Energy Vision2020 VOLUME ONE - TVA
21
3/5/2013 1 Jointly sponsored by AACE and CME-University Lewis S. Blevins, Jr., M.D. Hyponatremia: Epidemiology • 15% of hospitalized patients • Serum sodium of <130 mEq/L – Incidence of 1% and prevalence of 2.5% – 67% of cases were hospital acquired • Settings – ICU 30% – SAH30% – TBI 12% – CHF28% – HIV 30% Anderson RJ, et al. Ann Intern Med. 1985;102:164-168.
Transcript of Energy Vision2020 VOLUME ONE - TVA

3/5/2013
1
Jointly sponsored by AACE and CME-University
Lewis S. Blevins, Jr., M.D.
Hyponatremia: Epidemiology
• 15% of hospitalized patients
• Serum sodium of <130 mEq/L– Incidence of 1% and prevalence of 2.5%
– 67% of cases were hospital acquired
• Settings– ICU 30%
– SAH30%
– TBI 12%
– CHF28%
– HIV 30%
Anderson RJ, et al. Ann Intern Med. 1985;102:164-168.

3/5/2013
2
Risk of Hyponatremia Increases with Age
Hawkins RC. Clin Chim Acta. 2003;337:169-172.
Hyponatremia in the Elderly
• Overall incidence of [Na+] <137 mmol/L ~7% 1
• Prevalence increases to 18-22% in chronic care
facilities, with 53% incidence of one or more
episodes of hyponatremia 2,3
• Mortality rate = 16% for patients over 65 with
hyponatremia versus 8% for those without
hyponatremia on admission 4
1. Caird FI, et al. Br Heart J. 1973; 35: 5 527-530. 2. Kleinfeld M, et al. Geriatr Soc .1979;27:156-161.
3. Miller MJ. J Am Geriatr Soc. 1995:43:1410-1413. 4. Terzian C, et al. J Gen Intern Med. 1994; 9:89–91

3/5/2013
3
Relationship Between Hospital Admission
Serum [Na+] and In-hospital Mortality
Wald R, et al. Arch Intern Med. 2010; 170:294-302.
0.20
0.15
0.10
0.05
110 115 120 125 130 135 140 145
Admission Serum [Na+] Concentration (mEq/L)
Predicted Probability of
In-Hospital Mortality
Hyponatremia and Mortality
1. Anderson RJ et al. Ann Intern Med. 1985;102:164-168. 2. Terzian C et al. J Gen Intern Med. 1994; 9:89–91.
3. Tierney VM, et al. J Gen Intern Med. 1986; 1:380-85.
3/5/2013
4
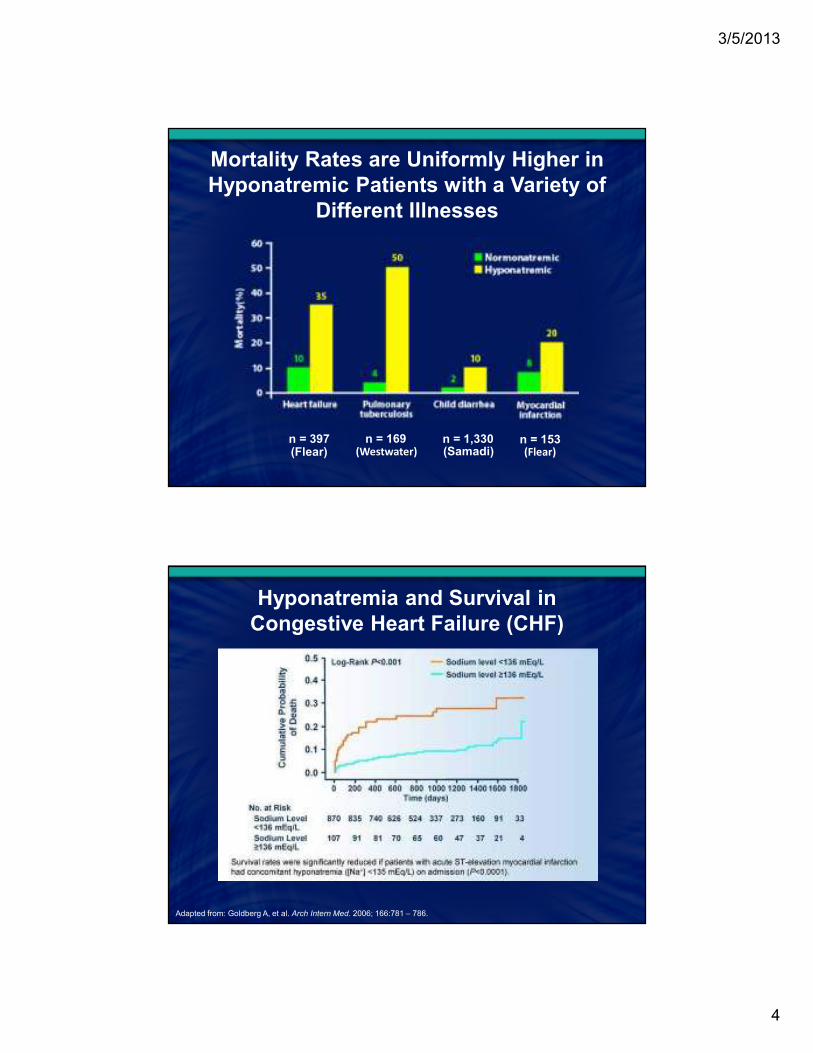
Mortality Rates are Uniformly Higher in
Hyponatremic Patients with a Variety of
Different Illnesses
n = 397 n = 169 n = 1,330 n = 153(Flear) (Westwater) (Samadi) (Flear)
Hyponatremia and Survival in
Congestive Heart Failure (CHF)
Adapted from: Goldberg A, et al. Arch Intern Med. 2006; 166:781 – 786.

3/5/2013
5
Hyponatremia in Cirrhosis
Impact on Survival
Kim R, et al. N Engl J Med. 2008; 359:1018-1026.
Neurohypophysis
• Arginine vasopressin
(AVP) secreting neurons
in SON and PVN
• Osmo- and thirst
receptors/centers in
anterior hypothalamus
• Ascending pathways from
ANS and brainstem
• Terminal boutons in
neurohypophysis

3/5/2013
6
Relationship between Plasma
Osmolarity and AVP
Arginine Vasopressin (AVP) Receptors
RECEPTOR LOCATION EFFECT
V1AVascular smooth
muscle, platelets
Vasoconstriction,
platelet aggregation
V1B Anterior pituitary ACTH release
V2Renal collecting
duct cellsFree water absorption

3/5/2013
7
Aquaporins
Adapted from Kaira PR, et al. Cardiovasc Res. 2001; 51:495-509.
Relationship between
Urine Osmolarity and AVP

3/5/2013
8
AVP Dynamics
Hyponatremia:
One of Many Algorithms
Adapted from Kumar S, & Berl T. Atlas of Diseases of the Kidney. 1999; 1.1-122.

3/5/2013
9
Clinical Features of CSW and SIADH
CSW SIADH
ECF* Decreased Increased
Hematocrit Increased Normal
Plasma albumin concentration Increased Normal
Plasma BUN/creatinine Increased Decreased
Plasma [K+] Normal or increased Normal
Plasma uric acid Normal or decreased Decreased
Treatment Normal saline Fluid restriction
*Determination of ECF is the primary way to differentiate CSW from SIADH.
BUN=blood urea nitrogen; CSW=cerebral salt wasting.
Palmer BF. Trends Endocrinol Metab. 2003; 14:182 – 187.
Unifying Hypothesis of Sodium and Water
Dysregulation After SAH
Mayer SA. The Neurologist. 1995; 1:71-85.

3/5/2013
10
Hyponatremia
• Disorders or processes that cause hyponatremia
are dynamic:
– Initiation
– Maintenance
– Recovery
• It is critical to ascertain where the patient might
be in their course as one initiates and measures
a response to management
Hyponatremia: Symptoms and Signs
FEATURE %
Nausea/Vomiting 71
Delirium/Confusion 50
Weakness 50
Lethargy 50
Myalgia/Cramps 21
Dizziness 21
Hiccups 14
Dysarthria 14
Illowsky BP, et al. Medicine. 1993; 72:359-373.
Headache!!!

3/5/2013
11
Correction of Hyponatremia Normalizes Gait
Stability in “Asymptomatic” Hyponatremia
serum [Na+] = 124 mEq/L
-500 -400 -300 -200 -100 -100 -2000
-40
-60
-80
0
-100
-120
140
-20
120
100
80
60
40
20
serum [Na+] = 130 mEq/L
-500 -400 -300 -200 -100 -100 -200
80
60
40
20
-20
-40
-60
-80
0
-100
-120
serum [Na+] = 139 mEq/L
100 200 200-500 -400 -300 -200 -100
80
60
40
20
-20
-40
-60
-80
0
-100
-120
serum [Na+] = 135 mEq/L
100 200 200-400 -300 -200 -100
80
60
40
20
-20
-40
-60
-80
0
-100
-120
100
Renneboog B, et al. Am J Med. 2006; 119:71.
Severe Hyponatremia168 patients Na+ <115 mEq/L
Nzerue CM, et al. J Natl Med Assoc. 2003;95:335-43.

3/5/2013
12
Treatments for Hyponatremia
Isotonic saline infusion
Hypertonic saline infusion
Vaptans: conivaptan, tolvaptan
Fluid restriction
Demeclocycline
Furosemide + NaCl
Mineralocorticoids
Urea
Vaptans: tolvaptan
long-term
short-term
Judicious use of 3% Saline
• Hyponatremic patients with significant
neurological symptoms, such as seizures,
severe altered mental status, or coma.
• The high likelihood of cerebral edema outweighs
the risk of possible demyelination.
• Target rate of correction is 1.5 to 2 mEq/L per
hour with 3% hypertonic saline for the first 3 to
4 hours, or more briefly, if symptoms improve or
the sodium level exceeds 120 mEq/L.

3/5/2013
13
Formula for Estimating Sodium Needs
3% Saline: An Alternative Approach
• Rate in mL/h is the desired rate of rise in Na+ in
mEq/L/h per kg body weight.
• Furosemide 20 mg iv.
• For a 70 kg patient with desired correction rate
of 1.5 mEq/L 3% saline infusion rate would be
105 mL/h.

3/5/2013
14
Fluid Restriction
?
Vasopressin Receptor Antagonists
DRUG ROUTE RECEPTOR EFFECTIVE DOSES
Conivaptan IV/Oral V1/V2 20-40 mg/d
Tolvaptan Oral V2 15-60 mg/d
Adapted from Ellison DH,& Berl T. N Engl J Med. 2007; 356:2064-2072.

3/5/2013
15
Conivaptan IV
8-10% experience rapid correction
Verbalis JG, et al. Clin Endocrinol (Oxf). 2008 Jul;69(1):159-68.
Conivaptan IV
Verbalis JG, et al. Clin Endocrinol (Oxf). 2008 Jul;69(1):159-68.

3/5/2013
16
SALT 1 and 2:
Mean Sodium Concentration Over Time
Schrier RW, et al. N Engl J Med. 2006;355:2099-2112.
Hyponatremia
Verbalis JG. TEM. 1992;3(1):1-7.

3/5/2013
17
Hyponatremia: Outcomes of Correction
Sterns RH, et al. J Am Soc Nephrol. 1994; 4:1533- 1530.
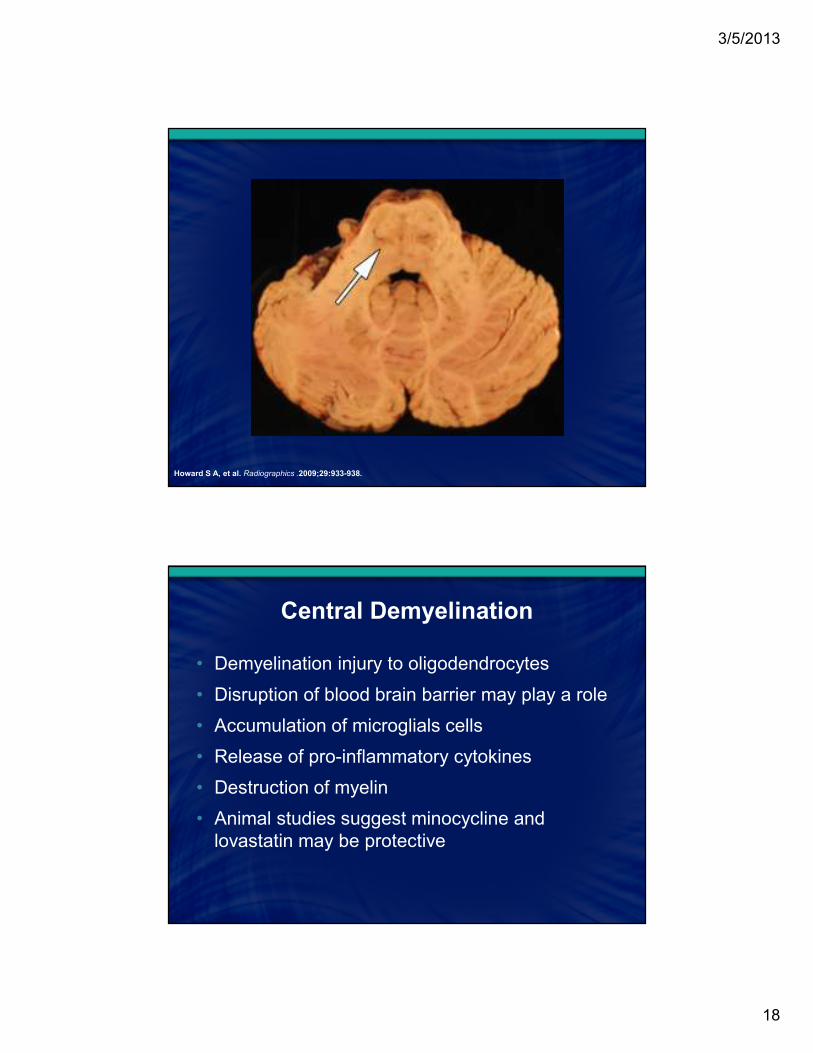
Osmotic Demyelination
Central Pontine Myelinolysis
Central Demyelination Syndrome
3/5/2013
18
Howard S A, et al. Radiographics .2009;29:933-938.
Central Demyelination
• Demyelination injury to oligodendrocytes
• Disruption of blood brain barrier may play a role
• Accumulation of microglials cells
• Release of pro-inflammatory cytokines
• Destruction of myelin
• Animal studies suggest minocycline and
lovastatin may be protective

3/5/2013
19
Clinical Features of Osmotic Demyelination
FEATURE %
Mutism/Dysarthria 71
Lethargy/Obtundation 57
Behavioral changes 29
Confusion 21
Movement difficulty 21
Muscle contractions 7
Dusphagia 7
Spasticity, rigidity, Babinski reflex, hyperreflexia, impaired gag reflex,
fasciculations, nonreactive or dilated pupils, snout, grasp or rooting reflexes,
impaired gait, ataxia,cognitive deficits.
Illowsky BP, et al. Medicine. 1993; 72:359-373.
Reducing Risks of Myelinolysis
• Limit correction of chronic hyponatremia to 10 to 12
mmol/L in 24 hours and to 18 mmol/L in 48 hours.
• When other recognized risk factors for myelinolysis
are present (menstruant women, hypokalemia, liver
disease, poor nutritional state, alcoholism, burns),
correction should not exceed 10 mEq/L/24h.
• In acute hyponatremia a more rapid initial
correction rate, roughly 1-2 mEq/L, is acceptable.
3/5/2013
20
Mismanagement of Hyponatremia
• 104 patients with Na+ <125 mEq/L in a 6 month period
• 42% of diagnoses incorrect
• 33% of patients with significant management errors
• Overall mortality 27%
– 41% in those with errors in management
– 20% in those managed appropriately
Huda MSB, et al. Postgrad Med J .2006; 82: 216–219.
Hyponatremia
The Endocrinologists Role
• Understand the epidemiology and
pathophysiology of hyponatremia
• Devise a systematic approach to the evaluation
of patients with hyponatremia
• Individualize therapy based on pathophysiology
• Educate colleagues and trainees
– Consultations
– Grand Rounds and other presentations
– Discussions

3/5/2013
21