
92
245
612
633,797
19,504
15,873
229
1,931
CUM. 1978
1
1
74
—
40
26

September 1, 1978
TABLE III (Cont.'d). Cases of specified notifiable diseases. United States, weeks ending
August 26,1978, and August 27, 1977 (34th week)
REPORTING AREA
UNITED STATES
NEW ENGLAND
Maine
N.H.t
Vt
Mass.
R.I.
Conn.
MID. ATLANTIC
Upstate N.Y.
N.Y. City
N.J.
Pa.
E.N. CENTRAL
Ohio
lnd.t
III.
Mich.
Wis.
W.N. CENTRAL
Minn.
Iowa
Mo.
N. Dak.
S.Dak.
Nebr.
Kara.
S. ATLANTIC
Del.
Md.
D.C
Va.
W. Va.
NX.
S.C.
Ga.
Fla.t
E.S. CENTRAL
Ky.
Tenn.
Ala.
Miss.
W.a CENTRAL
Ark.
La.
Okla.
Tex.
MOUNTAIN
Mont
MEASLES (RUBEOLA)
1971
91
2
—
—
_
2—
-
7
3
3
1
-
38-
5
T
24
2
_
—
—
-
—
—
—
-
19
1
4
-
2
2
—
_
—
10
2
_
—
2
_
_
_
-
-
_
_
CUM.
1978
22,637
1,968
1,314
46
25
253
8
322
2,147
1,363
335
74
355
9,867
475
187
628
7,124
1,453
378
34
52
11
191
—
i
95
4,827
7
50
—
2,80!i
1.032
116
1S6
17
604
1,379
118
956
89
216
1,009
u
341
13
639
247
105
CUM.
1977*
52,600
2,482
170
510
292
623
64
823
8, 305
3,787
710
195
3,613
11,128
1,842
4,302
1,66 0
525
2,399
9,437
2,620
4,267
1,038
23
67
214
1.208
4,517
22
371
14
2,701
222
62
14 7
764
214
1,969
1, 182
672
77
38
2.062
29
74
55
1,904
2,506
1,160
MENINGOCOCCAL INFECTIONS
1971
32
1
-
—
_
_
-
1
4
-
2
1
1
2
2
-
-
—
-
_
-
-
-
-
-
-
-
6
-
2
-
-
-
-
_
1
3
2
1
1
-
8
-
6
-
2
I
1
CUM.
1978
1,702
86
6
8
2
27
17
26
301
103
69
52
77
153
57
29
7
49
11
56
14
5
2 3
3
2
-
9
424
15
27
1
52
0
82
24
47
16 7
136
2d
iZ
42
34
269
li.
114
16
117
3b
2
CUM.
1977*
1.22o
52
3
3
5
17
1
23
162
36
44
37
45
134
44
9
34
35
12
54
19
8
16
1
4
1
5
2 68
19
18
—
23
9
62
28
44
85
132
26
33
49
24
215
11
83
10
114
30
2
1978
106
2
1
-
-
-
1
7
1
3
1
2
43
22
1
5
3
12
3
1
-
1
1
-
-
-
14
4
-
-
1
1
1
1
1
5
6
_
1
1
4
14
1
-
-
li
1 I
-
MUMPS
CUM.
1978
13.015
718
485
13
5
85
32
98
593
198
137
131
127
5,211
693
302
1,651
1,344
1,021
1,893
1%
120
1,154
li
6
21
560
741
53
65
1
133
165
66
16
65
177
1,108
iai
445
407
75
1,645
562
61
4
*93
394
141
PERTUSSIS
1978
54
3
-
-
_
3
-
-
a
4
2
—
2
10
1
4
-
-
5
2
-
-
-
-
1
1
-
4
-
-
-
-
-
—
1
2
1
3
1
2
-
-
4
1
-
I
2
13
-
RUBELLA
1971
65
5
—
1_
4
—
-
9
I
4
2
2
19
1
4
-
6
8
_
-
-
-
-
—
-
-
13
I
-
-
4
5
—
-
-
3
2
—
2
—
-
2
-
—
-
2
4
-
CUM.
1978
14.908
729
148
101
27
215
42
196
2,971
515
122
1,598
736
6,839
1,257
566
422
3,072
1,522
655
128
52
97
81
111
34
152
1,002
35
7
1
238
333
178
28
5
177
494
128
198
21
147
905
5b
483
11
353
199
17
TETANUS
CUM.
1978
53
1
-
-
1
-
-
3
1
-
—
2
2
1
1
-
-
-
6
1
-
-
-
1
-
4
11
-
2
1
-
2
1
-
6
3
2
-
—
1
14
1
1
3
9
1
-
tussis: N.H. +2; Rubella: Gu
Guam +2; Men. inf.: Fla. -1. Mumps: Ind. —1, Guam +4; Pe
September 1,1978
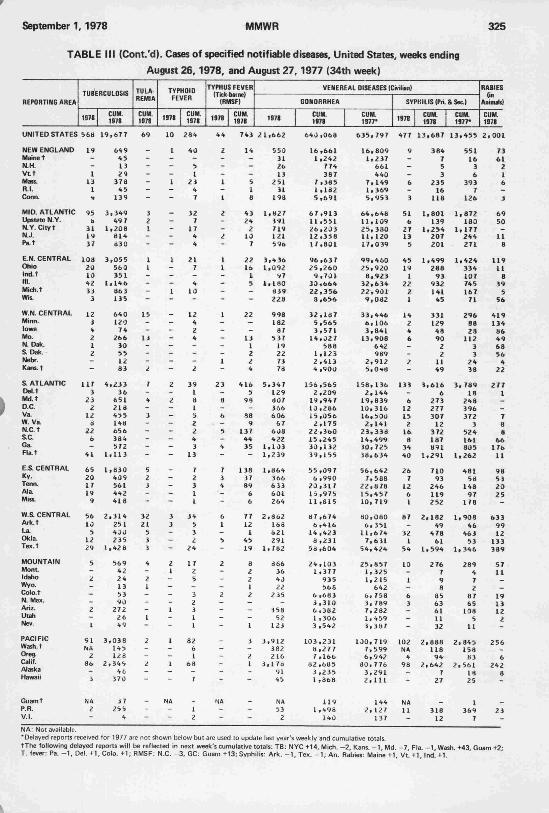
TABLE III (Cont.'d). Cases of specified notifiable diseases. United States, weeks ending
August 26,1978, and August 27, 1977 (34th week)
REPORTING AREA
TUBERCULOSIS
1978
UNITED STATES 568
NEW ENGLAND
Maine t
N.H.
Vtt
Mass.
R.I.
Conn.
MID. ATLANTIC
Upstate N.Y.
N.Y. Cityt
N.J.
Pat
E.N. CENTRAL
Ohio
IndT
III.
Mich.t
Wis.
W.N. CENTRAL
Minn.
Iowa
Mo.
N. Dak.
S. Dak.
Nebr.
Kam.t
& ATLANTIC
Del.t
k Md.t
1 D.C." Va.
W. Va.
N.C.t
S.C.
Ga.
Flat
E.S. CENTRAL
Ky.
Tenn.
Ala
Miss.
W.S. CENTRAL
Ark.t
La.
Okla.
Tex.t
MOUNTAIN
Mont.
Idaho
Wyo.
Colo.t
N. Mex.
Ariz.
Utah
Nev.
PACIFIC
Wash.t
Oreg.
Calif.
Alaska
Hawaii
Guamt
P.R.
V.I.
19
-
—
1
13
1
«♦
95
It
31
19
37
108
za
10
42
33
3
12
i
'♦
2
1
2
-
-
117
3
23
2
12
ZZ
6
—
41
65
20
17
19
9
56
U
5
12
29
5
-
2
-
—
-
2
-
1
91
Nm
2
86
-
3
NA
2
-
CUM.
1978
19,677
649
45
13
29
378
45
139
3,349
49 7
1,208
814
S30
3,055
560
351
1,146
86 3
135
640
120
74
266
30
55
12
83
4,233
36
651
218
455
148
656
384
572
1,113
1,830
409
561
442
418
2,314
251
400
235
1,42 6
569
42
24
13
53
90
272
26
49
3,038
145
128
2.34S
46
370
37
25 5
4
TULA
REMIA
CUM.
1978
69
_
-
-
—
-
-
-
3
2
I
-
-
1
1
-
-
-
-
15
-
-
-
-
-
2
7
-
4
-
3
-
-
-
-
-
5
2
J
-
-
32
21
5
3
3
4
-
2
1
-
-
-
1
-
2
-
-
2
-
_
-
—
TVPHOIO
FEVER
1978
10
1
-
—
—
1
—
-
_
-
-
—
-
1
-
-
-
1
-
_
-
-
—
—
—
-
-
2
—
2
—
—
—
—
—
—
-
_
-
-
—
-
3
3
—
-
-
2
1
—
—
-
-
1
—
-
1
-
-
—
NA
-
—
CUM.
1978
284
40
-
5
1
Zi
4
7
32
7
17
4
4
21
7
-
4
10
-
12
4
2
4
-
-
-
2
39
1
8
1
5
2
2
4
3
13
7
2
3
1
1
34
5
3
2
24
17
2
5
-
3
2
3
1
1
82
6
1
68
-
7
_
1
2
TYPHUS FEVER
(Tick-borne)
(RMSF)
1978
44
2
-
-
-
1
-
1
2
-
-
2
-
1
1
-
—
-
-
1
-
-
-
-
-
1
-
23
-
8
-
6
- —
5
-
4
-
7
3
4
—
-
6
1
-
5
-
2
-
-
—
2
-
-
-
-
_
-
-
-
-
NA
-
-
CUM.
1978
743
14
-
—
—
5
1
8
43
24
2
10
7
22
16
1
5
—
-
22
—
-
13
1
2
2
4
416
5
99
-
88
9
137
44
35
-
138
37
89
6
6
77
12
1
45
19
8
2
2
1
2
—
—
—
I
3
-
z
I
-
-
_
-
—
21
1
3
1
1
5
1
1
1
2
1
3
3
1978
,662
550
31
26
13
251
31
198
,1127
391
719
121
596
,4 36
,092
97
,180
839
223
998
182
87
5 37
19
22
73
78
.347
129
807
366
606
67
6J8
422
,103
,239
,864
366
633
601
2 64
,862
168
621
291
,782
d66
36
40
22
235
-
358
52
123
.912
3 82
216
,17a
91
45
NA
53
2
VENERF.AL DISEASES (C
GONORRHEA
CUM.
1978
640,068
16,661
1,242
774
387
7,385
1,182
5,691
67,913
11,551
26,203
12,358
17,801
96,637
25,260
9,701
30,664
22,356
8.656
32,187
5,565
3,571
14,027
588
1,123
2,413
4,900
156,565
2 ,209
19,947
10,286
15,056
2,175
22,360
15,245
30,132
39,155
55,097
6,990
20,317
15,975
11,815
87 ,674
6,416
14,423
8 ,231
5a,604
24,103
1,377
935
568
6,683
3,310
6 ,382
1 .306
3,542
103,231
b,277
7 ,166
82,685
3,235
1 ,868
119
1 ,496
140
CUM.
1S77*
635,797
16,809
1,237
661
440
7,149
1,369
5,953
64,646
11,109
25,330
11,120
17,039
99,460
25,920
8,923
32,634
22,901
9,0d2
33,446
6,106
3,841
13,908
642
989
2,912
5,0-»8
158,136
2,144
19,839
10,316
16,530
2,141
23,338
14,499
30,725
38,634
56,642
7,588
22,878
15,457
10,719
80,080
6,351
11,674
7,631
54.424
25,857
1,325
1,215
642
6, 758
3,789
7,282
1,459
3,387
100,719
7,5 99
6,942
80,776
3,291
2,111
144
2, 127
137
viiian)
SYPHILIS (Pri
1978
477
9
-
—
_
6
-
3
51
6
27
13
5
45
19
1
22
2
1
14
2
4
6
-
-
2
-
133
_
6
12
15
2
16
8
34
40
26
7
12
6
I
87_
32
1
54
10-
1
—
6
3-
_
-
102
NA
4
98
_
-
NA
11_
CUM.
1978
13,687
384
7
5
3
235
16
US
1,801
139
1,254
207
201
1.49S
288
93
932
141
45
331
129
48
10
2
2
11
49
3,616
6
273
277
307
12
372
187
891
1,291
710
93
246
119
252
2,182
49
478
61
1,594
2 76
7
9
8
85
63
61
11
32
2,888
118
94
2,642
7
27
318
12
SSec.)
EuS1977*
13,455
551
16
3
6
393
7
126
1,872
180
1,177
244
271
1,424
334
107
745
167
71
296
88
28
112
3
3
24
38
3,789
18
243
396
372
3
524
161
805
1,262
481
58
148
97
178
1,908
46
463
53
1,346
289
4
7
2
87
65
108
5
11
2,845
158
83
2,561
18
25
1
369
7
RABIESIn
Animals)
CUM.
1978
2,001
73
61
2
1
6
—
3
69
50
11
8
119
11
8
39
5
56
419
134
86
49
68
56
4
22
277
1
_
7
a
8
66
17b
11
98
53
20
25
633
99
12
133
389
57
11
_
19
13
12
2
256
6
242
8
23
lived for 1977 are not shown b
ing delayed reports will be reflected in next week
Pa. -1, Del. +I.C0I0. +1; RMSF: N.C. -3, GC: Gu
but are used to update last year's v
eflected in next week's cumulative totals: TB: NYC +14, Mich. -2, Kans. -1 Md. -7 Fla -1 Wash +43 Gua
SF: N.C. -3, GC: Guam +13; Syphilis: Ark. -1, Tex. -1; An. Rabies: Maine+1, Vt.+1, Ind. +1.

September 1,1978
TABLE IV. Deaths in 121 U.S. cities,* week ending
August 26,1978 (34th week)
ALL CAUSES. BY AGE (YEARS)
REPORTING AREA
Bridgeport. Conn.
Cambridge, Mass.
Fall River, Mass.
Hartford, Conn.
Lowell. Mass.
Lynn, Mass.
New Bedford, Mass.
New Haven, Conn.
Springfield, M
Waterbury, Conn.
Worcester, Mass.
MID. ATLANTIC
Albany, N.Y.
Allentown, Pa
Buffalo, N.Y.
Camden, N.J.
Elizabeth. N.J.
Jersey City, N.J.
Newark. N.J.
N.Y. City. N.Y.
Paterson, N.J.
Philadelphia. Pa.
Pittsburgh. Pa
Reading, Pa
Rochester. N.Y.
Schenectady. N.Y.
ton. Pa
Syracuse. N.Y.
Trenton. N.J.
. N.Y.
Yonkers. N.Y.
REPORTING AREA
24 S. ATLANTIC
5 Atlanta, Ga
4 Baltimore. Md.
I Charlotte. N.C.
Jacksonville, Ft
1 Norfolk. Va
1 Richmond. Va.
1 Savannah, Ga
St. Petersburg, Fla
5 Tampa, Fla
I Washington, D.C.
E.S. CENTRAL
Birmingha
131 Chattanoc
2 Knoxville, T
1 Louisville. Ky
7 Memphis. Tr
- Mobile. Ala
1 Montgomery, Ala
- Nashville, Tenn.
57 W.S. CENTRAL5 Austin, Tex.
3 ° Baton Rouge. La2 Corpus Christi. Te
EIP
Fort Worth, Tex.
1 New Orle~ San Anto.Mu,
? Shreveport, La
Tulsa. Okla.
ALL CAUSES. BY AGE (YEARS)
>65 45-64 2544
976 533
139 65
211 110
2M«
96
28
22
Li49
5
17
P&l**
TOTAL
34
5
6
EN. CENTRAL
Akron. Ohio
Canton. Ohio
Chicago. III.
Cincinnati, Ohio
Cleveland, Ohio
Dayton, Ohio
Detroit, Mich,
lie. Ind.
Fort Wayne, Ind.
Gary, Ind.
Grand Rapids. Mich.
Indianapolis. Ind.
Madi—
,171 1,305
37 19
33 24
494 299
145 87
178 114
140 78
105 67
Peoria, III.
Rockford. III.
South Bend. Ind.
Toledo. Ohio
Youngstown, Ohil
W.N. CENTRAL
Des Moines, Iowa
Duluth, Minn.
Kansas City, Kans.
"—as City, Mo.
oln, Nebr.
Omaha, Nebr.
St. Louis, Mo.
St. Paul. Minn.
•Mortality data in this table
reported by the place of it!
"Pneumonia and influenza
MOUNTAIN
Albuquerque, N. Mex
Colo. Springs, Colo.
Denver, Colo.
Las Vegas, Nev.
Ogden, Utah
Phoenix, Ariz.
Pueblo. Colo.
Salt Lake City. Utah
Tucson. Ariz.
PACIFIC
Berkeley. Calif.
Fresno. Calif.
Glendale, Calif.
Honolulu, Hawaii
Long Beach, Calif.
Los Angeles. Calif.
Oakland. Calif.
Pasadena, Calif.
Portland. Oreg.
Sacramento, Calif.
San Diego. Calif.
San Francisco. Calif.
San Jose, Calif.
Seattle, Wash.
Spok
10.662 6,483 2,537 71S
10,866 6,521 2,794 713
nost of which have populations of 100,000 or

September 1, 1978
Q Fever — Continued
Since the first described outbreak in this country in 1946 (3), numerous outbreaks
usually associated with cattle, sheep, and goats have been investigated. Various species
of ticks (including A. nuttalli) carry the rickettsial organisms, but man is usually infected
by inhaling aerosolized particles containing C. burneti.
Reptiles have rarely been documented as potential hosts for C. burneti (4). Never
theless, physicians seeing patients with a compatible illness and a history of ownership
of pythons or other exotic pets should consider Q fever in their differential diagnosis,
obtain suitable acute and convalescent blood specimens for serologic diagnosis, and
report the illness to local and state health authorities.
References
1. Hoeprich PD (ed): Infectious Diseases: A Modern Treatise of Infectious Processes. New York,
Harper and Row, 1977, pp 288-289
2. Freeman G, Hodson ME: Q fever endocarditis treated with trimethoprim and sulphamethoxasole.
Br Med J 1:419-420, 1972
3. Irons JV, Topping WH, Shepard CC, Cox HR: Outbreak of Q fever in the United States. Public
Health Rep 61:784-785, 1946
4. Tendeiro J: Nota previa sobre febre Q. Gaz Med Portuguesa 5:645-649, 1952
Recommendation of the Public Health Service
Advisory Committee on Immunization Practices
Meningococcal Polysaccharide Vaccines
INTRODUCTION
Polysaccharide vaccines against diseases caused by Neisseria meningitidis serogroups A
and C are now licensed in the United States. They are prepared as monovalent and as
bivalent antigens. The purpose of this statement is to summarize available information
on these antigens and to offer general guidance regarding their role in the control of epi
demics of meningococcal disease in the civilian population of the United States.
MENtNGOCOCCAL DISEASE
Meningococcal disease is endemic in the United States and throughout the world. It
caused serious epidemics approximately every 10 years from 1900 to 1945 in this coun
try. The fact that it also regularly caused outbreaks among military recruits was a catalyst
for the development of serogroup-specific vaccines.
During the last decade an estimated 3,000-6,000 cases a year of meningococcal disease
occurred in the United States. From 1964 to 1968 and since 1972, the serogroup most
often isolated from patients has been serogroup B. From 1969 through 1971 serogroup
C was most common in the civilian and military populations. Serogroup A was only
rarely identified until the occurrence recently of small outbreaks in several cities of the
Pacific Northwest. In 1971 the Armed Forces began administering serogroup C meningo
coccal polysaccharide vaccine routinely to all recruits. Since then, the incidence of men
ingococcal disease in the military has declined sharply, and serogroup C disease has been
virtually eliminated in that population.
Sulfa-sensitive serogroup B strains currently cause the majority of U.S. cases. Highest
attack rates are in infants. Serogroup C strains account for about one-third of cases. Al
though the highest age-specific attack rate for serogroup C is also in infants, about 70% of
serogroup C cases occur in persons over 2 years old. More than two-thirds of all meningo
coccal disease occurs in patients less than 20 years old.
September 1, 1978
Meningococcal Vaccine — Continued
In recent years meningococcal disease in civilians has occurred primarily as single iso
lated cases or, infrequently, as small, localized clusters. Secondary cases occur more fre
quently in household contacts than in the general population, and appropriate antibiotic
prophylaxis has been the principal means of reducing the risk for immediate contacts
of cases.
MENINGOCOCCAL VACCINES
Three meningococcal polysaccharide vaccines, monovalent A, monovalent C, and
bivalent A-C vaccine,* are licensed for selective use in the United States. These vaccines
are chemically defined antigens consisting of purified bacterial capsular polysaccharide,
each inducing specific serogroup immunity. The duration of immunity conferred by each
vaccine is unknown.
Serogroup A vaccine was evaluated in 62,000 Egyptian schoolchildren 6-15 years old
and appeared to be highly effective and not to induce any serious side effects. When used
to control an outbreak in Brazil, it appeared to be effective in all age groups beyond the
first year of life. Further confirmation of effectiveness was found in children of ages 3
months-5 years in a vaccine trial carried out in Finland. Serogroup A vaccine has also
been used to control outbreaks in the United States in Portland, Seattle, Anchorage, and
Fairbanks.
Serogroup C vaccine has been given routinely to American military recruits since
October 1971. More than 500,000 young adults have been vaccinated without significant
adverse reactions. Serogroup C vaccine has been studied in infants, preschool and school-
age children, and adults. It elicited antibody in all age groups, although older children and
young adults had the highest levels. Serogroup C vaccine does not appear to be effective
in children less than 2 years of age.
VACCINE USAGE
General Recommendations
Routinely vaccinating civilians with meningococcal polysaccharide vaccines is not
recommended because of insufficient evidence of its value when the risk of infection is
low. The serogroup-specific monovalent vaccines should be used, however, to control out
breaks of meningococcal disease caused by N. meningitidis serogroup A or C.
Vaccine may be of benefit for some travelers planning to visit countries recognized as
having epidemic meningococcal disease. Although cases among Americans traveling in
such areas are rare, prolonged contact with the local populace could enhance the risk of
infection and make vaccination a reasonable precaution.
Vaccination should be considered an adjunct to antibiotic chemoprophylaxis for
household contacts of meningococcal disease cases caused by serogroups A or C. This is
because half the secondary family cases occur more than 5 days after the primary case-
long enough to yield potential benefit from vaccination if the antibiotic chemoprophy
laxis has not been successful.
Primary Immunization
For both adults and children, vaccine is administered parenterally as a single dose in
the volume specified by the manufacturer.
PRECAUTIONS AND CONTRAINDICATIONS
Reactions
Adverse reactions to meningococcal vaccine are infrequent and mild, consisting princi
pally of localized erythema lasting for 1-2 days.
'Official names: Meningococcal Polysaccharide Vaccine, Group A; or , Group C; or , Groups A & C

0345 4September 1,197? ■ ' **IMWR II 329
Meningococcal Vaccine — Continued \\ HI I 11 11 I I Ml3 0001 00128 1270
Pregnancy
The safety of meningococcal vaccines in pregnant women has not been established. On
theoretical grounds, it is prudent not to use them unless there is a substantial risk of in
fection.
EPIDEMIC CONTROL
In an epidemic of meningococcal disease due to serogroups A or C, the population at
risk should be identified. It should be delineated by neighborhood, census tract, or other
reasonable boundary. If there is ample vaccine, all residents in that area should be vac
cinated. If not, persons expected or known to be at highest risk of disease by virtue of
age, socioeconomic status, or area of residence should receive priority vaccination.
SELECTED BIBLIOGRAPHY
Artenstein MS, Winter PE, Gold R, et at: Immunoprophylaxis of meningococcal infection. Milit
Med 139:91-95, 1974
Peltola H, Makela PH, Kayhty H, et al: Clinical efficacy of meningococcus group A capsular poly-
saccharide vaccine in children three months to five years of age. N Engl J Med 297:686-691, 1977
Wahdan MH, Rizk F, el-Akkad AM, et al: A controlled field trial of a serogroup A meningococcal
polysaccharide vaccine. Bull WHO 48:667-673, 1973
Revision of MMWR 24:381-382, 1975
The Morbidity and Mortality Weekly Report, circulation 78,750, is published by the Center for
Disease Control, Atlanta, Georgia. The data in this report are provisional, based on weekly tele
graphs to CDC by state health departments. The reporting week concludes at close of business on
Friday; compiled data on a national basis are officially released to the public on the succeeding Friday.The editor welcomes accounts of interesting cases, outbreaks, environmental hazards, or other
public health problems of current interest to health officials. Send reports to: Center for Disease
Control, Attn: Editor, Morbidity and Mortality Weekly Report, Atlanta, Georgia 30333.
Send mailing list additions, deletions, and address changes to: Center for Disease Control, Attn:
Distribution Services, GSO, 1 SB-36, Atlanta, Georgia 30333. When requesting changes be sure to
give your former address, including zip code and mailing list code number, or send an old address label.

September 1, 1978
U.S. DEPARTMENT OF HEALTH, EDUCATION. AND WELFARE
PUBLIC HEALTH SERVICE / CENTER FOR DISEASE CONTROL
ATLANTA, GEORGIA 30333 OFFICIAL BUSINESS
Director, Center for Disease Control
William H. Foege, M.D.
Director, Bureau of Epidemiology
Philip S. Brachman, M.D.
Editor
Michael B. Gregg, M.D.
Managing Editor
Anne D. Mather, M.A.
Chief, MMWR Statistical Activity
Dennis J. Bregman, M.S.
Postage and Fees Paid
U.S. Department of HEW
HEW 396
Creighton University
Health Sciences Library
2500 California Street
Omaha, NE 68178
421X3
HEW Publication No. (CDC) 78-8017 Redistribution using indicia is illegal.






![17 - Era_de_Apocalipsis_Xman_N1_por_Mall[CRG][].pdf](https://static.fdocuments.in/doc/165x107/577cdee01a28ab9e78affbb2/17-eradeapocalipsisxmann1pormallcrgwwwcomicreltkpdf.jpg)











